Embed Size (px)
Citation preview

Evidence based
population health
screening

Objectives
Describe the National Screening Committee criteria.
Describe epidemiological study designs.
Describe length time bias and repeatability in relation to
cancer screening.
Interpret sensitivity, specificity, positive predictive value,
negative predictive value and number needed to treat.
The NSC Screening Criteria (2003)
The condition
The test
The treatment
The screening programme

The condition
1. The condition should be an important health problem 2. The epidemiology and natural history of the condition, including development from latent to declared disease, should be adequately understood and there should be a detectable risk factor, disease marker, latent period or early symptomatic stage. 3. All the cost-effective primary prevention interventions should have been implemented as far as practicable. 4. If the carriers of a mutation are identified as a result of screening the natural history of people with this status should be understood, including the psychological implications.

The test
5. There should be a simple, safe, precise and validated screening test.
6. The distribution of test values in the target population should be known and a suitable cut-off level defined and agreed. 7. The test should be acceptable to the population. 8. Agreed policy on the further diagnostic investigation of individuals with a +ve test result.
9. Select mutations.

The treatment
10. Availability of effective treatment or intervention for patients identified through early detection, with evidence of early treatment leading to better outcomes than late treatment. 11. Evidence based policies covering which individuals should be offered treatment and the appropriate treatment to be offered. 12. Clinical management of the condition and patient outcomes should be optimised in all health care providers prior to participation in a screening programme.

The Screening Programme
13. There should be evidence from high
quality RCTs that the screening programme is
effective in reducing mortality or morbidity.
14. Programme is acceptable.
15. Benefit should outweigh harm.
16. Should be cost-effective.

17. All other options for managing the condition should have been considered.
18. There should be a plan for managing and monitoring the screening programme and an agreed set of quality assurance standards. 19. Adequate staffing and facilities for testing, diagnosis, treatment and programme management are available.
20. Evidence-based information
21. Public pressure for widening the eligibility criteria for reducing the screening interval, and for increasing the sensitivity of the testing process, should be anticipated.
22. If screening is for a mutation the programme should be acceptable to people identified as carriers and to other family members.

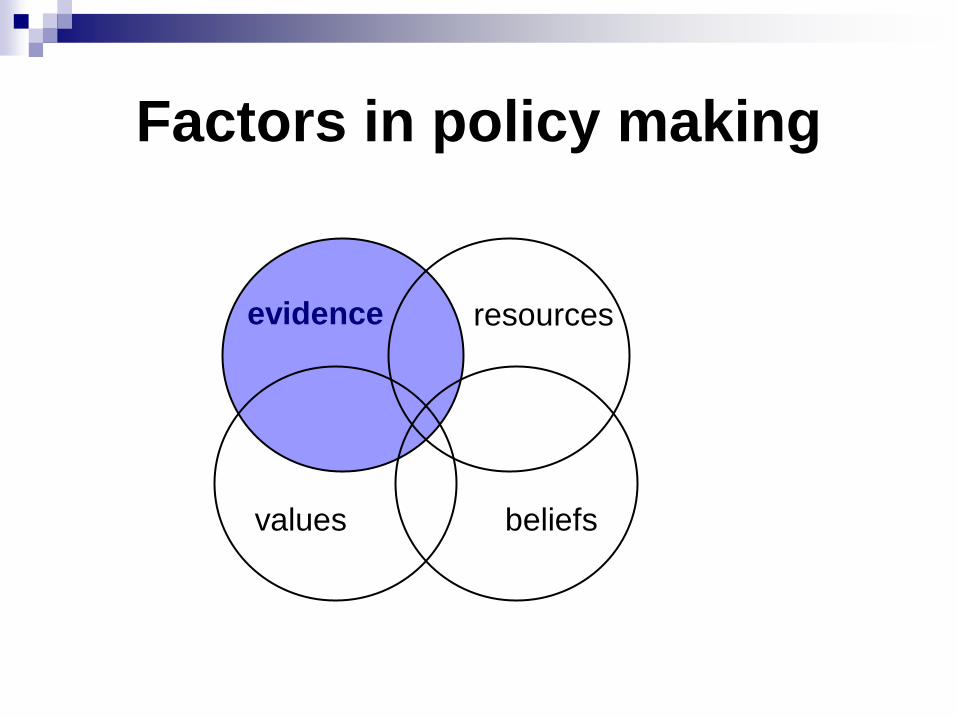
Factors in policy making
evidence resources
values beliefs
Factors in policy making
evidence resources
values beliefs

Assessing the evidence
Evaluation/study methods
Sources of Bias
Performance of the test

Study methods
Randomised
controlled
trials (RCTs)
Cohort
studies
Case-control
studies

Randomised controlled trials
Reference population
Target (study) population
Excluded
Refused
Study participants
Random
allocation
Screening No Screening
Outcome
Loss to follow up Loss to follow up

Cohort studies
Cancer
Screened Not Screened
Cancer No Cancer No Cancer
Prospective

Case-control studies
Cancer No Cancer
Screened Not Screened Screened Not Screened
Retrospective

Bias
Length time
effect
Lead time
effect
Selection
bias
Over
diagnosis
bias

Selection bias
The healthy screenee - Self-selection
process.
Those who attend screening may differ in
their underlying risk of disease/mortality
compared to those who don’t.
Characteristics of attendees? – Week 2

Over diagnosis bias
Cancers detected that would not have had
any clinically morbidity associated with
them and would not be fatal.

A randomized controlled trial is designed to examine bowel screening. The intervention group gets FOBt tests on an annual basis, the control group has no intervention.
Screening Assessment

After five years
There are more incident bowel cancers
identified in the screened group compared to
the control group.
The cancers in the screened group are of an
earlier stage than those in the control group.
Five year survival is higher for the people
with cancer in the screened group.
Can we conclude that this screening
program is effective?

Lead time bias
Mortality versus survival statistics Gates TJ. America Family Physician, 2001

Length time bias
Screening is more likely to detect cases of slowly progressing disease
Screening is less likely to pick up aggressive disease due to its rapid progression
Screen detected cases will automatically have a better prognosis , even if screening makes no difference, than those presenting with symptoms.

Length time bias
Gates TJ. America Family Physician, 2001

Test performance
Sensitivity
Specificity
Positive predictive values
Negative predictive values

Condition being tested for
Present Absent Totals
Test
result
Positive A
true positives
B
false positives
A+B
Negative C
false negatives
D
true negatives
C+D
Totals A+C B+D A+B+C+D

Condition being tested for
Present Absent Totals
Test
result
Positive A b a+b
Negative c D c+d
Totals A+C B+D a+b+c+d
Sensitivity = A / (A + C)
The ability of the test to detect the condition
when it is actually present
Specificity = D / (B+D)
The ability of the test to detect that the
condition is not present, when in fact it is absent

Condition being tested for
Present Absent Totals
Test
result
Positive A b A+B
Negative c D C+D
Totals a+c b+d a+b+c+d
Positive predictive value = A / (A + B)
The probability that an individual has the condition,
given that the result is positive
Negative predictive value = D / (C+D)
The probability that an individual does not have
the condition, given than the result is negative

Number needed to Treat/Screen
Number of people who would have to be
screened to prevent one death.
1/Absolute risk reduction.
Number needed to be screened.
Accounts for participation and selection
effects.

Presenting the evidence
Ease of understanding
Framing effects
Balanced presentation
Asking the right questions
Asking programme questions, not single issue questions

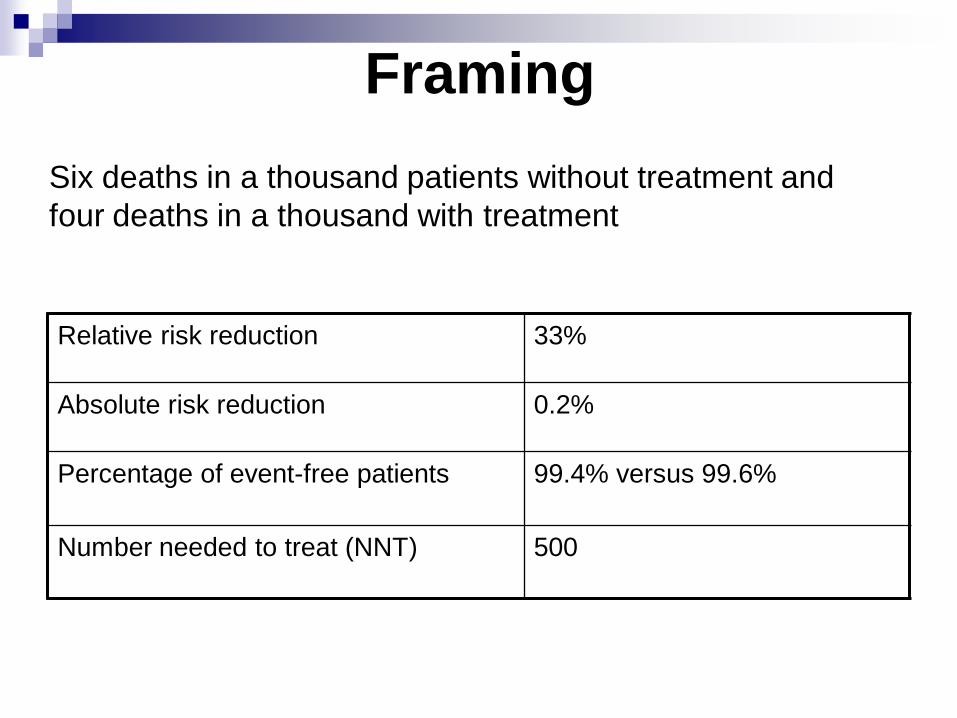
Framing
Relative risk reduction 33%
Absolute risk reduction 0.2%
Percentage of event-free patients 99.4% versus 99.6%
Number needed to treat (NNT) 500
Six deaths in a thousand patients without treatment and
four deaths in a thousand with treatment

Nottingham randomised trial of bowel cancer screening
(Hardcastle et al. 1996)
Mortality reduction = 15%,
(95% confidence limits 2-26%)
‘bowel screening could cut deaths by as much as 30%’
Getting the balance right

Asking the right questions
Years between
tests
% reduction in
cancer incidence
% of women with
false positive
smear tests in
their lifetime
10 64.1 15
5 83.6 30
3 90.8 50
2 92.5 75
1 93.5 100

Single issue question: Would bowel screening do more benefit than harm to
the population?
Programme question: Would bowel screening be more beneficial to the
population than any current healthcare activity that
could be stopped to release the necessary funding?
If we had an extra £3m to spend per year, would
bowel screening be the most beneficial thing we could
do with this investment?
Programme vs single issues








![Rectum Ovarian Cancer - collegeoncologie.be€¢ There is no place for CA 125 screening in the general population (evidence level C) [3,4]. • Screening can be considered for high](https://img.dokumen.tips/doc/110x75/5d21869a88c993722e8b9dc9/rectum-ovarian-cancer-there-is-no-place-for-ca-125-screening-in-the-general.jpg)




















