Embed Size (px)
Citation preview

Breast Cancer Research and Treatment 78: 7–15, 2003.© 2003 Kluwer Academic Publishers. Printed in the Netherlands.
Report
Family history of breast and ovarian cancer and the riskof breast carcinoma in situ�
Elizabeth B. Claus1, Meredith Stowe1, and Darryl Carter2
1Department of Epidemiology and Public Health, 2Department of Pathology, Yale University School of Medicine,New Haven, CT, USA
Key words: breast carcinoma in situ, DCIS, epidemiology, family history, LCIS
Summary
A family history of breast cancer is an important risk factor for breast carcinoma in situ (BCIS), however, thereare no detailed analyses of its variation in effect by number, type, laterality or age at onset of affected relativesnor by association with ovarian cancer. In addition, the role of the breast cancer susceptibility genes, BRCA1 andBRCA2, in the development of BCIS is unclear.
Objective. To better define the role of: (1) a family history of breast and ovarian cancer and (2) the cancersusceptibility genes, BRCA1 and BRCA2, in the development of BCIS.
Methods. The data are 875 ductal carcinoma in situ (DCIS) and 123 lobular carcinoma in situ (LCIS) casesdiagnosed among residents of the state of Connecticut from September 15, 1994 to March 14, 1998 and betweenthe age of 20 and 79 years. Controls (n = 999) are female Connecticut residents collected via random-digit-dialand frequency matched to the cases by 5-year age intervals. Telephone interviews were used to collect informationon risk factors and cancer screening history.
Logistic regression was used to provide maximum likelihood estimates of the odds ratios (OR) with 95%confidence intervals (95% CI). The probability of being a BRCA1 and/or BRCA2 gene carrier was calculatedfor each case and control, using family history of breast and ovarian cancer, age/age at diagnosis for relatives,prevalence and penetrance data for BRCA1/BRCA2, and self-report of Jewish heritage.
Results. Cases with DCIS or LCIS were significantly more likely to report a first degree family history of breastcancer (OR: 1.6, 95% CI: 1.3, 2.1 and 1.8, 95% CI: 1.2, 2.9, respectively) than were controls. In addition, DCIScases were 2.4 (95% CI: 0.8, 7.2) times more likely than controls to report both an affected mother and sister.An inverse association was suggested between age at onset and DCIS risk with cases aged 49 years or younger at2.1 (95% CI: 1.3, 3.4) times the risk of controls (95% CI) versus 1.5 (95% CI: 1.1, 2.0) for cases older than 49years. An elevated risk of DCIS was associated with a family history of ovarian cancer but did not reach statisticalsignificance (OR: 1.3, 95% CI: 0.7, 2.5). Approximately 3.7% and 1.9% of DCIS cases were predicted to carry amutation in BRCA1 and BRCA2, respectively.
Conclusions. A family history of breast cancer is associated with an increased risk of DCIS and LCIS, particu-larly among women with multiple relatives affected at early ages. Statistical risk models predict a low prevalencerate of BRCA1 and BRCA2 in DCIS; these estimates await confirmation through laboratory testing.
Introduction
The association between a family history of breastcancer and invasive breast cancer (IBC) is well es-
�This work was supported by the US Army Medical Researchand Material Command under DAMD-17-95-1-5006 and by NIHR01-CA81393.
tablished [1–9] and there is compelling evidence tosuggest that a similar association exists for breast car-cinoma in situ (BCIS) [10–17]. In general, a familyhistory of breast cancer has been associated with a twoto threefold increase in the risk of IBC [1–9]. Resultsfrom BCIS studies report a similarly increased riskwith odds ratios (OR) ranging from 1.5 to 2.7 [10–17].

8 EB Claus et al.
In more detailed analyses of family history in studiesof IBC, researchers have found that individuals withmultiple first degree family members diagnosed withovarian cancer or breast cancer, particularly at youngages, are at even greater risk. Examination of suchfamilies with multiple members affected with earlyonset breast cancer as well as with ovarian cancer hasled to the identification of several breast cancer sus-ceptibility alleles (BRCA1, BRCA2) [18, 19]. Theresults from studies of invasive disease coupled withthe observed increased risk of BCIS associated witha family history of breast cancer suggest that furtheranalyses of BCIS risk by type, number, age at onset,and disease laterality of affected relatives are neces-sary to determine whether a similar genetic mechan-ism may play a role in BCIS risk. To our knowledgeno existing study includes information on breast can-cer history on any relative other than a mother and/orsister(s). In addition, no published data exist whichincorporate information on the age at onset or lateral-ity of any relatives affected with breast cancer nor anyinformation on ovarian cancer among any relatives inthe calculation of BCIS risk. The data presented heretherefore represent the first large, population-basedeffort to examine in detail the association between afamily history of either breast or ovarian cancer and adiagnosis of BCIS across the full spectrum of age andhistologic subtype, while incorporating data on cancerscreening history.
Methods
The study population includes all cases of femaleBCIS diagnosed among residents of the state of Con-necticut from September 15, 1994 to March 14, 1998as well as a series of age-matched controls. Caseswere identified through the Rapid Case Ascertainment(RCA) Shared Resource of the Yale Cancer Centeras well as the Connecticut Tumor Registry locatedin the Connecticut Department of Public Health andwere between the ages of 20 and 79 years at the timeof diagnosis. Controls were female Connecticut res-idents selected by random-digit-dialing methods byan outside consulting firm (Northeast Research) andwere frequency matched by 5-year age intervals to thecases. Study subjects with a previous history of breastcancer and/or a breast biopsy of unknown outcomewere excluded. The study, consent forms and ques-tionnaire were approved by the Yale University Schoolof Medicine, Human Investigation Committee as well
as by the Connecticut Department of Public Health,Human Investigation Committee.
The physicians of each eligible case were contac-ted to request permission to approach the case. Casesapproved for contact by their physicians and controlsidentified by Northeast Research were sent a letter ofintroduction. Approximately 1–2 weeks later a trainedinterviewer contacted the potential study subject bytelephone to administer the interview. Intervieweeswere sent an oral contraceptive picture booklet de-veloped for the Harvard University Nurses’ HealthStudy [20] to allow them to review products usedin the past. Subjects were interviewed for an aver-age of 43 min. The questionnaire included detailedquestions on family history of cancer, pregnancy andmenstrual history, exogenous hormone history, demo-graphics, medical and screening history, and smokingand alcohol consumption.
Over the study period, 1606 cases and 1445 con-trols were identified. Two hundred and forty-onecases were ineligible due to out-of-state residency(8), language (21), a history of previous breast can-cer/biopsy of unknown outcome (181) or age-group(31). Ninety-one percent of eligible cases had a con-senting physician. Among cases with a consentingphysician, 83% participated in the interview portionof the study. Seventy-four controls were ineligible dueto out-of-state residency (3), language (18), a historyof previous breast cancer/biopsy of unknown outcome(51), or age-group (2). Among controls, the initialhousehold screening response rate when approachedby Northeast Research was 85.7%. These women werethen contacted by our study; 81% agreed to be inter-viewed. The final sample included 1068 case and 999control subjects, with overall response rates of 76%and 70% for cases and controls, respectively.
Cases were defined as in situ, either ductal (DCIS)(n = 875) or lobular (LCIS) (n = 123), if they werenon-infiltrating. All cases were initially identified bypathology report and confirmed via a uniform reviewby the study pathologist (D.C.). Cases with mixed orother pathology (i.e. both DCIS and LCIS, invasive,or no identifiable disease) (n = 70) were not includedin any analyses. Risk factor and screening informationwas truncated at the date of diagnosis for cases andthe date of interview for controls (hereafter referred toas the reference date). Data on screening variables in-cluded information on routine checkups, breast examsby a physician, breast self-exam (BSE), pap smears,and mammograms. For each of the screening methods,respondents were asked to provide their age at first

Family history of breast and ovarian cancer 9
screen. In an effort to determine the ‘usual’ screeningbehavior of study subjects, respondents were asked toprovide information on the date of most recent screenas well as the frequency of each screen in the timeperiod 1 year prior to the reference date. This in-formation was used to construct two mammographyscreening variables: (1) the existence of at least onemammogram in the 5-year period 1 year prior to thereference date and (2) the number of mammogramsin the 5-year period 1 year prior to the reference date(coded as 0, 1, or 2+).
With respect to family history, study subjects wereasked to provide the type, age at onset, and laterality(as appropriate) of up to three cancers for all male andfemale first degree (mother, father, sisters, brothers,daughters, and sons) and second degree relatives (ma-ternal and paternal grandmothers and grandfathers, aswell as aunts and uncles). In addition, the current ageor age at death was also obtained for all relatives.
Statistical analysis
The initial portion of the statistical analysis includeddescriptive statistics. t-Tests and chi-square tests wereused to examine the association between the riskof BCIS and independent covariates. To assess therelative risk of BCIS associated with risk factors,conditional logistic regression was used to providemaximum likelihood estimates of the OR (adjust-ed and unadjusted) with 95% confidence intervals(CI) using the statistical package PC-SAS version8.0 [21]. Relative risk estimates are adjusted for ageand, to control for the possible effect of confoundingassociated with cancer screening history, mammog-raphic history (categorized as having had at least onemammogram in the 5-year period 1 year prior tothe reference date). Additional adjustment for otherbreast cancer screening methods did not significantlyalter the risk estimates (primarily due to correlationbetween the screening variables) and hence were notincluded in the final model.
The probability of carrying a mutation in BRCA1or BRCA2 or both is calculated for each case andcontrol (i.e., proband) using BRCAPRO [22]. The pro-gram employs a model which uses Bayes theorem andMendelian genetics and assumes an autosomal dom-inant transmission for both BRCA1 and BRCA2 [23,24]. In each instance, a woman’s probability of be-ing a gene carrier is calculated conditional upon thebreast and ovarian cancer status of her first and seconddegree female relatives and the age at onset of any
affected female relatives as well as the current age/ageat death of any unaffected female relatives. The cal-culation of carrier probability also takes into accountwhether or not the proband was herself affected andwhether she identified herself as Jewish in the ques-tionnaire. The model uses BRCA1/BRCA2 prevalenceestimates from Ford et al. [25] as well as penetranceestimates from Easton et al. [26] for women who didnot identify themselves as Jewish and from Struewinget al. [27] for women who did identify themselves asJewish [27].
To estimate the proportion of cases and controlswho would be predicted to carry mutations in BRCA1,BRCA2 or either, study subjects were divided into twogroups (carrier or non-carrier) by carrier probability,using 0.10 as the cut-point, based on guidelines sug-gested by the American Society of Clinical Oncologyfor BRCA1 testing [28, 29].
Standardized incidence ratios (SIR) and 95% CIwere calculated for breast and ovarian cancer. In eachinstance, the number of affected mothers and sis-ters reported by controls was compared to the age-and site-specific incidences from the 1993 to 1997surveillance, epidemiology, and end results (SEER)centers.
Results
The general makeup of the case and control subjectsmatched well to that of the state of Connecticut, bothwith respect to those with a diagnosis of in situ breastcarcinoma as well as the population at large. Ap-proximately 91% of cases and 92% of controls werewhite with the remaining sample representing primar-ily women of African–American background. Casesand controls did not differ significantly by mean age(56.6 years for DCIS cases, 54.7 years for LCIS cases,and 55.7 years for controls, respectively). Approxi-mately 4% of controls, 6.5% of DCIS cases and 7.3%of LCIS cases identified themselves as being of Jewishbackground (p < 0.05).
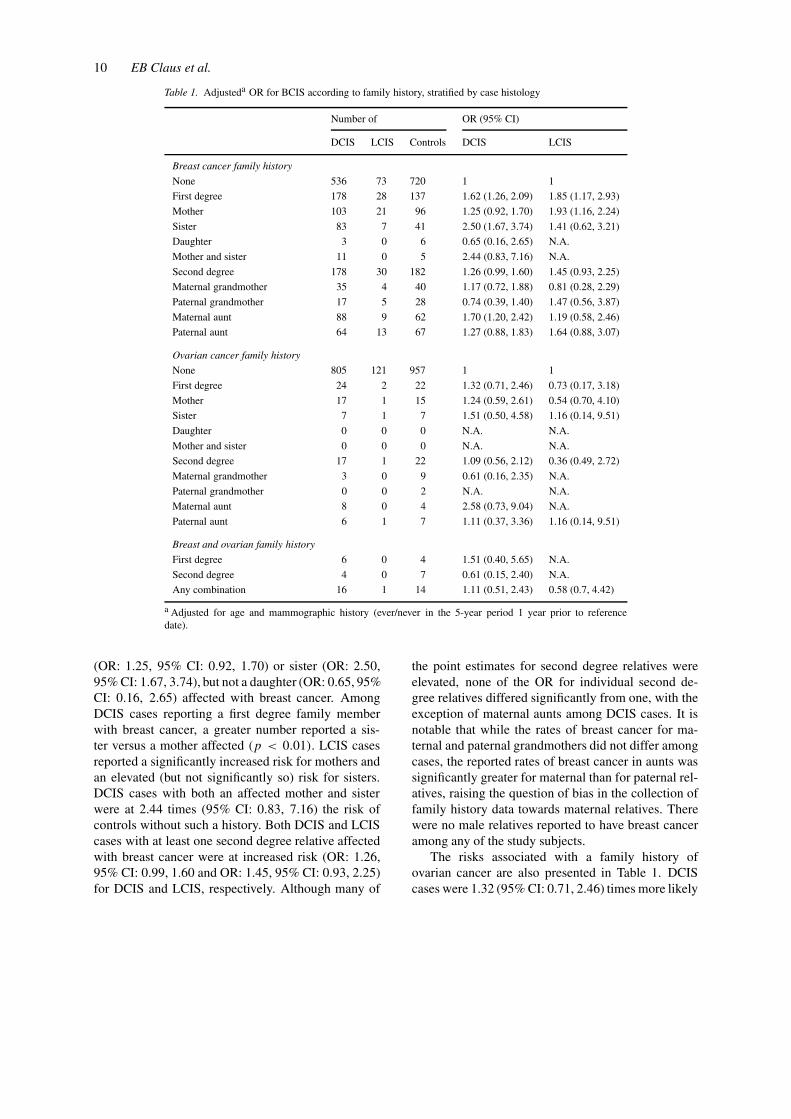
Adjusted ORs for a family history of breast andovarian cancer in the first and second degree relativesis presented by histologic subtype in Table 1. BothDCIS and LCIS cases were significantly more likelythan controls to report at least one first degree femalerelative affected with breast cancer (OR: 1.62, 95%CI: 1.26, 2.09 and OR: 1.85, 95% CI: 1.17, 2.93)for DCIS and LCIS, respectively. A higher propor-tion of DCIS cases than controls reported a mother
10 EB Claus et al.
Table 1. Adjusteda OR for BCIS according to family history, stratified by case histology
Number of OR (95% CI)
DCIS LCIS Controls DCIS LCIS
Breast cancer family history
None 536 73 720 1 1
First degree 178 28 137 1.62 (1.26, 2.09) 1.85 (1.17, 2.93)
Mother 103 21 96 1.25 (0.92, 1.70) 1.93 (1.16, 2.24)
Sister 83 7 41 2.50 (1.67, 3.74) 1.41 (0.62, 3.21)
Daughter 3 0 6 0.65 (0.16, 2.65) N.A.
Mother and sister 11 0 5 2.44 (0.83, 7.16) N.A.
Second degree 178 30 182 1.26 (0.99, 1.60) 1.45 (0.93, 2.25)
Maternal grandmother 35 4 40 1.17 (0.72, 1.88) 0.81 (0.28, 2.29)
Paternal grandmother 17 5 28 0.74 (0.39, 1.40) 1.47 (0.56, 3.87)
Maternal aunt 88 9 62 1.70 (1.20, 2.42) 1.19 (0.58, 2.46)
Paternal aunt 64 13 67 1.27 (0.88, 1.83) 1.64 (0.88, 3.07)
Ovarian cancer family history
None 805 121 957 1 1
First degree 24 2 22 1.32 (0.71, 2.46) 0.73 (0.17, 3.18)
Mother 17 1 15 1.24 (0.59, 2.61) 0.54 (0.70, 4.10)
Sister 7 1 7 1.51 (0.50, 4.58) 1.16 (0.14, 9.51)
Daughter 0 0 0 N.A. N.A.
Mother and sister 0 0 0 N.A. N.A.
Second degree 17 1 22 1.09 (0.56, 2.12) 0.36 (0.49, 2.72)
Maternal grandmother 3 0 9 0.61 (0.16, 2.35) N.A.
Paternal grandmother 0 0 2 N.A. N.A.
Maternal aunt 8 0 4 2.58 (0.73, 9.04) N.A.
Paternal aunt 6 1 7 1.11 (0.37, 3.36) 1.16 (0.14, 9.51)
Breast and ovarian family history
First degree 6 0 4 1.51 (0.40, 5.65) N.A.
Second degree 4 0 7 0.61 (0.15, 2.40) N.A.
Any combination 16 1 14 1.11 (0.51, 2.43) 0.58 (0.7, 4.42)
a Adjusted for age and mammographic history (ever/never in the 5-year period 1 year prior to referencedate).
(OR: 1.25, 95% CI: 0.92, 1.70) or sister (OR: 2.50,95% CI: 1.67, 3.74), but not a daughter (OR: 0.65, 95%CI: 0.16, 2.65) affected with breast cancer. AmongDCIS cases reporting a first degree family memberwith breast cancer, a greater number reported a sis-ter versus a mother affected (p < 0.01). LCIS casesreported a significantly increased risk for mothers andan elevated (but not significantly so) risk for sisters.DCIS cases with both an affected mother and sisterwere at 2.44 times (95% CI: 0.83, 7.16) the risk ofcontrols without such a history. Both DCIS and LCIScases with at least one second degree relative affectedwith breast cancer were at increased risk (OR: 1.26,95% CI: 0.99, 1.60 and OR: 1.45, 95% CI: 0.93, 2.25)for DCIS and LCIS, respectively. Although many of
the point estimates for second degree relatives wereelevated, none of the OR for individual second de-gree relatives differed significantly from one, with theexception of maternal aunts among DCIS cases. It isnotable that while the rates of breast cancer for ma-ternal and paternal grandmothers did not differ amongcases, the reported rates of breast cancer in aunts wassignificantly greater for maternal than for paternal rel-atives, raising the question of bias in the collection offamily history data towards maternal relatives. Therewere no male relatives reported to have breast canceramong any of the study subjects.
The risks associated with a family history ofovarian cancer are also presented in Table 1. DCIScases were 1.32 (95% CI: 0.71, 2.46) times more likely
Family history of breast and ovarian cancer 11
Table 2. Adjusteda OR for DCIS according to age and laterality of relative’s breast cancer
Breast cancer family history OR (95% CI)
Relative age ≤ 49 Relative age > 49
First degree 1.88 (1.20, 2.94) (n = 54) 1.52 (1.14, 2.04) (n = 124)
Mother 1.31 (0.66, 2.61) (n = 19) 1.24 (0.89, 1.72) (n = 84)
Sister 2.66 (1.44, 4.92) (n = 35) 2.40 (1.43, 4.01) (n = 48)
Bilateral Unilateral
First degree 2.08 (1.05, 4.09) (n = 23) 1.56 (1.20, 2.04) (n = 155)
Mother 1.80 (0.76, 4.23) (n = 13) 1.19 (0.86, 1.64) (n = 90)
Sister 2.07 (0.67, 6.36) (n = 9) 2.56 (1.67, 3.92) (n = 74)
a Adjusted for age and mammographic history (ever/never in the 5-year period 1 year prior toreference date).
Table 3. Adjusteda OR for DCIS according to family history and proband age
Number of OR (95% CI)
DCIS ≤ 49 Controls ≤ 49 DCIS > 49 Controls > 49 DCIS ≤ 49 DCIS > 49
Breast cancer family history
Any 104 89 206 189 1.64 (1.15, 2.34) 1.50 (1.16, 1.92)
First degree 55 31 123 106 2.12 (1.34, 3.40) 1.46 (1.08, 1.97)
≤ 49 23 12 31 24 2.54 (1.28, 5.05) 1.82 (1.03, 3.21)
> 49 32 19 92 82 1.85 (1.01, 3.39) 1.36 (0.98, 1.90)
Mother 35 26 68 70 1.72 (1.02, 2.90) 1.02 (0.70, 1.48)
Sister 22 6 61 35 3.74 (1.50, 9.35) 2.24 (1.44, 3.48)
Mother and sister 2 1 9 4 4.16 (0.43, 40.3) 1.90 (0.55, 6.54)
Second degree 64 69 114 113 1.18 (0.79, 1.74) 1.31 (0.97, 1.78)
None 192 89 344 458 1 1
Ovarian cancer family
history
First degree 7 7 17 15 1.34 (0.40, 4.49) 1.24 (0.60, 2.54)
Second degree 8 12 9 10 1.37 (0.56, 3.38) 0.94 (0.37, 2.44)
Breast and ovarian cancer
family history
First degree 2 1 4 3 1.34 (0.08, 22.0) 1.45 (0.32, 6.51)
Second degree 3 3 1 4 1.29 (0.21, 8.12) 0.27 (0.03, 2.40)
Any combination 7 4 9 10 1.73 (0.42, 7.19) 0.97 (0.39, 2.42)
a Estimates are adjusted for age and mammographic history (ever/never in the 5-year period 1 year prior to reference date).
than controls to report a first degree relative affectedwith ovarian cancer. A higher proportion of DCIScases than controls reported a mother (OR: 1.24, 95%CI: 0.59, 2.61) or sister (OR: 1.51, 95% CI: 0.50, 4.57)affected with ovarian cancer although neither estim-ate differed significantly from one. No study subjectreported a daughter or more than one first degree re-lative affected with ovarian cancer. The estimates for
women with second degree family members affectedwith ovarian cancer as well as family members af-fected with both breast and ovarian cancer are alsopresented; in general, the number of affected relativesamong these individuals is extremely small, makinginterpretation of these values difficult.
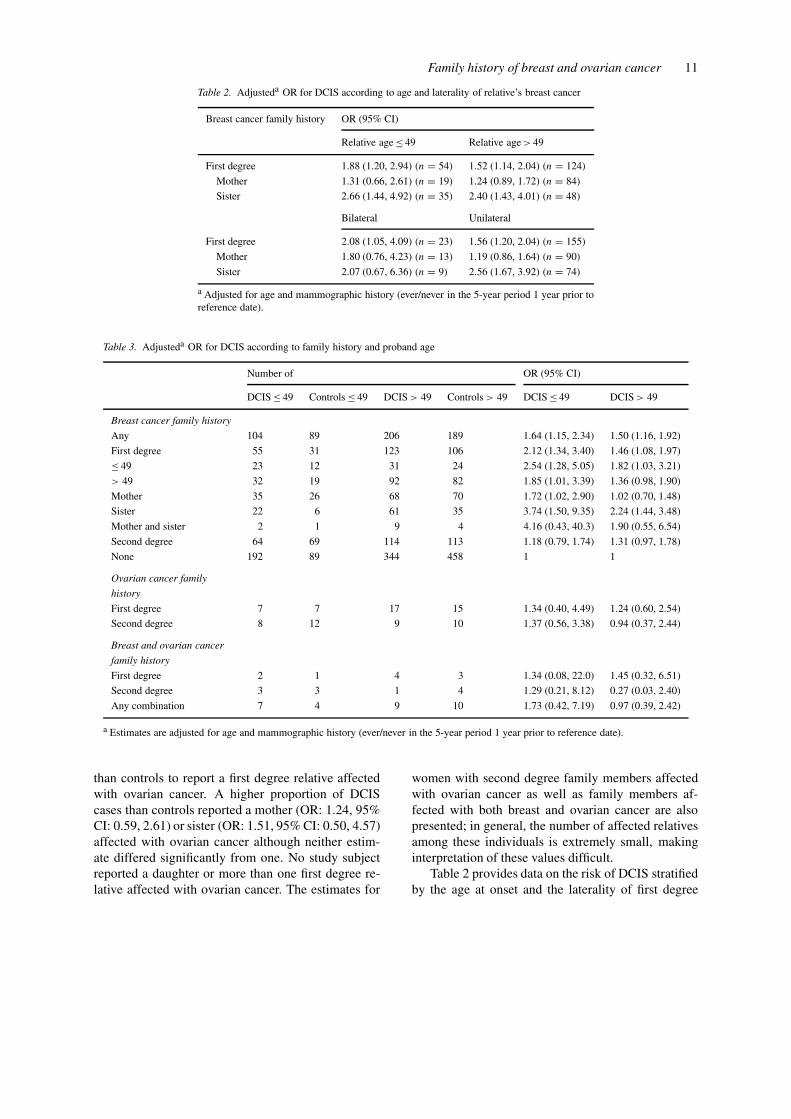
Table 2 provides data on the risk of DCIS stratifiedby the age at onset and the laterality of first degree

12 EB Claus et al.
relatives affected with breast cancer. In general, as istrue for IBC, increased risk was suggested (but wasnot statistically significant) with early age at onset andbilateral disease. Table 3 presents data which exam-ines the effect of a family history by age at onset ofthe DCIS cases themselves. The relationship betweenDCIS risk and a first degree family history of breastcancer appeared to vary by age at onset of both thecase and the relative with the greatest risk associatedwith younger women (although the differences werenot statistically significant). In general, this pattern isseen throughout the table.
To help assess the quality of family history report-ing in these data, SIRs were calculated for mothersand sisters of controls. Although the value for bothbreast and ovarian cancer (0.77 and 0.87, respectively)indicates that there is some under-reporting of bothbreast and ovarian cancer among first degree rela-tives of controls, neither estimate differed significantlyfrom one and both are similar to reports from otherlarge case/control studies which collected family his-tory data [30]. In addition, further analysis of the dataindicated that cases and controls were equally likelyto report cancer at an unknown site in a first degreerelative, suggesting that elevations in BCIS risk asso-ciated with a family history do not appear to be a resultof less knowledge of family history of cancer amongcontrols as compared to cases.
For each case and control, the program BRCAPROwas used to calculate the probability of being a carrierof a mutation in BRCA1 or BRCA2. With ‘carrier’defined as an individual with a calculated probabil-ity of 0.10 or greater, 3.7 and 1.9% of DCIS caseswould be predicted to carry mutations in BRCA1 andBRCA2, respectively. One control subject (0.1%) waspredicted to carry a deleterious allele in BRCA2.
Discussion
The present study is the largest case–control project todate to examine the relationship of a family history ofbreast and ovarian cancer with BCIS risk. The resultsconfirm the importance of a positive family historyof breast cancer and seem to suggest, as is true forIBC, that individuals with multiple first degree familymembers diagnosed with breast cancer, particularly atyoung ages, are at even greater risk. A number of pre-vious analyses have examined the association betweena history of breast cancer in at least one first degreerelative and BCIS and reported OR ranging from 1.5
to 2.7 [10–14, 17] including our report of a risk as-sociated with any family history of breast cancer of1.5 (95% CI: 1.2, 1.8) in these data [17]. The currentanalysis (which as in our preliminary analysis benefitsfrom the inclusion of women of all ages and correctionfor screening), examines this risk factor in greater de-tail, and defines OR estimates of 1.6 and 1.8 associatedwith a first degree family history of breast cancer forwomen diagnosed with DCIS and LCIS, respectively,and ratios of 1.3 and 1.4 associated with a second de-gree family history for women with DCIS and LCIS,respectively. Among cases with DCIS, women withmultiple first degree relatives affected with breast can-cer, in particular, a mother and sister affected withbreast cancer, were at even greater risk (OR: 2.4). Theprevious study able to examine DCIS risk for womenwith both an affected mother and sister also reportedan increased risk [10]. The magnitude of that risk (OR:6.93, 95% CI: 1.1–44) is much greater than that seenhere although the confidence interval from that studyis quite wide. It is notable that the risk estimates forfirst degree relatives presented here generally matchwell to studies which include women of similar agerange [12] but are somewhat lower than studies whichinclude relatively younger women [10, 11, 13]. How-ever, when risk is dichotomized by age in these data,an inverse relationship is seen between age at onsetand risk associated with family history with cases dia-gnosed by age 49 reporting a risk of 2.1, similar toother reports which include young cases [10, 11, 13]versus a risk of 1.5 for cases diagnosed over the age of49 years. A positive association between family his-tory and LCIS risk was also suggested in these dataas has been reported elsewhere [10, 16]. In general,the overall results for LCIS cases match those of theDCIS cases; however, extensive sub-analyses of LCIScases by age at onset and laterality of relatives wasnot possible given the relatively small number of LCIScases.
Given the findings here, at least with respect tobreast cancer family history, it is of interest to attemptto assess the role that BRCA1 and BRCA2 may playin the development of BCIS. A review [10–13, 16] ofstage-specific risk estimates associated with a breastcancer family history (used as a proxy variable forBRCA1 and BRCA2 status) provides no convincingevidence that the magnitude of risk associated withfamily history differs significantly by stage with somestudies reporting a greater [11, 16] association withBCIS or ‘early’ stage lesions while others report theopposite [12]. While there are extensive laboratory

Family history of breast and ovarian cancer 13
data [31–46] which estimate the prevalence of muta-tions in BRCA1 and BRCA2 for women with aswell as without a current diagnosis of invasive breastand/or ovarian cancer, there is currently little such datacollected for women diagnosed with ‘pure’ BCIS (al-though researchers have noted BCIS associated withIBC in BRCA1/BRCA2 carriers) [47].
In this report, an attempt was made to estimatethe extent to which BRCA1 and BRCA2 might beinvolved in BCIS via the use of statistical modeling[22–24]. The rates reported here are similar althoughslightly lower than those previously reported [31–46],a finding which may be due to several factors. Familyhistory data was obtained by telephone interview andnot confirmed by pathology report or medical recordreview. Although the rates of family history of breastand ovarian cancer reported here match well to previ-ous studies, there is some evidence of under-reporting,which although not statistically significant, may haveled to underestimates of rates of BRCA1 and BRCA2mutation prevalence. In addition, the sample examinedin this study differs from previously studied samples inseveral ways, including the fact that it is population-based, relatively large and includes only in situ casesdiagnosed within the United States, rather than froma clinic or hospital, an isolated population or fromoutside of the United States. As only a proportion ofin situ cases are likely to progress to invasive disease,it may be that rates of BRCA1 and BRCA2 mutationsin in situ disease are truly lower overall with the pres-ence of these mutations associated with progressionto IBC, although this hypothesis remains untested.Furthermore, because BCIS is primarily diagnosedthrough mammography and the majority of youngerwomen do not undergo mammography, there are fewcases under the age of 40 years in these data. Giventhe inverse relationship between age and risk of beinga BRCA1 carrier, the overall BRCA1 prevalence maybe underestimated in this group of women who havea mean age of approximately 55 years (although somestudies have reported a higher rate of BRCA1 muta-tions in older v.s. younger women with breast cancer)[39].
As is true of all statistical models of risk, accur-ate calculation of carrier probability depends upona correctly specified statistical model. Our estimatesare calculated using BRCAPRO based on a carriercut-point of 0.10 which although seemingly reason-able based on current knowledge of BRCA1/BRCA2testing [28, 29], is in itself just an estimate withouta clearly defined standard error. A recent study
examined the discriminatory ability of this model[28] in a data set of laboratory confirmed carriers ofBRCA1 and BRCA2 deleterious mutations. Using aprobability cut-point of 10%, the BRCAPRO com-puter model showed a sensitivity of 92%, a specificityof 32% and discriminatory accuracy of 0.71 for carrierprediction. It should be noted, however, that 26% ofthe families assigned a carrier probability of 95% orgreater did not show a mutation in either gene and16% of families defined as non-carriers (i.e., havinga predicted carrier probability of 10% or less) werefound to carry a mutation in BRCA1 or BRCA2. Someof these problems with over-prediction may be dueto the presence of other, as yet unidentified breastcancer susceptibility alleles or of non-detected muta-tions in BRCA1/BRCA2. In addition, it is possiblefor some family members in a BRCA1/BRCA2 familyto represent a case of sporadic breast cancer (hencethe tested individual will be negative despite the factthat family members do carry mutations in eitherBRCA1/BRCA2). With respect to under-predictionof carrier probability, there are some initial indica-tions that the currently used values of penetrances andprevalences in the BRCAPRO program may lead tounderestimating carrier probabilities for weak familyhistories and for non-Ashkenazi families with a his-tory of only ovarian cancer. Furthermore, at present,no risk model, including the BRCAPRO model im-plemented here, separates risk by histologic subtype,that is, by whether the breast case (be it proband orrelative) was diagnosed with in situ or invasive dis-ease but rather places all these women into the singlecategory of ‘affected’. If BRCA1/BRCA2 mutationcarrier risk varies by histologic subtype then obviouslyestimates based on this sort of model will be in er-ror. All of the above listed caveats highlight the factthat while it is of interest to examine these statisticallygenerated estimates of BRCA1/BRCA2 mutation car-rier status, it is difficult to fully define the extent ofBRCA1 and BRCA2 mutation prevalence in cases ofBCIS until laboratory testing is complete; the esti-mates provided here should therefore be interpreted aspreliminary.
Few studies have examined any aspect of the ge-netic epidemiology of BCIS; to our knowledge, thecurrent study is the largest done to date. The data hereprovide evidence that mechanisms similar to those in-volved in the development of IBC may be at workhere, although perhaps to a lesser extent. Whether thisis evidence that BRCA1 and BRCA2 are more likelyto be associated with a diagnosis of IBC versus BCIS

14 EB Claus et al.
remains to be confirmed using laboratory data. Oneadvantage of the data presented here is that the fullspectrum of age at onset and histology was includedas was information on screening; the estimates of riskpresented are controlled for screening history, particu-larly important in the analysis of non-invasive tumorswhich are more likely to be diagnosed at an early stageusing screening procedures such as mammograms.
Acknowledgements
The authors would like to acknowledge Sheila Griffinand Marjorie Jasmin for their work as interviewers onthe study and Edwin S. Iversen Jr, PhD and GiovanniParmigiani, PhD for their assistance with the use ofBRCAPRO.
References
1. Claus EB, Risch N, Thompson WD: Age at onset as an in-dicator of familial risk of breast cancer. Am J Epidemiol 131:961–972, 1990
2. Lynch HT, Watson P, Conway T, Fitzsimmons SL, Lynch J:Breast cancer family history as a risk factor for early onsetbreast cancer. Br Cancer Res Treat 11: 263–267, 1988
3. Ottman R, Pike MC, King MC, Casagrande JT, HendersonBE: Familial breast cancer in a population based series. AmJ Epidemiol 123: 15–21, 1986
4. Sattin RW, Rubin GL, Webster LA, Huezo CM, Wingo PA,Ory HW, Layde PM: The Cancer and Steroid HormoneStudy: Family history and risk of breast cancer. JAMA 253:1908–1913, 1985
5. Schwartz AG, King MC, Belle SH, Satariano WA, SwansonGM: Risk of breast cancer to relatives of young breast cancerpatients. J Nat Cancer Inst 75: 665–668, 1985
6. Kelsey JL, Gammon MD: Epidemiology of breast cancer. AmJ Epidemiol 12: 228–240, 1990
7. Slattery ML, Kerber RA: A comprehensive evaluation offamily history and breast cancer risk: the Utah PopulationDatabase. JAMA 270: 1563–1568, 1994
8. Colditz GA, Willett WC, Hunter DJ, Stampfer MJ, MansonJE, Hennekens CH, Rosner BA: Family history, age, and riskof breast cancer. JAMA 270: 338–343, 1548, 1993
9. Claus EB, Risch N, Thompson WD: Genetic analysis of breastcancer in the Cancer and Steroid Hormone Study. Am J HumGenet 48: 232–242, 1991
10. Weiss HA, Brinton LA, Brogan D, Coates RJ, Gammon MD,Malone KE, Schoenberg JB, Swanson CA: Epidemiology ofin situ and invasive breast cancer in women aged under 45.Br J Cancer 73(10): 1298–1305, 1996
11. Longnecker MP, Bernstein L, Paganini-Hill A, Enger SM,Ross RK: Risk factors for in situ breast cancer. Cancer Epi-demiol Biomarkers Prev 5: 961–965, 1996
12. Brinton LA, Hoover R, Fraumini Jr JF: Epidemiology ofminimal breast cancer. JAMA 249: 483–487, 1983
13. Kerlikowske K, Barclay J, Grady D, Sickles EA, Ernster V:Comparison of risk factors for ductal carcinoma in situ andinvasive breast cancer. JNCI 89: 77–82, 1997
14. Newcomb P, Storer BE, Marcus PM: Risk factors for car-cinoma in situ of the breast. Abstract, American Society ofPreventive Oncology, Bethesda, MD, 1994
15. Claus EB, Stowe M, Holford T, Carter D: The genetic epi-demiology of breast carcinoma in situ. US Army MedicalResearch and Material Command’s 1997 Meeting – DODBreast Cancer Research Program: An Era of Hope, 1997Proceedings. Washington, DC
16. Claus EB, Risch NR, Thompson WD, Carter D: Relationshipbetween breast histopathology and family history of breastcancer. Cancer 71: 147–153, 1993
17. Claus EB, Stowe M, Carter D: Breast carcinoma in situ:Risk factors and screening patterns. J Nat Cancer Inst 93:1811–1817, 2001
18. Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, HarshmanK, Tavtigian S, Liu Q, Cochran C, Bennett LM, Ding W: Astrong candidate for the breast and ovarian cancer suscepti-bility gene BRCA1. Science 266: 66–71, 1994
19. Wooster R, Neuhausen SL, Mangion J, Quirk Y, Ford D,Collins N, Nguyen K, Seal S, Tran T, Averill D: Localizationof a breast cancer susceptibility gene, BRCA2, to chromosome13q12-13. Science 265: 2088–2090, 1994
20. Colditz GA, Manson JE, Hankinson SE: The Nurses’ HealthStudy: 20-year contribution to the understanding of healthamong women. J Womens Health 6: 49–62, 1997
21. SAS Institute Inc.: SAS/STAT User’s Guide, Version 6. 4thedn, Vol 1, SAS Institute Inc., Cary, NC, 1989
22. Euhus D, Berry D, Parmigiani G, Iversen E, Frawley W:Cancer gene with BRCAPRO. University of Texas, 1998
23. Berry DA, Parmigiani G, Sanchez J, Schildkraut J, Winer E:Probability of carrying a mutation of breast–ovarian cancergene BRCA1 based on family history. J Nat Cancer Inst 89:227–238, 1997
24. Parmigiani G, Berry DA, Aguilar O: Determining carrier prob-abilities for breast cancer-susceptibility genes BRCA1 andBRCA2. Am J Hum Genet 62: 145–158, 1998
25. Ford D, Easton DF, Peto J: Estimates of the gene frequencyof BRCA1 and its contribution to breast and ovarian cancerincidence. Am J Hum Genet 57: 1457–1462, 1995
26. Easton D, Ford D, Bishop DT: The Breast Cancer LinkageConsortium: Breast and ovarian cancer incidence in BRCA1mutation carriers. Am J Hum Genet 56: 265–271, 1995
27. Struewing JP, Hartge P, Wacholder S, Baker SM, BerlinM, McAdams M, Timmerman MM, Brody LC, TuckerMA: The risk of cancer associated with specific muta-tions of BRCA1 and BRCA2 among Ashkenazi Jews.N Engl J Med 336: 1401–1408, 1997
28. Euhus DM, Smith KC, Robinson L, Stucky A, Olopade OI,Cummings S, Garber JE, Chittenden A, Mills GB, Rieger P,Esserman L, Crawford B, Hughes KS, Roche CA, Ganz PA,Seldon J, Fabian CJ, Klemp J, Tomlinson G: Pretest predictionof BRCA1 or BRCA2 mutation by risk counselors and thecomputer model BRCAPRO. JNCI 94: 844–851, 2002
29. Statement of the American Society of Clinical Oncology:Genetic testing for cancer susceptibility. Indications for ge-netic testing. Table 3 (Accessed July 3, 2002). Available at:http://www.asco.org/prof/pp/html/m_ppgenetc.htm#tab3
30. Schildkraut JM: Family history of cancer as a risk factorfor epithelial carcinoma of the ovary. PhD Dissertation, YaleUniversity Press, 1987
31. Myriad Genetics (Accessed July 3, 2002). Available at:http://www.myriad.com/med/brac/mutptables.html
32. Shattuck-Eidens D, McClure M, Simard J, Labrie F,Narod S, Couch F, Hoskins K, Weber B, Castilla, Erdos M: A
Family history of breast and ovarian cancer 15
collaborative study of 80 mutations in the BRCA1 breast andovarian cancer susceptibility gene. Implications for presymp-tomatic testing and screening. JAMA 273: 535–541, 1995
33. Langston AA, Malone KE, Thompson JD, Daling JR,Ostrander EA: BRCA1 mutations in a population-basedsample of young women with breast cancer. N Engl J Med334: 137–142, 1996
34. Fitzgerald MG, MacDonald DJ, Krainer M, Hoover I, O’NeilE, Unsal H, Silva-Arrieto S, Finkelstein DM, Beer-Romero P,Englert C, Sgroi DC, Smith BL, Younger JW, Garber JE, DudaRB, Mayzel KA, Isselbacher KJ, Friend SH, Haber DA: Germ-line BRCA1 mutations in Jewish and non-Jewish women withearly onset breast cancer. N Engl J Med 334: 143–149, 1996
35. Struewing JP, Abeliovich D, Peretz T, Avishai N, Kaback MM,Collins FS, Brody LC: The carrier frequency of the BRCA1185delAG mutation is approximately 1 percent in AshkenaziJewish individuals. Nat Genet 11: 198–200, 1995
36. Roa BB, Boyd AA, Volcik K, Richards CS: Ashkenazi Jewishpopulation frequencies for common mutations in BRCA1 andBRCA2. Nat Genet 14: 185–187, 1996
37. Oddoux C, Struewing JP, Clayton CM, Neuhausen S, BrodyLC, Kaback, Haas B, Norton L, Borgen P, Jhanwar S, GoldgarD, Ostrer H, Offit K: The carrier frequency of the BRCA26174delT mutation among Ashkenazi Jewish individuals isapproximately 1%. Nat Genet 14: 188–190, 1996
38. Neuhausen S, Gilewski T, Norton L, Tran T, McGuire P,Swensen J, Hampel H, Borgen P, Brown K, Skolnick M,Shattuck-Eidens D, Jhanwar S, Goldgar D, Offit K: Recur-rent BRCA2 617delT mutations in Ashkenazi Jewish womenaffected by breast cancer. Nat Genet 13: 126–128, 1996
39. Newman B, Mu H, Butler LM, Millikan RC, Moorman PG,King MC: Frequency of breast cancer attributable to BRCA1in a population-based series of American women. JAMA 279:915–921, 1998
40. Malone KE, Daling JR, Thompson JD, O’Brien CA, FranciscoLV, Ostrander EA: BRCA1 mutations and breast cancer in thegeneral population: analyses in women before age 35 years
and in women before age 45 years with first-degree familyhistory. JAMA 279: 922–929, 1998
41. Couch FJ, DeShano ML, Blackwood MA, Calzone K, StopferJ, Campeau L, Ganguly A, Rebbeck T, Weber BL: BRCA1mutations in women attending clinics that evaluate the risk ofbreast cancer. N Engl J Med 336: 1409–1415, 1997
42. Krainer M, Silva-Arrieta S, Fitzgerald MG, Shimada A,Ishioka C, Kanamaru R, MacDonald DJ, Unsal H, FinkelsteinDM, Bowcock A, Isselbacher KJ, Haber DA: Differential con-tributions of BRCA1 and BRCA2 to early onset breast cancer.N Engl J Med 336: 1416–1421, 1997
43. Loman N, Johannsson O, Kristoffersson U, Olsson H, Borg A:Family history of breast and ovarian cancers and BRCA1 andBRCA2 mutations in a population-based series of early onsetbreast cancer. J Nat Cancer Inst 93: 1215–1223, 2001
44. Peto J, Collins N, Barfoot R, Seal S, Warren W, Rahman N,Easton DF, Evans C, Deacon J, Stratton MR: Prevalence ofBRCA1 and BRCA2 gene mutations in patients with earlyonset breast cancer. J Nat Cancer Inst 91: 943–949, 1999
45. Szabo CI, King MC: Population genetics of BRCA1 andBRCA2. Am J Hum Genet 60: 1013–1020, 1997
46. Syrjakoski K, Vahteristo P, Eerola H, Tamminen A,Kivinummi K, Sarantaus L, Holli K, Blomqvist C,Kallioniemi OP, Kainu T, Nevanlinna H: Population-basedstudy of BRCA1 and BRCA2 mutations in 1035 unselectedFinnish breast cancer patients. J Nat Cancer Inst 92:1529–1531, 2001
47. Marcus JN, Watson P, Page DL, Narod SA, Lenoir GM,Tonin P, Linder-Stephenson L, Salerno G, Conway TA, LynchHT: Hereditary breast cancer. Pathobiology, prognosis, andBRCA1 and BRCA2 gene linkage. Cancer 77: 697–709
Address for offprints and correspondence: Dr Elizabeth B. Claus,Department of Epidemiology and Public Health, Yale University, 60College St., P.O. Box 208034, New Haven, CT 06520-8034, USA;Tel.: +1-203-785-6050; E-mail: [email protected]