Embed Size (px)
Citation preview

Femoral Block Provides Superior AnalgesiaCompared With Intra-Articular Ropivacaine AfterAnterior Cruciate Ligament Reconstruction
Henri Iskandar, M.D, Antoine Benard, M.D, Joelle Ruel-Raymond, M.D,Gyslaine Cochard, M.D, and Bertrand Manaud, M.D.
Background and Objectives: Arthroscopic anterior cruciate ligament (ACL) reconstruction of the knee is apainful procedure requiring intensive postoperative pain management. This prospective study investigatesanalgesic quality after a femoral block as compared with intra-articular injection of local anesthetic.
Methods: Eighty patients scheduled for elective ACL repair under general anesthesia were included in ourstudy. Upon completion of surgery, the patients were randomly assigned into 1 of 2 groups: femoral group (n �40) received a femoral block with 20 mL 1% ropivacaine; intra-articular group (n � 40) received 20 mL 1%ropivacaine injected intra-articularly. During the first 24 hours after surgery, all patients received 2 g propac-etamol and 100 mg ketoprofen, intravenously. Additional postoperative analgesia was available with parenteralmorphine if required. Analgesic duration was defined as the time from end of surgery to the first requirementfor a supplemental analgesic. Data collection included patient demographics, visual analog scale (VAS) scores,analgesic duration, and morphine use. Analysis of variance (ANOVA) test was used to compare the 2 groups
Results: VAS score in the recovery room and during rehabilitation was higher in the intra-articular groupthan in the femoral group (P � .001). Morphine use was lower in the femoral group than in the intra-articulargroup (P � .001). Similarly, analgesic duration was longer in the femoral group than the intra-articular group(P � .0001).
Conclusions: Compared with intra-articular injection of local anesthetic, femoral nerve block (FNB) providesbetter analgesia and allows a significant morphine-sparing effect after ACL repair.Reg Anesth Pain Med 2003;28:29-32.
Key Words: Regional anesthesia, ACL repair, Analgesia, Femoral block, intra-articular ropivacaine.
Arthroscopic anterior cruciate ligament (ACL)reconstruction is associated with significant
postoperative pain, with 50% of patients requiringopioid analgesia in the absence of other therapy.1 Itis recognized that adequate postoperative analgesiagreatly facilitates early rehabilitation.2 Effectivepostoperative analgesia has been achieved by usingepidural analgesia and patient-controlled analgesiawith opioids.3 These techniques require expensiveequipment and monitoring and are associated with
side effects, which limit their use. A femoral nerveblock (FNB) after ACL surgery also provides im-proved patient comfort and reduces parenteral nar-cotic administration.4 Postoperative intra-articularanesthetics have been shown to be effective foranalgesia of the knee for knee arthroscopic sur-gery.5 Many investigators suggest that the instilla-tion of local anesthetics into the knee joint at theend of arthroscopic surgery under general anesthe-sia reduces postoperative pain.6,7 Therefore, we de-signed a randomized blinded clinical trial to com-pare pain and opioid consumption after ACLsurgery in patients who received either a FNB or anintra-articular injection of local anesthetic immedi-ately after completion of the surgical procedure.
Materials and Methods
After informed consent and institutional ap-proval, 80 American Society of Anesthesiologists(ASA) physical status I patients scheduled to un-dergo elective ACL reconstruction were prospec-
From the Clinique chirurgicale Bordeaux-Merignac (H.I., J.R-R., G.C., B.M.), Merignac, France; and ISPED, Universite Bor-deaux 2 (A.B.), Bordeaux, France.
Accepted for publication October 25, 2002.Presented in part at the French Society of Anesthesiology
Annual Meeting, Paris, France, 1999.Reprint requests: Henri Iskandar, M.D., Clinique chirurgicale
Bordeaux-Merignac, 9 rue Jean-Moulin, 33700 Merignac,France. E-mail: [email protected]
© 2003 by the American Society of Regional Anesthesia andPain Medicine.
1098-7339/03/2801-0006$35.00/0doi:10.1053/rapm.2003.50019
Regional Anesthesia and Pain Medicine, Vol 28, No 1 (January–February), 2003: pp 29–32 29

tively enrolled in this study. Patients with a historyof allergic reaction to any of the study drugs, prioropioid use, and peripheral neuropathies were ex-cluded.
A standardized anesthetic technique was used forall patients. Premedication consisted of 5 mg oralmidazolam 1 hour before surgery. General anesthe-sia was induced with propofol 3 mg/kg and sufen-tanyl 0.35 �g/kg, and maintained with isofluraneand 50% N2O with O2 via a laryngeal mask airway.All patients subsequently underwent ACL repairusing hamstring tendon (semitendinosus and gra-cilis tendons) autograft through anatomical tibialand femoral tunnels. Surgical technique was iden-tical for all patients. A tourniquet was used in allcases. Upon completion of surgery, patients wererandomized by a computer-generated list into 1 of 2groups: femoral group (n � 40) received a FNBwith 20 mL 1% ropivacaine; intra-articular group(n � 40) received 20 mL 1% ropivacaine injectedintra-articularly.
The FNB was performed at the end of surgeryusing Winnie’s landmarks with a 24-gauge, 25-mmneedle (Stimuplex D, Braun, Germany) connectedto a nerve stimulator (Stimuplex, Braun) by a ster-ile cable. The femoral nerve was localized by amotor response (movement of the patella) obtainedat � 0.5 mA. The effectiveness of FNB was con-firmed by the criterion of decreased anterior thighsensation. The intra-articular instillation was per-formed by the surgeon at the end of surgery, 10minutes before tourniquet release.
Nurses and physical therapists, who were un-aware of study group and assignments, used thevisual analog scale (VAS) to rate postoperative painat rest and during passive mobilization (0 � no painand 100 � the worst imaginable pain). Assessmentswere performed in the postanesthesia care unit(PACU) and at 4, 8, 12, and 24 hours after surgery,at rest, and during early mobilization (initiated 6hours after surgery).
The postoperative analgesia protocol was initi-ated in the PACU and continued on the surgicalward. Analgesia in the PACU was provided by mor-phine titration in increments of 2 mg every 5 min-utes until VAS scores � 30 mm were obtained. Apatient-controlled analgesia (PCA) pump (Alaris,Bordeaux, France) was then connected, deliveringa bolus of 1 mg of morphine, with 5-minute lockoutperiod, and no limit or background infusion.
Side effects attributed to morphine included re-spiratory depression (rate � 10 breaths/minute),sedation (awakening or not awakening, in responseto painful stimulation), or nausea or vomiting re-quiring treatment.
During the 24 hours after surgery, all patientsreceived 2 g propacetamol and 100 mg ketoprofen,
infused intravenously at 8-hour intervals. Analgesicduration was defined as the time from end of sur-gery to first requirement of morphine.
Data collection included patient demographics,VAS scores, analgesic duration, and morphine use.Data analysis was performed using STATA version7.0 (STATA, College Station, TX) and SAS Software,version 6.12 (Allison, 1995). We defined VAS scoreat t0, morphine intake and analgesic duration asprincipal outcomes. All variables had a normal dis-tribution except postoperative analgesia duration;Kaplan-Meier estimate was used to present thisdata. ANOVA test was used to compare the 2 groupsaccording to the VAS scores at t4, t12, and t24. Wefound unequal variance between the 2 groups forVAS scores at t0, t8, and for morphine use. Thus,we used ANOVA test modified for heteroskedastic-ity (Welch’s ANOVA) to compare the 2 groups ac-cording to these variables.8 For these tests, a Pvalue � .05 was considered to be statistically signif-icant. For the comparison of VAS score at t0 andmorphine intake between groups, we used t testmodified for heteroskedasticity. For these tests, us-ing Bonferroni correction, a P value � .017 wasconsidered to be statistically significant. Two-sidedsignificance tests were used throughout.
Results
Patient Population
There were no significant differences between thetreatment groups with respect to age, sex, weight, orduration of surgery (P � .05, Table 1). No patient wasexcluded from the study. By the criterion of decreasedanterior thigh sensation, nerve block was successfullyachieved in all patients in the femoral group. Therewere no adverse effects linked to the FNB or intra-articular injection of ropivacaine.
Postoperative Pain
The VAS pain scores were significantly lower inthe femoral group than in the intra-articular groupduring PACU stay (P � .001) and during rehabili-
Table 1. Patient Demographics and Surgical Data
CharacteristicsFemoralGroup
Intra-articularGroup
Age (yr) mean � SD 26.8 � 8.4 28.3 � 7.8Weight (kg) mean �SD
70.0 � 12.4 71.6 � 11.6
Sufenta (�g) mean �SD
25.0 � 1.6 24.5 � 3.0
Surgery Duration (min)mean � SD
48.4 � 3.8 46.2 � 2.2
Male, n (%) 28 (70) 31 (77.5)
NOTE. No statistically significant differences were observedbetween the groups.
30 Regional Anesthesia and Pain Medicine Vol. 28 No. 1 January–February 2003
tation (P � .001). No significant difference wasobserved among the groups for VAS scores (Table2).
Morphine Use
The total morphine use over the entire postoper-ative period was significantly higher in the intra-articular group than in the femoral group (Table 2).
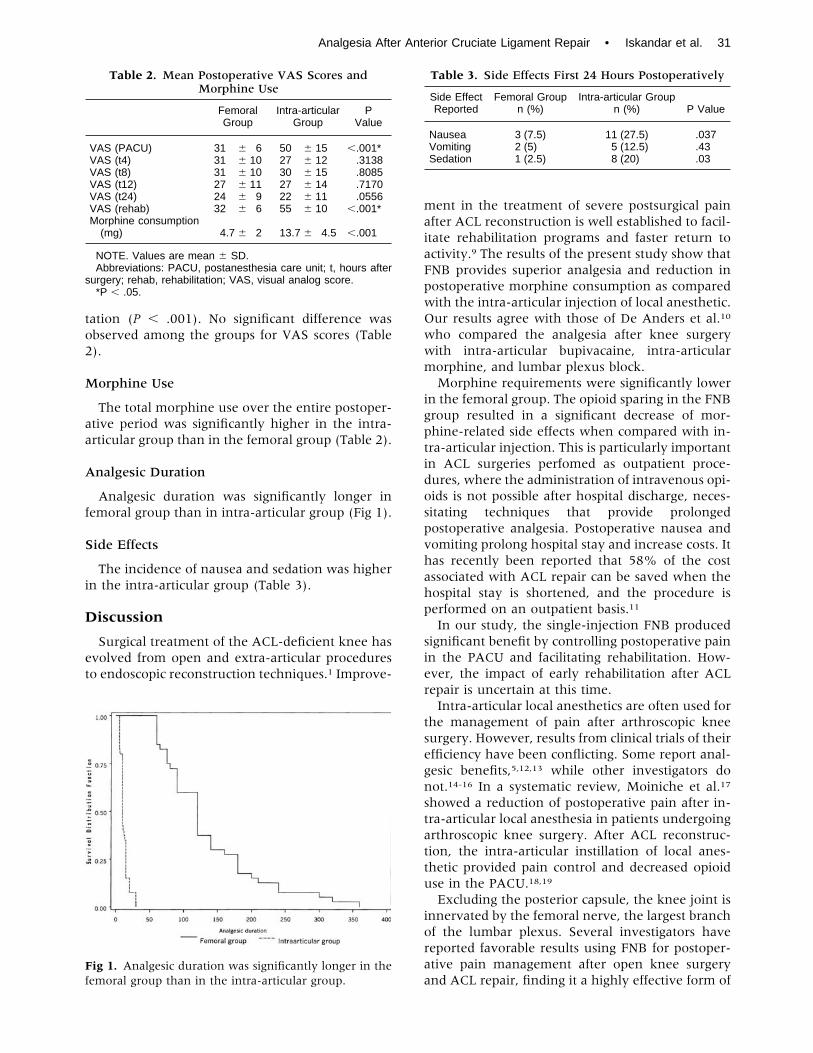
Analgesic Duration
Analgesic duration was significantly longer infemoral group than in intra-articular group (Fig 1).
Side Effects
The incidence of nausea and sedation was higherin the intra-articular group (Table 3).
Discussion
Surgical treatment of the ACL-deficient knee hasevolved from open and extra-articular proceduresto endoscopic reconstruction techniques.1 Improve-
ment in the treatment of severe postsurgical painafter ACL reconstruction is well established to facil-itate rehabilitation programs and faster return toactivity.9 The results of the present study show thatFNB provides superior analgesia and reduction inpostoperative morphine consumption as comparedwith the intra-articular injection of local anesthetic.Our results agree with those of De Anders et al.10
who compared the analgesia after knee surgerywith intra-articular bupivacaine, intra-articularmorphine, and lumbar plexus block.
Morphine requirements were significantly lowerin the femoral group. The opioid sparing in the FNBgroup resulted in a significant decrease of mor-phine-related side effects when compared with in-tra-articular injection. This is particularly importantin ACL surgeries perfomed as outpatient proce-dures, where the administration of intravenous opi-oids is not possible after hospital discharge, neces-sitating techniques that provide prolongedpostoperative analgesia. Postoperative nausea andvomiting prolong hospital stay and increase costs. Ithas recently been reported that 58% of the costassociated with ACL repair can be saved when thehospital stay is shortened, and the procedure isperformed on an outpatient basis.11
In our study, the single-injection FNB producedsignificant benefit by controlling postoperative painin the PACU and facilitating rehabilitation. How-ever, the impact of early rehabilitation after ACLrepair is uncertain at this time.
Intra-articular local anesthetics are often used forthe management of pain after arthroscopic kneesurgery. However, results from clinical trials of theirefficiency have been conflicting. Some report anal-gesic benefits,5,12,13 while other investigators donot.14-16 In a systematic review, Moiniche et al.17
showed a reduction of postoperative pain after in-tra-articular local anesthesia in patients undergoingarthroscopic knee surgery. After ACL reconstruc-tion, the intra-articular instillation of local anes-thetic provided pain control and decreased opioiduse in the PACU.18,19
Excluding the posterior capsule, the knee joint isinnervated by the femoral nerve, the largest branchof the lumbar plexus. Several investigators havereported favorable results using FNB for postoper-ative pain management after open knee surgeryand ACL repair, finding it a highly effective form of
Table 2. Mean Postoperative VAS Scores andMorphine Use
FemoralGroup
Intra-articularGroup
PValue
VAS (PACU) 31 � 6 50 � 15 �.001*VAS (t4) 31 � 10 27 � 12 .3138VAS (t8) 31 � 10 30 � 15 .8085VAS (t12) 27 � 11 27 � 14 .7170VAS (t24) 24 � 9 22 � 11 .0556VAS (rehab) 32 � 6 55 � 10 �.001*Morphine consumption(mg) 4.7 � 2 13.7 � 4.5 �.001
NOTE. Values are mean � SD.Abbreviations: PACU, postanesthesia care unit; t, hours after
surgery; rehab, rehabilitation; VAS, visual analog score.*P � .05.
Fig 1. Analgesic duration was significantly longer in thefemoral group than in the intra-articular group.
Table 3. Side Effects First 24 Hours Postoperatively
Side EffectReported
Femoral Groupn (%)
Intra-articular Groupn (%) P Value
Nausea 3 (7.5) 11 (27.5) .037Vomiting 2 (5) 5 (12.5) .43Sedation 1 (2.5) 8 (20) .03
Analgesia After Anterior Cruciate Ligament Repair • Iskandar et al. 31

analgesia with an excellent degree of patient satis-faction.20,21 When compared with nonsteroidal an-ti-inflammatory drugs and PCA opioids, FNB pro-vides a superior analgesic effect for patientsundergoing ACL reconstruction.22,23 In contrast tothese positive results and to our findings, Schwarzet al.24 found no effect on postoperative analgesicconsumption, as compared with intra-articular in-stillation with ropivacaine alone, in patients under-going ACL reconstruction. However, those investi-gators used a more dilute solution of ropivacaine(0.2%) for the femoral block. Recently, Frost et al.25
showed a significant reduction in pain on the nightof surgery after ACL hamstring reconstruction inpatients who received a femoral block.
One limitation of our study should be noted. Therecording of pain scores and analgesic consumptionwas limited in the first 24 hours. Nevertheless, datahave shown the ACL reconstruction continues to bepainful for the first 24 postoperative hours.1,4,9
In summary, we found that FNB with 20 mL 1%ropivacaine provided superior analgesia as com-pared with intra-articular ropivacaine for the first24 hours after ACL reconstruction.
References
1. William JS, Wexler G, Novak PJ. A prospective studyof pain and analgesic use in outpatient endoscopicanterior cruciate ligament reconstruction. Arthroscopy1998;14:613-616.
2. Anderson AF, Lipscomb AB. Analysis of rehabilita-tion techniques after anterior cruciate reconstruc-tion. Am J Sports Med 1989;17:154-160.
3. Lopper KA, Ready LB. Epidural morphine after an-terior cruciate ligament repair: A comparison withpatient-controlled intravenous morphine. AnesthAnalg 1989;68:350-352.
4. Edkin BS, Spindler KP, Flanagan JF. Femoral nerveblock as an alternative to parental narcotics for paincontrol after anterior cruciate ligament reconstruc-tion. Arthroscopy 1995;11:404-409.
5. Chirwa SS, Mac Leod BA. Intraarticular bupivacaineafter arthroscopic meniscectomy. A randomised dou-ble-blind controlled study. Arthroscopy 1989;5:33-35.
6. Henderson RC, Campion ER, De Masi RA. Postar-throscopy analgesia with bupivacaine. Am J SporstMed 1990; 18:614-617.
7. Milligan DA, Mowbray MJ, Mulrooney L. Intra-ar-ticular bupivacaine for pain relief after arthroscopicsurgery of the knee joint in day-case patients. Anes-thesia 1988;43:563-564.
8. Skovlund E, Fenstad GU. Should we always choose anonparametric test when comparing two apparently nonnormal distribution. J Clin Epidemiol 2001;54:86-92.
9. Cohn BT, Draeger RI, Jackson DW. The effects of coldtherapy in the postoperative management of pain inpatients undergoing cruciate ligament reconstruc-tion. Am J Sports Med 1987;17:344-349.
10. De Anders J, Bellver J. A comparative study of anal-
gesia after knee surgery with intraarticular bupiva-caine, intraarticular morphine and lumbar plexusblock. Anesth Analg 1993;77:727-730.
11. Kao JT, Giagarra CE, Singer G. A comparison ofoutpatient and inpatient anterior cruciate ligamentreconstruction surgery. Arthroscopy 1995;11:151-156.
12. Ruwe PA, Klein I. The effect of intraarticular injec-tion of morphine and bupivacaine on postarthro-scopic pain control. Am J Sporst Med 1995;23:59-64.
13. Reuben SS, Sklar J, El-Mansouri M. The preemptiveanalgesic effect of intraarticular bupivacaine andmorphine after ambulatory arthroscopic knee sur-gery. Anesth Analg 2001;92:923-926.
14. Aesbo V, Raeder JC, Grogaard B. No additional an-algesic effect of intraarticular morphine or bupiva-caine compared with placebo after elective knee ar-throscopy. Acta Anaesthesiol Scand 1996;40:585-588.
15. Cepeda MS, Uribe C. Pain relief after arthroscopy:Intraarticular morphine, intraarticular bupivacaine,or subcutaneous morphine? Reg Anesth Pain Med1997;22:233-238.
16. Rautoma P, Santanen U. Diclofenac premedicationbut not intraarticular ropivacaine alleviates pain fol-lowing day-case knee arthroscopy. Can J Anaesth2000;47:220-224.
17. Moiniche S, Mikkelsen S, Wetterslev J. A systematicreview of intraarticular local anesthesia for postoper-ative pain relief after arthroscopic knee surgery. RegAnesth Pain Med 1999;24:430-437.
18. Tetzlaff JE, Dilger JA. Preoperative intraarticularmorphine and bupivacaine for pain control after out-patient arthroscopic cruciate ligament reconstruc-tion. Reg Anesth Pain Med 1999;24:220-224.
19. Butterfield NN, Schwarz SK. Combined pre-and post-surgical bupivacaine wound infiltrations decreaseopioid requirements after knee ligament reconstruc-tion. Can J Anaesth 2001;48:245-250.
20. Edkin BS, McCarty EC. Analgesia with femoral nerveblock for anterior cruciate ligament reconstruction.Clin Orthop 1999;369:289-295.
21. Mulroy MF, Larkin KL, Manbir S. Femoral nerveblock with 0.25% or 0.5% bupivacaine improvespostoperative analgesia following outpatient arthro-scopic cruciate ligament repair. Reg Anesth Pain Med2001;26:24-29.
22. Peng P, Claxton A, Chung F. Femoral nerve blockand ketorolac in patients undergoing anterior cruci-ate ligament reconstruction. Can J Anaesth 1999;46:919-924.
23. Matheny LM, Hanks G. A comparison of patient-controlled analgesia and continuous lumbar plexusblock after anterior cruciate ligament reconstruction.Arthroscopy 1993;9:87-90.
24. Schwarz S, Franciosi L. Addition of femoral 3-in-1blockade to intraarticular ropivacaine 0.2% does notreduce analgesic requirements following arthro-scopic knee surgery. Can J Anaesth 1999;64:741-747.
25. Frost S, Grossfeld S. The efficacy of femoral nerveblock in pain reduction for outpatient hamstring an-terior cruciate ligament reconstruction: A double-blind, prospective, randomised trial. Arthroscopy2000;16:243-248.
32 Regional Anesthesia and Pain Medicine Vol. 28 No. 1 January–February 2003




























