Embed Size (px)
Citation preview
Extensive Resection Reconstruction Using Pectoralis Major Myocutaneous Flap
JOHN K. PONNAT
A case of extensive resection of an oral--oropharyngeal tumour and the reconstruction using pectoralis major myocutaneous flap is described.
The use of myocutaneous flaps have become common ever since the true introduction of this techni- que by Ariyan for a sebaceous gland carcinoma of the orbit (Ariyan, 1979). Advanced cancer of the tongue is perhaps one of the most painful cancers and in such cases palliative radiotherapy does not seem to neither improve the pro- gnosis nor the suffering. The very thought of the cancer pain and the versatality of myocutaneouts flaps make the surgeon think of an extensive resection--repair.
The vascular supply to the pectoralis major muscle or the flap is chiefly the pectoral branch of the acromiothoracic artery. Variations in technique regarding raising of the pectoralis major myocutaneous flap are essentially different in only the size of the pedicle.
Case Report
A 40 year old man reported to the E.N.T. Department of the Christian Medical College and Hospital, Ludhiana, with com- plaints of ulceration and pain tongue, of 3 months duration. Clinical examination of the case revealed an ulcerative growth with induration involving the anterior two-thirds of tongue bilaterally, with involvement of posterior one-third on right side, with exten-
Address for correspondence :
*PONNAT J. K., Lecturer, Department of E.NoT., Christain Medical College
Hospital, Ludhiana, Punjab, India.
sion of the lesion to the lower pole of right tonsil, right lower molar and pre-molar gums and adjacent floor of oral cavity. Two right upper deep cervical nodes were palpable, each measuring 2 cms x 1 cm non-tender, firm and mobile. There was no evidence of distant metastasis. A clinical dia- gnosis of carcinoma tongue stage IV (T N M ) Was made. A biopsy from the ulcer over the right margin of the tongue was taken and the histopathological examination of the specimen revealed a moderately differentiated infiltrating squa- mous cell carcinoma. Chest X-ray was normal.
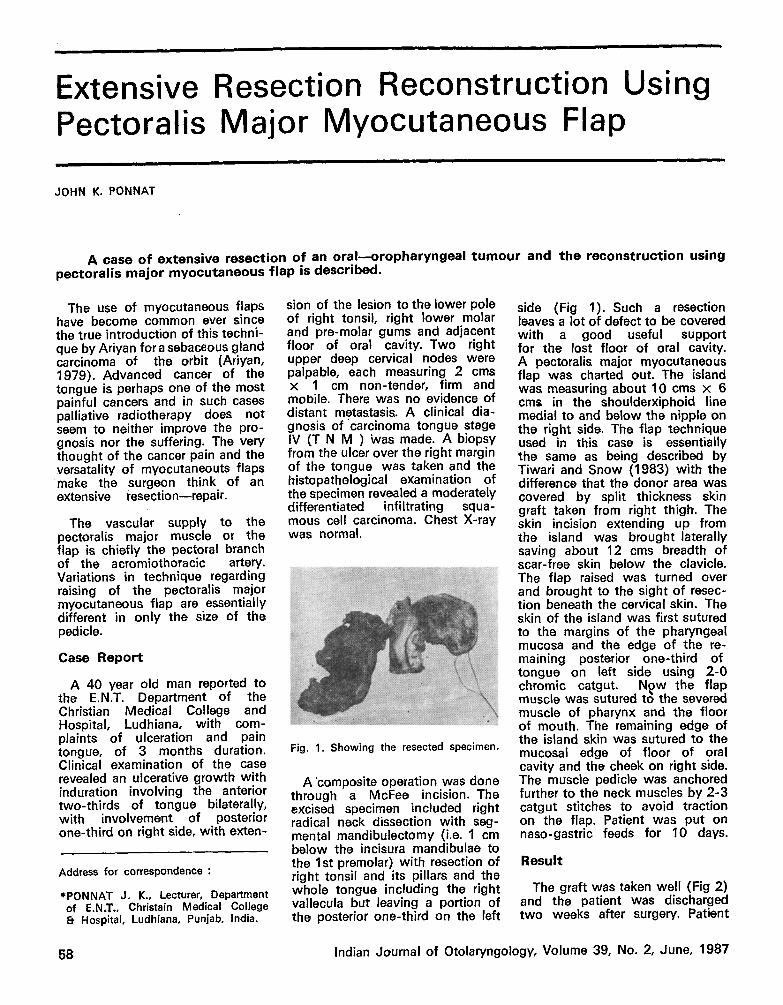
Fig. 1. Showing the resected specimen.
A 'composite operation was done through a McFee incision. The excised specimen included right radical neck dissection with seg- mental mandibulectomy (i.e. 1 cm below the incisura mandibulae to the 1st premolar) with resection of right tonsil and its pillars and the whole tongue including the right vallecula but leaving a portion of the posterior one-third on the left
side (Fig 1). Such a resection leaves a lot of defect to be covered with a good useful support for the lost floor of oral cavity. A pectoralis major myocutaneous flap was charted out. The island was measuring about 10 cms x 6 cms in the shoulderxiphoid line medial to and below the nipple on the right side. The flap technique used in this case is essentially the same as being described by Tiwari and Snow (1983) with the difference that the donor area was covered by split thickness skin graft taken from right thigh. The skin incision extending up from the island was brought laterally saving about 12 cms breadth of scar-free skin below the clavicle. The flap raised was turned over and brought to the sight of resec- tion beneath the cervical skin. The skin of the island was first sutured to the margins of the pharyngeal mucosa and the edge of the re- maining posterior one-third of tongue on left side using 2-0 chromic catgut. N~w the flap muscle was sutured t6 the severed muscle of pharynx and the floor of mouth. The remaining edge of the island skin was sutured to the mucosal edge of floor of oral cavity and the cheek on right side. The muscle pedicle was anchored further to the neck muscles by 2-3 catgut stitches to avoid traction on the flap. Patient was put on naso-gastric feeds for 10 days.
Result
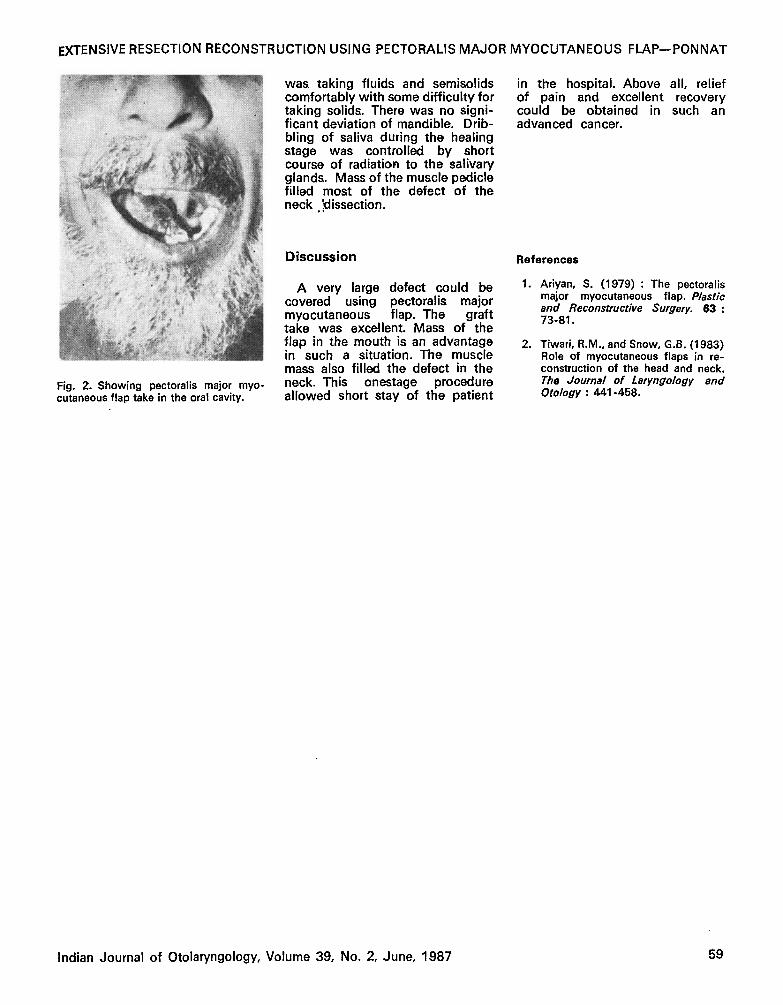
The graft was taken well (Fig 2) and the patient was discharged two weeks after surgery. Patient
58 Indian Journal of Otolaryngology, Volume 39, No. 2, June, 1987
EXTENSIVE RESECTION RECONSTRUCTION USING PECTORALIS MAJOR MYOCUTANEOUS FLAP--PONNAT
Fig. 2. Showing pectoralis major myo- cutaneous flap take in the oral cavity.
was taking fluids and semisolids comfortably with some difficulty for taking solids. There was no signi- ficant deviation of mandible. Drib- bling of saliva during the healing stage was controlled by short course of radiation to the salivary glands. Mass of the muscle pedicle filled most of the defect of the neck .Idissection.
Discussion
A very large defect could be covered using pectoralis major myocutaneous flap. The graft take was excellent. Mass of the flap in the mouth is an advantage in such a situation. The muscle mass also filled the defect in the neck. This onestage procedure allowed short stay of the patient
in the hospital. Above all, relief of pain and excellent recovery could be obtained in such an advanced cancer.
References
1. Ariyan, S. (1979) : The pectoralis major myocutaneous flap. Plastic and Reconstructive Surgery. 63: 73-81.
2. Tiwari, R.M., and Snow, G.B. (1983) Role of myocutaneous flaps in re- construction of the head and neck. The Journal of Laryngology and Otology : 441-458.
Indian Journal of Otolaryngology, Volume 39, No. 2, June, 1987 59





























