Embed Size (px)
Citation preview

Eur J Vasc Surg 7, 709-712 (1993)
Familial Abdominal Aortic Aneurysm: Prevalence and Implications for Screening
D. C. R. Adams, B. R. Tuiloh, S. W. Galloway, E. Shaw, A. J. Tulloh and K. R. Poskitt
Department of Vascular Surgery, Cheltenham General Hospital, Cheltenham, Gloucestershire, U.K.
The high prevalence of abdominal aortic aneurysm (AAA) in men over the age of 65 has led to the establishment of ultrasound screening programmes for this group. The apparent familial tendency towards AAA formation suggests that relatives of aneurysm patients may form another subpopulation in whom screening is appropriate. The first degree relatives of 100 consecutive aneurysm patients were identified. Of 110 relatives over 50 years of age, two were known to have had AAA and ultrasound scans were performed on 74, providing information on aortic size for 76 relatives (69%). No further aortic aneurysms (antero-posterior diameter ~4.0cm) were found on scanning. However, nine relatives were demonstrated to have aortic dilatation (2.5-3.9 cm). Aortic dilatation was observed in 21% of male first degree relatives over 50 years of age, affecting 27% of sons and 17% of brothers. Only 4% of the sisters and none of the daughters were found to have aortic dilatation. The prevalence of aortic enlargement seems to be sufficiently high amongst male first degree relatives of AAA patients over 50 years of age to justify aortic screening.
Key Words: Abdominal aortic aneurysm; Screening; Aortic enlargement.
Introduction
It has been sugges ted that there is a familial factor in the genesis of abdominal aortic aneu rysm (AAA) with a number of reports investigating the familial relat ionships and possible genetic mechanisms involved in aneu rysm formation. 1-4 These early repor ts did not a t tempt to assess the prevalence of AAA amongs t relatives. However , two recent studies based on patient in terview have suggested that up to 30% of first degree relatives may develop AAA, 5'6 and two u l t rasound studies have conf i rmed a similar prevalence amongs t brothers. 7' 8
Abdominal aortic aneurysm presents an ideal subject for screening in that it is a commo n condit ion, for which there is a simple, non-invasive test and an effective means of t reatment . 9-11 A county-wide screening p rog ramme for 65-year-old men has been inst i tuted in Gloucestershire. 12 It is recognised that screening may be r ende red more efficient if a "high- r isk" sub-popula t ion can be identified. Previous repor ts have examined the potential of using vascular risk factors such as hyper tens ion , 9'1°'13 smok-
Please address all correspondence to: K. R. Poskitt, Cheltenham General Hospital, Sandford Road, Cheltenham, Gloucestershire, GL53 7AN, U.K.
ing 9"1°'13 and peripheral vascular disease 1°'14 as a basis for AAA screening. However , the consensus of these reports is that a l though these risk factors are important , none of them individually provides an adequate basis for screening selection.
The current s tudy was established with two aims: first, to gain fur ther evidence of the prevalence of AAA in first degree relatives of AAA patients and second, to assess the feasibility of screening this g roup for AAA.
Patients and Methods
One h u n d r e d consecutive patients undergo ing sur- gery for AAA at Che l tenham General Hospital be- tween 1985 and September 1990 were identified. Con- tact was made with each patient 's general practi t ioner obtaining consent to approach the pat ient or a surviv- ing relative. A list of first degree relatives (brothers, sisters, sons and daughters) over the age of 50 years was compiled. In addition, we enqui red whe the r any of these relatives were k n o w n to have had an AAA.
Relatives living in Gloucestershire were con- tacted by letter and offered an appo in tmen t ei ther at
0950-821X/93/060709+04 $08.00/0 © 1993 Grune & Stratton Ltd.

710 D.C.R. Adams etaL
the patient 's general practice, the hospital 's vascular laboratory or in the patient 's home. With a senior nurse (ES) in a t tendance, an u l t rasound examinat ion of the aorta was per fo rmed by a radiographer (AJT) using an ALOKA SSD-500 ® portable u l t rasound scanner with a 3.5 mHz curvil inear probe (Aloka Co. Ltd., Japan).
The maximum antero-poster ior (AP) diameter of the infrarenal aorta was recorded. A history of smok- ing within the last 10 years, hyper t ens ion requiring drug t rea tment or per ipheral vascular disease (as def ined by the presence of claudication or rest pain at any stage) was noted. A r a n d o m blood sample was taken for serum cholesterol measurement .
Relatives living e lsewhere in the U.K. ei ther had a hom e visit u l t rasound, or were reques ted to seek one th rough their general practitioners. Relatives liv- ing outside the U.K. were also asked to request scans th rough their local practit ioners. Blood cholesterol and a history of smoking, hyper tens ion and periph- eral vascular disease was not recorded in all of these cases. The relatives and their general practit ioners were informed of the results.
In line with our local screening policy, we def ined aortic size as normal, dilated or aneurysmal if the maximum AP aortic d iameter was <2 .5cm, 2 .5- 3.9 cm or ~>4.0 cm respectively. Any person found to have an aneu rysm was to be referred to a vascular surgeon. If the aorta was dilated a repeat u l t rasound scan was arranged in twelve months . If the aorta was normal no fur ther follow-up was under taken.
Resul ts
Information was gained on the families of 92 of the original 100 patients. Four of the remaining eight pat ients had died wi thout k n o w n relatives, two were still alive but could not be traced and two declined to participate in the study. In the 92 families traced, there were 110 first degree relatives over the age of 50. Fifty-one of these lived locally, 50 lived e lsewhere in the U.K. and nine lived abroad.
Of the 51 relatives living locally, one 59-year-old male had previously unde rgone aneurysm repair and 44 (86%) were scanned. Four declined to participate and two failed to a t tend for their scans. Elsewhere in the U.K. 26 of 50 subjects (52%) were scanned and one 69-year-old w o m a n died from a rup tu red AAA after initial contact had been made but before a scan could be performed. Four of nine (44%) relatives overseas had scans per formed. Information on aortic size was therefore obtained on 76 of 110 first degree
3.5
3
2.5
*~ 1.5
~ 1
0.5
• o°o • • • . . . : . . .
• • • • 18• o • o ° U n •
",;'*" ",:= "|. ", ; •
• Male • Female
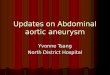
45 50 55 60 65 70 75 80 85 90 Age [years)
Fig. 1. The distribution of aortic size with age in the first degree relatives of AAA patients.
relatives (69%) comprising 88% of those living locally and approximate ly half of those living fur ther afield.
Excluding the two k n o w n aneurysms, the aortic diameters of those scanned ranged from 1.6 to 3.4 cm (mean 2.2cm) in males and 1.4 to 3 .0cm (mean 1.9 cm) in females (Fig. 1). Thus by our definit ions, no aneurysms were detected on screening. One female and eight males were found to have aortic dilatation (Table 1). Nine teen per cent of the 60-69 age g roup had dilated aortas (5 out of 27). Aortic dilatation affec- ted three of the 30 subjects be tween 50 and 59 (10%), and one of the four relatives over 80 years of age.
Aortic dilatation was seen in four of 23 brothers (17%) and four of 15 sons (27%), but in only one of 28 sisters (4%) and none of the daughters . Al though we arbitrarily chose 50 as the lower age limit for this s tudy, a fur ther 18 first degree relatives aged from 40-49 reques ted scanning after hear ing about the s tudy. All were found to have normal aortic diam- eters.
Including the 59-year-old male w h o had an AAA repaired, peripheral vascular disease affected one (10%) of 10 with enlarged aortas and two (4%) of 50
Table 1. Results of ultrasound scanning
Number Number Total Age of men of women number range (dilated) (dilated) (dilated)
50-59 18 (3) 12 30 (3)
60-69 13 (4) 14 (1) 27 (5)
70-79 4 9 13
80-89 3 (1) 1 4 (1)
Eur J Vasc Surg Vol 7, November 1993

Familial Abdominal Aortic Aneurysm 711
subjects with normal aortas. Hypertension affected one (10%) of 10 relatives with enlarged aortas and 12 (24%) of 50 normal subjects. Nine of 10 (90%) of those with enlargement were smokers compared with 31 of 50 (62%) of those with normal aortas. Mean (+S.D.) random serum cholesterol levels of subjects with enlargement were 6.8 (+0.6) mmol/1 compared with 6.15 (_+1.2) for normal subjects. None of these differ- ences attained statistical significance.
Discussion
Aortic aneurysm is a common condition, with a re- ported prevalence of approximately 2.5% in men over the age of 65.1°" 12,15,16 Moreover, the incidence of AAA appears to be increasing, particularly amongst elderly women. 17 Factors associated with develop- ment of AAA include peripheral vascular dis- ease,10,14 hypertension,9,10,13 smoking,9,10,13 hyper- cholesterolaemia 18 and hereditary influences. 19 In our study, there is a trend for enlargement amongst smokers although this was not significant. A heredi- tary predisposition to aneurysm formation has long been recognised in relation to connective tissue dis- orders such as Marfan's disease. More subtle and complex genetic influences involving either autoso- mal or sex chromosomes have been suggested in AAA formation. 1-5" 19 Regardless of the mechanism, further evidence of a familial factor has been provided by the ultrasound studies of Bengtsson 7 and Collin 8 who both found aortic aneurysm in 29% of brothers of their patients. Our findings of aortic enlargement in 27% of sons and 18% of brothers sup- port these studies.
Our results suggest that aneurysms induced by familial factors may become apparent at an earlier age than in the general population. Of the subjects aged from 50-59, 10% had aortic enlargement. The preva- lence of enlargement amongst males in this age group was 17%. This figure is about twice the prevalence of enlargement seen in our general male population at age 65,12 indicating that relatives of aneurysm patients may be at a greater risk at an earlier age. Lending support to this concept are the studies of familial aneurysms by Tilson 1 and Victor 2 in which over 60% of subjects were under the age of 65.
Rupture of AAA is responsible for 1.3% of all deaths in men aged over 65, 2o thus up to half of the population with untreated AAA die from rupture. 21 Moreover, this figure appears to be increasing with time. 22 Aneurysms are often difficult to recognise cli- nically 23 and ultrasound screening programmes for
AAA are becoming increasingly widespread. 9 1 ~, 24, 25 Although it will take years for aneurysm screening to prove its worth in terms of decreased rates of rupture and mortality, the rationale for screening is compel- ling. It focuses on a common condition, using a simple and effective method of detection, to allow treatment which confers a significant improvement in survival as well as a potential economic advantage. Our local screening programme has been projected at men aged 65 in the belief that screening at a younger age would be inefficient because of the lower preva- lence of AAA. 26 However, screening of male first degree relatives over 50 appears justified on the basis of these results. It may be that by identifying and controlling other risk factors in these subjects at an early age, we could diminish the progression in size and potentially avoid surgery altogether.
Aneurysm screening is readily accepted by the families of aneurysm patients as indicated by an 86% attendance rate of local relatives and the high number of relatives of aneurysm patients outside the study group who requested an ultrasound examination. There is a potential for screening programmes to increase anxiety amongst the subjects. However, we believe that anxiety amongst the relatives of AAA patients is already raised and that a normal scan result should diminish this anxiety.
Our observations indicate that aortic enlarge- ment is more common amongst first degree relatives of aneurysm patients than in the general population and that this tendency begins to appear in the 6th decade. Smoking, peripheral vascular disease, hyper- tension and raised serum cholesterol did not clearly influence the prevalence of aortic enlargement in this study. The high prevalence of aortic enlargement in male first degree relatives over 50 and their high com- pliance with this study both indicate that ultrasound screening is appropriate for this group.
Acknowledgements
We would like to thank Ms K. Sale for her help in conducting the study. We would also like to acknowledge the assistance given by the Department of Surgery at Charing Cross Hospital, London in arranging scans for the distant relatives.
References
1 TILSON MD, SEASHORE MR. Human genetics of the abdominal aortic aneurysm. Surg Gynecol Obstet 1984; 158: 129-132.
2 TILSON MD, SEASHORE MR. Fifty families with abdominal aortic aneurysms in two or more first-order relatives. Am J Surg 1984; 147: 551-552.
Eur J Vasc Surg Vol 7, November 1993

712 D .C .R . Adams et aL
3 VICTOR DW, MCCREADY RA, HYDE GL. The role of inheritance in the pathogenesis of abdominal aortic aneurysms. J Kentucky Med Assoc 1985; 84: 601-603.
4 JOHANSEN K, KOEPSELL T. Familial tendency for abdominal aortic aneurysms. JAMA 1986; 256: 1934-1936.
5 POWELL JT, GREENHALGH RM. Multifactorial inheritance of ab- dominal aortic aneurysm. Eur J Vasc Surg 1987; 1: 29-31.
6 COLE CW, BARBER GC, BOUCHARD AG, McPHAIL NV, ROBERGE C, WADDELL WG, WELLINGTON JL. Abdominal aortic aneurysm: consequences of a positive family history. Can J Surg 1989; 32: 117-120.
7 BENGTSSON H, NORRG~RD O, ANGQUIST KA, EKBERG O, OBERG L, BERGQVIST D. Ultrasonographic screening of the abdominal aorta among siblings of patients with abdominal aortic aneur- ysms. Br ] Surg 1989; 76: 589-591.
8 COLLIN J, WALTON J. Is abdominal aortic aneurysm familial? BMJ 1989; 299: 493.
90'KELLY TJ, HEATHER BP. General practice-based population screening for abdominal aortic aneurysms: a pilot study. Br J Surg 1989; 76: 479-480.
10 COLLIN J, WALTON J, ARAUJO L, LINDSELL D. Oxford screening programme for abdominal aortic aneurysm in men aged 65 to 74 years. Lancet 1988; ii: 613-615.
11 SCOTT RaP, ASHTON HA, KAY DN. Routine ultrasound screen- ing in management of abdominal aortic aneurysm. BMJ 1988; 296: 1709-1710.
12 LUCAROTTI ME, SHAW E, POSKITT KR, HEATHER BP. The Glouces- tershire Aneurysm Screening Programme: the first two years' experience. Eur J Vasc Surg 1993; 7: 397-401.
13 THURMOND AS, SEMLER HJ. Abdominal aortic aneurysm: inci- dence in a population at risk. J Cardiovasc Surg 1986; 27: 457- 460.
14 BERRIDGE DC, GRIFFITH CDM, AMAR SS, HOPKINSON BR, MAKIN GS. Screening for clinically unsuspected abdominal aortic aneurysms in patients with peripheral vascular disease. Eur J Vasc Surg 1989; 3: 421-422.
15 SCOTT RAP. Ultrasound screening in the management of ab- dominal aortic aneurysms. Inter Angio 1986; 5: 263-267.
16 COLLIN J. Screening for abdominal aortic aneurysms. Br J Surg 1985; 72: 851-852.
17 THOMAS PRS, STEWART RD. Abdominal aortic aneurysm. Br J Surg 1988; 75: 733-736.
18 NORRG~RD O, ANGQUIST KA, JOHNSON O. Familial aortic aneur- y sms- - se rum concentrations of triglyceride, cholesterol, HDL cholesterol and (VLDL + LDL) cholesterol. Br J Surg 1985; 72: 113-116.
19 NORRG~RD O. Looking for the familial connection in aortic aneurysm. In: GREENHALGH RM and MANNICK JA, eds., The Cause and Management of Aneurysms. London: WB Saunders, 1990: 29-36.
20 Office of population censuses and surveys. Mortality Statistics Cause: Review of the Registrar General on Deaths by Cause, Sex and Age in England and Wales 1983. London: HM Stationery Office, 1983: Series DH2 No. 10.
21 WALKER EM, HOPKINSON BR, MAKINGS. Unoperated abdominal aortic aneurysm: presentation and natural history. Ann R Coll Surg Engl 1983; 65: 311-313.
22 MEALY K, SALMAN A. The true incidence of ruptured abdominal aortic aneurysms. Eur J Vasc Surg 1988; 2: 405-408.
23 COLHN J, ARAUJO L, LINDSELL D. Screening for abdominal aortic aneurysms. Lancet 1987; ii: 736-737.
24 ALLEN PIM, GOUREVITCH D, McKINLEY J, TUDWAY D, GOLDMAN M. Population screening for aortic aneurysms. Lancet 1987; ii: 736.
25 ALLEN PIM. Screening for abdominal aortic aneurysm. Biomed Pharmacother 1988; 42: 451-454.
26 O'KELLY TJ, HEATHER BP. The feasibility of screening for ab- dominal aortic aneurysms in a district general hospital. Ann R Coll Surg Engl 1988; 70: 197-199.
Accepted 6 June 1993
Eur J Vasc Surg Vol 7, November 1993