Embed Size (px)
DESCRIPTION
Ethics and Professionalism: The Integrity of Medicine Medical Industry and Medical Practice. Richard L. Elliott, MD, PhD, FAPA Professor and Director Medical Ethics and Professionalism Mercer University School of Medicine Adjunct Professor Mercer University School of Law. - PowerPoint PPT Presentation
Citation preview

Ethics and Professionalism:The Integrity of Medicine
Medical Industry and Medical Practice
Richard L. Elliott, MD, PhD, FAPAProfessor and Director
Medical Ethics and ProfessionalismMercer University School of Medicine
Adjunct ProfessorMercer University School of Law
Questions about cases?
Threats to the Integrity of Medicine (continued)
The integrity of medical research– Last week - Protection of research subjects
• Tuskegee, IRBs– Today – Medicine and the medical industry
Tomorrow – Threats to medicine from within– Abuse of trainees, physician impairment
Wednesday – Medical malpractice
Relationships with the Pharmaceutical Industry
How good is the evidence in Evidence-Based Medicine?– What is publication bias?
What is the influence of medical industry on medical education?
What is the influence of industry on prescribing practices
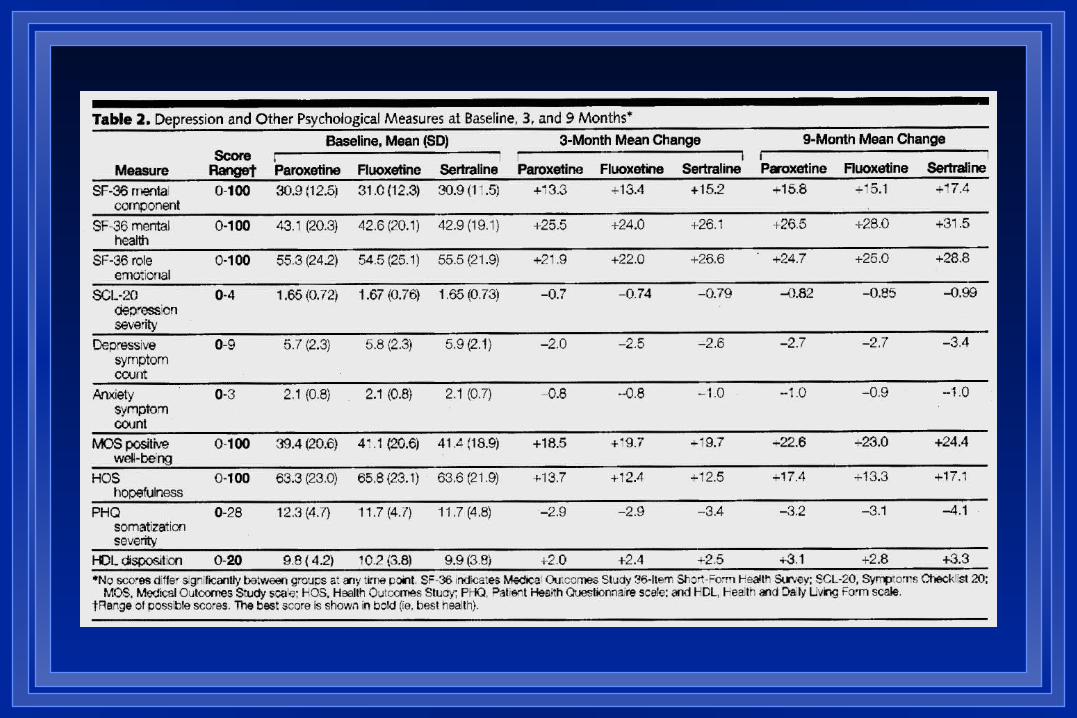
JAMA 2001;286(23):2947-55
Similar Effectiveness of Paroxetine, Fluoxetine, and Sertraline in Primary Care
K Kroenke et al. JAMA 2001;286:2947-2955 ARTIST: A Randomized Trial Investigating
SSRI Treatment 573 depressed adult patients 37 clinics 1999 Open label, randomized study Sponsored by Eli Lilly
ARTIST - Comparative Outcomes per Eli Lilly
No statistically significant differences in clinical outcomes
No differences among anxious-depressed patients
No differences among older patients No differences in patient satisfaction
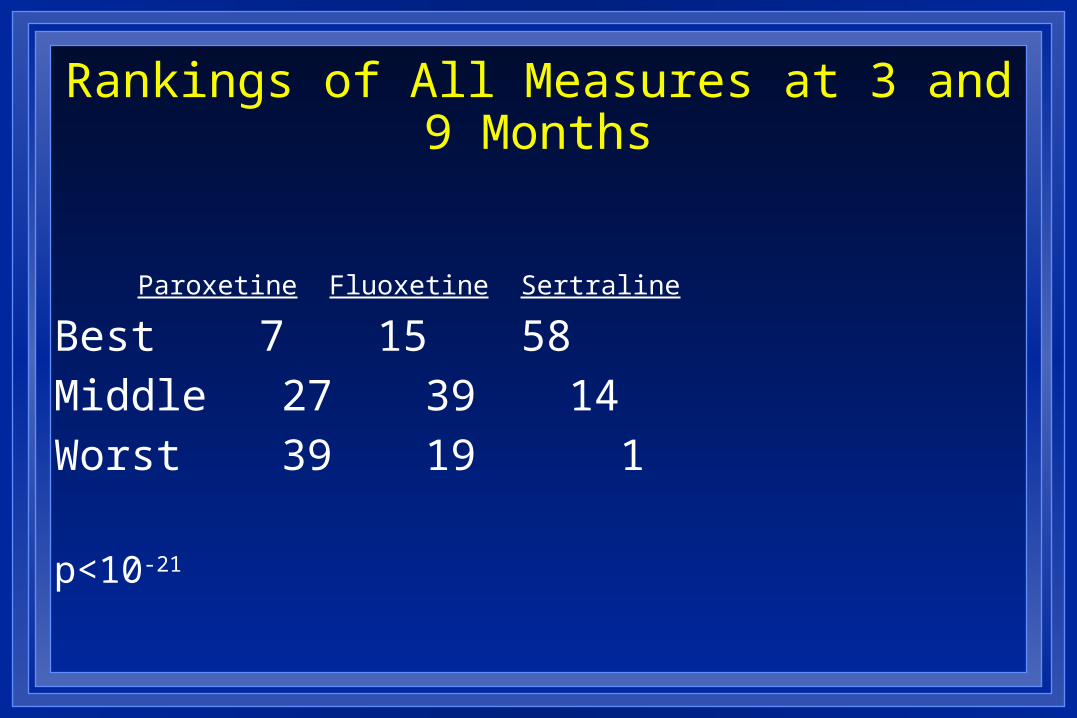
Rankings of All Measures at 3 and 9 Months
Paroxetine Fluoxetine Sertraline
Best 7 15 58
Middle 27 39 14
Worst 39 19 1
p<10-21
ARTIST
Rare example of reporting a positive study as negative
What influence did Eli Lilly have on editorial decisions?– Choice of reviewers?– Referral to JAMA statistician?
Why did JAMA publish this?– Reprints?
(A Few) Big Pharma Scandals Vioxx death data submitted to FDA concluded
no significant risk Intent-to-treat deaths in RCTs for Alzheimer’s
– Subjects 34/1069– Placebo 12/1078 – Hazard ratio 2.99
Vagal nerve stimulation and editorials– Editor wrote favorable opinion piece, did
nor disclose financial interests
Rosiglitazone (Avandia)
Peak sales $2.5 billion 2006 2007 meta-analysis of 42 triels
– OR MI 1.43 (95% CI, 1.03 - 1.98; P = 0.03)– OR death from all CV causes 1.64 (95% CI, 0.98 to 2.74; P
= 0.06) Recent meta-analysis confirmed risk Senate concluded GSK knew of risks, withheld data from FDA FDA voted not to withdraw – one member of panel later found to
have been paid by GSK Meta-analysis (BMJ 2010) that commented on two meta-
analyses found authors who had conflict more likely to give favorable opinion of risks (RR 3.5-6.5 depending on analysis)
Publication Bias
Perlis et al. Am J Psychiatry 2005;162:1957-60 162 randomized, double-blind, placebo-controlled
clinical trials between 2001-2003 AGP, AJP, J Clin Psych, J Clin Psychopharmacology 60% received funding from industry 47% authors reported potential conflict of interest Those with potential conflict of interest were 4.9 times
less likely to report negative results (6/75 vs. 26/87) Comparable results in non-psychiatric literature
Effectiveness of Antidepressants 74 FDA-registered trials of 12 antidepressants approved
between 1987-2004 74 trials, 38 positive (statistically significant benefits for drug
over placebo)– 37/38 published
Of 36 FDA-deemed negative trials:– 22 never published– 11 published in manner to appear positive– Only 3 negative trials published
Turner et al. NEJM 2008;358:252-60 Thus, the published evidence for the efficacy of
SSRIs is vastly different from the results of all trials:– 48/51 trials positive vs. 38/74
Efficacy of Cardiovascular Drugs
Results published in NEJM, JAMA, Lancet– 2000-2005
If study funded by for-profit, 67.2 % favored newer treatment
If study funded by non-profit, 49% favored newer treatment (51% did not)
Ridker PM, Torres J: JAMA 2006; 295. 2270-2274
JAMA. 2003;290:921-928 370 randomized drug trials from Cochrane data base Experimental drug recommended as treatment of
choice in 16% of trials funded by nonprofit organizations, 51% of trials funded
by for-profit organizations (P.001; 2 test). Adjusted analyses showed that trials funded by for-
profit organizations were significantly more likely to recommend the experimental drug as treatment of choice (odds ratio, 5.3; 95% confidence interval, 2.0-14.4) compared with trials funded by nonprofit organizations. This association did not appear to reflect treatment effect or adverse events.
Publication of Clinical Trials 451 study protocols submitted to one
research committee 375 publications resulted from 233
protocols (publication rate 52% - 233/451 protocols)
Odds ratios for publication:– Non-commercial funding 2.4– Commercial funding 0.7
Von Elm et al. Swiss Med Weekly
Reducing Publication Bias Authors must have submitted trial to
clinicaltrials.gov– Negative results available
Authors must report potential conflicts of interest– But funding sources can be buried in a
long list of honoraria, speakers bureaus, etc.
Mandatory reporting of payments from medical industries
How effective are author disclosure policies?
JAMA. 2011 Mar 9;305(10):1008-17– Reviewed 29 most recent meta-analyses in highest impaqct
medical journals involving RCTs of pharmacological treatments. 2/29 MAs reported on potential conflicts among RCT authors. Conclusion: Journals might require CoI disclosure, but MAs relying on RCTs do not use this info
Otolaryngol Head Neck Surg 2009 Sep;141(3):311-5– 25% of publications reviewed had disclosure discrepancies
between disclosures at annual meeting presentation and subsequent publication
J Vasc Surg. 2011 Sep;54(3 Suppl):55S-8S– Inconsistent disclosures in 27% of disclosures
Peer Review
Peer review – supposed to ensure submission has scientific validity and ethical integrity
“Peer review” is a term used loosely by some.– The editor/symposium chair looked at it
Peer Review One criterion for quality in a publication is peer review Reviewers are selected randomly from a pool of pre-
qualified experts having no conflicts of interest – avoids preselecting outcome of review– Some studies are so specialized that few experts
exist and cannot be assigned randomly– Conflicts can be buried in a list of funding sources
Blinded review: Authors are removed from reviewers copies– Not hard to identify some authors based on
references, previous work
Ghost Writing and Guest Authors
Ghost writer – person not identified who was involved in significant data or writing process
11-13% of articles – Flanagan et al. JAMA 1998;280:222– Ross JAMA 2008;299:1800
“Hundreds of articles” The Observer Dec 7, 2003
Guest author – inclusion of author who had minimal or no involvement in data or writing– Often honorarium– 16% research articles, 26% review articles, 21% editorials
ARTIST study? Nemeroff, Text published by APA, written by drug company
affiliate
Influence of Industry on Scientific Conclusions
Effects of passive smoking – harmful? 106 reviews 39/106 (37%) of reviews concluded no harm
– 29/39 (74%) of these reviews had tobacco affiliations 67/106 (63%) of reviews concluded passive smoke harmful
– 2/67 (3%) had tobacco affiliations Similar results in other biomedical research – affiliation with
industry is best predictor of pro-industry finding (odds ratio 3.60) Artist study? Barnes et al. JAMA 1998;279:1556 Bekelman et al. JAMA 2003;289:454

Evaluating bias in a publication or presentation
Lo JAMA 2013;310(10): 1019-1020 Options for managing a condition,
including generics and lifestyle changes; risks/benefits compared?
Limitations for studies of new drugs?
Accuracy of Advertising 69 journal advertisements 50.2% claims provided no source to support When sources cited, 65% claims supported Efficacy claims supported 53.2% Can you believe claims in medical journal
ads?– Flip a coin
Spielman et al. J Nerv Ment Dis 2008;196:267
Physicians and the Pharmaceutical Industry
Relationship(s) often mutually beneficial Gifts Educational funding Research support Information Samples
Gifts from the Pharmaceutical Industry
Industry spends approximately $10,000/physician/year
97% residents carry at least one item with industry logo
Six gifts/year 14 meals/year
– Much higher at MCCG Wazana and Primeau Psych Clin N Am 2002;25:647
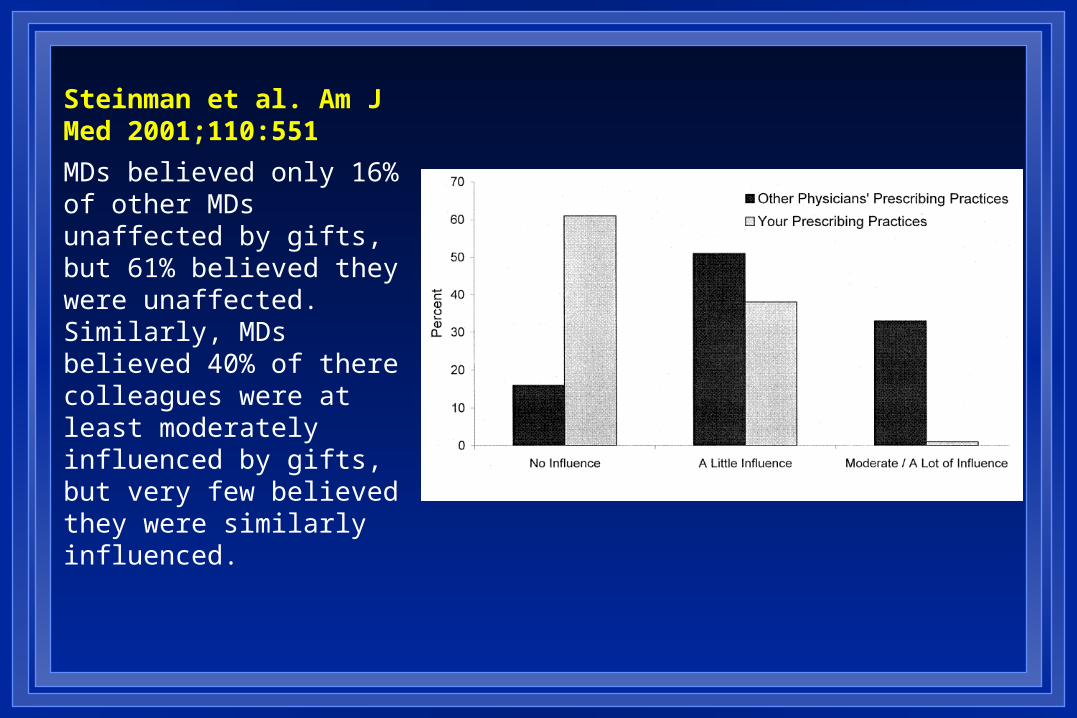
Steinman et al. Am J Med 2001;110:551
MDs believed only 16% of other MDs unaffected by gifts, but 61% believed they were unaffected. Similarly, MDs believed 40% of there colleagues were at least moderately influenced by gifts, but very few believed they were similarly influenced.
Industry CME and Prescribing Patterns
$2.45 billion spent on continuing education for health professionals in 2006– $1.4 billion paid for by industry (57%)
2011 75% CME providers received commercial funding
After event, 4-5x greater prescribing of product
Formulary Requests 40 physicians who requested a formulary addition
from January 1989 through October 1990. Control physicians were 80 randomly selected physicians who had not made requests.
Physicians were more likely to have requested that drugs manufactured by specific companies be added to the formulary if they had met with pharmaceutical representatives from those companies (OR, 13.2; 95% CI, 4.8 to 36.3) or had accepted money from those companies (OR, 19.2; 95% CI, 2.3 to 156.9)

Pharmaceutical Research and Manufacturers of America (PhRMA) Guidelines
Pre-2002– Golf, honoraria for attending presentations, trips, games
2002– Meals modest, without guests– Gifts of modest value (<$25-100) and primarily of benefit to
patient care or practice 2009
– No gifts (pens, notepads, stethoscopes, lights, etc.) which have value independent of patient education
– May have office meals

AMA and the Pharmaceutical Industry
Gifts should primarily entail a benefit to patients and should not be of substantial value
Individual gifts of minimal value are acceptable if work-related
Some are calling for rejection of all gifts, meals, speaking honoraria, GME support
Supports National Clinical Trials Registry– Trials begun after 7/05 will be considered for
publication only if publicly registered
Marcia Angell “It would be naïve to conclude that bias is
only a matter of a few isolated instances. It permeates the entire system.”
“Physicians can no longer rely on the medical literature for valid and reliable information.”
“Clinicians just do not know anymore how safe and effective prescription drugs really are, but the products are probably nowhere near as good as the published literature indicates.”– Angell M: JAMA 300. 1069-1071.2008
AMSA Scorecard Conflict of Interest Policies at Academic Medical
Centers (http://amsascorecard.org/) Gifts/Industry relationships
– Gifts, consulting, speaking, disclosure Samples, purchasing, access Education
– On/off campus, industry support, curriculum MUSM Grade “C” Not widely disseminated to faculty/trainees
You can make a difference.