Embed Size (px)
Citation preview

31 5
Evaluation of Chromosome Aneuploidy in Tissue Sections of Preinvasive Breast Carcinomas Using lnterphase Cytogenetics
Daniel W. Visscher, M.D.
Tracie L. Wallis, B.S. John D. Crissman, M.D.
Department of Pathology, Harper and Detroit Receiving Hospitals, Wayne State University School of Medicine, Detroit, Michigan.
Presenteld at the 1995 United States and Cana- dian Academy of Pathology annual meeting, To- ronto, Ontario, Canada, March l l to 17, 1995.
Address for reprints: Daniel W. Visscher, M.D., Department of Pathology, Harper Hospital, 3990 John R, Detroit, MI 48201.
Received May 26, 1995; revision received Sep- tember 22,1995; accepted September 22,1995.
BACKGROUND. Little is known about cellular level genetic alterations in preinvasive breast lesions, particularly lobular carcinoma in situ. METHODS. We employed fluorescence in situ hybridization (FISH) using pericen- tromeric (alpha satellite) probes to assess numerical alterations of chromosomes 1, 7, 8, 16, 17, and X in deparaffinized archival tissue sections of 9 lobular carcino- mas in situ (LCIS), 10 ductal carcinomas in situ (DCIS), and a spectrum of prolifera- tive lesions (including 3 ductal hyperplasias, 1 adenosis, 1 radial scar, and 2 atypical hyperplasias). Three of the LCIS lesions and five of the DCIS lesions were from patients who had a concurrent invasive neoplasm as a component of the tumor. RESULTS. None of the proliferative lesions exhibited detectable chromosome gains, and only 1 showed evidence of signal loss consistent with monosomy (chromosome 7 in the adenosis lesion). Six LCIS patients (67%) displayed evidence of monosomy, with involvement of chromosome 17 in 6 of 6 patients, chromosome 8 in 2 of 6 patients, and chromosome 7 in 2 of 6 patients. Two LCIS patients, each of whom had a concurrent invasive neoplasm, exhibited signal gains consistent with trisorny
for chromosomes 1 and 8 (1 patient each). Chromosome aneuploidies were ob- served in 7 of 10 (70%) DCIS patients, including 2 of 5 patiellts (40%) without concurrent invasive neoplasm and 5 of 5 patients (100%) with concurrent invasive neoplasm. The pattern of numerical chromosome alteration in DCIS included two patients with losses only, 2 patients with gains only, and 3 patients with both gains and losses (i.e., involving different chromosomes). Chromosome 17 aneuploidy was observed in all DCIS and all LCIS patients who exhibited abnormalities; how- ever, DCIS patients showed more frequent aneuploidies for chromosomes X and 16 (0 LCIS patients vs. 4 DCIS patients with each). CONCLUSIONS. Distinctive pathologic subsets of preinvasive breast neoplasia have divergent patterns of genetic instability. Foci of residual in situ neoplasia that accompany invasive disease may have a greater degree of genetic instability than neoplasms that lack progression to invasive phenotype. Cancer 1996; 77:315-20. 0 1996 American Cancer Society.
KEYWORDS: genetic instability, interphase cytogenetics, ductal carcinoma in situ, lobular carcinoma in situ.
enetic instability, which results in the accumulation of structural ge- G netic aberrations, is an important pathogenetic mechanism in malig- nant epithelial neoplasia. Such genetic alterations may be reflected at the cellular level by abnormal karyotype or by nuclear DNA content. Ultimately, genetic instability is believed to facilitate tumor progression by acting at the molecular level through alteration of gene expression. Although genetic instability is initiated before the onset of host invasion'-" and possibly before morphologic evidence of in situ mal ignan~y,~ ,~ little
0 1996 American Cancer Society

316 CANCER January 15 1996 / Volume 77 / Number 2
is known about the genetic pathology of early breast neo- plasia. A variety of factors have complicated genetic anal- ysis of early breast neoplasia, including the heterogeneity and lengthy natural history of breast carcinoma as well as the difficulty of isolating cells and DNA from microscopic precursor lesions, which may be admixed intimately with normal or invasive neoplastic cells.
One manifestation of genetic instability is chromo- some aneuploidy, which is the gain or loss of whole chro- mosomes in all or part of the tumor population. Using interphase cytogenetics, chromosome aneuploidy may be detected in archival tissue sections, thus permitting mor- phologically directed analysis of uncommon or micro- scopic lesions.6~’ The purpose of this study was to com- pare patterns of chromosome aneuploidy in different his- tologic types of precursor breast lesions, including lobular carcinoma in situ (LCIS) and representative variants of ductal carcinoma in situ (DCIS). Our hypothesis is that morphologic and clinical differences between precursor lesions may be reflected in divergent patterns or degrees of chromosome aneuploidy.
MATERIALS AND METHODS Case Selection The cases we studied were obtained from the Surgical Pathology Department files of Harper and Detroit Receiv- ing Hospitals, Detroit, Michigan. They included 10 pa- tients with DCIS, 9 patients with lobular LCIS, and 8 pa- tients with benign lesions. Three of the patients with LCIS had coexisting invasive lobular carcinoma, and 2 other patients had coexisting DCIS. Five of the DCIS patients had coexisting invasive ductal carcinoma, and 2 of the remaining 5 patients represented DCIS foci present in the LCIS patients. By cytologic features, the DCIS patients included 6 high grade lesions, 2 intermediate grade le- sions, 1 low grade lesion, and 1 heterogeneous tumor with an equal mixture of intermediate and high grade cytology. For comparison, 8 benign lesions were studied, including 3 moderate-florid ductal hyperplasias (DH), 1 radial scar, and 1 atypical ductal hyperplasia (ADH). Also, an area of atypical lobular hyperplasia (ALH) from the low grade DCIS patients was studied. Finally, we studied an area of adenosis and a benign terminal duct lobular unit, each from a different LCIS patient.
Hybridization Procedures A series of consecutive 4-pm sections were cut from the formalin-fixed, paraffin-embedded tissue blocks that contained the lesions of interest and were mounted on silanized slides. The last section was stained with hema- toxylin and eosin and was examined to confirm the pres- ence of residual lesion, which was then outlined. Details of our hybridization methods are reported e1sewhere.O Briefly, deparaffinized sections were treated with a prote-
ase (protease K, 20 minutes at 43°C) to expose target DNA. Reagents for pre- and posthybridization treatments in so- dium chloride sodium citrate buffer (Rapid wash) as well as the alpha-satellite probes were purchased from Oncor (Gaithersburg, MD). The probes used (to chromosomes 1, 7, 8, 16, 17, and X) were selected on the basis of fre- quency of numerical alterations for these chromosomes in karyotypes of breast carcinoma.y,’” Probes were conju- gated either to biotin or to digoxigenin, thus allowing simultaneous incubation of two probes with enumeration of two signals per slide after posthybridization incuba- tions with avidin-fluorescein isothiocyanate (FITC; green fluorescence) and antidigoxigenin rhodamine (red fluo- rescence). Individual nuclei were identified with the use of a fluorescence microscope (Zeiss Axioskop) after coun- terstaining with DAPI (blue fluorescence; Sigma).
Signal Enumeration and Interpretation In total, 200-300 nuclei were counted from each lesion. With a representative subset of slides, counts were per- formed twice to monitor intraobserver variability. All counts were made by one individual (T.W.) and were lim- ited to lesional cell nuclei that were intact and resolvable from neighbor cells. For each probe, the counts were ex- pressed as the percentage of nuclei with two signals, the
the percentage of nuclei with less than two signals. There are a number of factors that impact upon the
detection of chromosome aneuploidy using these meth- ods. These include hybridization inefficiency (either in- herent to individual probe affinity or to variability in tis- sue-DNA preparation), nuclear slicing due to tissue sec- tioning, and counting error (resulting from selection bias or misinterpretation of falsely overlapped signals). Thus, establishing reproducible criteria for the interpretation of signal counts is difficult but essential. Our laboratory has addressed this problem empirically by comparing signal counts for the employed probes in paired touch prepara- tions and corresponding tissue sections of benign lymph nodes as well as representative samples of normal, hyper- plastic, and malignant breast tissues.’ This approach has allowed analyses of degree of signal losses resulting from nuclear slicing vs. individual probe hybridization ineffi- ciency (i.e., by comparing whole nuclei to tissue section). It has also permitted the evaluation and optimization of hybridization or signal-detection artifacts that are intrin- sic to breast tissues (or cells), per se. Our studies have shown that “false trisomy” (i.e., apparent signal gain in diploid cells) is rare and is observed in <5% of “normal” cells. “False monosomy,” or apparent signal loss in intact “normal” cells, occurs in 5-15% of the population. Nu- clear truncation due to tissue sectioning, moreover, re- sults in signal losses involving 15-25% of cells. Based on these observations, we have determined that signal gain
percentage of nuclei with greater than two signals, and

Chromosome Aneuploidy in LCIS and DClSNisscher et al. 317
TABLE 1 Signal Loss Frequency in Benign Breast Tissues
Chromosome (% nuclei with loss)
Tissue I 7 8 16 17 X
Dli 19 24 28 35 31 31 DH 25 17 28 20 22 18 DH 26 19 23 33 14 21 Radial scar 19 29 34 18 29 16 AI)H 18 21 27 22 28 23 A1.H" 19 21 22 19 26 15
-
Aclenosisb 33 43 36 30 40 18 Narmal" NA 20 34 12 32 19
Dtl: ductal hperplasia; A D H atypical ductal hyperplasia; ALH: atypical lobular hyperplasia
"From LCIS cases (n = 2). From low grade IICIS case: 3% triploid nuclei with probe 8.
TABLE 3 Signal Counts in Cases of Ductal Carcinoma In Situ without Invasive Neoplasm
Chromosome (% with loss/% with gain)
Case/grade I 7 8 16 17 X
1 /Lou 1610 4010 3010 1210 3610 3210 21Moderate 2510 2910 2510 1710 3513 3110 31Higha 2510 2710 2313 1310 3910 2017 41Higha 4159 1413; 24145 5188 36122 17114 51High 1510 2610 38110 23115 37113 22118
'Coexisting lobular carcinoma in situ.
ke. , more than two spots) in more than 10% of counted nuclei constitutes reasonable evidence of trisomy (i.e., involving at least a subset of lesional cells). Conversely, signal loss (i.e., fewer than two spots) in more than 40% of counted nuclei was employed as the threshold for mo- tilosomy. We believe that these are conservative thresh- ojds, that they are comparable to the thresholds em- plloyed by others, and that they likely underestimate the true incidence of chromosome aneuploidy in breast le- sions."" 'I
RESULTS Tihe observed frequency of signal gains and losses are detailed by individual probe in Tables 1-4. None of the benign lesions exhibited evidence of trisomy, although the example of ALH, which was obtained from a DCIS patient, showed 3% triploid nuclei for chromosome 8 (Ta- ble 1). Only 1 benign lesion, an area of adenosis from an LCIS patient, displayed evidence of monosomy. This area showed 43% signal loss for the chromosome 17 probe.
TABLE 2 Signal Counts in Lobular Carcinoma In Situ Patients
Chromosome (% with loss/% with gain) Case no. I 7 8 16 17 X
I" 7145 3618 4512 3610 4812 25/4 z3 1810 3410 14126 2110 5210 1910 3h 2310 3511 3613 15.10 3310 2010 4b 2110 3010 3010 2010 4110 2410 5 2010 3210 3010 1210 4110 2210 6 2710 4310 5210 2410 4810 2810 7 2610 2410 3510 2310 3910 2310 8 2110 1610 3910 4010 3610 2310
2410 4310 3910 2910 4710 1910
a Coexisting invasive lobular carcinoma. Coexisting ductal carcinoma in situ.
TABLE 4 Signal Counts in Ductal Carcinoma In Situ Cases with Invasive Neoplasm
Chromosome (% with loss/% with gain)
Caselgrade 1 7 8 16 17 X
61Moderate 1810 2310 4010 2010 4710 2810 71Moderate t high NA 32126 2510 15111 6712 3110 81High 1317 23129 35121 910 6912 4617 91High 2510 22/23 29133 12121 4310 4319 lO1Hiah 1910 3510 4910 2510 4510 3810
The remaining benign lesions all demonstrated signal losses varying from 15% to 35%, in keeping with nuclear slicing artifact and expected degrees of hybridization inef- ficiency.
Signal counts for the LCIS patients are listed in Table 2. In 3 of the tumors (Cases 3, 7, and 8), no chromosome aneuploidies were identified. Each of the 6 tumors with abnormalities exhibited signal losses that involved one to three chromosomes (Fig. 1). Signal loss for the chromo- some 17 probe was observed in all of the abnormal pa- tients, signal loss for chromosome 8 was observed in 2 patients, and signal loss for the 7 probe was evident in 2 patients. There were no apparent losses involving chro- mosomes 1, 16, or X. Note that the signal losses involved 41 -52% of nuclei, consistent with monosomy involving only a subset of the neoplastic population. It should also be noted that borderline signal losses (>35% of nuclei) were present for Case 7 (chromosome 17) and Case 8 (chromosomes 8, 16, and 17). Two of the LCIS areas, both from patients with coexisting invasive neoplasm, exhib- ited signal gains meeting criteria for trisomy. Case 1 dem- onstrated 45% trisomic nuclei for chromosome 1, and Case 2 showed 26% trisomic nuclei for chromosome 8.

318 CANCER January 15 1996 / Volume 77 / Number 2
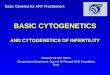
FIGURE 1. Example of dual hybridization for chromosomes 17 (red signal) and 8 (green signal) in a lobular carcinoma in situ (LCIS) patient. Signal loss, which is observed in many nuclei, may reflect hybridization inefficiency, nuclear slicing, or monosomy.
Signal counts for the DCIS patients are shown in Ta- bles 3 and 4. Three of the five tumors (Cases 1-3) without coexisting invasive neoplasm were free of any aneuploi- dies. Two of these three patients exhibited low or moder- ate grade cytologic features. Also, 2 of the 3 patients dem- onstrated borderline chromosome aneuploidies (Case 1, 40% loss for chromosome 7; Case 3,39% chromosome 17 loss and 7% trisomy for chromosome X). All of the DCIS lesions from patients with invasive neoplasia exhibited aneuploidies for at least one chromosome.
Among the 7 DCIS patients with detected chromo- some aneuploidy, 2 patients (Cases 4 and 5) exhibited signal gains only, 3 patients (Cases 7-9) exhibited both signal losses and gains, and 2 patients (Cases 6 and 10) exhibited signal losses only (Fig. 2). The pattern of indi- vidual chromosome involvement differed between LCIS and DCIS patients. Chromosome 17 was abnormal (2 pa- tients with gain, 5 patients with loss) in all of the DCIS lesions with chromosome aneuploidy, similar to the LCIS lesions. However, the DCIS patients showed more fre- quent aneuploidy for chromosome X (4 patients vs. 0 LCIS patients), 16 (4 patients vs. 0 LCIS patients), and 7 (4 patients vs. 2 LCIS patients). It should also be noted from Tables 3 and 4 that the degree of signal gain varied con- siderably, both between patients and probes, from 88% (Case 4, chromosome 16) to 11% (Case 6, chromo- some 16).
DISCUSSION Our results suggest that DCIS and LCIS are characterized by distinctive, but partially overlapping, patterns of ge- netic instability, at least as assessed by evaluation of chro- mosome aneuploidy. First, LCIS was characterized pri-
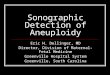
FIGURE 2. Example of a ductal carcinoma in situ (DCIS) patient demon- strating hybridization similar to that shown in Figure 1. Signal gain is consistent with trisomy for chromosome 8, but not for chromosome 17.
marily by apparent chromosome losses, with gains oc- curring less frequently. DCIS, in contrast, exhibited chromosome gains in the majority of abnormal patients. These patterns of chromosome aneuploidy are in keeping with the “low grade” cytologic pathology that character- izes LCIS (vs. DCIS) lesions. It is noteworthy that both subsets of preinvasive neoplasia exhibited a significant degree of heterogeneity with respect to the pattern of chromosome aneuploidy. This reflects the considerable morphologic, clinical, and likely biologic spectrum of le- sions that comprise either LCIS or (especially) DCIS.
The observed patterns of chromosome aneuploidy correlate with known aspects of cellular level genetic pa- thology in ductal vs. lobular breast carcinoma subsets. Lobular carcinomas are overwhelmingly flow cytophoto- metrically diploid range. Cytogenetic analyses of peridi- ploid breast tumors, however, typically reveal at least some whole chromosomal losses.’* These are either too few in number to be cytophotometrically resolved, or they are balanced by chromosome gains. If they are represen- tative of the entire genome, then the observed patterns of chromosome aneuploidy in our LCIS patients would produce a diploid-range cellular DNA content. Karyo- types of breast carcinomas, it should be noted, are typi- cally characterized by many chromosomal losses that are either whole or segmental, which, in most cases, outnum- ber chromosome gains9 Some have suggested that ge- netic losses represent the earliest manifestation of genetic instability in breast neoplasia and, thereby, that they pre- cede or antedate chromosomal gains.I5
The pattern of chromosome gain observed in most ductal lesions, conversely, very likely would produce a net cellular DNA content gain and would become manifest as cytophotometrically detectable increased DNA content. This correlates with the observed presence of DNA aneu-

Chromosome Aneuploidy in LCIS and DClSNisscher et al. 319
ploidy (i.e., hyperdiploidy) in many, if not most, ductal carcinomas. Our data, moreover, show that chromosome gains may be partial (that is, present in a minority of i.umor cells) or complete (i.e., present in a majority of the neoplastic populations). This phenomenon is also ob- served in karyotypes of breast lesions, which typically ireveal both intratumoral variation in modal chromosome inumber, reflecting “partial” gains due to variability asso- iciated with genomic destabilization as well as clonal du- lplication of all or part of the genome (i.e., so-called tetra- ~ploidization).~~”’.’~
Chromosome losses may also involve a subset of tu- imor cells; however, the loss of specificity imposed by nuclear truncation makes this distinction particularly dif- ficult using our methodology. Given the limited degree o f signal losses (relative to “normal”) that were observed iin our study, it may be debated properly whether the criteria employed for partial monosomy were too liberal ;and, thus, failed to fully exclude all slicing, hybridization, ;and signal enumeration artifacts as the cause(s1 for signal loss. However, it should be noted that monosomy was llimited primarily to chromosome 17, thus correlating ,with previous cytogenetic studies. It should also be noted that the mean frequency of signal loss for the chromo- :some 17 probe in LCIS lesions (42%) was roughly twice ,as great as the signal loss frequencies for chromosomes 1 (20%), 16 (24%), or X (23%) despite similar signal loss frequencies between the employed probes in control tis- sues. Although we contend that these data reflect actual (cytogenetic differences, we would also admit that detailed .karyotype analyses or more advanced interphase cytoge- netic proceduresL6 would be required to prove unequivo- ically the existence of partial monosomy in these patients.
DCIS and LCIS patients also differed with respect to .the distribution of chromosome gains or losses. We are not certain whether the apparently selective aneusomies ‘of chromosomes 16, X, and possibly 7 in DCIS reflect a histogenetic difference or merely reflect a manifestation of more widespread, or possibly of more advanced, ge- netic instability. Thus, it could be postulated that the ob- served pattern of chromosome aneuploidy in DCIS re- flects a greater degree of genomic destabilization inherent to a more aggressive form of neoplasia. This hypothesis is favored by the greater degrees of chromosome aneu- ploidy in both LCIS and DCIS lesions that were associated with invasive carcinoma, because progression is associ- ated with cytogenetic “evolution” or “instability.” Obvi- ously, evaluation of additional (in situ and invasive) pa- tients will be required to resolve this dilemma fully.
Apart from artifacts associated with hybridization and tissue sectioning, there are other factors in our study design that may have limited or obscured the assessment of genetic instability. First, numerical chromosome alter- ations in breast carcinomas are extremely heterogeneous
and are by no means limited to the panel that was tested. Second, it is also possible that there is intratumoral heter- ogeneity in type or degree of genetic instability. Our signal counts were obtained from a selected representative area of tumor, and we made no particular attempt to identify foci that may have exhibited more widespread or more numerous aneusomies. Third, chromosome aneu- ploidy is only one manifestation of genetic instability in epithelial neoplasia. Nonnumerical chromosomal re- arrangements as well as segmental alterations also occur, and they likely occur with greater frequency than chro- mosome aneuploidy.” These aberrations or aneuploidies of chromosomes that were not investigated were almost certainly present in patients found to be “normal” in this study (possibly including the benign proliferative le- sions). The precise nature of the relation between molec- ular and cellular level genetic alterations remains incom- pletely defined, and it must be investigated in detail be- fore data such as ours can be understood fully in the context of neoplastic progression.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
9.
Killeen JL, Namiki H. DNA analysis of ductal carcinoma in situ of the breast. A comparison with histologic features. Cancer 1991; 68:2602-7. Nielsen KV, Andersen IA, Blichert-Toft M. Chromosome changes of in situ carcinomas in the female breast. Eur 1 Swg Oncol 1987; 13225-9. Nielsen KV, Blichert-Toft M, Andersen J. Chromosome anal- ysis of in situ breast cancer. Acta OIicol 1989;28:919-22. Crissman JD, Visscher DW, Kubus 1. Image cytophotonietric DNA analysis of atypical hyperplasias and intrdductd carcino- mas of the breast. Ar-ch Pathol h b Med 1990;114:1249-53. Fisher ER, Paulson ID. Karyotypic abnormalities in precur- sor lesions of human cancer of the breast. A m 1 Cliiz hf/ iol
Kim SY, Lee JS, Ro JY, Gay ML, Hong WK, Hittelman WN. Interphase cytogenetics in paraffin sections of lung tumors by nonisotopic in situ hybridization. A m J Pathol 1993;
Dhingra K, Sahin A, Supak J, Kim SY, Hortobagyi G, Hittel- man WN. Chromosome in situ hybridization on formalin- fixed mammary tissue using non-isotopic, non-fluorescent probes: technical considerations and biological iniplica- tions. Br 1 Cancer Res Treat 1992;23:201-10. Visscher DW, Wallis TW, Ritchie CA. Detection of chrorno- some aneuploidy in breast lesions with fluorescence in situ hybridization: comparison of whole nuclei to thin tissue sec- tions and correlation with flow cytometric DNA analysis. Cytometry 1995; 2 1:95- 100. Geleick D, Muller H, Matter A, Torhorst J, Regenass U. Cyto- genetics of breast cancer. Cancer Genet Cj’togerier 1990; 46:217-29.
1978; 691284-8.
142307- 17.
10. Dutillaux B, Gerbault-Seureau M. Zafrani B. Characteriza- tion of chromosomal anomalies in human breast cancer. Cancer Genet Cytogeriet 1990;49:203- 17.
11. Kiechle-Schwarz M, Decker HJH, Berger CS, Fiebig HH, Sandberg AA. Detection of monosomy in interphase nuclei and identification of marker chromosomes using biotinyl- ated alpha-satellite DNA probes. Cancer G e w t Cytogerzef 1991; 51:23-33.

320 CANCER January 15 1996 I Volume 77 / Number 2
12. Devilee P. Thierry RF, Kievits T, Kolluri R, Hopman AHN, Prieur M. Breast cancer genetic evolution. I. Data from cyto- Willard HF, et al. Detection of chromosome aneuploidy in genetics and DNA content. Breast Cancer Res Treat interphase nuclei from human primary breast tumors using 1991; 19245-55. chromosome-specific repetitive DNA probes. Cancer Res PE, Nederlof PM, G~~~ JW. Thick- 1988;48:5825-30. sections fluorescence in situ hybridization on formalin-
13. Poddighe PJ, Ramaekers FCS, Hopman AHN. Interphase cy- fixed, paraffin-embedded archival tissue provides a histoge- netic profile. Am J Patlzol 1994; 144:237-43. togenetics of turnours. 1 Pathol 1992; 166215-24,
14. llodgers CS, Hill SM, Hulten MA. Cytogenetic analysis in 17. Matsumura K, Kallioniemi A, Kallioniemi 0, Chen L, Smith human breast carcinoma. I. Nine cases in the diploid range HS. Deletion of chromosome 17p loci in breast cancer cells investigated using direct preparations. Cancer Genet Cyro- detected by fluorescence in situ hybridization. Cmcer Res genet 1984; 13:95- 119. 1992; 52:3474-7. 15. Dutrillaux B, Gerbault-Seureau M , Remvikos Y, Zafrani B,
16. Thompson CT,