Embed Size (px)
Citation preview

Experimental Work
Chapter 4

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 74
4.1 MATERIALS AND METHODS
Table 4.1: List of chemicals and solvents
S. No. Drugs Source
1. Diltiazem HCl Lupin Pharmaceutical Ltd., India
2. Verapamil Triveni Chemicals, Gujrat, India
______________________________________________________________________________
S. No. Chemicals Source
1. Acrylic acid anhydrous Fluka
2. Poly(vinyl alcohol) S.A Pharmchem Pvt. Ltd, Dupont
3. Poly (vinyl pyrrolidone) USP Signet Chemical Corporation, BASF
4. Azoisobutyronitrile Mody Chemi - Pharma Pvt. Ltd.
5. Potassium persulphate SD Fine chemicals
6. HPMC K15M USP Colorcon Asia Pvt. Ltd
7. Potassium bromide for IR Merck India Ltd.
8. Magnesium stearate SD Fine chemicals
9. Talc Qualigens
10. Glycerine Qualigens
11. Povidone K-30 USP Signet Chemical Corporation, BASF
12. Silica bag Tyvel silica bags
13. Sodium hydroxide Loba Chemicals
14. Pharmactose DCL 21 McLeod’s Pharm. Ltd.
______________________________________________________________________________
S. No. Solvents Source
1. Ethanol GR SD Fine chemicals
2. Ethyl methyl ketone for synthesis Qualigens
3. Ethyl acetate extrapure SD Fine chemicals
4. Dichloromethane GR SD fine Chemicals
5. Methanol AR SD Fine chemicals
6. Dimethyl formamide GR SD Fine chemicals
7. Glacial acetic acid GR SD Fine chemicals
8. Hexane AR Qualigens
9. Isopropyl alcohol AR SD Fine chemicals
10. Benzoyl chloride for syn Spectrochem
11. Glacial acetic acid AR Qualigens
12. Dichloromethane AR SD Fine chemicals

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 75
Table 4.2 List of equipments
S. No. Equipments Manufacturer, Model
1. FTIR Perkin Elmer, Spectrun RX I
2. IR Pellet compression machine Kimaya Engineering KP
3. Electronic weighing balance Shimadzu, AUX 220
4. Automated sample applicator Camag, Linomat
5. Bioadhesion test analyzer Modified double balance
6. Centrifuge Eltec, TC 650 D
7. Tablet Compression machine Karanavati
8. Deep freezer Sanyo, MDF-U333
9. Densitometer Camag
10. Development chamber (HPTLC) Camag
11. Digital pH meter Labindia, PICO+
12. Dissolution test apparatus Electrolab, TDT-08L
13. Franz diffusion cell Lab glass
14. Hardness tester Labline
15. Orbital Shaker Scigenics Biotech, Orbitek
16. Hot air oven Meta Lab, 6318
17. Refrigerator Toshiba, GR-M53UD-IND
18. Sampling cannula In-house
19. Sonicator Toschcon, SN-2
20. Stability chamber Thermolab
21. UV spectroscopy Perkin-Elmer, Lambda 25
22. Vernier calliper Mitotoyo, Japan
23. Cyclomixer Remi, CM 101
24. Melting apparatus Veego VMP-III
25. Vaccum oven Scientico, EVO-01R
_______________________________________________________________________

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 76
4.2 Analytical Method development
4.2.1 UV Spectrophotometry (For assay)
UV spectroscopic analysis was employed to determine the drug content and the concentration of
drug in aliquots obtained after dissolution studies.
Preparation of standard curves of DLZ
Standard curve of DLZ in distilled water
DLZ (100 mg) was accurately weighed and transferred to 100 ml volumetric flask. The drug was
dissolved in distilled water and volume was made up to 100 ml with distilled water. The stock
solution was further diluted with distilled water to obtain concentration ranging from 2-12 µg/ml.
The absorbance of each solution was recorded at 237 nm using UV-visible spectrophotometer in
1 cm path length quartz cuvette. Distilled water was taken for blank determinations. The
absorbance values were plotted against concentration (µg/ml) to obtain standard calibration plot
of DLZ. The data was treated statistically using linear least square regression method. The
above procedure was repeated six times.
Accuracy
Accuracy of analytical method is the closeness of test results obtained by the method to the true
value. For determining of DLZ concentration, standard solution was prepared. The above
solutions were subjected to UV absorbance at 237 nm and compared for its accuracy. The
method is said to be accurate for estimation if it gives < 2.0 % RSD at each concentration level.
RSD= SD * 100/ Mean
Precision
The precision is agreement between the results obtained when determinations are conducted.
Precision provides an indication of random errors and is generally subdivided into to cases:
repeatability and reproducibility, which are determined by calculating RSD of inter-day and
intra-day of DLZ. RSD should be < 2.0 % for the method in both inter-day and intra-day
determinations.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 77
Linearity
The linearity of test procedure is defined as its ability (within a given range) to produce the
results which are directly proportional to concentration of analyte in the sample. Linearity of
light absorption determination should be examined to ensure that Beer’s law operates over the
range of interest. For evaluation of linearity of the UV method of DLZ, the standard solution was
prepared at 2, 4, 6, 8, 10 and 12 µg/ml concentration (n=3) and observation were taken at 237nm
in UV spectrophotometer. The method is said to be linear for estimation of DLZ if it is linear
over 2-12 µg/ml range. Least square regression method was used to determine the regression
coefficient, r and the equation y = mx + c for the best fitting line.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 78
4.2.2 Development and Validation of Diltiazem using HPTLC (For bioassay)
Method development and optimization:
Stationary phase
Type: Silica gel 60F 254 precoated HPTLC plates (E. Merck, Germany) were used.
Pre-washing of plates: The plates were pre-washed in methanol for removing any impurities
picked up during storage in the laboratory environment.
Preparation of standard solution
10 mg of working standard of Diltiazem was accurately weighed and dissolved in 10 ml.
methanol to give a stock solution of 1 mg/ml (solution A)
Preparation of plasma sample
Plasma sample (480µL) was placed in glass tube followed by addition of 10 µL of Diltiazem (1
mg/mL, solution A) and 10 µL of Verapamil (500 µg/mL) as internal standard solution. 100 µL
of 0.2 N NaOH as added to the sample, the mixture was vortexed for 2 minutes, then 2 mL n-
hexane with 5% IPA as added. The solution was vortexed for 5 minutes and then centrifuged at
4000 rpm for 10 minutes. The organic phase was separated and dried. The residue was
reconstituted with 200 µL of methanol.
Table 4.3: Optimized Chromatographic Conditions
Application mode CAMAG LINOMATV using 25 µL
syringe
Development mode CAMAG twin trough chamber
Application band width 6 nm
Developing solvent Ethanol: DCM: Acetic acid :Water
(12:10:0.5:1)
Chamber saturation time 10 min
Developing distance 80 mm
Developing time 20 min
Scanner CAMAG TLC Scanner III
Integrator WIN CATS V 1.2.2
Scanning wavelength 240 nm (UV)

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 79
Once the chromatographic conditions were set, validation of analytical method was done for
standard solutions.
The HPTLC method developed was validated for following parameters:
Sensitivity
The sensitivity of the method was determined in terms of LOD, LOQ, linearity range and
correlation coefficient. Diltiazem was extracted from working stock solution (1 µg/ml) and
spotted on TLC plate in the range of 40-280 ng. The LOD was calculated as three times the noise
level and LOQ was calculated as ten times the noise level. A graph was obtained by plotting the
area under the peak of DLZ against the amount of DLZ (ng) to determine the linearity range and
correlation coefficient.
Selectivity and specificity
The selectivity of the assay was determined in relation to interferences from endogenous
substances and other commonly used antihypertensive drugs in human plasma.
Precision and accuracy
Different amount of Diltiazem covering the low, medium and higher ranges of the calibration
curve were spotted on the TLC plate. These spots were analyzed (n = 3) by using above
described HPTLC method. Precision was expressed as the % coefficient of variation (% CV) and
accuracy was expressed as a percentage [(observed concentration/theoretical concentration) ×
100)].
Reproducibility
The intra day reproducibility was evaluated by analyzing the amount of Diltiazem spotted on
TLC plate covering low, medium and higher ranges of calibration curve in replicates (n = 3). The
inter day reproducibility was evaluated analyzing the same amount of analyte over period of three
days (n = 3).

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 80
Recovery study
Recovery of Diltiazem was determined by spiking Diltiazem in human plasma to obtain three
different concentrations covering the low (40 ng/spot), medium (160 ng/spot) and higher (280
ng/spot) ranges of the calibration curve. The samples were then extracted and analyzed as
described earlier. The recovery was calculated by comparing the resultant peak areas with those
obtained from pure standards in methanol at the same concentrations.
Robustness
To study the robustness of the method, small deliberate variations in the mobile phase
composition (± 2%), chamber saturation period (± 10%), development distance (± 10) and time
for drying after development to scanning (00, 60 and 120 min) were carried out. One factor was
varied while keeping other constants, % RSD as considered to assess the robustness of the
method.
Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 81
4.3 Polymer Synthesis
4.3.1.1 Synthesis of Poly acrylic acid (PAA)-Poly (vinyl pyrrolidone) (PVP)
interpolymer complex:
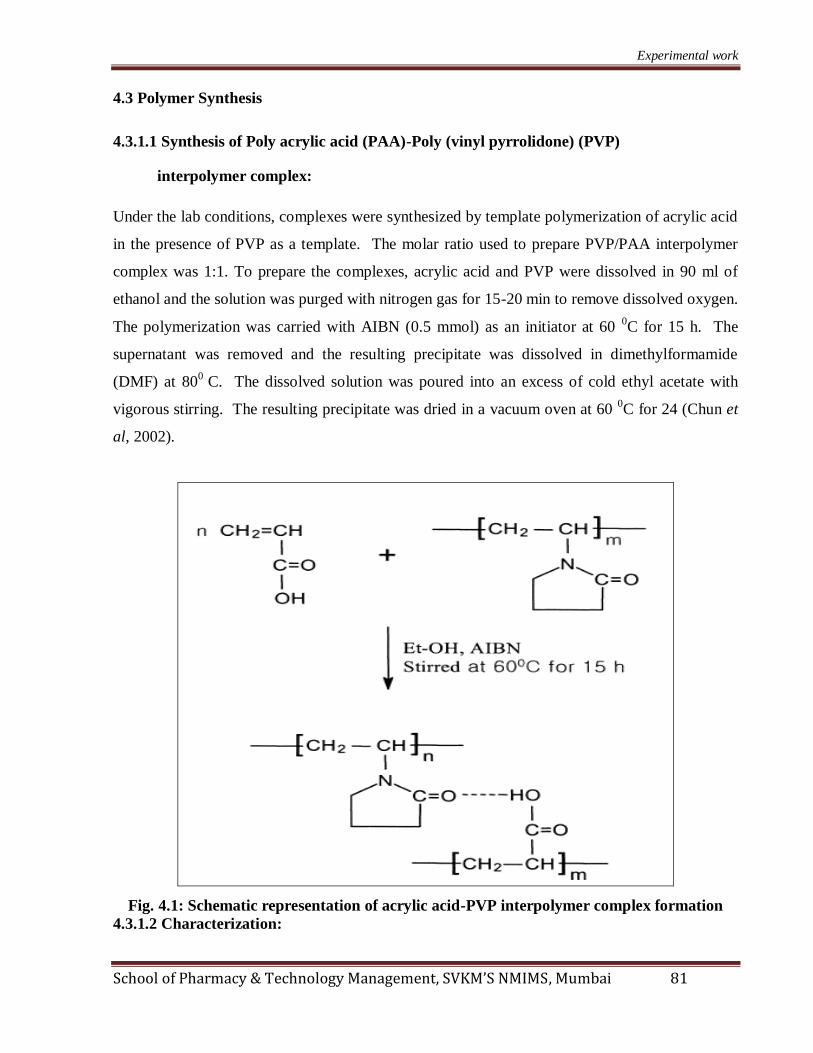
Under the lab conditions, complexes were synthesized by template polymerization of acrylic acid
in the presence of PVP as a template. The molar ratio used to prepare PVP/PAA interpolymer
complex was 1:1. To prepare the complexes, acrylic acid and PVP were dissolved in 90 ml of
ethanol and the solution was purged with nitrogen gas for 15-20 min to remove dissolved oxygen.
The polymerization was carried with AIBN (0.5 mmol) as an initiator at 60 0C for 15 h. The
supernatant was removed and the resulting precipitate was dissolved in dimethylformamide
(DMF) at 800
C. The dissolved solution was poured into an excess of cold ethyl acetate with
vigorous stirring. The resulting precipitate was dried in a vacuum oven at 60 0C for 24 (Chun et
al, 2002).
Fig. 4.1: Schematic representation of acrylic acid-PVP interpolymer complex formation
4.3.1.2 Characterization:

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 82
FTIR spectroscopy
PVP and AAPVP complex were subjected to Fourier Transform Infra-red spectroscopy in the
range of 4000- 400 cm-1
. FTIR spectrophotometer (Perkin-Elmer), USA) was used for the study.
DSC Analysis
Differential Scanning Calorimeter (Diamond TG/DTA, Perkin Elmer, USA) was used for
studying the thermal behaviour of the PVP and AAPVP complex. The melting studies were
performed in the temperature range of 50–300°C at the heating rate of 10°C/min in nitrogen
atmosphere.
4.3.1.3 Acute oral toxicity study
Previous reports in literature indicated that the polymer complex composed of AA and PVP in
1:1 mole ratio has adhesive properties higher than that of carbopol 971 P NF (Chun et al, 2002).
However, there have been no previous reports about the toxicity of this polymer complex to be
used in pharmaceutical formulation. So it was necessary to access its safety issue in our desired
buccal formulation. OECD guideline No.425 (Acute oral Toxicity-Acute Toxic class method)
was undertaken as a test procedure to ascertain the acute oral toxicity, occurred after the
administration of the test substance. The test procedure in this OECD guideline is of value of
minimizing the number of animals required to estimate the acute oral toxicity. The acute
intravenous toxicity study was conducted using preliminary limit dose test of the Up-and-Down
Procedure statistical program– AOT 425StatPgm (2001). In addition to the estimation of LD50
and confidence intervals, the test allows the observation of signs of toxicity.
Female Wistar rats (150-180 g) were individually identified and allowed to acclimate to the
laboratory conditions for 7 days before the start of the study. Only one rat received a dose at a
particular time. First animal received a dose of 55 mg/kg. Animal was observed for 3 hours after
oral administration for any toxicity signs, survival or death. If the first animal died or appeared
moribund, the second animal received a lower dose (175mg/kg). The dose progression or
Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 83
reduction factor was 3.2 times of the previous dose. If no mortality was observed in the first
animal then the second animal received a higher dose (175 mg/kg, 550 mg/kg and 2000 mg/kg).
Dosing of the next animal was continued depending on the outcome of the previously dosed
animal for a fixed time interval (3 hour).
The test was stopped when one of the stopping criteria was met:
a) 5 reversals occur in any 6 consecutive animals tested.
b) 3 consecutive animals died at one dose level.
Survived animals were observed for long-term outcomes for a period of 14 days. The LD50
values were calculated using AOT 425 software (Environmental Protection Agency, USA) based
on the short term (3 hour) and long term outcome (14 days).
4.3.1.4 Buccal irritation test
Wistar rat was anaesthetised for 6 hours and tablet was placed in buccal cavity. After 6 hours,
tablet was removed and the animal was sacrificed. Buccal mucosa was taken for histological
study to see any adverse effect on the oral mucosa part.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 84
4.3.2.1 Synthesis of Poly acrylic acid -Poly vinyl alcohol) (PVA) interpolymer
complex:
Under the lab conditions, complexes were synthesized by template polymerization of acrylic acid
in the presence of PVA. 15 ml of AA aqueous solution (6.7%) was mixed with 15 ml of the PVA
aqueous solution (4.1%). The monomer molar ratio used to prepare PVA/PAA interpolymer
complex was 1:1. Resultant solution was purged with nitrogen gas for 15-20 min to remove
dissolved oxygen. The polymerization was carried out with KPS (Potassium Persulphate)
(60mM), as an initiator, at 60˚C for 2 hours (Chun et al 2004).
CH2
H
OH
O + CH2 CH
n
CH2 CH
n
OH
Water, Potassium persulphateStirred at 60 0C for 3 hours
OHOH
CH2 CH
m
O
n
Acrylic acid Poly (vinyl alcohol)
Interpolymer complex
Nitrogen atmosphere
Fig. 4.2: Schematic representation of acrylic acid-PVA interpolymer complex formation

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 85
4.3.2.2 Characterization:
FTIR spectroscopy
PVA and AAPVA complex were subjected to Fourier Transform Infra-red spectroscopy in the
range of 4000- 400 cm-1
. FTIR spectrophotometer (Perkin-Elmer), USA) was used for the study.
DSC Analysis
Differential Scanning Calorimeter (Diamond TG/DTA, Perkin Elmer, USA) was used for
studying the thermal behaviour of PVA and AAPVA complex. The melting studies were
performed in the temperature range of 50–300°C at the heating rate of 10°C/min in nitrogen
atmosphere.
4.3.2.3 Acute oral toxicity study
Previous reports in literature indicated that the adhesive force of polymer complex composed of
AA and PVA was stronger than that of commercial Carbopol 971 P (Oh et al, 2004). However,
there have been no previous reports about the toxicity of this polymer complex to be used in
pharmaceutical formulation. So it was necessary to access its safety issue in our desired buccal
formulation. OECD guideline No.425 (Acute oral Toxicity-Acute Toxic class method) was
undertaken as a test procedure to ascertain the acute oral toxicity as mentioned in section 4.3.1.2.
4.3.2.4 Buccal irritation test
The rat was anaesthetised for 6 hours and patch was placed in buccal cavity. After 6 hours patch
was removed and the animal was sacrificed. Buccal mucosa was taken for histological study to
see any adverse effect on the oral mucosa part.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 86
4.3.3 Synthesis of Acrylic acid - HPMC interpolymer complex
4.3.3.1a Synthesis of Acryloyl Chloride (ACl)
A mixture of 21.6 gm (0.3 moles) of acrylic acid (AA), 84.4 gm (0.6 moles) of benzoyl chloride,
and 0.05 gm of hydroquinone was distilled at a fairly rapid rate through a distilling column. The
distillate was collected in a receiver containing half a gram of hydroquinone, immersed in ice.
When the temperature at the top of the column, which remained between 60-70oC for most of the
distillation, had reached 85oC the distillation was discontinued. The crude product, weighing
between 21-22 gm, was then redistilled through the same column and the fraction boiling at 72-
74oC at 740 mm was collected. The yield of the final product was 18-19 gm or 68-72%.
4.3.3.1b Esterification reaction
2.7 gm of HPMC was dissolved in 100 ml of water with constant stirring so as to avoid lump
formation. 30 ml of MEK was added to the aqueous solution of HPMC (Solution-A) and was
kept in an ice-bath with constant stirring so as to maintain a temperature of 0-5 oC. 0.5 ml of ACl
was mixed with 30 ml of MEK (Solution-B). Solution-B was added drop wise to the solution-A,
kept on stirring in an ice-bath and was stirred for 3 hrs. The reaction mixture was subsequently
transferred to a petri-dish and was kept for drying at room temperature for 48 hrs. The film, so
obtained, was repeatedly washed with rectified spirit to wash off the unwanted free acrylic acid,
if any. The yield of the final product was 80%.
HPMC Acrylic acid HPMC acrylate+Benzoyl chloride
0-5 C
Ethyl methyl ketone
Fig. 4.3: Schematic representation of acrylic acid-HPMC

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 87
4.3.3.2 Characterization of Acrylic acid - HPMC interpolymer complex
The newly formed complex was analysed for solubility and melting point determination.
FTIR spectroscopy
HPMC and HPMC acrylate were subjected to Fourier Transform Infra-red spectroscopy in the
range of 4000- 400 cm-1
. FTIR spectrophotometer (Perkin-Elmer), USA) was used for the study.
DSC Analysis
Differential Scanning Calorimeter (Diamond TG/DTA, Perkin Elmer, USA) was used for
studying the thermal behaviour of the HPMC and the developed film. The temperature and
energy scales were calibrated as per the standard protocols supplied by the manufacturer. The
melting studies were performed in the temperature range of 50–300°C at the heating rate of
10°C/min in nitrogen atmosphere.
XRD analysis
HPMC and the esterified product were subjected to X-ray diffraction (XRD-PW 1700, Philips,
USA) using CuKα radiation generated at 40KV and 40 mA; the range of diffraction angle 2θ was
10.00-60.00o.
4.3.3.3 Toxicity studies
4.3.3.3a Hemocompatibility study
The complex formed was subjected to hemocompatibility test. The haemocompatibility test of
HPMC and HPMCAA were done as per the reported literatures with necessary modifications (Pal
et al, 2007; Mishra et al, 2008; Pal et al, 2008). This test aims at determining the % haemolysis
of the RBCs in the presence of the samples. The % haemolysis may be mathematically defined
as:

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 88
% 100Test Negative
Positive Negative
A AHaemolysis x
A A
(Equation 4.1)
where,
Atest Absorbance for test samples;
Anegative Absorbance for negative control;
Apositive Absorbance for positive control
In short, 5 ml of citrated blood was collected from a pathological laboratory and was
subsequently diluted to 20 ml with normal saline. For the preparation of the positive control, 0.5
ml of the diluted blood was transferred to a 15 ml falcon tube with the subsequent addition of the
0.5 ml of 0.01N hydrochloric acid. Thereafter, the volume was made up to 10 ml with normal
saline. Hydrochloric acid is a corrosive liquid and leads to the disruption of RBC membrane
thereby causing haemolysis. The negative control was prepared in the similar manner where the
hydrochloric acid was replaced with normal saline. For test samples, solutions (10 %, 20 %, 40
% and 80%) of the HPMCAA were prepared in normal saline. 0.5 ml of the solution was diluted
to 1 ml with normal saline, which was further diluted to 10 ml with normal saline. The samples
(positive control, negative control and test samples), so obtained, were incubated at 37 oC for 1 hr
and were subsequently centrifuged at 3000 rpm for 10 min. The supernatant was analyzed
spectrophotometrically at 545 nm. % haemolysis was calculated as per eq.4.1. If the %
haemolysis ≤5%, the test material is considered as highly hemocompatible, if the % haemolysis
in the range of 5-10%, the test material is considered as hemocompatible and if the % haemolysis
is ≥20%, the test material is considered as non-hemocompatible.
4.3.3.3b Acute oral toxicity study
OECD guideline No.425 (Acute oral Toxicity-Acute Toxic class method) was undertaken as a
test procedure to ascertain the acute oral toxicity as mentioned in section 4.3.1.2.
4.3.3.3c 28 days repeated Dose Toxicity (Sub-acute Oral Toxicity)
OECD guideline No. 407 (Sub-Acute Toxic class method) was undertaken as a test procedure.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 89
Test animals:
i. Test Species: Rat (Rattus norvegicus) of either sex
ii. Strain: Wistar
iii. Total Number of Animals Used: 60
iv. Weight before study: 150-180g
Acclimatization Period:
7 days prior to commencement of dosing.
Animal Identification:
The animals were identified using picric acid. Appropriate labels were attached to the cages
indicating the study number, test substance code, group number and sex, dose, and cage number.
Environment Conditions:
Temperature: Maximum : 27 ºC, Minimum : 25ºC
Mean Relative Humidity: 70 %
Photoperiod: The photoperiod was 12 hours artificial light and 12
hours darkness
Housing:
i. Caging: Polypropylene rat cages covered with stainless steel grid top
were used. Clean rice husk was used as the bedding
material.
ii. Water Bottle: Each cage was supplied with propylene water bottles
(Capacity –250ml) with a stainless steel nozzle.
iii. Housing: 5 animals of 100 – 250 Grams of same sex per cage.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 90
Diet and Water:
i. Diet: Rodent pellet diet (manufactured by ‘Nav Maharashtra
Chakan Mills Ltd.’) was provided ad libitum.
ii. Water: Drinking water filtered through ‘Aqua guard’ water filter
system was provided ad libitum.
Table 4.4: Allocation of Wistar Rats in 28 days oral toxicity study
Test Group Dose to Animal (mg/kg) Male Female
Control Vehicle (Distilled Water) 3 3
Low 100 mg/kg 3 3
Medium 200 mg/kg 3 3
High 500 mg/kg 3 3
Satellite Control Vehicle (Distilled Water) 3 3
Satellite (High) 500 mg/kg 3 3
Experimental Procedure:
Adult Wistar rats of either sex weighing between 150 to 180 g.
The animals are divided into following groups:
Group 1 Control / Vehicle Group (Distilled Water).
Group 2 HPMCAA (100 mg/kg)
Group 3 HPMCAA (200 mg/kg)
Group 4 HPMCAA (500 mg/kg)
Group 5 Satellite group (Distilled Water)
Group 6 Satellite group HPMCAA (500 mg/kg)
Each group contains 3 male and 3 female. Each cage houses 3 animals of the same sex either
male or female. Cages are labelled and the animals are marked for identification.
Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 91
Route of Administration
Vehicle or drug solution was administered by oral route using a stainless steel feeding needle.
Maximum permissible volume to be administered was limited to 2ml/100 gm body weight in case
of aqueous solution. In case of doses where more volume of solution was required, total volume
of solution was divided into 2 or 3 equal fractions and administered after interval of 30 minutes.
The time of drug administered was kept same throughout the study.
Observations:
General health of the animals in terms of body weight, behavior, skin, hair, and food
consumption was carefully noted. Bedding material of each cage replaced regularly.
Food Consumption
Before administration of drug, the animals were weighed using a calibrated balance. For
recording the food consumption 150 g of standard rat food pellets (purchased from Amrut
laboratory manufactured by Nav Maharashtra Chakan Oil mills Ltd., Sangli) was kept in feed
tray of the animals. The unconsumed pellets was weighed and replaced with fresh 150 g of
pellets in each tray every day. The time of filling the food tray is noted down and kept constant
throughout the study. The animal’s had access to Aquaguard filtered water and food ad libitum.
Haematology
Before start of study and at the end of study period i.e. 28 days the animals were anaesthetized
(anaesthetic ether) and blood sample was collected. In case of satellite control and satellite 500
mg/kg group the blood sample was collected before the start of study and after one month of 28
days of study have been completed. The blood samples were collected in two separate bottles,
marked individually (animal number, group, haematology). EDTA (anti-coagulant) was used in
blood samples for heamatological parameters.
Histopathology
At the end of study period i.e. 28 days the animals were anaesthetized (anaesthetic ether) 24
hours after the last dose. In case of satellite control and satellite 500mg/kg group were killed by
anaesthetic ether 28 days of treatment.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 92
The abdomen of rat was cut opened using stainless steel scissors and forceps in a pre disinfected
stainless steel necropsy table. The organs were collected very carefully and washed in sterile
phosphate buffered saline and weighed individually using Mettler balance. Care was taken by
marking all the organs as per their Group no. and Animal Id Code. The organs after weighing
were transferred into individually marked (with indelible ink) glass bottles containing 10%
formalin.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 93
4.4. Preformulation studies
Preformulation testing is the first step in the rational development of dosage form. It can be
defined as an investigation of physical and chemical properties of a drug substance alone and
when combined with excipients. The overall objective of preformulation studies is to generate
information useful to the formulator in developing stable and bioavailable dosage forms, which
can be mass-produced.
4.4.1 API Characterization
Diltiazem HCl was received from Lupin Pharmaceutical Ltd, Pune, India. Following tests were
carried out which could result in essential information for formulation work.
Diltiazem has been authenticated by using techniques like TLC, FTIR, DSC and determining
melting point.
4.4.1.1 Organoleptic properties
Received drug was observed for general physical properties such as nature, colour and odour.
The solubility of the drug was determined in water as per IP.
4.4.1.2 Thin layer chromatography
It was carried out using silica gel GF 254 as the coating substance and ethanol: dichloromethane:
acetic acid: water in ratio of 12:10:1:05v/v/v/v was used as mobile phase. Development chamber
was saturated for 10 minutes and spotted plate was developed in mobile phase. Retention factor
was calculated as equation:
Rf = Distance travelled by solute front/ Distance travelled by solvent front (Equation 4.2)
4.4.1.3 Melting point
Melting point of DLZ was determined using digital melting point apparatus. Average of three
reading was calculated (n=3).
4.4.1.4 FTIR studies

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 94
FTIR studies were used for unique structural information extracted from the spectral data. Drug
was mixed with potassium bromide dried overnight at 1100C in ratio of 1:100. Mixture was
triturated for uniform mixing of drug. Mixture was pelletized in IR compression machine to
develop a thin film which was subjected to FTIR spectrophotometer in the range of 600-3600 cm-
1.
4.4.1.5 DSC studies
Differential scanning calorimetry (DSC) is one of the most widely used thermal analysis
technique for the characterization of pharmaceutical solids. Thermal events such as melting
point, recrystallization and glass transition temperature were measured. DSC studies of DLZ
were performed by 10 0C/min heating rate in the temperature range of 40-250
0C in inert
atmosphere.
4.4.2 Drug excipient compatibility studies
Drug- excipient compatibility study was carried out by placing drug alone and drug along with
individual excipients in certain ratio (tentative ratio of formulation) in stoppard vials at 40°C/
75%RH for two months. Samples were physically observed every weak and degradation was
examined by FTIR spectroscopy at the end of studies. Quantities of the excipients taken are
mentioned in Table 4.5. Physical observation of sample was done for any color change, lumps
formation or any other visual changes.
Table 4.5: Composition of samples for compatibility studies
S.No. Excipients Drug : Excipients ratio
1. Drug ---
2. AAPVP 1:4
3. PVP K-30 1:2
4. Magnesium stearate 1:0.25
5. Talc 1:0.25
6. DC Lactose 1:5
7. HPMCAA 1:3
8. AAPVP 1:4
Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 95
4.5 Formulation Studies
Tablets have been the most commonly investigated dosage form for buccal drug delivery to date.
However, buccal patch may be preferred over adhesive tablet in terms of flexibility and comfort.
It was planned to prepare both formulations, i.e. tablet and patch, using the mucoadhesive
polymers synthesized.
AAPVP interpolymer complex was found to be insoluble in most of the commonly used solvents.
Hence, was not a suitable candidate for buccal patch formulation as formulation of patch requires
the solution of drug and excipents in a common solvent. Therefore, AAPVP interpolymer
complex was employed in buccal tablets formulation.
On contrary, AAPVA polymer complex did not give powder but was found to form flexible patch
after getting dried, due to the presence of PVA. Hence, it was not a suitable candidate for tablet
formulation. So it was used in buccal patch formulation.
Tablets were prepared using HPMC acrylate at different concentration ranging from 20-70% and
its affect on drug release was studied.
The literature documents that the dose of DLZ can be reduced up to 80% via buccal delivery,
owing to the avoidance of a hepatic first-pass effect (Ahuja et al, 1995). Therefore,
buccoadhesive formulations containing the lowest dose of DLZ, i.e., 30 mg, were worked upon in
the current study. Another work carried out on buccal tablets and patches of DLZ corroborates
the use of this dose level (Saisivam et al, 2000; Shayeda et al, 2009). There are reports
indicating that the buccoadhesives have been studied for drug release up to 2 days (Han et al,
1999; Guo JH, 1994). However, as a buccoadhesive tablet, film, or patch is unlikely to remain on
the buccal mucosa for such long a time, drug release in the present study was investigated only
up to 6 hr.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 96
4.5.1 Preparation of Mucoadhesive Buccal Tablet
Direct compression technique was employed for the formulation. In this technique, first
medicated layer was formed and backing layer blend was placed on medicated layer and
compressed to get bilayered tablet. Drug, polymers and excipients were properly mixed to get a
uniform blend and compressed. Similarly, blend of protective layer containing ethyl cellulose
was compressed on the previously compressed medicated tablet or loose compact to get bilayered
tablet. Colourant was incorporated in backing layer in order discriminate the two layers of the
tablet.
Since the polymer compex was a novel one, no range was known for its application. Initially
trial batches were formulated using the polymer complex AAPVP in range of 20-80% keeping all
the other variables constants and its effect on the dissolution attributes was evaluated.
Experimental
Trial 1:
Table 4.6: Composition of tablets for the effect of AAPVP on dissolution profile
It was observed that at low concentration (20%) of AAPVP, 70% of drug was released in first
hour leading to dose dumping phenomenon. While only 30% of drug was released after 6 hours
when the complex was high concentration (80%). 50-60% of drug as released in the formulation
containing 40-60 % of AAPVP, therefore this range was selected for further studies. Moreever, it
was found in the literature that starch, PVP K- 30 is added in the formulation as release modifier
to enhance the extent and release rate of drug. PVP K-30 was selected to enhance the extent of
drug release. AAPVP was selected in two concentrations, 40 % and 60%. For each
Batch Code Ta Tb Tc Td
Drug (DLZ) (mg) 30 30 30 30
AA-PVP (%) 20 40 60 80
Talc (%) 1 1 1 1
Mag. Stearate (%) 1 1 1 1
Lactose (DC) qs qs qs qs
Backing layer
Total (mg) 180 180 180 180

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 97
concentration, PVP K-30 was used in 5, 10, 20 and 30% concentration to study its effect on the
dissolution profile.
Trial 2:
Table 4.7: Composition of tablets for the effect of PVP K-30 on dissolution profile
Dissolution studies indicated that there was no significant change in the release profile when PVP
K-30 as used in 5% concentration. At 30 % concentration, although more than 90 % drug was
released but more than 50% of drug was released within1 hour. 70-92% drug release was
obtained when PVP K-30 was used in range of 10-20 %.
4.5.1.1 Experimental Design
It is desirable to develop an acceptable pharmaceutical formulation in shortest possible time
using minimum man power and raw materials. Traditionally pharmaceutical formulation is
developed by changing one variable at a time. This method is time consuming and requires a lot
of imaginative efforts. Moreover, it may be difficult to evolve an ideal formulation using this
classical technique since the joint effects of independent variables are not considered. It is
therefore very essential to understand the complexity of pharmaceutical formulations by using
established tools such as factorial design.
Factorial designs are used in experiment where effect of different factors or condition on
experimental results is to be elucidated. Factorial designs are designs of choice for simultaneous
determinations of effects of several factors and their interactions. A 32 randomized full factorial
design was utilized in the present study. In this design two factors were evaluated, each at three
Batch Code Te Tf Tg Th Ti Tj Tk Tl
Drug (DLZ) (mg) 30 30 30 30 30 30 30 30
AA-PVP (%) 40 40 40 40 60 60 60 60
PVP K-30 5 10 20 30 5 10 20 30
Talc (%) 1 1 1 1 1 1 1 1
Mag. Stearate (%) 1 1 1 1 1 1 1 1
Lactose (DC) qs qs qs qs qs qs qs qs
Backing layer
Total (mg) 180 180 180 180 180 180 180 180

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 98
levels, and experimental trials were carried out at all nine possible combinations. The factors
were selected based on preliminary study described as above.
A three-level, two-factor experimental design, as shown in Table 4.8, describes the proportion in
which the independent variables AAPVP, (X1), and PVP K-30 (X2), were used in the formulation
of mucoadhesive patches. The levels of the two factors were selected on the basis of the
preliminary studies carried out before implementing the experimental design. All other
formulation and processing variables were kept invariant throughout the study. The response
variables tested includes: bioadhesion force and percentage release after 6 hours. The quantity of
AAPVP was varied at three levels: 45, 52.5 and 60 % (w/w), whereas the quantity of PVP K-30
was varied at the levels of 12, 16 and 20% (w/w). All nine formulations were prepared in three
sets and analyzed individually for percentage release after 6 hours, bioadhesion force and other
patch properties. Checkpoint batch was also prepared to prove the validity of the evolved
mathematical model. The linear regression model was derived from Enter Method using SPSS
version 11.5, statistical software. Significant terms were chosen at 95% confidence interval
(p<0.05) for final equations. In addition, contour and surface plots were obtained by Statistica-6,
to represent the effect of the independent variables graphically.
Table 4.8: Factor Combinations as per the Chosen Experimental Design
Formulation code AAPVP (X1) (%) PVP K-30(X2) (%)
T1 45 12
T2 45 16
T3 45 20
T4 52.5 12
T5 52.5 16
T6 52.5 20
T7 60 12
T8 60 16
T9 60 20

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 99
Table 4.9: Composition of buccal tablets (DLZ-AAPVP)
4.5.1.2 Tablet Evaluation
4.5.1.2a Technological parameters
The diameter and thickness of the formulated tablets were measured using Vernier Callipers.
Total weight of the tablets was determined using digital balance.
4.5.1.2b Assay
Twenty tablets were taken and powdered; powder equivalent to one tablet was taken and
dissolved in 100ml of water. The solution was filtered through a membrane filter and the
absorbance was measured, after suitable dilution, spectrophotometrically at 237 nm.
4.5.1.2c Surface pH Study
The surface pH of the buccal tablets was determined in order to investigate the possibility of any
side effects in vivo. As an acidic or alkaline pH may irritate the buccal mucosa, the surface pH
was maintained as close to neutral as possible. The method adopted by Bottenberg was used to
determine the surface pH of tablets (Bottenberg et al, 1991). A combined glass electrode was
used for this purpose. The tablet was allowed to swell by keeping it in contact with 1 mL of
distilled water for 2 hours at room temperature. The pH was identified by bringing the electrode
Batch Code T1 T2 T3 T4 T5 T6 T7 T8 T9
Medicated layer
Drug (DLZ) (mg) 30 30 30 30 30 30 30 30 30
AA-PVP (%) 45 45 45 52.5 52.5 52.5 60 60 60
PVP K 30 (%) 12 16 20 12 16 20 12 16 20
Talc (%) 1 1 1 1 1 1 1 1 1
Mag. Stearate (%) 1 1 1 1 1 1 1 1 1
Lactose (DC) qs qs qs qs qs qs qs qs qs
Backing layer
Ethyl cellulose
Coarse powder: fine powder 4:1(mg) 40 40 40 40 40 40 40 40 40
Total weight (mg) 220 220 220 220 220 220 220 220 220

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 100
into contact with the tablet surface and allowing the surface to equilibrate for 1 minute. The
experiments were performed in triplicate, and average values were reported.
4.5.1.2d Swelling Study
The swelling properties of the tablets were evaluated using swelling index by determination of %
swelling (Parodi et al, 1996). Buccal tablets were weighed individually (designated as W1) and
placed separately in 2% agar gel plates, incubated at 37°C ± 1°C, and examined for any physical
changes. At regular 1-hour time intervals until 6 hours, tablets were removed from the gel plates
and excess surface water was removed carefully using the filter paper. The swollen tablets were
then reweighed (W2) and the swelling index (SI) were calculated using the following formula:
SI = [(W 2 − W 1)/ W 1] × 100
The experiments were performed in triplicate, and average values were reported.
4.5.1.2e Ex vivo Mucoadhesive Strength
A modified balance method was used for determining the ex vivo buccoadhesive strength (Gupta
et al, 1992). Sheep buccal mucosa was obtained from a local slaughterhouse and used within 2
hours of slaughter. The mucosal membrane was separated by removing underlying fat and loose
tissues. The membrane was washed with distilled water and then with phosphate buffer pH 6.8 at
37°C. The mucosa was cut into pieces and washed with phosphate buffer pH 6.8. A piece of
buccal mucosa was tied to a lower Teflon block which was placed in a beaker filled with
phosphate buffer pH 6.6 touching mucosal surface at 37°C ± 1°C. The buccal tablet was stuck to
the upper Teflon block with cyanoacrylate glue. The two sides of the balance were made equal
before the study, by keeping a weight on the right-hand pan. A weight of 5 g was removed from
the right-hand pan, which lowered the pan along with the tablet over the mucosa. The balance
was kept in this position for 5 minutes contact time. The water (equivalent to weight) was added
slowly with a burette (100 drops/min) to the right-hand pan until the tablet detached from the
mucosal surface. This detachment force gave the buccoadhesive strength of the buccal tablet in
grams. Force of adhesion and bond strength parameters were calculated.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 101
4.5.1.2f. Ex vivo Residence Time
The Ex vivo mucoadhesion time was studied (n = 3) after application of tablets on freshly cut
sheep buccal mucosa. The fresh sheep buccal mucosa was fixed in the inner side of a beaker,
about 2.5 cm from the bottom, with cyanoacrylate glue. One side of each tablet was wetted with
1 drop of phosphate buffer (pH 6.6) and pasted to the sheep buccal mucosa by applying a light
force with a fingertip for 30 seconds. The beaker was filled with 200 mL of phosphate buffer
(pH 6.6) and was kept at 37°C ± 1°C. After 2 minutes, a 50-rpm stirring rate was applied to
simulate the buccal cavity environment, and tablet adhesion was monitored for 6 hours. The time
required for the tablet to detach from the sheep buccal mucosa was recorded as the mucoadhesion
time (Han et al, 1999).
4.5.1.2g Stability study of optimized formulation in human saliva
The stability studies of optimized tablets were performed in 5mL of natural human saliva kept at
room temperature for 6 hours. Tablets were physically examined for changes in shape at regular
time intervals of 0, 1, 2, 3, and 6 hours.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 102
4.5.2 Preparation of Mucoadhesive Buccal Patch
AAPVA polymer complex did not give powder but was found to form flexible patch after getting
dried, due to the presence of PVA. Hence, it was not a suitable candidate for tablet formulation.
So it was used in buccal patch formulation. Solvent casting technique was used for the
preparation of patches (Anders R and Merkle HP, 1989). The dried patches were checked for any
imperfections or air bubbles and cut into circulars pieces of diameter 14 mm diameter using
cutter. Patches were meant to release the drug from only one side; therefore an impermeable
backing membrane (Tegaderm TM
adhesive surgical dressing, 3M Health Care, Germany) was
placed on the other side of the patch.
Trial 1:
Amount of plasticizer greatly affects the film properties. Glycerine and Propylene glycol were
used in concentration ranging from 5 -50% w/w.
It was observed that at low concentration of plasticizer (0-20% w/w for glycerine and 0-40% w/w
for propylene glycol) film formed was brittle and difficult to remove. At high concentration
(≥40% w/w for glycerine and ≥60 %w/w for propylene glycol), although the film was flexible but
was found to be oily. 30% w/w for glycerine and 50 %w/w for propylene glycol were found to be
ideal for getting smooth and flexible film. Glycerine at 30% w/w concentration was used further
in all the buccal film formulation. The film formed was smooth, homogenous and flexible.
Trial 2:
Since the polymer compex was a novel one, no range was known for its application. Initially
trial batches were formulated using the polymer complex AAPVA in range of 25-100 mg keeping
all the other variables constants and its effect on the dissolution attributes was evaluated.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 103
Table 4.10: Composition of patches to study the effect of AAPVA on dissolution profile
It was observed that at low concentration (25mg) of AAPVA, more than 70% of drug was
released in first hour leading to dose dumping phenomenon. Whereas only a small fraction of
drug was released after 6 hours when the complex was used at high concentration (100 mg).50-
60% of drug as released in the formulation containing 50-75 mg of AAPVA. This range was
selected for further study. Hoever, it was found in the literature that PVP K- 30 is added in the
formulation to enhance the extent and release rate of drug. PVP K-30 was selected to enhance the
extent of drug release. AAPVA was selected in two concentrations, 50 and 75 mg. For each
concentration, PVP K-30 was used in 5, 10, 25 and 40 mg concentrations to study its effect on
the dissolution profile.
Trial 3: PVP K-30 was used in concentration of 5-40 mg keeping AAPVP at two levels (50 and
75 mg)
Table 4.11: Composition of patches for the effect of PVP K-30 on dissolution profile
No significant change as observed in the release profile when PVP K-30 was used in
concentration of 5 mg. At 40 mg concentration, although more than 90 % drug was released but
more than 50% of drug was release within1 hour. 70-92% drug release was obtained when PVP
K-30 was used in range of 10-40 mg.
Batch Code Pa Pb Pc Pd
Drug (DLZ) (mg) 30 30 30 30
AA-PVA (mg) 25 50 75 100
Glycerine (%w /w) 30 30 30 30
Water qs qs qs qs
Batch Code Pe Pf Pg Ph Pi Pj Pk Pl
Drug (DLZ) (mg) 30 30 30 30 30 30 30 30
AA-PVA (mg) 50 50 50 50 75 75 75 75
PVP K-30 (mg) 5 10 25 40 5 10 25 40
Glycerine (% w/w) 30 30 30 30 30 30 30 30
Water qs qs qs qs qs qs qs qs

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 104
4.5.2.1 Experimental Design:
A 32 randomized full factorial design was utilized in the present study as described in section
4.5.1.1. A three-level, two-factor experimental design, as shown in Table 4.12, describes the
proportion in which the independent variables AAPVA, (X1), and PVP K-30 (X2), were used in
the formulation of mucoadhesive patches. The response variables tested includes: bioadhesion
force (BF) and percentage release after 6 hours (Rel 6 hr). The quantity of AAPVP was varied at
three levels: 40, 60 and 80 mg, whereas the quantity of PVP K-30 was varied at the levels of 10,
20 and 30 mg. All nine formulations were prepared in three sets and analyzed individually for
percentage release after 6 hours, bioadhesion force and other patch properties.
Table 4.12: Factorial Combinations as per the Chosen Experimental Design
Formulation code AAPVA (X1) (mg) PVP K-30(X2) (mg)
P1 40 10
P2 40 20
P3 40 30
P4 60 10
P5 60 20
P6 60 30
P7 80 10
P8 80 20
P9 80 30
TABLE 4.13: Composition of buccal patch (DLZ-AAPVA)
Batch Code P1 P2 P3 P4 P5 P6 P7 P8 P9
Medicated layer
Drug (DLZ) (mg) 30 30 30 30 30 30 30 30 30
AA-PVA (mg) 40 40 40 60 60 60 80 80 80
PVP K 30 (mg) 10 20 30 10 20 30 10 20 30
Glycerin (%) 30 30 30 30 30 30 30 30 30
Backing layer
Tegaderm TM
adhesive surgical dressing

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 105
4.5.2.2 Patch Evaluation
4.5.2.2a Patch thickness
The thickness of each patch was measured at five different locations (center and four corners)
using a micrometer screw gauge and a mean value of five locations was used as a film thickness.
4.5.2.2b Folding endurance
The folding endurance of patches was determined by repeatedly folding the patch at the same
place till it broke or was folded up to 200 times without breaking (Khurana et al, 2000).
The
experiments were performed in triplicate, and average values were reported.
4.5.2.2c Content uniformity
Drug content uniformity was determined by dissolving the patch by homogenization in 100 mL
of an isotonic phosphate buffer (pH 6.6) under occasional shaking and then followed the
procedure given in section 4.5.1.2b.
4.5.2.2d Surface pH study
Surface pH was determined using combined glass electrode as mentioned in section 4.5.1.2c.
4.5.2.2e Swelling study
The swelling properties of the patches were evaluated using swelling index by determination of
% swelling as mentioned in section 4.5.1.2d.
4.5.2.2f Ex vivo Mucoadhesive Strength
Ex vivo Bioadhesive force was determined using in house modified double pan balance method
as mentioned in section 4.5.1.2 e.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 106
4.5.2.2g Ex vivo Residence Time
Ex vivo Residence Time was determined using the beaker method as mentioned in section
4.5.1.2f.
4.5.2.2h In vitro Drug Release
Dissolution study was conducted similar to that mentioned in section 4.5.1.2g.
4.5.2.2i Stability of optimized formulation in human saliva
The stability studies of optimized patches were performed in 5mL of natural human as mentioned
in section 4.5.1.2i.
4.5.2.2j Mechanical Parameters of Buccal Patches:
Mechanical properties of the films were evaluated using a microprocessor based advanced force
guaze (Ultra Test, Mecmesin, UK) equipped with a 25 kg load cell. Film strip with dimensions
60 x 10 mm and free from air bubbles or physical imperfections were held between two clamps
positioned at a distance of 3 cm. During measurement, the top clamp at a rate of 2 mm/s pulled
the strips to a distance till the film broke. The force and elongation were measured when the film
broke. The mechanical properties were calculated according to the following formulae (peh,
1999). Measurements were run in four replicates for each formulation.
The following equations were used to calculate the mechanical properties of the films:

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 107
The tensile testing gives an indication of the strength and elasticity of the film, reflected by the
parameters: tensile strength (TS), elastic modulus (EM) and elongation at break (E/B). A soft
and weak polymer is characterized by a low TS, EM and E/B; a hard and brittle polymer is
defined by a moderate TS, high EM and low E/B; a soft and tough polymer is characterized by a
moderate TS, low EM and high E/B; whereas a hard and tough polymer is characterized by a
high TS, EM and E/B (Aulton et al, 1981). Another parameter, Strain has been used as an
indicator of the overall mechanical quality of the film (Rowe, 1983). A high strain value
indicates that the film is strong and elastic. Hence, it is suggested that a suitable buccal film
should have a relatively high TS, E/B and Strain but a low EM.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 108
4.5.3 Formulation Studies
Tablets were prepared using HPMC acrylate at different concentration and its affect on drug
release was studied.
Preparation of Mucoadhesive Buccal Tablet
Direct compression technique was employed for the formulation. Physical blend of drug,
polymers and excipients were properly mixed and passed through 20 mesh screen, then
compressed in tablet compression machine (Karanawati, Mumbai) using 8 mm flat faced punch.
Since the polymer complex was a novel one, no range was known for its application. Initially
trial batches were formulated using the polymer complex HPMCAA in range of 20-70% keeping
all the other variables constant and its effect on the dissolution attributes was evaluated.
Experimental
Table 4.14: Composition of tablets proposed to study the effect of HPMCAA
Batch Code F1 F2 F3 F4
Drug (DLZ) (mg) 30 30 30 30
HPMCAA (%) 20 40 60 70
Talc (%) 1 1 1 1
Mag. Stearate (%) 1 1 1 1
Lactose (DC) qs qs qs qs
Total (mg) 120 120 120 120

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 109
4.6 Stability studies
Stability studies of both optimized formulations (T13 and P 13) were conducted as per ICH
guidelines. Packing material was selected based on high polymer composition of formulation.
Tablets were packed in 30cc thick walled HDPE bottles with CRC caps. Each bottle containing
30 tablets and 2 g of silica bags were kept for real time (25°C/ 60% RH) and accelerated (40°C/
75% RH) stability study. Patches were kept in aluminium foil and subjected to above mentioned
stability conditions. Samples at each time point were observed for physical change and were
analyzed for dissolution, bioadhesive strength and total drug content.

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 110
4.7 In vivo studies
In vivo experiments were performed after approval of the protocol (CPSEA/SPTM/78/2010) from
Institutional Animals Ethics Committee. As per the protocol, optimized formulations were tested
in Albino rabbits for bioavailability studies. Rabbits were obtained from Haffkine Institute,
Mumbai. Studies were conducted in four rabbits in the weight range of 3 to 4 kgs. After
habitation of ten days they were exposed to three samples (Diltiazem solution, optimized buccal
formulations T13 & P 13) in serial one after other with wash out period of seven days (more than
seven half lives).
Figure 4.4: Rabbit in restrainer Figure 4.5: Feeding of oral solution to rabbit
Figure 4.6: Withdrawal of blood Figure 4.7: Buccal adhesive tablet
sample from rabbit ear vein applied at mucosa of rabbit

Experimental work
School of Pharmacy & Technology Management, SVKM’S NMIMS, Mumbai 111
Rabbits were fasted for 24 h before drug administration and anaesthetised with pentobarbital (25
mg/kg). For oral administration, drug in aqueous solution in dose of 10mg/kg was administered
by a oral feeding needle (Figure 4.5) to all four rabbits and blood samples were withdrawn from
marginal ear vein (Figure 4.6) using insulin syringe at 0.5, 1, 1.5, 2, 3, 4, 5 and 6 hours. For the
blood withdrawal, rabbits were restrained in restrainer (Figure 4.4) and 1 mL of blood was
withdrawn from marginal ear vein. Withdrawn blood was mixed gently with a drop of heparin
solution (Inhep®) and centrifuged for 5 minutes at 5,000 rpm at 10°C. Centrifugation gives
sedimentation of blood component and supernatant plasma. Plasma was separated and processed
as mentioned earlier. Extracted drug was quantified in validated HPTLC method as mentioned in
section 4.2.2.2.
After a wash out period of seven days, optimized formulation (buccal tablet, T13) was positioned
just above the incisor tooth (on either side of the mouth) and held firmly in place with a finger
over the lip for 30 seconds to ensure adhesion (Figure 4.7). Blood sample were withdrawn and
treated as mentioned in earlier paragraph.
Third study sample of optimized formulation (buccal patch P 13) was also treated as that
mentioned in earlier paragraph for T13.





























