Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2011) 64, 84e90
Flap surgery for pressure sores: Should theunderlying muscle be transferred or not?*
Filip E. Thiessen a,*, Patricio Andrades a,b, Philip N. Blondeel a,Moustapha Hamdi a, Nathalie Roche a, Filip Stillaert a,Koenraad Van Landuyt a, Stan Monstrey a
aDepartment of Plastic Surgery, Gent University Hospital, De Pintelaan 185, B-9000 Gent, BelgiumbDivision of Plastic Surgery, University of Chile Clinical Hospital, Chile
Received 3 October 2009; accepted 18 March 2010
KEYWORDSPressure sores;Perforator flaps;Musculocutaneous flaps;Outcomes
* Presentations: EURAPS 2005, MarseRoyal Belgian Society of Plastic Surge* Corresponding author. Tel.: þ32 9E-mail address: filipthiessen@yaho
1748-6815/$-seefrontmatterª2010Bridoi:10.1016/j.bjps.2010.03.049
Summary Background: Musculocutaneous flaps have become the first choice in the surgicalrepair of pressure sores, but the indication for including muscle in the transferred flaps stillremains poorly defined. This study compares outcomes after muscle and non-muscle flapcoverage of pressure sores to investigate whether it is still necessary to incorporate muscletissue as part of the surgical treatment of these ulcers.Methods: A retrospective revision of 94 consecutive patients with ischial or sacral pressuresores operated between 1996 and 2002 was performed. Depending on the inclusion of muscleinto the flap, the patients were divided in two groups: musculocutaneous flap group and fas-ciocutaneous flap group. Charts were reviewed for patient characteristics, ulcer features andreconstructive information. Data between groups were compared with emphasis on early (hae-matoma or seroma, dehiscence, infections, necrosis and secondary procedures) and late(recurrence) postoperative complications.Results: A total of 37 wounds were covered with muscle and 57 wounds covered withoutmuscle tissue. The groups were comparable in relation to age, gender, ulcer characteristicsand timing for surgery. There were no significant differences in early complications betweenthe study groups. The mean follow-up period was 3.10� 1.8 years (range: 0.5 to 6.7). Therewere no statistical differences in ulcer recurrence between the groups. The type of flap usedwas not associated with postoperative morbidity or recurrence in the univariate and multivar-iate analyses.
ille, France.ry 2007, Leuven, Belgium.3323227.o.com (F.E. Thiessen).
tishAssociationofPlastic,ReconstructiveandAestheticSurgeons.PublishedbyElsevierLtd.All rightsreserved.

Flap surgery for pressure sores 85
Conclusions: The findings of this clinical study indicate that the musculocutaneous flaps are asgood as fasciocutaneous flaps in the reconstruction of pressure sores, and they question thelong-standing dogma that muscle is needed in the repair of these ulcers.ª 2010 British Association of Plastic, Reconstructive and Aesthetic Surgeons. Published byElsevier Ltd. All rights reserved.
Pressure sores are a challenge for the medical and nursingstaff because they are averse to healing, difficult to closeby surgery, have a tendency to recur and are extremelycostly to treat.1 It is accepted that invasive type 3 or 4pressure sores are best treated with surgery becauseconservative non-surgical treatment is protracted andfrequently culminates in either a non-healing wound orearly recurrence.2e4 Pressure sore surgery has a high earlysuccess rate with acceptable number of complications, butthe long-term results are variable and disappointing.Recurrence rates as low as 3e6%5e7 and as high as33e100%8e11 have been reported. This variability may beexplained by many factors, including the location of theulcer, level of spinal cord injury, history of prior ulceration,ambulatory status, daily habits, educational status, moti-vational level and associated medical problems. Anotherimportant factor is the type of flap used for reconstruction,but in the literature there are just a few studies comparingthe long-term outcomes of different surgical techniques.12
This issue is very important because flap selection may becrucial in achieving adequate and enduring wound healingwhile preserving as many future flap options as possible.
The accepted surgical treatment of pressures soresconsists of adequate debridement of the wound, includingthe affected bone, followed by tissue transfer to provideadequate dead space filling and healthy skin coverage.4,13,14
Over the past decennia, musculocutaneous flaps havebecome the first choice in the surgical repair of pressureulcers but the indications for including muscle in the trans-ferred flaps still remain poorly defined.2 The theoreticaladvantages of using muscle in the repair of pressure soresinclude (1) bulk to eliminate dead space, (2) a carrier forreliable blood supply to overlying soft tissue, (3) a mass ofcushioning tissue over a pressure-bearing area that will serveto distribute pressure and (4) superiority in infection controland eradication. Although the reported surgical resultsappear to be improved by using musculocutaneous flaps, ithas been shown that the transferred muscle becomes atro-phic, loses its dynamic function and overtime no longerfunctions as a cushion to absorb pressure.15 For these reasonsthe purpose of this study is to investigate whether it is stillnecessary to use muscle tissue in covering pressure sores byevaluating the difference in early and late complicationsafter coverage of pressure sores with a fasciocutaneous orperforator flap versus a musculocutaneous flap.
Materials and method
Patient and setting
A retrospective clinical study was performed including allconsecutive patients with sacral and ischial type 4 pressuresores who underwent a flap transfer between January 1996
and March 2002. All patients were operated at theDepartment of Plastic Surgery, Gent University Hospital.Four fully trained plastic surgeons, staff members at ourdivision and with a broad experience in muscle and non-muscle pressure sore reconstruction participated in thestudy. Flap selection (i.e., musculocutaneous, fasciocuta-neous or perforator flap) was based on the surgeons’ pref-erences after analysing each individual case. Trochantericulcers were excluded from the study because there wereonly six cases during the study period treated with just onesurgical modality.
Surgical technique
After adequatewound-bed preparation, infection control andimprovement of nutritional parameters, the surgery wasscheduled. The patients were placed in a prone position forthe operation after receiving general or regional anaesthesia.A tumescent solution containing epinephrine 1:200.000 wasused, and the pressure-sore margins and bursa were markedwithmethyleneblue.Thebasicprinciples for surgical repairofpressure sores were strictly followed in all cases. First, theulcer was excised, including the surrounding scar, underlyingbursa and soft tissue calcification, if any. Then a radicalremoval of the underlying bone and any heterotopic ossifica-tion padding of bone stumps was performed. Finally, theresultingdefectwascoveredbyaflap,and suctiondrainswereused. Depending on the inclusion of muscle into the flap, thepatients were divided in two groups: group 1 where a muscu-locutaneous flap was used for coverage; and group 2, wherefasciocutaneous or perforator flaps were used.
Outcome measures
During the follow-up period, data on the patients werecollected by retrospective chart review, patient interviewand physical examination. All patients were seen by anindependent observer for follow-up at the outpatient clinicor personally interviewed by telephone before they wereincluded in the study. Clinical charts were revised for thefollowing variables:
e Patient variables: gender, age, past medical history (e.g.,severe cardiovascular, respiratory or other organdysfunction that has required prolonged hospitalisationand/or medical treatment), spinal cord injury (para-lytics and non-paralytics) and hospitalisation (comingfrom home to solve the pressure sore or develop thepressure sore in the hospital).
e Pressure sore variables: location (ischial or sacral), type(type 1, 2, 3 or 4), chronic (developed recently or morethan 3 months), primary or recurrent, preoperativeswap cultures and use of antibiotics.

86 F.E. Thiessen et al.
e Surgical variables: type of flap (musculocutaneous orfasciocutaneous), number and days of drains andhospital stay. Despite our efforts, it was impossible toobtain reliable data about operative times.
e Outcome parameters included early postoperativecomplications (i.e., haematoma or seroma, dehiscence,infections, flap necrosis and secondary procedures) andlate postoperative complications (ulcer recurrence atthe site of a previously operated pressure sore).
Statistics
Continuous variables are described as mean and standarddeviation, and categorical variables as percentages. Formusculocutaneous and fasciocutaneous group comparisons,a Fisher’s exact test was used for categorical variables anda Mann-Whitney U test for continuous variables. A univar-iate analysis of the relationship among postoperativemorbidity, recurrence and the prognostic variables wasperformed using the chi-squared or Fisher’s exact test whenthe sample was small (n< 5) and a T or Mann-Whitney Utest depending on data distribution. For the multivariateanalysis, a logistic regression model was used to explore theprognostic role of the variables considered to have clinicalrelevance and to estimate the odds ratio for the occurrenceof postoperative morbidity and ulcer recurrence. A two-tailed p-value <0.05 was considered statistically signifi-cant and all confidence intervals are reported in the 95%range. All calculations were performed using SPSS forWindows, Version 14.0 (Chicago, IL, USA).
Results
A total of 94 patients with sacral or ischial pressure soreswere included in the study. There were 28 females and 66males, with a mean age of 45.99� 17.9 years, ranging from12 to 82. The average follow-up period was 3.10� 1.8years, ranging from 0.5 to 6.7. Comparison between mus-culocutaneous or fasciocutaneous groups is shown in Table1. Out of the 94 ulcers, 57 (61%) were repaired using a fas-ciocutaneous or perforator flaps, and 37 (39%) using a mus-culocutaneous flap. In the treatment of ischial sores, 21were reconstructed with fasciocutaneous (18 posteriorthigh flaps and three fasciocutaneous rotation flaps) and 17with musculocutaneous flaps (14 gluteus maximus muscleflaps and three hamstring flaps). In the treatment of sacralsores, 36 were reconstructed with fasciocutaneous flaps (31Superior Gluteal Artery Perforator flap (SGAP), five fas-ciocutaneous rotation flaps) and 20 with musculocutaneousflaps of the gluteus maximus muscle. The groups werecomparable in relation to patient, pressure sore andsurgical variables. During the study period, there was nostatistical relationship or pattern on the frequencies themusculocutaneous and fasciocutaneous flaps were per-formed (Table 2). Although there was a tendency for morenon-paralytics, chronic ulcers, shorter hospital stay andlonger time between surgery and recurrence in the fas-ciocutaneous group, none of these differences was statis-tically significant. Furthermore, we found no significantdifferences in early complications between the studied
groups in relation to wound dehiscence, infection, hae-matoma, seroma, flap necrosis and the need for secondaryprocedures. Moreover, there was no statistical difference inrecurrence rate between the musculocutaneous and fas-ciocutaneous groups (32% vs. 26%, respectively, pZ 0.648).
The univariate relationship between postoperativemorbidity and recurrence with the prognostic factors can beseen in Table 3. Patients who develop their pressure sores inthe hospital (pZ 0.005), and those with an ulcer with lessthan 3 months (pZ 0.003) had significantly more post-operative complications. Wound dehiscence (pZ 0.0001),infection (pZ 0.0001), haematoma and seroma (pZ 0.050)were the complications that more strongly influenced post-operative morbidity outcome. In addition, longer hospitalstay (pZ 0.001) and shorter time between surgery andrecurrence (pZ 0.018) were observed in the group ofpatients with higher postoperative morbidity. Recurrencewas associated with ischial pressure sore localisation(pZ 0.013), recurrent ulcer (pZ 0.050), longer use of drains(pZ 0.034) and dehiscence (pZ 0.002).
The estimation of postoperative morbidity risk andrecurrence risk according to clinically important variablesin a multivariate analysis is shown in Tables 4 and 5. Theonly two variables associated with postoperative morbiditywere ulcer aetiology and hospitalisation. Not surprising wasthe fact that a non-paralytic patient (odds ratio (OR)Z 0.081, 95% confidence interval (CI)Z 0.009e0.706,pZ 0.023) and ulcer development in a non-hospitalisedsetting (ORZ 0.108, 95% CIZ 0.0021e0.563, pZ 0.008)were protective factors for complications. The type of flapused had no influence on the incidence of postoperativemorbidity. Analysing subgroups of postoperative morbidity,a positive preoperative culture was a favouring factor fordehiscence (ORZ 5.897, 95% CIZ 1.664e20.899,pZ 0.006); the use of preoperative antibiotics(ORZ 19.173, 95% CIZ 1.784e206.096, pZ 0.015) anda positive preoperative cultures (ORZ 5.897, 95%CIZ 1.664e20.899, pZ 0.006) were favouring factors forinfection. No favouring or protective factors were identi-fied for seroma, haematoma and flap necrosis. Finally, theonly two variables associated with recurrence were ulcerlocation and dehiscence. A sacral pressure sore wasa protective factor (ORZ 0.386, 95% CIZ 0.166e0.898,pZ 0.027) and the development of immediate post-operative wound dehiscence was a favouring factor(ORZ 3.885, 95% CIZ 1.477e10.216, pZ 0.006) for pres-sure sore recurrence. The type of flap used did not have anyeffect on the recurrence rate in the multivariate analysis.
Discussion
There are several important disadvantages of a retrospectivecase series study as the one presented here.16 First, as withany retrospective study, the investigator depends on theavailability and accuracy of the medical record. Second,a case series is subject to selection bias because the inves-tigator self-selects the cases. Third, a case series is non-randomised, allowing for confounding variables to influ-ence the results and increase the probability of a type Istatistical error (e.g., alpha error, or false positive, orrejecting the null hypothesis when it is true). In our study,we

Table 1 Patient, ulcer, surgery and outcome characteristics by group
Musculocutaneous(nZ 37)
Fasciocutaneous(nZ 57)
Total(nZ 94)
P value*
Patient variablesAge 46.16� 19.1 45.74� 16.3 45.99� 17.9 0.910Gender (male/female) 28 (76%)/9 (24%) 35 (65%)/19 (35%) 66 (70%)/28 (30%) 0.260PMH 23 (61%) 32 (56%) 55 (58%) 0.832Etiology (paralytics/non-paralytics) 32 (87%)/5 (13%) 40 (70%)/17 (30%) 72 (77%)/22 (23%) 0.082Non-hospitalised patient 20 (53%) 21 (37%) 41 (43%) 0.144
Pressure sore variablesLocalisation (% ischial/sacral) 17 (45%)/20 (55%) 21 (37%)/36 (64%) 38 (40%)/56 (60%) 0.319Type IV ulcer 100% 100% 100% 1.000Chronic (>3 months) 22 (39%) 23 (61%) 45 (47%) 0.058Recurrent ulcer 10 (29%)/24 (71%) 15 (29%)/37 (71%) 25 (29%)/61 (71%) 1.000Preoperative positive cultures 17 (45%)/20 (55%) 12 (21%)/45 (79%) 29 (31%)/65 (69%) 0.192Preoperative antibiotics 39 (71%) 24 (65%) 63 (69%) 0.648
Surgical variablesFlap 37 57 94 NA
Gluteus maximum 34 (92%) 0 32 (34%)Hamstring 3 (8%) 0 3 (4%)Posterior thigh 0 18 (32%) 18 (19%)SGAP 0 31 (54%) 31 (33%)Local fasciocutaneous 0 8 (14%) 8 (10%)
Number of drains (1 or 2 drains) 22 (59%) 36 (63%) 59 (63%) 0.678Days of drains 10.78� 4.3 11.72� 6.8 11.19� 5.5 0.555Hospital stay 75.45� 52.2 64.76� 75.5 70.98� 62.8 0.059
OutcomesPostoperative morbidity 21 (56%) 39 (67%) 60 (63%) 0.202
Dehiscence 18 (47%) 25 (44%) 43 (46%) 0.835Infection 13 (35%) 27 (51%) 40 (45%) 0.135Hematoma or seroma 8 (22%) 15 (27%) 23 (25%) 0.628Flap necrosis 3 (8%) 6 (11%) 9 (10%) 0.735Need for secondary procedure 13 (34%) 22 (39%) 35 (37%) 0.668
Recurrence 12 (32%) 15 (26%) 27 (29%) 0.648Time between surgery and recurrence(months)
8.85� 6.4 16.73� 15.2 13.22� 12.6 0.261
Follow-upYears of follow-up 3.01� 1.9 3.22� 1.5 3.10� 1.8 0.671
*: For statistical analysis Fisher exact test was used for comparing proportions and Mann-Whitney test for means.PMH: Past medical history; NA: Not applicable.
Flap surgery for pressure sores 87
made our best effort to reduce all these problems. First, weincluded consecutive patients with sacral or ischial pressuresores. We excluded trochanteric ulcers because there werejust a few cases during the study period treatedwith just one
Table 2 Musculocutaneous and fasciocutaneous flaps performe
Year Fasciocutaneous
1996 101997 91998 91999 52000 82001 102002 6
Total 57
modality and were not suitable for the analysis. Second,independent observers tracked all the patients in the clinicor by telephone obtaining a 100% follow-up with an averageof 3.10� 1.8 years, ranging from 0.5 to 6.7. Third, the two
d during the study period
Musculocutaneous Relation F:M
4 2.53 3.0
10 0.96 0.89 0.93 3.32 3.0
37 1.5
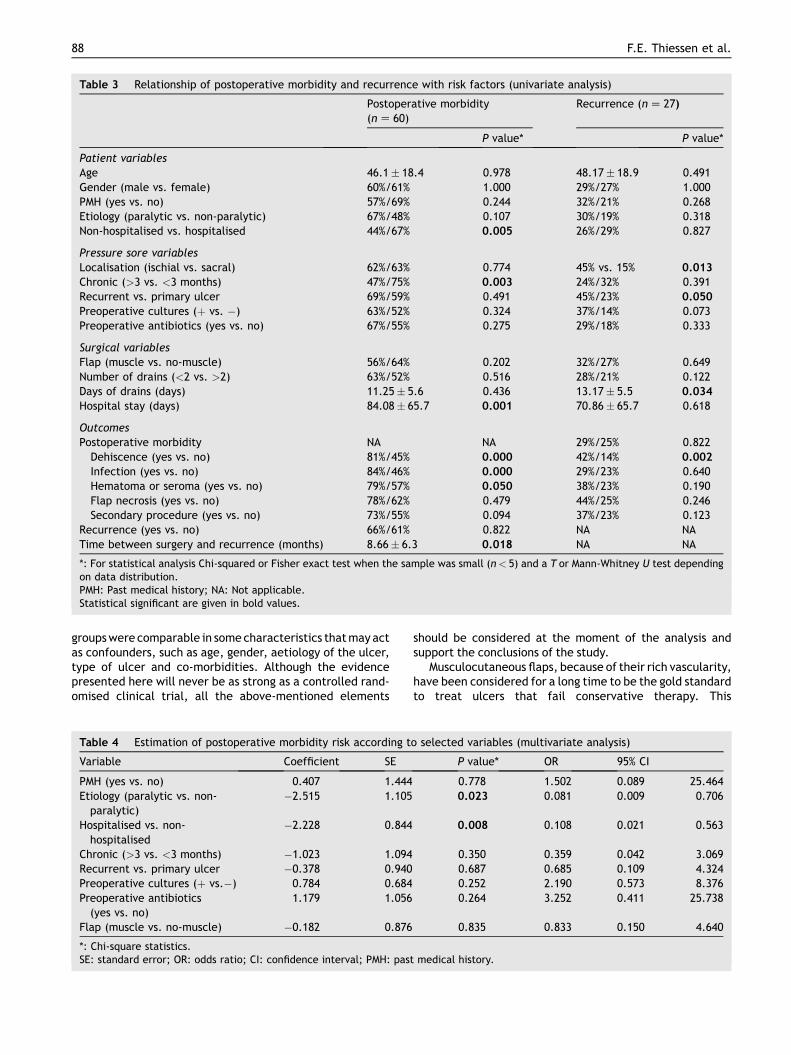
Table 3 Relationship of postoperative morbidity and recurrence with risk factors (univariate analysis)
Postoperative morbidity(nZ 60)
Recurrence (nZ 27)
P value* P value*
Patient variablesAge 46.1� 18.4 0.978 48.17� 18.9 0.491Gender (male vs. female) 60%/61% 1.000 29%/27% 1.000PMH (yes vs. no) 57%/69% 0.244 32%/21% 0.268Etiology (paralytic vs. non-paralytic) 67%/48% 0.107 30%/19% 0.318Non-hospitalised vs. hospitalised 44%/67% 0.005 26%/29% 0.827
Pressure sore variablesLocalisation (ischial vs. sacral) 62%/63% 0.774 45% vs. 15% 0.013
Chronic (>3 vs. <3 months) 47%/75% 0.003 24%/32% 0.391Recurrent vs. primary ulcer 69%/59% 0.491 45%/23% 0.050
Preoperative cultures (þ vs. �) 63%/52% 0.324 37%/14% 0.073Preoperative antibiotics (yes vs. no) 67%/55% 0.275 29%/18% 0.333
Surgical variablesFlap (muscle vs. no-muscle) 56%/64% 0.202 32%/27% 0.649Number of drains (<2 vs. >2) 63%/52% 0.516 28%/21% 0.122Days of drains (days) 11.25� 5.6 0.436 13.17� 5.5 0.034
Hospital stay (days) 84.08� 65.7 0.001 70.86� 65.7 0.618
OutcomesPostoperative morbidity NA NA 29%/25% 0.822Dehiscence (yes vs. no) 81%/45% 0.000 42%/14% 0.002
Infection (yes vs. no) 84%/46% 0.000 29%/23% 0.640Hematoma or seroma (yes vs. no) 79%/57% 0.050 38%/23% 0.190Flap necrosis (yes vs. no) 78%/62% 0.479 44%/25% 0.246Secondary procedure (yes vs. no) 73%/55% 0.094 37%/23% 0.123
Recurrence (yes vs. no) 66%/61% 0.822 NA NATime between surgery and recurrence (months) 8.66� 6.3 0.018 NA NA
*: For statistical analysis Chi-squared or Fisher exact test when the sample was small (n< 5) and a T or Mann-Whitney U test dependingon data distribution.PMH: Past medical history; NA: Not applicable.Statistical significant are given in bold values.
88 F.E. Thiessen et al.
groupswerecomparable in somecharacteristics thatmayactas confounders, such as age, gender, aetiology of the ulcer,type of ulcer and co-morbidities. Although the evidencepresented here will never be as strong as a controlled rand-omised clinical trial, all the above-mentioned elements
Table 4 Estimation of postoperative morbidity risk according t
Variable Coefficient SE
PMH (yes vs. no) 0.407 1.444Etiology (paralytic vs. non-paralytic)
�2.515 1.105
Hospitalised vs. non-hospitalised
�2.228 0.844
Chronic (>3 vs. <3 months) �1.023 1.094Recurrent vs. primary ulcer �0.378 0.940Preoperative cultures (þ vs.�) 0.784 0.684Preoperative antibiotics(yes vs. no)
1.179 1.056
Flap (muscle vs. no-muscle) �0.182 0.876
*: Chi-square statistics.SE: standard error; OR: odds ratio; CI: confidence interval; PMH: pas
should be considered at the moment of the analysis andsupport the conclusions of the study.
Musculocutaneous flaps, because of their rich vascularity,have been considered for a long time to be the gold standardto treat ulcers that fail conservative therapy. This
o selected variables (multivariate analysis)
P value* OR 95% CI
0.778 1.502 0.089 25.4640.023 0.081 0.009 0.706
0.008 0.108 0.021 0.563
0.350 0.359 0.042 3.0690.687 0.685 0.109 4.3240.252 2.190 0.573 8.3760.264 3.252 0.411 25.738
0.835 0.833 0.150 4.640
t medical history.

Table 5 Estimation of recurrence risk according to selected variables (multivariate analysis)
Variable Coefficient SE P value* OR 95% CI
PMH (yes vs. no) �7.179 4.245 0.091 0.001 0.000 3.132Etiology (paralytic vs. non-paralytic)
�0.194 3.534 0.956 0.824 0.001 839.87
Localisation (ischial vs. sacral) �0953 0.431 0.027 0.386 0.166 0.898Recurrent vs. primary ulcer 1.486 2.741 0.588 4.419 0.021 952.11Flap (muscle vs. no-muscle) 0.864 1.820 0.635 2.373 0.067 84.028Days of drains (<10 vs.>10 days)
1.391 2.047 0.497 4.017 0.073 222.15
Dehiscence (no vs. yes) 1.357 0.493 0.006 3.885 1.477 10.216Hematoma or seroma(no vs. yes)
5.452 3.035 0.072 233.27 0.609 89376.7
Infection (no vs. yes) �3.810 3.394 0.262 0.222 0.000 17.153Flap necrosis (no vs. yes) 0.728 0.782 0.352 2.070 0.447 9.588Secondary procedure(no vs. yes)
�0.427 0.602 0.478 0.652 0.200 2.122
*: Chi-square statistics.SE: standard error; OR: odds ratio; CI: confidence interval; PMH: past medical history.
Flap surgery for pressure sores 89
assumption was challenged by Kroll and Rosenfield,17 whostated that the greater reliability of the musculocutaneousflap comes from the improved blood supply and not from anyintrinsic qualities of the muscle itself. So if a way could befound to give a skin flap the improved blood supply charac-teristics of amusculocutaneous flap, one could have the bestof both worlds. In the 1980s, it became apparent that fas-ciocutaneous flaps were also appropriate to cover pressuresore defects especially over pressure-bearing areas.15 Duringthe past years, with the advent of perforator flaps, it hasbeen possible to isolate a skin paddle on one or more perfo-rating blood vessels only. Kroll17 published for thefirst time in1988 the use of perforator flaps for coverage of low midlinedefects, and Koshima et al.18 confirmed the reliability of theblood supply and the advantages of this flap based on thedetailed anatomy of the dissected cadaver. The use of mus-culocutaneous, fasciocutaneous and perforator flaps tocover pressure sores iswell suited to the surgical principles ofthe treatment of these ulcers, namely they both provideenough tissue to cover dead space, they are both well vas-cularised and they generally allow tension-free closure.However, there is still no unanimity about the necessity ofincluding muscle tissue in the flap.
In our study, we found no differences between muscu-locutaneous and fasciocutaneous flaps in relation to infec-tion, haematoma, seroma, dehiscence and the need forsecondary procedures. Although some experimental reportshave shown the advantage of using muscle flaps over fas-ciocutaneous flaps in the treatment of infectedwounds,19e21 we could not find a clinical significantdifference in the risk to develop postoperative infectionsbetween the two groups. This discrepancy could beexplained by the lack of an adequate model in the experi-mental studies where a much vascularised muscle wascompared with a borderline vascularised fasciocutaneousflap. The observations in our study are supported by recentpublications comparing these flaps in pressure sores15,22
and lower extremity defects23 that have shown no differ-ences between musculocutaneous and fasciocutaneousflaps. As for the late postoperative complications, our
results compare favourably with the recurrence rate ofother studies.9,11,24,25 We also found no statistical differ-ence in the recurrence rate between the musculocutaneousand fasciocutaneous flaps. Moreover, the type of flap wasnot associated with postoperative morbidity and ulcerrecurrence in the univariate and in the multivariate anal-ysis. In concordance with other studies,10,26,27 patients whohad fasciocutaneous flaps did not seem to be at greater riskof wound breakdown or flap failure than musculocutaneousflaps. Unfortunately, some variables such as operatingtime, surgical simplicity and surgeons’ preferences werenot evaluated. The surgeon may choose the faster andeasier surgical technique but the findings in our studycorroborate the fact that pressure sore surgery outcomesare dependent on a multitude of factors other than flapselection alone. Larger and prospective cohort studies willbe needed to determine the real importance of thisphenomenon.
In addition to the clinical results of this study, webelieve there are additional theoretical reasons why theinclusion of muscle tissue is not necessary in the surgicalmanagement of pressure sores. First, covering pressuresores by muscle is contradictory to normal anatomy. Danieland Faibisoff28 investigated the normal soft tissue coverageof pressure points in autopsy specimens. They observedthat all pressure points in the human body are covered byskin and subcutaneous tissue and not by muscle. Second,the use of muscle tissue is not a panacea in coveringpressure sores. Muscle tissue is less tolerant to ischaemiathan skin tissue. Experimentally, it has been demonstratedthat applying pressure over musculocutaneous flapsgenerates hypoxia in the tissue, which results in musclenecrosis without skin necrosis.29 The pressure-spreadingfunction of muscle flaps disappears early after surgerybecause the muscle portion in the transferred flaps showsa remarkable atrophic change. Ultimately, skin, subcuta-neous tissue and fascia are the only elements that staycovering the defect over time. Third, reduction of donor-site morbidity, preservation of muscle integrity andmuscle function are among of the greatest assets of

90 F.E. Thiessen et al.
fasciocutaneous flaps, especially of perforator flaps.30e34 Innon-paralysed patients it is very important to save themuscle function for the recovery of ambulation. In para-lysed patients, pressure ulcers are subject to recurrenceand often need repeated reconstruction, and by usingmuscle tissue as a first-line reconstruction we diminishfuture reconstructive possibilities with fasciocutaneousflaps. Fourth, fasciocutaneous flaps have good bloodsupply, tolerance to infection and coverage capabilitiessimilar to musculocutaneous flaps. Muscle is not necessaryto supply blood to the overlying soft tissue because axial- orperforator-based fasciocutaneous flaps have an adequatevascularity without a muscle.35 Only extremely largedefects justify the use of muscle, but usually a fasciocuta-neous flap is sufficient to cover the average size lesions. Inaccordance with the results of the present study, wesuggest that there are theoretical reasons to support thefact that fasciocutaneous flaps are a good alternative in thereconstruction of pressure sores.
Flap selection plays an important role in pressure sorereconstruction. The findings of this clinical study indicatethat the musculocutaneous flaps are not superior to fas-ciocutaneous flaps in the reconstruction of pressure sores.These results question the long-standing dogma that muscleis needed in the repair of these ulcers. Flap selectionshould be made on the basis of the quality of tissue to betransferred instead of the quantity. The three-dimensionalanalyses of the defect and the geometrical flap optionsshould help us find a solution that achieves adequate andlong-lasting wound control, while preserving as many futuretherapeutic options as possible.
Disclosure
The authors declare they have nothing to disclose.
References
1. Thoroddsen A. Pressure sore prevalence: a National survey. JClin Nurs 1999;8:170e9.
2. Janis JE, Kenkel JM. Pressure sores. Selected Readings PlastSurg 2003;9:1e42.
3. Bauer J, Phillips LG. MOC-PSSM CME article: pressure sores.Plast Reconstr Surg 2008;121:1e10.
4. Colen SR. Pressure sores. In: McCarthy JG, editor. PlasticSurgery. Philadelphia: Saunders; 1990. p. 3797e838.
5. Ger R, Levine SA. The management of decubitus ulcers bymuscle transposition. An 8-year review. Plast Reconstr Surg1976;58:419e28.
6. Hentz VR. Management of pressure sores in a specialty center.A reappraisal. Plast Reconstr Surg 1979;64:683e91.
7. Stevenson TR, Pollock RA, Rohrich RJ, et al. The gluteusmaximus musculocutaneous island flap: refinements in designand application. Plast Reconstr Surg 1987;79:761e8.
8. MinamiRT,MillsR,PardoeR.Gluteusmaximusmyocutaneousflapsfor repair of pressure sores. Plast Reconstr Surg 1977;60:242e9.
9. Relander M, Palmer B. Recurrence of surgically treated pressuresores. Scand J Plast Reconstr Surg Hand Surg 1988;22:89e92.
10. Yamamoto Y, Tsutsumida A, Murazumi M, et al. Long-termoutcome of pressure sores treated with flap coverage. PlastReconstr Surg 1997;100:1212e7.
11. Disa JJ, Carlton JM, Goldberg NH. Efficacy of operative cure inpressure sore patients. Plast Reconstr Surg 1992;89:272e8.
12. Foster RD, Anthony JP, Mathes SJ, et al. Flap selection asa determinant of success in pressure sore coverage. Arch Surg1997;132:868e73.
13. Dansereau JG, Conway H. Closure of decubiti in paraplegics.Report of 2000 cases. Plast Reconstr Surg 1964;33:474e80.
14. Griffith BH, Schultz RC. The prevention and surgical treatmentof recurrent decubitus ulcers in patients with paraplegia. PlastReconstr Surg Transplant Bull 1961;27:248e60.
15. Yamamoto Y, Ohura T, Shintomi Y, et al. Superiority of thefasciocutaneous flap in reconstruction of sacral pressure sores.Ann Plast Surg 1993;30:116e21.
16. Guyatt G, Rennie D, Meade M, et al. Users’ Guides to theMedical Literature: a Manual for Evidence-based ClinicalPractice. 2nd ed. USA: McGraw-Hill; 2008.
17. Kroll SS, Rosenfield L. Perforator-based flaps for low posteriormidline defects. Plast Reconstr Surg 1988;81:561e6.
18. Koshima I, Moriguchi T, Soeda S, et al. The gluteal perforator-based flap for repair of sacral pressure sores. Plast ReconstrSurg 1993;91:678e83.
19. Calderon W, Chang N, Mathes SJ. Comparison of the effect ofbacterial inoculation in musculocutaneous and fasciocuta-neous flaps. Plast Reconstr Surg 1986;77:785e94.
20. Chang N, Mathes SJ. Comparison of the effect of bacterialinoculation in musculocutaneous and random-pattern flaps.Plast Reconstr Surg 1982;70:1e10.
21. Mathes SJ, Alpert BS, Chang N. Use of the muscle flap inchronic osteomyelitis: experimental and clinical correlation.Plast Reconstr Surg 1982;69:815e29.
22. Wong TC, Ip FK. Comparison of gluteal fasciocutaneous rota-tional flaps and myocutaneous flaps for the treatment of sacralsores. Int Orthop 2006;30:64e7.
23. Yazar S, Lin CH, Lin YT, et al. Outcome comparison betweenfree muscle and free fasciocutaneous flaps for reconstructionof distal third and ankle traumatic open tibial fractures. PlastReconstr Surg 2006;117:2468e75.
24. Kierney PC, Engrav LH, Isik FF, et al. Results of 268 pressuresores in 158 patients managed jointly by plastic surgery andrehabilitation medicine. Plast Reconstr Surg 1998;102:765e72.
25. Goodman CM, Cohen V, Armenta A, et al. Evaluation of resultsand treatment variables for pressure ulcers in 48 veteran spinalcord-injured patients. Ann Plast Surg 1999;42:665e72.
26. Ohjimi H, Ogata K, Setsu Y, et al. Modification of the gluteusmaximus V-Y advancement flap for sacral ulcers: the gluteal fas-ciocutaneousflapmethod.PlastReconstrSurg1996;100:1247e52.
27. Park C, Park BY. Fasciocutaneous V-Y advancement flap forrepair of sacral defects. Ann Plast Surg 1988;21:23e6.
28. Daniel RK, Faibisoff B. Muscle coverage of pressure pointsetherole of myocutaneous flaps. Ann Plast Surg 1982;8:446e52.
29. Nola GT, Vistnes LM. Differential response of skin and muscle inthe experimental production of pressure sores. Plast ReconstrSurg 1980;66:728e33.
30. Aydin G, Zekeriya K, Zafer O. Long-term outcome with theadductor perforator flap for ischial pressure sores. PlastReconstr Surg 2008;122:49ee50e.
31. Kim YS, Lew DH, Roh TS, et al. Inferior gluteal artery perfo-rator flap: a viable alternative for ischial pressure sores. J PlastReconstr Aesthet Surg; 2008.
32. Prado A, Ocampo C, Danilla S, et al. A new technique of“double-A” bilateral flaps based on perforators for the treat-ment of sacral defects. Plast Reconstr Surg 2007;119:1481e90.
33. Seyhan T, Ertas NM, Bahar T, et al. Simplified and versatile useof gluteal perforator flaps for pressure sores. Ann Plast Surg2008;60:673e8.
34. Verpaele AM, Blondeel PN, Van Landuyt K, et al. The superiorgluteal artery perforator flap: an additional tool in the treat-ment of sacral pressure sores. Br J Plast Surg 1999;52:385e91.
35. Hallock GG. In an era of perforator flaps, are muscle flapspasse? Plast Reconstr Surg 2009;123:1357e63.