Embed Size (px)
Citation preview

Fever in paediatrics
Dr Ehsan Ahmed(Consultant PaediatricianWalsall Manor Hospital)
Dr Sasan Iraji GPVTS1

Fever
• Indicates infection in child<5yr in most cases• Parental perceptions of fever are accurate
Fever definition
A fever is a high temperature. As a general rule, in children, a temperature of over 37.5°C (99.5°F) is a fever
Thermometers and the detection of fever
• Do not routinely use the oral and rectal routes to measure the body temperature of children aged 0–5 years.
• In infants <4 weeks use electronic thermometer in the axilla.• In children 4wk- 5yrs use one of the following:• electronic thermometer in the axilla• chemical dot thermometer in the axilla• infra-red tympanic thermometer
- Forehead chemical thermometers are unreliable
- Reported parental perception of a fever should be considered valid and taken seriously by healthcare professionals
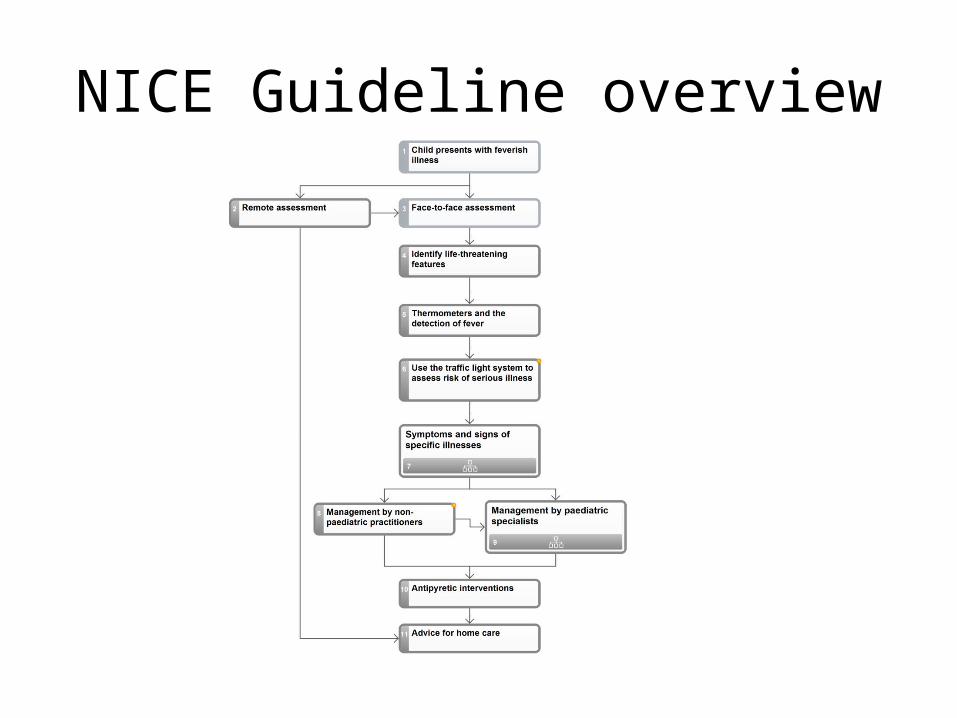
NICE Guideline overview
Remote assessment
• identify symptoms and signs of serious illness using the traffic light system and specific diseases
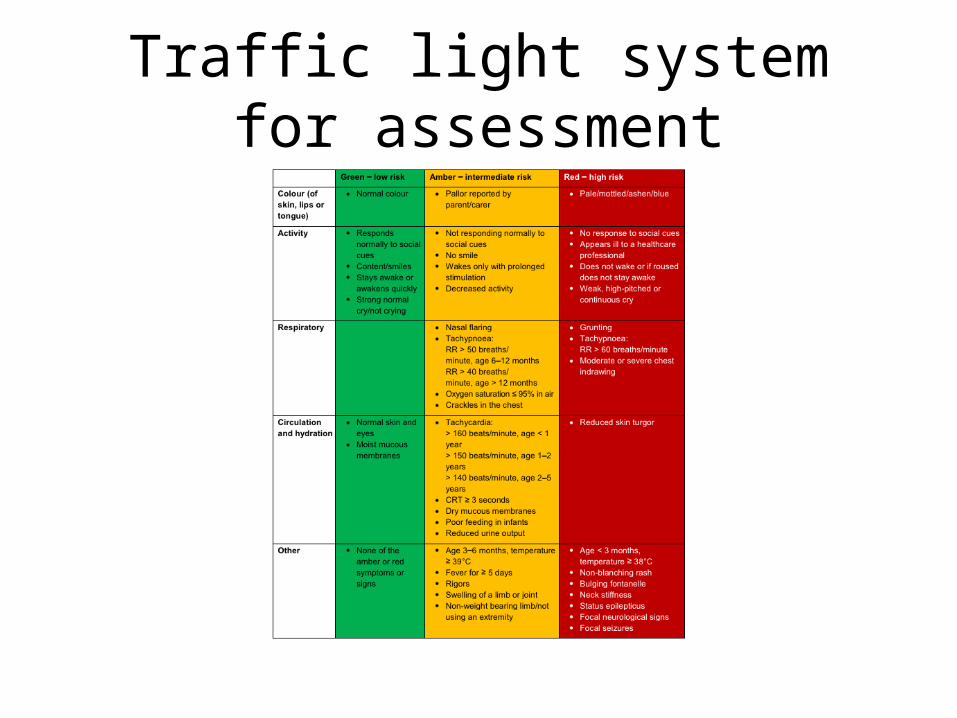
Traffic light system for assessment

Traffic light system
Red : Face-to-face assessment by a healthcare professional within 2 hours.
Amber : Face-to-face assessment by a healthcare professional- The urgency of this assessment should be determined by the clinical judgement of the healthcare professional carrying out the remote assessment
Green : Suitable for home care
Identify life-threatening features
Airway, breathing or circulation compromise and decreased level of consciousness
(A,B,C,D approach)
Face to face assessment; Use the traffic light system to assess risk of serious illness
Routinely check T, HR, RR and capillary refill time, BP
- Children <3 months with T 38°C or higher → high-risk group
- Children 3-6 months with T 39°C or higher, CRT>3 sec and Children with tachycardia → At least Amber group
• Fever >5 days assess for Kawasaki dx• Do not forget travel history
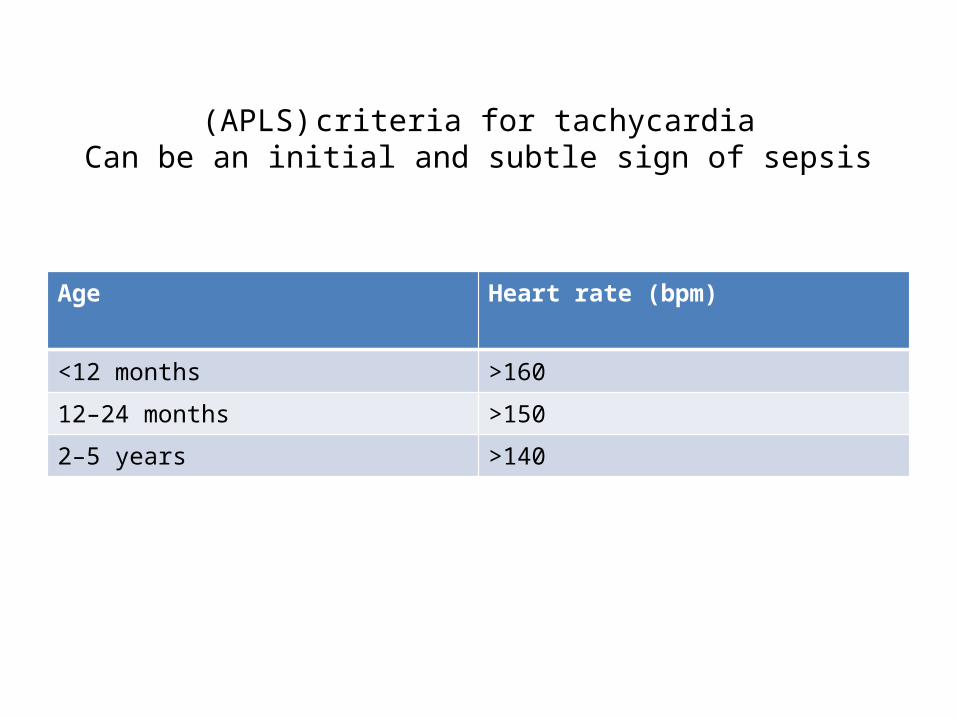
(APLS) criteria for tachycardiaCan be an initial and subtle sign of sepsis
Age Heart rate (bpm)
<12 months >160
12–24 months >150
2–5 years >140
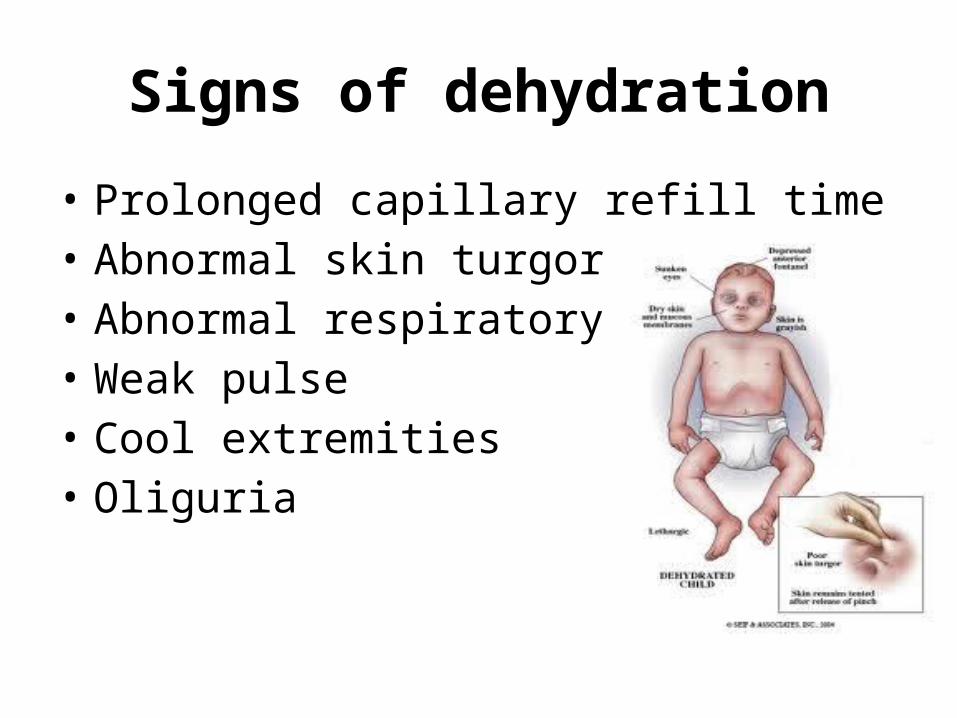
Signs of dehydration
• Prolonged capillary refill time• Abnormal skin turgor• Abnormal respiratory pattern• Weak pulse• Cool extremities• Oliguria
Other signs and symptoms in high risk group (Red light) → Urgent referral
• pale/mottled/ashen/blue skin, lips or tongue• no response to social cues• appearing ill to a healthcare professional• does not wake or if roused does not stay awake• weak, high-pitched or continuous cry• grunting• respiratory rate greater than 60 breaths per minute• moderate or severe chest indrawing• reduced skin turgor• bulging fontanelle.• Petechial rash
Other signs and symptoms in intermediate risk group (amber light) → face-to-face assessment
• pallor of skin, lips or tongue reported by parent or carer• not responding normally to social cues• no smile• wakes only with prolonged stimulation• decreased activity• nasal flaring• dry mucous membranes• poor feeding in infants• reduced urine output• rigors
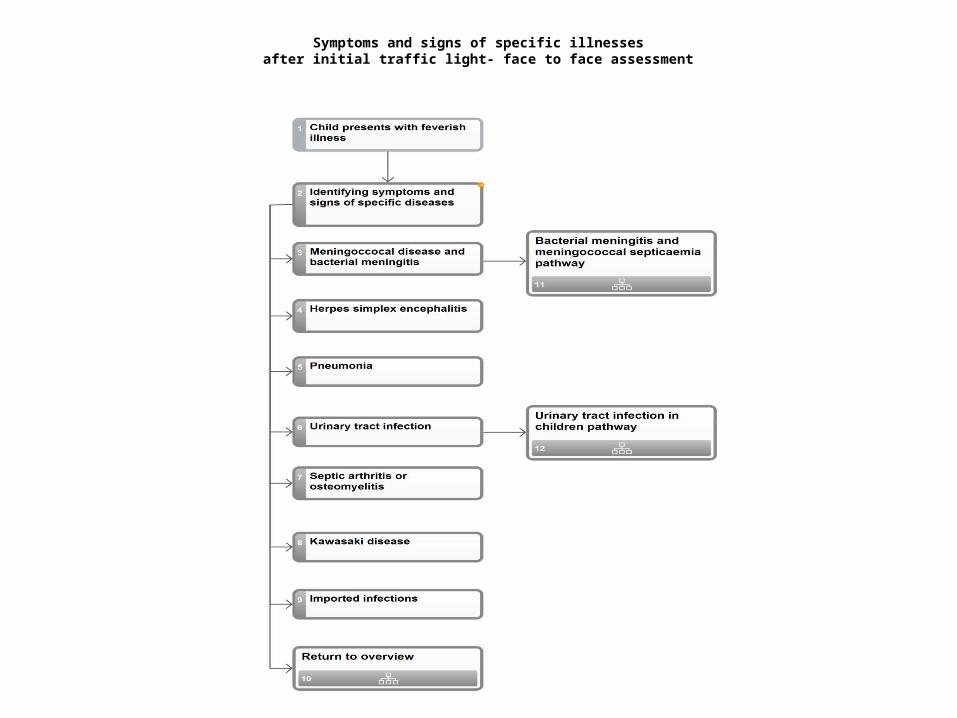
Symptoms and signs of specific illnessesafter initial traffic light- face to face assessment
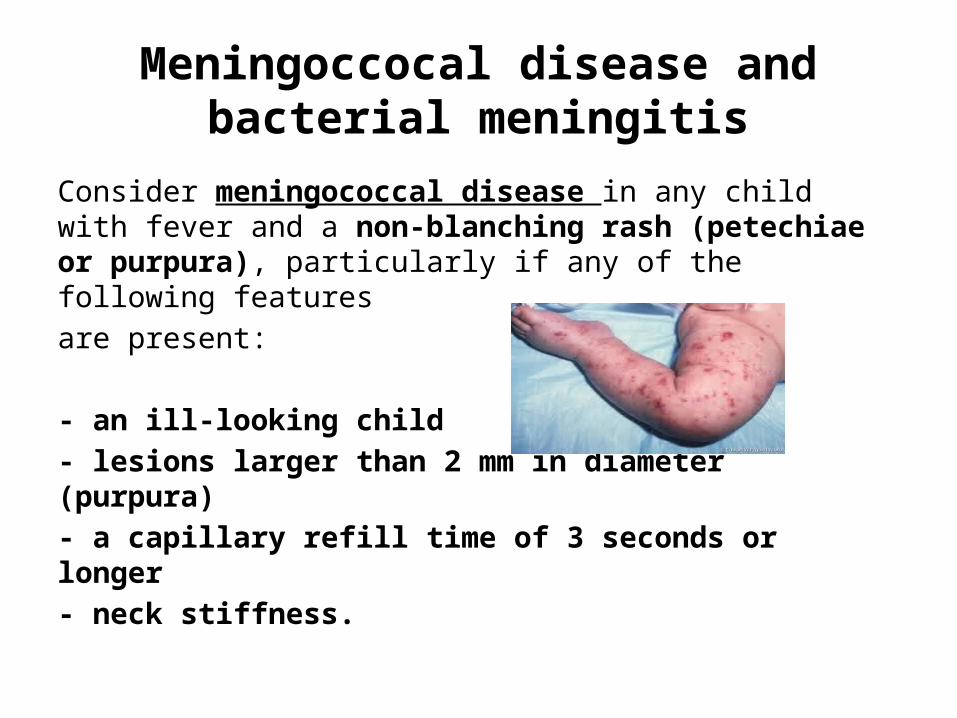
Meningoccocal disease and bacterial meningitis
Consider meningococcal disease in any child with fever and a non-blanching rash (petechiae or purpura), particularly if any of the following features are present:
- an ill-looking child- lesions larger than 2 mm in diameter (purpura)- a capillary refill time of 3 seconds or longer- neck stiffness.
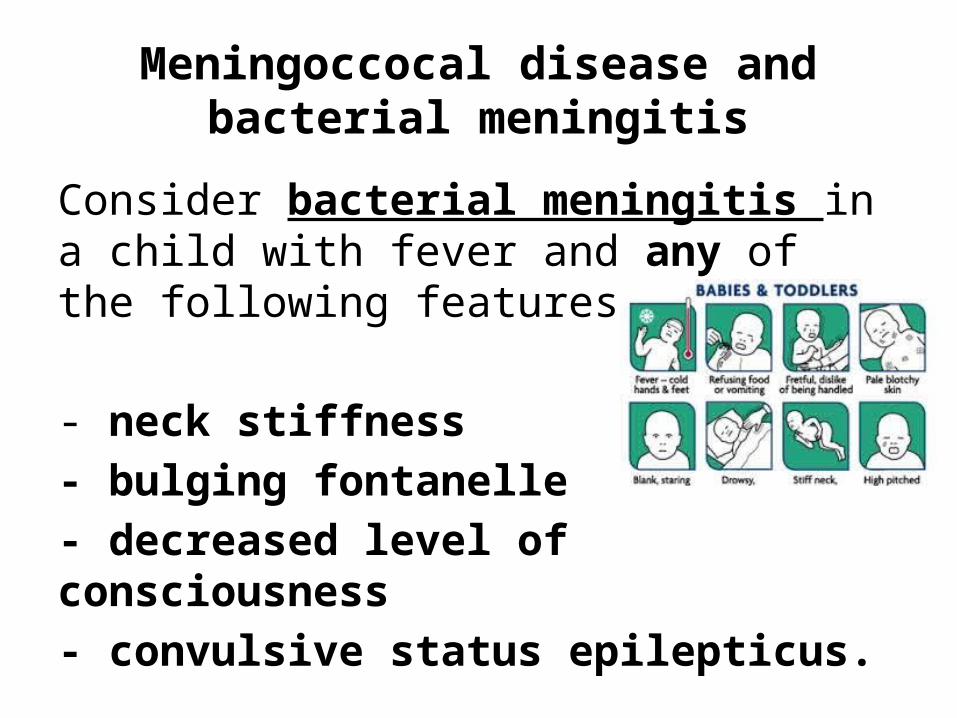
Meningoccocal disease and bacterial meningitis
Consider bacterial meningitis in a child with fever and any of the following features:
- neck stiffness- bulging fontanelle- decreased level of consciousness- convulsive status epilepticus.

Herpes simplex encephalitis
Consider in a child with fever and any of the following:
• focal neurological signs• focal seizures• decreased level of consciousness.
Pneumonia
Fever and any of the following signs
• tachypnoea • crackles • nasal flaring• Recession • cyanosis• oxygen saturation ≤95% in room air
Urinary tract infection
- Consider in any child <3 months with fever
- Consider UTI in >3 months with fever and any of the following
• vomiting• poor feeding• lethargy• irritability• abdominal pain or tenderness• urinary frequency or dysuria
Septic arthritis or osteomyelitis
- Fever and any of the following signs:
• swelling of a limb or joint• not using an extremity• Limping non-weight bearing
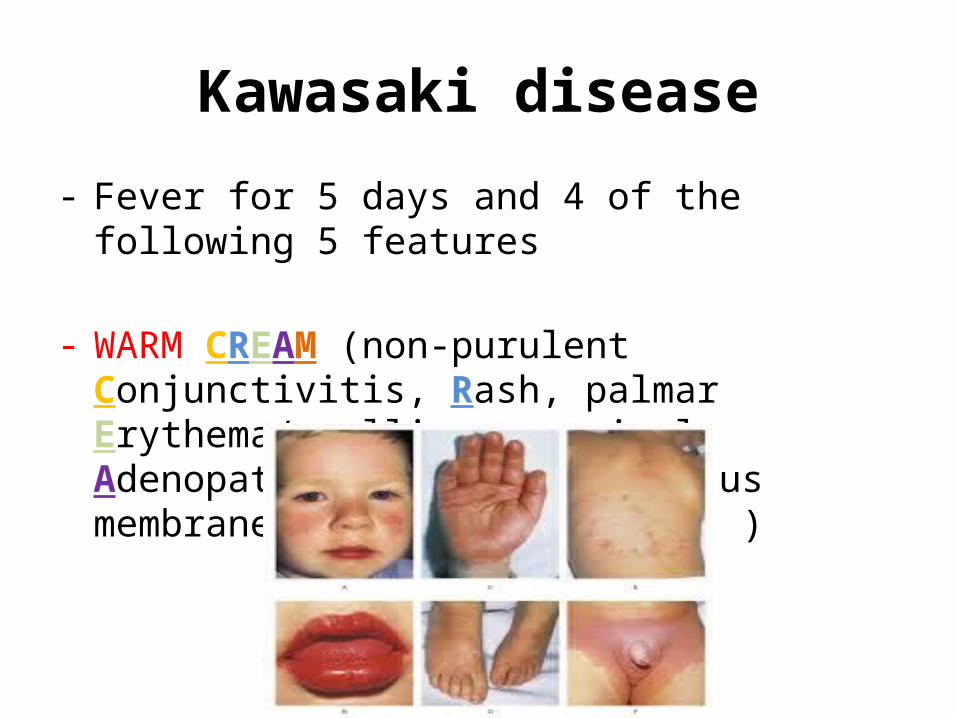
Kawasaki disease
- Fever for 5 days and 4 of the following 5 features
- WARM CREAM (non-purulent Conjunctivitis, Rash, palmar Erythema/swelling, cervical Adenopathy, dry and red Mucous membranes, strawberry tongue )
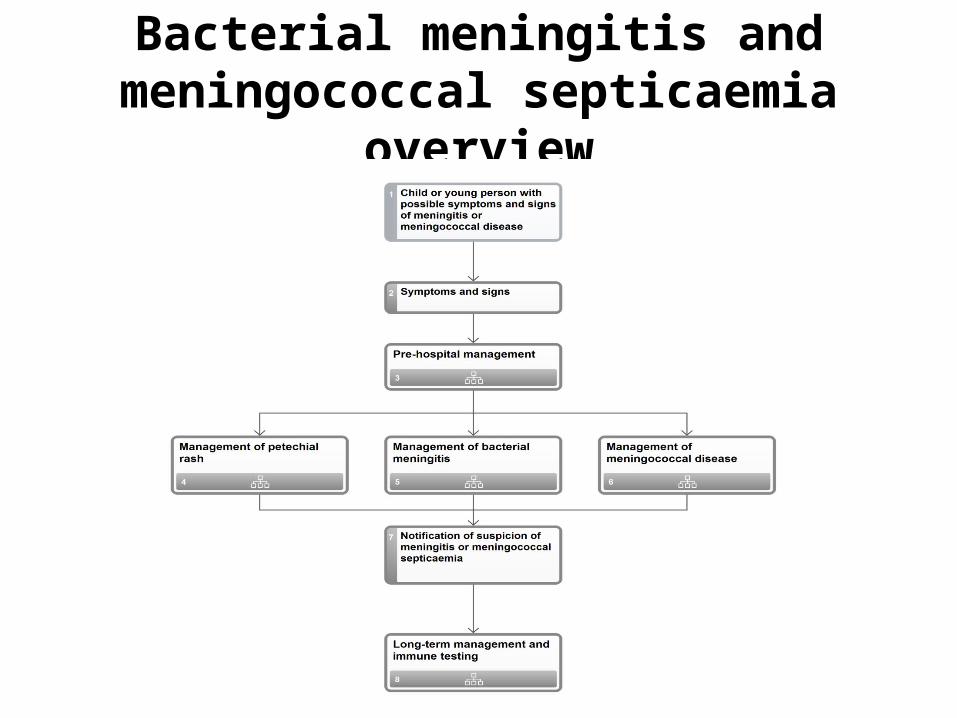
Bacterial meningitis and meningococcal septicaemia overview
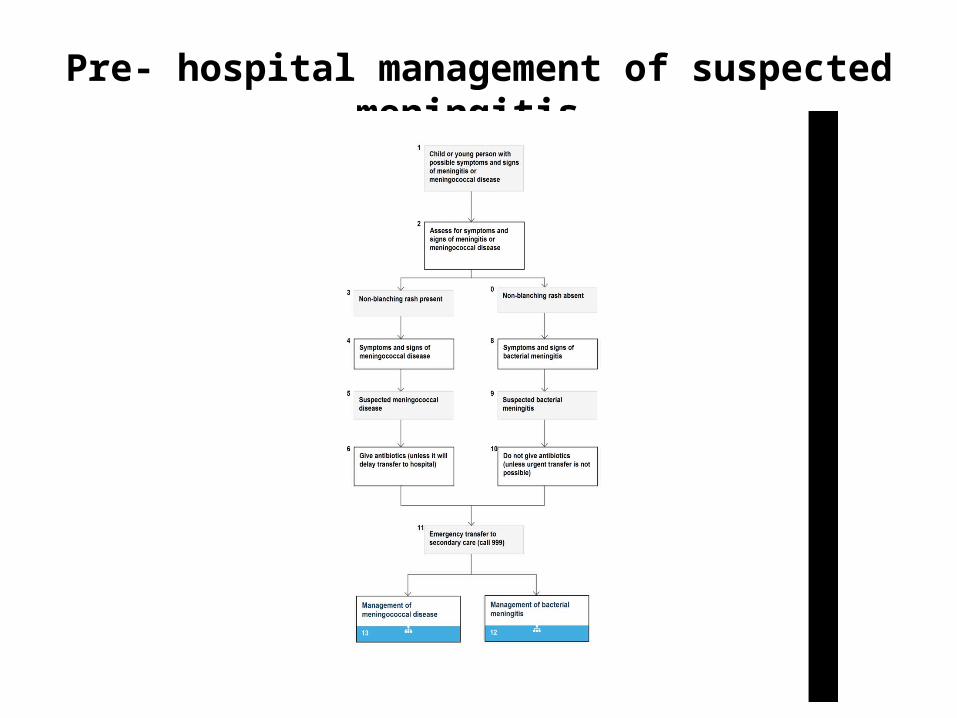
Pre- hospital management of suspected meningitis
Management a child with fever by non-paediatric practitioners
• Three stages assessment:
• 1- Identify life-threatening features (A,B,C,D)• 2- Traffic light system for assessment• 3- Attempt to identify source of infection/feature
• Red features: urgent referral to paediatric specialist
Management a child with fever by non-paediatric practitioners
• Amber features: If any 'amber' features but no diagnosis
a) safety nets to parents (verbal and/or written information on
warning symptoms, arranging further follow-up or access to OOH providers)
------OR------
b) referral to paediatric team
• Green features: home care with appropriate advice
Antipyretic interventions
• Antipyretic agents do not prevent febrile convulsions and should not be used specifically for this purpose
• Tepid sponging is not recommended
• Children with fever should not be underdressed or over-wrapped.
• Consider using either paracetamol or ibuprofen in children with fever who appear distressed.
Antipyretic interventions
When using paracetamol or ibuprofen in childrenwith fever:
• continue only as long as the child appears distressed
• do not give both agents simultaneously• only consider alternating these agents if the
distress persists or recurs before the next dose is due
Advice for home care
• To encourage their child to drink more fluids• How to detect signs of dehydration• How to identify a non-blanching rash• To check their child during the night• To keep their child away from nursery or
school
When to seek further help
• Any fits• Non-blanching rash• Child is less well than when they previously
sought advice• Parents are more worried than when they
previously sought advice• Fever > 5 days• the parent is distressed, or concerned that they
are unable to look after their child.

Take home messages
• Three stages assessment in a child with fever:
• 1- Identify life-threatening features (A,B,C,D)• 2- Traffic light system for assessment. Prompt
action as per clinical assessment.• 3- Attempt to identify source of
infection/feature and treat or act as necessary.
Take home messages
- Children <3 months with fever → high-risk group
- Children 3-6 months with T 39°C or higher, CRT>3 sec and Children with tachycardia → At least Amber group
- Do not give paracetamol and ibuprofen simultaneously
- Parental education and safety nets
THANKS FOR LISTENING
ANY QUESTIONS?
References
• http://pathways.nice.org.uk/pathways/feverish-illness-in-children
• Paediatric Guidelines 2013-2014, Bedside Clinical Guideline Partnership
• http://pathways.nice.org.uk/pathways/bacterial-meningitis-and-meningococcal-septicaemia
• http://www.uptodate.com/contents/fever-in-children-beyond-the-basics
• http://www.nice.org.uk/guidance/cg160/chapter/key-priorities-for-implementation