Embed Size (px)
Citation preview


�
Contents
Foreword 2
Chapter 1. Skeletal-related events: clinical context 3Hypercalcemiaofmalignancy 3Multiplemyeloma 8Advancedmalignanciesinvolvingbone 8Metabolicbonedisorders �0
Chapter 2. Skeletal-related events: management options 15Hypercalcaemiaofmalignancy �5Multiplemyeloma �6Advancedmalignanciesinvolvingbone �8Metabolicbonedisorders �9
Chapter 3. Zoledronic acid: clinical evidence for efficacy and safety 23Hypercalcemiaofmalignancy 23Multiplemyeloma 25Advancedmalignanciesinvolvingbone 26 breastcancer 27 lungcancer 3� renalcancer 33 prostatecancer 34Metabolicbonedisorders 37 Paget’sdiseaseofbone 37 osteoporosis 38 rheumatoidarthritis 39Additionalpotentialapplicationsofzoledronicacid 40
Chapter 4. Zoledronic acid: management issues 43Pharmacological profile 43Infusionprotocol 44Durationofbisphosphonatetherapy 44Managingbisphosphonate-relatedadverseevents 44
Conclusions 47

2
Foreword
Zoledronicacidisahighlypotentandwell-toleratedintravenousbisphosphonatewidelyusedforthemanagementofhypercalcemiaofmalignancy,multiplemyeloma,andadvancedmalignanciesinvolvingbone,includingbreast,prostate,lung,andothersolidtumormetastases.ZoledronicisalsolicensedinnumerouscountriesforthemanagementPaget’sdiseaseofboneandclinicaltrial data support the efficacy of this bisphosphonate in further metabolic bone diseases including postmenopausal osteoporosis and rheumatoid arthritis. In all patient groups, the benefits of zoledronicacidincludereversalofboneloss,reductioninfracturerates,alleviationofpain,andimprovementsinqualityof life.Inpivotaltrials,zoledronicaciddemonstratessuperiorityoverplacebo and intravenous pamidronate in terms of efficacy, tolerability, and patient acceptability.
This book appraises the clinical benefits of zoledronic acid across its wide range of clinical applications,basedontheextensivepublishedevidencebase.
ProfessorPierFrancoConteDepartmentofOncologyandHematologyUniversityofModenaandReggioEmiliaModena,Italy

3
Skeletal-related events: clinical context
Chapter 1.
Zoledronic acidhas clinical applications in a rangeof conditions including hypercalcemia ofmalignancy, multiple myeloma, bone metastases, and metabolic disorders, which have incommonunderlyingpathologicalprocesses.Theclinicalbackgroundtotheseskeletal-relatedeventsisthefocusofthischapter.
Hypercalcemia of malignancyHypercalcemiaofmalignancyandprimaryhyperparathyroidismtogetheraccountformorethan90%ofallcasesofhypercalcemia.Forthisreason,otherpossiblecausesofelevatedserumcalcium are usually not considered as potential diagnoses until malignancy and parathyroiddiseaseareexcluded(Table 1).
Hypercalcemiaofmalignancyisaseriousandunpleasantskeletalcomplicationthatcanoccurbothinthepresenceandabsenceofmetastases,andaffects�0-20%ofallcancerpatientsatsometimeduringtheirdisease, including20-40%ofpatientswithadvanceddisease(Mundyetal�984;Vassilopoulou-Sellinetal�993;Wattersetal�996).Patientswithhypercalcemiaof malignancy generally have a poor prognosis with a life expectancy of weeks to months.Duringthatperiod,managementisachallengebecauseoftheunpleasantgastrointestinalandneurologicalsymptoms.
PathophysiologyHypercalcemia of malignancy can be divided into two types with different pathogeneses:osteolytic and humoral. Osteolytic hypercalcemia results from direct destruction of bone byprimary or metastatic tumor cells that release osteoclastic activating factors. These factorsactlocallytoincreasetheactivityofosteoclasts(bone-resorbingcells)withoutcorrespondingincreasesintheactivityofosteoblasts(bone-formingcells).Humoralhypercalcemiaismediatedby circulating factors including parathyroid hormone (PTH)-related protein (PTHrP) (Warrell�997).PTHrPissimilarinstructuretoPTHandactstoincreaseboneresorptionwhiledecreasingcalciumexcretionattherenaltubules(Broadusetal�988;Horiuchietal�987;Suvaetal�987).Approximately25%ofpatientswithhypercalcemiaofmalignancyhaveelevatedPTHrPlevels.
ThereareadditionalcirculatinggrowthfactorsinvolvedinhumoralhypercalcemiabesidesPTHrP,includingtransforminggrowthfactor-alphaand-beta,interleukin-�and-6,tumornecrosisfactor-alphaand -beta,prostaglandins,cathepsins,andosteoprotegerin ligand (Figure 1).Furthermediators that await identification may also be involved in the complex interactions that stimulate osteoclastactivity.

4
Table 1. Causes of hypercalcemia
Malignancy
Parathyroid diseasePrimaryhyperparathyroidismSporadic,familial,associatedwithmultipleendocrineneoplasiaIorIITertiaryhyperparathyroidismAssociated with chronic renal failure or vitamin D deficiency
Other endocrine disordersHyperthyroidismAdrenal insufficiency AcromegalyPheochromocytomaAintoxication(includinganalogsusedtotreatacne)
Vitamin D-relatedVitaminDintoxicationUsually25-hydroxyvitaminD2inover-the-countersupplementsGranulomatousdiseasesarcoidosis,berylliosis,tuberculosisHodgkin’slymphoma
MedicationsThiazidediuretics(usuallymild)LithiumMilk-alkalisyndrome(fromcalciumantacids)Vitamins
Genetic disordersFamilialhypocalciurichypercalcemia:mutatedcalcium-sensingreceptor
OtherImmobilization,withhighboneturnover(e.g.,Paget’sdisease,bedriddenchild)Recoveryphaseofrhabdomyolysis

5
Thereislittlecorrelationbetweentheoccurrenceofhypercalcemiaofmalignancyandtheextentofmetastaticbonedisease(Grilletal2000).
Figure 1. Diagram of the molecular interactions between osteoclasts and tumor cells.TGF = transforming growth factor; TNF = tumor necrosis factor; EGF = epidermal growth factor; PGs = prostaglandins; OIF = osteoclast inhibitory factor; OAF = osteoclast activating factor
IncidenceTheincidenceofhypercalcemiaofmalignancyvarieswiththetumortype.Itismostcommoninpatientswithmultiplemyeloma,where30%tomorethan80%ofpatientsareaffected(Wattersetal�996).Some25-65%ofpatientswithmetastaticbreastcanceralsodevelophypercalcemiaofmalignancyduringtheirdisease.Bycontrast,hypercalcemiaofmalignancyisrareinpatientswithprostatecancer.SometypicalincidencesareshowninTable 2.
Tumor Type Percentage of Patients Who Develop Hypercalcemia
Lung 27.3
Breast 25.7
Headandneck 6.9
Unknownprimary 4.7
Lymphoma/leukemia 4.3
Renal 4.3
Gastrointestinal 4.� *Adaptedfrom Lang-KummerJ:Hypercalcemia.In:GroenwaldSL,GoodmanM,FroggeMH,etal.,eds.:CancerNursing:PrinciplesandPractice.4thed.Sudbury,Mass:JonesandBartlettPublishers,�997,pp684-70�.
Table 2. Incidence of Hypercalcemia by Tumor Type

6
SymptomsThe symptoms of hypercalcemia of malignancy typically reflect the underlying cancer type as wellasthedurationoftimeoverwhichthecancerdevelops,thehistoryofcancertreatments,andtheoverallphysicalhealthofthepatientincludingthepresenceofcoexistingcomorbidities.
Symptomsdonotcorrelatecloselywithserumcalciumconcentrations.Somepatientsdevelopsymptomswhencalciumisonlyslightlyelevated,whileotherstoleratehighcalciumlevels(>�3mg/dL,6.5mEq/Lor3.24mmol/L).
The symptoms of hypercalcemia of malignancy are wide-ranging and can be difficult to diagnose withoutsuspicion(Table 3)(Bajorunas�990;Mahon�989).Earlyrecognitionofsymptomsis,however,vitalsince,ifuntreated,hypercalcemiaofmalignancycanprogressrapidlytobecomelife-threatening. Common symptoms include nausea, vomiting, alterations in mental state,constipation,malaise,lethargy,muscleweakness,polyuria,andheadachethatmayprogressto loss of consciousness and coma. Malaise and fatigue are reportedly the most commoncomplaintsatpresentation(Ralstonetal�990).
Thesesymptomscanthemselvescontributetoaworseninginthepatient’scondition.Forexample,nauseaandvomitingcancausedehydrationandincreasedcalciumlevels,whileimmobilizationcausedbyweaknessandlethargymayexacerbatecalciumresorptionfrombone.Fewpatientsexperienceallthesymptomsthatareassociatedwithhypercalcemia,andsomepatientsmayexperiencenone.Intheabsenceofsymptomsofhyercalcemiaofmalignancy,thesymptomsorsignsoftheunderlyingmalignancymayleadthepatienttoseekmedicalattention.

7
Table 3. Symptoms of hypercalcemia of malignancy
RenalNephrolithiasisNephrogenicdiabetesinsipidusDehydrationPolyureaNephrocalcinosis
SkeletalBonepainArthritisOsteoporosisOsteitis fibrosa cystica in hyperparathyroidism (subperiosteal resorption, bonecysts)
GastrointestinalNausea,vomitingAnorexia,weightlossConstipationAbdominalpainPancreatitisPepticulcerdisease
NeuromuscularImpairedconcentrationandmemoryConfusion,stupor,comaLethargyandfatigueMuscleweaknessHeadacheCorneal calcification (band keratopathy)
CardiovascularHypertensionShortenedQTintervalonelectrocardiogramCardiacarrhythmiasVascular calcification
OtherItchingKeratitis,conjunctivitis

8
Multiple myelomaMultiplemyelomaisaprogressiveandincurableplasmacellcancer.Recentadvancesintherapyhave, however, significantly helped lessen the severity of its effects.
PathophysiologyMultiple myeloma is characterized by the proliferation of malignant plasma cells and theproduction of aberrant monoclonal immunoglobulins (IgG, IgA, IgD, or IgE) or Bence-Jonesprotein(freemonoclonalKandAlightchains).
Plasma cell proliferation interferes with blood cell production in the marrow to causeleukopenia, anemia, and thrombocytopenia. The plasma cells may also produce soft tissuemasses(plasmacytomas)andlyticlesionsintheskeleton,causingweaknessandbonepain.Immunoglobulin overproduction causes hyperviscosity, amyloidosis, and renal failure. Theaberrant immunoglobulins may additionally impair humoral immunity, predisposing patientsto infection.Multiplemyelomacanalsoaffect thekidneys in severalways,bydirect tubularinjury,amyloidosis,orinvolvementofaplasmacytoma,andthepresenceofrenalimpairmentisassociatedwithaparticularlypoorprognosis.
IncidenceAnestimated5-6newcasesofmultiplemyelomaoccurper�00000personsperyear.Patientswithmultiplemyelomaexperienceanaverageof twoskeletal eventsayear (Menssenetal2002;Berensonetal�998).
SymptomsMultiple myeloma can be asymptomatic or it may display an array of symptoms includinghypercalcemia, anemia, renal damage, and increased susceptibility to infection. Presentingsymptomstypicallyinvolvebonepain,pathologicfracturesduetoosteoporosis,andweaknessrelatedtoanemia.
Bonepainispresentinapproximately70%ofpatientsatpresentationandmostusuallyinvolvesthelumbarvertebrae.Spinalcordcompressiondevelopsin20%ofpatientsandisoneofthemostsevereadverseeffectsofmyeloma, leadingtobackpain,weaknessorparalysis in thelegs,numbness,ordysesthesia inthe lowerextremities.Onceestablished, theseeffectsarerarelyfullyreversed.
Advanced malignancies involving boneMetastases from solid cancers are the most common tumors that involve the skeleton.The clinical course of metastatic bone disease is typically long and patients may experience bone pain, fractures, hypercalcemia, and spinal cord compression over several years. These complications profoundly impair the patient’s quality of life and their severity can contribute eventually to the patient’s death,independentoftheunderlyingmalignancy.

9
PathophysiologyMetastasesinvolvebonethroughthreemainmechanisms:seedingviathecirculation,directextension, and retrograde venous flow. Once sited within the bone marrow cavity, tumor cellscansecreteavarietyofparacrinefactorsthatstimulatebonecellactivity(Figure2).
Stimulationofosteoclastactivitywithoutaccompanyingincreasesinosteoblastfunctionisofparticularimportanceinmanytumortypes,includingbreastcancers;theresultisosteolysis.Othertumortypesstimulateosteoblastactivitytodepositweakenedbone(sclerosis).Inyetothertumors,bothosteolysisandsclerosiscanbepresentsimultaneously(mixedpattern).These changes in bone cell function characteristically alter levels of serum and urinarymarkersofbonemetabolismthatcanbeusedtomonitordiseaseprogressionandresponsetotherapy.
Inadditiontoweakeningthebone,patientswithbonemetastasesfrequentlyhavereducedmobility,pain,andboneweakness.Together,theseeffectspredisposepatientstofractures,spinalcordcompression,andbonemarrowfailure.Survivalafterthedevelopmentofbonemetastasesrangesfrom6–48months,dependingonthetumortype(Coleman�997).
IncidenceThefrequencyofskeletalinvolvementvarieswiththetumortype.Thetumorsthatmostcommonlyinvolveboneareprostate,lung,bladder,stomach,rectum,andcolontumorsinmenandbreast,uterus, colon, stomach, rectum, and bladder tumors in women.Approximately 80% of menwithadvancedprostatecancer,70%ofwomenwithadvancedbreastcancer,and30-65%ofpatientswithmetastaticlungcancerdevelopbonemetastases(Coleman�997;Coleman�997;Bloomfield 1998; Carlin & Andriole 2000; Pentyala et al 2000).
Skeletaleventsareexperiencedbyapproximatelyonehalfofpatientswithsolid tumorsthat metastasize to bone (Theriault et al �999; Lipton et al �999). Women with breastcarcinomaandbonemetastasesexperienceanaverageoffourskeletalevents,includingtwopathologicfractures,eachyearintheabsenceofeffectivetherapy(Liptonetal�999).Menwithprostatecancerhaveameanannualincidenceof�.5eventsperyear(Saadetal2002),andthisriskincreaseswiththebonelossassociatedwithorchiectomyorhormonaltherapy(Townsendetal�997;Collinsonetal;�994;Daniell�997;Clarkeetal�993).
Figure 2. Interaction of tumor and bone cells within the bone microenvironment.

�0
SymptomsSkeletalsymptomsincludebonepain,fractures,neurologicimpairmentduetospinalcordcompression,andsignsofhypercalcemia.Thedevelopmentofbonepaininapatientknowntohaveaprimary tumor ishighlysuggestiveofbonemetastases. Ingeneral,bonepainintensitydoesnotcorrelatedirectlywithanincreasedfracturerisk,butpainexacerbatedby movement does appear to predict impending fracture. The probability of a fracturealso increaseswiththedurationofmetastatic involvement.Fracturesarethereforemorecommoninpatientswithpredominantlybone-onlydiseasewhootherwisehavearelativelygoodprognosis.
Common sites for metastases are the vertebrae, pelvis, proximal femur, ribs, proximalhumerus, and skull. More than 90% of metastases fall within this distribution. Certaincarcinomasmayhaveapredilectionforparticularskeletalsites.Forexample,primarytumorsarisinginthepelvistendtospreadtothelumbosacralspine,whileone-halfofmetastasesinthehandoriginatefromlungcancers.Bonemetastasesarefrequentlypresentatmultiplesitesbythetimeofdiagnosis.
Skeletalcomplicationscontributeimportantlytothedeteriorationinqualityoflifeandlossofindependenceofcancerpatients;therefore,checkingboneformetastaticdiseaseiscriticalifalesionissuspected.
Metabolic bone disorders
Paget’s disease of bonePaget’s disease of bone is a variably progressive disorder in which normal bone is replaced with disorganized bone that is prone to deformity and fracture.
PathophysiologyPaget’sdiseasebeginswiththeproliferationofabnormallylargeosteoclasts,whichresorbboneup to20 times thenormal rate.This increasedosteoclasticactivity is followedby increasedosteoblastic activity, which produces structurally disorganized bone (‘woven bone’) that ismechanically weaker and more susceptible to fracture. Lesions in Paget’s disease may besingleormultipleandcaninvolveanypartoftheskeleton,althoughtheyhaveapredilectionforthe spine, pelvis, femur, sacrum, and skull. In the final phase of Paget’s disease, cellular activity diminishestoleavescleroticbone.
Although theetiologyofPaget’sdisease remainsunknown,bothgeneticandenvironmental(infectious)factorshavebeenimplicated,whichmayexplainwhysome40%ofpersonswithPaget’s disease have a family history of the disease and why its geographical distributionworldwide isuneven.Up to6-7%of theelderlypopulation inWesternEurope isaffectedbyPaget’sdisease(Cooperetal�999).

��
IncidenceTheelderlyareprimarilyaffected.Withinthisagegroup,Paget’sdiseaseisthesecondmostcommonbonedisorderafterosteoporosis.RatesofPaget’sdiseaseintheUSare2%ofthepopulationolderthan60years(Altmanetal2000).
SymptomsMostpatientswithPaget’sdisease(70-90%)areasymptomatic.Theremaindermayexperiencebonepain(thecommonestsymptom),osteoarthritis,bonydeformity(commonlybowingofanextremity),fractures,excessivewarmthfromhypervascularity,andneurologicalcomplications,particularlyhearing loss, fromcompressionofneural tissues.Vertebraldeformitycan leadtospinal stenosis or cord compression.After onset, symptoms of the disease tend to worsenprogressively.
Adiagnosis ofPaget’s diseasemaybe considered in anelderly person by thepresenceofbonepain,deformity,compressionneuropathy,orother typicalsymptoms. In theabsenceofsymptoms,Paget’sdiseasemaybedetectedbyanalteredbiochemicalmarkerlevel,anx-rayabnormality,orhypercalcemia.Furtherevaluationscanincludex-raysandatechnetium-labeledbonescan.
OsteoporosisOsteoporosis is a systemic disease of the skelton characterized by low bone mass anddeterioration in bone microarchitecture, leading to increased bone fragility and susceptibilityto fracture. Osteoporotic fractures are a major cause of disability, mortality, and economicburdenworldwide,particularly inpostmenopausalwomenandintheelderlyofbothgenders.Approximately50%ofpatientswhohaveahipfracturedonotrecoverfullyandexperiencea20% increased risk of mortality in the next year (Cummings & Melton 2002).
PathophysiologyAfter the thirddecadeof life, theactivitiesofosteoblasticandosteoclasticcellsbecomeuncoupled,with the result thatbone resorptionexceedsbone formation.The imbalancebetween resorption and formation is greatest in women following the climacteric. In thecourseoftheirlifetime,womenlose30-40%oftheircorticalboneand50%oftheirtrabecularbone,comparedtolossesof�5-20%and25-30%,respectively,inmen.Otherriskfactorsfor osteoporosis include a family history, Caucasian race, smoking, and use of certainmedications(includingchemotherapy).
IncidenceOsteoporosisisthecommonestmetabolicbonediseaseworldwideandwomenconstitute80%ofallthoseaffected.Osteoporosisisalsotheleadingcauseoffracturesintheelderly,beingassociatedwith80%ofallfracturesinpeopleaged50yearsorolder.

�2
SymptomsTherearenosymptomsintheearlystagesofosteoporosis.Symptomsandsignsoccurringlatermay include fractures to the vertebrae, wrists, or hips (often the first indication of osteoporosis), lowbackorneckpain,andprogressivelossofheightwithstoopedposture.
Rheumatoid arthritisRheumatoid arthritis is a chronic inflammatory disease typically involving erosion and destruction of synovial membranes and articular structures of multiple joints simultaneously.Thediseasecoursecanbeshortandlimitedorprogressive,leadingtoseverejointdeformitiesanddisability.
PathophysiologyThecauseof rheumatoidarthritis remainsunclear,butcontributory factors includeageneticpredispositionandinfectioustriggers.AcomplexautoimmuneresponseinvolvingCD4+Tcellsand cytokines such as TNF-alpha and IL-1 is implicated, which produces inflammation, cell proliferation, anddegeneration. Increasedosteoblast activity isbelieved tobecentral to thedevelopmentofbonedamage,andisarationaleforinvestigationofbisphosphonatetherapyinrheumatoidarthritis.
IncidenceTheprevalenceof rheumatoidarthritis isapproximately�% in theUS, ranging from0.5%togreaterthan5%dependingonethnicvariation.Thediseasecanoccuratanyagebuttendstopeak in the fourth and fifth decades. The female-to-male ratio is approximately 3:1.
SymptomsRheumatoidarthritishasaninsidiousonsetusually,althoughitcanbeabrupt.ThediagnosistypicallyismadewhenfourofsevenqualifyingcriteriaestablishedbytheAmericanRheumatismAssociationaremet:
• Morningstiffnesslastinglongerthan�hourbeforeimprovement
• Arthritisinvolving3ormorejoints
• Arthritisofthehand,particularlyinvolvementoftheproximalinterphalangeal,metacarpophalangeal,orwristjoints
• Bilateralinvolvementofjointareas(ie,bothwrists,symmetricPIPandMCPjoints)
• Positiveserumrheumatoidfactor(RF)
• Rheumatoidnodules
• RadiographicevidenceofRA

�3
References
AltmanRD,BlochDA,HochbergMC,MurphyWA.PrevalenceofpelvicPaget’sdiseaseofboneintheUnitedStates.JBoneMinerRes2000;�5:46�-465.
BajorunasDR:Clinicalmanifestationsofcancer-relatedhypercalcemia.SeminOncol�990;�7(2Suppl5):�6-25.
BerensonJR,LichtensteinA,PorterLetal.Long-termpamidronatetreatmentofadvancedmultiplemyelomapatientsreducesskeletalevents.MyelomaArediaStudyGroup.JClinOncol�998;�6:593-602.
Bloomfield D. Should bisphosphonates be part of the standard therapy of patients with multiple myeloma or bone metastases from othercancers?Anevidence-basedreview.JClinOncol�998,16:�2�8-�225.
Broadus AE, Mangin M, Ikeda K et al. Humoral hypercalcemia of cancer. Identification of a novel parathyroid hormone-like peptide. N EnglJMed�988;3�9:556-563.
ClarkeNW,McClureJ,GeorgeNJ.Theeffectsoforchiectomyonskeletalmetabolisminmetastaticprostatecancer.ScandJUrolNephrol�993;27:475-483.
ColemanRE.Skeletalcomplicationsofmalignancy.Cancer�997;80(suppl8):�588-�594.
ColemanRE.Skeletalcomplicationsofmalignancy.Cancer�997;80(suppl8):�588-�594.
CollinsonMP,TyrellCJ,HuttonC.OsteoporosisoccurringintwopatientsreceivingLHRHanalogsforcarcinomaoftheprostate[letter].CalcifTissueInt�994;54:327-328.
Cooper C, Schafheutle K, Dennison E, Kellingray S, Guyer P, Barker D. The epidemiology of Paget’s disease in Britain: is theprevalencedecreasing?JBoneMinerRes�999;�4:�92-�97.
CummingsSR,MeltonLJIII.Epidemiologyandoutcomesofosteoporoticfractures.Lancet2002;359:�76�-�767.
DaniellHW.Osteoporosisafterorchiectomyforprostatecancer.JUrol�997;�57:439-444.
DodwellDJ.Malignantboneresorption:cellularandbiochemicalmechanisms.AnnOncol�992;3:257-267.
DomchekSM,YoungerJ,FinkelsteinDMetal.Predictorsof skeletal complications inpatientswithmetastaticbreastcarcinoma.Cancer2000;89:363-368.
GrillV,MartinTJ.Hypercalcemia.In:RubensRD,MundyGR,eds.CancerandtheSkeleton.London:MartinDunitzLtd.,2000:75-89.
Horiuchi N, Caulfield MP, Fisher JE et al. Similarity of synthetic peptide from human tumor to parathyroid hormone in vivo and in vitro. Science�987;238:�566-�568.
LiptonA,TheriaultRL,HortobágyiGNetal.Pamidronatepreventsskeletalcomplicationsandiseffectivepalliativetreatmentinwomenwith breast carcinoma and osteolytic bone metastases: long term follow-up of two randomized, placebo-controlled trials. Cancer2000;88:�082-�090.
MahonSM:Signsandsymptomsassociatedwithmalignancy-inducedhypercalcemia.Cancer Nurs �989;�2):�53-�60.CancerNurs�989;�2):�53-�60.
MenssenHD,SakalovaA,FontanaAetal.Effects of long-term intravenous ibandronate therapy on skeletal-related events, survival,Effectsoflong-termintravenousibandronatetherapyonskeletal-relatedevents,survival,andboneresorptionmarkersinpatientswithadvancedmultiplemyeloma.JClinOncol2002;20:2353-2359.
MundyGR,IbbotsonKJ,D’SouzaSMetal.Thehypercalcemiaofcancer:clinicalimplicationsandpathogenicmechanisms.NEnglJMed�984;3�0:�7�8-�727.
RalstonSH,GallacherSJ,PatelUetal.:Cancer-associatedhypercalcemia:morbidityandmortality.Clinicalexperiencein�26treatedpatients.AnnInternMed�990;��2:499-504.
SaadF,GleasonDM,MurrayRetal.Arandomized,placebo-controlledtrialofzoledronicacidinpatientswithhormone-refractorymetastaticprostatecarcinoma.JNatlCancerInst2002;94:�458-�468.
SuvaLJ,WinslowGA,WettenhallREetal.:Aparathyroidhormone-relatedproteinimplicatedinmalignanthypercalcemia:cloningandexpression.Science�987;237:893-896.
TheriaultRL,LiptonA,HortobágyiGNetal.Pamidronatereducesskeletalmorbidityinwomenwithadvancedbreastcancerandlyticbonelesions:arandomized,placebo-controlledtrial.Protocol�8ArediaBreastCancerStudyGroup.JClinOncol�999;�7:846-854.
TownsendMF,SandersWH,NorthwayRO,GrahamSDJr.Bonefracturesassociatedwithluteinizinghormone-releasinghormoneagonistsusedinthetreatmentofprostatecarcinoma.Cancer�997;79:545-550.
Vassilopoulou-Sellin R, Newman BM, Taylor SH et al. Incidence of hypercalcemia in patients with malignancy referred to acomprehensivecancercenter.Cancer�993;7�:�309-�3�2.
WarrellRPJr:Metabolicemergencies.In:DeVitaVTJr,HellmanS,RosenbergSA,eds:Cancer:PrinciplesandPracticeofOncology.

�4
5thed.Philadelphia,Pa:Lippincott-RavenPublishers,�997:2486-93.
WattersJ,GerrandG,DodwellD.Themanagementofmalignanthypercalcaemia.Drugs�996;52:837-848.
WattersJ,GerrandG,DodwellD.Themanagementofmalignanthypercalcaemia.Drugs�996;52:837-848.
ZekriJ,AhmedN,ColemanRE,HancockBWTheskeletalmetastaticcomplicationsofrenalcellcarcinoma.IntJOncol200�;�9:379-382.

�5
Skeletal-related events: management options
Chapter 2.
Toprovideacontextfortheusesofbisphosphonatesincurrentclinicalpractice,thischapterpresentsanoverviewofthemanagementoptionsinhypercalcemiaofmalignancy,malignantmelanoma, metastases to bone, and metabolic bone diseases based on current clinicalconsensusderivedfrommajorreviews,guidelines,andformularies.
Hypercalcaemia of malignancyDefinitive treatment for hypercalcemia of malignancy is effective management of the underlying malignantdisease,whichwillreducetheproductionofhumoralfactors,particularlyPTHrP,thatstimulate bone resorption and renal tubular calcium reabsorption. Effective new anticancertherapieshavereducedtheincidenceofhypercalcemiaofmalignancy,andpatientsnowtypicallydevelophypercalcemiaonlyinthelaterstagesofadvancedmetastaticdisease.
Themagnitudeofhypercalcemiaandtheseverityofsymptomsisthebasisfordecidingwhethertoinitiatehypocalcemictreatment.Immediateandaggressivetreatmentisrequiredforpatientswithacorrectedtotalserumcalciumlevel>�4mg/dL(>7mEq/L,3.5mmol/L).Forpatientswithaserumcalciumbetween�2and�4mg/dL(6-7mEq/L,3.0-3.5mmol/L),clinicalmanifestationsguidetherapy.Forpatientswithmildhypercalcemia(serumcalcium<�2mg/dL[<6mEq/L,3.0mmol/L]),treatmentisgenerallynotindicated(Bilezikian�992).
Symptomatic treatment of hypercalcemia focuses initially on correcting dehydration andenhancing renal calcium excretion. Subsequently treatment is with agents that inhibit boneresorption.A response to treatment is indicated by reductions in serum calcium levels andinurinarycalciumandhydroxyprolineexcretionandby resolutionof symptoms. It hasbeensuggestedthatpolyuria,polydipsia,centralnervoussystemsymptoms,nausea,vomiting,andconstipationaremorelikelytobemanagedsuccessfullythananorexia,malaise,andfatigue.Paincontrolisachievableinpatientswhogainnormocalcemia(Ralstonetal�990).
Pharmacologic inhibition of bone resorptionAn intravenous bisphosphonate is the treatment of choice for managing hypercalcemia ofmalignancy following correction of dehydration. With this approach, 70-90% of patients willachievenormocalcemia,reliefofsymptoms,andanimprovedqualityoflife(Coleman�999).
Bisphosphonatesmaybedivided into twodistinctpharmacologicclasses thathavedifferentmechanisms of action. Non-nitrogen-containing bisphosphonates (for example, etidronate,clodronate, and tiludronate) are metabolized intracellularly by osteoclasts to cytotoxic,nonhydrolyzable ATP analogs. Nitrogen-containing bisphosphonates (including alendronate,ibandronate, pamidronate disodium, risedronate, and zoledronic acid) inhibit prenylation

�6
(Nussbaumetal�993).Prenylationofguanosinetriphosphatasesisnecessaryforregulatingavarietyofintracellularprocessesinosteoclastsincludingmorphology,function,andsurvival(Russell et al �999)], and therefore inhibition of prenylation by bisphosphonates disruptsosteoclastactivitiesandinducesapoptosis(Benfordetal�999).
Although oral bisphosphonates are effective in treating hypercalcemic episodes, they havelimited efficacy compared with intravenous bisphosphonates (Major et al 2000; Body et al 1998). Theuseoforalformulationsisfurtherlimitedbyapoorbioavailabilitythatrequiresadministrationathighdoses,which isassociatedwithgastrointestinal toxicity includingesophagitis.Amongintravenousformulations, thenitrogen-containingbisphosphonatesaremorepotent inhibitorsofosteoclast-mediatedboneresorptionthannon-nitrogen-containingbisphosphonates,withalowertendencytotoxicrenaleffectsateffectivedoses(Purohitetal�995;Ralstonetal�989;Warrelletal�99�;Nussbaumetal�993;Pecherstorferetal�996).Prior to the introductionof zoledronic acid, the standard therapy for hypercalcemia of malignancy was intravenouspamidronate, which was effective in providing normocalcemia (Thiébaud et al �986, �988;Gucalp et al 1992; Body & Dumon 1994). Zoledronic acid is the most potent inhibitor of bone resorption identified to date and demonstrates superior efficacy to pamidronate in clinical trials (describedinChapter3).
Other therapeutics for hypercalcemia of malignancySalmoncalcitoninrapidlyinhibitscalciumandphosphorousresorptionfromboneanddecreasesrenal calcium reabsorption, but its calcium-lowering effect persists for a few days only andtachyphylaxisiscommon.Combiningcalcitoninwithbisphosphonatesmayofferarapidonsetofhypocalcemicresponse(Thiébaudetal�990).
Another agent with potential efficacy is plicamycin (mithramycin), which inhibits osteoclast RNA synthesis. Maximum response, however, does not occur until 48 hours after administrationandreboundhypercalcemiausuallyfollowsmultipledoses(Kennedy�970).Repeateddosesalso predispose patients to adverse effects such as thrombocytopenia, increases in hepatictransaminases,nephrotoxicity,andhypophosphatemia.
Gallium nitrate was developed as an antineoplastic agent but was found also to possesshypocalcemicactivity.Galliumnitrateinterfereswithprotonpumpsintheosteoclastmembrane,whichimpairstheabilityofthesecellstodissolvebonematrix.Disadvantagestoitsuseincludeacontinuous5-dayintravenousinfusionscheduleandapotentialfornephrotoxicity(Warrelletal�997).
Multiple myelomaDecidingfromamongtherangeofpotentialtreatmentsformyelomamaybeacomplexprocess.Treatmentistailoredtotheindividualpatient’srequirementsincludingageandgeneralhealth,stageofdisease,thepresenceofcomplications,andoutcomesfromprevioustreatments
Patients typically receive chemotherapy (e.g. bortezomib) to reduce the disease burdenof multiple myeloma, often given in high-dose and combined with stem cell transplantation.Adjunctive therapy frequently includes radiation therapy to specific areas of pain or impending fracture.

�7
Pharmacologic inhibition of osteoclastic bone resorptionBisphosphonateshavean important role in thepreventionofbonycomplicationsofmultiplemyeloma,includingthemanagementofhypercalcemia,fracture,andspinalcordcompression.Theseagentsarealsoabletopromotebonehealing.Based on trial evidence, theUSFoodand Drug Administration has approved the intravenous bisphosphonates, pamidronate andzoledronicacid,inmultiplemyeloma.
Current treatment guidelines by the American Society of Clinical Oncology (ASCO) recommend using intravenous bisphosphonates at first radiographic evidence of osteopenia in patients with multiple myeloma (Table 1).AsdiscussedinChapter3,thereisnowsubstantialevidencethatzoledronicacidisclinicallymoreeffectivethanpamidronate,inadditiontoofferingasuperioradministrationregimen.
Other therapies for multiple myelomaErythropoietinmayamelioratetheanemiathatresultsfrommyelomaitselforthechemotherapythatisusedtotreatit,andisshowntoimprovequalityoflife.Patientswithspinalcordcompressionmaybegincorticosteroidtherapyimmediatelytoreduceswelling.Surgicaldecompressionmaybeappropriate,butlaminectomyinthispopulationisreportedtohaveahighmortalityrate(6-�0%)andmaynottobesuperiortoradiation.Patientspresentingwithacuterenalfailuremaybenefit from plasmapheresis.
Table 1. Selected ASCO recommendations for intravenous bisphosphonate use in multiple myeloma and bone metastases
Lytic disease on plain radiographs• Intravenouspamidronate90mgdeliveredoveratleast2hoursorzoledronicacid4mg
over�5minutesevery3to4weeksisrecommendedformultiplemyelomapatientswithlyticdestructionofboneonplainradiographs
Monitoring• In patients with pre-existing renal disease and a serum creatinine <265 μmol/L or <3.0 mg/
dL,nochangeisrequiredindosage,infusiontime,orintervalofpamidronateorzoledronicacid
• Evaluationevery3to6monthsisrecommendedforpatientsreceivingchronicpamidronateorzoledronicacidtherapyforalbuminuriaandazotemia.Inpatientsexperiencingunexplainedalbuminuriaorazotemia,drugdiscontinuationiswarranteduntiltherenalproblemsresolve
Duration of therapy• Onceinitiated,intravenouspamidronateorzoledronicacidissiggestedtobecontinued
untilthereisevidenceofasubstantialdeclineinthepatient’sgeneralperformancestatus
Myeloma patients with osteopenia based on normal plain radiograph or bone mineral density measurements
• Itisreasonabletostartintravenousbisphosphonatesinmultiplemyelomawithosteopeniabutwithoutradiographicevidenceoflyticbonedisease
Pain control for bone involvement• Intravenouspamidronateorzoledronicacidisrecommendedforpatientswithpaindueto
osteolyticdiseaseandasanadjunctivetreatmentforpatientsreceivingradiationtherapy,analgesics,orsurgicalinterventiontostabilizefracturesorimpendingfractures

�8
Advanced malignancies involving boneRadiotherapy and systemic endocrine or cytotoxic therapy are the mainstays of definitive treatment for advanced cancers. Chemotherapeutic approaches currently being refined include theuseoftotalandrogenblockadeinprostatecancer;unfortunately,asdiscussedlater,androgenblockadeisassociatedwithreductionsinbonemineraldensity.
Forthemanagementofmetastases,externalbeamradiotherapyprovidespalliationforlocalizedbonepain,butislesseffectiveinthepresenceofwidespreadbonepainorforpatientswhosepain recurs at previously irradiated sites. Strontium-89 shows efficacy in patients with prostate cancer(Lewingtonetal�99�).Becausestrontium-89istakenuppreferentiallyatsitesofnewbone formation, it may have greatest efficacy for sclerotic metastases, although it appears also tobeeffectiveinosteolyticbonemetastasesfrombreastcancer(Robinsonetal�993).Morerecentlysamarium-�53,whichislinkedtothebisphosphonateethylenediaminetetramethylenephosphonic acid, has been evaluated in prostate and breast cancer (Resche et al �997).Samarium-�53,likestrontium-88,ispreferentiallytakenupatsitesofboneformation,whereitemitsalphaandgammaparticlesthatprovideimagingandtherapeuticeffects,respectively.
Pharmacologic inhibition of osteoclastic bone resorptionBisphosphonatesareanimportanttreatmentforreducingboththesymptomsandcomplicationsofbone involvementanddosoby restoring the rateofbone resorption tonormal.Greatestexperience to date of bisphosphonate use has been to treat bone pain due to metastasesfromadvancedbreastcancer.Controlled trialsofpamidronate,clodronate, ibandronate,andzoledronic acid have all demonstrated significant pain relief in this indication (Body et al 1998, �999; Berenson et al �998). As with hypercalcemia of malignancy, intravenous infusion isnecessarytoobtainoptimaleffects.
The efficacy of bisphosphonates in pain relief appears to be independent of the nature of the tumorortheradiographicappearanceofmetastases,andscleroticlesionsrespondaswellaslyticmetastases.Asthereappearstobeanassociationbetweenmetastaticbonepainandtherate of bone resorption, greatest benefit with bisphosphonates may be in those with most severe symptoms(Vinholesetal�997).
Largeplacebo-controlledstudieshaveinvestigatedpamidronategivenmonthlyatadoesof90mgbyintravenousinfusioninpatientswithadvancedbreastcancerandmultiplemyelomawhowerealsoreceivingsystemicendocrineorcytotoxictherapy(Hortobagyietal�996;Janjanetal1997; Berenson et al 1998). These trials showed that pamidronate significantly reduced skeletal morbidityinbothconditions.Improvementsmorbiditybegantoappearafterthreemonthsandwere maintained throughout the two-year study period. In addition, the pamidronate-treatedpatientsdemonstratedamaintainedqualityof lifeandareduction inpainandanalgesicusecompared to the placebo group. No significant overall effects on survival have been reported for pamidronate.Morerecently,large,well-designedtrialscomparingpamidronateandzoledronicacidhavebeenperformed.AsdescribedindetailinChapter3,theseshowthatzoledronicacidis superior in efficacy with a more rapid onset of effect than pamidronate.

�9
Bisphosphonates includingclodronate,pamidronate,andmorerecentlyzoledronicacidhavealso been investigated for efficacy in the treatment of metastases from prostate cancer (Lipton etal200�;Dearnaleyetal200�;Saadetal2002).Asdiscussed indetail inChapter3, theclinicaltrialdatabasehasbeenextendedfurtherbylargetrialsofzoledronicacidinlungandothersolidtumors(Rosdenetal2003).
Prostate cancer – therapy-induced osteoporosisMenwhoreceiveandrogen-deprivationtherapyororchiectomyforprostatecancerareatriskforreducedbonemassandanincreasedincidencesoffractures(Townsendetal�997).Smithetal (200�), forexample,observedan8.5%decrease in trabecularbonemineraldensityofthelumbarspineafteroneyearoftherapywithleuprolide(agonadotropinreleasinghormone[GnRH]agonist).CalciumandvitaminDsupplementationarenotadequatetopreventbonelossduringGnRHagonist therapy.Other therapies thathavebeen investigated includeselectiveestrogenreceptormodulators(e.g.raloxifeneandtoremifene),whicheffectivelypreventlossofbonemineraldensityinpostmenopausalwomen(Smithetal2004).Anotheragentwithpotentialisbicalutamide,whichbindsselectivelytoandrogenreceptorsintargettissue,andisindicatedincombinationwithaGnRHagonisttotreatmetastaticprostatecancer.
Pharmacologic inhibition of treatment-related bone lossAs may be predicted from the mode of action of bisphosphonates, these agents show efficacy in preventingtreatment-relatedbonelossinpatientswithprostatecancer.Intermittent(3-monthly)administrationofintravenouspamidronateorzoledronicacidpreventsorevenincreasesbonelossinmenwithprostatecancertreatedbyandrogen-deprivationtherapyororchiectomy(Smithetal200�;Ryanetal2006).Ryanetalfurtherobservedthatzoledronicacidincreasesbonemineraldensityeven if initiated6-�2monthsafter initiationofandrogen-deprivation therapy;furtherdetailsofthistrialarepresentedinChapter3.
Metabolic bone disorders
Paget’s diseaseTheshort-termobjective in the treatmentofPaget’sdisease isalleviationofbonepain,andfor this nonsteroidal anti-inflammatories and acetaminophen may be adequate. Longer term objectivesaretopreventorminimizediseaseprogressioninpatientsatriskofcomplications.AlthoughcalciumandvitaminDsupplementationmayhelpreduceimpairedbonemineralization,treatment with bisphosphonates should be considered as first-line therapy, with salmon calcitonin heldasasecond-lineoptionifbisphosphonatesarecontraindicated.
Bisphosphonatetherapyiscapableofnormalizingbiochemicalmarkersofboneturnoverandreplacing woven bone with normal lamellar bone (Reid et al �996). Bisphosphonates mayalsoreducebonepain(Milleretal�999;Smalletal2003).Intravenousbisphosphonatesarepreferableoveroralbisphosphonatesbecauseoral formulations requiredailydosing for twotosixmonths,withfastingbeforeandaftertreatmentandaneedtoremainuprightforatleast30minutestoreduceriskofuppergastrointestinalcomplications.Intravenouspamidronateisinconvenientbecauseit isgivenbyslowintravenousinfusionseachlastingafewhoursover

20
multiple visits. Zoledronic acid offers the advantages of a more convenient administrationschedule than pamidronate and a greater efficacy than oral risedronate, and to many authorities is considered the first-line medication (Reid et al 2005).
OsteoporosisNumerous therapeuticoptionsexist in the treatmentofosteoporosis inpostmenopausalwomenandtheelderly.Hormonereplacementtherapyhasbeenusedformanyyearstoincreaseserumestrogenlevelsanddecreasetherateofboneresorptioninpostmenopausalosteoporosis,but recentcontrolled trialssuggested that theharmof long-termhormonereplacement may outweigh the benefits (Rossouw et al 2002).
Selectiveestrogen-receptormodulators(SERMs),suchasraloxifene,mimictheeffectsofestrogensinbonewithoutstimulatoryeffectsinothertissues,anddemonstratebonelosspreventionandvertebralfractureratereductioninwomenwithpostmenopausalosteoporosis.Toremifene isanewerSERMapproved to treatadvancedbreastcancerandalsobeinginvestigatedtotreattheosteoporosisassociatedwithhormonetherapyinprostatecancer.
Bisphosphonates are now considered first-line agents for the prevention and treatment of osteoporosis,byofferingconsistentincreasesinbonemineraldensityandreducedratesoffracture.Oralbisphosphonatessuchasalendronateandrisedronatereducetheriskofvertebralandnon-vertebralfracturesby40-50%.Oralbisphosphonates,however,requiretobetakendailyonanemptystomach,whichraisesconcernsofgastrointestinalintoleranceandcompliance.Forthisreason,intravenousbisphosphonatesofferpotentialadvantages.AsshownbyReidetal,anannualinfusionofzoledronicacidincreasesbonemineraldensitytoasimilardegreeasdailyadministrationoforalbisphosphonate(Chapter3).
Rheumatoid arthritisMany therapies are available for treating rheumatoid arthritis, including non-steroidalanti-inflammatories (NSAIDs), disease-modifying anti-rheumatologic drugs (DMARDs), immunosuppressants, biologic response modifiers, and corticosteroids.
Traditionally,thetreatmentofrheumatoidarthritishasutilizedastepwiseprogressionbeginningwithsalicylatesandNSAIDsandprogressingtodisease-modifyingmedications.NSAIDs(andCOX-2 inhibitors, used with caution) are the cornerstone of therapy for mild, well-controlleddisease, offering reductions in pain and inflammation and improvements in mobility and function.
DMARDs such as methotrexate and sulfasalazine are used frequently as components ofcombination therapy regimens. Current recommendations suggest that for all but minordisease, DMARDs, biologic response modifiers, and combination therapy regimens are more effectiveifinitiatedearlyinthediseasecourse,whendestructionofsynovialtissueandjointsisbeginning.
Althoughthemedicationsdescribedabovemaybeeffectiveinmanypatientswithrheumatoidarthritis,theprognosisofthisdiseaseisextremelyvariableandnoveltherapeuticapproachescontinuetobeexplored.Asdemonstratedinarecentproofofconceptstudy,zoledronicacidtherapyadministeredat�3-weekintervalsreducestheprogressionoferosionscomparedwithplaceboandwarrantsfurtherinvestigation(Jarrettetal2006)

2�
References
AdamsonBB,GallacherSJ,ByarsJetal.MineralisationdefectswithpamidronatetherapyforPaget’sdisease.Lancet�993;342:�459-�460.
AmericanCollegeofRheumatology:Guidelinesforthemanagementofrheumatoidarthritis:2002Update.ArthritisRheum2002;46:328-346
BenfordHL,HelfrichMH,SebtiSetal.InhibitionofproteingeranylgeranylationbybisphosphonatesandGGTI298causesactivationofcaspase3-likeproteasesinosteoclasts.CalcifTissueInt�999;64(suppl�):S45.
BerensonJR,LichtensteinA,PorterLetal.Long-termpamidronatetreatmentofadvancedmultiplemyelomapatientsreducesskeletalevents.JClinOncol�998;�6:593-602.
BerensonJR,LiptonA,RosenLSetal.PhaseIclinicalstudyofanewbisphosphonate,zoledronate(CGP-42446),inpatientswithosteolyticbonemetastases.Blood�998;88(suppl�):586a.
BilezikianJP:Managementofacutehypercalcemia.NEnglJMed�992;326:��96-�203.
BodyJJ,BartlR,BurckhardtPetal.Currentuseofbisphosphonatesinoncology.InternationalBoneandCancerStudyGroup.JClinOncol�998;�6:3890-3899.
BodyJJ,DielIJ,LichinitserMRetal:Intravenousibandronatereducestheincidenceofskeletalcomplicationsinpatientswithbreastcancerandbonemetastases.AnnOncol2003;�4:�399-�405.
BodyJJ,DielIJ,LichinitzerMetal:Oralibandronatereducestheriskofskeletalcomplicationsinbreastcancerpatientswithmetastaticbonedisease:Resultsfromtworandomised,placebo-controlledphaseIIIstudies.BrJCancer2004;90:��33-��37.
BodyJJ,DumonJC.Treatmentof tumour-inducedhypercalcaemiawith thebisphosphonatepamidronate:dose-response relationshipandinfluence of tumour type. Ann Oncol 1994;5:359-363 .
BodyJJ,LichinitserMR,DiehlIEetal.Double-blindplacebocontrolledtrialofibandronateinbreastcancermetastatictobone.ProcAmSocClinOncol�999;�8:575a.
BoyceBF,AdamsonBB,GallacherSJetal.MineralisationdefectsafterpamidronateforPaget’sdisease.Lancet�994;343:�23�-�232.
ColemanRE.Pamidronatedisodiuminthetreatmentandmanagementofhypercalcaemia.RevContempPharmacother�998;9:�47-�64.
DearnaleyDP,SydesMR,onbehalfoftheMRCPr05Collaborators.Preliminaryevidencethatoralclodronatedelayssymptomaticprogressionof bone metastases from prostate cancer: first results of the MRC Pr05 Trial [abstract]. Proc ASCO 2001;20:174a.
GucalpR,RitchP,WiernikPHetal.Comparativestudyofpamidronatedisodiumandetidronatedisodiuminthetreatmentofcancer-relatedhypercalcemia.JClinOncol�992;�0:�34-�42.
Hortobagyi GN, Theriault RL, Porter L et al. Efficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bonemetastases.Protocol�9ArediaBreastStudyGroup.NEnglJMed�996;335:�785-�79�.
JanjanNA.Radiation forbonemetastases:conventional techniquesand the roleofsystemic radiopharmaceuticals.Cancer�997;80(suppl8):�628-�645.
Jarrett SJ, Conaghan PG, Sloan VS, et al. Preliminary evidence for a structural benefit of the new bisphosphonate zoledronic acid in early rheumatoidarthritis.ArthritisRheum2006;54:�4�0-�4�4.
KennedyBJ:Metabolicandtoxiceffectsofmithramycinduringtumortherapy.AmJMed�970;49:494-503.
Lewington VJ, McEwan AJ, Ackery DM et al. A prospective, randomised double-blind crossover study to examine the efficacy of strontium-89 in painpalliationinpatientswithadvancedprostatecancermetastatictobone.EurJCancer�99�;27:954-958.
LiptonA,SmallE,SaadFetal.Thenewbisphosphonate,ZometaTM(zoledronicacid)decreasesskeletalcomplicationsinbothlyticandblasticlesions:acomparisontopamidronate[abstract34].CancerInvest200�;20:45-47.
MajorPP,LiptonA,BerensonJetal.Oralbisphosphonates:areviewofclinicaluseinpatientswithbonemetastases.Cancer2000;88:6-�4.
MillerPD,BrownJP,SirisES,HoseyniMS,AxelrodDW,BekkerPJ.Arandomized,double-blindcomparisonofrisedronateandetidronateinthetreatmentofPaget’sdiseaseofbone.AmJMed�999;�06:5�3-520.
NussbaumSR,WarrellJrRP,RudeRetal.Dose-responsestudyofalendronatesodiumforthetreatmentofcancer-associatedhypercalcemia.JClinOncol�993;��:�6�8-�623.
Nussbaum SR, Younger J, Vandepol CJ et al. Single-dose intravenous therapy with pamidronate for the treatment of hypercalcemia ofmalignancy:comparisonof30-,60-,and90-mgdosages.AmJMed�993;95:297-304.
PecherstorferM,HerrmannZ,BodyJJetal.RandomizedphaseIItrialcomparingdifferentdosesofthebisphosphonateibandronateinthetreatmentofhypercalcemiaofmalignancy.JClinOncol�996;�4:268-276.
Purohit OP, Radstone CR, Anthony C et al. A randomised double-blind comparison of intravenous pamidronate and clodronate in thehypercalcaemiaofmalignancy.BrJCancer�995;72:�289-�293.
Ralston SH, Gallacher SJ, Dryburgh FJ et al. Treatment of severe hypercalcaemia with mithramycin and aminohydroxypropylidenebisphosphonate.Lancet�988;2:277.
Ralston SH, Gallacher SJ, Patel U et al. Comparison of three intravenous bisphosphonates in cancer-associated hypercalcemia. Lancet�989;2:��80-��82.
RalstonSH,GallacherSJ,PatelUetal.Cancer-associatedhypercalcemia:morbidityandmortality.Clinicalexperiencein�26treatedpatients.

22
AnnInternMed�990;��2:499-504.
ReidIR,BrownJP,BurckhardtP,HorowitzZ,RichardsonP,TrechselU.Intravenouszoledronicacidinpostmenopausalwomenwithlowbonemineraldensity.NEnglJMed2002;346:653.
ReidIR,MillerP,LylesKetal.ComparisonofasingleinfusionofzoledronicacidwithrisedronateforPaget’sdisease.NEnglJMed2005;353:898-908.
ReidIR,NicholsonGC,WeinsteinRSetal.BiochemicalandradiologicimprovementinPaget’sdiseaseofbonetreatedwithalendronate:arandomized,placebo-controlledtrial.AmJMed�996;�0�:34�-348.
RescheI,ChatalJF,PeckingAetal.Adose-controlledstudyof�53Sm-Ethylenediaminetetramethylenephosphate(EDTMP)inthetreatmentofpatientswithpainfulbonemetastases.EurJCancer�997;33:�583-�59�.
Robinson RG, Preston DF, Baxter KG et al. Clinical experience with strontium-89 in prostatic and breast cancer patients. Semin Oncol�993;20(suppl2):44-48.
RosenLS,GordonD,TchekmedyianS,etal:Zoledronicacidversusplacebointhetreatmentofskeletalmetastasesinpatientswithlungcancerandothersolidtumors:AphaseIII,double-blind,randomizedtrial—TheZoledronicAcidLungCancerandOtherSolidTumorsStudyGroup.JClinOncol2003;2�:3�50-3�57.
Rossouw JE, Anderson GL, Prentice RL et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. Principal results fromtheWomen’sHealthInitiativerandomizedcontrolledtrial.JAMA2002;288:32�-333.
RussellRG,RogersMJ,FrithJCetal.Thepharmacologyofbisphosphonatesandnewinsightsintotheirmechanismsofaction.JBoneMinerRes�999;�4(suppl2):53–65.
Ryan CW, Huo D, Demers LM, Beer TM, Lacerna LV. Zoledronic acid initiated during the first year of androgen deprivation therapy increases bonemineraldensityinpatientswithprostatecancer.JUrol2006;�76:972-978.
SaadF,GleasonDM,MurrayRetal.Zoledronicacidreducesskeletalcomplicationsinpatientswithhormone-refractoryprostatecarcinomametastatictobone:arandomized,placebo-controlledtrial.JNatlCancerInst2002;94:�458-�468.
SmallEJ,SmithMR,SeamanJJetal.Combinedanalysisoftwomulticenter,randomized,placebo-controlledstudiesofpamidronatedisodiumforthepalliationofbonepaininmenwithmetastaticprostatecancer.JClinOncol2003;2�:4277-4284
SmithMR,FallonMA,LeeH,FinkelsteinJS.Raloxifenetopreventgonadotropin-releasinghormoneagonist-inducedbone loss inmenwithprostatecancer:arandomizedcontrolledtrial.JClinEndocrinolMetab2004;89:384�-3846.
SmithMR,McGovernFJ,ZietmanALetal.Pamidronatetopreventbonelossduringandrogen-deprivationtherapyforprostatecancer.NEnglJMed200�;345:948-955.
ThiébaudD,JacquetAF,BurckhardtP.Fastandeffectivetreatmentofmalignanthypercalcemia.Combinationofsuppositoriesofcalcitoninandasingleinfusionof3-amino�-hydroxypropylidene-�-bisphosphonate.ArchInternMed�990;�50:2�25-2�28.
ThiébaudD,JaegerP,JacquetAFetal.Asingle-day treatmentof tumor-inducedhypercalcemiaby intravenousamino-hydroxypropylidenebisphosphonate.JBoneMinerRes�986;�:555-562.
ThiébaudD,JaegerP,JacquetAFetal.Dose-responseinthetreatmentofhypercalcemiaofmalignancybyasingleinfusionofthebisphosphonateAHPrBP.JClinOncol�988;6:762-768.
TownsendMF,SandersWH,NorthwayRO,GrahamSDJr.Bonefracturesassociatedwithluteinizinghormone-releasinghormoneagonistsusedinthetreatmentofprostatecarcinoma.Cancer�997;79:545-550.
VinholesJJ,PurohitOP,AbbeyMEetal.Relationshipsbetweenbiochemicalandsymptomaticresponseinadouble-blindtrialofpamidronateformetastaticbonedisease.AnnOncol�997;8:�243-�250.
WarrellJrRP,MurphyWK,SchulmanPetal.Arandomizeddouble-blindstudyofgalliumnitratecomparedwithetidronateforacutecontrolofcancer-relatedhypercalcemia.JClinOncol�99�;9:�467-�475.
WarrellRPJr.Metabolicemergencies.In:DeVitaVTJr,HellmanS,RosenbergSA,eds.Cancer:PrinciplesandPracticeofOncology.5thed.Philadelphia,Pa:Lippincott-RavenPublishers,�997:2486-93.

23
Zoledronic acid is a new-generation bisphosphonate and the most potent inhibitor of bone resorption in its class. Zoledronicacidislicensedinmanycountriesforthefollowingindications:
�. Hypercalcemiaofmalignancy
2. Multiplemyeloma
3. Bonemetastasesorbonepainpresumedduetobonemetastasesfrombreastcancer,lungcancer,prostatecancer,andothersolidtumortypes
4. Prophylaxisofbonelosssecondarytoandrogendeprivationtherapyinprostatecancer
5. Paget’sdiseaseofbone
Zoledronicacidisalsoanexperimentaltherapyforosteoporosis,rheumatoidarthritis,andotherindications.Theextensiveclinicaldatathatsupporttheseapplicationsofzoledronicacidwillbedescribedindetailinthischapter.
Hypercalcemia of malignancyZoledronicacidwasapprovedbytheUSFoodandDrugAdministrationin200�forthetreatmentof hypercalcemia of malignancy based on pivotal clinical studies that directly comparedzoledronicacidwithpamidronateadministeredintravenously.Inpatientswithmoderatetoseverehypercalcemia of malignancy, zoledronic acid demonstrated a significantly higher response rate than pamidronate with the benefit of a more rapid infusion time (15 minutes, versus 2 hours for pamidronate). Given the superior efficacy, more convenient administration schedule, and comparable safety profile of zoledronic acid compared with pamidronate, zoledronic acid may becomethetreatmentofchoiceforhypercalcemiaofmalignancy.
Efficacy dataEarlyclinicaltrialsincludingadose-rangingstudyinpatientswithhypercalcemiaofmalignancy(Bodyetal�999;Berensonetal200�)establishedthatzoledronicacidwaseffectiveinreducingserumcalciumlevelswithadurationofnormocalcemiaexceeding2�daysandwassafeandwelltolerated.
The superior efficacy of zoledronic acid (4 or 8 mg, by single daily intravenous injection) compared withpamidronate (90mg)wasdemonstrated inapooledanalysisof two large, randomized,
Zoledronic acid: clinical evidence for efficacy and safety
Chapter 3.

24
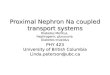
Figure�.Proportionofpatientsachievingacompleteresponsebytreatmentgroup.
Figure2.MeanCSClevelsatbaselineanddays4,7,and�0forpatientstreatedwithzoledronicacid, 4 mg (filled circles) or 8 mg (filled squares), or pamidronate disodium, 90 mg (filled triangles). Per-protocolentrancecriteria(meanCSC 3.0mmol/l[�2.0mg/dl],solidline)andnormalizationvalue(meanCSC 2.7mmol/l[�0.8mg/dl],dashedline)areindicated.
phase III trials based in the US/Canada and Europe/Australia, respectively, in 287 patientswithmoderatetoseverehypercalcemiaofmalignancy(i.e.baselinecorrectedserumcalcium3.0mmol/l[�2.0mg/dll])(Majoretal200�).Thesetrialsrepresentedthelargestcomparativeinvestigations of bisphosphonate therapy ever conducted in patients with hypercalcemia ofmalignancy.Pamidronatewaschosenascomparatorbecauseofitswidespreaduseinpatientswith osteolytic lesions from multiple myeloma or metastatic breast cancer. Zoledronic acidwasadministeredviaa5-minuteinfusionandpamidronateviaa2-hourinfusion.Patientswhorelapsedorwererefractorytoinitialtreatmentwithzoledronicacidorpamidronatewereeligiblefortreatmentwithzoledronicacidat8mginasecondphaseofthetrial.Patientswerefollowedfor56daysoruntilserumcalciumlevelswere 2.9 mmol/l. Complete response was defined as acorrectedserumcalciumlevel<2.7mmol/lbyday�0.
The complete response rate was significantly higher for zoledronic acid (88.4% for 4 mg and 86.7%for8mg)thanforpamidronate(69.7%)(Figure 1).Patientstreatedwithzoledronicacidalsoachievedamorerapidnormalizationofserumcalciumthan those treatedwithpamidronate(Figure 2)andexperiencedalongermediandurationofresponsethanthoseinthepamidronategroup.The4mgdoseofzoledronicacidwasnearlyaseffectiveasthe8 mg dose, with no significant differences.
In the 69 patients who relapsed or were refractory to therapy in the first phase of the trial, retreatmentwith8mgzoledronicacidachievedacompleteresponsein36(52%)patientsbyday�0.Thisresponseraterepresentsaclinicallymeaningfuleffectinapopulationwhoexhibiteddiminishedserumcalciumresponsivenesstoearlierbisphosphonatetherapy(Nussbaumetal�993;Thiébaudetal�990).
Zoledronic acid was equally effective regardless of the patients’ gender, age, tumor type,presenceofbonemetastases,orserumPTHrPlevel.Incontrast,pamidronatewaslesseffectiveinpatientswithhumoral-typehypercalcemiaofmalignancy(6�%completeresponserate)thaninpatientswiththeosteolyticform(80%)(Majoretal200�).Zoledronicacidwassafeandwell

25
toleratedatboth4mgand8mgdoses(Majoretal200�).
The outcomes of these pivotal provided the basis for concluding that zoledronic acid issuperiortopamidronateforthetreatmentofhypercalcemiaofmalignancy.
The benefits of zoledronic acid that were demonstrated in these trials based in North America, Europe, and Australia were confirmed in an open-label trial from Japan (Kawada et al 2005). Patients (n=27) with hypercalcemia of malignancy, defined as a corrected serum calcium level �2.0mg/dl,weretreatedwithasingledoseofzoledronicacid,4mg,by�5-minuteinfusion.
Themeancorrectedserumcalciumleveldecreasedfrom�4.5to9.6mg/dlbyday�0.Completeresponse, defined as a decrease of corrected serum calcium �0.8 mg/dl by day �0, wasachievedin84%ofpatients(similartoMajoretal200�).Themediantimetorelapsewas23daysand,interestingly,wasshorterinpatientswithhighPTHrPlevelsthaninpatientswithlowlevels.Clinicalsymptomsassociatedwithhypercalcemiaofmalignancy, includingdepressedlevelofconsciousness,anorexia,nausea,vomiting,fatigueandmouthdryness, improvedasthecorrectedserumcalciumlevelwasdecreased.
Themost frequentlyobservedadverseeventwas fever ( 38°C).Noseriousadverseeventsassociated with renal toxicity were reported. Based on these results, zoledronic acid wasconcludedtobeaseffectiveandwelltoleratedforhypercalcemiaofmalignancyinJapanesepatientsasinotherpatientpoulationsinvestigated.
Infusion time benefitsTheobservationofincreasesinserumcreatinineinsomepatientsreceivinga5-minuteinfusionof zoledronic acid, comparable with those following a 2-hour infusion of pamidronate (90mg) (Berensonetal200�),caused therecommended infusionrate forzoledronicacid tobeincreasedfrom5to�5minutesinpatientswhorequirerepeatedadministration.Afterextensionoftheinfusionrateto�5mintues,increasesinserumcreatininelevelsaresimilartoplaceboinpatientswithmetastaticbonedisease(Saadetal2002).
The�5-minuteinfusiontimeforzoledronicacid(comparedwith2hoursforpamidronate)offerssignificant advantages. Gammon and Le (2003) observed that the shorter administration time ofzoledronicacidcomparedtopamidronateofferstheopportunitytotreatmorepatientswithexistingclinicalstaffandimprovesthequalityofpatients’livesbyshorteningtheirtimeinclinic.
Inconclusion,thesepivotaltrialsinpatientswithmoderatetoseverehypercalcemiaofmalignancyhave demonstrated that zoledronic acid is significantly superior to pamidronate. Incidences of adverse events were similar between zoledronic acid and pamidronate. The superior efficacy andconvenienceofzoledronicacidsuggestthatzoledronicacidmayrepresentthetherapyofchoiceforthetreatmentofhypercalcemiaofmalignancy.
Multiple myelomaTheUSFoodandDrugAdministrationin2002approvedanexpandedindicationforzoledronicacidforthetreatmentofpatientswithbonemetastasesthatincludemultiplemyeloma.Treatment guidelines by the American Society of Clinical Oncology recommend use of intravenous bisphosphonates including zoledronic acid at first radiographic evidence of osteopenia in patients with multiple myeloma to significantly reduce the occurrence and delay the

26
onset of skeletal complications (Berenson et al 2002). The trial evidence reviewed below shows that zoledronic acid is at least comparable in efficacy to pamidronate in multiple myeloma.
ZoledronicacidwascomparedtopamidronateinaphaseIIstudyof280patientswithlyticbonemetastases frommultiplemyeloma(n=�08)orbreastcancer(n=�72)(Berensonetal200�).Patientswererandomizedtoninemonthlyinfusionsof0.4mg,2mg,or4mgzoledronicacidviaa5-minuteinfusionorto90mgofpamidronateasa2-hourinfusion.Theprimaryendpointwasidentification of the dose of zoledronic acid that reduced the need for radiation to less than 30% oftreatedpatients.Zoledronicacidat2mgand4mgreducedtheneedforradiationto�8%and2�%ofpatients,respectively.
Alarger,international,multicenter,double-blind,randomizedtrialcompared4or8mgdosesofzoledronicacidto90mgpamidronateevery3to4weeksfor�2monthsin�648patientswithstage IIImultiplemyeloma(n=5�0)orbreastcancer (n=��38)whohad lyticdisease (Rosenet al 200�).The infusion time for zoledronic acid was �5 minutes compared to 2 hours forpamidronate.Theprimaryendpointwas theproportionofpatientswithat leastoneskeletal-related event, defined as pathologic fracture, spinal cord compression, radiation therapy, or surgerytoboneat�3months(after�2monthsoftreatmentand�monthoffollow-up).
In the zoledronic acid 4 mg arm, 44% of patients had at least one skeletal-related eventcompared with 46% in the pamidronate arm, which confirmed the non-inferiority of zoledronic acid compared to pamidronate. In addition, zoledronic acid significantly reduced the need for radiotherapy compared with pamidronate (�5% versus 20%). Further details of this trial aredescribedintheBreastCancersection,below.
Rosen and colleagues (2003) reported a longer-term (25-month) safety and efficacy study comparing zoledronic acid with pamidronate in these patients with multiple myeloma orbreast carcinoma.Patients receivedzoledronicacid4mgor8mg (reduced to4mg)or90mgpamidronateevery3-4weeksfor24months.After25months,zoledronicacidreducedtheoverallproportionofpatientswithaskeletal-relatedeventandreducedtheskeletalmorbidityrate similarly to pamidronate. However, compared with pamidronate, zoledronic acid significantly reducedtheoverallriskofskeletalcomplications(includinghypercalcemiaofmalignancy)byanadditional�6%(P=0.030).Zoledronicacidandpamidronatewereequallywelltolerated.Theselong-term follow-up data confirm that zoledronic acid has at least similar efficacy to pamidronate inpatientswithmultiplemyeloma.
Additionaltrialsoffersupportfortheselargeinvestigations.Forexample,asingle-centerstudyofninepatientswhichcomparedzoledronic acid and pamidronate in multiple myeloma patientszoledronicacidandpamidronatein multiple myeloma patientsinmultiplemyelomapatientssubstantiated that zoledronic acid offers equivalent efficacy and safety to pamidronate at 12zoledronic acid offers equivalent efficacy and safety to pamidronate at 12 monthswhenadministeredbythesameregimensandusingsimilarassessmentsasdescribedabove(Krajetal2002).
Advanced malignancies involving boneThree pivotal studies evaluated the efficacy and safety of zoledronic acid in patients with cancer bone metastases.These studies included an investigation of patients with breast cancer ormultiple myeloma using pamidronate as active control (described above) and two placebo-

27
controlledinvestigationsinpatientswithsolidtumorsandprostatecancer.Studydurationswere�3,9,and�5months,respectively.Ineachstudy,theprimaryanalysiswasacomparisonoftheproportions of patients with at least one skeletal-related event, defined as a pathologic fracture, spinalcordcompression,needforradiotherapytobone,orsurgerytobone.
Basedon the resultsof these randomized,phase IIIclinical trials thatenrolled in totalmorethan3000patients,zoledronicacid(4 mg by 15-minute infusion) has receivedmultinationalregulatoryapproval for the treatmentofbonemetastasessecondary toall solid tumor typesaswellasbonelesionsfrommultiplemyeloma.Unlikepamidronate,zoledronicacidhasbeenshowntoreduceskeletalmorbidityinpatientswithbothosteolyticandosteoblasticbonelesions.Zoledronicacidcanbesafelyadministeredvia�5-minuteinfusion,comparedwiththeminimumrecommended infusion time of 2 hours for pamidronate. On the basis of these benefits, zoledronic acidisemergingasthenewstandardofcareformanagingskeletalmorbidityinpatientswithadvancedcancersinvolvingbone.
For patients with breast cancer, guidelines from theAmerican Society of Clinical Oncologyrecommend that bisphosphonate therapy should be initiated at first radiographic evidence of bonedestructionoranabnormalbonescanwith localizedpain (Hillneretal2000).Patientswhoarereceivingbisphosphonatetherapyshouldcontinuetodosothroughoutthecourseoftheirdiseaseforaslongasitistolerated.Noguidelineshavebeendevelopedforpatientswithsolid tumors other than breast cancer, but treatment with zoledronic acid at first diagnosis of metastaticbonediseasemaybeareasonableapproachbasedonphaseIIItrialsofzoledronicacidinprostatecancer,lungcancer,orothersolidtumors,asdescribedbelow.Zoledronicacidremainstheonlybisphosphonatethatisproveneffectiveinthetreatmentofbonemetastasesinpatientswithadvancedprostatecancerandothersolidtumors.
An additional benefit of therapy with zoledronic acid is pain relief (Vogel et al 2004). A recent open-label study investigated zoledronic acid 4 mg intravenously over 15 minutes every 3-4 weeks as treatment for bone metastases in patients with multiple myeloma, breast cancer, or prostate cancer. The majority of patients (65%) had received other bisphosphonate therapy previously (pamidronate in 95%). Ofthe6�3patientsinvestigated,46� (75%) reported pain at baseline.At every visit, these patients experienced statisticallysignificant decreases in mean pain score compared with baseline. While overall quality of life measures remained stable during the study, individual score items including mean physicalwell-being and emotional well-being improved significantly. Zoledronic acid was generally well tolerated,with77%ofpatientscompletingallsixinfusions.The authors concluded that, with appropriate monitoring, cancer patients with bone metastases achieve clinical benefits from zoledronic acid therapy, including those who previously received alternative intravenous bisphosphonate treatment.
Breast cancerThe benefits of bisphosphonate therapy in breast cancer patients include correction of hypercalcemia, relief of pain, and reduction in skeletal-related events.The potent effects ofzoledronic acid in treating hypercalcemia of malignancy are reported above. For metastaticbone pain, at least 50% of the patients obtain a clinically relevant analgesic effect frombisphosphonate therapy.The frequency of skeletal-related events is reduced by 30-40% on

28
prolonged administration, and intravenous bisphosphonates are now recognized as thepreferredtreatmentforpreventionofskeletalcomplications.TheAmericanSocietyofClinicalOncologyguidelinesforpatientswithbreastcancerrecommendtherapywithzoledronicacidorpamidronateforpreventionofskeletalcomplicationsinpatientswithradiologicevidenceofbonelesions(Hillneretal2004).Pamidronatewastheearlystandardofcareinthesepatients.Subsequently, comparative trials have demonstrated the non-inferiority and, in longer-terminvestigations,thesuperiorityofzoledronicacidrelativetopamidronateinpatientswithbreastcancer.
Efficacy dataInalargenon-inferioritytrial,Rosenetal(200�)randomlyassigned�648patientswitheitherstageIIImultiplemyelomaoradvancedbreastcancerandatleastonebonelesiontotreatmentwith4or8mgofzoledronicacidvia�5-minuteintravenousinfusionor90mgofpamidronatevia2-hour intravenous infusion every 3-4 weeks for 12 months. The primary efficacy endpoint was theproportionofpatientsexperiencingatleastoneskeletal-relatedeventover�3months.
Theproportionofpatientswithatleastoneskeletal-relatedeventwassimilarinalltreatmentgroups(including44%ofpatientswhoreceived4mgzoledronicacidversus46%ofpatientswhoreceived pamidronate). The median time to first skeletal-related event was approximately one yearineachtreatmentgroup.Theskeletalmorbidityratewasslightlylowerinpatientstreatedwith zoledronic acid than in those receiving pamidronate, and zoledronic acid (4 mg) significantly decreasedtheincidenceofradiationtherapytobone,bothoverallandinthesubsetofpatientswhowerereceivinghormonaltherapy.Painscoresdecreasedinalltreatmentgroups.
Zoledronicacid(4mg)andpamidronatewereequallywelltolerated.Themostcommonadverseeventsinthesegroupswerebonepain,nausea,fatigue,andfever.Fewerthan5%ofseriousadverseeventswererelatedtothestudydrug.Theincidenceofrenalimpairmentamongpatientstreatedwith4mgofzoledronicacidvia�5-minuteinfusionwassimilartothatinpatientstreatedwithpamidronate.
Inconclusion,zoledronicacid(4mg)via�5-minuteintravenousinfusionwasaseffectiveandwelltoleratedas90mgofpamidronateinthetreatmentofosteolyticandmixedbonemetastases/lesionsinpatientswithadvancedbreastcancerormultiplemyeloma.
Asubanalysisthatconcentratedonpatientswhohadbreastcarcinomawithatleastoneosteolyticlesionatstudyentry(n=528)showedthattheproportionwithaskeletal-relatedeventwaslowerin the4mgzoledronicacidgroup than thepamidronategroup (48%versus58%,P=0.058)(Rosen et al 2004). In addition, the time to first skeletal-related event was significantly longer inthe4mgzoledronicacidgroupthanthepamidronategroup(median3�0versus�74days;P=0.013). Moreover, multiple-event analysis demonstrated significant further reductions in the riskofdevelopingskeletal-relatedeventsforzoledronicacidcomparedwithpamidronate(30%intheosteolyticsubset[P=0.0�0]and20%forallpatientswithbreastcancer[P=0.037]).Thesedataindicatethat4mgzoledronicacidwasmoreeffectivethan90mgpamidronateinreducingskeletalcomplicationsinpatientswithbreastcarcinomawithatleastoneosteolyticlesion.
The same authors compared the longer-term safety and efficacy of zoledronic acid and pamidronateinpatientswithbonelesionssecondarytoadvancedbreastcarcinomaormultiplemyeloma(Rosenetal2003).After25monthsoffollow-up,zoledronicacidreducedtheoverallproportion of patients with a skeletal-related event and reduced the skeletal morbidity rate

29
Fig3.Proportionofpatientswitheachtypeofskeletal-relatedevent(SRE).Comp,compression;HCM,hypercalcemiaofmalignancy.(*),excludingHCM.
Fig4.MeanchangefrombaselineBriefPainInventory(BPI)compositepainscoresbytreatmentgroupandtimeonstudy.(*),P<.05.
similarly topamidronate.Comparedwithpamidronate,however,zoledronicacid reduced theoverallriskofdevelopingskeletalcomplications(withinclusionofhypercalcemiaofmalignancy)byanadditional�6%(P=0.030).Inpatientswithbreastcarcinoma,4mgzoledronicacidwassignificantly more effective than pamidronate, reducing the risk of skeletal-related events byanadditional20% (P=0.025).Zoledronicacid (4mg)andpamidronatewereequallywelltolerated.These long-term follow-updatademonstrate thatzoledronicacid ismoreeffectivethanpamidronateinreducingtheriskofskeletalcomplicationsinpatientswithbonemetastasesfrom breast carcinoma and is of similar efficacy in patients with multiple myeloma.
More recently, a �2-month, multicenter, randomized, placebo-controlled study in Japanesewomenwithmetastaticbonediseasesecondary tobreastcancer(n=228)demonstratedthatzoledronic acid was significantly more effective than placebo in decreasing the incidence of skeletal-relatedevents.ThetrialwasplacebocontrolledbecausenobisphosphonatehadbeenapprovedinJapanfortreatingpatientswithbonemetastases.Zoledronicacidorplacebowereadministeredvia�5-minuteinfusionsevery4weeksforoneyear.
Theskeletal-relatedeventratewas0.63events/yearinthezoledronicacidgroupversus�.�0events/yearintheplacebogroup(rateratio,0.57;P=0.0�6).Theskeletal-relatedeventrateratioatoneyear(excludinghypercalcemiaofmalignancy)was0.6�(P=0.027),showingthatzoledronicacidreducedtherateofskeletal-relatedeventsby39%comparedwithplacebo.Thepercentageofpatientswithatleastoneskeletal-relatedevent(excludinghypercalcemiaofmalignancy)wasreduced20%byzoledronicacid (29.8%versus49.6%;P=0.003). Inaddition,zoledronicacidconsistentlyreducedtheincidenceofalltypesofskeletal-relatedevents(Figure 3).
Zoledronic acid significantly delayed the time to first skeletal-related event (median not reached versus364days;P=0.007).ZoledronicacidalsoconsistentlyreducedBriefPainInventory(BPI)compositescoresfrombaselineandcomparedwithplacebothroughoutthestudy(Figure 4).

30
Figure5.Percentageofpatientswhoexperiencedaskeletal-relatedeventbyfrequency(intent-to-treatpopulation).
Zoledronicacidwaswelltoleratedandmostadverseeventsweremildtomoderateinseverity.Similar tootherbisphosphonate studies, themost frequentadverseevents suspected tobestudydrug-relatedwerepyrexia,nausea,and fatigue.Therewasnoevidenceofdecreasedrenalfunctionamongpatientstreatedwithzoledronicacidcomparedwithplacebo.
The authors comment that the magnitude of the therapeutic benefit after one year was striking. Zoledronicacidproducedanabsolute20%andarelative40%reductioninthepercentageofpatientswithatleastoneskeletal-relatedeventcomparedwithplacebo.Incomparison,earlierpamidronate trials thatenrolledsimilarpatientsdemonstratedanabsolute�0-�3%reductionand a relative �8-23% reduction in the percentage of patients with a skeletal-related eventafter one year (Theriault et al 1999; Hortobagyi et al 1996). This is consistent with the findings oftherandomizedtrialbyRosenetal(2004),whichshowedthatzoledronicacidissuperiortopamidronate,particularlyamongpatientswithpredominantlyosteolyticlesions.
Cartenì and colleagues (2006) described a recent open-label study of the efficacy and safety of zoledronic acid in breast cancer patients with newly diagnosed ( 6weeks)bone metastases. Zoledronicacid(4mg)wasadministeredviaa�5-minute infusionevery3or4weeks for 12 infusions. Skeletal-related events were defined as pathologic bone fractures, spinal cord compression, surgery to bone, radiation therapy to bone, and hypercalcemia ofmalignancy.
Among3�2patientsenrolled,30%experiencedatleastoneskeletal-relatedeventduringthe�2-monthstudyand22%experiencedonlyoneskeletal-relatedevent(Figure 5).
Themostcommonskeletal-relatedeventwasradiationtobone(22%),followedbypathologicnon-vertebral fractures (4.8%). The median time to first skeletal-related event was not reached. Of237evaluablepatients,�38(58%)experiencedadecreaseinpainscore,�9%nochangefrombaseline,and23%anincreaseinpain.Inqualityoflifeanalysis,totalFACT-Gindicatednochangeinoverallscoreandimprovementsinthephysicalwell-being,emotionalwell-being,andfunctionalwell-beingsubscales.
Zoledronicacidwaswelltolerated.Adverseeventsweregenerallymildtomoderateinseverityand were consistent with the known safety profile of intravenous bisphosphonates. The most frequentlyreportedadverseevents,regardlessofrelationshiptostudydrug,werepyrexia(22%)andbonepain (�0%).Of thepatientswho reportedpyrexia,85%hadonlyasingleepisodefollowing the first infusion. Serum creatinine levels did not increase significantly from baseline.
Inconclusion,breastcancerpatientswithnewlydiagnosedbonemetastaseswhoweretreatedwith zoledronic acid experienced a low incidence of skeletal-related events compared with

3�
patients who received placebo, and pain was decreased from baseline. This study confirms both the efficacy and safety of zoledronic acid in the treatment of patients with bone metastases fromadvancedbreastcancer.
Themorerecenttrials(suchasthatbyCartenì et al, above) havefrequentlyincludedformalqualityoflife(QoL)assessments.AdetailedstudybyWeinfurtetal(2004)measuredhealth-relatedQoLinpatientswithmetastaticbreastcancerwhoweretreatedwithzoledronicacidorpamidronate.Asmaybepredicted,patientswithahistoryofskeletal-relatedeventsbeganthestudy with significantly lower QoL scores. Patients receiving zoledronic acid or pamidronate over thecourseof the�2-monthstudyreportedimprovements inQoLincludingareasofphysical,functional,andemotionalwell-being.Bothpainandanalgesicusedecreased frombaseline.These results suggest that by, effectivelypreventing skeletal-relatedevents,QoL is likely toimprove.
Clemons and colleagues (2006) evaluated whether additional benefits would be gained from useofzoledronicacid (4mg) inmetastaticbreastcancerpatientswhosufferedprogressivemetastases or skeletal-related events despite prior therapy with pamidronate or clodronate.Thirty-one women completed the 8-week study. By week 8, patients experienced significant improvementinpaincontrol(P<0.00�)withadownwardtrendinaboneturnovermarker(urinaryN-telopeptide) (P=0.008). This is the first study to demonstrate that patients with progressive bone metastases or skeletal-related events can obtain clinically relevant palliative benefits by a switch from clodronate or pamidronate to zoledronic acid. If confirmed in randomized trials, this finding would have major implications for the use of bisphosphonates in both metastatic and adjuvantsettings.
Lung cancerSkeletal-relatedeventscomplicatetheclinicalcourseformanypatientswithlungcancerandother solid tumors, despite improvements in primary therapy. Compared to investigations ofskeletal complicationsassociatedwithbreastcancer,studiesofbisphosphonates inpatientswithothersolidtumorshavebeenmorelimited.Againstthisbackground,trialsofzoledronicacidin patients with lung and other solid tumors offer evidence of significant clinical benefit.
Rosen et al (2003) assessed the efficacy and safety of zoledronic acid in 773 patients with bone metastasessecondary tosolid tumorsother thanbreastorprostatecancer inamulticenter,randomized, placebo-controlled, nine-month trial. Approximately 50% of patients had non-small cell lung cancer (NSCLC), 8% small-cell lung cancer, and �0% renal cell carcinoma.Twothirdsofthepatientshadexperiencedaskeletal-relatedeventbeforestudyentry.Patientswererandomlyassignedtoreceivezoledronicacid(4or8mg)orplaceboevery3weeksfor9months,withconcomitantantineoplastictherapy.The8mgdosewasreducedto4mg(8/4mggroup)duringthetrialbecauseofconcernsoverdecreasedrenaltolerabilityatthehigherdoselevel. The primary efficacy assessment was the proportion of patients with at least one skeletal-related event, defined as pathologic fracture, spinal cord compression, radiation therapy to bone,andsurgerytobone.
Theproportionofpatientswithaskeletal-relatedeventwas reduced inbothzoledronicacidgroupscomparedwithplacebo(38%for4mgand35%for8/4mgzoledronicacidversus44%forplacebo;P=0.�27andP=0.023,respectively).Intheanalysisofallskeletalevents(including

32
Fig 6. Kaplan-Meier estimates of time to first skeletal-relatedevent(notincludinghypercalcemiaofmalignancy).
hypercalcemia of malignancy), 4 mg zoledronic acid significantly reduced the proportion of patientswithaneventcomparedwithplacebo(38%versus47%;P=0.039).Additionally,4mgzoledronic acid significantly increased the time to first event (median 230 versus 163 days for placebo;P=0.023)(Figure 6) and significantly reduced the risk of developing skeletal events (hazardratio0.732;P=0.0�7).
Theskeletalmorbidityrate(thenumberofeventsperyear;includinghypercalcemia)wassignificantly lower among patients treated with 4 mg zoledronic acid (mean ± SD 2.24 ± 9.12; P=0.017) compared with placebo (2.73 ± 5.29).
ThemeanBPIcompositepainscoreincreasedslightlyfrombaselinetomonth9inalltreatmentgroups.However,themeancompositepainscoredecreasedinpatientsinthe4mgzoledronicacid group who had pain at baseline. There were no statistically significant differences between zoledronic acid andplacebo with respect to anyglobal quality of life outcomes.Allmarkersofbonemetabolismdecreasedfrombaselinetostudyendinpatientstreatedwithzoledronicacid.
Zoledronicacidwaswelltolerated.Theproportionofpatientsexperiencingnausea,vomiting,anddyspneawashigherinthe4mgzoledronicacidgroupthantheplacebogroup,whereasmore patients experienced bone pain in the placebo group. The proportion of patients withdecreased renal function (based on change in serum creatinine) was not significantly different betweenthe4mgzoledronicacidandplacebogroups.
Inconclusion,zoledronicacidattherecommendeddoseof4mgviaa�5-minuteinfusionevery3weeksproducedaconsistentreductioninskeletalmorbiditycomparedwithplaceboinpatientswith lung cancer and other solid tumors. The authors point out that zoledronic acid is the first bisphosphonateshowntoreduceskeletalcomplicationsinpatientswithbonemetastasesfromsolidtumorsotherthanbreastandprostatecancer.
Rosen et al (2004) subsequently reported on the efficacy and safety of zoledronic acid therapy administeredover2�monthsinthesepatients.Atendpoint,fewerpatientstreatedwithzoledronicaciddevelopedatleastoneskeletal-relatedeventcomparedwithpatientstreatedwithplacebo(39% with 4mg dose [P=0.�27] and 36% with 8/4 mg dose [P=0.023], compared with 46%treated with placebo). Furthermore, 4 mg zoledronic acid significantly delayed the median time to first skeletal-related event (236 days versus 155 days with placebo; P=0.009) and significantly reducedtheannualincidenceofskeletal-relatedevents(�.74versus2.7�peryear;P=0.0�2).

33
Fig.7. Kaplan-Meier estimates of time to first skeletal-relatedeventinpatientswithbonemetastasesfromrenalcellcarcinomaduringa9-monthtrialofzoledronicacid.Datapresentedareforthe4-mgzoledronicacidandplacebogroups.Thenumberofevaluablepatientsineachgroupislistedforeachofthetimepoints.NR,notreached;SRE,Skeletal-relatedevent.
The4mgdoseofzoledronicacidreducedtheriskofdevelopingaskeletaleventby3�%(hazardratio0.693;P=0.003).Zoledronicacidwaswelltoleratedonlong-termuse;themostcommonlyreportedadverseeventsinalltreatmentgroupsincludedbonepainandtransient,acute-phasereactions of nausea, anemia, and emesis. To the authors’ knowledge, zoledronic acid is the first bisphosphonate to demonstrate longer-term safety and efficacy in this patient population.
A retrospective exploratory analysis of these patients concentrated on the influence of a historyofskeletalcomplicationson the response tozoledronicacid.Beforestudyentry,347(69%) of 503 patients evaluable for efficacy experienced one or more skeletal-related events. Thesepatientshadahigherriskofdevelopingaskeletal-relatedeventduringthestudythanpatientswithnopriorevent(oddsratio�.4�).Forpatientswithaskeletal-relatedeventbeforestudyentry,zoledronicacidwhencomparedwithplaceboreducedtheriskoffurthereventsby3�%(P=0.009),reducedthemeanskeletalmorbidityrate(�.96versus2.8�eventsperyear;P=0.030), and prolonged the median time to first event (215 days versus 106 days; P=0.011). Inpatientswithnoskeletal-relatedeventbeforestudyentry,zoledronicacidreducedtheriskofeventsby23%(P=0.308),reducedthemeanskeletalmorbidityrate(�.34versus2.53eventsper year; P=0.332), and prolonged the median time to first event by 2.5 months (P=0.534). This exploratoryanalysisindicatesthatzoledronicacidreducesskeletalmorbidityregardlessofthehistoryofskeletal-relatedevents.
Renal cancerAsubsetanalysisof thesolid tumor trialbyRosenetal (reportedabove)wasperformed toinvestigate the efficacy of zoledronic acid in renal cell carcinoma patients (Lipton et al 2003). Among the 74 renal carcinoma patients in the trial, there was a high incidence of skeletal-relatedeventsandheavyburdenofdiseasefrombonemetastasesatbaselinecomparedwiththe overall trial population, reflecting the aggressive nature of bone metastases from renal cell carcinoma.
Significantly fewer patients treated with 4 mg zoledronic acid had a skeletal-related event comparedwithplacebo(37%versus74%,P=0.0�5).(Thiscompareswitheventratesof44%for placebo in the overall trial population.) Zoledronic acid significantly prolonged the time to first skeletal-relatedevent(mediannotreachedat9monthsversus72daysforplacebo;P=0.006)(Figure 7).

34
Zoledronic acid also significantly reduced the annual incidence of skeletal-related events by 21% (mean 2.68 versus 3.38 events per year for placebo, P=0.014) and significantly reduced theriskofdevelopingaskeletal-relatedeventby6�%comparedwithplacebo(riskratio0.394,P=0.008). Median time to progression of bone lesions was significantly extended with zoledronic acidtreatment(P=0.0�4).Theauthorscommentthat,becauseoftheclinicallyaggressivenatureofbonelesionsinrenalcellcarcinoma,thesepatientshavethepotentialtoreceivesubstantialbenefit from treatment with zoledronic acid.
Zoledronic acid was well tolerated and the adverse event profile of zoledronic acid was similar to thatofplacebo.Adverseeventsoccurringmorefrequentlyinpatientsreceivingzoledronicacidincludednausea,fatigue,pyrexia,rigors,andlower-limbedema.Consistentwiththereportedanalgesiceffectsof zoledronicacid,morepatients in theplacebogroup reportedbonepain(63%versus52%with4mgzoledronicacid).Renal functionwascloselymonitoredand theprofile of renal-related adverse events was similar in the 4 mg zoledronic acid and placebo groups. Therefore, 4 mg of zoledronic acid appears not to be associated with any significant elevatedriskofdecreasedrenalfunctioninpatientswithrenalcellcarcinoma.
Atotalof�3renalcellcarcinomapatientswereenrolled in the2�-monthextensionphaseofthe trial (Lipton et al 2004). Results from the extension phase confirmed the nine-month study. Median times to first event (median 424 versus 72 days; P=0.007) and to bone lesion progression (median 589 versus 89 days; P=0.014) were significantly prolonged in the 4 mg zoledronic acid group compared with placebo. A non-significant trend to improved survival was also observed for patientstreatedwithzoledronicacid(median347versus2�6days;P=0.�04).Thesafetydatawere consistent with the nine-month core analysis. The efficacy results may suggest possible antitumoreffectsforzoledronicacid,whicharebeingfurtherinvestigated.
Zoledronic acid is the first bisphosphonate to provide the clinically meaningful benefits of significantly reduced skeletal morbidity and significantly prolonged time to bone lesion progression inpatientswithbonemetastasesfromrenalcellcarcinoma.
Prostate cancerThe effect of zoledronic acid on skeletal complications in patients with hormone-refractoryprostate cancer and a history of bone metastases was investigated by Saad et al (2002).Patientswererandomlyassignedtodouble-blindtreatmentwithintravenouszoledronicacidat4mg(n=2�4)or8mg(subsequentlyreducedto4mg;8/4)(n=22�),orplacebo(n=208)every3 weeks for 15 months. Proportions of patients with skeletal-related events, time to the first skeletal-relatedevent,skeletalmorbidityrate,painandanalgesicscores,diseaseprogression,andsafetywereassessedinthiswell-designedtrial.
Therateofskeletal-relatedeventswashigherinpatientswhoreceivedplacebo(44.2%)thaninthose who received zoledronic acid at 4 mg (33.2%; –11.0% difference, 95% confidence interval [CI]–20.3%to–�.8%;P=0.02�)orat8/4mg(38.5%;–5.8%difference,95%CI=–�5.�%to3.6%; P=0.222). Compared with patients who received placebo, significantly fewer patients who receivedzoledronicacid4mgexperiencedafracture(22.�%versus�3.�%,P=0.0�5)andany

35
skeletal-related event other than fracture (34.6% versus 25.7%, P=0.048). Median time to first skeletal-relatedeventwas32�daysforpatientswhoreceivedplaceboandwasnotreachedforpatientswhoreceivedzoledronicacid4mg(P=0.0��)(Figure 8).
Urinary markers of bone resorption (N-telopeptide-, pyridinoline-, and deoxypyridinoline-to-creatinine ratios) were significantly decreased in patients who received zoledronic acid comparedwithplacebo.Serumbonealkalinephosphatase,asameasureofboneformationactivity, increased significantly more in patients who received placebo than in patients who receivedzoledronicacidat4mg(33.7%,95%CI=2�.�%to56.3%,P=0.00�).LevelsofserumPTH increased significantly more in patients who received zoledronic acid 4 mg than in patients whoreceivedplacebo(�7.�%,95%CI=3.3%to27.5%,P=0.00�).
Themediansurvival timewas464daysforpatientswhoreceivedplaceboand546daysforpatients who received zoledronic acid at 4 mg (P=0.091). There were no significant differences between patients who received zoledronic acid and those who received placebo regardingpercent change from baseline in serum prostate specific antigen (PSA), indicating that zoledronic acidhadnoapparenteffectonthesecretionorclearanceofPSA.
Painandanalgesicusescoresincreasedmoreinpatientswhoreceivedplacebothaninpatientswho received zoledronic acid. Disease progression, performance status, and quality-of-lifescoresdidnotdifferbetweenthegroups.Zoledronicacid4mggivenasa�5-minuteinfusionwaswell tolerated.Fatigue,anemia,myalgia, fever,and lower limbedemaoccurred inmorepatientsinthezoledronicacidgroupsthanintheplacebogroup.Renalfunctiondeteriorationoccurredin�5.2%ofpatientswhoreceivedzoledronicacidat4mgcomparedto��.5%whoreceivedplacebo.
Thestudyhadalowcompletionrate,withaboutonethirdofpatientscompletingtheplanned�5monthsofstudytreatment.Theauthorscommentthatthisisnotsurprisinggiventhemediantimetodiseaseprogressionof84days foreach treatmentgroupand themediansurvivalofapproximately�5monthsintheplacebogroup.
Inconclusion,allmajorstudyoutcomesconcerningskeletal-relatedeventsweresuperior forpatientswhoreceivedzoledronicacid4mgthanforpatientswhoreceivedplacebo.Zoledronicacid4mgwasconcludedtoreduceskeletal-relatedeventsinprostatecancerpatientswithbonemetastases.
Inananalysisof�22patientswhocompleted24monthson thestudy, fewerpatients in the
Fig.8.Kaplan–Meierestimatesofeventratesfortime to the first on-study skeletal-related event for all intent-to-treatpatientswithmetastaticprostatecancerrandomlyassignedtoreceivezoledronicacidat4mg,zoledronicacidat8/4mg,orplacebo.Thenumberofpatientsatriskateachtimepointisshowninthetablebelowthegraph.Atthelaststudyevaluation(450days),Pvalue(two-sided)fromCoxregression=.0��forzoledronicacidat4mgversusplaceboandP=.49�forzoledronicacidat8/4mgversusplacebo.

36
zoledronicacid4mggroupthanintheplacebogrouphadatleastoneskeletal-relatedevent(38% versus 49%, difference –��.0%, 95% CI –20.2% to –�.3%; P=0.028), and the annualincidence of events was 0.77 versus 1.47 (P= 0.005). The median time to first skeletal-related eventwas488daysforthezoledronicacid4mggroupversus32�daysforplacebo(P=0.009).Comparedwithplacebo,zoledronicacid4mgreducedtheongoingriskofskeletal-relatedeventby36%(risk ratio0.64,95%CI=0.485 to0.845;P=0.002).Long-termtreatmentwith4mgof zoledronic acid was therefore concluded to provide sustained clinical benefits for men with metastatichormone-refractoryprostatecancer.Theoptimaldurationofzoledronicacidtherapyis not known and therefore, similar to the treatment guidelines for breast cancer, it may bereasonabletotreatpatientswithzoledronicacidforaslongasitistoleratedoruntilthepatientexperiencesasubstantialdeclineinperformancestatus.
Asubanalysisofthistrialwasalsoperformedtoassessclinicallymeaningfulchangesinpainusing the BPI over 60 weeks (Weinfurt et al 2006). For all �� pain assessments, patientsreceivingzoledronicacid(n=76)reportedmorefavorable,clinicallymeaningfulchangesinpainscoresthanpatientsreceivingplacebo(n=62).Overall,patientsreceivingzoledronicacidhada33%chanceofafavorablepainresponse,comparedwith25%forpatientsreceivingplacebo(P=0.04;95%CI0.5%to�5.6%).Zoledronicacidwas thereforemore likely thanplacebo tobeassociatedwithclinicallymeaningfulreductionsinpain.Inconclusion,zoledronicacidmayhelptoavertthepainexperiencedbypatientswithprogressingmetastaticdiseasesecondarytoprostatecancer.
Applications in androgen deprivation therapyAndrogendeprivationasprimary tumor therapyreducesbonemineraldensityand increasesthe risk of fracture in patients with prostate cancer. Even in the absence of metastases tobone, therefore, zoledronic acid may be expected to offer benefits for skeletal integrity in these patients.Ryanetal (2006)evaluated theeffectsofzoledronicacidonbonemineraldensityandbiochemicalmarkersofboneturnover in�20patientswithprostatecancerwithoutbonemetastaseswhohad receivedandrogendeprivation therapy for�2monthsor less.Patientswererandomizedtoreceive4mgzoledronicacidorplacebointravenouslyevery3monthsforone year, with stratification according to androgen deprivation therapy duration (less than 6 monthsversus6-�2months).Comparedwithplacebo,zoledronicacidincreasedbonemineraldensityatoneyearatthefemoralneck,totalhip,andlumbarspineby3.6%(P=0.0004),3.8%(P<0.0001) and 6.7% (P<0.0001), respectively. The benefits of zoledronic acid on bone mineral density were independent of androgen deprivation therapy duration. Additionally, bone specific alkalinephosphataseandN-telopeptidelevelsdecreasedfrombaselineinthezoledronicacidgroup(P<0.000�)butincreasedintheplacebogroup.Inconclusion,zoledronicacidincreasedbonemineraldensityandsuppressedmarkersofboneturnoverinpatientswithprostatecancerwithoutbonemetastases.
Saadandcolleagues(2006)havecommentedrecently thatatreatmentalgorithmdevelopedatthe3rdInternationalConsultationonProstateCancerhadrecommendeduseofzoledronicacidforthepreventionofskeletalcomplicationsinpatientswithbonemetastasesfromprostatecancer,regardlessofhormonestatus,andforthepreventionof treatment-inducedbonelossinpatientswithoutevidenceofbonemetastases.Accordingtothisalgorithm,zoledronicacidshouldbeconsideredforthepreventionofskeletalmorbidity inpatientswithprostatecancerthroughouttheirtreatmentcontinuum.

37
Fig.9.Medianchangefrombaseline(percent)valuesforurinaryN-telopeptide-to-creatinineratio(A),serumbonealkalinephosphatase(B),andserumparathyroidhormone(C),allmeasuresofbonemetabolism,inpatientswithmetastaticprostatecancerenrolledinarandomized,placebo-controlledphaseIIItrial of zoledronic acid. Error bars show 95% confidence intervals formedianpercentchangeat3months,9months,andattheendofthestudy.Atthelastvisit,allPvalues(two-sided)fromCochran–Mantel–Haenszel test with modified ridit score = .001 for thedifferencebetweeneachzoledronicacidgroupandplacebo,withtheexceptionthatP=.003forthedifferenceinserumbonealkalinephosphatasebetweenzoledronicacidat8/4mgandplacebo.
Metabolic bone disorders
Paget’s disease of boneTworandomized,double-blind,active-controlledtrialscomparedasingle�5-minuteinfusionof5mgzoledronicacidwith60daysoforalrisedronate(30mgperday)in357menandwomenwith radiologically confirmed Paget’s disease of bone. The primary efficacy endpoint was the rate of therapeutic response at six months, defined as normalization or at least a 75% reduction inalkalinephosphataselevels.
Inthepooledresults,serumalkalinephosphataselevelsweremorerapidlyandmarkedlyreducedin thezoledronicacidgroup than in the risedronategroup (Figure9A).Ratesof therapeuticresponsewereconsistentlyhigher inthezoledronicacidgroupthanintherisedronategroupfrom�0daysonward,attainingratesof96.0%and74.3%,respectively,atsixmonths(P<0.00�)(Figure9B).Alkalinephosphataselevelsnormalizedin88.6%and57.9%ofpatients,respectively(P<0.00�)(Figure9C).
Zoledronic acid was associated with a shorter median time to first therapeutic response than risedronate(64versus89days,P<0.00�).Thehigherratesofresponseinthezoledronicacidgroupwereindependentofpatientage,sex,baselinealkalinephosphataselevel,andpresenceorabsenceofprevioustherapyforPaget’sdisease.SerumlevelsoftheN-terminalpropeptideof type I collagen, a specific index of osteoblast activity, showed a pattern similar to alkaline phosphatasebuttheresponsetendedtobegreater.Boneresorption,assessedbyserumlevelsofC-telopeptideandtheratioofurinary C-telopeptidetocreatinine,showedgreaterreductionswithzoledronicacidthanrisedronateatalltimes.
Qualityoflife,measuredbythephysical-componentscoreoftheMedicalOutcomesStudy36-item Short-Form General Health Survey, increased significantly from baseline at both three and

38
six months in the zoledronic acid group and differed significantly from the risedronate group at threemonths.Painscores improved inbothgroups.Duringpost-trial follow-up (median�90days),2�of82patients(25.6%)intherisedronategroupsufferedalossoftherapeuticresponse,comparedwithoneof��3patients(0.9%)inthezoledronicacidgroup(P<0.00�).
The numbers of patients with adverse events (�46 in the zoledronic acid group and �33 intherisedronategroup)andseriousadverseevents(9and��,respectively)weresimilarinthetwo groups. The mean serum creatinine level decreased slightly but significantly by day 10 in thezoledronicacidgroupcomparedwith the risedronategroup.Atsubsequentvisits,serumcreatinine values were similar and did not differ significantly.
Asingle infusionof5mgzoledronicacidovera�5-minuteperiod isconcludedtoproduceamorerapid,complete,andsustainedresponsethandailytreatmentwithrisedronateinpatientswith Paget’s disease. No other currently used agent has been demonstrated to yield significant improvementsinquality-of-lifemeasuresinrandomized,controlledtrials.Thegreaterconveniencefor the patient from the zoledronic acid regimen is an additional benefit of importance for patients withPaget’sdisease.Onthebasisofthesedata,zoledronicacidreceivedEuropeanmarketingauthorizationforthetreatmentofPaget’sdiseaseofthebone.
OsteoporosisOralbisphosphonatesarewidelyusedagentsinthetreatmentofosteoporosis,buttheyrequiredailyadministrationonanemptystomach,whichisassociatedwithgastrointestinalintoleranceinadditiontothepoorbioavailabilityfromthisrouteofadministration.Theglobalrateofnon-compliancewithlong-termoralbisphosphonatetherapyforosteoporosishasbeenreportedtobeabove50%.Analternativerouteofdelivery,byintravenousadministration,hasnotbeenasextensivelystudied,buttrialsofzoledronicacidofferpromisingoutcomes.
Reidetal(2002)examinedtheeffectsofintravenouszoledronicacidonboneresorptionin35�postmenopausalwomenwithlowbonemineraldensityinarandomized,double-blind,placebo-controlledtrial.Patientsreceivedzoledronicacidat0.25mg,0.5mg,or�mgatthree-monthintervals. A fifth group received zoledronic acid 4 mg as a single annual dose and a sixth group receivedtwodosesof2mgeach,sixmonthsapart.
Bone mineral density of the lumbar spine increased 4.3–5.�% in all zoledronic acid groupscompared to placebo (P<0.00�). Femoral neck BMD increased 3.�-3.5% in zoledronic acidgroupscomparedtoplacebo(P<0.00�),whiledistalradiusBMD(0.8to�.6%)andtotalbodyBMD (0.9 to 1.3%) were also significantly elevated in all but one zoledronic acid treatment group.Biochemicalmarkersofboneresorptionwerecomparablysuppressedinallzoledronicacidgroupscomparedtoplacebo,reachinganadirat�month(mediandecreasesof65-83%inserumC-telopeptideand50-69%inurinaryN-telopeptide:creatinineratio)whichwassustainedat�2months.Biochemicalmarkersofboneformation,includingserumosteocalcinandbone-specific alkaline phosphatase, showed suppression persisting at 12 months for all zoledronic aciddoses(P<0.00�).
In general, zoledronic acid was well-tolerated, with the most common adverse effects ofdecreasedcalciumconcentrations,myalgia,andpyrexia.Meanserumcalciumconcentrations

39
declinedbyapproximately0.08mmol/Lbetweenbaselineandonemonthinthezoledronicacidgroups (P<0.05 forall comparisons).From3monthsonwards, calciumconcentrationsweresimilarbetweenzoledronicacidandplacebogroups.Treatment-relateddropoutrateswerenotsignificantly different between the groups.
Theseresultsindicatethatanannualinfusionofzoledronicacidcanproduceanincreaseinbonemineraldensitysimilar to thatof thedailyadministrationoforalbisphosphonates.Anannualinfusionofzoledronicacidmaybeaneffectivetreatmentforpostmenopausalosteoporosisandmayrepresentanattractiveoptionwiththepotentialtoincreasepatientcomplianceandpossiblyminimizetheriskofadverseeffectscomparedtooralbisphosphonatetherapy.
Supportivedatawerepresentedrecentlyatthe2006AmericanSocietyforBoneandMineralResearch conference. The Health Outcomes and Reduced Incidence with Zoledronic acidOnce yearly (HORIZON) Pivotal Fracture Trial (n=7736) evaluated the potential of yearlyinfusionofzoledronicacid5mg todecreaseriskof fracture inpostmenopausalwomenwithosteoporosis.Interimanalysisencompassing99%ofdatafromthestudyshowedthatpatientstakingzoledronicacidexperienceda70%riskreductioninnewspinefractures(P<0.000�)anda40%riskreductioninhipfractures(P=0.0032)over3yearscomparedtoplacebo.Thismetthestudy’stwoprimaryendpoints.Themostcommonsideeffectsincludedfever,musclepain,flu-like symptoms, and bone pain.
Rheumatoid arthritisBased on the results of a recent proof of concept study, zoledronic acid shows promise asa treatment in early rheumatoid arthritis. Jarrett and colleagues (2006) assessed whetherzoledronicacidcouldachievea50%orgreaterreductioninthedevelopmentofnewerosionsin39patientswithearlyrheumatoidarthritisandclinicalsynovitisofthehandorwrist.Patientswererandomizedtoreceiveinfusionsofeitherzoledronicacid(5mg)orplaceboatbaselineandatweek�3,andbothgroupsadditionallyreceivedmethotrexate(MTX)7.5-20mg/week.
Atweek26, themeanchange inhandandwristerosionsassessedatmagnetic resonanceimaging(MRI)was6�%lowerinthezoledronicacidthantheplacebogroup(0.9versus2.3;P=0.�76).Themean increase innumberofhandandwristboneswitherosionswas0.3 forzoledronicacidcomparedwith�.4forplacebo(P=0.029).TheproportionofpatientswithnewMRI-visualizedboneedemawasnumericallylowerinthezoledronicacidgroupcomparedwithplacebo (33% versus 58%; P=0.121). The safety profile of zoledronic acid was similar to that of placebo.
The results of this study suggest that zoledronic acid therapy proves structural benefit to bone inpatientswithrheumatoidarthritis.

40
Additional potential applications of zoledronic acid
Transplant-related bone lossClinicallyimportantbonelossthatisassociatedwithfracturesoccurswithin3to6monthsoflivertransplantation.A�2-month,randomized,double-blind,placebo-controlledtrialof62adultsundergoing liver transplantation forchronic liverdisease investigated theeffectofzoledronicacid4mg(n=32)orsaline(n=30) infusedwithin7daysof transplantationandatmonths�,3,6,and9(Crawfordetal2006).Allpatientsadditionallyreceivedcalciumcarbonateandergocalciferolsupplementation.Theprimaryoutcomewasbonemineraldensitymeasuredbydualx-rayabsorptiometry.
Differencesinbonelossat3monthsaftertransplantationfavoredzoledronicacidoverplacebo.Groupdifferences,afteradjustingforbaselineweightandserumPTHlevel,were4.0%(95%CI�.�%to7.0%)atthelumbarspine,4.7%(�.9%to7.6%)atthefemoralneck,and3.8%(�.7%to6.0%)atthetotalhip.At�2months,groupdifferenceswere�.�%(-2.�%to4.4%),2.7%(0.0%to5.4%),and2.4%(0.�%to4.7%),respectively.
The authors concluded that treatment with zoledronic acid can prevent bone loss within the first yearafterlivertransplantation.
Thalassemia-induced osteoporosis
Voskaridou and colleagues (2006) evaluated the effect of zoledronic acid in patients withthalassemia-inducedosteoporosis.Sixty-sixpatientswererandomizedtoreceive4mgzoledronicacidintravenouslyevery6months(23patients;groupA)orevery3months(2�patients;groupB)ortoreceiveplaceboevery3months(22patients;groupC)forone�year.Bonemineraldensityofthelumbarspine,femoralneckandwristwasmeasuredbeforeandat�2monthsaftertreatment.
PatientsingroupAshowednochangeinbonemineraldensityatanysiteat�2months,butexperienced reductions in bone pain, bone-specific alkaline phosphatase, osteocalcin, and osteoprotegerin. Patients in group B showed a significant increase in lumbar spine bone mineral density, accompanied by reductions in bone pain, C-telopeptide, bone-specific alkaline phosphatase,C-telopeptide,andosteocalcin.PatientsingroupCshowednoalterationinbonemineraldensityatanysiteandnoimprovementinbonepain,whiletheyexperiencedanincreaseinmarkersofboneresorption.
Zoledronicacidatadoseof4mg intravenouslyevery3monthsappears tobeaneffectivetreatment for increasing bone mineral density and reducing bone resorption in thalassemia-inducedosteoporosis.

4�
References
BerensonJR,HillnerBE,KyleRAetal.AmericanSocietyofClinicalOncologyclinicalpracticeguidelines:theroleofbisphosphonatesinmultiplemyeloma.JClinOncol2002;20:37�9-3736.
BerensonJR,RosenLS,HowellAetal.Zoledronicacid reducesskeletal-relatedevents inpatientswithosteolyticmetastases:adouble-blind,randomizeddose-responsestudy.Cancer200�;9�:��9�-�200.
BerensonJR,VescioRA,RosenLSetal.AphaseIdose-rangingtrialofmonthly infusionsofzoledronicacidforthetreatmentofosteolyticbonemetastases.ClinCancerRes200�;7:478-485.
Body JJ, Lortholary A, Romieu G et al. A dose-finding study of zoledronate in hypercalcemic cancer patients. J Bone Miner Res �999;�4:�557-�56�.
Cartenì G, Bordonaro R, Giotta F et al. Efficacy and safety of zoledronic acid in patients with breast cancer metastatic to bone: a multicenterclinicaltrial.TheOncologist2006;��:84�-848.
Clemons MJ, Dranitsaris G, Ooi WS et al. Phase II trial evaluating the palliative benefit of second-line zoledronic acid in breast cancer patients with either a skeletal-related event or progressive bone metastases despite first-line bisphosphonate therapy. J Clin Oncol 2006Sep25;[Epublicationaheadofprint]
CrawfordBA,KamC,PavlovicJetal.Zoledronicacidpreventsbone lossafter liver transplantation:a randomized,double-blind,placebo-controlledtrial.AnnInternMed2006;�44:239-248.
Gammon DC, Le HT. Zoledronic acid vs pamidronate for the prevention of hypercalcemia of malignancy or bone metastases inhospitaloutpatients:TimeanalysisandeconomicimplicationsHospPharm2003;38:��48-��50.
HillnerBE,IngleJN,BerensonJRetal.AmericanSocietyofClinicalOncologyguidelineontheroleofbisphosphonatesinbreastcancer.AmericanSocietyofClinicalOncologyBisphosphonatesExpertPanel.JClinOncol2000;�8:�378-�39�.
HillnerBE,IngleJN,ChlebowskiRTetal.AmericanSocietyofClinicalOncology2003updateontheroleofbisphosphonatesandbonehealthissuesinwomenwithbreastcancer.JClinOncol2003;2�:4042-4057.
Hirsh V, Tchekmedyian NS, Rosen LS, Zheng M, Hei YJ. Clinical benefit of zoledronic acid in patients with lung cancer and other solid tumors:analysisbasedonhistoryofskeletalcomplications.ClinLungCancer2004;6:�70-�74.
Hortobagyi GN, Theriault RL, Porter L et al: Efficacy of pamidronate in reducing skeletal complications in patients with breast cancer andlyticbonemetastases:Protocol�9ArediaBreastCancerStudyGroup.NEnglJMed�996;335:�785-�79�
Jarrett SJ, Conaghan PG, Sloan VS et al. Preliminary evidence for a structural benefit of the new bisphosphonate zoledronic acid in earlyrheumatoidarthritis.ArthritisRheum.2006;54:�4�0-�4�4.
KenjiK,HironobuM,KeniichiOetal.Amulticenterandopenlabelclinicaltrialofzoledronicacid4mginpatientswithhypercalcemiaofmalignancy.JpnJClinOncol2005;35:28-33.
Kohno N, Aogi K, Minami H et al. Zoledronic acid significantly reduces skeletal complications compared with placebo in Japanese womenwithbonemetastasesfrombreastcancer:arandomized,placebo-controlledtrial.JClinOncol2005;23:33�4-332�
Kraj M, Poglod R, Maj S, Pawlikowski J, Sokolowska U, Szczepanik J. Comparative evaluation of safety and efficacy of pamidronate andzoledronicacidinmultiplemyelomapatients(singlecenterexperience).ActaPolPharm.2002;59:478-482.
LiptonA,Colombo-BerraA,BukowskiRMetal.Skeletalcomplicationsinpatientswithbonemetastasesfromrenalcellcarcinomaandtherapeutic benefits of zoledronic acid. Proceedings of the First International Conference. Clinl Cancer Res 2004;10:6397S-6403S.
LiptonA,TheriaultRL,HortobagyiGNetal:Pamidronatepreventsskeletalcomplicationsandiseffectivepalliativetreatmentinwomenwithbreast carcinomaandosteolyticbonemetastases:Long term follow-upof two randomized,placebo-controlled trials.Cancer2000;88:�082-�090.
LiptonA,ZhengM,SeamanJ.Zoledronicaciddelays theonsetofskeletal-relatedeventsandprogressionofskeletaldisease inpatientswithadvancedrenalcellcarcinoma.Cancer2003;98:962-969.
MajorP,LortholaryA,HonJetal.Zoledronicacidissuperiortopamidronateinthetreatmentofhypercalcemiaofmalignancy:apooledanalysisoftworandomized,controlledclinicaltrials.JClinOncol200�;�9:558-567.
NussbaumSR,Warrell JrRP,RudeRetal.Dose-responsestudyof alendronate sodium for the treatmentof cancer-associatedhypercalcemia.JClinOncol�993;��:�6�8-�623.
ReidIR,BrownJP,BurckhardtP,HorowitzZ,RichardsonP,TrechselU.Intravenouszoledronicacidinpostmenopausalwomenwithlowbonemineraldensity.NEnglJMed2002;346:653.
RosenLS,GordonD,KaminskiMetal.Zoledronicacidversuspamidronateinthetreatmentofskeletalmetastasesinpatientswithbreastcancerorosteolyticlesionsofmultiplemyeloma:aphaseIII,double-blind,comparativetrial.CancerJ200�;7:377-387.
Rosen LS, Gordon D, Kaminski M et al. Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in thetreatmentofskeletalcomplicationsinpatientswithadvancedmultiplemyelomaorbreastcarcinoma:arandomized,double-blind,multicenter,comparativetrial.Cancer2003;98:�735-�744.
RosenLS,GordonD,TchekmedyianSetal.Zoledronicacidversusplacebointhetreatmentofskeletalmetastasesinpatientswithlungcancerandothersolidtumors:aphaseIII,double-blind,randomizedtrial—TheZoledronicAcidLungCancerandOtherSolid

42
TumorsStudyGroup.JClinOncol2003;2�:3�50-3�57.
Rosen LS, Gordon D, Tchekmedyian NS et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases inpatientswithnonsmallcelllungcarcinomaandothersolidtumors:arandomized,PhaseIII,double-blind,placebo-controlledtrial.Cancer2004;�00:26�3-262�.
RosenLS,GordonDH,DuganWJretal.Zoledronicacidissuperiortopamidronateforthetreatmentofbonemetastasesinbreastcarcinomapatientswithatleastoneosteolyticlesion.Cancer2004;�00:36-43.
RossJR,SaundersY,EdmondsPMetal.Asystematicreviewoftheroleofbisphosphonatesinmetastaticdisease.HealthTechnolAssess2004;8:�-�76.
Ryan CW, Huo D, Demers LM, Beer TM, Lacerna LV. Zoledronic acid initiated during the first year of androgen deprivation therapy increasesbonemineraldensityinpatientswithprostatecancer.JUrol2006;�76:972-978.
SaadF,GleasonDM,MurrayRetal;fortheZoledronicAcidProstateCancerStudyGroup.Randomized,placebo-controlledtrialofzoledronicacidinpatientswithhormone-refractorymetastaticprostatecarcinoma.JNatlCancerInst2002;94:�458-�468.
Saad F, Gleason DM, Murray R et al; for the Zoledronic Acid Prostate Cancer Study Group. Long-term efficacy of zoledronic acid for the preventionofskeletalcomplicationsinpatientswithmetastatichormone-refractoryprostatecancer.JNatlCancerInst2004;96:879-882.
SaadF,McKiernanJ,EasthamJ.Rationaleforzoledronicacidtherapyinmenwithhormone-sensitiveprostatecancerwithorwithoutbonemetastasis.UrolOncol2006;24:4-�2.
Smith MR, Eastham J, Gleason DM et al. Randomized controlled trial of zoledronic acid to prevent bone loss in men receivingandrogendeprivationtherapyfornonmetastaticprostatecancer.JUrol2003;�69:2008-20�2.
TheriaultRL,LiptonA,HortobagyiGNetal:Pamidronatereducesskeletalmorbidityinwomenwithadvancedbreastcancerandlyticbonelesions:Arandomized,placebo-controlledtrial:Protocol�8ArediaBreastCancerStudyGroup.JClinOncol�999;�7:846-854.
ThiébaudD,JaegerP,BurckhardtP.ResponsetoretreatmentofmalignanthypercalcemiawiththebisphosphonateAHPrBP(APD):respectiveroleofkidneyandbone.JBoneMinerRes�990;5:22�-226.
VogelCL,YanagiharaRH,WoodAJetal.Safetyandpainpalliationofzoledronicacidinpatientswithbreastcancer,prostatecancer,ormultiplemyelomawhopreviouslyreceivedbisphosphonatetherapy.Oncologist2004;9:687-695.
Voskaridou E, Anagnostopoulos A, Konstantopoulos K et al. Zoledronic acid for the treatment of osteoporosis in patients with β-thalassemia:resultsfromasingle-center,randomized,placebo-controlledtrial.Haematologica2006;9�:��93-�202.
WeinfurtKP,AnstromKJ,CastelLD,SchulmanKA,SaadF.Effectofzoledronicacidonpainassociatedwithbonemetastasis inpatientswithprostatecancer.AnnOncol2006;�7:986-989.
Weinfurt KP, Castel LD, Li Y et al. Health-related quality of life among patients with breast cancer receiving zoledronic acid orpamidronatedisodiumformetastaticbonelesions.MedCare2004;42:�64-�75.

43
Chapter4describescharacteristicsofzoledronicacidthatarerelevanttoclinicalmanagementincluding information on its pharmacological profile, infusion profile, and aspects of adverse eventmanagementapplicabletoallagentsintheclass.
Zoledronic acid is an antihypercalcemic and bone resorption inhibitor that is administeredparenterally.Approvedindicationsvarybycountry,butincludetreatmentforhypercalcemiaofmalignancy,multiplemyeloma,bonemetastasesfromsolidtumorsinconjunctionwithstandardantineoplastic therapy, including breast carcinoma, prostate carcinoma (those that progressaftertreatmentwithat leastonehormonaltherapy),othersolidtumors,andPaget’sdisease.Zoledronic acid also demonstrates efficacy for preventing bone loss in men taking androgen-deprivationtherapyforprostatecarcinoma,inpostmenopausalwomenwithosteoporosis,andinpatientswithearlyrheumatoidarthritis.
For the treatmentofhypercalcemiaofmalignancy,multiplemyeloma,andbonemetastases,adultstypicallyreceive4mginsolutioninjectedintoaveininnotlessthan�5minutes.
Pharmacological profile
ChemistryThe active ingredient of zoledronic acid is (�-hydroxy-2-imidazol-�-yl-phosphonoethyl)phosphonicacidmonohydrate.ThemolecularformulaisC5H�0N2O7P2·H2Oandthemolecularweight290.��.Zoledronicacidisanodorless,whitecrystallinematerial.ItissolubleatalkalinepHandsparinglysolubleinwater.Thedrugissuppliedasasterile,lyophilizedpowderintendedforreconstitutionbeforeinfusion.Therecommendedstoragetemperatureis25°C.
AbsorptionTheareaundertheplasmaconcentrationversustimecurve(AUC)forzoledronicacidisdoseproportionalfrom2to�6mg.Accumulationoverrepeatedcyclesislow.Patientswithmildandmoderaterenal impairmentshowan increasedAUCof�5%and43%,respectively,althoughno significant relationship between zoledronic acid exposure (AUC) and adverse events hasbeenestablished.Theuseofzoledronicacid inpatientswithsevere renal failure isnotrecommended.
Protein bindingProteinbindingisapproximately22%andisindependentofconcentration.
Zoledronic acid: management issues
Chapter 4.

44
EliminationThe excretion of zoledronic acid is primarily renal, at a clearance rate of 3.7 ± 2.0 liters per hour. Theremainderisboundtoboneandisslowlyreleasedbackintosystemiccirculation,givingrisetoa�46hourterminalhalf-life.
Dose-finding studiesDosesselectedforclinicaltrialswerebasedonchangesinboneresorptionmarkersandevidenceof efficacy. In studies of patients with cancer bone metastases, markers were consistently suppressedforatleast4weeksatdoses 4mg.Inpatientswithmultiplemyelomaorbreastcancer bone metastases who received zoledronic acid at 0.4, 2, or 4 mg, there was a significant differenceinskeletal-relatedeventratebetweenthe0.4and4mggroups.Onthebasisofthesestudies,zoledronicaciddosesof4and8mgwereselectedforPhaseIIIevaluation.Inlatertrialsthe4mgdosehasbeenmostfrequentlyinvestigated.
Infusion protocolTheprotocolforadministeringzoledronicacidhasbeenstandardizedasinfusionbyaperipheralintravenous line over no less than �5 minutes. All intravenous bisphosphonates have thepotential to increase serum creatinine levels, and patients with serum creatinine 3.0 mg/dlwereexcludedfromphaseIIIzoledronicacidtrials,sopatientsshouldhaveserumcreatininelevels<3.0mg/dl(<4.5mg/dlinpatientswithhypercalcemiaofmalignancy)inordertoreceivezoledronicacidtreatment.Patientsshouldbeencouragedtodrinktwoglassesofwaterbeforereceivingtheirbisphosphonateinfusion.Thepatient’svitalsignsandtheinfusionsiteshouldbemonitoredperiodicallyduringinfusionandafterinfusioniscompleted.
Duration of bisphosphonate therapyTherearelimiteddataontheoptimaldurationofzoledronicacidtherapy.Currentguidelinesforpatientswithbonemetastasesfrombreastcancersuggestthat,onceinitiated,bisphosphonatetherapy should be continued for as long as it is well tolerated or until there is a significant decreaseintheperformancestatus(Hillneretal2003).Therearenoconsensusguidelinesforthedurationofbisphosphonatetherapyinpatientswithprostatecancer,butrecommendationsfrom a multidisciplinary panel suggest that bisphosphonate treatment should be ongoingafter bone metastases are diagnosed (Carroll et al 2003).This is supported by reports thatthe efficacy of zoledronic acid does not decrease during long-term use. In patients with bone metastasesfromsolidtumorsotherthanbreastorprostatecancer,noformalrecommendationshave been published. However, zoledronic acid has demonstrated significant benefits in this settinginpatientswhohaveexperiencedpriorskeletal-relatedevents,sotreatmentshouldnotbediscontinuedonthebasisofskeletal-relatedeventhistory(Hirshetal2004).
Managing bisphosphonate-related adverse eventsThe safety profile of zoledronic acid has been well established, based on randomized controlled trials and extensive clinical experience. In general, intravenous administration of zoledronicacid is well tolerated with a predictable and manageable side effect profile. The monitoring

45
guidelinesandtreatmentinterruptioncriteriadetailedintheprescribinginformationarethesameforzoledronicacidandpamidronate.
Themostcommonadverseeventsassociatedwithadministrationofintravenousbisphosphonatesare self-limiting flu-like symptoms related to an acute-phase reaction. These symptoms typically develop within 24 hours after the first infusion, and symptoms generally persist for 48hours(Zojeretal�999).Acute-phasereactionsusuallydiminishordisappearfollowingthesecondorthirdinfusion.
Alesscommonadverseeventisdecreasedrenalfunction,whichmayoccuraftertheadministrationofanyintravenousbisphosphonate.Approximately�0%ofpatientstreatedwithzoledronicacid(4 mg via 15 minute infusion) develop renal function deterioration, defined as an increase of 0.5 mg/dlinpatientswithnormalbaselineserumcreatinineoranincreaseof�.0mg/dlinpatientswith baseline serum creatinine �.4 mg/dl, which is similar to the frequency reported for 90mgpamidronatevia2-hourinfusion.Itisbelievedthatunderlyingdisease-relatedfactorsmaycontributetotheincidenceofrenalimpairmentinpatientswithmultiplemyelomaoradvancedcancer(Corsoetal2002).
Renalmonitoringguidelineshavebeenestablishedtominimizetheriskofrenaldeteriorationduringintravenousbisphosphonatetherapy(Berensonetal2002;Hillnesetal2000).Serumcreatinine should be measured within 7 to 10 days of the first infusion and measured before administrationofeachsubsequentdose(Hillneretal2003).Infusionofbisphosphonateshouldbewithheldinanypatientwhoseserumcreatininelevelhasincreasedby50%abovebaseline,inpatientswithnormalbaselineserumcreatininewhoselevelsincreasedby 0.5mg/dl,andinpatientswithabnormalbaselineserumcreatininewhoselevelshaveincreasedby �.0mg/dl.Infusioncanberesumedafterserumcreatininehasreturnedtowithin�0%ofbaseline.
Acomplicationoccurring in less than2%ofpatients inphase IIIclinical trialsof intravenousbisphosphonates is ocular inflammation. For patients who develop ocular symptoms, prompt ophthalmologicevaluationwilldeterminethesafetyofsubsequentbisphosphonatetherapy.
Recently, retrospective case studies have reported an association between long-termbisphosphonatetherapyandosteonecrosisofthejaws.Theincidenceofosteonecrosisappearstoberare,occurringin<�in�0000patients.Theriskofdevelopingosteonecrosisatanysiteisfourtimeshigherincancerpatientsthaninthenormalpopulationduetomultipleriskfactors,includingchemotherapyorradiationtherapy.Trauma,infection,andahistoryofdentalprocedurescontribute to an elevated risk (Tarassoff & Csermak 2003). Physicians should assess the dental statusofpatientsbeforeadministrationofbisphosphonatetherapyandmonitorpatientsfororalhygieneandtheoccurrenceofjawosteonecrosis.
Attentiontoproperadministration,dose,andschedulearecrucialtominimizetheincidenceandseverityoftheadverseeventsofintravenousbisphosphonatesincludingzoledronicacid.

46
References
Atula S, Powles T, Paterson A et al. Extended safety profile of oral clodronate after long-term use in primary breast cancer patients. DrugSaf2003;26:66�-67�.
BerensonJR,HillnerBE,KyleRAetal.AmericanSocietyofClinicalOncologyclinicalpracticeguidelines:theroleofbisphosphonatesinmultiplemyeloma.JClinOncol2002;20:37�9-3736.
BodyJJ,DielIJ,LichinitzerMetal.Oralibandronatereducestheriskofskeletalcomplicationsinbreastcancerpatientswithmetastaticbonedisease:resultsfromtworandomised,placebo-controlledphaseIIIstudies.BrJCancer2004;90:��33-��37.
BodyJJ.Dosingregimensandmainadverseeventsofbisphosphonates.SeminOncol200�;28(suppl��):49–53.
BounameauxHM,SchifferliJ,MontaniJPetal.Renalfailureassociatedwithintravenousdiphosphonates.Lancet�983;�:47�.
CarrollPR,AltweinJ,BrawleyOetal.Managementofdisseminatedprostatecancer.In:DenisL,BartschG,KhourySetal.eds.ProstateCancer:3rdInternationalConsultationonProstateCancer—Paris.Paris:HealthPublications,2003:249-284.
Coleman RE, Purohit OP, Black C et al. Double-blind, randomised, placebo-controlled, dose-finding study of oral ibandronate in patientswithmetastaticbonedisease.AnnOncol�999;�0:3��-3�6.
ColemanRE.Bisphosphonates:clinicalexperience.TheOncologist2004;9(suppl4):�4-27.
Conte PF, Guarneri V. SafetyofIntravenousandOralBisphosphonatesandComplianceWithDosingRegimens.TheOncologist2004;Suppl4:28–37.
CorsoA,ZappasodiP,LazzarinoM.Urinaryproteinsandrenaldysfunctioninpatientswithmultiplemyeloma.BiomedPharmacother2002;56:�39-�43.
EasthamJA.Bisphosphonatesandprostatecancer:maintainingboneintegrityandqualityoflife.AmJUrolRev2004;2(suppl2):5–8.
EzraA,GolombG.Administrationroutesanddeliverysystemsofbisphosphonatesforthetreatmentofboneresorption.AdvDrugDelivRev2000;42:�7-�95.
GreenJR,MüllerK,JaeggiKA.PreclinicalpharmacologyofCGP42’446,anew,potent,heterocyclicbisphosphonatecompound.JBoneMinerRes�994;9:745-75�
HillnerBE,IngleJN,BerensonJRetal.AmericanSocietyofClinicalOncologyguidelineontheroleofbisphosphonatesinbreastcancer.AmericanSocietyofClinicalOncologyBisphosphonatesExpertPanel.JClinOncol2000;�8:�378-�39�.
HillnerBE,IngleJN,ChlebowskiRTetal.AmericanSocietyofClinicalOncology2003updateontheroleofbisphosphonatesandbonehealthissuesinwomenwithbreastcancer.JClinOncol2003;2�:4042-4057.
Hirsh V, Tchekmedyian NS, Rosen L et al. Clinical benefit of zoledronic acid in patients with lung cancer and other solid tumors: analysisbasedonpriorhistoryofskeletalcomplications.ProcAmSocClinOncol2004;23:669.
PatersonAHG,PowlesTJ,KanisJAetal.Double-blindcontrolledtrialoforalclodronateinpatientswithbonemetastasesfrombreastcancer.JClinOncol�993;��:59-65.
PowlesT,PatersonS,KanisJAetal.Randomized,placebo-controlled trialofclodronate inpatientswithprimaryoperablebreastcancer.JClinOncol2002;20:32�9–3224.
Saad F. The role of intravenous bisphosphonates in the management of prostate cancer: treatment guidelines.Am J Urol Rev2004;2(suppl2):9-�5.
TarassoffP,CsermakK.Avascularnecrosisofthejaws:riskfactorsinmetastaticcancerpatients.JOralMaxillofacSurg2003;6�:�238-�239.
WozniakAJ.Lungcancer:principlesandpractice.Managementofbonemetastasesinlungcancer.Updates2004;4:�-�2.
ZojerN,KeckAV,PecherstorferM.Comparativetolerabilityofdrugtherapiesforhypercalcaemiaofmalignancy.DrugSaf�999;2�:389-406.

47
Conclusions
Thismonographhasreviewedtheevidencebaseforzoledronicacidinarangeofindications,ineach of which significant clinical need exists.
In hypercalcemia of malignancy, zoledronic acid is a potent and well-tolerated therapy withefficacy at least equivalent to the previous gold standard, intravenous pamidronate, and with theadditionaladvantageofamorerapid(�5-minute)infusionschedule.Zoledronicacidisthefirst bisphosphonate to demonstrate significant and long-lasting benefit for reducing skeletal complicationsinpatientswithmultiplemyelomaandavarietyofsolidtumors,includingbreast,prostatecancer,lungcancer,andrenalcancers.Uniquely,osteolytic,osteoblastic,andmixedbonelesionsallimprovewithzoledronicacidtherapy.Treatmentwithzoledronicacidpreventsordelaysdebilitatingskeletalcomplications,slowsthedeteriorationinqualityoflife,andshowspotential antitumor efficacy in these patients. In metabolic bone disease, zoledronic acid is widely licensed for the treatment of Paget’s disease of bone and has efficacy in osteoporosis of differentcausesaswellasrheumatoidarthritis.Long-termtreatmentwithzoledronicacidhasbeenshown tobesafeandwell tolerated inclinicalpractice.Adherence to renalmonitoringcontributeseffectivelytorenalsafety.
The consistent efficacy demonstrated for zoledronic acid in large, well-designed trials and in clinical practice suggests that this medication may become first-choice therapy across the range ofindicationsdiscussedinthispublication.