Embed Size (px)
Citation preview

This article was downloaded by: [Stony Brook University]On: 24 October 2014, At: 12:47Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH,UK
Journal of Ethnic And CulturalDiversity in Social WorkPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/wecd20
Exploring Dimensions ofCulturally Sensitive ClinicalStyles with LatinosYuhwa Eva Lu PhD a , Kurt C. Organista PhD b ,Salvador Manzo Jr. MSW, Lisa Wong, MSW , Lisa WongMSW & Jessica Phung BSWa Ehrenkranz School of Social Work , New YorkUniversity , USAb School of Social Welfare , University of California ,Berkeley, USAPublished online: 11 Oct 2008.
To cite this article: Yuhwa Eva Lu PhD , Kurt C. Organista PhD , Salvador ManzoJr. MSW, Lisa Wong, MSW , Lisa Wong MSW & Jessica Phung BSW (2001) ExploringDimensions of Culturally Sensitive Clinical Styles with Latinos, Journal of Ethnic AndCultural Diversity in Social Work, 10:2, 45-66, DOI: 10.1300/J051v10n02_04
To link to this article: http://dx.doi.org/10.1300/J051v10n02_04
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all theinformation (the “Content”) contained in the publications on our platform.However, Taylor & Francis, our agents, and our licensors make norepresentations or warranties whatsoever as to the accuracy, completeness,or suitability for any purpose of the Content. Any opinions and viewsexpressed in this publication are the opinions and views of the authors, andare not the views of or endorsed by Taylor & Francis. The accuracy of theContent should not be relied upon and should be independently verified withprimary sources of information. Taylor and Francis shall not be liable for any

losses, actions, claims, proceedings, demands, costs, expenses, damages,and other liabilities whatsoever or howsoever caused arising directly orindirectly in connection with, in relation to or arising out of the use of theContent.
This article may be used for research, teaching, and private study purposes.Any substantial or systematic reproduction, redistribution, reselling, loan,sub-licensing, systematic supply, or distribution in any form to anyone isexpressly forbidden. Terms & Conditions of access and use can be found athttp://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

Exploring Dimensionsof Culturally Sensitive Clinical Styles
with Latinos
Yuhwa Eva LuKurt C. Organista
Salvador Manzo, Jr.Lisa Wong
Jessica Phung
ABSTRACT. This study sought to identify dimensions of culturallysensitive clinical practice by comparing the personal clinical styles ofLatino and non-Latino clinicians, and their clinical decisions in respectto Latino immigrant clients. A combination of qualitative and quantita-tive methods were used. Sixty Latino American clinicians and 47non-Latino (White) clinicians in Northern California completed theAchieving Styles Inventory (ASI) which yields information on direct, in-strumental and relational styles. Demographic data were obtained aswell as information on language proficiency and years of clinical experi-ence. Statistical analysis included uses of t-test, ANOVA, and multipleregression analysis and revealed significant differences between the twogroups in personal achieving styles within all three domains. There wereno significant differences on the demographic variables. Nine clinicianmembers of each ethnic group were interviewed in-depth throughnon-directive interviewing styles to assess their clinical decision making
Yuhwa Eva Lu, PhD, is Associate Professor, Ehrenkranz School of Social Work,New York University. Kurt C. Organista, PhD, is Associate Professor, School of So-cial Welfare, University of California, Berkeley. Salvador Manzo, Jr., MSW, LisaWong, MSW, and Jessica Phung, BSW, are social workers practicing in Bay Area.
The authors wish to thank Dr. Elfriede Schlesinger for her helpful suggestions andcomments on the manuscript.
Journal of Ethnic & Cultural Diversity in Social Work, Vol. 10(2) 2001http://www.haworthpressinc.com/store/product.asp?sku=J051
2001 by The Haworth Press, Inc. All rights reserved. 45
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

via use of a case vignette. Content analysis pointed to similarities anddifferences in proposed assessment and intervention strategies. TheLatino group displayed more culturally relevant interpretations. Thenon-Latino clinicians were more directive and instrumental than theLatinos who put more emphasis on self disclosure, case management,use of Spanish with the client, and crisis intervention. This finding isconsistent with both the quantitative data analysis of ASI hypothesesand the expected linguistic/cultural findings of the qualitative contentanalysis. Bilingual non-Latino White clinicians showed more culturalsensitivity and competence than the monolingual non-Latino clini-cians. These findings suggest that linguistic/cultural match and linguis-tic/cultural compatibility are important in cross-cultural clinicalpractice. [Article copies available for a fee from The Haworth Document DeliveryService: 1-800-HAWORTH. E-mail address: <[email protected]>Website: <http://www.HaworthPress.com> © 2001 by The Haworth Press, Inc. Allrights reserved.]
KEYWORDS. Clinical cultural competence, clinicians’ achieving styles,Latino vs. non-Latino clinicians, Latino immigrant clients/families, so-cial work practices, cultural sensitivity
INTRODUCTION
The purpose of this study was to explore dimensions of culturally sensitiveclinical practice by comparing the achieving styles, clinical interviewing pro-cesses, and clinical decisions of Latino and non-Latino White clinicians work-ing with Latino clients. This research represents an effort to elucidate specificdimensions of culturally sensitive clinical services. By specifying componentsof culturally competent psychotherapy, the mental health and social serviceprofessions will be better able to train clinicians to meet the mental health needsof diverse populations. Cultural sensitivity involves clinicians’ appropriate re-sponses to clients’ needs as derived from culturally specific dispositions.
The study replicated key aspects of Lu’s work (1994, 1996) that comparedbilingual/bicultural Asian American clinicians and non-Asian American clini-cians with regard to achieving styles and their approaches to clinical work withAsian American clients. The term “achieving styles” refers to preferred strate-gies or characteristic styles that individuals use to accomplish a wide variety oftasks and goals (Lipman-Blumen, 1987). Lipman-Blumen’s (1987) AchievingStyles Inventory (ASI) divides achieving styles into nine distinctive styles that
46 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

are grouped into three primary domains: (1) direct (competitive, power, intrin-sic); (2) instrumental (personal, social, reliant); and (3) relational (collabora-tive, contributory, vicarious).
Clinicians often have little awareness of their own personal achieving styleswhich closely link and relate to their own clinical practice. According toLipman-Blumen (1987), people with direct achieving styles tend to be highlyindependent and individualistic, confronting goals by taking charge and byrelying on competitive and power-driven methods. These individuals tend to(1) tightly control how goals are defined and the means by which to achievethem, (2) offer direct advice as a helping authority for clients, and (3) be highlyindependent, individualistic, and confront problems by taking charge, relyingon intrinsic strength and direction oriented methods. They are inclined to exertinfluence on how treatment goals are defined and on the means to achievethem. Direct problem-solving approaches are often preferred. Individuals withinstrumental achieving styles tend to (1) reach goals by extensive networkingand by relying on their own status, influence, and personal and professional re-lationships to accomplish tasks, (2) reach goals by extensive networking andby relying on their own professional knowledge and status to influence per-sonal and professional relationships to accomplish treatment goals, and(3) rely on clients to assume partial or full responsibility for their goals.Finally, individuals with relational styles tend to rely on collaborative actionsand are highly contributory to the goals of others, often to the extent of sharingvicariously in the accomplishments of others. These individuals identify in-tensely with others and relinquish tight control over goal-directed activities. Cli-nicians with relational styles often allow clients to select or decide on the meansand the ends of their goal accomplishments. They use collaborative or contribu-tory approaches to help clients accomplish their own goals through group effort.
Just as the clinician’s decision making process (including clinical assess-ment and choice of goals and intervention strategies) is shaped by his/hercultural self, the client also comes with his/her “culturally contained self”(Roland, 1996). Hence, competent cross-cultural clinical practice is oftencolored by the clinician’s awareness of the impact of culturally based per-spectives and the matching of individual styles. Recognizing the importanceof this style matching is essential for a successful cross-cultural clinical pro-cess (Lu, Lim, & Mezzich, 1995; Matsumoto, 1996).
LITERATURE REVIEW
It is well established in the literature that Latinos underutilize mentalhealth services for a variety of reasons, including a lack of culturally sensi-
Lu et al. 47
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

tive services (Acosta, 1979; Barrera, 1978; Cheung & Snowden, 1990;Padgett et al., 1994; Padilla & Ruiz, 1974; Snowden et al., 1995; Sue, 1977;Sue et al., 1991). For example, in a chart review of patients in the Los An-geles County mental health system during a five year period, Sue et al.(1991) found that although Latinos and Asians comprised 33.7% and 8.7% ofthe county, respectively, they comprised only 25.5% and 3.1% of county’smental health patients, respectively. In contrast, non-Hispanic Whites com-prised 44.2% of L.A. county and 43% of county mental health patients. Thesame pattern of results was found in an earlier studies of Los Angeles County(Flaskerud, 1986; Flaskerud & Liu, 1991), as well as in a study of nearly14,000 mental health charts, from 17 community mental health centers inKing County, Seattle (Sue, 1977).
It has been established that utilization barriers for Latinos and other ethnicminorities include lack of available services, lack of access to existing ser-vices, and lack of culturally competent services when services are utilized(Parron, 1982). For example, in Sue’s (1977) major study of King Countymentioned above, it was found that when Latino, Asian, and other ethnic mi-nority patients did utilize county mental health services, about half droppedout of treatment after one session of therapy as compared to 30% of AngloAmerican patients.
One highly advocated solution to Latino underutilization is to provide men-tal health services that are responsive to the Latino culture and experience pro-vided either by bilingual/ bicultural Latino clinicians or by culturally sensitivenon-Latino clinicians. Evidence which demonstrates that providing Latinoswith culturally sensitive services results in greater utilization of services andbetter treatment outcome is beginning to emerge. For example, Sue et al.(1991) tested the “ethnic match” hypothesis by examining 12,000 L.A. countymental health charts, 3000 of each of four ethnic groups: Latino, Asian, Afri-can American, and White. As hypothesized, results showed that ethnic match-ing was indeed related to lower drop-out and better treatment outcome, butonly for Latino and Asian patients low in acculturation. Thus, it appears thatthe presence of bilingual and/or bicultural mental health professionals is im-portant for the large percentages of Latino and Asian populations low in accul-turation who appear to most need matching given their special linguistic andadaptational needs.
Although the above findings are encouraging, they provide little informa-tion about how bilingual/bicultural clinicians (e.g., Latino therapists) conducttherapy sessions or how their clinical styles differ from clinicians that are nei-ther bilingual nor bicultural (e.g., non-Latino therapists). In their definitive re-view of the literature on ethnic matching, and culturally responsive versus
48 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

traditional mental health services, Atkinson and Lowe (1995) concluded thatculturally responsive mental health services were superior to traditional ser-vices in increasing perceived credibility of therapists, willingness to return totreatment, satisfaction with therapy, and depth of disclosure in therapy on thepart of ethnic minority clients. These results were related to the finding thatethnic minority clients generally preferred similar ethnic therapists over dis-similar ones. Still, these findings provide very little insight into the clinicalstyles employed in culturally responsive services. Atkinson and Lowe did findthat Latino, Asian American and American Indian clients perceived therapistsas more credible when they used directive versus non-directive clinical styles.
The above findings are consistent with recommendations in the literatureto provide traditionally oriented Latino clients with active and directive ther-apists (Miranda, 1976) who are able to personalize the therapeutic relation-ship being formal yet warm, judiciously self- disclosing, and respectful toclients in the traditional sense (Roll, Millen, and Ramirez, 1980). In an ex-ploration of cultural competence in Latino clinicians, Manoleas, Organista,Nrgron-Velasquez, and McCormick (2000) found that their sample reportedmany differences in how they work with Latino versus non-Latino clients. Forexample, in response to missed therapy sessions, Latino clinicians were morelikely to telephone, make home visits, and to inquire with family members andother services providers about the Latino client’s whereabouts. Latino clini-cians also reported greater amounts of self-disclosure with Latino versusnon-Latino clients. Interestingly, commitment to working with Latino clientsin this study was associated with a family systems practice orientation versus acognitive-behavioral or eclectic approach (the sample was divided into thesethree primary orientations).
Obviously much more examination of culturally responsive clinical stylesand processes are needed. In the current study, both quantitative and qualitativeresearch methods were combined to compare Latino and non-Latino White cli-nicians on a number of clinically relevant dimensions. With regard to quantita-tive methods, the ASI (Achieving Styles Inventory) was used to assess and tocompare the general goal-related styles of Latino and non-Latino White clini-cians. In terms of qualitative methods, study participants were interviewed andpresented with a case vignette of an immigrant Mexican family with a number ofpsycho-social problems and issues. The clinicians were then asked to respond tothe vignette with regard to assessment and intervention thoughts, ideas, and di-rections (see the Appendix). The qualitative component of this study was in-tended to supplement the quantitative analysis of ASI findings which have beenhelpful in differentiating ethnic minority from non-minority clinician styles. Forexample, Lu (1994) in comparing the achieving styles of Asian American &
Lu et al. 49
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

non-Asian clinicians found that the former scored higher on the relational do-main of the ASI. Lu concluded that the greater relational achieving style ofAsian American clinicians may be an important component of their culturallyresponsive approach to mental health services with Asian American clients, anethnic minority group well known for underutilizing mental health services inspite of need (Sue, 1977; Sue et al., 1991).
Parallels exist between traditional Asian & Latino cultures that suggest thepossible relevance of Lu’s (1994) findings for the latter group. Like Asian cul-tures, Latino cultures are more traditional than the non-Latino White mainstream American culture (Hofstede, 1992). Traditionally, Latino culture placesemphasis on the value of family and extended family relations that are inter-de-pendent versus independent and promotes a collective attitude in terms of pool-ing resources to help family members get ahead. The role of women and theelderly are traditionally more rigidly defined and differentiated in Latino groupsthan in the United States. For instance, age has traditionally been the primary in-dicator of authority and maturity in these communities. Latino relationship andcommunication protocols are governed by more traditional values that empha-size a style of social interaction which is generally less direct, non- confronta-tional, more personal, informal, and deferential to those of higher-status basedon age, gender, professional status, etc., (Falicov, 1996; Roll et al.; 1980).Hence, even in professional relationships, such as those between clinicians andclients, one would expect Latino clinicians to demonstrate traditional Latino re-lationship protocol more frequently than their non-Latino White counterparts.To examine such differences, a two-stage research process was undertaken. Thefirst stage of the research focuses on the comparison of achieving styles and usesquantitative methods to determine whether Latino and non-Latino White clini-cians differ in their achieving styles. Three hypotheses are tested in this study:
Hypothesis # 1: Latinos will be less directive than non-Latino White cli-nicians;
Hypothesis # 2: Latinos will be less instrumental than non-Latino Whiteclinicians; and
Hypothesis # 3: Latinos will be more relational than non-Latino Whiteclinicians.
The second stage of the research process uses qualitative methods to explorethe differences in the clinicians’ clinical decisions through content analysis ofthe in-depth interview transcripts.
50 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

METHODS
Subjects
To test the three hypotheses, survey data were collected from two conve-nience samples. The first group consisted of 60 experienced Latino Americanclinicians primarily from the Bilingual Association of Spanish Speaking Clini-cians and Advocates (BASSTA) in the San Francisco Bay Area. This is a vol-untary, non-profit organization of Latino mental health professionals thatpromotes the advancement of culturally competent services for Latino clientsthrough various activities. The Latino group was comprised of 10 (18.9%)Central American, 5 (9.4%) Cuban/Cuban-American, 4 (7.5%) South Ameri-can, 4 (7.5%) Puerto Rican, 26 (49.1%) Chicano/Mexican/Mexican-Americanclinicians, 4 (7.5%) classified as others and 7 missing data. The comparisongroup of subjects included 47 non-Latino, White American clinicians whowere working for county mental health agencies in the Bay Area. Names forthis second group were obtained from a list provided by the San FranciscoMental Health Board.
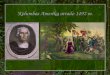
As can be seen in Table 1, there were slightly more females (n = 63) thanmales (n = 44); 36 of the subjects were less than 39 years old, 35 of the sub-jects were age 50 or older, and 33 of the subjects were between age 39 and 50.The great majority (n = 73)were clinicians with MSW degrees and 28 heldPh.D./M.D. degrees. Of the subjects, 22 were administrator/professors and79 were clinicians. Chi square tests were conducted to examine possible con-founding effect on race/ethnicity from other variables, such as age, gender,degree, and occupation status. No statistically significant differences werefound on any of the variables.
All survey participants were asked in the survey if they wished to partici-pate in a follow- up interview. Twenty-two agreed. Nine licensed Latino, and 9licensed non-Latino White clinicians were interviewed in order to assess theirclinical decisions and decision making processes regarding a case vignette. Alleighteen interviewees were working in the Bay Area with either county orcounty affiliated mental health agencies. Of the remaining respondents, twowere not able to participate due to out of state residence status, unexpected re-location, and two simply did not show up for the interview.
Measures
Achieving Styles Inventory (ASI). The ASI is a 45-item, self-report pen-cil-and-paper instrument designed to measure how frequently an individualuses each of the aforementioned nine achieving styles grouped into the three
Lu et al. 51
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

primary domains: direct, instrumental, and relational. Extensive reliability andvalidity tests have been conducted on the ASI using pooled data from3,758 subjects from 18 individual exploratory samples. Reliability, esti-mated by using Cronbach’s Alpha procedures for internal consistency, re-sulted in alphas ranging from .82 to .91. Split-half reliability coefficientsfor the individual Likert scales ranged from .79 to .88. In addition, normshave been established for age, gender, marital, educational, and occupa-tional groups. The Cronbach’s Alpha value of our sample ranged from .69to .92 (Lipman-Blumen, 1983).
The mean scores of ASI measure the strength of preference for a particularstyle and the frequency with which that style is selected by an individual. Op-erationally, the means are measured on a scale ranging from l to 7. Scale scoresare divided into high (5 to 7), medium (3 to 4), and low (l to 2). An individualwith a higher intensity and a higher range of scores on achieving styles canmove easily from one achieving style to another in response to situational cuesand external feedback; in other words, the person has more flexibility.
Interviews. By conducting in-depth interviews, the authors had an opportu-nity to experience a real event in the lives of the clinicians’ subjectivity(Beekman, 1986). The goal was to analyze the qualitative data without com-promising inter-subject interpretation and an understanding of the participat-
52 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
TABLE 1. Selected Characteristics of the Survey Participants1
LatinoN (%)
Non-LatinoN (%)
Total χ2
Gender Male 29 (65.9%) 15 (34.1%) 44
Female 31 (49.2%) 32 (50.8%) 63
Total 60 (56.1%) 47 (43.9%) 107 χ2 = 2.934; df = 1; N.S.
Age 39 and younger 21 (58.3%) 15 (41.7%) 36
40-49 20 (60.6%) 13 (39.4%) 33
50 and older 18 (51.4%) 17 (48.6%) 35
Total 59 (56.7%) 45 (43.3%) 104 χ2 = .640; df = 2; N.S.
Degree M.D./Ph.D. 12 (42.9%) 16 (57.1%) 28
M.A./M.S.W. 43 (58.9%) 30 (41.1%) 73
Total 55 (54.5%) 46 (45.5%) 101 χ2 = 2.101; df = 1; N.S.
Occupation Administrator/Professor
11 (50.0%) 11 (50.0%) 22
Clinician 43 (54.4%) 36 (45.6%) 79
Total 54 (53.5%) 47 (46.5%) 101 χ2 = .136; df = 1; N.S.
1 N’s vary by missing data.
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

ing clinicians. When pursuing an understanding of subjects of exceptionality,such as minority groups and cross-cultural studies, it is often more difficult toarrive at the validity of the inter-subjective interpretation (Haworth, 1986).Whereas quantitative research identifies the relationship between differentvariables among different cultural groupings in a statistically positive or nega-tive direction, qualitative research gives us more specific information aboutdifferent interactional structures and allows interpretation of their symbolicworldviews with unique sets of cultural premises, values, and rules. In general,many conceptual and experiential differences do not lend themselves to quan-titative measurement (Smith, 1983).
The main tools used in the qualitative part of the study were a case vignetteand an interview guide. This vignette was a composite of actual cases that rep-resented typical problems and issues encountered by authors of this paperwhen working with Latino American clients. The vignette presents a Mexicanimmigrant family referred to community mental health services following a re-ferral of their 15-year-old son for substance abuse and other problems.
Procedures
The Survey. After an initial phone contact, each respondent or agency on thetwo lists of clinicians received a package with four items: a cover letter de-scribing the purpose of the study, a background information sheet, the ASI in-strument with an option to sign up for further participation in the case vignetteinterview, and a self-addressed stamped envelope. In order to insure confiden-tiality, there was no identifiable information on the questionnaire, except apreassigned tracking number. All agencies from the list were approached.Three hundred and nineteen copies of questionnaires were mailed and 117copies returned within a three-month time period for a response rate of 36.7%.No follow-up mailings were conducted.
Interviews. To explore the question concerning differences in clinical pro-cesses between the two groups, eighteen guided interviews were conductedwith members of both groups of mental health clinicians. By utilizing a“non-directive,” “guided,” “in-depth” interview method, the authors had anopportunity to elicit “subjective” interpretations by the clinicians from theirown experiences (Beekman, 1986). All interviews were audio taped by the in-terviewers and subsequently transcribed into written form. Analysis of thetranscripts of the interviews served to answer questions concerning the clinicaldecision making processes. The interview process was non-directive and littleprompting was given by the interviewer. This deliberate restraint was appliedto reduce potential bias or influence upon interviewee perceptions.
Lu et al. 53
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

Clinicians were interviewed for about 30-45 minutes, usually at their placeof work. The case vignette involving hypothetical Latino clients set the stagefor this informal, conversational interview. Both interviewers (one male andone female) were Spanish-speaking graduate students of social work. Therewas no specific effort to match on gender.
The interview guide was used to insure that similar types of informationwere obtained from all interviewees. These in-depth interviews were struc-tured around the following questions:
1. What would be your assessment of this case vignette?2. What would be your intervention for this case vignette?3. How would you describe your clinical/therapeutic style?4. If this were a Caucasian family, would you help them differently?5. Would a Latino (or non-Latino) clinician treat this case differently than
you would?6. Any other comments?
Data Analysis
The Survey. A series of Chi-square, t-tests, and ANOVA were used to com-pare Latino American and non-Latino White American ASI mean scores. Theinfluence of demographic variables such as age, gender, degree/education, oc-cupational status (administrator/professor vs. clinicians), and race/ethnicity onachieving styles were also examined using multiple regression analysis. Therewere less than 8 individuals with a total of 10 items missing, and they were notincluded in the data analysis.
Interviews. More than 100 typewritten pages of transcripts were producedfrom the qualitative interviews. The transcripts were analyzed according to thecross-cases content- analysis approach. With this approach, no single cases arepresented; instead, the individual cases serve as the evidentiary base for thestudy and are used solely in the cross-cases analysis.
The transcripts from the interviews formed a database for the purpose ofidentifying information relevant to the concepts and clinical categories derivedfrom the previous literature review. In addition, new categories were gener-ated. New category generation was facilitated by segmenting the transcriptsinto units and re-grouping them into major themes according to identifiedcharacteristics. Re-grouping is a dynamic process of looking for similaritiesand differences within the categories. The dominant analytic techniques usedin this design were pattern matching and explanation-building techniques. Pri-marily, the research design of these case studies was based on Yin’s (1984)“multiple cases, replication design.”
54 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

Instead of using traditional narrative text, which is often bulky and cumber-some, a “process outcome matrix” was organized. This matrix transformedand abstracted information from transcripts (raw data) into an immediately ac-cessible compact form, which permitted easier comparison and conclusionforming. This data analysis process consisted of three concurrent flows of ac-tivity: (1) data reduction; (2) data display; and (3) conclusion drawing (Miles &Huberman, 1984).
The main patterns and interpretations of the interview data were identified,analyzed, and synthesized as well as cross examined with the findings fromthat survey data. In order to safeguard possible coder biases, the transcriptswere all typed in generic format without any demographic data attached. Thesummary of the interview findings were derived from the group consensus ofthe four coders.
RESULTS
Quantitative Survey Findings
To test the first research question, ANOVA, t-tests, and multiple regressionwere conducted on the total ASI, three domains, and the nine styles with eachindependent variable.
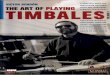
The analysis showed statistically significant differences in total ASI stylesand in all three domains between the Latino and non-Latino White clinicians(p < .05) (see Table 2). Few significant effects emerged from some other de-mographic variables–age, gender, or education (see Table 3).
As predicted, non-Latino White clinicians (M = 4.4, SD = .56) and LatinoAmerican clinicians (M = 4.1, SD = .69) differed in their overall ASI profile (F =3.59, p < .05), supporting hypothesis one. With regard to ASI domain differ-ences, results showed that the non-Latino White American group (M = 4.2, SD =.71) scored significantly higher than the Latino American group (M = 3.8, SD =.88) on the direct domain (F = 3.26, p < .05), as predicted in Hypothesis #1.Specifically, non-Latino Whites scored higher on the power direct style (p =.05) of the Direct domain.
With regard to the instrumental domain mean scores, non-Latino White cli-nicians (M = 4.2, SD = .71) scored higher than the Latino group (M = 3.8, SD =.95; F = 3.13, p < .05) as predicted in Hypothesis #2. Specifically, non-LatinoWhites scored higher on the self- instrumental (M = 4.3, SD = 1.08; vs. M = 3.7,SD = 1.41; F = 2.96, p < .05) and reliant- instrumental styles (M = 4.7, SD = .75;vs. M = 4.5, SD < 1.01; F = 6.40, p < .001).
Lu et al. 55
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

In the Relational Domain, Latino American (M = 4.7, SD = .88) and non-La-tino whites (M = 4.8, SD = .77) also differed significantly, (F = 3.40, p < .05),however, in the opposite direction from that predicted in the Hypothesis #3. Spe-cifically, Latino clinicians were found to be less relational than non-LatinoWhite clinicians.
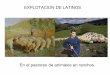
In order to further explore the relationship between achieving styles and cli-nician background characteristics, multiple regression analysis was conductedto predict ASI scores with the following sets of predictors: age, gender,race/ethnicity, occupational status (clinician vs. Administrator/professor), andeducation (PhD/MD vs. MA/MSW degree).
56 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
TABLE 2. Comparison of Achieveing Styles–Test of Between Subject Effect 1)
Dependent variable CronbachAlpha
Mean (s.d.)Type IIISum of
Squares
MeanSquare F Sig.
Latino (2)(N = 53)
Non-LatinoWhite
(N = 47)
Achieving Style Inventory .80 4.1 (.69) 4.4 (.56) 2.933 1.466 3.590 *
DIRECT .77 3.8 (.88) 4.2 (.71) 4.520 2.260 3.260 *
INTRINSIC .83 4.8 (.91) 5.2 (.77) 4.213 2.107 2.890
COMPETITIVE .82 2.8 (.92) 3.1 (.92) 2.068 1.034 1.121
POWER .91 3.9 (1.27) 4.5 (1.10) 11.092 5.546 3.954 *
INSTRUMENTAL .69 3.8 (.95) 4.2 (.71) 4.522 2.261 3.136 *
SELF .92 3.7 (1.41) 4.3 (1.08) 9.445 4.722 2.964
OTHERS .80 3.4 (1.11) 3.7 (.92) 2.441 1.220 1.166
RELIANT .81 4.5 (1.01) 4.7 (.75) 10.735 5.368 6.394 **
RELATIONAL .73 4.7 (.88) 4.8 (.77) 4.717 2.359 3.403 *
COLLABORATIVE .89 5.1 (1.16) 5.1 (.86) 4.072 2.036 1.945
CONTRIBUTORY .85 5.0 (.95) 5.0 (.76) 4.112 2.056 2.661
VICARIOUS .85 4.0 (1.22) 4.3 (1.23) 6.731 3.365 2.362
1 Degrees of freedom = 22 In Latino sample: with 7 missing data3 * p � .05** p � .01*** p � .001
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

As shown in Table 3, results indicated the race/ethnicity predictor was sig-nificantly related to the ASI (p < .01), direct (p < .05), and instrumental do-mains (p < .01). Latino clinicians scored lower in general. However, aftertaking into account the socio-demographic characteristics, the pattern of dif-ference had varied slightly. Significant score differences appeared in self- andother-instrumental styles rather than in reliant instrumental style; and in vicari-ous relational style rather than in relational domain in the multiple regressionanalysis. Other significant beta values were observed for administrator/clini-cian status, and degree as predictors of their achieving styles (p < .01). Admin-
Lu et al. 57
TABLE 3. Multiple Regression–Least Square Analysis of Latino Clinicians’Achieving Styles
Achieving Styles Clinicians(With vs.Without
Adm/TeachingExperiences)
Gender Age Ethnicity
(53 Latino vs.47 Non-Latino
White)
Degrees
(PhD/MDvs.
MA/MSW)
AdjustedR-square
total ASI .46 ** .22 �.004 �.40 * * .27 ** .22 **
Direct DomainIntrinsic-DirectCompetitive-DirectPower-Direct
.59 **
.41(*)
.41
.94 **
.16
.08
.37
.19
�.01�.004�.01�.013
�.42 *�.26�.39(*)�.60 *
.14
.45 *
.11
.94 **
.15 **
.09 *
.03
.10 *
Instrumental-DomainSelf-InstrumentalOther-InstrumentalReliant-Instrumental
.44 *
.60
.45
.27
.23
.33
.34
.03
�.01�.005�.01�.01
�.56 **�.74 **�.57 **�.36
.27
.19
.45
.31
.17 *
.11 *
.14
.03
Relational-DomainCollaboral-RelationalContributory-RelationalVicarious-Relational
.34
.60 *
.29
.13
.25
.03
.41(*)
.03
�.003�.007
.01
.01
�.21�.01�.11�.50 *
.40 *
.43
.32
.47
.12
.10
.03
.12 *
* p � .05** p � .01*** p � .001
(In Latino sample: with 7 missing data)
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

istrators and individuals with higher degrees (PhD/MD) scored higher onintrinsic, and power-direct styles than clinicians and MA/MSW. The clinicianswith higher degree/education reported higher relational scores.
Qualitative Interview Findings
The interview findings were consistent with the survey findings in that indi-vidual achieving styles differences were reflected in clinicians’ clinical deci-sions. Latino clinicians were rated as less directive, less intrinsic, and lesspower-direct, thus allowing their clients to have more influence on the processthan were their non-Latino counterparts. Latino clinicians expressed frequentdesires to establish rapport with the father first, develop relationships withother family members, and provide concrete assistance and referral services.Non-Latino White clinicians relied more on their own professional knowledgeand skills to analyze and make decisions. These findings were consistent withsurvey results in which Non-Latino clinicians scored higher than Latino clini-cians on both direct and self instrumental styles. The only incongruence ob-served between the survey and interview data was that the non-Latino Whiteclinicians perceived themselves as having a higher relational orientation whiletheir ASI scores indicated that they had the highest score on intrinsic directstyle (M = 5.2, SD = 2.10), a significantly higher mean than the relational styles(M = 4.8, SD = 2.36).
Findings from the interviews also helped to clarify the relationship betweenthe clinicians’ achieving style differences and their specific clinical decisions.The clinicians’ decisions were examined on assessment and intervention strat-egies, and their self-perceived clinical styles, as well as the possible impact ofrace/ethnicity on clinical processes. Differences found were not in kind, but inintensity and magnitude, and are enumerated below:
1. Response to question number one: What would be your assessment ofthis case vignette?
Both groups of clinicians commented on the family’s immigrant status, cul-tural adjustment to the U.S., and low socioeconomic status as being related tothe family’s problems. Specifically, all Latino clinicians assessed the vignetteas having a “combination” of acculturation/immigration adjustment difficultyand a problem with the family system. In contrast, only half of the non-LatinoWhite clinicians recognized cultural adjustment/immigration related issues,while the other half viewed the problems solely in terms of family system is-sues. Two thirds of Latino clinicians, compared to one third of non-LatinoWhite clinicians, felt optimistic and positive about treatment prognosis. Fur-
58 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

thermore, Latino clinicians viewed the case as less severe and described it ascharacteristic of immigration/acculturation difficulties. They also emphasizedinvolving the whole family in the treatment process and were less likely to per-ceive the fifteen year old son referred to in the vignette as the identified patient.Both groups of clinicians made individual assessments of each familymember. All addressed the key issues of the father’s underemployment,drinking problem, loss of status at home, and lack of language proficiencyand job skills; the mother’s drug/sleeping pill use and possible symptomsof somatization; and the son’s acting out behaviors and role as a scapegoat.However, the Latino clinicians gave more interpretation and insight than didthe non-Latino clinicians into how the cultural adjustment might have im-pacted the family’s living situation. Latino clinicians addressed issues such asthe impact of gender role identity and patriarchal family structure difference.Lastly, among all 18 interviewees, only four Latino clinicians addressed thefamily’s mandatory treatment and related issues of “shame.”
2. Response to question number two: What would be your intervention forthis case vignette?
Findings showed that, in general, the non-Latino White clinicians coveredmore treatment goals and areas of intervention than did the Latino group. Theyplaced more emphasis more on strengthening the “individual’s personal senseof self and identity” as opposed to focusing on “Latino cultural issues.” Theyalso focused more on treatment of substance abuse and further assessment ofsuicidal ideation and family violence. Only about half of the non- Latino Whiteclinicians emphasized the importance of language/cultural matches in treat-ment and identified the acculturation issue as a major concern of the treatment.The Latino clinicians did not talk much about the importance of cultural sensi-tivity as much as the White clinicians; however, they provided more specificstrategies to accommodate Latino culture in interventions, such as, establish-ing rapport with the whole family, (e.g., using culturally appropriate methodsto connect with the father first and thus prevent potential resistance from him).
Another distinction was that while both groups emphasized “family togeth-erness” and treating families as a system, among all interviewees, only Latinoclinicians (eight of the nine) elaborated on the importance of beginning thetreatment with acknowledging traditional family structure. For example, theyemphasized giving the father special recognition and showing respect (eventhough he was portrayed as having little power in the family) and working withhim first. Latino clinicians emphasized speaking Spanish with the father, talk-ing about the country of origin, and using culturally appropriate gestures andbody language to establish common ground. Furthermore, while both groups
Lu et al. 59
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

emphasized the combined intervention strategies of both family work and casemanagement, Latinos put more emphasis on case management services.
Both groups addressed the following issues: (a) improving spousal rela-tionships and family communication patterns; (b) solidifying parental unity,clarifying the family role-confusion, and working on problems such as trian-gulation and mother-son alliance problems; (c) recognizing the father’s lack ofacculturation, drinking and unemployment problems; (d) validating and sup-porting the mother, raising her drug awareness, establishing primary care ar-rangement, treating somatic complaints; and (e) finding role model and youthsupport groups for the son and daughter.
3. Response to question number three: How would you describe your clini-cal style?
Among non-Latino White clinicians, three main categories of answersemerged in fairly equal proportions: family systems approach, psycho-dy-namic approach with emphasis on education, and cognitive behavioral ap-proach. For Latino clinicians, the following three styles emerged: culturallyrelevant relationship oriented, contributory styles, intensive case managementand crisis intervention style, and eclectic approaches of family systems theory,psycho-dynamic, and behavioral interventions.
4. Response to question number four: If this were a Caucasian family,would you help them differently?
Among Latino clinicians, six out of nine reported that they would intervenedifferently with Caucasian families. Specifically, with immigrant Latino fami-lies as opposed to mainstream families, they would: (a) consider more cultur-ally relevant interpretations in clinical assessment; (b) use more crisisintervention and educational models; (c) focus more on family work versusindividuals; (d) use more self-disclosure and more personal and informalclinical styles in the clinical process, and (e) use both English and Spanishlanguages. The remaining three Latino clinicians reported that they wouldtreat all families similarly, but clarified with the following considerations:(a) that immigrant families would have different needs and different familydynamics from Caucasian families; (b) that there would be different inter-pretations of certain behaviors according to whether the clients were Latinoor Caucasian (e.g., a mother dressing up for the therapy session is not nota-ble in Latino culture, because it is a tradition for females to dress elabo-rately and formally); (c) that there would be more self-disclosure, rolemodeling, and educational process when working with Latino families,
60 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

and (d) that they assume that they would establish rapport more quickly andarrive at a diagnosis faster than non-Latino clinicians.
Among the non-Latino White group, seven out of nine clinicians reportedthat they would conceptualize the problems or treat the Caucasian family dif-ferently without specifying how. The remaining two non-Latino clinicians an-swered that there would be absolutely no differential treatment, except that oneindividual commented that “Caucasian families may not have accultura-tion/immigration problems.”
5. Response to question number five: Would a Latino- (or a non-LatinoWhite-) clinician treat this case differently from you?
Two-thirds of the Latino clinicians believed that there would be differencesbetween Latino and non-Latino clinicians, noting that Latino clinicians could:(a) have a better understanding of cultural nuances, (b) have a better under-standing of the issues of shame, loss/grief, and be less likely to label; (c) bemore likely to work with the whole family than with the individuals; and (d) bemore likely to employ different styles such as informal mannerism, and be lessdirect, less clinically focused, and use more self-disclosure. The other third ofthe Latino clinicians responded that this is not a race/ethnicity issue, but a cul-tural competency issue, and that it depends on the clinician’s cultural sensitiv-ity and conceptual framework.
Among the non-Latino White clinicians, eight out of nine believed thatthere would be some differences: that Latino clinicians with language and cul-tural competency would have more cultural awareness, better understandingof culturally related nuances, and would be better interpreters of body lan-guage and family dynamics. They also indicated that Latino clinicians mightestablish the connection with the Latino family more quickly. However, therewas no consensus on whether the Latino clinicians would be more effective inoutcomes. One remaining clinician, who is bilingual, commented that the an-swer would depend on the Latino clinicians’ levels of acculturation, theoreti-cal orientations, clinical styles, and language/cultural competency.
DISCUSSION
This study was an effort to combine both quantitative and qualitative meth-odologies to explore the central dimension of clinical practice, the clinical pro-cess, and how it is affected by clinicians’ cultural competence. Overall, thestudy has supported the authors’ position that clinicians’ racial/ethnic and lan-
Lu et al. 61
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

guage/cultural background will impact their personal achieving styles, clinicalprocess, and clinical decisions.
Quantitative Findings. Both Latino and Non-Latino clinicians had similarachieving style profiles with the same peak styles (intrinsic, collaborative, andcontributory styles), although they had different rank orders. This similarity inprofiles probably reflects the nonrandom sample of mental health providersgiven generally similar professional characteristics and attributes. The patternof the data supports the first three hypotheses that Latino clinicians differ in in-tensity from their non-Latino White American colleagues in all three domains(direct, instrumental, and relational). These findings appear consistent withprevious studies showing that cultural factors influence personality and cogni-tive development, learning processes (Dasen, 1977; Kaplan, 1961; Triandis,1975), personal achieving styles (Lu, 1994), and clinical processes and deci-sions (Lu, 1996).
With the exception of the relational domain, differences found on the directand instrumental domains appear consistent with differences between Latinoand mainstream American cultures often noted in the literature. For example,while effective Latino clinicians have frequently been described as being ac-tive and directive in therapy (e.g., Miranda, 1976; Organista, 2000), they arenot described as tightly controlling the therapeutic process and goals, nor asbeing individualistic and competitive in their problem-solving styles, as wouldbe predicted from the direct domain achieving style (Lipman-Blumen, 1987).Hence their lower score on this domain relative to White clinicians seems cul-turally consistent. Similarly, the lower scores of Latino clinicians on the in-strumental achieving style domain, relative to White clinicians, may alsoreflect the cultural tendency of the former to rely less on their professional sta-tus and networks to achieve treatment goals. Instead, it is more likely that La-tino and other culturally competent clinicians attempt to empower their clientsby providing the technical assistance necessary for them to solve their ownproblems and to internalize the credit (Gutierrez, Parsons, and Cox; 1998).
Findings related to the relational domain were in the opposite direction ofHypothesis #3 (Latinos will be more relational than non-Latino White clini-cians). The authors speculate that the influence of professional training mayhave had an equalizing effect on the relational domain scores of all cliniciansin the sample given their similar professional background characteristics.While Latino clinicians were lower than White clinicians on this domain, thestatistical difference may not be a real one considering the negligible differ-ence in mean scores on this domain for Latino and White clinicians (Ms = 4.7 &4.8, respectively). Thus, taken at face value, results for the relational domainseem to suggest that both Latino and White clinicians engage in a collaborativetherapeutic process with clients, providing space for them to define and solve
62 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

their own problems, while therapists identify with their clients and vicariouslyshare in their accomplishments.
Qualitative Findings. The findings, in general, were consistent with thequantitative data. Between-group differences among the interviewee answerswere not in kind but in intensity and magnitude. Although the non-LatinoWhite group displayed “cultural awareness,” and “culturally sensitivity,” theLatino clinicians were able to demonstrate more culturally relevant insightsand additional “cultural competency.”
Similar to ASI findings, the qualitative interviewing data indicated that thenon-Latino White clinicians used more directive statements, unilateral deci-sion-making processes, and put less emphasis on self disclosure. They also didnot emphasize establishing cultural common-grounds as did the Latino clini-cians. Other important differences between the two groups were: (1) a differ-ent degree of emphasis on assessment–Latino clinicians giving more emphasison the combination of cultural adjustment and family systems problems; theNon-Latino White group focused on one or the other, (2) different assessmentof level of case severity–non-Latino clinicians were less optimistic on caseprognosis, (3) different foci for treatment goals–Latino clinicians gave exten-sive acknowledgment of traditional family structure and culturally appropriateinterpretations; non-Latino clinicians focused more on family violence assess-ment and strengthening individual identity as treatment goals, (4) differentemphasis on intervention strategies–Latinos emphasized culturally specificstrategies (e.g., using Spanish language, culturally appropriate protocols, selfdisclosure, and more reference to concrete services), and (5) diverse opinionson the relationship between racial/ethnic match, linguistic/cultural match andclinical outcomes. With regard to the issue of racial/ethnic impact on clinicaloutcomes, both groups agreed that a linguistic/cultural match is more impor-tant than a racial/ethnic match in helping minority clients which is verifiedthrough our interview findings. Whether clinicians of both groups would treata non-Latino, non-immigrant family differently can not be ascertained fromthis study.
The interview data showed that Latino clinicians exercised less control,used more extrinsic, context oriented styles, and acknowledged the conven-tional family structure more than did non-Latino clinicians with the Latino im-migrant clients. Bilingualism showed little impact statistically in the ASIscores; however, the interview data indicated the bilingual non-Latino Whiteclinician demonstrated higher level of cultural competency than mono-lingual,non-Latino Whites. However, due to the small and non-representative sampleand the lack of direct client observations, generalization of the findings is sig-nificantly limited. Further systematic studies are essential for better under-
Lu et al. 63
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

standing of the relations between clinicians’ racial/ethnic, linguistic/culturalbackgrounds, and clinical decisions, processes, and outcomes.
IMPLICATIONS
Responses to issues of low utilization of and unequal access to mentalhealth services, as well as differential treatment outcomes, vary. However,most attention has been paid to the acquisition of a knowledge base about cli-ent populations’ cultural diversity, and to cultural awareness and cultural sen-sitivity. More recently, emphasis has begun to shift to cultural competencewith greater focus on the clinicians’ cultural self-awareness, clinical out-comes, and accountability. However, so far, there is limited understanding ofthe clinicians’ decision making processes and clinical styles.
Both quantitative and qualitative data strongly support the view that there isa linguistic/ cultural impact on clinicians’ personal styles and their practice.The findings reported here are in line with the noted emerging emphasis onculturally sensitive clinical styles and process. Especially important contribu-tions are the tools used here to delineate cultural sensitivity and competence.The case vignette is a long honored social work teaching tool. Here it isadapted to highlighting culturally based needs and approaches. Used cre-atively this tool holds considerable potential for teaching in this area. Alongwith the increasing emphasis on cultural competence, attention is being paidonce more to self awareness, as a way of sharpening worker interactive skills.As was demonstrated here, it is possible to link understanding of personalachieving styles with linguistic and cultural competence. The clinicians can notonly expand their repertoire through assessing and becoming aware of their ownstyles, but also attempt to match their personal styles appropriately with the cli-ents’ styles. Although beyond the immediate purview of this paper, the futuredevelopment of additional tools which can link these levels of understandingmore directly could have profound effects on teaching and practice.
REFERENCES
Acosta, F. X. (1984). Psychotherapy with Mexican Americans: Clinical an empiricalgains. In L. Martinez, Jr. & R. H. Mendoza (Eds.), Chicano Psychology (2nd Ed.)(pp.163-168). Orlando, FL: Academic Press, Inc.
Beekman, G. M. (1986, March/April). Legal barriers, what barriers? Atlanta EconomicReview, 44-46
Carkhuff, R., & Pierce, R. (1967). Different effects of therapist race, and social classupon patient depth of self exploration in the initial interview. Journal of CounselingPsychology, 31, 632-634.
64 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

Cheung, F. & Snowden, L (1990). Community mental health and ethnic minority pop-ulations. Community Mental Health Journal, 26. 277-291.
Cross, T. L., Bazron, B. J., Dennis, K. W. et al. (1989). Towards a culturally competentsystem of care. Washington, DC: CASSP Technical Assistance Center.
Dasen, P. R., Berry, J. W., & Sartorius, N. (1988). Health and cross-cultural psychol-ogy: Towards applications. CA: Sage.
Gutierrez, L. M., Parsons, R. J., & Cox, E. O. (1998). A model for empowerment prac-tice. In L. M. Gutierrez, R. J. Parsons, & E. O. Cox (Eds.), Empowerment in socialwork practice: A sourcebook (pp. 3-23). Pacific Grove, CA: Brooks/Cole Pub-lishing Company.
Haworth, G. O. (1986). My paradigm beats your paradigm. Unpublished paper. SanDiego: San Diego State University.
Hofstede, G. (1992). The cultural relativity of organizational practice and theories. InColeman Raider International (Ed.) Collaborative Negotiation Skills: United Na-tions Staff Development and Learning Service. NY: Coleman Raider International,Inc.
Kaplan, B. (Ed.). (1961). Study personality cross culturally. N.Y.: Harper & Row.Lipman-Blumen, J., Handley-Isaksen, A., & Leavitt, H. J. (1983). Achieving styles in
men and women: A model, an instrument, and some findings. In J. Spence (Ed.),Achievement and achievement motives. San Francisco; Freeman & Co.
Lipman-Blumen, J. (1987). Individual and organizational achieving styles: A handbookfor researchers and human resource professionals. Claremont, CA: Achieving StylesInstitute.
Lorenzo, M. K., & Adler, D. A. (1984, December). Mental health services for Chinesein a community health center. Social Casework: The Journal of Contemporary So-cial Work. 600-609.
Lu, Y. E. (1994). A comparison of achieving styles of Asian American and non-AsianAmerican psychotherapists. Psychotherapy in Private Practice 13, (2), pp. 45-69.
Lu, Y. E. (1996). Underutilization of mental health services by Asian American cli-ents: The impact of language and culture in clinical assessment and intervention.Psychotherapy in Private Practice, 15, (2), pp. 43-61.
Manoleas, P., Organista, K.C., Negron-Velasquez, G., & McCormick, K. (2000).Characteristics of Latino mental health clinicians: A preliminary examination.Community Mental Health Journal, 36 (4), 383-394.
Miles, M. B., & Huberman, A. M. (1984). Qualitative Data Analysis: A source book ofnew methods. CA: Sage.
Miranda, M. R. (Ed.) (1976). Psychotherapy with the Spanish-speaking: Issues in re-search and service delivery (Monograph No. 3). Los Angeles: Spanish-SpeakingMental Health Research Center, University of California.
Organista, K. C. (2000). Latinos. In J. R. White & A. S. Freeman (Eds.), Cognitive-be-havioral group therapy for specific problems and populations (pp. 281-303).Washington DC: American Psychological Association.
Padgett, D. K.; Patrick, C.; Burns, B. J. & Schlesinger, H. J. (1994). Ethnicity and theuser of outpatient mental health services in a national insured population. AmericanJournal of Public Health, 84 (2), 222-226.
Padilla, A. M. & Ruiz, R. A. (1974). Latino mental health: A review of the literature(2nd ed.). Washington, D. C.: National Institute of Mental Health.
Lu et al. 65
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4

Roland, A. (1988). In search of self in India and Japan. New Jersy: Princeton Univer-sity Press.
Smith, J. (1983). Quantitative versus qualitative research: An attempt to clarify the is-sue. Educational Research, 2 (3), 6-13.
Samovar, L., Porter, R., & Jain, N. (1981). Understanding intercultural communica-tion. Belmont, CA: Wadsworth Co.
Snowden, L. R., Hu, T. W., Jerrell, J. M. (1995). Emergency care avoidance: Ethnicmatching an participation in minority service programs. Community Mental HealthJournal, 31, 463-473.
Sue, D. W. (1977). Counseling the culturally different: A conceptual analysis. Person-nel and Guidance Journal, 56 (7), 422-425.
Sue, S., & McKinley, H. (1975). Asian American in the community mental health caresystem. American Journal of Ortho-psychiatry, 45, 111-118.
Sue, S. (1977). Community mental health services to minority groups. American Psy-chologist, 32, 616-624.
Sue, S. (1977). Psychological theory and implications for Asian Americans. Personneland Guidance Journal, 55 (7), 381-388.
Sue, S.,Fujino, D.,Hu, L.,Takeuchi, D. T.,& Zane, N. (1991). Community mentalhealth services for ethnic minority groups: A test of the cultural responsiveness hy-pothesis. Journal of Counseling and Clinical Psychology, 59, (4), pp. 533-540.
Triandis, H. C. (1975). Cultural training, cognitive complexity, and interpersonal atti-tudes. In R. W. Brislin et al. (Eds). Cross-cultural perspective of learning. N.Y.:Wiley & Sons.
Triandis, H. C., & Draguns, J. G. (Eds.). (1980). Handbook on cross-cultural psychol-ogy: Vol. 6. Psychopathology.
Yamamoto, J., James, Q. C., Bloombaum, M., & Hatten, L. (1967). Racial factors inpatient selection. American Journal of Psychiatry, 124, 630-636.
Yin, R. K. (1984). Case study research: Design and methods. Los Angeles: Sage.
66 JOURNAL OF ETHNIC & CULTURAL DIVERSITY IN SOCIAL WORK
Dow
nloa
ded
by [
Ston
y B
rook
Uni
vers
ity]
at 1
2:47
24
Oct
ober
201
4