Embed Size (px)
Citation preview

British Joumal of Plastic Surgery (1988),41, 15&l 53 0 1988 The Trustees of British Association of Plastic Surgeons
Fasciocutaneous flaps for burn reconstruction: a report of 57 flaps
A. H. N. ROBERTS and W. A. DICKSON
Departments of Plastic Surgery, Stoke Mandeville Hospital, Aylesbury and St Luke’s Hospital, Bradford
Summary-We have used 57 fasciocutaneousflaps in 24 patients to correct burn contractures. There were six complications, four of which healed with dressings alone. The flaps were used either locally (22 patients) or as a cross-leg flap (2 patients). The local flaps have clearly shown that grafted areas can be raised as flaps provided that the fascia is included in the flap, and that the flap can also be based distally.
Fasciocutaneousflaps have several advantages over the technique of cross-cutting the contracture, followed by split skin grafting. Firstly, there is no skin graft, which may result in further contracture. Secondly, if a patient does not have a skin graft on the secondary defect (83% in this series), the patient has the advantage of a shorter hospital stay.
The techniques of the design and raising of fasciocutaneous flaps for burn reconstruction are discussed.
The standard method of correcting burn contrac- tures running across the flexor surfaces of joints, or of hollows in the body surface, is to cross-cut the scar tissue down to underlying normal tissue and to fill the defect created with a split skin graft. This method has several disadvantages :
1.
2.
3.
4.
5.
6.
The grafted area can recontract. Although the amount can be reduced by the use of a thick skin graft, this may lower the percentage take of the graft. Some surgeons attempt to put in an excess of skin so that any further recontracture will take up this skin. This can leave an ugly wrinkled area of graft. Part of the split skin graft can fail to take, which may result in further surgery or repeated dress- ings, leading to a delay in healing. A greater extent of contracture can then occur. In the case of severe burns, there may be an absence of suitable donor sites to yield a good single sheet of skin graft. Pocket formation may occur at both ends of the incision. These can be unattractive and difficult to keep clean. This complication can be reduced by fish-tailing the ends of the incision. A long hospital stay is involved so that the graft may have the best chance of taking and for the donor area to heal. The skin graft donor area is painful. This is a very major problem for patients who need
7.
multiple readmissions for contractures in differ- ent parts of the body. Long-term splinting, often used to reduce graft contracture, can be cumbersome, need frequent checking and readjustment, and may be expen- sive.
Scars from other causes around the body may often be corrected by local rearrangements of the skin. However, in burns this is often not possible because of the wide area of scarring that had occurred and it is the experience of most burns surgeons that attempts to raise the local grafted skin as a Z-plasty or other local rearrangement almost invariably leads to necrosis of part or all of the tissue raised. This is probably due to destruction of the subdermal plexus of blood vessels at the time of the burn or during treatment, and may not occur after tangential excision.
Since their introduction by PontCn (1981) fascio- cutaneous flaps have been used on legs, arms and trunk; they would appear to be possible in most parts of the body except around the malleoli of the ankle (Dickson et al., 1987). Tolhurst and Haeseker (1982) reported 15 fasciocutaneous flaps used to correct contractures of the axilla, but these were usually raised in normal skin. They noted that the two flaps that contained previously grafted skin (10% and 50% of the respective flaps) had no necrosis of the grafted areas.
150

FASCIOCUTANEOUS FLAPS FOR BURN RECONSTRUCTION : A REPORT OF 57 FLAPS 151
Method
The lines of contracture are marked on the patient preoperatively when the tight bands that are reducing function can be most easily demonstrated.
The flap or flaps are designed along the lines of contracture. Wherever possible, the flap should be in an area where there is low tension in the tissue at right angles to its axis so that the secondary defect can be closed directly. Multiple small flaps are to be preferred to one larger flap, and where possible the angle of transposition should be not greater than 90” as this will reduce both the stress on the flap and the final dog-ear. The length-to- width ratio of the flap can be three-to-one or less.
The defect is created by dissection through the scar to underlying normal tissue. The technique of raising the flap is important; a lateral incision is made first, and the fascia defined. The other lateral incision is then made and dissection deep to the fascia beneath the flap joins the two lateral incisions before the tip is released. Tacking sutures may be applied to prevent the fascia stripping from the rear of the flap. It is important that the base of the flap is sufficiently undermined to allow easy trans-
position. It is then sutured into position with two layers of sutures, the deep layer attaching the fascia to the surrounding tissue. The secondary defect is closed directly, if this is possible, or a split skin graft may need to be applied.
Results
In this group of 24 patients, 57 flaps were raised (average of 2.5 flaps per patient). The anatomical distribution of the flaps is shown in Table 1 and the complications are listed in Table 2. All the remaining flaps healed perfectly and, with two exceptions, gave good release of the contracture. Of the flaps with initial complications, one flap
Table 1 Anatomical sites of 57 fasciocutaneous flaps.
Axilla 15 Upper limb 29 Neck 9 Other sites 4
_
Total 51
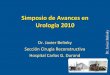
Fig. 1
Figure lPContracture of the axilla (A) preoperative (B) postoperative.

152 BRITISH JOURNAL OF PLASTIC SURGERY
Table 2 Complications of fasciocutaneous flaps used for the releases of burn contractures.
Distal necrosis 3 Incomplete release 2 Sepsis 1 Thinning required 1 Muscle hernia 1
Total 8
with distal necrosis required a secondary skin graft on the underlying fascia which had survived. The secondary defect closed directly in 83% of the flaps.
During a follow-up period of 27.5 months (range 40-54 months), two patients required further surgery to previously operated areas. One patient
has had a further flap to give adequate correction and one patient had the flap thinned. Typical examples of the results obtained are shown in Figures 1 to 3.
Discussion
Local tissue rearrangement to relieve contractures overcomes the major disdadvantages of cross- cutting and split skin grafting. In particular, further contractures do not occur, hospital in-patient time is markedly reduced, and there is less pain for the patient who does not have a donor site. This latter feature is particularly important in burned patients as many of them are children who may need release of contractures over many years. Several patients
Fig. 2
Figure 2-Contracture of the neck (A) preoperative (B) postoperative.

FASCIOCUTANEOUS FLAPS FOR BURN RECONSTRUCTION : A REPORT OF 57 FLAPS 153
Fig. 3
Figure 3 --Contracture of the forearm (A) preoperative (B) postoperative
who had previously had contracture release and References grafting have expressed their gratitude for the reduction of pain with this technique.
Dickson, W. A., Dickson, M. G. and Roberts, A. H. N. (1987).
The success of the procedure is dependent on The complications of fasciocutaneous flaps. Annals r$P/astic Surgery (in press).
careful design and maintaining the fascia on the Pontkn, B. (1981). The fasciocutaneous flap: its use in soft tissue
flap during dissection. It is easy to dissect in the defects of the lower leg. British Journal of Plastic Surgery. 34. . .
correct layer On the limbs where the fascia ls a veq 215.
definite layer, but can be more difficult on the trunk Tolhurst, D. E. and Haeseker, B. (1982). Fasciocutaneous flaps
and particularly in the axilla. in the axillary region. British Journal qf Plastic Surgery. 35. 430.
Acknowledgements The Authors
A. H. N. Roberts, MA, BSc, BM, BCh, FRCS. Consultant Plastic
We would particularly like to thank Mr T. L. Barclay, Emeritus Surgeon, Stoke Mandeville Hospital. Aylesbury, Bucking-
Consultant Plastic Surgeon, St Luke’s Hospital, Bradford, who hamshire HP21 8AL.
extended the use of the fasciocutaneous flap to include previously W. A. Dickson, BSc, MB, ChB, FRCSG, Registrar in Plastic
grafted skin. Most of the patients studied in this paper were his, Surgery, St Luke’s Hospital, Bradford, West Yorkshire.
as was much of the surgery. We would also like to thank Mr D. J. Crockett whose patients are included in this series. We are
Requests for reprints to Mr A. H. N. Roberts
grateful to the Photographic Department at St Luke’s Hospital, Bradford, and to Miss C. M. McCree for typing the paper.
Paper received 5 May 1987. Accepted 10 June 1987.