Embed Size (px)
Citation preview

FACE RESURFACING USING A CERVICOTHORACICSKIN FLAP PREFABRICATED BY LATERAL THIGHFASCIAL FLAP AND TISSUE EXPANDER
QINGFENG LI, M.D., Ph.D.,* TAO ZAN, M.D., Ph.D., BIN GU, M.D., KAI LIU, Ph.D.,
GUOXIONG SHEN, M.D., YUN XIE, M.D., and RUI WENG, Ph.D.
Background: Resurfacing of facial massive soft tissue defect is a formidable challenge because of the unique character of the region andthe limitation of well-matched donor site. In this report, we introduce a technique for using the prefabricated cervicothoracic skin flap for fa-cial resurfacing, in an attempt to meet the principle of flap selection in face reconstructive surgery for matching the color and texture, largedimension, and thinner thickness (MLT) of the recipient. Materials: Eleven patients with massive facial scars underwent resurfacing proce-dures with prefabricated cervicothoracic flaps. The vasculature of the lateral thigh fascial flap, including the descending branch of the lat-eral femoral circumflex vessels and the surrounding muscle fascia, was used as the vascular carrier, and the pedicles of the fascial flapwere anastomosed to either the superior thyroid or facial vessels in flap prefabrication. A tissue expander was placed beneath the fascialflap to enlarge the size and reduce the thickness of the flap. Results: The average size of the harvested fascia flap was 6.5 3 11.7 cm.After a mean interval of 21.5 weeks, the expanders were filled to a mean volume of 1,685 ml. The sizes of the prefabricated skin flapsranged from 12 3 15 cm to 15 3 32 cm. The prefabricated skin flaps were then transferred to the recipient site as pedicled flaps for facialresurfacing. All facial soft tissue defects were successfully covered by the flaps. The donor sites were primarily closed and healed withoutcomplications. Although varied degrees of venous congestion were developed after flap transfers, the marginal necrosis only occurred intwo cases. The results in follow-up showed most resurfaced faces restored natural contour and regained emotional expression. Conclu-sion: MLT is the principle for flap selection in resurfacing of the massive facial soft tissue defect. Our experience in this series of patientsdemonstrated that the prefabricated cervicothoracic skin flap could be a reliable alternative tool for resurfacing of massive facial soft tissuedefects. VVC 2009 Wiley-Liss, Inc. Microsurgery 29:515–523, 2009.
Facial deformity and disfigurement, especially resulted
from massive soft tissue defects after burn injury or tu-
mor excision, represent a profound disruption of body
image and may constitute a major social and psychologi-
cal crisis. Skin grafts and flap techniques have been com-
monly used following the removal of scar tissue for
resurfacing the lost skin in patients. However, contracture
of skin graft may cause not only deformity and disability
of facial function and expression but also color and tex-
ture mismatched to the recipient, especially in nonwhite
patients. Local flap transfer techniques often encounter
some problems, such as insufficient donor sites, limited
vascular territory, and difficulty for flap inset.1–8 The free
flap transfer has revolutionized reconstruction, especially
in the head and neck, where local flap is seldom avail-
able. However, free flaps are usually used for coverage
of the tissue defect, rather than for aesthetically and func-
tionally resurfacing the face because free flaps also have
problems for color, texture, and thickness mismatched
and notable bulk.1 Thus, there has not been an ideal tech-
nique for achieving satisfactory functional and aesthetic
results in facial resurfacing.
On the basis of the special anatomic characteristic of
head and neck area, we proposed the principle of
‘‘matching, large size, and thinner thickness’’ (MLT) in
flap selection for reconstruction and resurfacing of mas-
sive facial soft tissue defects. The principle requires that
the selected flap should have 1) the color and texture
matched to the recipient region; 2) the size large enough
to cover massive defects; and 3) the thinner thickness to
mediate facial expression and coincide the facial contour.
According to anatomic characteristics, the closer the do-
nor site is located to the recipient, the better skin texture
matches the recipient site. The skin of cervicothoracic
area is considered a good donor site for reconstruction of
massive facial skin defects because its color and texture
well matched to face and the potential large size for har-
vest. However, the traditional flaps raised from this area
are lack of reliable axial blood supplies and thus are not
consistent in size of flap and length of pedicles to reach
the recipient.3–7 A more sophisticated approach is needed
for optimal resurfacing of massive facial soft tissue
defects.
The technique of flap prefabrication has been proved
for creating new skin flaps that are not restricted to
natural vascular territories by means of neovasculariza-
tion.9–13 In this report, we present our experience on pre-
fabrication of a cervicothoracic skin flap with the lateral
thigh fascial flap as vascular carrier and tissue expander
for creating large and thinner flap to match the MLT
Department of Plastic and Reconstructive Surgery, The Ninth Hospital, Medi-cal School of Shanghai Jiao Tong University, Shanghai, China
Grant sponsor: National Natural Science Foundation of China; Grant number:30730092; Grant sponsor: Research Special Fund Public Welfare Industry ofHealth; Grant number: 200802014.
*Correspondence to: Qingfeng Li, M.D., Ph.D., Department of Plastic andReconstructive Surgery, The Ninth Hospital, Medical School of ShanghaiJiao Tong University, Shanghai 200011, China. E-mail: [email protected]
Received 14 November 2008; Accepted 16 January 2009
Published online 23 March 2009 in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/micr.20640
VVC 2009 Wiley-Liss, Inc.

principle. We used the prefabricated skin flaps for facial
resurfacing in a series of 11 patients.
PATIENTS AND METHODS
From March 2006 to April 2008, 11 patients received
prefabricated cervicothoracic pedicled skin flaps for head
and neck reconstruction and facial resurfacing of massive
soft tissue defects after scar resections in our institution.
There were six male and five female patients with age
ranging from 11 to 56 years old (average 31.7 years old).
The initial causes of the defects included burn injuries
with molten steel (four cases), acid or lye (three cases),
high voltage electricity (two cases), and flame (two
cases). The prefabricated skin flaps were used for recon-
struction of the lower jaw and cheek in five cases, peri-
oral reconstruction in three cases, releasing neck contrac-
ture in two cases, and perioral and nasal reconstruction in
one case.
Surgical Technique for Flap
Prefabrication and Transfer
Fascial flap harvest. The lateral thigh fascial flap
nourished by the descending branch of the lateral circum-
flex femoral artery was designated as the vascular carrier
for flap prefabrication based on its characters of the vas-
cular pedicle around 8–16 cm in length, with a vessel di-
ameter larger than 2 mm (see Fig. 1).14–16 In the opera-
tion design, a reference line was drawn from the anterior
superior iliac spine to the superolateral border of the pa-
tella. An ‘‘S’’-shaped incision was made along the lower
2/3 of the line. The tensor fascia lata muscle was sepa-
rated for exposure of the lateral intermuscular septum
between the rectus femoris and the vastus lateralis mus-
cle. The rectus femoris muscle was retracted medially.
The descending branch of the lateral circumflex femoral
artery and its venae comitantes were carefully dissected
from the rectus femoris and vastus lateralis muscles. The
distal end of the vessels before penetrating the muscles
were divided and ligated. The motor nerve to the vastus
lateralis was preserved by separating it from the main
vascular pedicle during harvest of the fascial flap.
Fascial flap transfer and tissue expander place-
ment. The recipient vessels and the donor site for pre-
fabricated flap were designed under consideration of eas-
ier rotation of the pedicled flap and skin texture close to
the recipient in face and neck. An approximate 6–7 cm
in length incision was made along the upper half of the
anterior margin of the sternocleidomastoid muscle,
extending into the anterior margin of the trapezius mus-
cle. Either the superior thyroid artery or the facial artery
and its venae comitantes were dissected as the recipient
vessels. The lateral thigh fascial flap with its vascular
pedicles was inset into a subcutaneous pocket of the cer-
vicothoracic area after the blood perfusion to the flap was
reestablished by microvascular anastomoses. A rectangu-
lar remote filling tissue expander was then placed under-
neath the fascial flap. A negative pressure drain was
placed in the tissue pocket until the volume of drainage
was less than 10 ml.
Tissue expansion. After the fascial flap transfer, an
Ultrasound Doppler was used to identify the patency of
the microvascular anastomosis. With confirming persist-
ence of pulsation in the pedicle, tissue expansion begun 2
weeks postoperatively and was performed twice a week
with 5–10% expansion of the total volume of the ex-
pander. When the expanded area of skin was estimated
over the size of the tissue defect, expansion was stopped
and the flap transfer was planned.
Inset of the prefabricated flap. Angiogram or Ultra-
sonic Doppler was used to assess the persistence of blood
flow in the vascular pedicles and neovascularization
induced by flap prefabrication before the flap transfer
procedure. The prefabricated cervicothoracic skin flap
was then raised from the underlying tissue expander, and
the vascular pedicles were identified. Dissection was per-
formed carefully because of fibrous tissue around the
pedicle. After the scar tissue in the face and neck was
removed and the fibrous synechiae was completely
released, the prefabricated skin flap was rotated to cover
the skin defect based on the pedicle of lateral circumflex
femoral vessels. The donor site was primarily closed.
Figure 1. Graphical diagram of vascular carrier. The fascial flap
nourished by the descending branch of the lateral femoral circum-
flex vessels. The descending branch gives off up to 10 branches
that penetrate the deep surface of the proximal and middle thirds of
the vastus lateralis muscle in the company of supplying nerves.
[Color figure can be viewed in the online issue, which is available
at www.interscience.wiley.com.]
516 Li et al.
Microsurgery DOI 10.1002/micr

RESULTS
The average size of harvested lateral thigh fascial
flaps was 6.5 3 11.7 cm (ranging from 3 3 8 cm to 7 315 cm). The average length of the vascular pedicles was
5.1 cm (ranging from 3 to 6 cm). After a mean interval
of flap prefabrication for 21.5 weeks (ranging from 10 to
32 weeks), the tissue expanders were filled to a mean
volume of 1,685 ml (ranging from 830 to 2,670 ml).
The sizes of raised prefabricated skin flaps ranged
from 12 3 15 cm to 15 3 32 cm, and all flaps could
covered and resurfaced the entire defects of the face and
neck. All flaps survived after transfer. Varied degrees of
venous congestion were observed after flap insets in all
cases. Three flaps with venous congestion were treated
by the technique of venous bloodletting from the flap
edges, whereas other flaps did not receive any treatment.
Marginal skin necrosis (<3 cm) was eventually found in
two cases. The wounds healed with dressing changes.
Three flaps underwent secondary debulking procedures
for the skin pedicles of flap rotation. In follow-ups rang-
ing from 3 to 21 months, the texture and color of trans-
ferred flaps were found matched to the adjacent skin
around the repair sites. No complications were observed
in either thigh or cervicothoracic donor sites. All patients
were satisfied with the functional and esthetic outcomes.
Case Report
Case 1. A 40-year-old man sustained a severe burn
injury over 40% of his total body surface in a forest fire.
The patient received burn treatment for body in a burn
unit, but requested further facial reconstruction in our
institution. The patient presented a facial disfigurement
caused by hypertrophic scarring in the perioral, nasal,
and mandibular regions, and functional disability with
difficulty in nasal breathing and mouth eating (Fig. 2,
above). The patient underwent a four-step procedure for
facial resurfacing. A 7 3 12 cm lateral thigh fascial flap
based on the descending branches of the lateral femoral
circumflex vessels was transferred to the cervicothoracic
area, and the vascular pedicles of flap were anastomosed
to the right superior thyroid vessels. The flap was inset
over a 600-ml rectangular tissue expander under the cer-
vicothoracic skin (Fig. 3, above). The expanders were
Figure 2. Preoperative and postoperative views in case 1. Above: Preoperative views of hypertrophic scarring in the perioral, nasal, and
mandibular areas. Below: Postoperative views for appearance of nose and mouth after debulking procedure. [Color figure can be viewed in
the online issue, which is available at www.interscience.wiley.com.]
Prefabricated Flap for Face Resurfacing 517
Microsurgery DOI 10.1002/micr
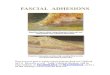
expanded twice a week until a total volume of 1,800 ml
was achieved. At 6 months after flap prefabrication, the
facial scars were removed and the prefabricated cervico-
thoracic skin flap with 21 3 20 cm in size was raised
and transferred for coverage of lower face including
entire mouth and nose (Fig. 3, Below). The flap survived
after surgery. However, a slight venous congestion was
developed postoperatively, which subsided in 2 weeks
without special treatment. Three weeks after flap transfer,
the flap was partially divided to form the mouth and
nose. At the fourth postoperative month, the patient
underwent debulking procedure for the skin pedicle. At
7 months of follow-up, the patient could breathe and eat
without difficulty and was satisfied with the outcomes
(Fig. 2, below).
Case 2. A 35-year-old woman had extensive scarring
and disfigurement of chin and cheek caused by burn and
requested a improved aesthetic appearance (Fig. 4,
above). A flap was prefabricated over the right cervico-
thoracic area by inset of a later thigh fascial flap with the
descending branches of the lateral femoral circumflex
vessels as the vascular pedicles. The vessels were anasto-
mosed to the facial artery and vein. A tissue expander
was placed under the lateral thigh fascial flap. Six months
after flap prefabrication, the total volume of tissue expan-
sion was 1,240 ml. The angiogram showed the extensive
neoangiogenesis in the prefabrication area. The facial
scar was excised and the prefabricated cervicothoracic
skin flap with 28 3 12 cm in size was dissected based
on its vascular pedicles and then rotated to cover the skin
defect. Both sides of the lower third of cheek, chin, and
lower lip were resurfaced with the flap (see Fig. 5). The
flap survived after surgery. A mild venous congestion of
flap presented in the first postoperative week. The venous
congestion was released by multiple puncturing on the
marginal part of flap with a needle and topical applica-
tion of heparin. Partial necrosis occurred at the distal
margin of flap and the wound healed after dressing
Figure 3. Prefabricated skin flap for face resurfacing in case 1, Above, left: Harvest of the lateral thigh fascial flap with the descending
branches of the lateral femoral circumflex vessels as the pedicles. Above, center: Design for the position of the tissue expander, the free
fascia flap, and the recipient vessels (superior thyroid vessels). Above, right: Pedicles of the fascial flap anastomosed to the right superior
thyroid vessels. Below, left: Expansion of the prefabricated skin flap at 6 months before harvest. Below, center: Elevation of the prefabri-
cated skin flap. Below, right: Inset of the pedicled prefabricated skin flap. [Color figure can be viewed in the online issue, which is available
at www.interscience.wiley.com.]
518 Li et al.
Microsurgery DOI 10.1002/micr

Figure 4. Preoperative and postoperative views in case 2. Above: Preoperative appearance of the extensive scar on the chin and cheek.
Below: Postoperative views after facial resurfacing with mild scar remaining in the margin of right cheek. [Color figure can be viewed in the
online issue, which is available at www.interscience.wiley.com.]
Figure 5. Prefabricated skin flap for face resurfacing in case 2. (a) Arteriogram showed the patency of the vascular pedicles (arrow) and
the neoangiogenesis area over the transferred fascia flap 6 months after prefabrication. (b) Design of the pedicled flap based on the
implanted vessels. (c) Rotation of the prefabricated cervicothoracic skin flap (1, supraclavicular vessels; 2, facial vessels). (d) Inset of the
prefabricated skin flap and primary close of the donor site. (e) Venous congestion at first day after operation. (f) Venous congestion
released by puncturing with a needle and topical application of heparin. (g) Partial necrosis at the distal margin of the flap and wound
healing with mild scar formation 2 weeks postoperatively. [Color figure can be viewed in the online issue, which is available at www.
interscience.wiley.com.]
changes (see Fig. 5). The patients were satisfied with the
functional and aesthetic outcomes at 4 months of follow-
up (Fig. 4, below).
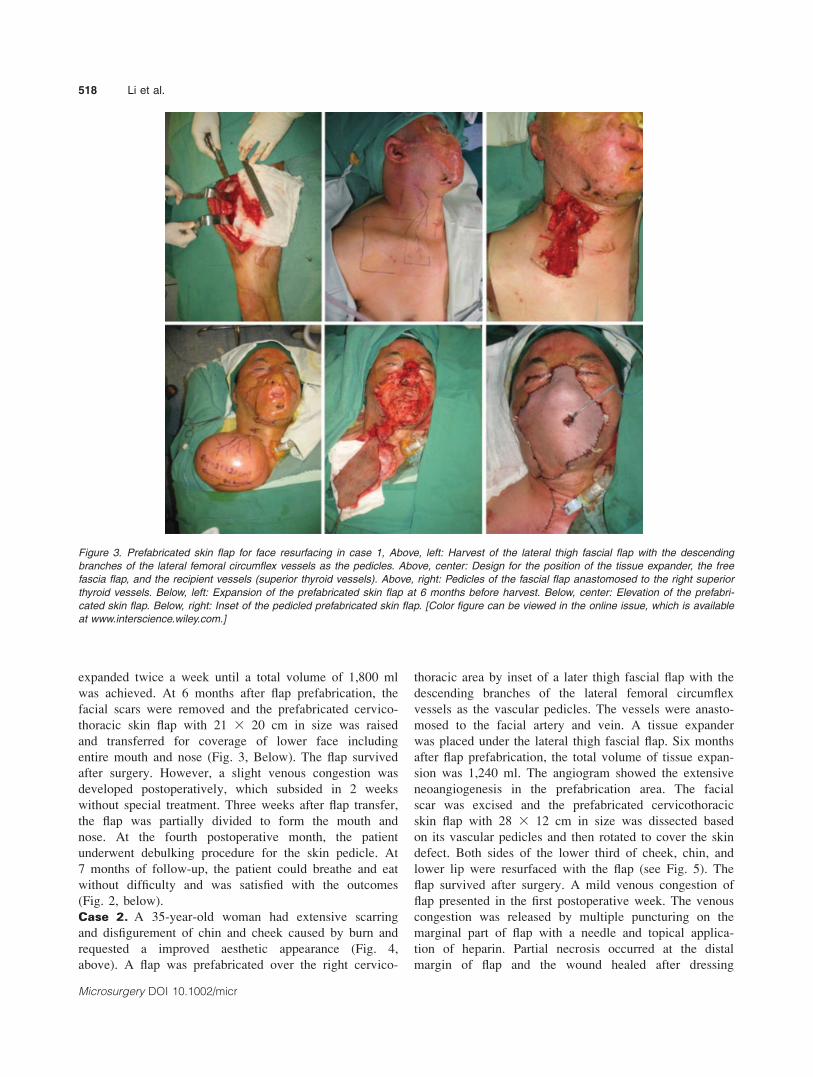
Case 3. A 28-year-old woman suffered from the burn
injury on the face, neck, extremities, and chest. The
wound was initially treated by skin grafting. The patient
developed mentosternal contracture with an unstable ulcer
1 year after injury (Fig. 6, above). A skin flap was pre-
fabricated at the right shoulder region where a relatively
healthy patch of skin remained. The prefabricated skin
flap was nourished by a 3 3 8 cm lateral thigh fascial
flap based on the descending branches of the lateral fem-
oral circumflex vessels that were anastomosed to the
superior thyroid vessels. The fascial flap was fixed to a
subcutaneous pocket and a 300-ml tissue expander was
placed underneath the fascial flap. Three months after
flap prefabrication, the vasculature of flap was identified
by an Ultrasonic Doppler examination. A 16 3 12 cm
prefabricated skin flap was then raised and transferred to
the skin defects at chin and neck after scar resections
(see Fig. 7). The donor site was primarily closed. The
postoperative course was uneventful. Complete release of
mentosternal contracture was achieved at 3 months of
follow-up (Fig. 6, below).
DISCUSSION
Reconstruction and resurfacing of massive soft tissue
deformity in the face and neck is a great challenge to
reconstructive surgeons.1,2,10–12 Besides coverage of the
defects, the major aim of reconstruction is to restore the
facial aesthetics and function. Flap prefabrication is a rel-
atively new and evolving technique that provides a
ready-for-use alternative when traditional options are not
available. With this technique, the tissue suitable for face
and neck reconstruction and resurfacing may be used for
flap prefabrication. When compared with free flaps, the
prefabricated flap could be achieved with improved prop-
erties to aesthetic and functional match of the recipient
site. Moreover, the donor site morbidity could be signifi-
cantly reduced. The prefabricated flap may be a valuable
tool for reconstruction of large defects in the head and
neck region where aesthetics and function are highly
demanded. The disadvantage of this technique is that the
Figure 6. Preoperative and postoperative views in case 3. Above: Postburn mentosternal contracture with skin ulcer after skin grafts.
Below: Improvement of the range of motion after complete release of synechiae and reconstruction with transfer of the prefabricated skin
flap 3 month postoperatively. [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
520 Li et al.
Microsurgery DOI 10.1002/micr

patient suffers from multiple procedures in delayed
stages.13 However, this complex technique is worthwhile
for achieving improved results of reconstruction. Clini-
cally, tissue expansion technique is often combined with
flap prefabrication procedure. Tissue expansion increases
the size and vascularity of the prefabricated flap, while
allowing primary closure of the donor site.17 In addition,
tissue expansion could reduce the thickness of subcutane-
ous tissue and dermis,2,18 which would be more suitable
for the face and neck resurfacing.
The skin flap prefabrication means creating an axial
pattern flap suitable for either pedicled or free-flap trans-
fer with an angiogenic response after vascular carrier im-
plantation into the subdermal level of donor tissue.9–13
The prefabricated skin flap mainly consisted of two ele-
ments, the donor site selection and the vascular carrier
creation. For massive facial resurfacing, the ideal donor
site is cervicothoracic skin because its color and texture
match the recipient site. Ideally, a vascular carrier does
not contain any tissue other than a densely spread capil-
lary network, and it is maintained with a very long pedi-
cle with large-caliber blood vessels that facilitates micro-
vascular anastomosis. Several tissues, such as muscle,19
fascia,11,20–22 omentum,23 and vessel bundles13,24,25 have
been used as the carriers. Kimura et al.22 reported that
the vessel bundle and muscle are not adequate as carriers
for making a thin and large prefabricated skin flap. The
vascularized fascia may be the most suitable tissue as a
carrier for making a thin prefabricated skin flap. There
have been several reports that described use of the tem-
poroparietal fascia,11,20 radial forearm fascia,21 and trans-
versalis fascia22 for flap prefabrication.
In this report, we describe a new vascular carrier for
prefabrication of a cervicothoracic skin flap with a fascial
flap nourished by the descending branches of the lateral
femoral circumflex vessels. The descending branch of the
lateral femoral circumflex artery is commonly used as the
pedicle for supplying the anterolateral thigh flap, which is
one of the most versatile and reliable tools in soft-tissue
reconstruction.15,26–29 The descending branch of the lat-
eral femoral circumflex artery was also used as an arterial
graft for the coronary artery bypass grafting.14,30 Pribaz
et al.10–12 described use of the descending branches of
the lateral femoral circumflex vessels as a vascular carrier
in flap prefabrication. The vascular pedicle along with the
muscle cuff was used to provide blood supply to the
Figure 7. Prefabricated skin flap for neck reconstruction in case 3. Above, left: Identification of the vessels by Ultrasonic Doppler blood-
flow signals (arrow) 3 months after implantation of the vascular carrier. Above, right: Design of the pedicled skin flap based on the
implanted vessels. Below, left: Elevation of the prefabricated skin flap with vascular pedicles (arrow). Below, right: Inset of the prefabricated
skin flap and primary close of the donor site. [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.
com.]
Prefabricated Flap for Face Resurfacing 521
Microsurgery DOI 10.1002/micr

overlying skin. However, this technique would make a
prefabricated flap bulky because the muscle content was
included. We chosen the fascial flap nourished by the de-
scending branches of the lateral femoral circumflex ves-
sels as the vascular carrier based on: 1) the descending
branches have adequate length and diameter, which facili-
tates anastomosis in the skin flap prefabrication and flap
rotation in the reconstruction; 2) although anatomical var-
iants of the lateral femoral circumflex artery have been
reported,30,31 in our experience, the main trunk of the de-
scending branches had a constant location in the groove
between the rectus femoris and vastus lateralis muscles;
3) the fascia usually remains healthy and available even
in the severe burn injury because of its deep location; 4)
it is a relatively simple procedure for harvesting a fascial
flap with at least 6 3 8 cm in size without damaging the
accompanying nerve.32 In our experience, no notable
complications were found at the donor sites after harvest
of fascial flaps.
Selection of the recipient vessels in the flap prefabrica-
tion is important for achieving good results in facial resur-
facing. The recipient vessels near the region of deformity
or disfigurement in the face and neck areas allow transfer
of the pedicled prefabricated flap without performing a
complex manipulation. In our series, both the facial artery
and superior thyroid artery were selected as the recipient
arteries, and either facial vein or a branch of the internal
jugular vein was chosen as the recipient vein.
The supraclavicular island flap described by Lamberty
and Pallua et al.3–7 has been used for facial reconstruc-
tion, providing satisfactory results without need of micro-
vascular anastomoses. However, the supraclavicular island
flap is designed based on the supraclavicular vessels. The
pivot of the supraclavicular flap is about 7–12 cm lower
than the facial artery and the superior thyroid artery,
which cause difficulty for flap to cross the median line to
reach distal areas of defect in the face. The prefabricated
skin flap described in our report was supplied by either
the facial artery or the superior thyroid artery. Therefore,
the pivot of prefabricated flap was more close to the
facial defect so that the flap was transferred without ten-
sion. Furthermore, the technique of flap prefabrication
allowed us to have more choices for selection of the do-
nor sites in areas of neck, shoulder, and upper chest.
Thus, the flap prefabrication technique is able to provide
sufficient tissue for optimal face reconstruction and resur-
facing. The prefabricated supraclavicular flap with thora-
coacromial vessels was introduced by Margulis et al.25
for reconstruction of the anterior cervical contractures.
However, because of the low position of the pivot of
rotation and the short length of the vessel pedicle, this
flap based on the implanted thoracoacromial vessels could
be difficult for reconstruction of the upper and middle
face areas.
The skin flap prefabrication is based on neovasculari-
zation between the implanted vascular carries and the
overlying skin of donor site. Nevertheless, if the process
of neovascularization is insufficient, the risk of partial
flap necrosis will inevitably occur. In our series, the arte-
riogram studies showed that the vascularized area was la-
ger than the initial size of the transferred fascia flap.
However, it was difficult to define the exact size of the
flap that could be transferred without risk of necrosis. Ex-
perimental and clinical studies have demonstrated that
survival of the prefabricated skin flap with tissue
expansion was improved as the prefabrication period was
prolonged. Under safety consideration, a longer pre-
fabrication interval with overexpansion was recom-
mended.11,33–34 Clinically, moderate overexpansion could
modify the characters of the flap and increase the surface
area.35 In our series, overexpansion with long interval could
provide an abundant tissue to facilitate donor sites closure.
The venous congestion is another common problem
after transfer of the prefabricated skin flap. Pribaz and
Guo12 postulated that the venous congestion may be
caused by unequal neovascularization of the lower venous
pressure compared with the higher arterial pressure from
the vascular pedicles. This problem could be ameliorated
with different techniques, such as flap delay, prolonging
prefabrication interval, increasing the contact area
between the pedicle and overlyingskin, temporary leech-
ing (chemical or medicinal), avoiding flap folding, and
performing an additional venous anastomosis using a sub-
cutaneous vein in the prefabricated flap.12 In our series,
many of these maneuvers were attempted. However, var-
ied degrees of venous congestion were found in all trans-
ferred prefabricated skin flaps. The venous congestion
was found more serious in the distal area of flap. The
size of harvested prefabricated flap over the implanted
fascia vascular carrier could be the another cause of ve-
nous congestion. From our experience, we suggest that
size of prefabricate flap should be designed carefully
based on the size of implanted vascular fascia flap to
ensure the flap survival. The ratio of sizes between the
harvested prefabricated flap and implanted vascular fascia
flap needs to be further studied.
In summary, we report use of a lateral thigh fascial
flap nourished by the descending branches of the lateral
femoral circumflex vessels as the vascular carrier for the
skin flap prefabrication, based on its thinner thickness
and dense capillary network of the fascial flap. The cervi-
cothoracic skin flap prefabricated by the vascularized
fascial flap and tissue expender matches the principle of
‘‘matching, large size, and thinner thickness’’ in flap
selection, it and is reliable and versatile alternative in
reconstruction and resurfacing of massive soft tissue
defects of the face and neck. The venous congestion and
distal necrosis of the prefabricated flap are problems in
522 Li et al.
Microsurgery DOI 10.1002/micr

the flap transfer. Improvement of flap survival and the
ideal size of flap for transfer need to be further investi-
gated.
REFERENCES
1. Menick FJ. Facial reconstruction with local and distant tissue: Theinterface of aesthetic and reconstructive surgery. Plast Reconstr Surg1998;102:1424–1433.
2. MacLennan SE, Corcoran JF, Neale HW. Tissue expansion in headand neck burn reconstruction. Clin Plast Surg 2000;27:121–132.
3. Lamberty BG. The supra-clavicular axial patterned flap. Br J PlastSurg 1979;32:207–212.
4. Pallua N, Machens HG, Rennekampff O, Becker M, Berger A. Thefasciocutaneous supraclavicular artery island flap for releasing post-burn mentosternal contractures. Plast Reconstr Surg 1997;99:1878–1884.
5. Pallua N, Magnus Noah E. The tunneled supraclavicular island flap:An optimized technique for head and neck reconstruction. PlastReconstr Surg 2000;105:842–851.
6. Pallua N, von Heimburg D. Pre-expanded ultra-thin supraclavicularflaps for (full-) face reconstruction with reduced donor-site morbidityand without the need for microsurgery. Plast Reconstr Surg2005;115:1837–1844.
7. Vinh VQ, Ogawa R, Van Anh T, Hyakusoku H. Reconstruction ofneck scar contractures using supraclavicular flaps: Retrospectivestudy of 30 cases. Plast Reconstr Surg 2007;119:130–135.
8. Rose EH. Aesthetic restoration of the severely disfigured face inburn victims: A comprehensive strategy. Plast Reconstr Surg1995;96:1573–1585.
9. Khouri RK, Upton J, Shaw WW. Principles of flap prefabrication.Clin Plast Surg 1992;19:763–771.
10. Pribaz JJ, Fine NA. Prefabricated and prelaminated flaps for headand neck reconstruction. Clin Plast Surg 2001;28:261–272.
11. Pribaz JJ, Fine N, Orgill DP. Flap prefabrication in the head andneck: A 10-year experience. Plast Reconstr Surg 1999;103:808–820.
12. Pribaz JJ, Guo L. Flap prefabrication and prelamination in head andneck reconstruction. Semin Plast Surg 2003;17:351–362.
13. Morrison WA, Penington AJ, Kumta SK, Callan P. Clinical applica-tions and technical limitations of prefabricated flaps. Plast ReconstrSurg 1997;99:378–385.
14. Wang Wl, Cai KC, Zhong SZ, Wang WJ. Study on feasibility ofusing the descending branch of lateral circumflex femoral artery asan autograft for coronary artery bypass grafting. J Reg Anat OperSurg 2000;4:309–312.
15. Ribuffo D, Cigna E, Gargano F, Spalvieri C, Scuderi N. The inner-vated anterolateral thigh flap: Anatomical study and clinical implica-tions. Plast Reconstr Surg 2005;115:464–470.
16. Kawai K, Imanishi N, Nakajima H, Aiso S, Kakibuchi M, HosokawaK. Vascular anatomy of the anterolateral thigh flap. Plast ReconstrSurg 2004;114:1108–1117.
17. Maitz PK, Pribaz JJ, Hergrueter CA. Impact of tissue expansion onflap prefabrication: An experimental study in rabbits. Microsurgery1996;17:35–40.
18. Leighton WD, Russell RC, Feller AM, Eriksson E, Mathur A, ZookEG. Experimental pretransfer expansion of free-flap donor sites. II.Physiology, histology, and clinical correlation. Plast Reconstr Surg1988;82:76–87.
19. Shintomi Y, Ohura T. The use of muscle vascularized pedicle flaps.Plast Reconstr Surg 1982;70:725–735.
20. Khouri RK, Ozbek MR, Hruza GJ, Young VL. Facial reconstructionwith prefabricated induced expanded (PIE) supraclavicular skin flaps.Plast Reconstr Surg 1995;95:1007–1015.
21. Teot L, Cherenfant E, Otman S, Giovannini U. Prefabricated vascu-larized supraclavicular flaps for face resurfacing after postburns scar-ring. Lancet 2000;355:1695–1696.
22. Kimura N, Hasumi T, Satoh K. Prefabricated thin flap using thetransversalis fascia as a carrier. Plast Reconstr Surg 2001;108:1972–1980.
23. Erol OO, Spira M. Reconstructing the breast mound employing asecondary island omental skin flap. Plast Reconstr Surg 1990;86:510–518.
24. Yao ST. Vascular implantation into skin flap: Experimental studyand clinical application: A preliminary report. Plast Reconstr Surg1981;68:404–410.
25. Margulis A, Agam K, Icekson M, Dotan L, Yanko-Arzi R, NeumanR. The expanded supraclavicular flap, prefabricated with thoracoa-cromial vessels, for reconstruction of postburn anterior cervical con-tractures. Plast Reconstr Surg 2007;119:2072–2077.
26. Song YG, Chen GZ, Song YL. The free thigh flap: A new free flapconcept based on the septocutaneous artery. Br J Plast Surg 1984;37:149–159.
27. Shieh SJ, Chiu HY, Yu JC, Pan SC, Tsai ST, Shen CL. Free antero-lateral thigh flap for reconstruction of head and neck defects follow-ing cancer ablation. Plast Reconstr Surg 2000;105:2349–2357.
28. Koshima I. Free anterolateral thigh flap for reconstruction of headand neck defects following cancer ablation. Plast Reconstr Surg2000;105:2358–2360.
29. Wei FC, Jain V, Celik N, Chen HC, Chuang DC, Lin CH. Have wefound an ideal soft-tissue flap? An experience with 672 anterolateralthigh flaps. Plast Reconstr Surg 2002;109:2219–2226.
30. Fabbrocini M, Fattouch K, Camporini G, DeMicheli G, Bertucci C,Cioffi P, Mercogliano D. The descending branch of lateral femoralcircumflex artery in arterial CABG: Early and midterm results. AnnThorac Surg 2003;75:1836–1841.
31. Fukuda H, Ashida M, Ishii R, Abe S, Ibukuro K. Anatomical var-iants of the lateral femoral circumflex artery: An angiographic study.Surg Radiol Anat 2005;27:260–264.
32. Kimata Y, Uchiyama K, Ebihara S, Nakatsuka T, Harii K. Anatomicvariations and technical problems of the anterolateral thigh flap: Areport of 74 cases. Plast Reconstr Surg 1998;102:1517–1523.
33. Kostakoglu N, Manek S, Green CJ. The development of neovascu-larisation in flap perfabrication with vascular implantation: Anexperimental study. Br J Plast Surg 1997;50:428–434.
34. The Hoang N, Kloeppel M, Staudenmaier R, Schweinbeck S, BiemerE. Neovascularization in prefabricated flaps using a tissue expanderand an implanted arteriovenous pedicle. Microsurgery 2005;25:213–219.
35. Di Mascio D, Castagnetti F, Mazzeo F, Caleffi E, Dominici C. Over-expansion technique in burn scar management. Burns 2006;32:490–498.
Prefabricated Flap for Face Resurfacing 523
Microsurgery DOI 10.1002/micr


























![Fascial Flap Reconstruction of the Hand a Single.25[1]](https://img.dokumen.tips/doc/110x75/55147566497959ee1d8b4746/fascial-flap-reconstruction-of-the-hand-a-single251.jpg)