Embed Size (px)
Citation preview
588
Fetal Ductus Arteriosus LigationPulmonary Vascular Smooth MuscleBiochemical and Mechanical Changes
Jaques Belik, A.J. Halayko, K. Rao, and Newman L. Stephens
To evaluate the smooth muscle mechanical and biochemical changes associated with persistent pulmo-nary hypertension syndrome of the newborn, we studied 31 fetal sheep in which the ductus arteriosus wasligated at 125 days of gestation. Sixty-one noninstrumented and six sham-operated fetuses served as
controls. All animals were delivered by cesarean section at 137-140 days of gestation, and theexperimental group had the ductus arteriosus ligated for 12±3 days. The ligated group demonstrated a
higher mean (±SEM) pulmonary artery pressure (72.3±3.8 versus 54.1±2 mm Hg, p<0.01) and rightventricular mean free wall weight (12.5±0.7 versus 6.8±0.3 g, p<0.01) as compared with the sham-operated group. Significant changes in the pulmonary vascular smooth muscle of the ligated group wereobserved. The myosin content of vessels from the second through fifth generation demonstrated a
significant increase in actin and myosin content (p<0.01), but given their disproportional changes, thenoninstrumented group demonstrated a lower actin/myosin ratio than the experimental group (p<0.01).Changes in the myosin heavy chain isoform stoichiometry, characterized by an increase in both the meanhigh/low myosin heavy chain isoform ratio (1.8±0.3 versus 1.0±0.1, p<0.05) and the nonmuscle isoformas a percentage of the total myosin heavy chain (12.4±0.7% versus 2.7±0.9%o,p <0.01), were also observedin the ligated as compared with the noninstrumented animals. In addition, the muscle Mg-ATPase activitywas significantly (p<0.05) reduced in the experimental group. The pulmonary vascular smooth muscle ofligated animals developed less force (p<0.01) and shared similar maximum shortening capacity andlonger isotonic half-relaxation time (p<O0.05) as compared with the noninstrumented group. To the extentthat the present data can be extrapolated to persistent pulmonary hypertension syndrome of the newborn,it is unlikely that the postnatal maintenance of a high resistance in this syndrome is the result of greatervascular muscle contractility. (Circulation Research 1993;72:588-596)KEY WoRDs * ductus arteriosus * pulmonary hypertension * hypoxemia
P ersistent pulmonary hypertension syndrome ofthe newborn (PPHN) is a clinical entity charac-terized by persistent hypoxemia secondary to
the maintenance of a high pulmonary vascular resis-tance and right-to-left shunting across the fetal channelsafter birth.' Its etiology and pathogenesis are unknownbut believed to be secondary to intrauterine abnormalevents.1
It has recently been recognized that complete orpartial occlusion of the fetal ductus arteriosus in prena-tal sheep is associated with lung histological changessimilar to those observed in infants dying with thePPHN syndrome.2-7 After birth, the ductus arteriosus-ligated animal has a high pulmonary vascular resistance,abnormal pulmonary vasoreactivity to increased in-spired oxygen, and evidence of right-to-left shunting atthe foramen ovale level.8 Thus, the ductus arteriosus-ligated fetal sheep is the first animal model of PPHNrepresentative of the human disease and is perhaps
From the Departments of Pediatrics and Physiology, Universityof Manitoba, Winnipeg, Canada.
Supported by a grant from The Heart and Stroke Foundation ofCanada and The Hospital for Sick Children Foundation, Toronto,Canada.Address for correspondence: Jaques Belik, MD, Room WR 004,
735 Notre Dame, Winnipeg, Manitoba, R3E OL8 Canada.Received June 26, 1992; accepted November 23, 1992.
suitable for determining the mechanism involved in themaintenance of a high pulmonary vascular resistanceafter birth in affected newborns.Concerning the pathogenesis of PPHN syndrome, a
commonly held view is that the failure of the pulmonaryvascular resistance to decrease after birth is secondaryto the increased muscularization of the pulmonaryvasculature.910 Implicit in this hypothesis is that thepersistence of a high pulmonary vascular resistance inthe syndrome is secondary to the effect produced bysmooth muscle cells that, either by their increasednumber or increased responsiveness to humoral factors,have a greater potential to induce and maintain vaso-constriction. Little is known, however, about the me-chanical properties of the vascular smooth muscle inPPHN syndrome.We recently demonstrated that perinatal pulmonary
vascular smooth muscle is at a mechanical disadvantageas compared with adult muscle." In normal sheep, thefetal and newborn pulmonary vasculature generates lessforce and has a lower shortening capacity than the adultpulmonary vasculature,1" indicating that, under physio-logical conditions, the pulmonary vascular muscle of thefetus has less potential for shortening and thus lesspotential for increasing vascular resistance.
Furthermore, in at least one model of pulmonaryhypertension - monocrotaline-induced pulmonary hy-
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

Belik et al Pulmonary Vascular Muscle and Fetal Ductus Arteriosus Ligation 589
pertension in the rat- in which excessive pulmonaryvascular muscularization is also seen, the pulmonaryvascular muscle was shown to generate less force than inthe control condition.'2 Although morphological sub-strate differences between the fetal sheep and adult ratlung do exist, these data suggest that the medial hyper-trophy of the pulmonary vasculature in the rat model ofpulmonary hypertension consists of hypertrophiedsmooth muscle cells with reduced contractility.
Therefore, to ascertain the role of muscle contractionin the maintenance of a high resistance to blood flowafter birth in the PPHN syndrome, we evaluated bio-chemical and mechanical property changes of pulmo-nary vascular smooth muscle after ductus arteriosusligation in fetal sheep.
Materials and MethodsAnimal Preparation
Pregnant ewes between 123 and 127 days of gestation(term, 145 days) were fasted for at least 24 hours beforesurgery. The ewes were anesthetized with intravenouspentobarbital sodium (loading dose, 20 mg/kg; mainte-nance, 1 mg/kg every 30 minutes). Under sterile condi-tions, the fetal head and upper chest were deliveredthrough a uterine incision. A left fetal thoracotomy wasperformed, exposing the heart and great vessels. Theductus arteriosus was identified and ligated with 2-0 silksuture in 31 fetuses (ligated group). The chest wasclosed in layers. The fetus was carefully returned to theuterus, the wall of which was closed in layers. Particularcare was taken to avoid any significant amniotic fluidloss. Catheters, when placed, were tunneled to the flankof each ewe, and ampicillin (1 g) was injected into theamniotic sac and abdominal cavity at the time ofsurgical closure. Thereafter, both ewe and fetus re-ceived antibiotics for 4 days. The ewe received 1x 106units penicillin and 50 mg gentamicin intramuscularlytwice daily, and the fetus received one half of this doseintravenously once a day when a catheter was in place.All wounds were cleaned daily, and the catheters werefilled with fresh heparin solution (1,000 units/ml) toprevent clotting.
Six ewes were subjected to the same surgical proce-dure, but the ductus arteriosus was only visualized andnot ligated (sham-operated group). In twelve of theligated and in all sham-operated animals, polyvinylcatheters (5F) were placed into the carotid artery andjugular vein for hemodynamic measurements. In thesefetuses, blood samples (0.3 ml) were obtained dailyfrom the carotid artery for blood gas and pH measure-ments carried out with a blood gas analyzer (modelABL-3, Radiometer, Copenhagen). In the ductus arte-riosus-ligated fetuses in which no intravascular cathe-ters were placed, daily two-dimensional real time ultra-sound images were obtained to confirm that the fetuseswere alive by documenting the presence of heart beats.Sixty-one noninstrumented sheep fetuses served ascontrols (noninstrumented group).
Experimental DesignBetween 137 and 140 days of gestation the noninstru-
mented, sham-operated and ligated ewes were sub-jected to a cesarian section under pentobarbital sodium
and a 5F Swan-Ganz catheter was advanced from thejugular vein into the pulmonary artery. Sequentialmeasurements of mean right atrial, ventricular, andpulmonary arterial pressures were obtained. Systemicarterial pressure was also recorded by the carotid arterycatheter. Vascular and intracardiac pressures weremeasured with pressure transducers (Gould Inc., Ox-nard, Calif.) and continuously recorded on paper. Mea-surements of heart rate were derived from the pressure-wave frequency. Subsequently, the fetus was subjectedto a left thoracotomy, and a precalibrated electromag-netic flow probe (flowmeter and probe, Carolina Med-ical Electronics, Inc., King, N.C.) of adequate size (lessthan 20% constriction of the vessel) was placed aroundthe main pulmonary artery immediately proximal to theductus arteriosus; then a measurement of right ventric-ular output was obtained. Finally, the left atrial pressurewas obtained by direct puncture of the left atrium. Allfetuses were rendered apneic at the time of cesareansection by the pentobarbital sodium anesthesia admin-istered to the ewe; thus, the lungs were never inflated or
oxygenated.After the hemodynamic measurements, the fetus was
rapidly killed with an intravenous dose of potassiumchloride, and after the body weight was obtained, thelungs and heart were removed en bloc.
Confirmation of the effective ligature of the ductusarteriosus was always sought by probing the ductusarteriosus from the pulmonary artery side during thepostmortem examination.
Organ WeightsThe hearts from all animals were dissected to obtain
the free wall weights of the right and left ventricles,septum, and atria. In addition, the liver weights were
also obtained from all animals. These measurementswere obtained to evaluate the impact of chronic in-creased afterload on the fetal heart. Total fresh wetlung weight was obtained as a crude measurement oflung edema.
Vascular Smooth Muscle MechanicsA segment of the second generation intralobar pul-
monary artery of randomly selected ligated and nonin-strumented animals was carefully dissected and placedin ice-cold Krebs-Henseleit solution. Using our leversystem to obtain pulmonary vascular muscle mechanicalmeasurements in pilot experiments in sheep, we ob-served that only second-generation intralobar pulmo-nary arterial strips yielded consistent results. Smallerarteries (third and fourth generations) showed poorforce development and shortening (authors' unpub-lished data), likely related to the deleterious effect oftissue dissection and handling on the contractility of thesmooth muscle cells. Thus, in the present study themechanical properties of only the second-generationintralobar pulmonary arterial strips were delineated.The pulmonary vessel rings were transversely opened,
yielding a 2-mm-wide rectangular strip. The strips wereattached to a clamp fixed to the bottom of a 10-ml bathcontaining Krebs-Henseleit solution at 37°C, pH 7.4,P02 of 600 mm Hg, and Pco2 of 40 mm Hg. The upperend was tied by 7- 0 graded silk to the magnesium arm of
anesthesia. The fetal head was carefully exteriorized, an electromagnetic muscle lever system.
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

590 Circulation Research Vol 72, No 3 March 1993
The following mechanical measurements were ob-tained: 1) Length-force curves were initially obtained toestablish the optimal length and the maximum isometrictension. 2) Maximal shortening capacity was obtainedby the quick-release method, which consisted of releas-ing the muscle to a quasi-zero load (0.5 mN) underpassive and active contraction. For the passive contrac-tions, the degree of muscle shortening after passiverecoil (releasing the muscle to a quasi-zero load from itsresting tension without stimulation) was measured. Forthe measurement of active contraction, 2 seconds afterthe onset of the electrical stimulation (18 V, 10 sec-onds), the muscle was released to a quasi-zero load andallowed to shorten maximally. The maximal active short-ening capacity was represented by the difference be-tween total and passive shortening and expressed as apercentage of the optimal length. 3) Isometric half-relaxation time was measured as the time for the forcegenerated during an electrically stimulated isometriccontraction to decrease by 50%. 4) Isotonic half-timerelaxation was measured by a previously describedtechnique to obtain a load and initial contractile ele-ment-length independent index of isotonic relaxationtime, based on the fact that muscle relaxation dependson the load that it is subjected to, the state of muscleactivation, and the length of the muscle contractileelement at the onset of relaxation.1314 Briefly, at theirideal lengths, the muscle strips were supramaximallyelectrically stimulated to elicit maximal isotonic short-ening. The stimulus was turned off at peak shortening,and the muscle strips were allowed to elongate. Imme-diately after the termination of the electrical stimula-tion, a series of load clamps were applied. The applica-tion of instantaneous load clamps at the same point intime for each contraction ensures that the muscle stripswill begin to relax at the same length of the musclecontractile element even under different loads. For eachof the loads, the time to elongate 50% of the initiallength (half-time) was determined. The half-times foreach curve with their respective loads were fit by linearregression, and the zero-load half-time was extrapo-lated. For all vessel strips, the correlation coefficient forthe load versus half-time was 0.95 or higher (p<0.01).The intercept of the linear regression equation yieldsthe isotonic relaxation index, which is load and initialcontractile element-length independent. 5) Vessel wallcompliance was measured as the slope of the changes inlength induced by loads of different magnitude afterpapaverine (10`4 M) was added to the muscle bath toprevent stretch-induced contraction.
Measurement of Myosin and Actin ContentRight and left pulmonary arterial strips were care-
fully dissected from lung parenchyma and connectivetissue in Krebs-Henseleit solution (4°C) within 2 hoursof procurement. The pulmonary vascular generationschosen for study were selected according to the classi-fication of Levin et al.15The dissected vascular tissues were stored separately
at -70°C until required for myosin and protein extrac-tion. The method used has been previously described."Briefly, thawed tissue was homogenized for 1 minute in4 vol extraction buffer (40 mM Na4P207, 1 mM MgCI2,1 mM EGTA, 20 gM leupeptin, 1 mM dithiothreitol,
a Potter-Elvehjem tissue grinder. After homogeniza-tion, the crude supernatant extracts obtained wereassayed for protein content by the method of Brad-ford.16 This technique enabled us to measure the tissuesmooth muscle cell protein content, as represented bythe supernatant protein concentration. All collagen-and elastin-derived proteins have been previouslyshown to fully precipitate after centrifugation as pres-ently carried out in a procedure used by us.17Sodium dodecyl sulfate-polyacrylamide gel electro-
phoresis (SDS-PAGE) was carried out according to theprocedure of Laemmlil8 by using 4-20% linear poly-acrylamide gradient separating gels with 3% stackinggels. Known amounts of crude original supernatant andpellet extracts were applied to the gels, and electropho-resis was carried out for 3-3.5 hours using a constantcurrent of 20 mA at 15°C. Myosin heavy chain and actincontents of the gels were determined by quantitativedensitometry using an LKB Ultroscan XL laser densi-tometer. To avoid any overestimation or underestima-tion of the contractile proteins, the relative dye-bindingcapacities of purified myosin heavy chain and actin weredetermined as described by Sutoh.'9The total amounts of myosin heavy chain and actin in
the supernatant and pellet extracts were summed andthen normalized to the original fresh wet weight of thetissue sample to obtain the myosin content of the wholetissue. The identity of the myosin heavy chain banddetected by SDS-PAGE was confirmed by Westernimmunoblot by using antibodies specific for smoothmuscle (rabbit anti-chicken gizzard myosin supplied byDr. Ute Groschel-Stewart, University of Darmstadt[FRG]). The identity of bands corresponding specifi-cally to actin was confirmed by using commerciallyavailable monoclonal antibodies specific for smoothmuscle a-actin (Boehringer Mannheim Corp., India-napolis, Ind.).
Myosin Heavy Chain Isoform DistributionSmooth muscle and nonmuscle myosin heavy chain
isoforms were separated by 4% SDS-PAGE at 10°C on8x10-cm minigels using the Laemmli'8 buffer system.Crude pulmonary artery sample loads were kept below3 ,ug and at the smallest possible volume (usually under10 gl) to obtain maximal separation of heavy chains.Gels were run at a constant voltage of 200 V for 60-65minutes and immediately used in Western blottingexperiments or were fixed in 40% (vol/vol) methanol-10% (vol/vol) acetic acid for silver staining. Proteinbands in unblotted gels were visualized by use of acommercial silver-staining kit (Rapid-Ag-Stain, ICNBiomedicals, Cleveland, Ohio). Gels were scanned withan LKB Ultroscan XL laser densitometer (663 nm) toevaluate myosin heavy chain isoform stoichiometry.For Western blot studies, proteins were electroblot-
ted to nitrocellulose paper at 4-8°C by a 25 mMTris-192 mM glycine (pH 8.3) transfer buffer.20 Blotswere blocked overnight and then were shaken in phos-phate-buffered saline (0.05% Tween 20) containingeither 10 ,ug/ml rabbit anti-chicken gizzard myosinimmunoglobulin G21 or 10 gg/ml rabbit anti-chickenthrombocyte myosin immunoglobulin G22 for 2.5 hoursto identify smooth muscle and nonmuscle myosin heavychains. Goat anti-rabbit immunoglobulin G conjugated
and 250,OM phenylmethylsulfonyl fluoride, pH 8.8) with with horseradish peroxidase, diluted 1: 2,000 as per the
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

Belik et al Pulmonary Vascular Muscle and Fetal Ductus Arteriosus Ligation 591
TABLE 1. Fetal Arterial Blood Gases and pH After SurgerySham-operated (n =6) Ligated (n= 12)
Time after surgery (hours) 24 72 24 72pH 7.30±0.01 7.38+0.00 7.25+0.03 7.35+0.00*Paco2 (mm Hg) 49.1±1.2 47.3±1.4 57.7+3.3t 53.0±1.1*Pao2 (mm Hg) 22.3±1.5 14.7±1.0 19.3±1.4 15.9±1.4Standard bicarbonate (mM/1) 21.6±0.6 24.4±0.6 20.6±1.3 25.7±0.6
n, Number of sheep. Values are mean±SEM.*p<0.01 and tp<0.05 compared with respective values in the sham-operated group.
manufacturer's instructions (ICN ImmunoBiologicals,Cleveland, Ohio), was used as the secondary antibody;then blots were developed in Tris-buffered saline con-
taining 0.05% chloronaphthol, 16.7% (vol/vol) metha-nol, and 0.015% H202.
Measurement of Myosin A TPase ActivityMyosin ATPase activity was measured in crude ho-
mogenates of ligated and noninstrumented pulmonaryarteries prepared as described previously.2324 Briefly,Mg-ATP (final concentration, 2 mM) was added to thecrude homogenates to initiate the reaction, which was
subsequently halted after 30 seconds with the additionof trichloroacetic acid to 10% (vol/vol). The concentra-tion of inorganic phosphate liberated was quantified bythe malachite green colorimetric assay.24 Rates of inor-ganic phosphate liberation (ATP hydrolysis) were nor-malized to crude homogenate myosin heavy chain con-tent determined by the quantitative SDS-PAGEdescribed earlier.To exclude any error related to differences in vascular
tissue water content, the wet/dry weight ratios of secondgeneration strips from the noninstrumented and ligatedgroups were obtained.
Statistical AnalysisData were processed by Students' t test and two-way
analysis of variance. All data are reported asmean+SEM and p<0.05 was considered significant.
ResultsOf all ligated fetuses, 10 were alive at the time of the
scheduled cesarean section, and another two fetuseswere delivered vaginally after natural labor within 24hours from the scheduled cesarean date (total of 12ligated animals). Nineteen other ligated fetuses werestillborn. The mean gestational age of the animalsstudied at cesarean section was 136±2 days, and theductus arteriosus of these animals was ligated for 12±3days. All stillborn animals were alive at least 24 hoursbefore abortion, based on daily fetal ultrasound assess-ment, and had a gestational age of 135± 1 days andduration of ductus arteriosus ligation of 6±1 days. Allsix sham-operated animals were alive at the time of thecesarean section, had a gestational age of 136±2 days,and were surgically instrumented 8±3 days before de-livery. The noninstrumented fetuses (n=61) had a
gestational age of 137±3 days and were all alive at thetime of cesarean section.
For the first 3 days after surgery, arterial blood gasesand pH were consistently obtained in all animals inwhich a catheter had been placed but were not availableon a daily basis from every fetus thereafter because of
technical problems (obstruction or displacement of thearterial catheter). At 24 and 72 hours after surgery, thevalues were similar in both groups except for a small butsignificantly higher Paco2 at 24 and 72 hours and lowerpH at 72 hours in the ligated group (Table 1).
Hemodynamic MeasurementsThe ligated fetuses had a significantly higher pulmo-
nary arterial pressure (p<0.01) with no differences insystemic arterial pressure, atrial pressure, and heartrate when compared with the sham-operated group.
The mean right ventricular output was reduced byalmost 50% in the ligated animals (p<0.05) (Table 2).
Organ WeightsThe measured organ weights for the noninstru-
mented, sham-operated, and ligated groups are summa-
rized in Table 3. Ductus arteriosus ligation resulted in a
65% increase in total heart weight (p<0.01) and a smallincrease in liver weight (p<0.01 when compared withthe noninstrumented group only). The lungs and totalbody weight did not significantly vary between groups.
As a percentage of the total heart weight, the rightventricular free wall was greater and the left was lowerwhen compared with the noninstrumented and sham-operated groups (p<0.01, Table 4). No significant dif-ferences between the noninstrumented and sham-oper-ated animals were present for these variables.
TABLE 2. Hemodynamic Measurements
Sham-operated Ligated(n =6) (n= 10)
Blood pressureSystemic arterial (mm Hg)
Systolic 62.4± 1.2 59.8+2.5Diastolic 52.4±1.3 50.7+2.1Mean 57.2+1.3 55.3+2.1
Pulmonary arterial (mm Hg)Systolic 59.7+2.4 81.7+6.6*Diastolic 50.2+2.1 65.7±2.9*Mean 54.1±2.0 72.3 3.8*
Right atrial (mm Hg) 3.9+0.8 5.9+1.4Left atrial (mm Hg) 3.2±0.4 2.5 +0.7
Right ventricular output(ml* min-1 * kg-') 117.7±23.9 63.2+17.8tHeart rate (bpm) 221±8.0 191.7±13.9
n, Number of sheep; bpm, beats per minute. Values aremean± SEM.
*p<0.01 and tp<0.05 compared with the sham-operated group.
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

592 Circulation Research Vol 72, No 3 March 1993
TABLE 3. Body and Organ Weights
Noninstru-mented Sham-operated Ligated
Weight (n=61) (n=6) (n=31)Body (kg) 3.1+0.1 3.3±0.2 3.1+0.2Heart (g/kg body wt) 7.9+0.1 7.34+0.2 11.9+0.6*Liver (g/kg body wt) 24.3+0.6 29.1+3.8 31.7+1.7tLungs (g/kg body wt) 25.6±+1.4 31.7± 1.3 27.2+2.0
n, Number of sheep. Values are mean±SEM.*p<0.01 compared with the two other groups; tp<0.01 com-
pared with the noninstrumented group only.
Pulmonary Vascular MechanicsThe pulmonary vascular muscle stresses following
supramaximal electrical and high potassium stimulationwere significantly decreased in the experimental ani-mals (Figure 1), whereas the shortening capacity andthe isometric relaxation half-time were not significantlydifferent between groups. The isotonic relaxation half-time was significantly prolonged in the ligated group(Table 5). The vascular wall compliance was 23±5,um/mN (n= 12) in the noninstrumented and 20±4(n=12) in the ligated group (p=NS).Biochemical ChangesThe myosin heavy chain content of second through
fifth generation vessels was at least twofold greater in theligated group as compared with the noninstrumentedgroup (Figure 2). The second through fifth generationcombined actin content of the ligated group also in-creased (2.20±0.19 [n=11] versus 0.85±0.06 [n=25],ug/mg wet tissue in the noninstrumented group,p< 0.01).However, given the disproportional changes between thetwo proteins, the actin/myosin ratio was significantlylower in the ligated group (p<0.01) (Figure 3).The stoichiometry of the pulmonary vascular muscle
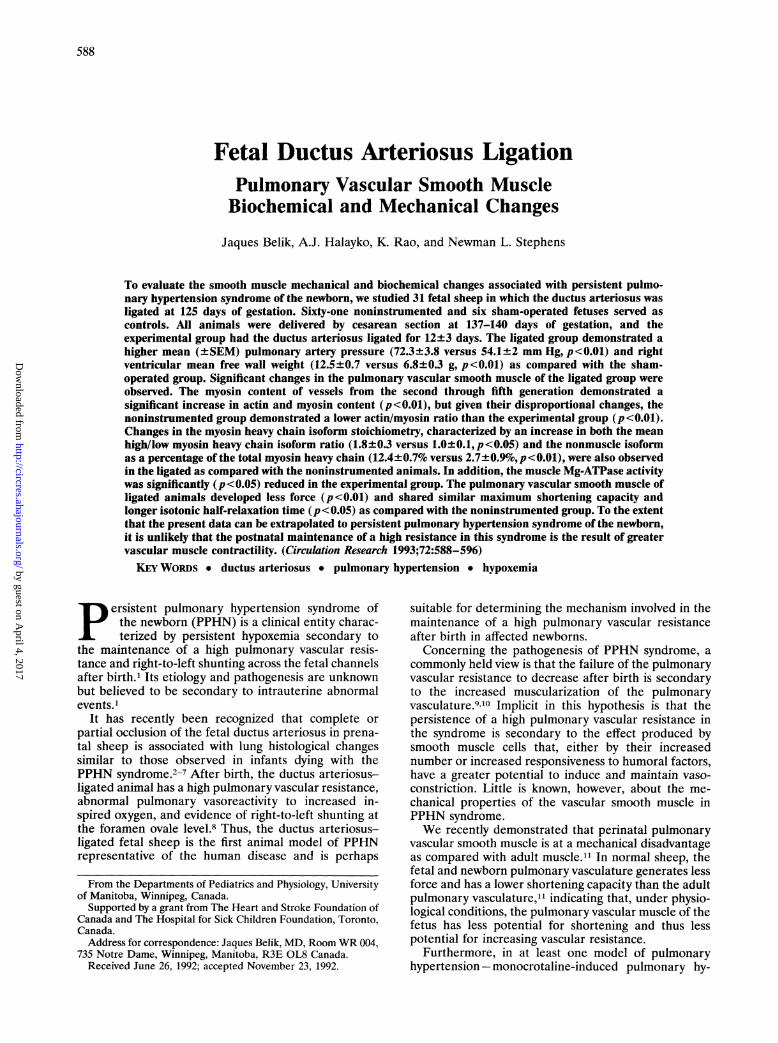
myosin heavy chain isoforms was significantly altered byductus arteriosus ligation (Figure 4). For the secondgeneration vascular tissue, the high/low myosin heavychain isoform ratio was significantly increased in theligated group (p<0.01). A third myosin heavy chainisoform, the nonmuscle fraction, was greatly increasedin the ductus arteriosus-ligated pulmonary vasculartissue, representing up to 12% of the total myosincontent. This represents a greater than fourfold in-crease in this isoform as compared with the noninstru-mented vascular tissue (Table 6).
15 r
COi 10cnW
W.F_.en 5
ELECTRICAL
HIGH K+
* * pcO.O1
0'
CONTROL LIGATEDFIGURE 1. Bar graph showing pulmonary vascular smoothmuscle mechanical stress in response to electrical and highpotassium stimulation in the noninstrumented (control,n=10) and ligated (n=12) groups. **p<0.01 compared withthe corresponding noninstrumented group.
The second generation pulmonary vascular musclemyosin ATPase activity was significantly decreased inthe experimental group (Figure 5), indicating a lowerpotential for myosin phosphorylation. No significantdifference in the wet/dry weight ratio for the secondgeneration vascular strips of the noninstrumented(5.78+0.73, n=10) and ligated (6.05±0.42, n=10)groups was observed.
Newborn DataHemodynamic, blood gas, and pH data were obtained
in one of the two ductus arteriosus-ligated fetuses bornalive. The hemodynamic measurements were obtainedwhile the animal was awake and breathing room air.The results were as follows: systemic arterial pressuresof 79, 56, and 64 mm Hg (systolic, diastolic, and meanpressures, respectively) and pulmonary arterial pres-sures of 79, 45, and 56 mm Hg. The arterial blood gasand pH values while the animal was breathing room airwere as follows: pH 7.25; Pao2, 39.6 mm Hg; Paco2, 46.2mm Hg; and standard bicarbonate, 19.1 mM/l. After 15minutes of 100% oxygen exposure, the results were asfollows: pH 7.24; Pao2, 64 mm Hg; Paco2, 48 mm Hg;and standard bicarbonate, 19 mM/1.
DiscussionDuctus arteriosus ligation in fetal sheep for an aver-
age of 12 days was associated with a sustained increase
TABLE 4. Heart Chamber Weight
Noninstrumented Sham-operated LigatedSite (n=61) (n=6) (n=31)RV free wallWeight (g) 6.8+0.3 7.3+0.6 12.5+0.7*Percent of total heart weight 27.8+0.4 29.9+1.1 34.8+0.6*
LV free wallWeight (g) 7.9+0.4 8.1+0.6 9.2+0.5*Percent of total heart weight 32.3+±0.5 33.0+0.8 25.7+0.5*
Septum (g) 4.4+0.2 4.3+0.5 7.0+0.5*Atria (g) 5.3±+0.2 4.7+0.2 7.2+0.4*
n, Number of sheep; RV, right ventricular; LV, left ventricular. Values are mean+SEM.*p<0.01 compared with the noninstrumented and sham-operated groups.
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

Belik et al Pulmonary Vascular Muscle and Fetal Ductus Arteriosus Ligation 593
TABLE 5. Smooth Muscle Mechanics
Noninstru-mented Ligated(n=10) (n=12)
lo (mm) 4.7+0.5 3.8+0.8Resting tension (mN) 8.4+0.8 6.7±1.2Shortening capacity (percent of lo) 5.9±1.0 5.9±2.0Relaxation half-time (seconds)
Isometric 32.2±4.8 39.1±5.5Isotonic 166.5 ±48.5 516.0±157.6*
n, Number of sheep; 10, optimal length. Values are mean±SEM.*p<0.05 compared with the noninstrumented group.
in pulmonary arterial pressure, decreased right ventric-ular output, and increased total heart and right ventric-ular free wall weight. The myosin heavy chain content ofsecond through fifth generation pulmonary vessels inthe ligated group was increased with an abnormalstoichiometric distribution of its isoforms. The latterwas characterized by a greater proportion of the non-muscle myosin isoform and an increased high/low MHCisoform ratio. In addition, both decreased actin/myosinratio and myofibrillar ATPase activity were observed inthe ductus arteriosus-ligated pulmonary vascular tissue,suggesting a lower potential for crossbridge cycling andmyosin light chain phosphorylation. In keeping withthese changes, the pulmonary vascular muscle in theligated group developed less response to electrical andhigh potassium stimulation and showed prolonged iso-tonic relaxation.
In sheep, we have previously reported that the fetalpulmonary vascular smooth muscle develops less forceand has a lower shortening capacity than do the new-born and adult counterparts.'1 On the basis of theprevious suggestion that the maintenance of a highpulmonary vascular resistance in the PPHN syndrome issecondary to the increased muscularization of the pul-monary vasculature,9'10 an enhanced pulmonary vascu-lar muscle ability to vasoconstrict (greater stress andshortening capacity) was expected. The present datademonstrated that, after ligation of the ductus arterio-
-0- CONTROL
3
Z
C) oZ_ z
;i E 10
-0- LIGATED
** **
T*~**
\TU
O O~~
SECOND THIRD FOURTH FIFTHGENERATION
FIGURE 2. Graph showingpulmonary vascular wall myosincontent for second through fifth generation vessels in thenoninstrumented (control, n=25) and ligated (n=11) groups.**p<0.01 compared with the noninstrumented group.
1.5 r
0
F
zF0
T**
T
1.0 I
0.50.0
CONTROL LIGATEDFIGURE 3. Bar graph showing actin/myosin ratio of com-bined second through fifth generation values for pulmonaryvascular smooth muscle in the noninstrumented (control,n=25) and ligated (n=11) groups. **p<0.01 compared withthe noninstrumented group.
sus, the pulmonary vascular tissue has an even lowerstress in response to electrical and high potassiumstimulation. The shortening capacity was comparable tothe control fetal vascular tissue but still much reducedas compared with newborn and adult sheep vasculartissue." A decrease in smooth muscle force generationin response to pressure overload has also been observedin the rat portal vein25 and grafted saphenous vein.26 Incontrast, the smooth muscle force generation of largeand small resistance systemic arterial vessels is main-tained in response to a sustained increase in arterialpressure in rats with either experimentally induced27 orspontaneous28 hypertension. The reasons for the dis-crepancy in smooth muscle contractility in response topressure load between the veins and arteries is unclear,but the present data suggest that the fetal pulmonaryartery behavior is more in keeping with that of the veins.Nevertheless, the lower pulmonary arterial musclestress observed in the pulmonary hypertensive fetusessuggests that either structural reorganization of thecontractile proteins or changes in the excitation-con-traction coupling are responsible for the altered me-chanical properties of the smooth muscle. Based on thepresent data, the former is the likely mechanism.The smooth muscle cell changes that are presently
described in pulmonary arterial vessels after ductusarteriosus ligation are not unique. Pressure overload "invivo" or vascular stretch "in vitro" is known to inducesmooth muscle hypertrophy, hyperplasia, and an in-crease in extracellular matrix components.29-35 Thesechanges can also be accompanied by smooth muscle cellalterations, but the extent to which pulmonary hyper-tension influences smooth muscle cell differentiation ata given time in gestation in a certain species is presentlyunknown. After portal vein hypertension in rabbits,hypertrophy of the smooth muscle is associated with adisproportionate increase in thin, intermediate, andthick filaments. In this model of hypertension, the portalvein smooth muscle develops an increase in the thin/thick filament ratio and a reduction in force-generatingability.34 In rats, after portal vein hypertension themuscle force-generating ability is increased in propor-tion to the smooth muscle mass, but the maximalshortening velocity is decreased.36 Although the pulmo-
1
p
f
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

594 Circulation Research Vol 72, No 3 March 1993
B C D
NM-MHC
nary vascular muscle shortening velocity was not mea-
sured in our ligated animal group, the lower ATPaseactivity is indicative of abnormalities in this parameterafter pulmonary hypertension.
Together, the decreased pulmonary vascular muscleforce generation and biochemical changes observed inour fetal pulmonary hypertension animals, especiallywith respect to myosin heavy chain, suggest that prena-tal ductus arteriosus ligation induces phenotypic mod-ulation of the smooth muscle. This phenomenon ischaracterized by a change in cell phenotypic expressionof the cell from a contractile to a synthetic form.Synthetic smooth muscle cells predominantly prolifer-ate and produce extracellular matrix components. Insmooth muscle cell culture, recent data indicate that a
change from a contractile to a synthetic phenotype isassociated with an increase in the nonmuscle myosinheavy chain isoform, suggesting that the latter is a
marker for phenotypic modulation. Thus, although we
have not actually measured smooth muscle syntheticfunction, the fourfold increase in content of pulmonaryvascular myosin heavy chain nonmusele isoform, thelower myosin heavy chain ATPase activity, and thedecreased muscle-force generation presently reportedin this model of pulmonary hypertension suggest phe-notypic modulation of vascular smooth muscle.
Phenotypic changes in pulmonary vascular smoothmuscle cells have also been previously reported innewborn animals after chronic hypoxia-induced pulmo-nary hypertension.38,39 The pulmonary vascular smoothmuscle cells in these animals undergo functionalchanges, and a mixed population of phenotypicallydistinct cells is seen in the arterial wall.38 Synthesis ofone or more low molecular weight elastogenic factors
TABLE 6. Myosin Heavy Chain Isoform Stoichionmetry
Noninstrumented Ligated(n=10) (n=10)
MHC1/MHC2 1.0+0.1 1.8+0.3*Nonmuscle myosin(percent of total MHC) 2.7+0.9 12.4+0.7t
n, Number of sheep; MHC1/MHC2, high/low molecular weightmyosin heavy chain (MHC) ratio. Values are mean+SEM.
*p<0.05 and tp<0.01 compared with the noninstrumentedgroup.
MHCQMH"C
FIGURE 4. Representative 4% sodium do-decyl sulfate-polyacrylamide gel electropho-resis of ligated fetal sheep second generationpulmonary arterial tissue is shown in lanes Band C. LanesA andD correspond to Westernblots that identify, respectively, nonmusclemyosin heavy chain (NM-MHC) and highand low molecular weight myosin heavy chainisoforms (MHC1 and MHC2, respectively).
that stimulate the production of elastin in both fibro-blasts and smooth muscle cells have been demonstratedafter chronic hypoxia in the newborn calf.39 This evi-dence strongly suggests that phenotypically altered pul-monary vascular smooth muscle cells participate in theprocess of vascular remodeling characteristically seen inpulmonary hypertension. Also, in children with pulmo-nary hypertensive congenital heart disease, markedchanges in immunostaining for smooth muscle contrac-tile proteins and intermediate filaments precede intimalproliferation,40 suggesting that vascular remodeling is a
late manifestation of increased pressure overload.Among the mechanical properties of muscle studied,
a prolonged isotonic relaxation half-time of the pulmo-nary vascular smooth muscle was observed in the li-gated group. We have previously reported that theisotonic relaxation half-time is significantly increased infetal and newborn pulmonary vascular muscle as com-pared with adult muscle.13Abnormalities of the relax-ation phase of smooth muscle contraction have alreadybeen implicated in the pathogenesis of systemic arterialhypertension.41 45 Since at birth the pulmonary vascularsmooth muscle has to relax to allow for the decrease inlung resistance to blood flow to take place, abnormali-ties of the muscle relaxation phase may also account for
4
3
_ _C)OD
2
c,1
0
h T
*
CONTROL LIGATEDFIGURE 5. Bar graph showing pulmonary vascular smoothmuscle A TPase activity in the noninstrumented (control,n=6) and ligated (n=4) groups. MHC, myosin heavy chain.*p<O.OS compared with the noninstrumented group.
A
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

Belik et al Pulmonary Vascular Muscle and Fetal Ductus Arteriosus Ligation 595
the maintenance of a high vascular resistance in thissheep model of PPHN syndrome. Whether any of thesmooth muscle changes presently described are respon-sible for the prolonged relaxation is unclear. Since themyosin light chain phosphatase is the enzyme responsi-ble for the vascular smooth muscle relaxation phase,46we speculate that differences in quantity and/or distri-bution of this enzyme may account for the observedabnormalities in vascular smooth muscle relaxationpresently reported. Further investigation of the role ofabnormalities in pulmonary vascular muscle relaxationmechanics in this animal model of PPHN syndrome iswarranted.As judged by the increased myosin heavy chain
content of large and medium-sized vessels (secondthrough fifth generation), ductus arteriosus ligation inthe fetal sheep induces increased muscularization notonly of small vessels, as previously described,47 but alsoof larger vessels, such as the ones used for the mechan-ical and biochemical measurements in the presentstudy. In the monocrotaline rat model of pulmonaryhypertension, decreased smooth muscle force genera-tion was observed in small resistance vessels as well asin large elastic arteries,12 suggesting that, whatever isthe cause for the altered muscle mechanics, it affects themuscle mechanical properties of the entire pulmonaryvasculature. Further studies addressing the mechanicalproperties of the smooth muscle mechanics of smallresistance vessels in this model of PPHN are necessarybefore our results can be extrapolated to the humansyndrome.
In summary, we have demonstrated that, in this fetalsheep model of persistent pulmonary hypertension syn-drome, the pulmonary vascular smooth muscle under-goes significant changes in contractile protein content,stoichiometry of myosin heavy chain isoform distribu-tion, and myofibrillar ATPase activity that may accountfor the decrease in muscle force generation and alteredrelaxation properties presently described. The presentnovel data indicate that the maintenance of a postnatalhigh pulmonary vascular resistance in this model of thePPHN syndrome is not due to pulmonary smoothmuscle-enhanced potential for vasoconstriction, as pre-viously proposed, but is possibly the result of abnormal-ities in the muscle relaxation properties and vessel wallgeometric changes.
AcknowledgmentWe are thankful to Mrs. P. MacIntosh for expert secretarial
assistance with this manuscript.
References1. Spitzer AR, Davis J, Clarke WT, Bernbaum J: Pulmonary hyper-
tension and persistent fetal circulation in the newborn. Clin Peri-natol 1988;15:389-413
2. Abman SH, Shanley PF, Accurso FJ: Failure of postnatal adapta-tion of the pulmonary circulation after chronic intrauterine pul-monary hypertension in fetal lambs. J Clin Invest 1989;83:1849-1858
3. Abman SH, Accurso FJ: Acute effects of partial compression ofductus arteriosus on fetal pulmonary circulation. Am J Physiol1989;257:H626-H634
4. Heyman MA, Rudolph AM: Effects of acetylsalicylic acid on theductus arteriosus and circulation in fetal lambs in utero. Circ Res1976;38:418-422
5. Levin DL, Mills U, Parkey M, Garriott J, Campbell W: Constric-tion of the fetal ductus arteriosus after administration of indo-methacin to the pregnant ewe. J Pediatr 1979;94:647-650
6. Levin DL, Mills LJ, Weinberg AG: Hemodynamic, pulmonaryvascular, and myocardial abnormalities secondary to pharmaco-logic constriction of the fetal ductus arteriosus. Circulation 1979;60:360-364
7. Morin FC III, Egan EA: The effect of closing the ductus arteriosuson the pulmonary circulation of the fetal sheep. J Dev Physiol1989;11:283-287
8. Morin FC III: Ligating the ductus arteriosus before birth causespersistent pulmonary hypertension in the newborn lamb. PediatrRes 1989;25:245-250
9. Haworth SG, Reid L: Persistent fetal circulation: Newly recog-nized structural features. J Pediatr 1976;88:614-620
10. Murphy JD, Rabinovitch M, Goldstein JD, Reid LM: The struc-tural basis of persistent pulmonary hypertension of the newborninfant. J Pediatr 1981;98:962-967
11. Belik J, Halayko A, Rao K, Stephens NL: Pulmonary vascularsmooth muscle: Biochemical and mechanical developmentalchanges. JAppl Physiol 1991;71:1129-1135
12. Langleben D, Szarek JL, Cofiesky JT, Jones RC, Reid LM, EvansJN: Altered artery mechanics and structure in monocrotaline pul-monary hypertension. J Appl Physiol 1988;65:2326-2331
13. Belik J, Stephens NL: Developmental differences in vascularsmooth muscle mechanics in pulmonary and systemic circulations.JAppl Physiol (in press)
14. Jiang H, Stephens NL: Isotonic relaxation of sensitized bronchialsmooth muscle. Am J Physicol 1992;262(Lung Cell Mol Physiol 6):L344-L350
15. Levin DL, Rudolph AM, Heymann MA, Phibbs PH: Morpholog-ical development of the pulmonary vascular bed in fetal lambs.Circulation 1976;53:144-151
16. Bradford M: A rapid and sensitive method for the quantification ofmicrogram quantities of protein utilizing the principles of dyebindings. Anal Biochem 1976;72:248-254
17. Cohen DM, Murphy RA: Differences in cellular contractile pro-tein contents among porcine smooth muscles: Evidence for varia-tion in the contractile system. J Gen Physiol 1978;72:369-380
18. Laemmli UK: Cleavage of structural proteins during the assemblyof the head of bacteriophage T4. Nature 1970;227:680-685
19. Sutoh K: Mapping of actin-binding sites of heavy chain of myosinsubfragment. Biochemistry 1983;22:1579-1585
20. Towbin H, Gordon J: Immunoblotting and dot immunoblotting:Current status and outlook. J Immunol Methods 1984;72:313-340
21. Groschel-Stewart U, Rokousky C, Franke R, Peleg I, Kahane I,Eldor A, Muhlrad M: Immunohistochemical studies with antibod-ies to myosins from the cytoplasm and membrane fraction ofhuman blood platelets. Cell Tissue Res 1985;241:399-404
22. Groschel-Stewart U, Chamley JH, McConnell JD, Burstock G:Comparison of the reaction of cultured smooth and cardiac musclecells and fibroblasts to specific antibodies to myosin. Histochemistry1975;43:215-224
23. Kong SK, Halayko AJ, Stephens NL: Increased myosin phosphor-ylation in sensitized canine tracheal smooth muscle. Am J Physiol1990;259(Lung Cell Mol Physiol 3):L53-L56
24. Stephens NL, Halayko AJ, Swynghedauw B: Myosin heavy chainisoform distribution in normal and hypertrophied rat aortic smoothmuscle. Can J Physiol Pharmacol 1990;69:8-14
25. Johansson B: Structural and functional changes in rat portal veinsafter experimental portal hypertension. Acta Physiol Scand 1976;98:381-383
26. Seidel CL, Lewis RM, Bowers R, Bukoski RD, Kim HS, Allen JC,Hartley C: Adaption of canine saphenous veins to grafting: Cor-relation of contractility and contractile protein content. Circ Res1984;55:102-109
27. Arner A, Malmqvist U, Uvelius B: Structural and mechanicaladaptations in rat aorta in response to sustained changes in arterialpressure. Acta Physiol Scand 1984;122:119-126
28. Arner A, Uvelius B: Force-velocity characteristics and active ten-sion in relation to content and orientation of smooth muscle cellsin aortas from normotensive and spontaneously hypertensive rats.Circ Res 1982;50:812-821
29. Hume WR: Proline and thymidine uptake in rabbit ear arterysegments in vitro increased by chronic tangential load. Hyperten-sion 1980;2:738-743
30. LaBourene JI, Coles JG, Johnson DJ, Mehra A, Keeley FW,Rabinovitch M: Alterations in elastin and collagen related to themechanism of progressive pulmonary venous obstruction in a pig-let model. Circ Res 1990;66:438-456
31. Rovner AS, Murphy RA, Owens GK: Expression of smooth muscleand nonmuscle heavy chains in cultured vascular smooth musclecells. J Biol Chem 1986;261:14740-14745
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

596 Circulation Research Vol 72, No 3 March 1993
32. Todorovich-Hunter L, Johnson DJ, Ranger P, Keeley FW, Ra-binovitch M: Altered elastin and collagen synthesis associated withprogressive pulmonary hypertension induced by monocrotaline.Lab Invest 1988;58:184-195
33. Seidel CL, Schildmeyer LA: Vascular smooth muscle adaptation toincreased load. Annu Rev Physiol 1987;49:489-499
34. Berner PF, Somlyo AV, Somlyo AP: Hypertrophy-inducedincrease of intermediate filaments in vascular smooth muscle. J CellBiol 1981;88:96-101
35. Malmqvist U, Arner A: Isoform distribution and tissue content ofcontractile and cytoskeletal proteins in hypertrophied smooth mus-cle from rat portal vein. Circ Res 1990;66:832-845
36. Malmqvist U, Arner A: Contractile properties during developmentof hypertrophy of the smooth muscle in the rat portal vein. ActaPhysiol Scand 1988;133:49-61
37. Seidel C, Kahn A, Collier H, Allen JC, Navran S: Smooth musclecontraction and migration correlate with the type of myosin heavychain isoform expressed. (abstract) FASEB J 1992;614:A1042
38. Stenmark KR, Aldshev AA, Orton EC, Durmowicz AG, BadeschDB, Parks WC, Mecham RP, Voelkel NF, Reeves JT: Cellularadaptation during chronic neonatal hypoxic pulmonary hyperten-sion. Am J Physiol 1991;261:97-104
39. Mecham RP, Whitehouse LA, Wrenn DS, Parks WC, Griffin GL,Senior RM, Crouch EC, Stenmark KR, Voelkel NF: Smooth mus-
cle-mediated connective tissue remodeling in pulmonary hyperten-sion. Science 1987;237:423-426
40. Allen KM, Haworth SG: Cytoskeletal features of immature pul-monary vascular smooth muscle cells: The influence of pulmonaryhypertension on normal development. J Pathol 1989;158:311-317
41. Cohen ML, Berkowitz BH: Decreased vascular relaxation in hyper-tension. J Pharmacol Exp Ther 1976;196:396-406
42. Packer CS, Stephens NL: Mechanics of caudal artery relaxation incontrol and hypertensive rats. Can J Physiol Pharmacol 1985;63:209-213
43. Packer CS, Stephens NL: Mechanics of caudal artery relaxation incontrol and hypertensive rats. Can J Physiol Pharmacol 1985;63:209-213
44. Packer CS, Stephens NL: Prolonged isobaric relaxation time insmall mesenteric arteries of the spontaneously hypertensive rat.Can J Physiol Pharmacol 1987;65:230-235
45. Packer CS, Stephens NL: Tension-velocity relationships in hyper-tensive mesenteric resistance arteries. Can J Physiol Pharmacol1985;63:675-680
46. Murphy RA: Control of the actin-myosin interaction in vascularsmooth muscle. Blood Vessels 1977;14:241-242
47. Wild LM, Nickerson PA, Morin FC III: Ligating the ductus arte-riosus before birth remodels the pulmonary vasculature of thelamb. Pediatr Res 1989;25:251-257
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from

J Belik, A J Halayko, K Rao and N L Stephensmechanical changes.
Fetal ductus arteriosus ligation. Pulmonary vascular smooth muscle biochemical and
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1993 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.72.3.5881993;72:588-596Circ Res.
http://circres.ahajournals.org/content/72/3/588World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Researchin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on April 4, 2017
http://circres.ahajournals.org/D
ownloaded from





























