Embed Size (px)
Citation preview
The Journal of Pain, Vol 15, No 12 (December), 2014: pp 1282-1293Available online at www.jpain.org and www.sciencedirect.com
Expectancy-Induced Placebo Analgesia in Children and the Role of
Magical Thinking
Peter Krummenacher,*,y,z Joe Kossowsky,*,x,jj Caroline Schwarz,* Peter Brugger,{
John M. Kelley,jj,**,yy Andrea Meyer,zz and Jens Gaab**Department of Psychology, Clinical Psychology and Psychotherapy, University of Basel, Basel, Switzerland.yCollegium Helveticum, University of Zurich and ETH Zurich, Zurich, Switzerland.zbrainability LLC, Zurich, Switzerland.xDepartment of Anesthesiology, Perioperative and PainMedicine, Boston Children’s Hospital, HarvardMedical School,Boston, Massachusetts.jjProgram in Placebo Studies, Beth Israel Deaconess Medical Center/Harvard Medical School, Boston, Massachusetts.{Neuropsychology Unit, Department of Neurology, University Hospital Zurich, Zurich, Switzerland.**Psychiatry Department, Massachusetts General Hospital/Harvard Medical School, Boston, Massachusetts.yyPsychology Department, Endicott College, Beverly, Massachusetts.zzDepartment of Psychology, Clinical Psychology and Epidemiology, University of Basel, Switzerland.
Received2014.J.K. andThis resesupporteported(P2BSP1_The authAddressUniversit8092 Zur
1526-590
ª 2014 b
http://dx
1282
Abstract: Expectations and beliefs shape the experience of pain. This is most evident in context-
induced, placebo analgesia, which has recently been shown to interact with the trait of magical
thinking (MT) in adults. In children, placebo analgesia and the possible roles that MT and gender
might play as modulators of placebo analgesia have remained unexplored. Using a paradigm in
which heat pain stimuli were applied to both forearms, we investigated whether MT and gender
can influence the magnitude of placebo analgesia in children. Participants were 49 right-handed chil-
dren (aged 6–9 years) who were randomly assigned—stratified for MT and gender—to either an
analgesia-expectation or a control-expectation condition. For both conditions, the placebo was a
blue-colored hand disinfectant that was applied to the children’s forearms. Independent of MT, the
placebo treatment significantly increased both heat pain threshold and tolerance. The threshold pla-
cebo effect was more pronounced for girls than boys. In addition, independent of the expectation
treatment, low-MT boys showed a lower tolerance increase on the left compared to the right side.
Finally, MT specifically modulated tolerance on the right forearm side: Low-MT boys showed an
increase, whereas high-MT boys showed a decrease in heat pain tolerance. This study documented
a substantial expectation-induced placebo analgesia response in children (girls > boys) and demon-
strated MT and gender-dependent laterality effects in pain perception. The findings may help
improve individualized pain management for children.
Perspective: The study documents the first experimental evidence for a substantial expectancy-
induced placebo analgesia response in healthy children aged 6 to 9 years (girls > boys). Moreover,
the effect was substantially higher than the placebo response typically found in adults. The findings
may help improve individualized pain management for children.
ª 2014 by the American Pain Society
Key words: Placebo analgesia, expectation, children, magical thinking, pain.
PMay10, 2014; Revised August 23, 2014; Accepted September 12,
C.S. contributed equally to this work.arch was supported by the University of Basel. P.K. was alsod by brainability LLC. J.K.’s contributions to this study were sup-by the Swiss National Science Foundation, grant project148628).ors declare that there is no conflict of interest.reprint requests to Peter Krummenacher, PhD, ETH Zurich andy of Zurich, Collegium Helveticum, Schmelzbergstrasse 25, CH-ich, Switzerland. E-mail: [email protected]
0/$36.00
y the American Pain Society
.doi.org/10.1016/j.jpain.2014.09.005
lacebo responses arise from complex and heteroge-neous psychoneurobiological learning processes,23
involving contextual conditioning, expectation for-mation, and social learning mechanisms.22 They can beelicited by a variety of psychosocial and environmentalcues that are associated with the patient-clinician rela-tionship.5 Placebo responses account for a significantportion of clinical outcomes in many somatic diseases4
and mental disorders,40 and they substantially modulatepain perception.8,22
Krummenacher et al The Journal of Pain 1283
Although placebo analgesia has received substantialscientific scrutiny in adults,6,27,37,43 empiricalinvestigations in children are rare. This is especiallynoteworthy because findings from the small number ofpediatric clinical trials that have been conducted so farsuggest that placebo responses might be morepronounced in children than in adults.15,60,79 Forexample, clinical trials of local anesthetics1,2 andvenipuncture33 suggest that placebo responses in childrenare substantial. This is evenmore interesting fromaneuro-biological perspective, as the prefrontal cortex (PFC) hasbeen consistently shown to be important in thetop-down mediation of expectation-related placeboresponses6,27,43,78; in addition, the PFC undergoesconsiderable maturation during childhood.31,32
Surprisingly, to date there have been no experimentalattempts to study placebo analgesia in healthy children.Moreover, very few clinical studies of pediatric placeboresponses have differentiated between subgroups orexamined potential moderator variables.69
Placebo analgesia has been shown to be mediated bythe release of interacting endogenous neuromodula-tors, such as opioids and reward-related dopamine.5,68
Dopaminergic activity has also been associated withpersonality traits such as reward susceptibility,67 whichpartially predicts the magnitude of placebo anal-gesia.66,67 More recently, the personality dimension ofmagical thinking (MT), which is thought to be relatedto dopaminergic function,44 has been implicated inmodulating expectation-related lateralized placeboanalgesia in healthy adults.41 MT—the belief that onecan bring about a circumstance or event simply bythinking about it or wishing for it—is a fundamentaldimension of a child’s thinking.62,81 MT in healthyadults has been associated frequently with enhancedmeaning attribution,44 and it has been shown to facili-tate associative processing, possibly mediated by theright hemisphere.13,30 Indeed, right hemispheredominance has been suggested as being related toboth MT54 and pain processing—albeit with inconsistentfindings.20,73
We used a lateralized heat pain paradigm to address 3aims: 1) to determine the magnitude of expectation-related placebo analgesia in healthy children, 2) toexamine whether MT and gender influence placeboanalgesia and pain perception, and 3) to explorewhether there is an asymmetry between the hemi-spheres in pain perception. In a between-subjects design,boys and girls with high and low MT underwent painassessments on both forearms before and after assign-ment to either an analgesia-expectation or a control-expectation treatment condition.We tested 3main hypotheses. First, we predicted that a
deceptive induction of analgesia expectationwould pro-duce placebo analgesia, as shown by an increase in heatpain threshold and tolerance. Second, we predicted thatplacebo analgesia would be moderated by MT. Specif-ically, we predicted greater placebo analgesia in high-MT children compared to low-MT children. Finally, onthe basis of adult data,41 we hypothesized that painperception would be asymmetric as a function of MT,
with higher pain sensitivity for the left compared tothe right forearm.
Methods
SubjectsForty-nine healthy right-handed children (23 girls, 26
boys) aged 6 to 9 years (mean = 8.17; standard deviation[SD] = .84) were included in the study. The study was con-ducted in accordance with the Declaration of Helsinkiand approved by the Local Ethics Committee of theCanton Basel, Switzerland.Participants were screened using a health assessment
questionnaire for parents. Exclusion criteria were acuteor chronic disease, neurological disorder, mental illness,skin pathologies or sensory abnormalities, acute orchronic pain, or current regular use of any medicationthat would affect study measurements.Right-handedness was determined using the standard
Edinburgh self-report handedness inventory57 (cutofflaterality quotient $ .60; mean = .93; SD = .11;range = .60–1.00). Sufficient receptive German languageskills were assessed and confirmed for all children withthe Intelligence and Development Scales34 (cutoffscore $ 3.5; mean = 7.63; SD = 1.89; range = 3.50–11.00). All children received a CHF 30 toy shop gift certif-icate and a medal for their participation.Participants were recruited through mass mailing.
Children of the targeted age group were randomlyselected through the birth announcements of theCanton Basel-Stadt. Families who were still living in thecanton or its surrounding area were contacted by letter.Of the 430 letters sent to parents, 47 families (11%) re-sponded, resulting in 47 participating children. Addi-tionally, 2 children of university staff membersparticipated in the study, for a total of 49 participants.The letters that were sent to the parents introducedthe study as an ‘‘Investigation to better understand chil-dren’s heat and pain perception.’’ All parents gave writ-ten informed consent and all children provided assentafter being provided with information about the testprocedure. Theywere informed that they could interruptthe study at any time without any relational disadvan-tages or personal consequences from the authorities,such as the experimenter (C.S.) or the parents. At theend of the experiment, children and parents were de-briefed and fully informed about the true aims of theexperiment (delayed informed consent).Half of the children were randomly allocated—strati-
fied for MT score and gender—to either the analgesia-expectation condition or to the control-expectationcondition (Fig 1). The randomization code was gener-ated using the built-in random number generator inMicrosoft Excel for the Macintosh, version 11 (MicrosoftCorp, Redmond, WA). The placebo was a blue-coloredhand disinfectant lotion. In the analgesia-expectationcondition, children were informed that the study wasevaluating the effectiveness of a powerful lotion thathelps children feel much less pain. In the control-expectation condition, children were told that the lotion

Figure 1. Experimental design. Half of the childrenwere randomly assigned—stratified forMTand gender—to either the analgesia-expectation (blue hand disinfectant as painkiller [upper panel]) or a control-expectation condition (blue hand disinfectant as mea-surement facilitator [lower panel]). Children’s heat pain tolerance and threshold as well as subjective pain judgments by means ofFaces Pain Scale–Revised and FASweremeasured onboth volar forearms (counterbalanced andhomologous site) at baseline and afterthe expectation induction procedure. Participants’ state anxiety was assessed before each of the 2 pain measurements. Trait anxietywas judged at the end of the experiment.
1284 The Journal of Pain Placebo Analgesia and Magical Thinking in Children
was necessary in order to facilitate pain measurementsbut would have no effect on the pain experience itself.Participants in both treatment conditions were dividedinto high- and low-MT groups based on the median spliton their Magical Thinking Questionnaire (MTQ) scores9
(Fig 1). The 4 groups were matched for a comparablegirl-to-boy ratio (c2 = 1.90, P = .593).All participants were tested individually in a quiet
room at constant temperature without their parents.The children could not see the investigator during painassessments. Parents were asked to leave the roombefore the start of the experiment to avoid any psychoso-cial stimulation potentially influencing the child’sbehavior.75 The study session lasted approximately 2hours.One child was frightened by the pain measurements
and withdrew from participation. The last tolerancemeasurement of a second participant is missing becausethe child did not wish to complete it.
Heat Pain Stimuli and MeasurementHeat pain measurement procedures were performed
twice for each participant, at baseline and after treat-ment, regardless of expectation condition. Heat stimuliwere administered in a randomly counterbalanced orderto the left and right volar forearm using a 30 � 30-mmPeltier device (TSA-II; Medoc, Ramat Yishai, Israel) placedat the midpoint between wrist and elbow and securedusing a Velcro strap. To avoid physical injury, the heatpain measurements stopped automatically at 50�C(122.00�F).52 Before the actual measurements, an elabo-rate training session was performed to familiarize theparticipants with the heat sensations and the controllingdevice as well as to ensure that the experimental proce-dure and instructions had been understood properly.
Individual pain thresholdwas measured using the self-control search method starting at 32�C (89.60�F), with amouse-click-induced increase of .1�C (.18�F) per click. Par-ticipants were asked to adjust the magnitude of the heatstimulus till they felt it change from ‘‘hot’’ to ‘‘painful.’’Thus, the child controlled the onset and increase of thethermal stimulation and stopped it when the heatbecame painful. They were further instructed to deter-mine the transition point as precisely as possible. Theexperimenter (C.S.) demonstrated the procedure usingequally long response intervals (ie, constant rate ofmouse clicks per time unit) for augmenting temperature.Pain tolerance was determined by the method of
limits: individuals were asked to stop the heat stimulusthe moment it became too uncomfortable or pain-ful.49,80 Three measurements starting at 32�C (89.60�F),with a rise of 1.5�C/s (2.70�F/s), were averaged.52 Aftereach tolerance measurement, the child first rated painintensity using the Faces Pain Scale–Revised36 and thenthe affective dimension of pain using the Facial AffectiveScale (FAS).51 Pain threshold was always measuredbefore measuring pain tolerance in order to minimizeinterference between pain threshold and tolerance.
Expectation Induction and PlaceboAdministrationRobust placebo and nocebo responses are highly
dependent on the expectations induced during thedescription of the experiment.76 We therefore devel-oped an elaborate child-oriented narrative that used ametaphor to suggest that the experimental lotion hadpowerful analgesic properties.Participants in the analgesia-expectation condition
were told a story by the (female) experimenter (C.S.)about a child who wants to go treasure hunting in the

Krummenacher et al The Journal of Pain 1285
desert accompanied by his or her friend, a lion. To avoidbeing burnt by the hot sand, the child protagonist ap-plies a lotion to his or her hands and feet. The partici-pants were then told that the purpose of theexperiment was to test how well this lotion protects aperson from heat. The placebo, a cool blue–tintedhand disinfectant with no anesthetic properties, wasthen applied on both volar forearms.The analgesia-expectation instruction was as follows:
‘‘This is a lotion that helps children by making you feelmuch less pain. We will measure how much warmer thetemperature can get until it starts hurting and howmuch longer you can wait until you press the button.’’Participants in the control-expectation condition read
a nonfiction animal book with the experimenter, thusensuring the same amount of contact and attentionbut with no induction of analgesia expectations. Thesame hand disinfectant was also applied on both volarforearms with the explanation that the lotion was neces-sary to facilitate measurement and maximize accuracy.The control-expectation instruction was as follows: ‘‘Wewill measure how warm the temperature can get untilit starts to hurt and how long you canwait until you pressthe button. The lotion is necessary to better measure thetemperature of the device.’’The experimenter was trained to convey the instruc-
tions to both groups in a warm, trustful, encouraging,and caring manner because it has been shown that agood relationship between health provider and patientplays an important role in shaping the placeboresponse.38,39 Both instructions were conveyed in astandardized manner to ensure that the participant-experimenter relationship was comparable in terms offriendliness and attention across both treatment groups.
Questionnaires
Magical Thinking
Participants’ MT was assessed at the beginning of theexperiment with the validated 30-item MTQ.9 The MTQhas 2 subscales, thought and action, each consisting of10 questions. The thought subscale questions askwhether it is possible to make an event happen by justthinking about it (eg, ‘‘Is it possible to make somethinggood happen to you or someone else just by thinkingabout it?’’). The action subscale questions ask whetherit is possible to perform an action to make an eventhappen even if the specified action is causally unrelatedto the specified event (eg, ‘‘Is it possible that a friendcould get the flu just because you argued withthem?’’). These 2 subscale scores are combined to formthe MTQ total score. The remaining 10 questions assessbias for responding yes or no. Each question can beanswered with yes, no, or maybe, which are scored as2, 0, or 1 points, respectively. MT scores range from 0 to40, with higher scores indicating more pronounced MT.The authors of the measure report a test-retest reliabilityof .90 (N = 17) for theMTQ total score in a sample of chil-dren and adolescents aged 5–17 years. For the purpose ofthis study, we translated the questionnaire into German.
Subjective Pain Judgments
Participants rated pain intensity and unpleasantnessimmediately after each pain tolerance measurement.Pain intensity was assessed with the Faces Pain Scale–Revised.36 The child was asked to point to the face thatbest reflected his or her experienced pain intensityfrom a series of 6 pictures of facial expressions, arrangedin a horizontal sequence that depicts progressivelyincreasing pain intensity from least to most pain. Thereliability and validity of the Faces Pain Scale–Revisedfor the assessment of pain intensity in children aged 4to 12 years has been repeatedly supported,74 and excel-lent interscale agreement has been demonstrated in chil-dren as young as 4 years of age.36
After the intensity rating, the child rated the affectivedimension of pain using the FAS.51 The FAS is a self-report measure used to assess the unpleasantness of achild’s pain experience. It is composed of 9 face drawingspresented in a randomized 3-by-3 matrix representinggradual increases in distress. The child was asked tochoose the face that best fit his or her affective statefrom the set of faces. The specific instructions were as fol-lows: ‘‘Now I amgoing to show you some faces and I wantyou to choose the face that looks like how you feel downinside. Choose the face that looks like how you feel downinside, not just the face you showon the outside.’’ The FASis scored on a 0 to 1 scale, where the maximum negativeaffective value equals 1 and the maximum positive valueequals 0. The endpoints were explained as ‘‘very happy’’and ‘‘very sad.’’ The FAS has been validated in a sampleof children aged 5 to 17 years.51
Measurement of Participants’ Anxiety
Participant anxiety was assessed with the State-TraitAnxiety Inventory for Children (STAIC).70 The STAIC con-sists of two 20-item self-report scales. Each item is ratedon a 3-point intensity scale. The trait scale measureslong-term trait anxiety, which addresses how the childgenerally feels, while the state scale measures short-term anxiety specific to a particular moment in time.The STAIC was originally designed and normed for usewith fourth-, fifth-, and sixth-graders (aged 9–12 years),though the usefulness of the STAIC has also been demon-strated in younger children (6–9 years) with average orabove average reading ability.35 Both the STAIC-Statesubscale (Cronbach’s alpha ranging from .71 to .76) andthe STAIC-Trait subscale (Cronbach’s alpha rangingfrom .82 to .89) have demonstrated good reliability coef-ficients.59 State anxiety (STAIC-S) was assessed prior toeach of the 2 pain measurements. Trait anxiety (STAIC-T) was measured at the end of the experiment.
Subjective Treatment Efficacy
In order to minimize social reporting biases, perceivedtreatment efficacy was assessed indirectly after all painmeasurements had been taken using systemic relationalcircular open-ended questions. In particular, the childwas asked how he or she would describe the functionof the lotion to parents, siblings, or friends, and whetherhe or she would recommend the lotion to those persons.

1286 The Journal of Pain Placebo Analgesia and Magical Thinking in Children
Perception of the Experimenter
After subjective treatment efficacy was assessed, thelikeability of the experimenter (C.S.) was measured indi-rectly by using a relational circular open-ended question-naire assessing what the child would tell parents,siblings, or friends about the experimenter.
Statistical AnalysesInitially, 4 separate 3-way analyses of variance
(ANOVAs) were conducted with strength of right-handedness, trait anxiety, baseline state anxiety, andage as dependent variables. The independent variableswere treatment condition (analgesia vs control), MTgroup (high vs low), and gender (boys vs girls). To assessthe effect of treatment condition on state anxiety, wecomputed a difference score by subtracting posttreat-ment state anxiety from pretreatment state anxiety.To assess placebo responses, the principal outcome
measures were within-subject difference scores betweenbaseline and posttreatment for heat pain threshold andtolerance (in degrees Celsius). Negative values indicatelower threshold and tolerance compared to baseline.Positive values indicate placebo analgesia. For these 2outcomes, group differences were analyzed using 2separate 4-way, repeated-measures analyses of covari-ance (ANCOVAs) with treatment condition (analgesia vscontrol), MT group (high vs low), and gender (girls vsboys) as the 3 between-subject factors, and the forearmside of pain application (right vs left) as the solewithin-subject factor, and including age and trait anxietyas covariates. The selection of the 2 covariates was basedon the results of the 4 initial 3-way ANOVAs.In order to assess effects of repeated pain measure-
ments (eg, altered sensitivity or fatigue), deviationsfrom baseline were tested by means of 1-sample t-testsand were compared against a value of zero.Subjective pain rating differences between treatment
and baseline condition were analyzed using nonpara-metric tests, because an interval level of children’s painintensity and unpleasantness ratings cannot be guaran-teed. The difference scores between treatment and base-line were subjected to Mann-Whitney U tests for thetreatment condition, MT, and gender factors, and toWilcoxon signed rank test for related samples for theforearm-side factor.
Perceived Treatment Efficacy
The open-ended answers that the children providedregarding the efficacy of the lotion were categorizedinto 4 degrees of perceived treatment efficacy: 1) ‘‘noefficacy,’’ 2) ‘‘a little helpful’’ (eg, ‘‘it stopped the pain,but only a little’’), 3) ‘‘helpful’’ (eg, it hurts less with theblue lotion), and 4) ‘‘very helpful’’ (eg, I could waitmuch longer until it started to hurt).To assess experimenter likeability, children were asked
about the experimenter. All gave a positive answer andused at least 1 of the following adjectives: nice, great,good, or funny. The answers were categorized into 3groups: 1) only 1 of these adjectives, 2) more than 1adjective or positive characteristics (eg, polite, you had
good ideas, or I trusted you), and 3) 1 or more adjectivesor characteristics reinforced with ‘‘very, very much’’ or asimilar expression. Associations between perceived treat-ment efficacy or likeability and the different groups(treatment condition, MT, and gender group) wereanalyzed with chi-square tests.Post hoc comparisons were performed using 2-tailed
Student t-tests. Homogeneity of covariance matriceswas checked by Box’s M tests (pain tolerance; F = 1.189,P = .249). Homogeneity of variances in the pain measurewas assessed using Levene’s test (pain tolerance;F = 1.677, P = .143). Normal distribution of these 2 mea-sures was assessed by the Kolmogorov-Smirnov test(Z # .933, Ps $ .348). All P values are 2-tailed, and thelevel of significance was set to a # .05. Sphericity wasassessed, and when the assumption was violated, theGreenhouse-Geisser correction was applied.All statistical analyses were computed using SPSS for
Mac, version 21 (IBM Corp, Armonk, NY).
Results
Subject CharacteristicsThe 8 groups (treatment condition � MT group �
gender) did not differ in strength of right-handedness(F[1, 40] # 1.846, Ps $ .182) or baseline state anxiety(F[1, 40] # 3.126, Ps $ .084). However, there were groupdifferences in trait anxiety (F[1, 40] # 5.149, Ps $ .029)and age (F[1, 40] # 7.399, Ps $ .010) (Table 1).
State AnxietyThe 3-way ANOVA for state anxiety difference
scores revealed neither statistically significant maineffects (F[1, 40] # 1.657, Ps $ .205) nor interactions(F[1, 40] # 2.351, Ps $ .133).
Pain ThresholdThe ANOVA for pain threshold indicated a significant
main effect for treatment condition (F[1, 38] = 59.950,P < .001, hp
2 = .612, Cohen’s d = 2.512; analgesia >control) and for the covariate trait anxiety (F[1, 38] =5.384, P = .026, hp
2 = .124, Cohen’s d = .753; low > high).Among the 2-way interactions, those between treatmentcondition and gender (F[1, 38] = 9.778, P = .003,hp
2 = .205)and MT group and gender (F[1, 38] = 5.221, P = .028,hp
2 = .121)were significant. For the first interaction (treat-ment condition� gender), post hoc comparisons revealeda higher pain threshold score in the analgesia-expectationthan in the control-expectation condition for boys(P = .003) and girls (P < .001, Fig 2). Moreover, in theanalgesia-expectation condition, the pain threshold scoreincrease was comparable for the 2 gender groups(P = .083), but there was a lower threshold score in girlsas compared to boys in the control-expectation group(P = .036) (Fig 2).For the second interaction (MT group � gender), post
hoc comparisons showed a marginally higher thresholdscore for the boys in the low-MT compared to the high-MT group (P = .078), but no such difference for the girls(P = .869) (Fig 3).
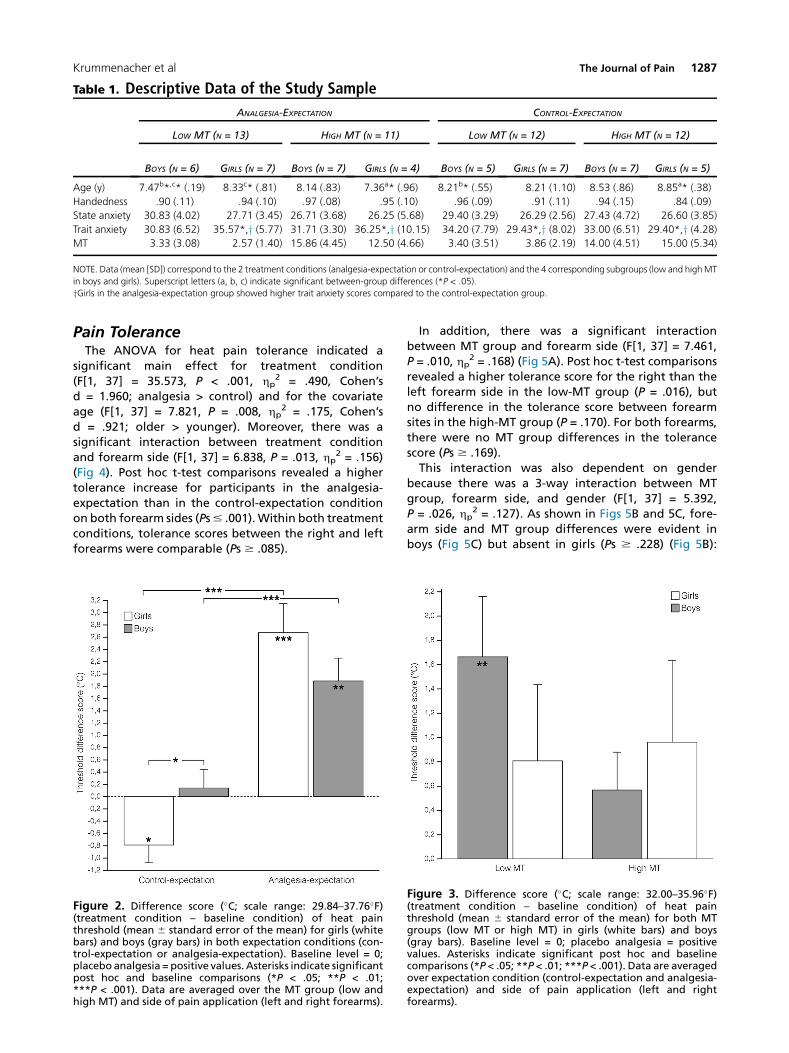
Table 1. Descriptive Data of the Study Sample
ANALGESIA-EXPECTATION CONTROL-EXPECTATION
LOW MT (N = 13) HIGH MT (N = 11) LOW MT (N = 12) HIGH MT (N = 12)
BOYS (N = 6) GIRLS (N = 7) BOYS (N = 7) GIRLS (N = 4) BOYS (N = 5) GIRLS (N = 7) BOYS (N = 7) GIRLS (N = 5)
Age (y) 7.47b*,c* (.19) 8.33c* (.81) 8.14 (.83) 7.36a* (.96) 8.21b* (.55) 8.21 (1.10) 8.53 (.86) 8.85a* (.38)
Handedness .90 (.11) .94 (.10) .97 (.08) .95 (.10) .96 (.09) .91 (.11) .94 (.15) .84 (.09)
State anxiety 30.83 (4.02) 27.71 (3.45) 26.71 (3.68) 26.25 (5.68) 29.40 (3.29) 26.29 (2.56) 27.43 (4.72) 26.60 (3.85)
Trait anxiety 30.83 (6.52) 35.57*,y (5.77) 31.71 (3.30) 36.25*,y (10.15) 34.20 (7.79) 29.43*,y (8.02) 33.00 (6.51) 29.40*,y (4.28)MT 3.33 (3.08) 2.57 (1.40) 15.86 (4.45) 12.50 (4.66) 3.40 (3.51) 3.86 (2.19) 14.00 (4.51) 15.00 (5.34)
NOTE. Data (mean [SD]) correspond to the 2 treatment conditions (analgesia-expectation or control-expectation) and the 4 corresponding subgroups (low and highMT
in boys and girls). Superscript letters (a, b, c) indicate significant between-group differences (*P < .05).
yGirls in the analgesia-expectation group showed higher trait anxiety scores compared to the control-expectation group.
Krummenacher et al The Journal of Pain 1287
Pain ToleranceThe ANOVA for heat pain tolerance indicated a
significant main effect for treatment condition(F[1, 37] = 35.573, P < .001, hp
2 = .490, Cohen’sd = 1.960; analgesia > control) and for the covariateage (F[1, 37] = 7.821, P = .008, hp
2 = .175, Cohen’sd = .921; older > younger). Moreover, there was asignificant interaction between treatment conditionand forearm side (F[1, 37] = 6.838, P = .013, hp
2 = .156)(Fig 4). Post hoc t-test comparisons revealed a highertolerance increase for participants in the analgesia-expectation than in the control-expectation conditionon both forearm sides (Ps# .001).Within both treatmentconditions, tolerance scores between the right and leftforearms were comparable (Ps $ .085).
Figure 2. Difference score (�C; scale range: 29.84–37.76�F)(treatment condition – baseline condition) of heat painthreshold (mean 6 standard error of the mean) for girls (whitebars) and boys (gray bars) in both expectation conditions (con-trol-expectation or analgesia-expectation). Baseline level = 0;placebo analgesia = positive values. Asterisks indicate significantpost hoc and baseline comparisons (*P < .05; **P < .01;***P < .001). Data are averaged over the MT group (low andhigh MT) and side of pain application (left and right forearms).
In addition, there was a significant interactionbetween MT group and forearm side (F[1, 37] = 7.461,P = .010, hp
2 = .168) (Fig 5A). Post hoc t-test comparisonsrevealed a higher tolerance score for the right than theleft forearm side in the low-MT group (P = .016), butno difference in the tolerance score between forearmsites in the high-MT group (P = .170). For both forearms,there were no MT group differences in the tolerancescore (Ps $ .169).This interaction was also dependent on gender
because there was a 3-way interaction between MTgroup, forearm side, and gender (F[1, 37] = 5.392,P = .026, hp
2 = .127). As shown in Figs 5B and 5C, fore-arm side and MT group differences were evident inboys (Fig 5C) but absent in girls (Ps $ .228) (Fig 5B):
Figure 3. Difference score (�C; scale range: 32.00–35.96�F)(treatment condition – baseline condition) of heat painthreshold (mean 6 standard error of the mean) for both MTgroups (low MT or high MT) in girls (white bars) and boys(gray bars). Baseline level = 0; placebo analgesia = positivevalues. Asterisks indicate significant post hoc and baselinecomparisons (*P < .05; **P < .01; ***P < .001). Data are averagedover expectation condition (control-expectation and analgesia-expectation) and side of pain application (left and rightforearms).
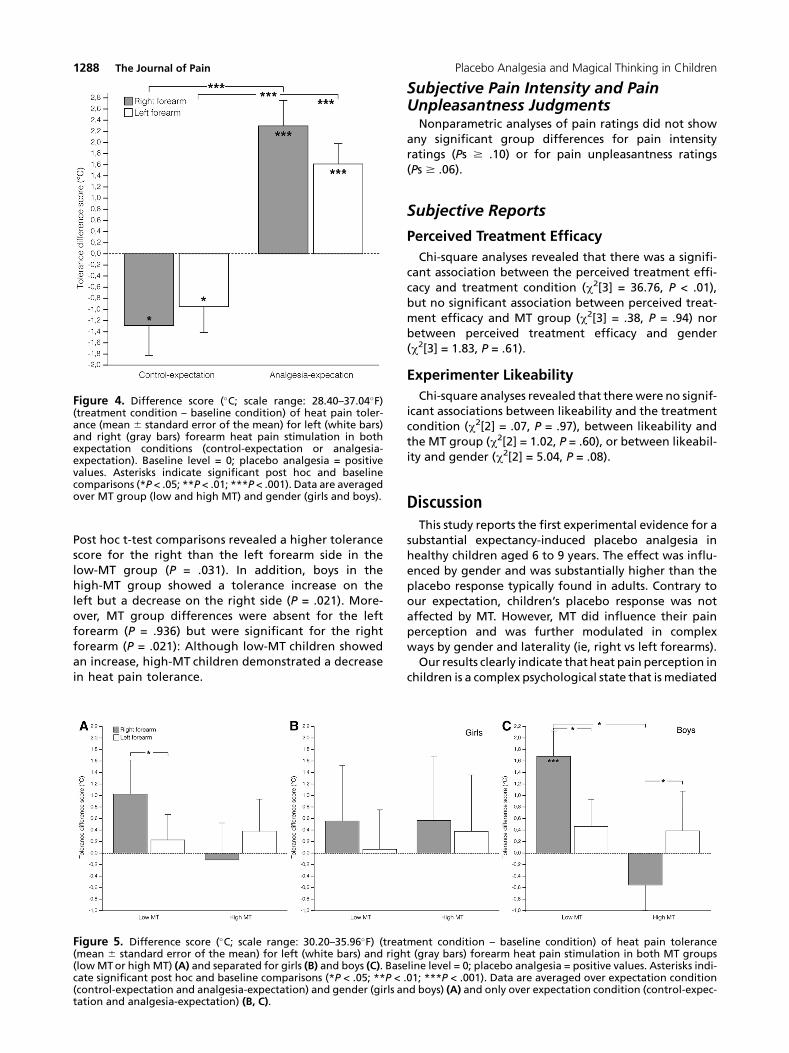
Figure 4. Difference score (�C; scale range: 28.40–37.04�F)(treatment condition – baseline condition) of heat pain toler-ance (mean 6 standard error of the mean) for left (white bars)and right (gray bars) forearm heat pain stimulation in bothexpectation conditions (control-expectation or analgesia-expectation). Baseline level = 0; placebo analgesia = positivevalues. Asterisks indicate significant post hoc and baselinecomparisons (*P < .05; **P < .01; ***P < .001). Data are averagedover MT group (low and high MT) and gender (girls and boys).
1288 The Journal of Pain Placebo Analgesia and Magical Thinking in Children
Post hoc t-test comparisons revealed a higher tolerancescore for the right than the left forearm side in thelow-MT group (P = .031). In addition, boys in thehigh-MT group showed a tolerance increase on theleft but a decrease on the right side (P = .021). More-over, MT group differences were absent for the leftforearm (P = .936) but were significant for the rightforearm (P = .021): Although low-MT children showedan increase, high-MT children demonstrated a decreasein heat pain tolerance.
Figure 5. Difference score (�C; scale range: 30.20–35.96�F) (treat(mean 6 standard error of the mean) for left (white bars) and righ(lowMTor high MT) (A) and separated for girls (B) and boys (C). Basecate significant post hoc and baseline comparisons (*P < .05; **P <(control-expectation and analgesia-expectation) and gender (girls antation and analgesia-expectation) (B, C).
Subjective Pain Intensity and PainUnpleasantness JudgmentsNonparametric analyses of pain ratings did not show
any significant group differences for pain intensityratings (Ps $ .10) or for pain unpleasantness ratings(Ps $ .06).
Subjective Reports
Perceived Treatment Efficacy
Chi-square analyses revealed that there was a signifi-cant association between the perceived treatment effi-cacy and treatment condition (c2[3] = 36.76, P < .01),but no significant association between perceived treat-ment efficacy and MT group (c2[3] = .38, P = .94) norbetween perceived treatment efficacy and gender(c2[3] = 1.83, P = .61).
Experimenter Likeability
Chi-square analyses revealed that therewere no signif-icant associations between likeability and the treatmentcondition (c2[2] = .07, P = .97), between likeability andthe MT group (c2[2] = 1.02, P = .60), or between likeabil-ity and gender (c2[2] = 5.04, P = .08).
DiscussionThis study reports the first experimental evidence for a
substantial expectancy-induced placebo analgesia inhealthy children aged 6 to 9 years. The effect was influ-enced by gender and was substantially higher than theplacebo response typically found in adults. Contrary toour expectation, children’s placebo response was notaffected by MT. However, MT did influence their painperception and was further modulated in complexways by gender and laterality (ie, right vs left forearms).Our results clearly indicate that heat pain perception in
children is a complex psychological state that is mediated
ment condition – baseline condition) of heat pain tolerancet (gray bars) forearm heat pain stimulation in both MT groupsline level = 0; placebo analgesia = positive values. Asterisks indi-.01; ***P < .001). Data are averaged over expectation conditiond boys) (A) and only over expectation condition (control-expec-

Krummenacher et al The Journal of Pain 1289
by context-induced, short-term expectancies of anal-gesia as well as long-term beliefs such as MT.
Placebo Analgesia ResponsesIn line with our first hypothesis, children exposed to
the ‘‘analgesia-expectation’’ condition via a single ver-bal suggestion with a strong metaphorical characterdemonstrated a substantial placebo analgesia response,as shown by a significant increase in heat pain toleranceand threshold on both forearm sides. Moreover, theanalgesia expectancy effect for heat pain thresholdwas greater for girls than for boys. All associated subjec-tive pain ratings were uninfluenced by any of thesefactors.It has been suggested that children and adolescents
generally show larger placebo responses thanadults.60,79 Our experimental approach stronglysupports this age effect. The difference scores betweenbaseline and posttreatment in the analgesia-expectation group were 5.6 times higher for heat paintolerance and 3.6 times higher for heat pain thresholdthan those found in a healthy adult sample using asimilar paradigm.43 Several psychological and neurode-velopmental reasons may account for the larger placeboresponses in children. First, children may be predisposedto larger placebo responses because of their higher sug-gestibility.60 Suggestibility changes over the processesof neurodevelopment58 and has been shown to increasesteadily from an early age, to peak between 9 and12 years, and to decline thereafter.56 Moreover, concep-tualizing placebo processes as learning phenomena,24
children may show higher placebo responses becauseof their possibly greater learning capacities, opennessto new experiences, and learning motivation.60 Also,Parellada et al pointed out that children’s framing andbelief system might not yet have been modulated byexperience as it is in adults.60 Similarly, their predictionand prejudice system is not yet shaped by learning.Finally, the larger placebo responses may also relate todifferences in placebo interventions. Indeed, hero roleplaying–induced modulation of self-perception hasbeen demonstrated to increase heat pain tolerance inhealthy adults.45
There are several reasons why experimenter or‘‘parent’’ bias are unlikely as explanations for the presentfindings: 1) All children were tested individually withouttheir parents, 2) children were visually shielded from theexperimenter during the pain assessment, and 3) experi-menter and study likability—assessed via systemic indi-rect circular questions—were not judged differentlyacross the treatment conditions.Expectations of analgesia induced by verbal sugges-
tions have been repeatedly demonstrated to be pivotalinitiators and modulators of placebo responses.6 Severalpsychological mechanisms have been proposed toexplain placebo analgesia, including such activation ofreward processes,25,48 reframing,7 reduction in self-defeating thoughts,72 motivational gain,64 and anxietyreduction.61 However, anxiety reduction seems to be anunlikely explanation for our results. Although highertrait anxiety scores were associated with lower heat
pain threshold scores, state anxiety difference scoreswere comparable in both treatment conditions.Our behavioral data only allow for speculation about
the neural underpinnings that might explain why chil-dren appear to exhibit a more robust placebo analgesiaresponse as compared to adults. There are, of course,significant structural and functional differences be-tween adults and children.31 The PFC6,43 and itsconnectivity with the rest of the brain71 has beenrepeatedly demonstrated as being critically importantin the top-down, expectation-mediated model of adultplacebo responses. The PFC does not reachmaturity andfull connectivity until at least adolescence, and possiblynot even until early adulthood.18,31,32 Moreover,patterns of cortical activation during cognitive taskssuch as word generation,11 response inhibition16 andselective attention10 have been reported to be morediffuse in children and to rely more on subcortical brainnetwork activation.50 The changing balance betweenearly-maturing subcortical and limbic systems andlate-maturing, high-association frontal lobe corticalnetworks17 make comparisons between pediatric andadult populations difficult. Presumably, expectation-related placebo analgesia in children relies more onsubcortical neural pathways and processing strategiesrelative to adults’ susceptibility to placebo treatment.As contrasted with a more cognitively mediated pla-cebo analgesia in adults, we speculate that in children,reward-related motivational and emotional appraisal(eg, safety) and associated changes in intrasubcorticallimbic-related circuitries77 as well as attachment maybe critical mediators of placebo analgesia.
Gender-Dependent Differences inPlacebo AnalgesiaThe placebo response for heat pain threshold was
stronger for girls compared with boys. The literatureregarding gender differences in placebo responding issparse and equivocal,28 and studies of gender-specificplacebo responses in the pediatric population havebeen especially neglected.79 Whereas one review failedto find differences,29 another reported a slight placebosusceptibility advantage for girls in a migraine head-ache.47 In the adult population, several factors havebeen proposed as explanations for gender differencesin placebo responding, including differences in stresslevels, cortical processing styles, type of placebo learningparadigm, hormonal influences, reporting biases, or thegender of the experimenter.28 Given that our partici-pants were prepubertal, our results suggest mechanismsother than hormonal influences, such as a slightly highersuggestibility for girls53 (but see Bruck et al12 for anopposing view), which is not attributable to differencesin receptive language skills.12
MT Modulates Pain Processing in Boys,but Not Placebo AnalgesiaThe findings both contradict and support our original
hypotheses. Contrary to our prediction, placebo anal-gesia was not influenced by MT. Previous findings in a

1290 The Journal of Pain Placebo Analgesia and Magical Thinking in Children
study by Klemenz et al in healthy adults suggestedgreater placebo susceptibility for high-MT participants.41
Several reasons may account for our failure to replicatethis finding. First, pronounced MT is a healthy propertyof a child’s thinking62,81 and not an indicator ofsubclinical psychotic development.26 Therefore, quanti-tative and qualitative differences in youngsters’ versusadults’ MT may hamper direct comparison with previousstudies. Likewise, suggestibility is extremely high ataround 12 years of age,3whichmay have blurred hypoth-esized MT-related suggestibility differences because of aceiling effect. Lastly, these inconsistenciesmay have beenproduced by differences in the type of pain stimuli andthe absence of a control group without a placebo inter-vention in the study conducted by Klemenz et al.41
In line with our hypothesis, pain perception was asym-metrically modulated by MT. In the group with low MT,pain tolerancewas higher for the right than the left fore-arm. Surprisingly, however, no such difference wasobserved in the high-MT group. This modulation is anexact replication of the pattern that has recently beenreported in a similar study with healthy men41 and maybe a consequence of reduced functional hemisphericdifferences characteristic of declared MT in adults, onboth the behavioral44,46 and electrophysiologicallevels.63 The present result suggests that the associationbetweenMTand a heightened right hemispheric activity,previously described in adults,14,55 can also be observedin children. A general bias toward right-hemisphere pro-cessing has long been described in infants and children.19
However, the complex interaction among gender, MT,and the laterality of pain perception must await furtherresearch.
Limitations, Implications, and FutureStudiesUndoubtedly, our study findings require replication in
larger samples. Moreover, the underlying neural mecha-nisms of expectation-induced placebo analgesia need tobe unraveled, especially as they relate to the cognitiveand emotional development of children. It would beinteresting to compare children with adults to examinehow progressively greater maturity in cognitive andmotivational neurodevelopment affects placeboresponses, focusing especially on the connections be-tween subcortical areas and the prefrontal cortex.
Regarding assessment tools, the German adaption oftheMTQ needs to be validated in a large sample. In addi-tion, given that heat pain threshold was difficult toassess reliably in our study, more intuitive, real-time,and nonverbal measurement tools such as the recentlyproposed ‘‘pain mouse’’65 or immediate analgesic rescuedesigns42 could be implemented in future pain assess-ment designs.The generalizability and potential implications to clin-
ical practice of our data are limited because our studywas designed to investigate the role of experimentallyinduced placebo analgesia in acute, controllable thermalpain. Also, our present data do not allow us to disen-tangle the different components of the placebo inter-vention, such as the expectancy-inducing narrative; thecolor, smell, or other characteristics of the disinfectant;or the warm relationship with the experimenter. Futurestudies should compare different types of verbal versusnonverbal and conscious versus nonconscious sugges-tions,38 as well as investigate the use of other learningparadigms such as associative learning and learning byobservation21 and imitation to induce placebo responsesin children.In conclusion, the present study provides the first
experimental evidence for a substantial expectation-related placebo analgesia response on pain thresholdand pain tolerance in healthy children. In addition, inde-pendent of analgesia expectations, MT modulated paintolerance exclusively in male children. Overall, thisresearch suggests that context-induced, short-term anal-gesia expectations and long-term MT beliefs indepen-dently modulate the experience of pain. These findingschallenge the simple view of interpolating adult findingsto the pediatric population. An improved understandingof the interaction among subjective belief and meaningsystems, gender, and age-related neurodevelopmentalphases in pain processing has the potential to enhancetherapeutic outcomes in the individualized manage-ment of children’s pain.69
AcknowledgmentsWe thank Marco Annoni for thoughtful advice
regarding ethical issues and Ted Kaptchuk for helpfulcomments in the preparation phase of the manuscript.
References
1. Abbott K, Fowler-Kerry S: The use of a topical refrigerantanesthetic to reduce injection pain in children. J Pain Symp-tom Manage 10:584-590, 1995
2. Arts SE, Abu-Saad HH, Champion GD, Crawford MR,Fisher RJ, Juniper KH, Ziegler JB: Age-related response tolidocaine-prilocaine (EMLA) emulsion and effect of musicdistraction on the pain of intravenous cannulation. Pediat-rics 93:797-801, 1994
3. BaumanDE, Bul PI: [Human inheritability of hypnotizabil-ity]. Genetika 17:352-356, 1981
4. Benedetti F: Mechanisms of placebo and placebo-relatedeffects across diseases and treatments. Annu Rev PharmacolToxicol 48:33-60, 2008
5. Benedetti F: Placebo and the new physiology of thedoctor-patient relationship. Physiol Rev 93:1207-1246,2013
6. Benedetti F, Arduino C, Costa S, Vighetti S, Tarenzi L,Rainero I, Asteggiano G: Loss of expectation-related mecha-nisms in Alzheimer’s disease makes analgesic therapies lesseffective. Pain 121:133-144, 2006
7. Benedetti F, ThoenW, Blanchard C, Vighetti S, Arduino C:Pain as a reward: Changing the meaning of pain from
Krummenacher et al The Journal of Pain 1291
negative to positive co-activates opioid and cannabinoidsystems. Pain 154:361-367, 2013
8. Bingel U, Wanigasekera V, Wiech K, NiMhuircheartaigh R, Lee MC, Ploner M, Tracey I: The effectof treatment expectation on drug efficacy: Imaging theanalgesic benefit of the opioid remifentanil. Sci TranslMed 3:70ra14, 2011
9. Bolton D, Dearsley P, Madronal-Luque R, Baron-Cohen S:Magical thinking in childhood and adolescence: Develop-ment and relation to obsessive compulsion. Br J Dev Psychol20:479-494, 2002
10. Booth JR, Burman DD, Meyer JR, Trommer BL,Davenport ND, Parrish TB, Gitelman DR, Mesulam MM:Brain-behavior correlation in children depends on the neu-rocognitive network. Hum Brain Mapp 23:99-108, 2004
11. Brown TT, Lugar HM, Coalson RS, Miezin FM,Petersen SE, Schlaggar BL: Developmental changes in hu-man cerebral functional organization for word generation.Cereb Cortex 15:275-290, 2005
12. Bruck M, Melnyk L: Individual differences in children’ssuggestibility: A review and synthesis. Appl Cognit Psychol18:947-996, 2004
13. Brugger P: Tracking a finer madness. Sci Am Mind 10:77-79, 2007
14. Brugger P,Mohr C: The paranormalmind: How the studyof anomalous experiences and beliefs may inform cognitiveneuroscience. Cortex 44:1291-1298, 2008
15. Buck M: The placebo response in pediatric clinical trials.Pediatr Pharmacol 18, 2012
16. Casey BJ, Castellanos FX, Giedd JN, Marsh WL,Hamburger SD, Schubert AB, Vauss YC, Vaituzis AC,Dickstein DP, Sarfatti SE, Rapoport JL: Implication of rightfrontostriatal circuitry in response inhibition andattention-deficit/hyperactivity disorder. J Am Acad ChildAdolesc Psychiatry 36:374-383, 1997
17. Casey BJ, Duhoux S, Malter Cohen M: Adolescence:What do transmission, transition, and translation have todo with it? Neuron 67:749-760, 2010
18. Casey BJ, Tottenham N, Liston C, Durston S: Imaging thedeveloping brain: What have we learned about cognitivedevelopment? Trends Cogn Sci 9:104-110, 2005
19. Chiron C, Jambaque I, Nabbout R, Lounes R, Syrota A,Dulac O: The right brain hemisphere is dominant in humaninfants. Brain 120(Pt 6):1057-1065, 1997
20. Coghill RC, Gilron I, Iadarola MJ: Hemispheric lateraliza-tion of somatosensory processing. J Neurophysiol 85:2602-2612, 2001
21. Colloca L, Benedetti F: Placebo analgesia induced by so-cial observational learning. Pain 144:28-34, 2009
22. Colloca L, Klinger R, Flor H, Bingel U: Placebo analgesia:Psychological and neurobiological mechanisms. Pain 154:511-514, 2013
23. Colloca L, Miller FG: How placebo responses are formed:A learning perspective. Philos Trans R Soc Lond B Biol Sci 366:1859-1869, 2011
24. Colloca L, SigaudoM, Benedetti F: The role of learning innocebo and placebo effects. Pain 136:211-218, 2008
25. de la Fuente-Fernandez R, Ruth TJ, Sossi V, Schulzer M,Calne DB, Stoessl AJ: Expectation and dopamine release:
Mechanism of the placebo effect in Parkinson’s disease. Sci-ence 293:1164-1166, 2001
26. Eckblad M, Chapman LJ: Magical ideation as an indi-cator of schizotypy. J Consult Clin Psychol 51:215-225,1983
27. Eippert F, Bingel U, Schoell ED, Yacubian J, Klinger R,Lorenz J, Buchel C: Activation of the opioidergic descendingpain control system underlies placebo analgesia. Neuron 63:533-543, 2009
28. Enck P, Benedetti F, Schedlowski M: New insights intothe placebo and nocebo responses. Neuron 59:195-206,2008
29. Evers S, Marziniak M, Frese A, Gralow I: Placebo efficacyin childhood and adolescence migraine: An analysis ofdouble-blind and placebo-controlled studies. Cephalalgia29:436-444, 2009
30. Folley BS, Park S: Verbal creativity and schizotypal per-sonality in relation to prefrontal hemispheric laterality: Abehavioral and near-infrared optical imaging study. Schiz-ophr Res 80:271-282, 2005
31. Giedd JN, Rapoport JL: Structural MRI of pediatric braindevelopment: What have we learned and where are wegoing? Neuron 67:728-734, 2010
32. Gogtay N, Giedd JN, Lusk L, Hayashi KM, Greenstein D,Vaituzis AC, Nugent TF 3rd, Herman DH, Clasen LS,Toga AW, Rapoport JL, Thompson PM: Dynamic mappingof human cortical development during childhood throughearly adulthood. Proc Natl Acad Sci U S A 101:8174-8179,2004
33. Goodenough B, Kampel L, Champion GD, Laubreaux L,Nicholas MK, Ziegler JB, McInerney M: An investigation ofthe placebo effect and age-related factors in the report ofneedle pain from venipuncture in children. Pain 72:383-391, 1997
34. Grob A, Meyer CS, Hagmann-von Arx P: Intelligence andDevelopment Scales (IDS). Bern, Hans Huber, 2009
35. Hedl JJ, Papay JP: The factor structure of the State-TraitAnxiety Inventory for Children: Kindergarten through thefourth grades. Pers Indiv Differ 3:439-446, 1982
36. Hicks CL, von Baeyer CL, Spafford PA, van Korlaar I,Goodenough B: The Faces Pain Scale-Revised: Toward a com-monmetric in pediatric painmeasurement. Pain 93:173-183,2001
37. Jensen KB, Kaptchuk TJ, Kirsch I, Raicek J, LindstromKM,Berna C, Gollub RL, Ingvar M, Kong J: Nonconscious activa-tion of placebo and nocebo pain responses. Proc Natl AcadSci U S A 109:15959-15964, 2012
38. Kaptchuk TJ, Kelley JM, Conboy LA, Davis RB, Kerr CE,Jacobson EE, Kirsch I, Schyner RN, Nam BH, Nguyen LT,Park M, Rivers AL, McManus C, Kokkotou E, Drossman DA,Goldman P, Lembo AJ: Components of placebo effect: Rand-omised controlled trial in patients with irritable bowel syn-drome. BMJ 336:999-1003, 2008
39. Kelley JM, LemboAJ, Ablon JS, Villanueva JJ, Conboy LA,Levy R, Marci CD, Kerr CE, Kirsch I, Jacobson EE, Riess H,Kaptchuk TJ: Patient and practitioner influences on the pla-cebo effect in irritable bowel syndrome. PsychosomMed 71:789-797, 2009
40. Kirsch I, Sapirstein G: Listening to Prozac but hearingplacebo: A meta-analysis of antidepressant medication.Prev Treatment 1:2a, 1998
1292 The Journal of Pain Placebo Analgesia and Magical Thinking in Children
41. Klemenz C, Regard M, Brugger P, Emch O: Laterality ofpain: Modulation by placebo and participants’ paranormalbelief. Cogn Behav Neurol 22:186-189, 2009
42. Kossowsky J, Donado C, Berde CB: Immediate rescue de-signs in pediatric analgesic trials: A systematic review andmeta-analysis. Anesthesiology. 2014 Sep 12. http://dx.doi.org/10.1097/ALN.0000000000000445
43. Krummenacher P, Candia V, Folkers G, Schedlowski M,Sch€onb€achler G: Prefrontal cortex modulates placebo anal-gesia. Pain 148:368-374, 2010
44. Krummenacher P, Mohr C, Haker H, Brugger P: Dopa-mine, paranormal belief, and the detection of meaningfulstimuli. J Cogn Neurosci 22:1670-1681, 2010
45. Kut E, Schaffner N, Wittwer A, Candia V, Brockmann M,Storck C, Folkers G: Changes in self-perceived role identitymodulate pain perception. Pain 131:191-201, 2007
46. Leonhard D, Brugger P: Creative, paranormal, and delu-sional thought: A consequence of right hemisphere seman-tic activation? Neuropsychiatry Neuropsychol Behav Neurol11:177-183, 1998
47. Lewis DW, Kellstein D, Dahl G, Burke B, Frank LM, Toor S,Northam RS, White LW, Lawson L: Children’s ibuprofen sus-pension for the acute treatment of pediatric migraine.Headache 42:780-786, 2002
48. Lidstone SC, Schulzer M, Dinelle K, Mak E, Sossi V,Ruth TJ, de la Fuente-Fernandez R, Phillips AG, Stoessl AJ:Effects of expectation on placebo-induced dopaminerelease in Parkinson disease. Arch Gen Psychiatry 67:857-865, 2010
49. Lu Q, Zeltzer LK, Tsao JC, Kim SC, Turk N, Naliboff BD:Heart rate mediation of sex differences in pain tolerancein children. Pain 118:185-193, 2005
50. Luna B, Thulborn KR, Munoz DP, Merriam EP, Garver KE,Minshew NJ, Keshavan MS, Genovese CR, Eddy WF,Sweeney JA: Maturation of widely distributed brain func-tion subserves cognitive development. Neuroimage 13:786-793, 2001
51. McGrath PA, Seifert CE, Speechley KN, Booth JC, Stitt L,Gibson MC: A new analogue scale for assessing children’spain: An initial validation study. Pain 64:435-443, 1996
52. Meier PM, Berde CB, DiCanzio J, Zurakowski D,Sethna NF: Quantitative assessment of cutaneous thermaland vibration sensation and thermal pain detection thresh-olds in healthy children and adolescents. Muscle Nerve 24:1339-1345, 2001
53. Messerschmidt R: The suggestibility of boys and girls be-tween the ages of six and sixteen years. Pedagogical Semin JGenet Psychol 43:422-437, 1933
54. Mohr C, Bracha HS, Brugger P: Magical ideation modu-lates spatial behavior. J Neuropsychiatry Clin Neurosci 15:168-174, 2003
55. Mohr C, Krummenacher P, Landis T, Sandor PS, Fathi M,Brugger P: Psychometric schizotypy modulates levodopaeffects on lateralized lexical decision performance. J Psy-chiatr Res 39:241-250, 2005
56. Morgan AH, Ernest RH: Age differences in susceptibilityto hypnosis. Int J Clin Exp Hypn 21:78-85, 1973
57. Oldfield RC: The assessment and analysis of handedness:The Edinburgh inventory. Neuropsychologia 9:97-113, 1971
58. Page RA, Green JP: An update on age, hypnotic suggest-ibility, and gender: A brief report. Am J Clin Hypn 49:283-287, 2007
59. Papay JP, Spielberger CD: Assessment of anxiety andachievement in kindergarten and first- and second-grade children. J Abnorm Child Psychol 14:279-286,1986
60. Parellada M, Moreno C, Moreno M, Espliego A, dePortugal E, Arango C: Placebo effect in child and adolescentpsychiatric trials. Eur Neuropsychopharmacol 22:787-799,2012
61. Petrovic P, Dietrich T, Fransson P, Andersson J, Carlsson K,Ingvar M: Placebo in emotional processing–induced expec-tations of anxiety relief activate a generalized modulatorynetwork. Neuron 46:957-969, 2005
62. Piaget JP: The Child’s Conception of the World. London,Routledge & Kegan Paul, 1929
63. Pizzagalli D, Lehmann D, Gianotti L, Koenig T, Tanaka H,Wackermann J, Brugger P: Brain electric correlates of strongbelief in paranormal phenomena: Intracerebral EEG sourceand regional Omega complexity analyses. Psychiatry Res100:139-154, 2000
64. Price DD, Finniss DG, Benedetti F: A comprehensivereview of the placebo effect: Recent advances and currentthought. Annu Rev Psychol 59:565-590, 2008
65. Schaffner N, Folkers G, Kappeli S, Musholt M,Hofbauer GF, Candia V: A new tool for real-time pain assess-ment in experimental and clinical environments. PLoSOne 7:e51014, 2012
66. Schweinhardt P, Seminowicz DA, Jaeger E, Duncan GH,Bushnell MC: The anatomy of the mesolimbic reward sys-tem: A link between personality and the placebo analgesicresponse. J Neurosci 29:4882-4887, 2009
67. Scott DJ, Stohler CS, Egnatuk CM, Wang H, Koeppe RA,Zubieta JK: Individual differences in reward respondingexplain placebo-induced expectations and effects. Neuron55:325-336, 2007
68. Scott DJ, Stohler CS, Egnatuk CM, Wang H, Koeppe RA,Zubieta JK: Placebo and nocebo effects are defined by oppo-site opioid and dopaminergic responses. Arch Gen Psychia-try 65:220-231, 2008
69. Simmons K, Ortiz R, Kossowsky J, Krummenacher P,Grillon C, Pine D, Colloca L: Pain and placebo in pediatrics:A comprehensive review of laboratory and clinical findings.Pain, 2014. http://dx.doi.org/10.1016/j.pain.2014.08.036.[Epub ahead of print]
70. Spielberger CD: STAIC. PreliminaryManual for the State-Trait Anxiety Inventory for Children. Palo Alto, CA, Consul-ting Psychologists Press, 1973
71. Stein N, Sprenger C, Scholz J, Wiech K, Bingel U: Whitematter integrity of the descending pain modulatory systemis associated with interindividual differences in placeboanalgesia. Pain 153:2210-2217, 2012
72. Stewart-Williams S, Podd J: The placebo effect: Dissolv-ing the expectancy versus conditioning debate. PsycholBull 130:324-340, 2004

Krummenacher et al The Journal of Pain 1293
73. Symonds LL, Gordon NS, Bixby JC,MandeMM: Right-lat-eralized pain processing in the human cortex: An FMRIstudy. J Neurophysiol 95:3823-3830, 2006
74. Tomlinson D, von Baeyer CL, Stinson JN, Sung L: A sys-tematic review of faces scales for the self-report of pain in-tensity in children. Pediatrics 126:e1168-1198, 2010
75. Trapanotto M, Pozziani G, Perissinotto E, Barbieri S,Zacchello F, Benini F: The cold pressor test for the pediatricpopulation: Refinement of procedures, development ofnorms, and study of psychological variables. J Pediatr Psy-chol 34:749-759, 2009
76. Vase L, Riley JL 3rd, Price DD: A comparison of placeboeffects in clinical analgesic trials versus studies of placeboanalgesia. Pain 99:443-452, 2002
77. Wager TD, Atlas LY, Leotti LA, Rilling JK: Predicting indi-vidual differences in placebo analgesia: Contributions of
brain activity during anticipation and pain experience. JNeurosci 31:439-452, 2011
78. Wager TD, Rilling JK, Smith EE, Sokolik A, Casey KL,Davidson RJ, Kosslyn SM, Rose RM, Cohen JD: Placebo-induced changes in FMRI in the anticipation and experienceof pain. Science 303:1162-1167, 2004
79. Weimer K, Gulewitsch MD, Schlarb AA, Schwille-Kiuntke J, Klosterhalfen S, Enck P: Placebo effects in chil-dren: A review. Pediatr Res 74:96-102, 2013
80. Wollgarten-Hadamek I, Hohmeister J, Zohsel K,Flor H, Hermann C: Do school-aged children withburn injuries during infancy show stress-induced activa-tion of pain inhibitory mechanisms? Eur J Pain 15:423.e1-423.e10, 2011
81. Zusne L, Jones WH: Anomalistic Psychology: A Study ofMagical Thinking, 2nd ed. Hillsdale, Erlbaum, 1989
![Proposals to Extend Healthy Life Expectancy in Shizuoka ...€¦ · [Gap between life expectancy and healthy life expectancy in Shizuoka Prefecture] Healthy life expectancy *Source:](https://img.dokumen.tips/doc/110x75/5f427921a09c2479a15262fb/proposals-to-extend-healthy-life-expectancy-in-shizuoka-gap-between-life-expectancy.jpg)




























