Embed Size (px)
Citation preview

Hritlsii Journal oJ Dermatohay (1994) 1 iO. fi4S-fi49,
Evidence for genetic homogeneity of Setleis* syndromeand focal facial dermal dysplasia
K.A.WARD AND C.MOSSDepartment of Dermatohnff, Birminglmm Children's Hospital
Accepteil for publication 2(1 October 1 99i
iyd Middlewafj. Hirmingham BI6 SET. V.K,
S u m m a r y A healthy H-month-old boy hiid miilliplf. cirfitUir, sair-Iikf depressions on both temples, which hiidbeen present since birth. Deli\ery had been normal, and had not required the tise of forceps or t)therinstruments. His mother and one sister had similar, but less obvious, lesions on the temples. The threeaffected family members had similar fat i;tl features, v\ ith laterally delicient eyebrows, and a prominentupper lip with down-turned mouth. Additional features in the baby were sparse lower eyelashes,medial epicanthal folds, and skin dimpling on one side of the chin.
Focal facial dermal dysplasia (FFDD) denotes a condition in which there are bilemporal, round, scar-like lesions. It is inherited as an autosomal dominant trait with variable penetrance and expressivity,and there are no associated features. Setleis' syndrome is recessively inherited, and is characterized bysimilar bitemporal defects associated with other dysmorphic features, including deficient eyelashesand a prominent upper lip. 'I'his report of dominantly inherited bileniporal dermal defects withcharacteristic facies supports the idea ihat FFDD aud Setleis' syndrome are a single disorder.
In I S)29, Brauer described a large Dutt'h-Clermankinship in which bitemporal scar-like depressions wereinherited in an autosomal dominant pattern.' I,,atcrreports noted an association with linear depressions inthe lower central portion of the forehead, vertical cleftingof the chin, and round, hairless depressions locatedlaterally on the chin, ' ' Histological exaniination (t( atypical lesion on the temple revealed a thinned epidermisand an atrophic dermis, w ith virtual absence of connec-tive and adipose tissue, and adnexal structures.- ' Occa-sional bundles of striated muscle were present in theupper dermis.*
The Setleis' bitemporal forceps marks' syndrome'denotes clinically and histologically identical bitemporalscar-like depressions, associated with characteristic dys-morphic facial features, apparently inherited as anautosomal recessive trait (Table 1).'' '̂
In this report, we describe a family who show facialfeatures of the Setleis' syndrome, but with an autosomaldominant inheritance pattern. We propose that Setleis'syndrome and FFDD are a single entity.
Case reports
Case 1
This boy was the third child of unrelated Caucasianparents. He was the product of an uncomplicatedpregnancy, and was delivered vaginally without the aid
of forceps or other instrumentation. His birth weight was1864 g. At hirth he was noted to have multiple, sharplydemarcated, roinid. pink depressions on both templesUarying in size from 2 to 12 mm in diameter!. Inaddition to the bitemporal "forceps marks', he had medialepicatithal folds, arched, laterally deficient eyebrows, adimple on the left side oi' the chin, absent lowereyelashes, but noniial upper eyelashes, and a prominent
Tiibk" I. I'ticiiil itnomalic's dcsirlbed in Setleis' svndronie
I-'acial anomalyPresent
case
Ritemporiil defectsAbnortiiiilities of eyelashesi'X'ebriiws whicb slant upwards and [atenillyAged, leonine itppfuranceVenical cleftiny olibe ehiii'Rubbery' noso and cbin un palpationI'lattened iiasul bridpePeriorbit.ll piiffinessProminent vermillion border ol' upper lipNasal si'ptum extends below alat* nasaeKpieantliusSkin ditiiples located laterally on tbe ebinRecurrent conjunctivitisLinear depressions on the ToreheddAbiiortnulities ultbo earn,'\bnorrnulities iiflbe bair
645

646 K.A.WARD AND C.MOSS
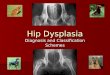
Figure 1. Case 1. aged 3 months, showing bitempt)ral defect.s. laterallydeficient eyebrows, absent lower eyelashes, medial t'picanthal foldsand prominent upper lip with Jnwri-turned mcmtli.
Figure 2. Case 1. aged 14 months, showing unchanged bitemporaldefects, lalcrally deticienl eyebrows and prominenl iippt-r lip withdown-turned mouth. Lower eyelashes are
Kigurt- J. Prolileofcase l.iiged 14 months, showing prominent upperlip.
Upper lip with down-turned mouth (Fig. 1). By the age of14 months, sparse lower eyelashes had appeared, but hislat'ial appearance was otherwise unchanged (Figs 2 andi). His general health and development, and the rest ofthe physical examination, were normal, except forrecurrent conjtinctivitis.
Case 2
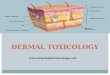
This 35-year-old woman, the mother of cases 1 and 5.had flesh-coloured, oval, bitemporai depressions, whichwere tirst noted at birth, and were attributed to theapplication of forceps during delivery. The eyebrowswere thin, arched and delicient laterally. Additionalfeatures included bilateral dimples on the chin, and adown-turned moutb. The eyelashes were normal(Fig. 4a and b).
disc i
Ihis 6-year-old girl is the older sister of case 1. At birth, awell-demarcated circtilar pink depression was noted onthe left temple, and attributed to the use of forceps duringdelivery. In addition to the unilateral temporal lesion.

SETLEIS' SYNDROME AND FFDD 647
Figurv 4. |a | Case 2. showing insigniticanl tle.sh-coloured bitcmporiil defects, best sect) on the right (b).
she had thin, arched eyebrows, a down-turned mouth,and sparse lower eyelashes, but normal upper eyelashes.No skin dimpling was noted {Fig. S|. Her general healthand development were normal, except for recurrentconjunctivitis.
Unaffi'cU'dfamihi nicntbers
The father and the 4-year-old sister of case 1 appearednormal, and showed none of the abnormalities noted inthe other family members. The maternjil grandparentswere unavailahlc for examination, hut temporal lesionswere said to have been absent. There was no history ofconsanguinity in the family.
Discussion
Bitemporal scars with abnormal eyelashes (Setleis' syn-drome. McKusick no. 227260) and local facial dermaldysplasia (FFDD. Brauer's syndrome. McKusick no.1 36506) are regarded as two distinct genetic dis-orders.'''" In this report, we have described a family withthe facial features of Setleis" syndrome (Table I I. butwith the dominant inheritance pattern of FFDD. suggest-ing genetic homogeneity of these twt) syndromes on
several grounds. Review of the pertinent literaturesupports our proposition.
Firstly, both syndromes are characterized by identicalscar-like depressions on the temples.-"'^ In FFDD, thetemporal lesions miiy vary in size from small, insignifi-cant defects to iesions greater ihan I ctn in size. Ingeneral, the temporal lesions of FFDD are bilaterallylocated, but unilateral defects have been reported.' ' InSetieis' syndrome, the temporal lesions arc consistentlybilateral, often extenditig from the scalp to the supraorbi-tal ridge."* ** These observations suggest a single diseaseentity characterized by a spectrum of facial anomalies,ranging from minor temporal lesions to large, bilateraltemporal defects associated with other dysmorphic facialfeatures.
Secondly, the facial features said to be characteristic ofSetleis' syndrome have previously been observed inFFDD. The typical leonine facies described by Setleis ctai, results from a combination of frontal bossing,redundant facial skin, periorbital puffiness, and flattenednasal bridge with a bulbous nasal tip.^ Comparison withthe facial appearance of an adult with I'I'DD' revealsremarkable similarities to the Setleis' sytulrome.^''' " Inaddition to similar temporal defects, the followingfeatures have been described in both syndromes: eye-

648 K.A.WARD AND C.MOSS
jraaj
Figure 5. Case i. aged 6 years, showing a small defect on the lefttemple. lA)wer eyelashes are sparse, and the upper lip is prtjminenl.
brows which are deficient laterally, in the region ofthetemporal defect.'"" linear depressions on the lowercentral portion ofthe forehead.'*^ vertical clefting ofthechin.'"*'' and dimpling of the skin on the sides of thechin.''*'*" The concurrence of multiple, similar facialanomalies in FFDD and in Setleis' syndrome supports acommon aetiology for these two disorders."
Thirdly, the reported differences in inheritancebetween Setleis' syndrome and FFDD may be apparentrather than real, because the temporal lesions maybecome less noticeable with age in FFDD. and in adultsmay be missed without careful examination.' In somereported instances the FFDD trait skipped several genera-tions, only to reappear.'*' Magid et ai. recently describeda male infant with typical bitemporul defects and nodysmorphic features, but with normal parents." Thesereports support the proposition that FFDD is transmittedas an autosomal dominant trait, but with highly variablepenetrance and expressivity. The absence of any
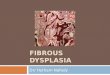
Figure 6. Di;iceph;ili(; border malfoniiations. The distribution ofthepotential embryologJL'al lesions of facial skin, mucosa aiid musculatureis shown by the shaded area.
abnormality in the parents of children with Setleis'syndrome"*"" has been interpreted as consistent withautosomal recessive inheritance, but does not excludedominant inheritance with variable penetrance. DiIjernia ct al., reported bitemporal defects, absence oflower eyelashes, thick, down-turned upper lip. low-sethairline, and rubbery chin in a mother and her maleinfant.'- Furthermore, in the original report by Setleis eta!.. Mrs ().. the mother of two affected siblings, althoughnot showing any defects of the temporal areas, clearlyhad narrowed palpebral fissures and a nasal septumwhich extended below the alae nasae. both of which areconsidered to be features ofthe Setleis' syndrome (Hg. 5in their article).'' This observation supports a dominantpattern of inheritance for the Setleis' syndrome as well asfor FFDD.
The underlying pathogenesis of the facial abnormali-ties is unknown. Matsumoto (*( al. proposed an embryo-logical disorder in both the frontonasal process and thefirst branchial arch, and found similarities to mandibulo-facial dysostosis.** However, all the common anomaliesseen in FFDD and in Setleis' syndrome can be attributedto partial failure of mesodennal penetration into the

SETLHIS" SYNDROME AND FFDD 549
diacephalic border, resulting in multiple, but embryolo-gically associated. lesions of the faciul skin, mucosu andmusculature (Fig. f)|.' ' The less frequently ()bser\Tdfacial anomalies in FFDD and in Setleis' syndrome(vertical median chin ridge, laterally located chin dim-pling, and abnt)rm<il ears) can be attributed to failure ofmesodermal penetration into the rhombencephalicregion."
The phenotypic similarities of Setleis' syndrome withFFDD. together with a plausible common embryt)logit aldefect, suggest a single entity inherited in a dominiintpattern, but with highly variable penetrance and ex-pression. We propose that the term focal facial dermaldysplasia should be used to describe both these condi-tions.
References
1 Brauer A. HcR'ditarcr symmctrisc'hiT syslcmatisiiTter Naevusaplasticus bei iH IVniont-n. Dermainl Wodmmhr 1929:89: 1 I fi J-S.
2 Jensen N\i. Congenital ectodcmial dysplasia of llie I'iici.', /{/ /Iknmtoi I971:84:41<)-lf>.
J ,ML'( A'mh AH. Roctt WB. I'amilial focal facial dermai dysplasia. ArchOermatol 197J: 107: 591-5.
4 St'tlcls H. Kramer B. Valcarcel M et ul. Congenital eclodermaidysplasia or thf face. l\-dUitriiS I96 i : U: S4()-H,
5 Kiulnlpli RI. Sihwiirlz W. l-t-ydcn )]. Bilemporal aplasia cutisnmm'iiila, Ardi ikrimU't 1974: i 10: (.i S- IS,
(l ,Miiri(»n KVV. Chilayiil 1), Hulciieon Rti cl «/, Aulosomiil reci'ssiveu'u in Sclk-is bitcniporal 'forceps marks' syndrome. Am }
i987: 141: 895 7.7 Clark Ri). fioiabi M. Lacassie Y el at. Expanded phenotype and
ethnicity in Sclleis syndrome. Am / Med Cerwl \ 9S9: 14: iS4-7.8 MiiiMimoUi S. Kimo 1. iiiinui.-iuki Y i'( ill. Seiieis bilomporal 'forceps
inariis' syndrome ami its pathogenesis: a case report. Actii Pai'tliiUrtl>n 1941: SJ: i8fi-9n,
4 liiirtdii Jl., Kook A, Cierii'tirs in lieriiiHlolotiy, In: Tiwlhtitik ofDiTmatohfiji (Rook A, Wilkinson US. Kbling ['JC. Champion RH.Kurton ]l., eds). 4th edn. Oxford: Biackweil Scientiiic Publications,
HI MiKusick VA. Meniielian inheritance in man. in: Catalogs ofAiitos^iwuil Dtiminant, Auwstmud Recessivf ami S-Unki'd Phenotiityrs,
iltlh eilii. IJiiltinuiru: Tiie Johns Hopkins University i'ress, 1 99 i;400, i JdJ,
i i Magid Mi,. Prendiville JS. iisteriy NB. Foeal faciai dermai dysplwsia:bilemporal iesions rescnibiing apiasia cutis congenita. / Am AcadIkrnunol i988: 18: i2()J-7.
i i i>i iemia V. Neri i. i*atrizi A. Focai facial dermal dysplasia: twofamilial cases, / Aw Acitd Ikrtiuiton'i^il: 2S: JH9-91.
i ! Pft'iler li, Crtiniol'ai'iiil iiimniiilies—thf iicy lo a surgical flassillca-Ilim of human malforinatiims. In: Cranioftuuil ,-\bnormalmcs andi'lijts (1/ thf Up, Alwoliis and I'alatc, iPfcifer Ci, ed). New York:Thieme Medicai Publishers, i 99 i: 27-40.