Embed Size (px)
Citation preview

First dorsal metacarpal artery flap cover for extensive pulp defects in the normal length thumb
SUMMARY. Use of the first dorsal metacarpal artery flap to cover extensive pulp defects in the normal length thumb in five patients is described. The advantages of the procedure include provision of sensate cover of exposed distal phalanx to the tip of the thumb with minimal donor site morbidity. Its use, particularly in the older patient, with immediate postoperative mobilisation and the avoidance of nerve repair or more complicated microsurgical procedures, is discussed.
Traumatic loss of pulp from the thumb presents a challenging problem to the reconstructive surgeon. Local Ilap coverage is particularly difficult when thumb length is preserved but pulp loss is extensive. exposing structures in the distal thumb. In 1979 Foucher and Braun described a neurovascular island flap based on the first dorsal metacarpal artery (DMCA). This was used to transfer skin from the dorsum of the index finger to resurface dorsal thumb defects or the stumps of shortened thumbs, but they did not comment on its use for pulp loss in the normal length thumb. This paper reports five cases of extensive pulp loss extending to the tip of normal length thumbs that were resurfaced using the first DMCA flap in a single stage procedure.
Patients and operative technique
The details of the patients undergoing first DMCA flap thumb reconstruction are shown in Table I. Their ages ranged from 34-64 years (mean 55.4 years). All were male manual workers and all were injured at work. First DMCA flap reconstruction was chosen after full discussion with the patient of the techniques available to reconstruct the injured thumb.
The thumb pulp defects varied in size. In all five patients the defect extended longitudinally from the volar aspect of the interphalangeal joint to the thumb tip. Transversely the defects varied from the whole width of the thumb pulp to a missing linear segment of thumb pulp tissue with exposed bone.
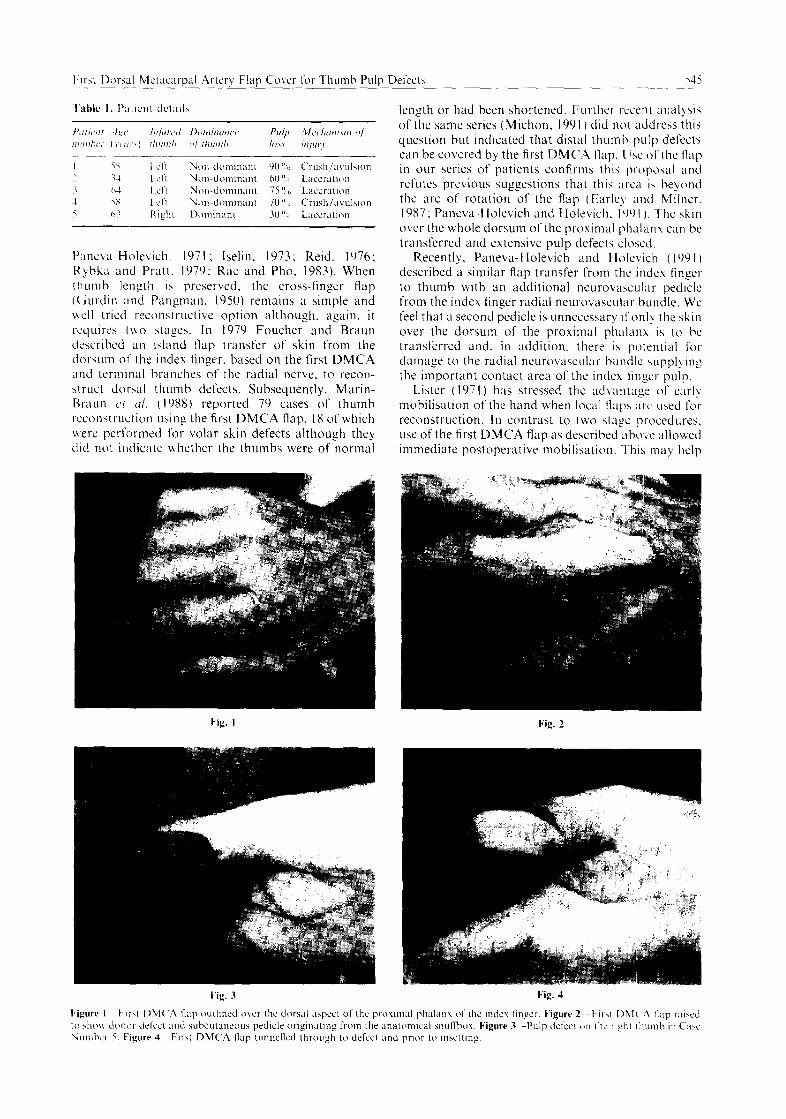
An identical technique was used in all cases to raise the first DMCA flap from the dorsal surface of the proximal phalanx of the index finger. The margins of the flap are outlined laterally to run along the mid- lateral lines of the finger. Proximally and distally the flap margins are outlined to preserve the dorsal skin of the metacarpophalangeal joint and proximal inter- phalangeal joint respectively (Fig. 1). Elevation of the flap commences distally and laterally, preserving the paratenon over the extensor apparatus. Proximally the skin overlying the first web space is raised subdermally.
Following this. a pedicle of subcutaneous tissue is developed raising the fascia over the first dorsal interosseus muscle to ensure inclusion of the first DMCA or smaller axial fascial branches (Earley, 1986: Earley and Milner, 1987). Several subcutaneous veins and one or more terminal branches of the radial nerve are included in the pedicle which is raised towards the origin of the first DMCA. distal to the tendon of extensor pollicis longus at the ulnar aspect of the anatomical snufIbox (Fig. 2). Any small arterial branches penetrating the aponeurosis of the first dorsal interosseous muscle must be carefully ligated or coagulated. By doing so. the maximum potential length of the flap pedicle is achieved. thus allowing it to reach the thumb tip. A subcutaneous tunnel is then developed along the ulnar aspect of the thumb from the snuffbox to the proximal margin of the pulp defect. A single skin hook is passed through the tunnel from distal to proximal and the first DMCA flap is then transferred easily by gentle traction into the thumb pulp defect (Figs 3, 4). The first DMCA flap is then tailored to close the surgically debrided thumb pulp defect. The donor defect on the index finger is closed with a full thickness skin graft.
All our patients were encouraged to mobilise the reconstructed thumb and donor index finger from the first postoperative day. In all patients flap survival was 100% and graft survival at the donor site was complete (Fig. 5). All flaps were sensate, the sensation being perceived as originating from the dorsum of the index finger.
Discussion
Use of the dorsal skin of the index finger to provide sensate skin cover in thumb injuries has been described by several authors. Many of these techniques have been two stage procedures (Adamson et ~1.. 1967; Bralliar and Horner, 1969: Gaul, 1969; St&r and Radivojevic, 1985) or have only been applicable to shortened thumbs (Holevitch. 1964; Holevich and
PLlnc\;a-Holelich. 1971 ; Iselin. 1973; Reid, 1976; Ryhka and Pratt. 1979: Rae and Pho, 1983). When thumb length is prcser\ed, the cross-finger flap (Gurdin and Pangman. i93.I) remains a simple and h\ell tried reconstructive option although, again. it requires two stages. In 1979 Foucher and Braun described an i4and Hap transfer of skin from the dor\um 0.1‘ the index finger. based on the first DMCA and terminal branches of the radial nerve. to recon- struct doraI thumb defects. Subsequently. Marin- Braun c’t (11. ( 198X) reported 79 cases of thumb rcconhtruction using the first DMCA flap. IX of which were performed for volar skin defects although they did not indicate whether the thumbs were of normal
length or had been shortened. Further recent analysis of the same series (Michon. 1991 ) did not address this question but indicated that distal thumb p~llp defects can be covered by the first DMC.A tlap. li\c of the Ilap
in our series of patients confirms thi\ proposal irnd refutes previous suggestions that this area i4 bevond the arc of rotation of the flap (Earley and Milner. 1987; Paneva-Holevich and Holevich. 194 I ). T~he skin over the whole dorsum of the proximal phalanx c;m be transferred and extensive pulp defects closed.
Recently. Paneva-Holevich and Holevich ( 199 I ) described :I similar flap transfer from the indcs finger to thumb with an additional neurovaaJ;lr pediclc from the index finger radial neurovascular bundle. WC feel that a second pedicle is unnecessary ifonlb, the skin over the dorsum of the proximal phalanx is to be transferred and. in addition. there ih potential fol damage to the radial neurovascular hundlc ~,uppl! ing the important conlact area of the index finger pulp.
Lister (1971) has stressed the ad\,antag: of earlv mobilisation of the hand when local Ilap ;irc’ used for reconstruction. In contrast to two atage procedures. use of the first DMCA Rap as described alxwc allowed immediate postoperative mobilisation. This, may help
Fig. 2
Fig. 3 Fig. 4

546 British Journal of Plastic Surgery
Fig. 5
Figure S-Earl) result in Case Number 3 showing complete first DMCA flap survival and donor site grali ‘take’.
minimise loss of function due to postoperative stiffness and this may be ofparticular value in older patients. In addition. the flap is applicable where microsurgical transfer of toe pulp tissue is not possible or felt to be unsuitable. for example in smokers or older patients where there is diminished potential for nerve regen- eration. Toe pulp transfer in such cases may yield moderate or poor two point discrimination in the reconstructed thumb (Ratcliffe and McGrouther. 1991).
In the five patients reported in this paper there was no morbidity related to the donor area on the dorsum of the index finger. Good take of grafts on preserved paratenon and design of the first DMCA flap so that incisions do not violate the specialised skin over the metacarpophalangeal and interphalangeal joints are contributing factors to this.
Acknowledgements
The authors wish to thank Mr John C. Dickinson and Mr Anthony H. N. Roberts for allowing us to report on their patients. We also acknowledge the Medical Illustration Department and Medical Library Services at Stoke Mandcwlle Hospital for their assistance. Mrs Karen M. Ratcliffe is thanked for her careful preparation of the manuscript.
References
Adamson. J. E.. Horton, C. E. and Crawford, H. H. I 1967). Sensory rehabilitation of the injured thumb. Phstic LOKI Recmsr~~tirc .Sll):fyI:l.. 40. 53.
Bralliar, F. and Horner, R. L. ( lY6Y). Senwry cross-linger pcdiclc graft. T/w Joumrl o/ Bow ttm/ Joiur .Su):~~~‘):l~. 51. 1264.
Earley, M. J. (1986). The arterial supply of the thumb. lirst web and mdex linger and its surgical apphcation. T/w Jww~ri o/ Wwrcl Sw~c,r>~. 1 I-B. 16.1.
Earley. M. J. and Milner, R. H. (IYX7). Dorsal metacarpal Rap\. &i/i.\/1 Jourwl (If P/o.\tic~ S/w~rr:l~. 40. 333.
Foucher, G. and Braun, J. B. ( 1979). A neh island tlap transfer from the dorsum of the index to the thumb. Plrrsrrc o/I(/ Rwrvr\tv~~ //I.(’ Sw~+,r>.. 63. IN.
Gurdin, M. and Pangman. W. J. ( 1950). The Ircpair of surface defect\ of fingers by transdigital flaps. P/cI.\!/I, ~rr~c/ Kww\/wt.rir o .Slrr,cwl,. 5. 36X.
Holevich, J. and Paneta-Holevich, E. (1971). Blpediclcd ~&nci tlap. .d<,lu Chiwr~~iuc, P6rvtiw. 13. 106.
Holevitch, Y. (1964). Use of skin islet llap from the dorsal aspect ot index finger for restoration of the scnsitivlty in the thumb. .-1<,/o Chirrrr,yirrc Plmricw. 6. I
Lister, G. (1981 ). The theor) of the transposition ilap and its practical application m the hand. C’/i/ric,.c i/l P/cr.ctic, .Grr~c,‘:i’. 8. I 15.
Marin-Braun, F., Merle, 31. and Foucher, G. (1X-Z). Lc lambcau cerf-volant. .-l~ft~ok~r I/C Cl~iwr~+ t/e ltl ,\/trOl, I. 147.
Michon, J. (I991 1. Kite flap in reconstruction of distal thumb. In Foucher. G. (Ed. ). Fin~~w/;/~ t/m/ .Vtri/hecl I?~jwiw. First edition. Edinburgh, Churchill Livingstone. p, 79.
Paneva-Holevich, E. and Holevich, Y. (1991). Further rxpctxnce with the bipedicled neurovascular island tlap in thumb recon- struction. The JOWIU/ of Htrnd Sur,yo:1~. 16-A. 594.
Rae, P. S. and Pho, R. W. H. (1983). The radial transposition flap- a useful composite flap. T/w Hmtf. 15. 96.
Ratcliffe, R. J. and McGrouther, D. A. ( I99 I ). Free toe pulp transfer in thumb reconstruction. Experience in the West of Scotland Regional Plastic Surgery Unit. Jo~wzu[ o/‘Hrr,~~lSlrr:ee~~,, 16B. 165.
Reid, D. A. C. (1976). The nrurovascular flap. .l<,/cr Or~/wpwr/ic~tr Belgica. 42. 349.
Rybka, F. J. and Pratt, F. E. (1979). Thumb reconstruction with :I sensory flap from the dorsum of the index linger. Phtic cm/ R~c.o,isl,.~rc.til.~ Szrrgc~r~, 64. I3 I
Sukur, D. and Radivojevic, M. (19X5). Cross linger flap, A new technique. The Jozrrr~ul of Htnrd .Swpr~. IO-B. 425.
The Authors
Robert J. Ratcliffe, BSc, FRCS(Ed). FRCS(Eng), Senior Registrar in Plastic Surgery.
Padraic J. Regan, FRCSI, Registrar m Plastic Surgrr). Codwin Y. Scerri, FRCS(Eng), RAF. Honorar> Senior Houac
Officer in Plastic Surgery.
The Plastic Surgery and Jaw Injury Service, Stoke Mandevillc Hospital. Mandeville Road. Aylesbury. Bucks HP21 XAL.
Requests for reprints to Mr R. J. Ratclifle.
Paper received 5 November 199 I, Accepted I8 May 1992. after revision.





























