Embed Size (px)
Citation preview
7/8/2009
1
ESSENTIALS OF NEPHROLOGY:ESSENTIALS OF NEPHROLOGY:
ACUTE AND CHRONIC ACUTE AND CHRONIC KIDNEY DISEASEKIDNEY DISEASE
ShievaShieva KhayamKhayam--BashiBashi, M.D., M.D.
Assoc Assoc ClinClin Prof , Dept. of Family & Community MedicineProf , Dept. of Family & Community Medicine
UCSF/ SFGH FCM Residency ProgramUCSF/ SFGH FCM Residency ProgramMedical Director, Skilled Nursing Facility/4A SFGHMedical Director, Skilled Nursing Facility/4A SFGH
Email: Email: [email protected]@fcm.ucsf.edu or or [email protected]@att.net415415--206206--35183518
7/8/2009
2
Friday, February 13, 2009Inventor of kidney dialysis machine in wartime Holland ,Dr Willem Kolff dies aged 98
(“father of dialysis”)
After 16 previous failed attempts, the first successfully treated patient was a 67-year-old woman in uremic coma who regained consciousness after 11 hours of hemodialysis with Kolff’s dialyzer in 1945. She lived 7 more years and died of other causes.
Kolff’s goal was to provide life support during recovery from acute renal failure.
After World War II ended, Kolff donated the five dialyzers he had made to hospitals around the world, so that others could learn and use hemodialysis.
Famous people with kidney Famous people with kidney diseasedisease
�� Wolfgang Amadeus Mozart Wolfgang Amadeus Mozart –– may have may have died of kidney failure ? died of kidney failure ? age 35 (1756age 35 (1756--1791)1791)(speculations are many:(speculations are many:pain, fever, headache,pain, fever, headache,rash, swelling of armsrash, swelling of arms
and legs)and legs)
�� Erma Erma BombeckBombeck, columnist , columnist -- long historylong historyof polycystic kidney disease, died from of polycystic kidney disease, died from complications of kidney transplant in complications of kidney transplant in San Francisco (1927San Francisco (1927--1996)1996)
7/8/2009
3
�� Barry White, Grammy awardBarry White, Grammy award--winning singer winning singer --chronic HTN, kidney disease/chronic HTN, kidney disease/failure,diedfailure,died of stroke of stroke and kidney failure (1944and kidney failure (1944--2003)2003)
�� Neil Simon, playwright Neil Simon, playwright ––polycystic kidney disease,polycystic kidney disease,received Kidney transplant received Kidney transplant in 2004, donated by longtime in 2004, donated by longtime friend/publicist. (1927friend/publicist. (1927-- ))
�� Mary Tyler Moore (1936Mary Tyler Moore (1936-- ) ) -- type I Diabetes type I Diabetes since age 33; diabetic retinopathy, nephropathysince age 33; diabetic retinopathy, nephropathy
Well, Mr.Osborne, Well, Mr.Osborne,
it may not be kidney stones, after all.it may not be kidney stones, after all.

7/8/2009
4
OVERVIEWOVERVIEW
Part 1: Part 1: ACUTE RENAL FAILUREACUTE RENAL FAILURE--
ACUTE KIDNEY INJURY:ACUTE KIDNEY INJURY:
�� HistoryHistory�� Physical ExamPhysical Exam�� Evaluation: Lab/StudiesEvaluation: Lab/Studies�� TreatmentTreatment
Part 2:Part 2:CHRONIC KIDNEY DISEASECHRONIC KIDNEY DISEASEScreening for CKD:Screening for CKD:–– WhomWhom do you screen?do you screen?–– WhyWhy do you screen ?do you screen ?–– HowHow do you screen ?do you screen ?
Diagnosing CKD: Diagnosing CKD:
–– How do you diagnose the How do you diagnose the causecause of CKD?of CKD?
–– How do you How do you slow the progression slow the progression of CKD? of CKD?
–– How do you How do you treat the effectstreat the effects of CKD?of CKD?
7/8/2009
5
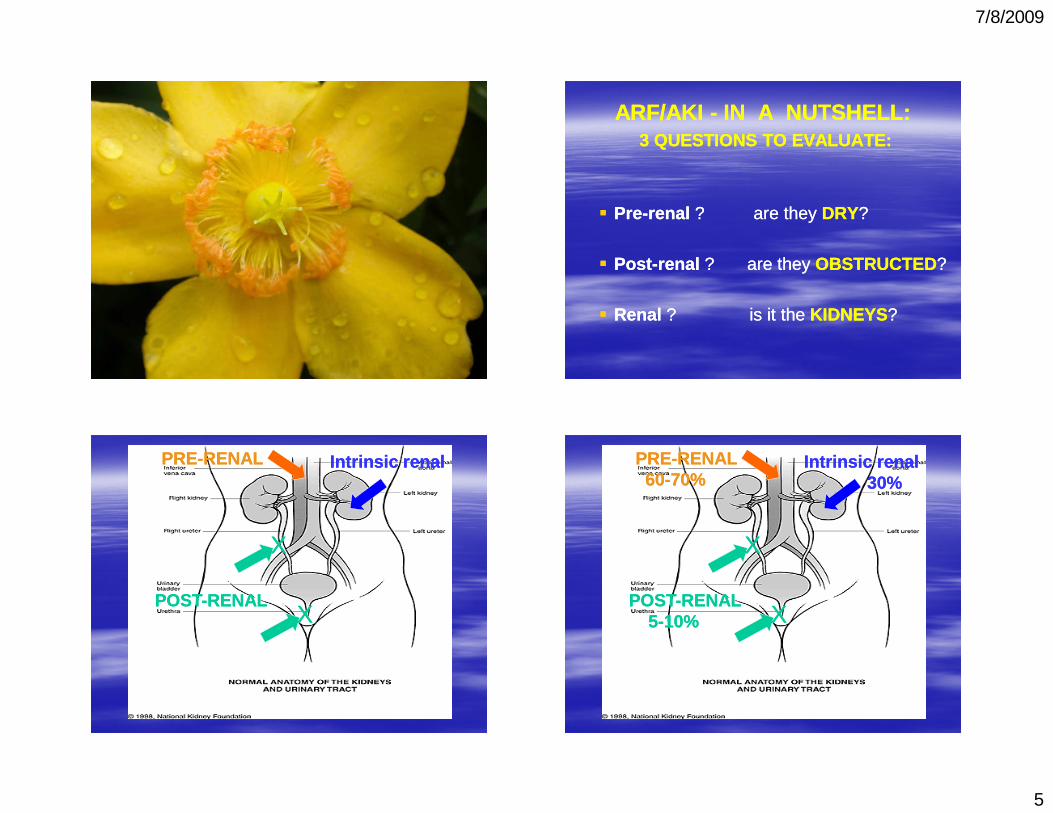
ARF/AKI ARF/AKI -- IN IN A NUTSHELL:A NUTSHELL:3 QUESTIONS TO EVALUATE:3 QUESTIONS TO EVALUATE:
�� PrePre--renalrenal ? are they ? are they DRYDRY??
�� PostPost--renal renal ?? are they are they OBSTRUCTEDOBSTRUCTED??
�� Renal Renal ? is it the ? is it the KIDNEYSKIDNEYS??
PREPRE--RENALRENAL
POSTPOST--RENALRENAL
Intrinsic renalIntrinsic renal
XX
XX
PREPRE--RENAL RENAL 6060--70%70%
POSTPOST--RENALRENAL55--10%10%
Intrinsic renalIntrinsic renal30%30%
XX
XX
7/8/2009
6
ACUTE RENAL FAILUREACUTE RENAL FAILURE
casecase-- Mr. M.Mr. M.
�� 55 55 yoyo man, man, hxhx DM, HTN, DJD:DM, HTN, DJD:
�� 3 day h/o 3 day h/o N/V/poor N/V/poor popo intake/Diarrhea intake/Diarrhea
�� 1 day 1 day hxhx oliguriaoliguria ��anuriaanuria, confusion, , confusion, pruritispruritis
7/8/2009
7
�� MedsMeds : Benazepril, Hctz, Glipizide, Ibuprofen: Benazepril, Hctz, Glipizide, Ibuprofen
�� PHYSICAL EXAMINATION: PHYSICAL EXAMINATION:
�� Vital Signs: Vital Signs: BP 95/50BP 95/50, , HR 125HR 125, , RR 28RR 28, O2: , O2: 91% RA91% RA�� Gen: Gen: confusedconfused , tired, tired�� HEENT: HEENT: mucus membranes DRYmucus membranes DRY�� Heart : Heart : tachycardictachycardic�� Lungs: Lungs: tachypneictachypneic , , diffuse ralesdiffuse rales�� Abdomen: no mass, NTAbdomen: no mass, NT�� Skin: excoriations, no rash/petechiae/purpuraSkin: excoriations, no rash/petechiae/purpura�� Prostate: normal sizeProstate: normal size
LabsLabs ::
Na= Na= 129129K=K= 6.06.0CO2=CO2= 2020BUN=BUN= 6464CreatCreat== 3.63.6 (baseline =1.2 one month ago)(baseline =1.2 one month ago)
Glucose=Glucose= 425425
7/8/2009
8
INITIAL TREATMENTINITIAL TREATMENT
�� IV STARTEDIV STARTED–– GIVEN GIVEN NS BOLUSESNS BOLUSESFOR HYPOTENSION FOR HYPOTENSION
�� FOLEY CATHETERFOLEY CATHETER INSERTED: NO INSERTED: NO URINEURINE�� not obstructed at bladder levelnot obstructed at bladder level
�� HYPERKALEMIAHYPERKALEMIA : EKG= WITHOUT : EKG= WITHOUT ACUTE CHANGES, TREATED WITH ACUTE CHANGES, TREATED WITH INSULIN/GLUCOSE,CALCIUM, INSULIN/GLUCOSE,CALCIUM, KAYEXALATEKAYEXALATE
�� HCTZ, ACEI, AND NSAIDS HELDHCTZ, ACEI, AND NSAIDS HELD
�� UA SENT FOR MICROSCOPY AND CX: UA SENT FOR MICROSCOPY AND CX: S.G.1.025S.G.1.025, , NO RBC, NO WBCNO RBC, NO WBC, , NO CELLULAR CASTSNO CELLULAR CASTS (HYALINE ONLY)(HYALINE ONLY)
�� RENAL U/SRENAL U/S NEGATIVE FOR NEGATIVE FOR HYDRONEPHROSIS (obstruction)HYDRONEPHROSIS (obstruction)
�� KUBKUB NEGATIVE FOR CALCULINEGATIVE FOR CALCULI
HOSPITAL COURSEHOSPITAL COURSE
�� OVER NEXT HOURS: BP INCREASED, OVER NEXT HOURS: BP INCREASED, UOP IMPROVED, MENTAL STATUS UOP IMPROVED, MENTAL STATUS CLEAREDCLEARED
�� BUN, CREAT DECREASEDBUN, CREAT DECREASED OVER NEXT OVER NEXT DAYS IN HOSPITAL, DAYS IN HOSPITAL, WITH IV FLUIDSWITH IV FLUIDS
�� Dx: Dx: AKIAKI ::PREPRE--RENAL AZOTEMIARENAL AZOTEMIA , , SECONDARY TO ACUTE VIRAL SECONDARY TO ACUTE VIRAL GASTROENTERITIS GASTROENTERITIS
7/8/2009
9
ACUTE RENAL FAILURE(ARF)ACUTE RENAL FAILURE(ARF)or or
ACUTE KIDNEY INJURY (AKI)ACUTE KIDNEY INJURY (AKI)�� Definition: Definition: nono universal definitionuniversal definition –– generally generally
noted by a noted by a rapid rise in Creat, BUN, rapid rise in Creat, BUN, +/+/-- decreased UOP :decreased UOP :
---- if the baseline Creat is < 2.5 mg/dl : ARF if the baseline Creat is < 2.5 mg/dl : ARF can be defined by an increase in serum can be defined by an increase in serum Creatinine of at least Creatinine of at least 0.5 mg/dl0.5 mg/dl , for 2 weeks , for 2 weeks or less or less ----Or, if the baseline Creat is > 2.5 mg/dl:Or, if the baseline Creat is > 2.5 mg/dl:ARF can be defined by an increase in serum ARF can be defined by an increase in serum Creatinine Creatinine by more than 20%.by more than 20%.
ARF / AKIARF / AKI
�� can be can be nonoliguricnonoliguric or can be or can be oliguricoliguric(oliguria=less than (oliguria=less than 400 ml urine400 ml urine output/day output/day in adults or less than ½ cc/kg/hr) in adults or less than ½ cc/kg/hr)
�� AnuriaAnuria usually has worse prognosis (except usually has worse prognosis (except in dehydration) and is defined as less than in dehydration) and is defined as less than 100 ml/day100 ml/day of urine output in adults. of urine output in adults.
�� ARF occurs in ~ 5% of hospitalized patients.ARF occurs in ~ 5% of hospitalized patients.
�� mortality rate estimates vary from 25mortality rate estimates vary from 25--90%.90%.
�� inin--hospital mortality rate is 40hospital mortality rate is 40--50% 50%
�� in intensive care settings, the mortality rate is in intensive care settings, the mortality rate is 7070--80%. 80%.
(Note: the higher mortality rates are seen in (Note: the higher mortality rates are seen in pts requiring dialysis)pts requiring dialysis)
7/8/2009
10
Mortality is due to Complications:Mortality is due to Complications:
�� pulmonary edema 30pulmonary edema 30--50%50%
�� cardiac (MI, arrhythmias) 30cardiac (MI, arrhythmias) 30--40%40%
�� GI (GI bleed, pancreatitis) 30%GI (GI bleed, pancreatitis) 30%�� Infections 50Infections 50--70%70%
�� Neurologic abnormalities 30Neurologic abnormalities 30--50%50%
�� Electrolyte disorders (hyperkalemia, Electrolyte disorders (hyperkalemia, metabolic acidosis, hyperuricemia, metabolic acidosis, hyperuricemia, hyperphosphatemia) 50hyperphosphatemia) 50--75%75%
Evaluating for Causes of AKI/ARF:Evaluating for Causes of AKI/ARF:
�� HistoryHistory
�� Physical ExamPhysical Exam
�� Lab/StudiesLab/Studies
7/8/2009
11
IN A NUTSHELL: IN A NUTSHELL:
Hx, PE, Labs are to determine :Hx, PE, Labs are to determine :
�� PrePre--renalrenal ? are they ? are they DRYDRY??
�� PostPost--renal renal ?? are they are they OBSTRUCTEDOBSTRUCTED??
�� Renal Renal ? is it the ? is it the KIDNEYSKIDNEYS??
HistoryHistory ::
�� Ask for clues to help determine CAUSE: Ask for clues to help determine CAUSE:
(dry vs. obstructed vs. kidneys?)(dry vs. obstructed vs. kidneys?)
1.1. “Are You Dry“Are You Dry?”:?”:�� Decreased PO intake? Decreased PO intake?
�� Increased fluid Losses? (N/V/D/diuretic Increased fluid Losses? (N/V/D/diuretic use)use)
�� Other reasons for volume Other reasons for volume depletion?depletion?�� anaphylaxis,sepsis,MIanaphylaxis,sepsis,MI//CHF,cirrhosisCHF,cirrhosis
7/8/2009
12
History: History:
2.2. “Is There An Obstruction?”:“Is There An Obstruction?”:
�� Abdominal pain / signs of bladder obstruction?Abdominal pain / signs of bladder obstruction?�� SuddenSudden anuriaanuria??�� HematuriaHematuria? Flank pain? Renal/bladder stones?? Flank pain? Renal/bladder stones?�� Weight loss / cancer symptoms? Weight loss / cancer symptoms? �� (also may have no urinary symptoms at all)(also may have no urinary symptoms at all)
History:History:
3.3. “Is it the Kidneys?”:“Is it the Kidneys?”:�� MEDSMEDS: : NephrotoxicNephrotoxic medicines? IV medicines? IV
contrast? contrast? aminoglycosidesaminoglycosides, , amphotericinamphotericin, , cisplatincisplatin, PCNs, , PCNs, cephalosporinscephalosporins, sulfas, , sulfas, NSAIDs, NSAIDs, rifampinrifampin??
�� Family HistoryFamily History Kidney Disease?Kidney Disease?
�� Previous urologic / Previous urologic / renal historyrenal history??
�� AutoimmuneAutoimmune/ / vasculitisvasculitis history? history?
�� ViralViral diseases which can affect kidneys?diseases which can affect kidneys?
7/8/2009
13
Also, ASK for SYMPTOMS which Also, ASK for SYMPTOMS which can be the can be the consequenceconsequence of ARF:of ARF:
�� EncephalopathyEncephalopathy ? (confusion/somnolence)? (confusion/somnolence)
�� Chest pain?Chest pain? ((pericarditispericarditis ))
�� CHF/Fluid CHF/Fluid overloadoverload symptoms?symptoms?
��Pulmonary or Peripheral Pulmonary or Peripheral EdemaEdema? ? ��Significant Significant HypertensionHypertension? ?
�� BleedingBleeding? (platelet dysfunction)? (platelet dysfunction)
PHYSICAL EXAMINATIONPHYSICAL EXAMINATION
7/8/2009
14
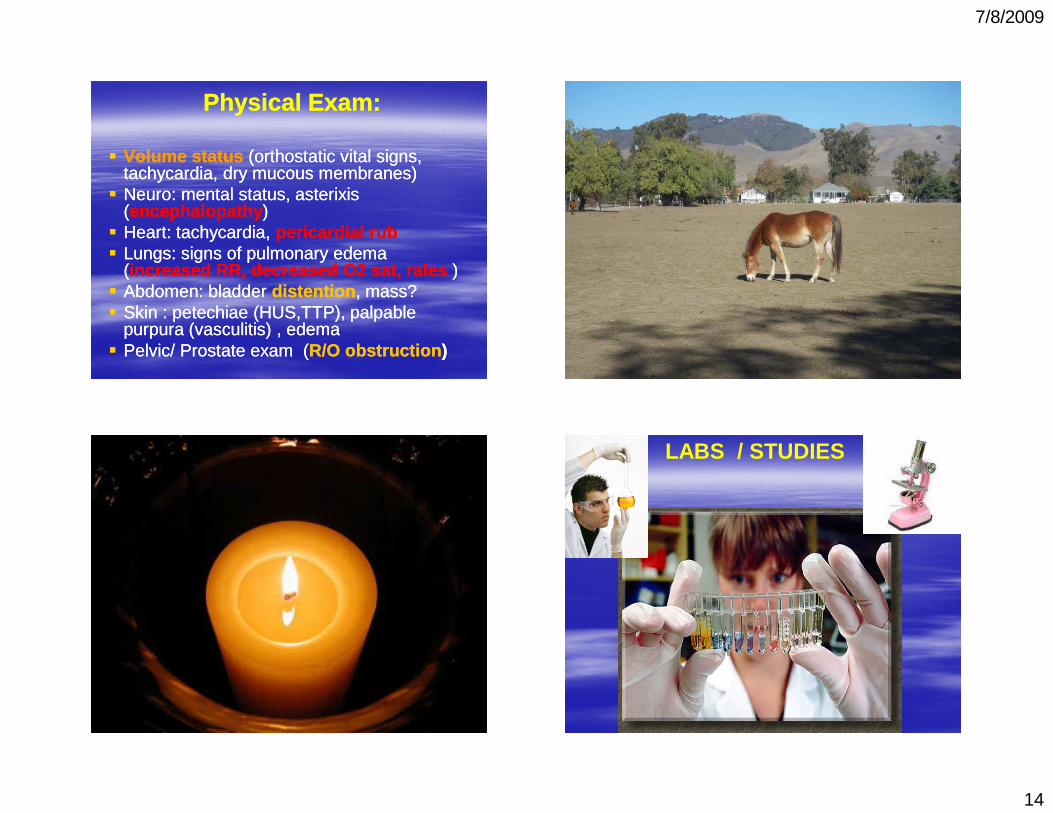
Physical Exam:Physical Exam:
�� Volume statusVolume status (orthostatic vital signs, (orthostatic vital signs, tachycardia, dry mucous membranes)tachycardia, dry mucous membranes)
�� NeuroNeuro: mental status, : mental status, asterixisasterixis((encephalopathyencephalopathy ) )
�� Heart: tachycardia, Heart: tachycardia, pericardial rubpericardial rub�� Lungs: signs of pulmonary edema Lungs: signs of pulmonary edema
((increased RR, decreased O2 sat, increased RR, decreased O2 sat, ralesrales ))�� Abdomen: bladder Abdomen: bladder distentiondistention , mass?, mass?�� Skin : Skin : petechiaepetechiae (HUS,TTP), palpable (HUS,TTP), palpable
purpurapurpura ((vasculitisvasculitis) , edema) , edema�� Pelvic/ Prostate exam (Pelvic/ Prostate exam (R/O obstructionR/O obstruction ))
LABS / STUDIES
7/8/2009
15
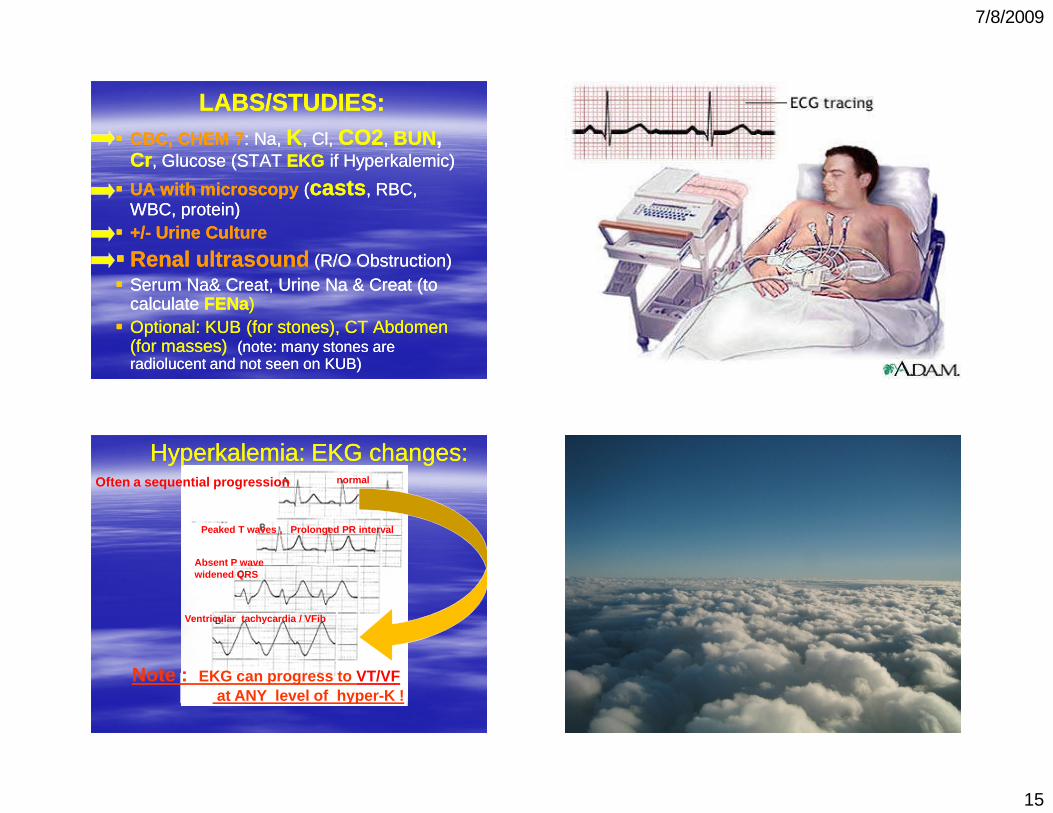
LABS/STUDIES:LABS/STUDIES:�� CBC, CHEM 7CBC, CHEM 7: Na, : Na, KK , , ClCl, , CO2CO2, , BUNBUN, ,
CrCr , Glucose (STAT , Glucose (STAT EKGEKG if if HyperkalemicHyperkalemic))
�� UA with microscopyUA with microscopy ((castscasts , RBC, , RBC, WBC, protein)WBC, protein)
�� +/+/-- Urine Urine CultureCulture
�� Renal ultrasoundRenal ultrasound (R/O Obstruction)(R/O Obstruction)�� Serum Na& Serum Na& CreatCreat, Urine Na & , Urine Na & CreatCreat (to (to
calculate calculate FENaFENa))�� OptionalOptional: KUB (for stones), CT Abdomen : KUB (for stones), CT Abdomen
(for masses)(for masses) (note: many stones are (note: many stones are radiolucent and not seen on KUB)radiolucent and not seen on KUB)
normal
Peaked T waves , Prolonged PR interval
Absent P wavewidened QRS
Ventricular tachycardia / VFib
Hyperkalemia: EKG changes:Hyperkalemia: EKG changes:
Note : EKG can progress to VT/VF at ANY level of hyper-K !
Often a sequential progression
7/8/2009
16
EvaluationEvaluation
Calculate the Calculate the FENaFENa:(:(Fractional Excretion of Sodium)Fractional Excretion of Sodium)
U Na / P NaU Na / P Na X 100X 100U Cr / P CrU Cr / P Cr
((make sure the U and P values are in the same unitsmake sure the U and P values are in the same units))
FENa < 1 % usually suggests Pre-renalFENa > 1 % usually suggests ATN (renal)
BUT interpreting BUT interpreting FENaFENacan be problematic !can be problematic !
�� FENaFENa can also be can also be lowlow with several intrinsic renal with several intrinsic renal problems such as acute GN, early ATN, problems such as acute GN, early ATN, rhabdorhabdo, , contrast nephropathy, sepsis! contrast nephropathy, sepsis!
FENaFENa is is elevatedelevated by diuretic useby diuretic use
�� Pts with CKD Pts with CKD can lose their ability to reabsorb can lose their ability to reabsorb sodium (chronically elevated sodium (chronically elevated FENaFENa) & thus ) & thus not not have a decreased have a decreased FENaFENa when prewhen pre--renal.renal.
Fractional Excretion of UreaFractional Excretion of UreaFEFE-- UreaUrea
�� If pt has recently received diuretic, If pt has recently received diuretic, can use FEcan use FE--Urea instead of FEUrea instead of FE--NaNa::
(less influenced by diuretic therapy)(less influenced by diuretic therapy)
�� FEFE--Urea= Urea= U Urea / P Urea U Urea / P Urea X 100X 100U Cr / P CrU Cr / P Cr
< 35 %< 35 % favors prefavors pre--renalrenal>35 %>35 % favors ATNfavors ATN
7/8/2009
17
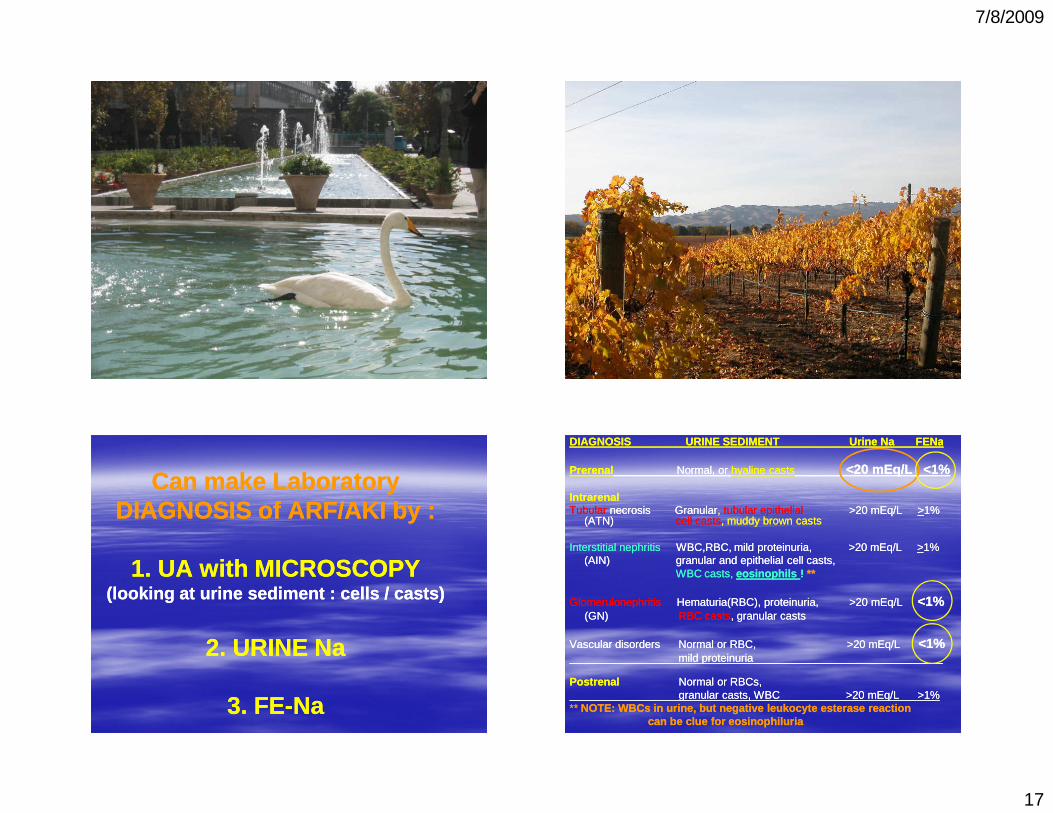
Can make Laboratory Can make Laboratory DIAGNOSIS of ARF/AKI by :DIAGNOSIS of ARF/AKI by :
1. UA with 1. UA with MICROSCOPYMICROSCOPY(looking at urine sediment : cells / casts) (looking at urine sediment : cells / casts)
2. URINE Na 2. URINE Na
3. FE3. FE--NaNa
DIAGNOSIS URINE SEDIMENT Urine Na DIAGNOSIS URINE SEDIMENT Urine Na FENaFENa
PrerenalPrerenal Normal, or Normal, or hyaline castshyaline casts <20 <20 mEqmEq/L/L <1%<1%
IntrarenalIntrarenalTubularTubular necrosis Granularnecrosis Granular, , tubulartubular epithelialepithelial >20 >20 mEqmEq/L /L >>1% 1%
(ATN) (ATN) cell castscell casts, muddy brown casts, muddy brown casts
Interstitial nephritis Interstitial nephritis WBC,RBC, mild WBC,RBC, mild proteinuriaproteinuria, >20 , >20 mEqmEq/L /L >>1% 1% (AIN)(AIN) granular and epithelial cell casts, granular and epithelial cell casts,
WBC casts, WBC casts, eosinophilseosinophils ! ! ****
GlomerulonephritisGlomerulonephritis HematuriaHematuria(RBC), (RBC), proteinuriaproteinuria, >20 , >20 mEqmEq/L /L <1%<1%(GN)(GN) RBC castsRBC casts, granular casts, granular casts
Vascular disorders Normal or RBC, >20 Vascular disorders Normal or RBC, >20 mEqmEq/L /L <1%<1%mild mild proteinuriaproteinuria_______________________________ _______________________________
PostrenalPostrenal Normal or RBCs, Normal or RBCs, granular casts, WBC >20 granular casts, WBC >20 mEqmEq/L >1%/L >1%
** ** NOTE: WBCs in urine, but negative leukocyte esteras e reaction NOTE: WBCs in urine, but negative leukocyte esteras e reaction can be clue for can be clue for eosinophiluriaeosinophiluria

7/8/2009
18
�� Hylaine casts: Hylaine casts: prepre--renalrenal
�� Granular cast + tubular epithelial cell Granular cast + tubular epithelial cell casts: casts: ATN,AIN :ATN,AIN :
�� WBC cast: WBC cast: AIN , chronic GNAIN , chronic GN ::
�� RBC casts : RBC casts : GN:GN:
�� Oval fat bodies: Oval fat bodies: nephrotic syndromenephrotic syndrome ::

7/8/2009
19
Urinalysis with Urinalysis with microscopymicroscopy ::
�� Hyaline and fine granular casts often seen in Hyaline and fine granular casts often seen in prepre--renal failurerenal failure
�� Tubular epithelial cells or castsTubular epithelial cells or casts ::ATN, ATN, AINAIN
�� WBC CASTS, Urine WBC CASTS, Urine eosinophilseosinophils ��AINAIN
�� RBC, RBC CASTS RBC, RBC CASTS proteinuriaproteinuria��suggestssuggestsGlomerulonephritisGlomerulonephritis
�� + blood on Dipstick but + blood on Dipstick but no RBCsno RBCs on microscopic on microscopic ��consider consider RhabdomyolysisRhabdomyolysis , check serum CK level, check serum CK level
7/8/2009
20
TreatmentTreatment
TREATMENTTREATMENT..
GenerallyGenerally::�� 11stst managemanage CONSEQUENCESCONSEQUENCES of of ARFARF
andand look for look for PrePre--Renal and PostRenal and Post--RenalRenal causes causes and treat accordingly and treat accordingly
THEN THEN
�� 22ndnd consider consider Intrinsic RenalIntrinsic Renal causes causes it is generally more difficult to assess for it is generally more difficult to assess for
Intrinsic Renal Causes of ARF, & not as immediateIntrinsic Renal Causes of ARF, & not as immediate
INTERVENTIONS/TREATMENTINTERVENTIONS/TREATMENT
�� Give IV Fluids as trial, since preGive IV Fluids as trial, since pre--renal is renal is most common most common cause (60cause (60--70%)70%)… … (unless (unless volume overloaded)volume overloaded)
�� Foley catheterFoley catheter –– to relieve obstruction/ urine to relieve obstruction/ urine retention. retention. (5(5--10%)10%)
�� If If Foley is already in Foley is already in placeplace��flushflush with NSwith NS(to clear any sediment/clot obstructing)(to clear any sediment/clot obstructing)
MOST LIFEMOST LIFE--THREATENING THREATENING CONSEQUENCESCONSEQUENCES::
�� hyperkalemiahyperkalemia
�� acidosisacidosis
�� fluid overload (CHFfluid overload (CHF))
�� bleedingbleeding
7/8/2009
21
REASONS FOR INITIATING REASONS FOR INITIATING EMERGENT HEMODIALYSISEMERGENT HEMODIALYSIS
�� 1 ~ 1 ~ HYPERKALEMIAHYPERKALEMIA�� 2 ~ 2 ~ CHFCHF�� 3 ~ 3 ~ METABOLIC ACIDOSISMETABOLIC ACIDOSIS�� 4 ~ 4 ~ UREMIC ENCEPHALOPATHYUREMIC ENCEPHALOPATHY�� 5 ~ 5 ~ UREMIC PERICARDITISUREMIC PERICARDITIS(BUN, (BUN, CreatCreat values are not independent values are not independent
indications for dialysis)indications for dialysis)
REASONS FOR INITIATING REASONS FOR INITIATING EMERGENT HEMODIALYSISEMERGENT HEMODIALYSIS
aka :“Aaka :“A--EE--II--OO--U”U”
�� A = ACIDOSISA = ACIDOSIS
�� E = ELECTROLYTES (high K)E = ELECTROLYTES (high K)�� I = INGESTIONSI = INGESTIONS
�� O = OVERLOADO = OVERLOAD
�� U = UREMIA U = UREMIA (uremic ENCEPHALITIS/PERICARDITIS)(uremic ENCEPHALITIS/PERICARDITIS)
7/8/2009
22
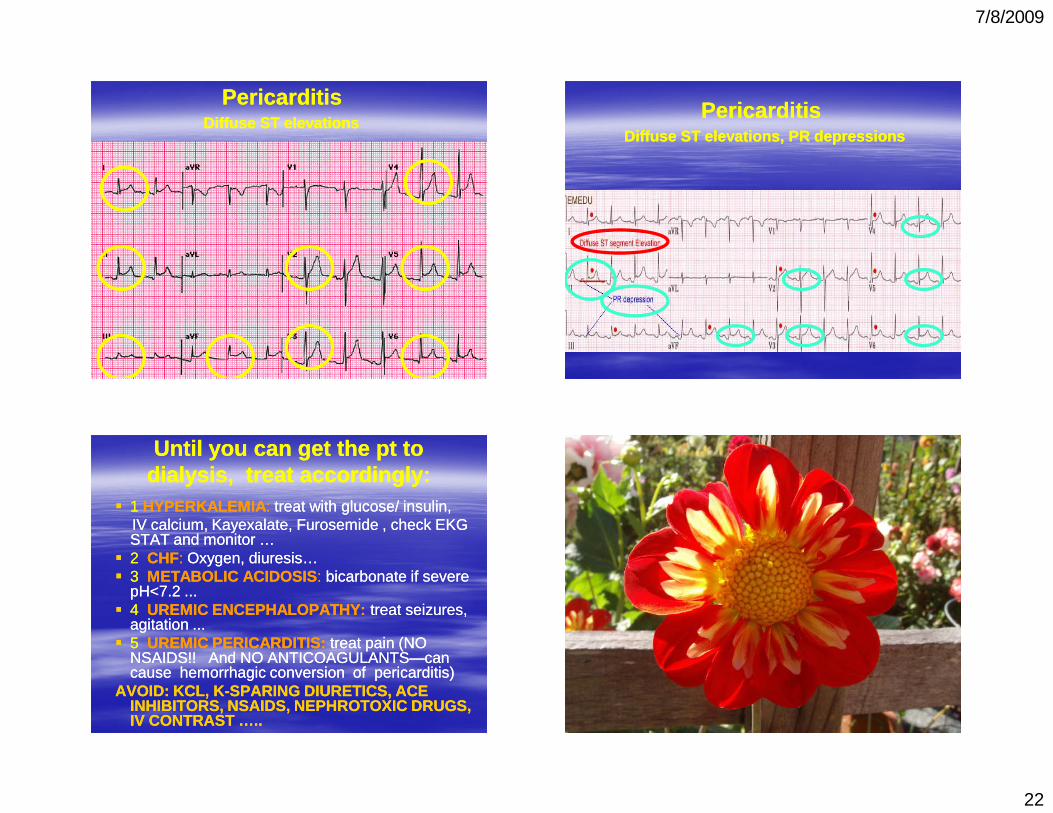
PericarditisPericarditisDiffuse ST elevationsDiffuse ST elevations
PericarditisPericarditisDiffuse ST elevations, PR depressionsDiffuse ST elevations, PR depressions
Until you can get the pt to Until you can get the pt to dialysis, treat accordingly:dialysis, treat accordingly:
�� 11 HYPERKALEMIAHYPERKALEMIA :: treat with glucose/ insulin,treat with glucose/ insulin,IV calcium, IV calcium, KayexalateKayexalate, , FurosemideFurosemide , check EKG , check EKG STAT and monitor …STAT and monitor …
�� 22 CHFCHF:: Oxygen, Oxygen, diuresisdiuresis……�� 33 METABOLIC ACIDOSISMETABOLIC ACIDOSIS :: bicarbonate if severe bicarbonate if severe
pH<7.2 ...pH<7.2 ...�� 44 UREMIC ENCEPHALOPATHY:UREMIC ENCEPHALOPATHY: treat seizures, treat seizures,
agitation ...agitation ...�� 55 UREMIC PERICARDITIS:UREMIC PERICARDITIS: treat pain (NO treat pain (NO
NSAIDSNSAIDS!! And NO ANTICOAGULANTS!! And NO ANTICOAGULANTS——can can cause hemorrhagic conversion of cause hemorrhagic conversion of pericarditispericarditis))
AVOID: KCL, KAVOID: KCL, K--SPARING DIURETICS, ACE SPARING DIURETICS, ACE INHIBITORS, NSAIDS, NEPHROTOXIC DRUGS, INHIBITORS, NSAIDS, NEPHROTOXIC DRUGS, IV CONTRAST …..IV CONTRAST …..
7/8/2009
23
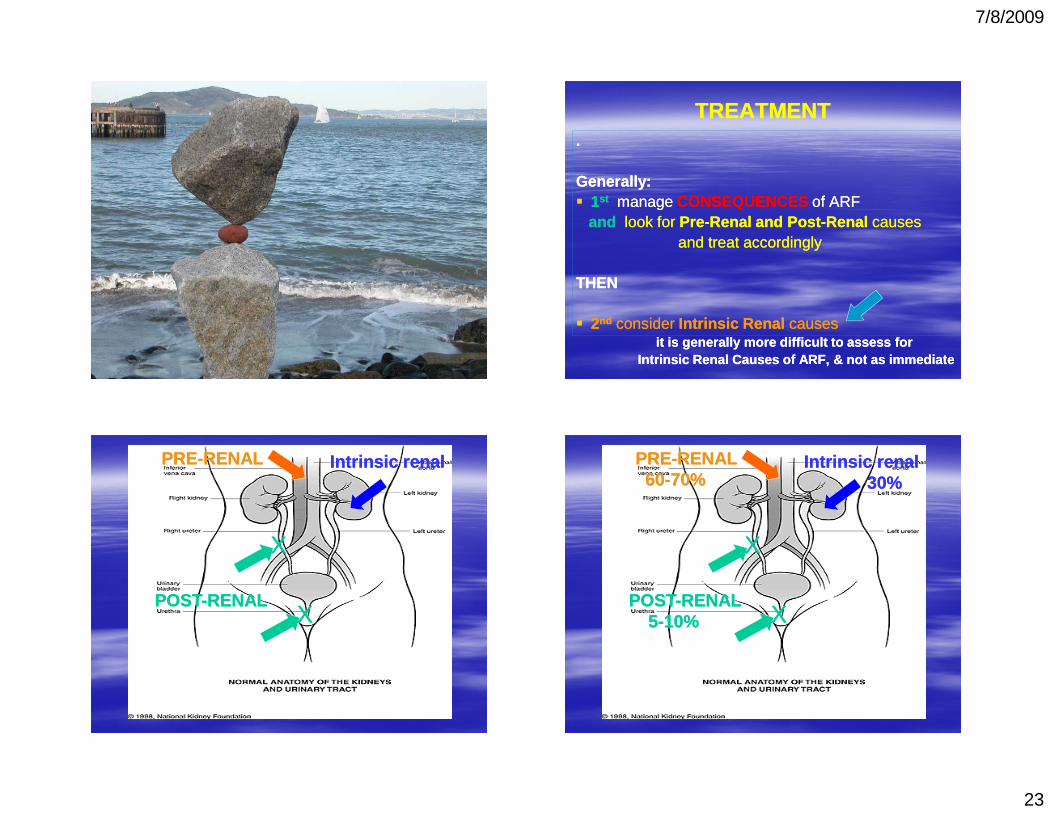
TREATMENTTREATMENT..
GenerallyGenerally::�� 11stst managemanage CONSEQUENCESCONSEQUENCES of of ARFARF
andand look for look for PrePre--Renal and PostRenal and Post--RenalRenal causes causes and treat accordingly and treat accordingly
THEN THEN
�� 22ndnd consider consider Intrinsic RenalIntrinsic Renal causes causes it is generally more difficult to assess for it is generally more difficult to assess for
Intrinsic Renal Causes of ARF, & not as immediateIntrinsic Renal Causes of ARF, & not as immediate
PREPRE--RENALRENAL
POSTPOST--RENALRENAL
Intrinsic renalIntrinsic renal
XX
XX
PREPRE--RENAL RENAL 6060--70%70%
POSTPOST--RENALRENAL55--10%10%
Intrinsic renalIntrinsic renal30%30%
XX
XX
7/8/2009
24
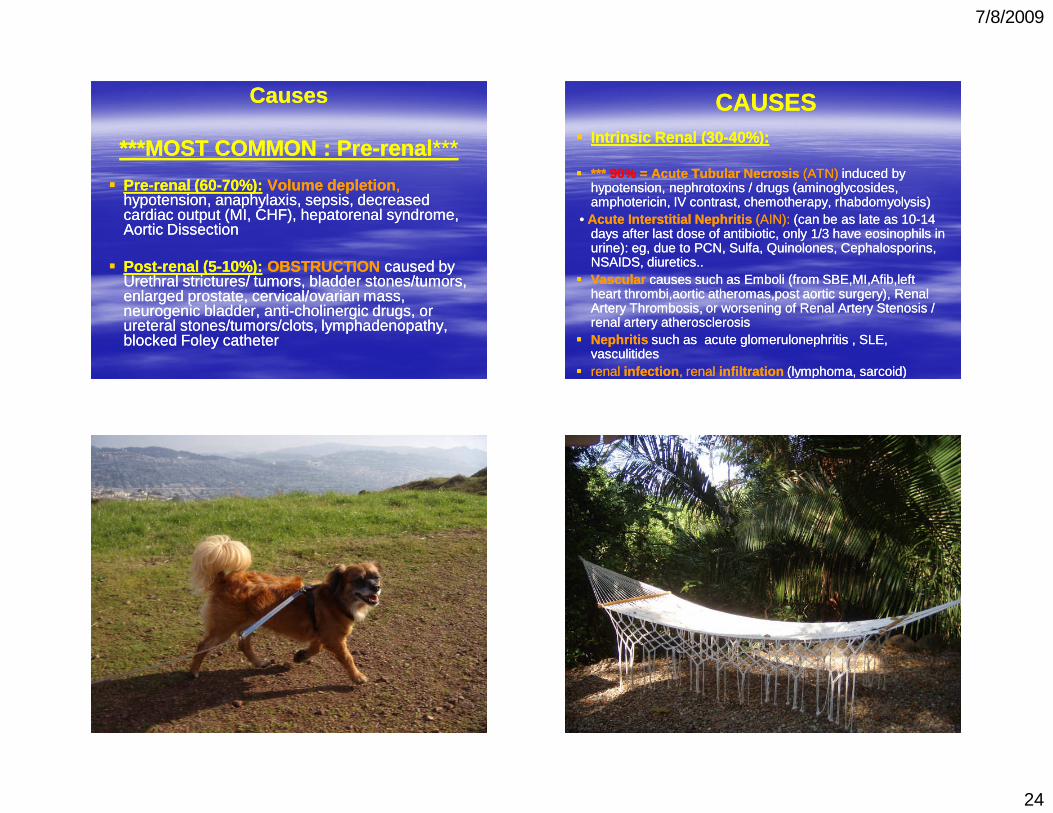
CausesCauses
***MOST COMMON : Pre***MOST COMMON : Pre--renalrenal ******
�� PrePre--renal (60renal (60--70%):70%): Volume depletionVolume depletion ,,hypotension, anaphylaxis, sepsis, decreased hypotension, anaphylaxis, sepsis, decreased cardiac output (MI, CHF), hepatorenal syndrome, cardiac output (MI, CHF), hepatorenal syndrome, Aortic DissectionAortic Dissection
�� PostPost--renal (5renal (5--10%):10%): OBSTRUCTIONOBSTRUCTION caused by caused by Urethral strictures/ tumors, bladder stones/tumors, Urethral strictures/ tumors, bladder stones/tumors, enlarged prostate, cervical/ovarian mass, enlarged prostate, cervical/ovarian mass, neurogenic bladder, antineurogenic bladder, anti--cholinergic drugs, or cholinergic drugs, or ureteral stones/tumors/clots, lymphadenopathy, ureteral stones/tumors/clots, lymphadenopathy, blocked Foley catheterblocked Foley catheter
CAUSESCAUSES�� Intrinsic Renal (30Intrinsic Renal (30--40%):40%):
�� *** *** 90% 90% = Acute = Acute Tubular NecrosisTubular Necrosis (ATN)(ATN) induced by induced by hypotension, hypotension, nephrotoxinsnephrotoxins / drugs (/ drugs (aminoglycosidesaminoglycosides, , amphotericinamphotericin, IV contrast, chemotherapy, , IV contrast, chemotherapy, rhabdomyolysisrhabdomyolysis))
• • Acute Interstitial NephritisAcute Interstitial Nephritis (AIN):(AIN): (can be as late as 10(can be as late as 10--14 14 days after last dose of antibiotic, only 1/3 have days after last dose of antibiotic, only 1/3 have eosinophilseosinophils in in urine): urine): egeg, due to PCN, Sulfa, , due to PCN, Sulfa, QuinolonesQuinolones, , CephalosporinsCephalosporins, , NSAIDS, diuretics..NSAIDS, diuretics..
�� VascularVascular causes such as Emboli (from causes such as Emboli (from SBE,MI,Afib,leftSBE,MI,Afib,leftheart heart thrombi,aorticthrombi,aortic atheromas,postatheromas,post aortic surgery), aortic surgery), Renal Renal Artery Artery Thrombosis, or worsening of Renal Artery Thrombosis, or worsening of Renal Artery StenosisStenosis / / renal artery atherosclerosisrenal artery atherosclerosis
�� NephritisNephritis such as acute such as acute glomerulonephritisglomerulonephritis , SLE, , SLE, vasculitidesvasculitides
�� renal renal infectioninfection , renal , renal infiltrationinfiltration (lymphoma, (lymphoma, sarcoidsarcoid))
7/8/2009
25
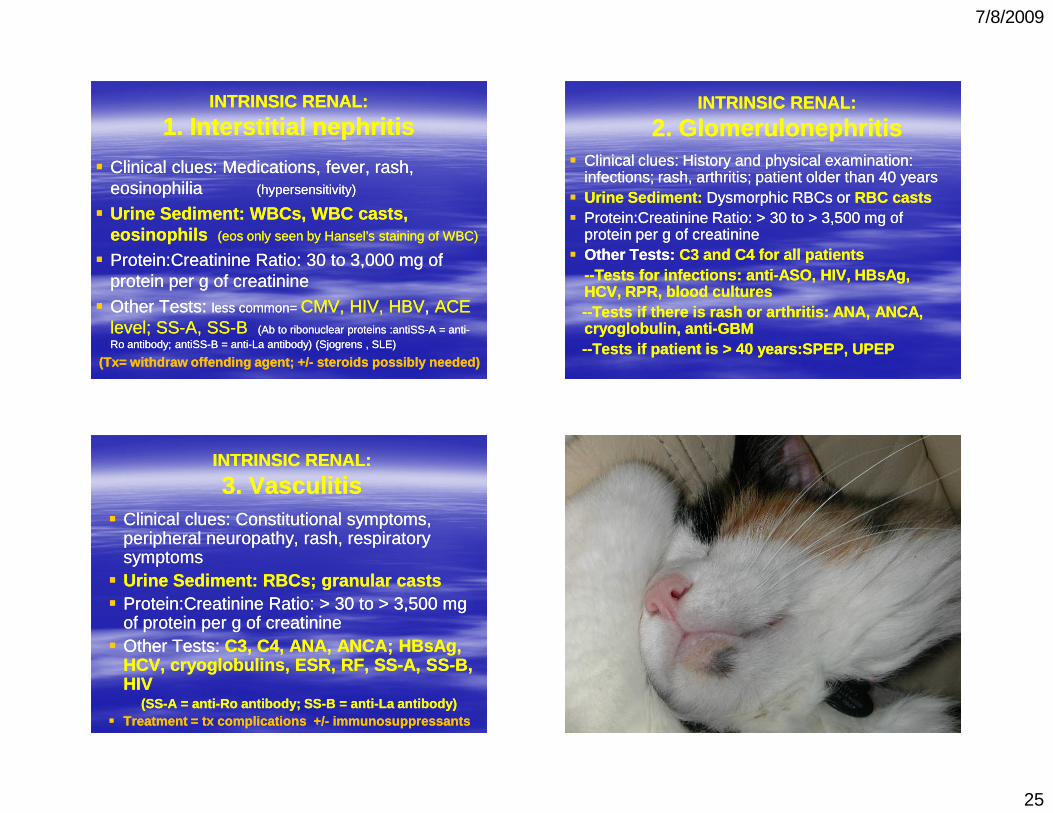
INTRINSIC RENAL:INTRINSIC RENAL:
1. 1. Interstitial nephritisInterstitial nephritis
�� Clinical clues:Clinical clues: Medications, fever, rash, Medications, fever, rash, eosinophiliaeosinophilia (hypersensitivity)(hypersensitivity)
�� Urine Sediment:Urine Sediment: WBCs, WBC casts, WBCs, WBC casts, eosinophilseosinophils ((eoseos only seen by Hansel’s staining of WBC)only seen by Hansel’s staining of WBC)
�� Protein:CreatinineProtein:Creatinine RatioRatio: 30 to 3,000 mg of : 30 to 3,000 mg of protein per g of protein per g of creatininecreatinine
�� Other TestsOther Tests: : less common= less common= CMV, HIV, HBVCMV, HIV, HBV, , ACE ACE level; SSlevel; SS--A, A, SSSS--BB ((AbAb to to ribonuclearribonuclear proteins :proteins :antiSSantiSS--A = A = antianti--Ro antibody; Ro antibody; antiSSantiSS--B B = anti= anti--La antibody) La antibody) ((SjogrensSjogrens , SLE), SLE)
((TxTx= withdraw offending agent; +/= withdraw offending agent; +/-- steroids possibly n eeded)steroids possibly needed)
INTRINSIC RENAL: INTRINSIC RENAL:
2. 2. GlomerulonephritisGlomerulonephritis�� Clinical clues: Clinical clues: History and physical examination: History and physical examination:
infections; rash, arthritis; patient older than 40 yearsinfections; rash, arthritis; patient older than 40 years�� Urine Sediment:Urine Sediment: DysmorphicDysmorphic RBCs or RBCs or RBC castsRBC casts�� Protein:CreatinineProtein:Creatinine RatioRatio: > 30 to > 3,500 mg of : > 30 to > 3,500 mg of
protein per g of protein per g of creatininecreatinine�� Other TestsOther Tests : : C3 and C4 for all patientsC3 and C4 for all patients
----Tests for infections: Tests for infections: antianti--ASO, ASO, HIV, HIV, HBsAgHBsAg, , HCV, RPR, blood HCV, RPR, blood culturescultures----Tests if there is rash or arthritis: ANA, ANCA, Tests if there is rash or arthritis: ANA, ANCA, cryoglobulincryoglobulin, anti, anti--GBM GBM ----Tests if patient is > 40 Tests if patient is > 40 years:SPEPyears:SPEP, UPEP, UPEP
INTRINSIC RENAL: INTRINSIC RENAL:
3. 3. VasculitisVasculitis�� Clinical clues:Clinical clues: Constitutional symptoms, Constitutional symptoms,
peripheral neuropathy, rash, respiratory peripheral neuropathy, rash, respiratory symptomssymptoms
�� Urine Sediment:Urine Sediment: RBCs; granular casts RBCs; granular casts �� Protein:CreatinineProtein:Creatinine RatioRatio: > 30 to > 3,500 mg : > 30 to > 3,500 mg
of protein per g of of protein per g of creatininecreatinine�� Other TestsOther Tests: : C3, C4, ANA, ANCA; C3, C4, ANA, ANCA; HBsAgHBsAg, ,
HCV, HCV, cryoglobulinscryoglobulins, ESR, RF, SS, ESR, RF, SS--A, SSA, SS--B, B, HIV HIV
(SS(SS--A = antiA = anti--Ro antibody; SSRo antibody; SS--B = antiB = anti--La antibody)La antibody)�� Treatment = Treatment = txtx complications +/complications +/-- immunosuppressantsimmunosuppressants

7/8/2009
26
A Few A Few Final NotesFinal Notes::
�� Remember to Remember to adjust doses of all drugsadjust doses of all drugs for for new GFR/Creat clearance (assume the new GFR/Creat clearance (assume the lowest eGFR if status is still dynamic)lowest eGFR if status is still dynamic)
�� For ATN from For ATN from rhabdomyolysisrhabdomyolysis , treat with , treat with IV bicarbonate: D5W w/ 3 amps NaHCO3/L IV bicarbonate: D5W w/ 3 amps NaHCO3/L at 100at 100--150ml/hr, titrate to high volume UOP, 150ml/hr, titrate to high volume UOP, and use furosemide to force diuresis.and use furosemide to force diuresis.
�� Historically, diuretics have often been used Historically, diuretics have often been used to convert oliguric to nonto convert oliguric to non--oliguric renal oliguric renal failure. This is of unclear benefit and may failure. This is of unclear benefit and may cause increased mortality.cause increased mortality.
�� Recent studies show no benefit for use of Recent studies show no benefit for use of renalrenal--dose dopamine.dose dopamine.
7/8/2009
27
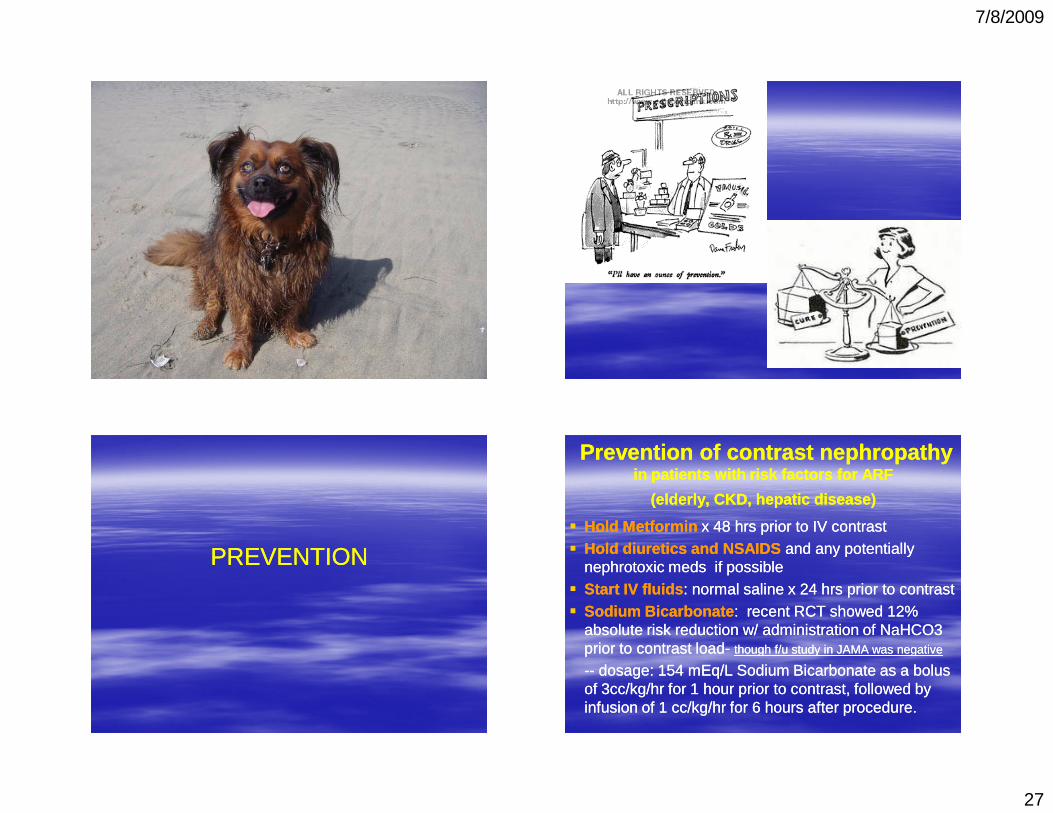
PREVENTIONPREVENTION
PreventionPrevention of contrast nephropathy of contrast nephropathy in patients with risk factors for ARF in patients with risk factors for ARF
(elderly, CKD, hepatic disease)(elderly, CKD, hepatic disease)
�� Hold Hold MetforminMetformin x 48 hrs prior to IV contrastx 48 hrs prior to IV contrast�� Hold diuretics and NSAIDSHold diuretics and NSAIDS and any potentially and any potentially
nephrotoxicnephrotoxic meds if possible meds if possible �� Start IV fluidsStart IV fluids : normal saline x 24 hrs prior to contrast: normal saline x 24 hrs prior to contrast�� Sodium BicarbonateSodium Bicarbonate : recent RCT showed 12% : recent RCT showed 12%
absolute risk reduction w/ administration of NaHCO3 absolute risk reduction w/ administration of NaHCO3 prior to contrast prior to contrast loadload-- though f/u study in JAMA was negativethough f/u study in JAMA was negative
---- dosage: 154 dosage: 154 mEqmEq/L Sodium Bicarbonate as a bolus /L Sodium Bicarbonate as a bolus of 3cc/kg/hr for 1 hour prior to contrast, followed by of 3cc/kg/hr for 1 hour prior to contrast, followed by infusion of 1 cc/kg/hr for 6 hours after procedure.infusion of 1 cc/kg/hr for 6 hours after procedure.

7/8/2009
28
PreventionPreventionof contrast nephropathyof contrast nephropathy
�� Use oral Use oral acetylcysteineacetylcysteine ((MucomystMucomyst)) before before administering iodinated contrast loads in administering iodinated contrast loads in patients with risk factors patients with risk factors
�� Dose = 600 mg Dose = 600 mg popo bid the day before and bid the day before and the day of the study, along with adequate the day of the study, along with adequate hydration. (4 doses totalhydration. (4 doses total))
�� controversial, with metacontroversial, with meta--analyses reaching analyses reaching different conclusions about efficacy in preventiondifferent conclusions about efficacy in prevention
of Part 1 !!
7/8/2009
29
A deep, restoring b-r-e-a-t-h . . . . .
BEFORE PART 2 !
7/8/2009
30
Part 2:Part 2:CHRONIC KIDNEY DISEASECHRONIC KIDNEY DISEASEScreening for CKD:Screening for CKD:–– WhomWhom do you screen?do you screen?–– WhyWhy do you screen ?do you screen ?–– HowHow do you screen ?do you screen ?
Diagnosing CKD: Diagnosing CKD:
–– How do you diagnose the How do you diagnose the causecause of CKD?of CKD?
–– How do you How do you slow the progression slow the progression of CKD? of CKD?
–– How do you How do you treat the effectstreat the effects of CKD?of CKD?
2 Typical scenarios:2 Typical scenarios:
�� #1 You are seeing a new patient, and #1 You are seeing a new patient, and reviewing PMH, etc. You decide that she is reviewing PMH, etc. You decide that she is at “increased risk for CKD” . at “increased risk for CKD” . Who is at risk and What do you do?Who is at risk and What do you do?
OROR
�� #2 You are seeing a patient, and you notice #2 You are seeing a patient, and you notice on routine labs that his on routine labs that his CreatinineCreatinine is is somewhat elevated, and somewhat elevated, and eGFReGFR is low.is low.
What do you do?What do you do?
2 Typical scenarios:2 Typical scenarios:�� #1 You are seeing a new patient, and #1 You are seeing a new patient, and
reviewing PMH, etc. You decide that she is reviewing PMH, etc. You decide that she is at “increased risk for CKD” . What do you at “increased risk for CKD” . What do you do? do? (Answer: SCREEN for CKD)(Answer: SCREEN for CKD)
�� #2 You are seeing a patient, and you notice #2 You are seeing a patient, and you notice on routine labs that his on routine labs that his CreatinineCreatinine is is somewhat elevated, and somewhat elevated, and eGFReGFR is low.is low.
What do you do?What do you do?
(Answer: Diagnose CKD (Answer: Diagnose CKD ---- look for the look for the causecause and try to and try to slow the progressionslow the progression ))
7/8/2009
31
WHOM WHOM to screen for CKDto screen for CKD::
Screen all w/ Screen all w/ risk factors for kidney diseaserisk factors for kidney disease ::
�� DMDM ((DMDM isis most common cause of CKDmost common cause of CKD ),),�� HTN, HTN, �� age over 60 age over 60 yoyo, , �� Family Family HxHx of renal of renal dzdz, , �� h/o recurrent UTI, h/o recurrent UTI, �� h/o urinary obstruction, h/o urinary obstruction, �� or systemic illness that affects the kidneysor systemic illness that affects the kidneys
Of note, regarding Of note, regarding ESRDESRD::
�� 4040--60%60% of pts w/ ESRD have of pts w/ ESRD have DMDM
�� 1515--30%30% of pts w/ ESRD have of pts w/ ESRD have HTNHTN
�� <10 % have <10 % have glomerulonephritisglomerulonephritis�� 22--3% have cystic kidneys3% have cystic kidneys
WHY WHY screen for CKDscreen for CKD: :
�� it’s inexpensive & easy, and we can try to it’s inexpensive & easy, and we can try to prevent or prevent or slow disease progressionslow disease progression to kidney to kidney failure, and failure, and reduce complicationsreduce complications from from decreased kidney function, and decreased kidney function, and prevent prevent development of cardiovascular disease and development of cardiovascular disease and other effectsother effects–– CKD is a risk factor for cardiovascular disease CKD is a risk factor for cardiovascular disease –– Cardiovascular disease is the most common cause of Cardiovascular disease is the most common cause of
death in patients with chronic kidney disease. death in patients with chronic kidney disease. –– The risk of cardiovascular disease and associated The risk of cardiovascular disease and associated
mortality mortality increases in proportion to the decrease in increases in proportion to the decrease in the GFR.the GFR.
HowHow to screen for CKD:to screen for CKD:
�� Blood pressure Blood pressure
�� CreatCreat�� eGFReGFR (w/ serum electrolytes =Chem7)(w/ serum electrolytes =Chem7)
�� random urine sample for random urine sample for ProteinuriaProteinuria( I( Instead of a timed urine collection, a nstead of a timed urine collection, a random urine sample for the random urine sample for the
albuminalbumin--creatininecreatinine ratio or proteinratio or protein--creatininecreatinine ratioratio ))
+ UA with microscopy + UA with microscopy
( to examine urine sediment/casts/cells etc)( to examine urine sediment/casts/cells etc)
7/8/2009
32
A bit about A bit about
1. 1. eGFReGFR
andand
2. 2. proteinuriaproteinuria
Creatinephosphate
CreatinePhosphate
creatinine creatinine
About About CreatinineCreatinine and GFRand GFR
�� CreatinineCreatinine is made from creatine, a is made from creatine, a compound found almost exclusively in compound found almost exclusively in muscle and made at a relatively constant muscle and made at a relatively constant rate. rate.
�� Creatinine leaves muscle and enters blood, Creatinine leaves muscle and enters blood, and is removed by the kidneys. and is removed by the kidneys.
�� If the kidneys lose their ability to filter blood, If the kidneys lose their ability to filter blood, more creatinine will accumulate and the more creatinine will accumulate and the serum serum creatininecreatinine will rise. will rise.
About About CreatinineCreatinine and GFR…and GFR…
�� GlomerularGlomerular Filtration Rate (GFR) is a Filtration Rate (GFR) is a more accurate more accurate estimateestimate of the filtering capacity of the kidneys. of the filtering capacity of the kidneys.
----It is usually expressed as It is usually expressed as mLmL per minute , & adjusted per minute , & adjusted to a “standard” body size with a surface area of 1.73 to a “standard” body size with a surface area of 1.73 meters2. (meters2. (mLmL/min/1.73m/min/1.73m22))
----normal GFRnormal GFR ranges between ranges between 95 95 --120120 mLmL/min/1.73m/min/1.73m22
but it varies but it varies depending on agedepending on age, gender and body size., gender and body size.---- GFR is usually estimated GFR is usually estimated ((eGFReGFR)) from a mathematical from a mathematical
equation based principally on the serum equation based principally on the serum creatininecreatinine, , age, gender, and race. age, gender, and race.
7/8/2009
33
AverageAverage GFR GFR by Ageby Age
�� According to National Kidney Foundation According to National Kidney Foundation (NKF), the average estimated GFR for a (NKF), the average estimated GFR for a given age group is: given age group is:
�� Age 20Age 20--30: 30: 116 mL/min/1.73m2 116 mL/min/1.73m2 �� Age 30Age 30--40: 40: 107 mL/min/1.73m2 107 mL/min/1.73m2 �� Age 40Age 40--50: 50: 99 mL/min/1.73m2 99 mL/min/1.73m2 �� Age 50Age 50--60: 60: 93 mL/min/1.73m2 93 mL/min/1.73m2 �� Age 60Age 60--70: 70: 85 mL/min/1.73m2 85 mL/min/1.73m2 �� Age 70+: Age 70+: 75 mL/min/1.73m275 mL/min/1.73m2
“OK, but a “OK, but a creatininecreatinine of 1 is of 1 is normal, no matter what, right?”normal, no matter what, right?”
OROR
“I don’t’ have to worry if the “I don’t’ have to worry if the creatininecreatinine is around 1, is around 1,
right?”right?”
Serum Serum creatininecreatinine �� used to used to calculate calculate estimated estimated glomerularglomerular filtration ratefiltration rate ((eGFReGFR))
because:because:
–– There can be considerable renal dysfunction There can be considerable renal dysfunction despite a normal serum despite a normal serum creatininecreatinine levellevel ::
–– ““An estimation of the An estimation of the GFRGFR based on the serum based on the serum creatininecreatinine level level correlates better with direct correlates better with direct measures of the GFR and measures of the GFR and detects more cases of detects more cases of chronic kidney disease than does the serum chronic kidney disease than does the serum creatininecreatinine level alonelevel alone .” .”

7/8/2009
34
eGFReGFR = 186 x (Creat / 88.4)= 186 x (Creat / 88.4) --1.1541.154
x (Age)x (Age) --0.2030.203 x (0.742 if female) x x (0.742 if female) x (1.210 if black) (1.210 if black)
go to: go to: http://mdrd.com/ http://mdrd.com/
abbreviated MDRD equation : –– EgEg: patients with the : patients with the same serum same serum creatininecreatininelevel may have different estimated GFRslevel may have different estimated GFRs ::
–– For example, a 45For example, a 45--yearyear--old Africanold African--American American man whose serum man whose serum creatininecreatinine level is 1 mg/dllevel is 1 mg/dlper per dLdL (88 µmol per L) has kidney function with (88 µmol per L) has kidney function with an estimated GFR of an estimated GFR of 104 104 mLmL per minute per per minute per 1.73 m2, 1.73 m2,
–– whereas a 65whereas a 65--yearyear--old white woman with the old white woman with the same serum same serum creatininecreatinine level of 1 mg/level of 1 mg/dLdL has has an estimated GFR of an estimated GFR of 5959 mLmL per minute per 1.73 per minute per 1.73 m2, or m2, or stage 3 kidney diseasestage 3 kidney disease .” (AFP).” (AFP)
–– useful GFR calculator: useful GFR calculator: http://mdrd.com/ http://mdrd.com/
ORORhttp://www.kidney.org/professionals/kdoqi/gfr_calculator.cfmhttp://www.kidney.org/professionals/kdoqi/gfr_calculator.cfm
A bit about A bit about
1. 1. eGFReGFR
andand
2. 2. proteinuriaproteinuria
7/8/2009
35
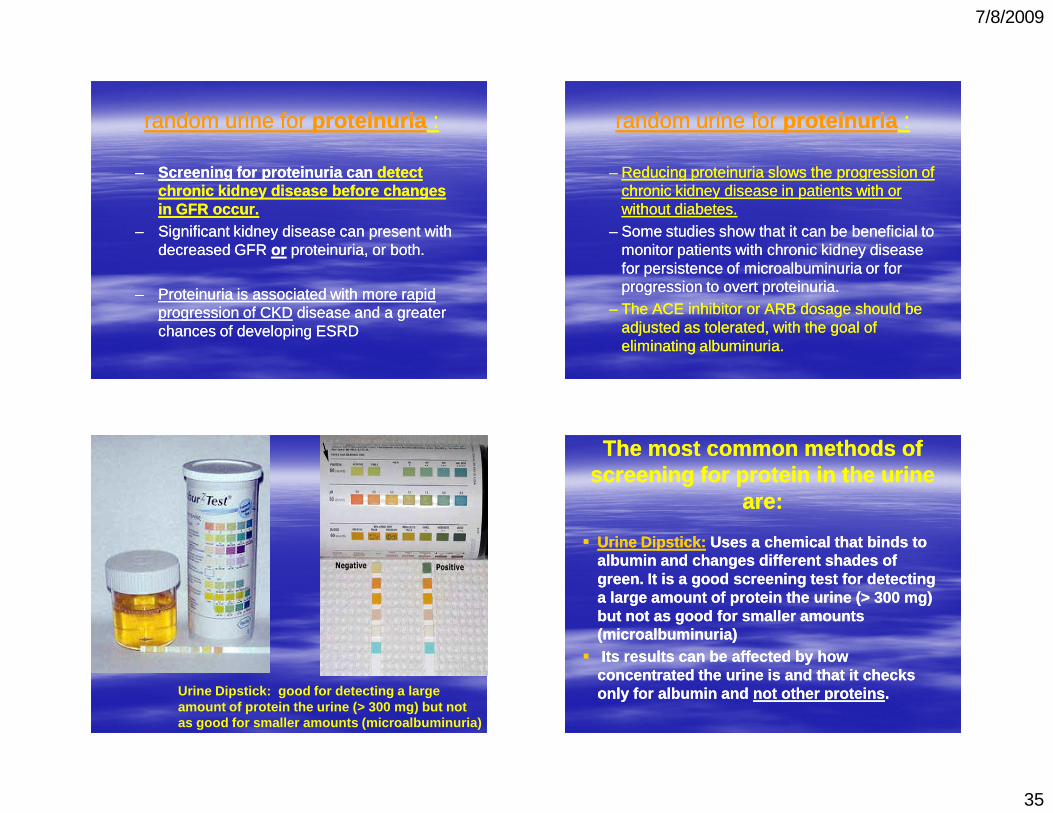
random urine for random urine for proteinuriaproteinuria ::
–– Screening for proteinuria can Screening for proteinuria can detect detect chronic kidney disease chronic kidney disease beforebefore changes changes in GFR occur.in GFR occur.
–– Significant kidney disease can present with Significant kidney disease can present with decreased GFR decreased GFR oror proteinuria, or both. proteinuria, or both.
–– Proteinuria is associated with more rapid Proteinuria is associated with more rapid progression of CKDprogression of CKD disease and a greater disease and a greater chances of developing ESRDchances of developing ESRD
random urine for random urine for proteinuriaproteinuria ::
–– Reducing proteinuria slows the progression of Reducing proteinuria slows the progression of chronic kidney disease in patients with or chronic kidney disease in patients with or without diabetes.without diabetes.
–– Some studies show that it can be beneficial to Some studies show that it can be beneficial to monitor patients with chronic kidney disease monitor patients with chronic kidney disease for persistence of microalbuminuria or for for persistence of microalbuminuria or for progression to overt proteinuria. progression to overt proteinuria.
–– The ACE inhibitor or ARB dosage should be The ACE inhibitor or ARB dosage should be adjusted as tolerated, with the goal of adjusted as tolerated, with the goal of eliminating albuminuria.eliminating albuminuria.
Urine Dipstick: good for detecting a large amount of protein the urine (> 300 mg) but not as good for smaller amounts (microalbuminuria)
The most common methods of The most common methods of screening for protein in the urine screening for protein in the urine
are:are:
�� Urine Dipstick:Urine Dipstick: Uses a chemical that binds to Uses a chemical that binds to albumin and changes different shades of albumin and changes different shades of green. It is a good screening test for detecting green. It is a good screening test for detecting a large amount of protein the urine (> 300 mg) a large amount of protein the urine (> 300 mg) but not as good for smaller amounts but not as good for smaller amounts (microalbuminuria)(microalbuminuria)
�� Its results can be affected by how Its results can be affected by how concentrated the urine is and that it checks concentrated the urine is and that it checks only for albumin and only for albumin and not other proteinsnot other proteins ..
7/8/2009
36
�� Urine AlbuminUrine Albumin ::�� Since the dipstick is not very sensitive to low Since the dipstick is not very sensitive to low
levels of albumin in the urine, it is helpful to levels of albumin in the urine, it is helpful to measure the urine albumin directly measure the urine albumin directly ((microalbuminuriamicroalbuminuria). ).
�� MicroalbuminMicroalbumin is the term ascribed to the is the term ascribed to the measurement of albumin in urine at measurement of albumin in urine at concentrations below the sensitivity of concentrations below the sensitivity of dipstick tests for total protein . dipstick tests for total protein .
�� Collecting urine for a 24Collecting urine for a 24--hour period has hour period has been considered been considered thethe gold standardgold standard . .
�� However, because it is very inconvenient However, because it is very inconvenient and prone to error if the urine isn’t collected and prone to error if the urine isn’t collected properly, we use urine properly, we use urine protein : creatinineprotein : creatinineratio instead. (or albumin: creat ratio)ratio instead. (or albumin: creat ratio)
�� It is requires only a small sample of urine It is requires only a small sample of urine and it is relatively accurate and convenient. and it is relatively accurate and convenient.
Interpretation of Interpretation of Urine ProteinUrine Protein to to Urine Urine CreatinineCreatinine
RatioRatio
�� Child under age 2 years Child under age 2 years –– Normal Ratio <0.5 (500 mg/g)Normal Ratio <0.5 (500 mg/g)
�� Adults and children over age 2 years Adults and children over age 2 years –– Normal ratio <0.2 grams protein per gm Normal ratio <0.2 grams protein per gm CreatinineCreatinine
(normal is < 200mg per gram of (normal is < 200mg per gram of CreatinineCreatinine))�� Correlates with 0.2 g protein/day Correlates with 0.2 g protein/day
–– NephroticNephrotic Ratio >3.5 (correlates with 3.5 g protein) Ratio >3.5 (correlates with 3.5 g protein)
Interpretation of Interpretation of Urine AlbuminUrine Albumin to to CreatinineCreatinine
RatioRatio
�� Normal Ratio (in general <30 mg/g is normal) Normal Ratio (in general <30 mg/g is normal) –– Men: < 0.017 (or 17 mg albumin to 1 gram Men: < 0.017 (or 17 mg albumin to 1 gram CreatinineCreatinine) ) –– Women: <0.025 (or 25 mg albumin to 1 gm Women: <0.025 (or 25 mg albumin to 1 gm CreatinineCreatinine) )
�� Microalbuminuria: 30Microalbuminuria: 30--300 mg albumin/g 300 mg albumin/g CreatinineCreatinine�� Macroalbuminuria: >300 mg albumin/g Macroalbuminuria: >300 mg albumin/g CreatinineCreatinine
7/8/2009
37
screening
(Incidental UA/dip)
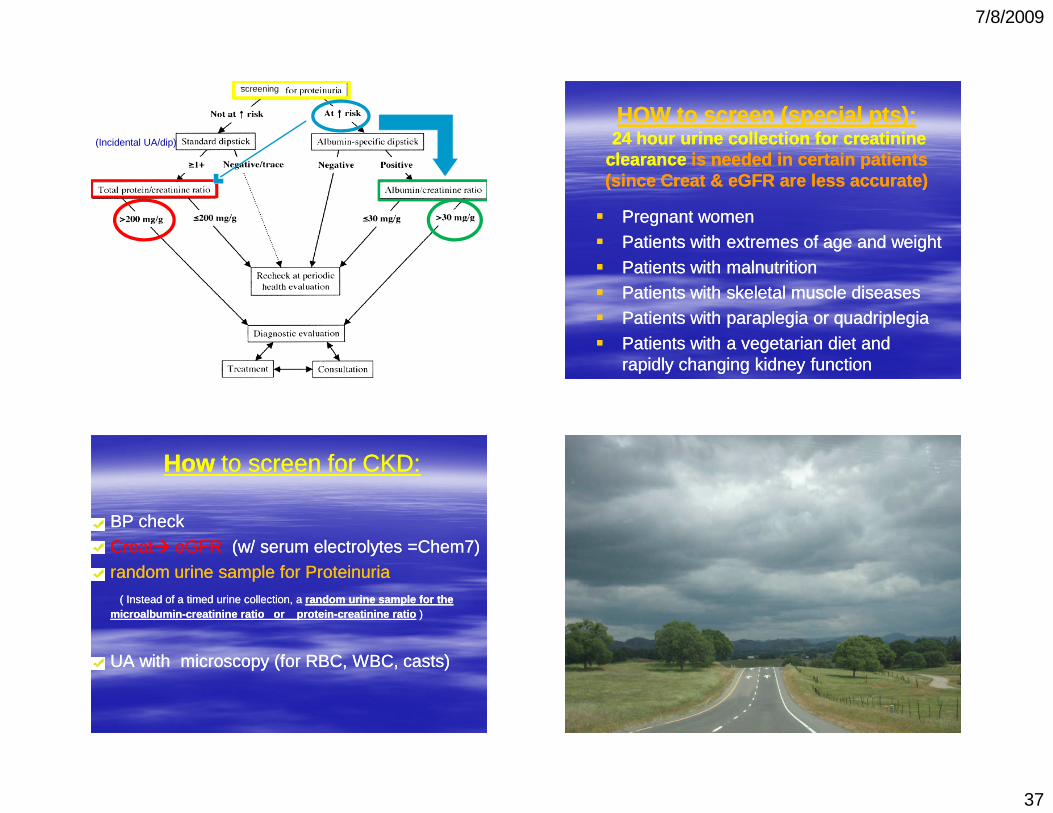
HOW to screen (special pts):HOW to screen (special pts):24 hour urine24 hour urine collection for creatinine collection for creatinine
clearanceclearance is needed in certain patients is needed in certain patients (since Creat & eGFR are less accurate)(since Creat & eGFR are less accurate)
�� Pregnant womenPregnant women
�� Patients with extremes of age and weightPatients with extremes of age and weight
�� Patients with malnutritionPatients with malnutrition�� Patients with skeletal muscle diseasesPatients with skeletal muscle diseases
�� Patients with paraplegia or quadriplegiaPatients with paraplegia or quadriplegia
�� Patients with a vegetarian diet and Patients with a vegetarian diet and rapidly changing kidney functionrapidly changing kidney function
HowHow to screen for CKD:to screen for CKD:
�� BP checkBP check
�� CreatCreat�� eGFReGFR (w/ serum electrolytes =Chem7)(w/ serum electrolytes =Chem7)
�� random urine sample for random urine sample for ProteinuriaProteinuria( I( Instead of a timed urine collection, a nstead of a timed urine collection, a random urine sample for the random urine sample for the
microalbuminmicroalbumin--creatininecreatinine ratio or proteinratio or protein--creatininecreatinine ratioratio ))
�� UA with microscopy (for RBC, WBC, casts)UA with microscopy (for RBC, WBC, casts)
7/8/2009
38
OverviewOverview
Screening for CKD:Screening for CKD:–– WhomWhom do you screen?do you screen?–– WhyWhy do you screen ?do you screen ?–– HowHow do you screen ?do you screen ?
Diagnosing CKD: Diagnosing CKD:
–– How do you diagnose the How do you diagnose the causecause of CKD?of CKD?
–– How do you How do you slow the progression slow the progression of CKD? of CKD?
–– How do you How do you treat the effectstreat the effects of CKD?of CKD?
2 Typical scenarios:2 Typical scenarios:�� #1 You are seeing a new patient, and #1 You are seeing a new patient, and
reviewing PMH, etc. You decide that she is at reviewing PMH, etc. You decide that she is at “increased risk for CKD” . What do you do? “increased risk for CKD” . What do you do? (Answer: SCREEN for CKD)(Answer: SCREEN for CKD)
�� #2 You are seeing a patient, and you notice #2 You are seeing a patient, and you notice on routine labs that his on routine labs that his CreatinineCreatinine is is somewhat elevated, and somewhat elevated, and eGFReGFR is low.is low.
What do you do?What do you do?
(Answer: Diagnose CKD (Answer: Diagnose CKD ---- look for the look for the causecause ,try to ,try to slow progression, + treat effects)slow progression, + treat effects)
Definitions from the National Kidney Definitions from the National Kidney Foundation's Kidney Disease Foundation's Kidney Disease Outcomes Quality InitiativeOutcomes Quality Initiative
Definition of Definition of Chronic kidney disease (CKD):Chronic kidney disease (CKD):�� Kidney damage Kidney damage for 3 or more months for 3 or more months based on findings based on findings
of abnormal of abnormal structurestructure (imaging studies(imaging studies) ) oror abnormalabnormal function function (blood tests, urinalysis)(blood tests, urinalysis)
Or Or GFR below 60GFR below 60 mLmL per minute per 1.73 m2 for per minute per 1.73 m2 for 3 or more months with or without evidence of kidney 3 or more months with or without evidence of kidney
damagedamage
Definition of Definition of EndEnd--stage renal diseasestage renal disease (kidney failure)(kidney failure)�� GFR below 15 GFR below 15 mLmL per minute per 1.73 m2 per minute per 1.73 m2 �� OR OR Need for kidney replacement therapy (dialysis or Need for kidney replacement therapy (dialysis or
transplant) transplant)
7/8/2009
39
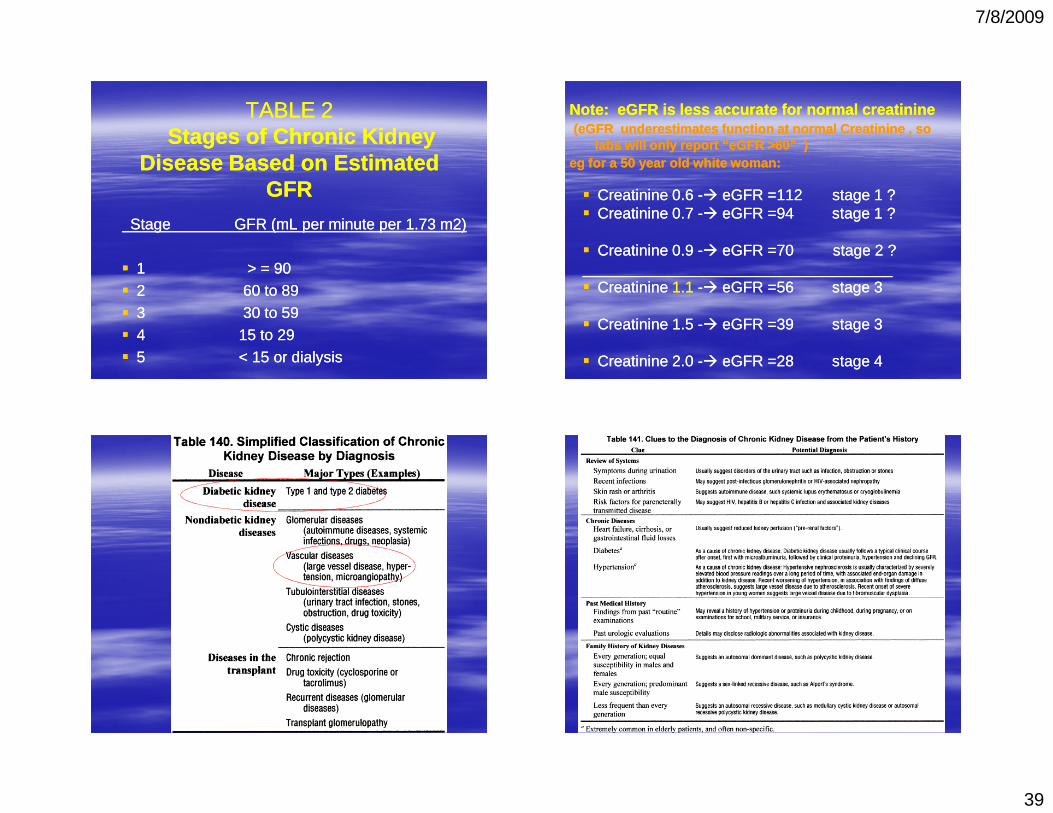
TABLE 2 TABLE 2 Stages of Chronic Kidney Stages of Chronic Kidney
Disease Based on Estimated Disease Based on Estimated GFRGFR
Stage GFR (mL per minute per 1.73 m2)Stage GFR (mL per minute per 1.73 m2)
�� 1 > = 901 > = 90�� 2 60 to 892 60 to 89�� 3 30 to 593 30 to 59�� 4 15 to 294 15 to 29�� 5 < 15 or dialysis 5 < 15 or dialysis
Note: Note: eGFReGFR is less accurate for normal is less accurate for normal creatininecreatinine((eGFReGFR underestimates function at normal underestimates function at normal CreatinineCreatinine , so, so
labs will only report “labs will only report “eGFReGFR >60” ) >60” ) egeg for a 50 year old white woman:for a 50 year old white woman:
�� CreatinineCreatinine 0.6 0.6 --�� eGFReGFR ==112 stage 1 ?112 stage 1 ?�� CreatinineCreatinine 0.7 0.7 --�� eGFReGFR ==94 stage 1 ?94 stage 1 ?
�� CreatinineCreatinine 0.9 0.9 --�� eGFReGFR ==7070 stage 2 ?stage 2 ?________________________________________________________________________�� CreatinineCreatinine 1.11.1 --�� eGFReGFR ==56 stage 356 stage 3
�� CreatinineCreatinine 1.5 1.5 --�� eGFReGFR ==39 stage 339 stage 3
�� CreatinineCreatinine 2.0 2.0 --�� eGFReGFR ==28 stage 428 stage 4

7/8/2009
40
Evaluation for Causes of Evaluation for Causes of Chronic Kidney Disease:Chronic Kidney Disease:
�� CBC, CHEM 7CBC, CHEM 7: Na, : Na, KK , , ClCl, , CO2CO2, , BUNBUN, , CrCr , , Glucose (STAT Glucose (STAT EKGEKG if if HyperkalemicHyperkalemic))
�� UA with microscopyUA with microscopy ((castscasts , RBC, WBC, , RBC, WBC, protein)protein)
�� +/+/-- Urine CultureUrine Culture�� Urine proteinUrine protein--creatcreat or albuminor albumin--creatcreat ratioratio
�� Renal ultrasoundRenal ultrasound�� OptionalOptional: KUB (for stones), CT Abdomen (for : KUB (for stones), CT Abdomen (for
masses if suspicion exists by masses if suspicion exists by HxHx/PE)/PE)�� If needed : other “special labs” If needed : other “special labs”
Best to have done these tests at leastBest to have done these tests at leastprior to referring prior to referring to to NephrologistNephrologist
7/8/2009
41
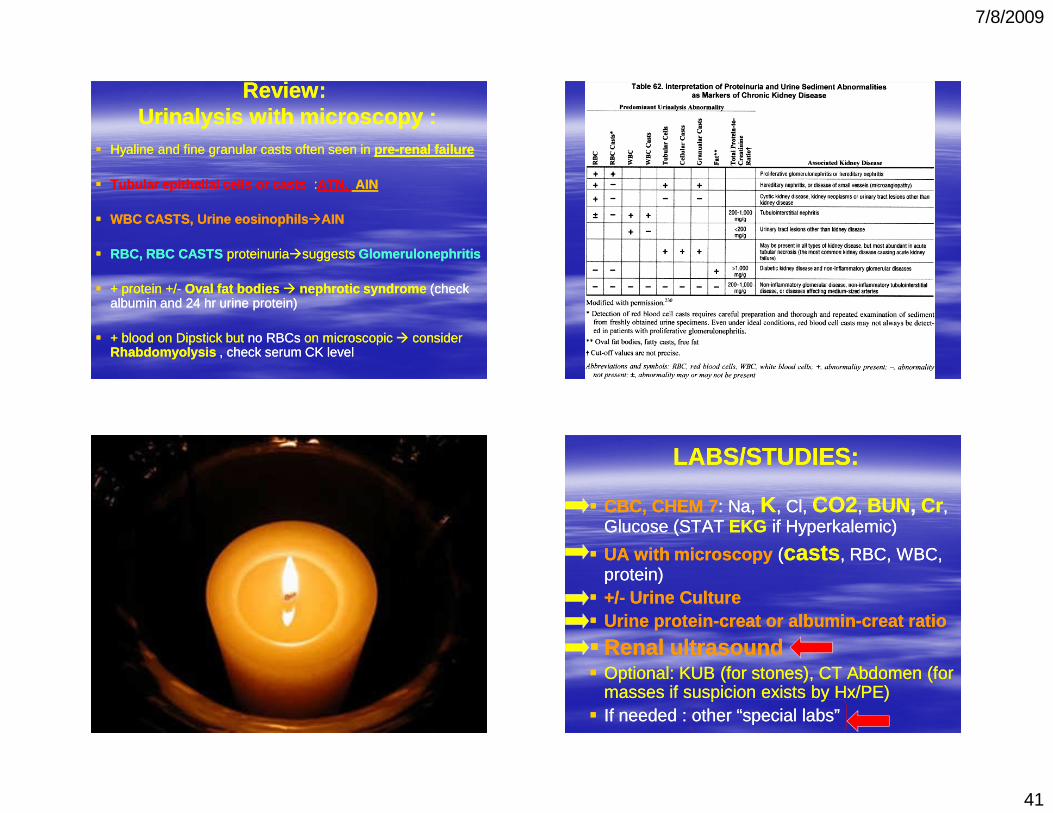
Review:Review:Urinalysis with Urinalysis with microscopymicroscopy ::
�� Hyaline and fine granular casts often seen in Hyaline and fine granular casts often seen in prepre--renal failurerenal failure
�� Tubular epithelial cells or castsTubular epithelial cells or casts ::ATN, ATN, AINAIN
�� WBC CASTS, Urine WBC CASTS, Urine eosinophilseosinophils ��AINAIN
�� RBC, RBC CASTS RBC, RBC CASTS proteinuriaproteinuria��suggestssuggests GlomerulonephritisGlomerulonephritis
�� + protein +/+ protein +/-- Oval fat bodiesOval fat bodies �� nephroticnephrotic syndromesyndrome (check (check albumin and 24 hr urine protein) albumin and 24 hr urine protein)
�� + blood on Dipstick but + blood on Dipstick but no RBCsno RBCs on microscopic on microscopic �� consider consider RhabdomyolysisRhabdomyolysis , check serum CK level, check serum CK level
LABS/STUDIES:LABS/STUDIES:
�� CBC, CHEM 7CBC, CHEM 7: Na, : Na, KK , , ClCl, , CO2CO2, , BUNBUN, , CrCr , , Glucose (STAT Glucose (STAT EKGEKG if if HyperkalemicHyperkalemic))
�� UA with microscopyUA with microscopy ((castscasts , RBC, WBC, , RBC, WBC, protein)protein)
�� +/+/-- Urine CultureUrine Culture�� Urine proteinUrine protein--creatcreat or albuminor albumin--creatcreat ratioratio
�� Renal ultrasoundRenal ultrasound�� OptionalOptional: KUB (for stones), CT Abdomen (for : KUB (for stones), CT Abdomen (for
masses if suspicion exists by masses if suspicion exists by HxHx/PE)/PE)�� If needed : other “special labs” If needed : other “special labs”
7/8/2009
42
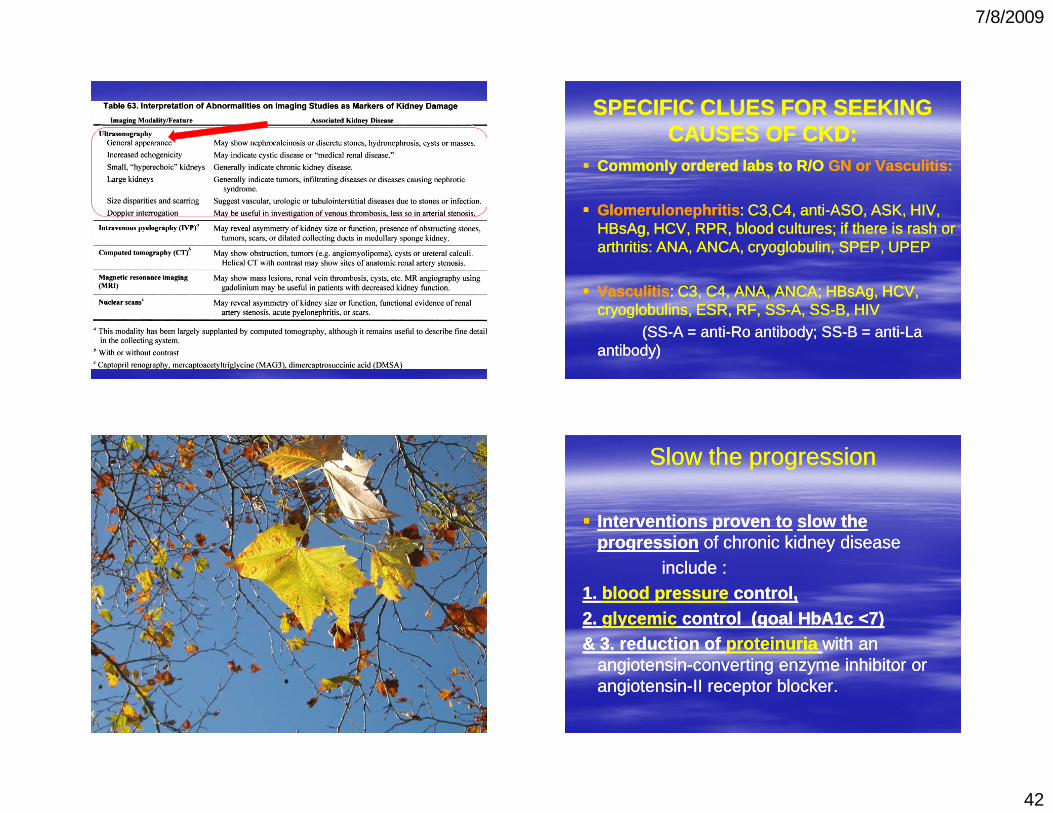
SPECIFIC CLUES FOR SEEKING SPECIFIC CLUES FOR SEEKING CAUSES OF CKD:CAUSES OF CKD:
�� Commonly ordered labs toCommonly ordered labs to R/OR/O GN or GN or VasculitisVasculitis::
�� GlomerulonephritisGlomerulonephritis : : C3,C4, antiC3,C4, anti--ASO, ASK, HIV, ASO, ASK, HIV, HBsAgHBsAg, HCV, RPR, blood cultures; if there is rash or , HCV, RPR, blood cultures; if there is rash or arthritis: ANA, ANCA, arthritis: ANA, ANCA, cryoglobulincryoglobulin, SPEP, UPEP, SPEP, UPEP
�� VasculitisVasculitis : : C3, C4, ANA, ANCA; C3, C4, ANA, ANCA; HBsAgHBsAg, HCV, , HCV, cryoglobulinscryoglobulins, ESR, RF, SS, ESR, RF, SS--A, SSA, SS--B, HIVB, HIV
(SS(SS--A = antiA = anti--Ro antibody; SSRo antibody; SS--B = antiB = anti--La La antibody) antibody)
Slow the progressionSlow the progression
�� Interventions proven toInterventions proven to slow the slow the progressionprogression of chronic kidney diseaseof chronic kidney disease
include : include :
1. 1. blood pressureblood pressure control, control, 2. 2. glycemicglycemic control (goal HbA1c <7) control (goal HbA1c <7) & 3. reduction of & 3. reduction of proteinuriaproteinuria with an with an
angiotensinangiotensin--converting enzyme inhibitor or converting enzyme inhibitor or angiotensinangiotensin--II receptor blocker.II receptor blocker.

7/8/2009
43
Complications in Chronic Kidney Complications in Chronic Kidney Disease Disease
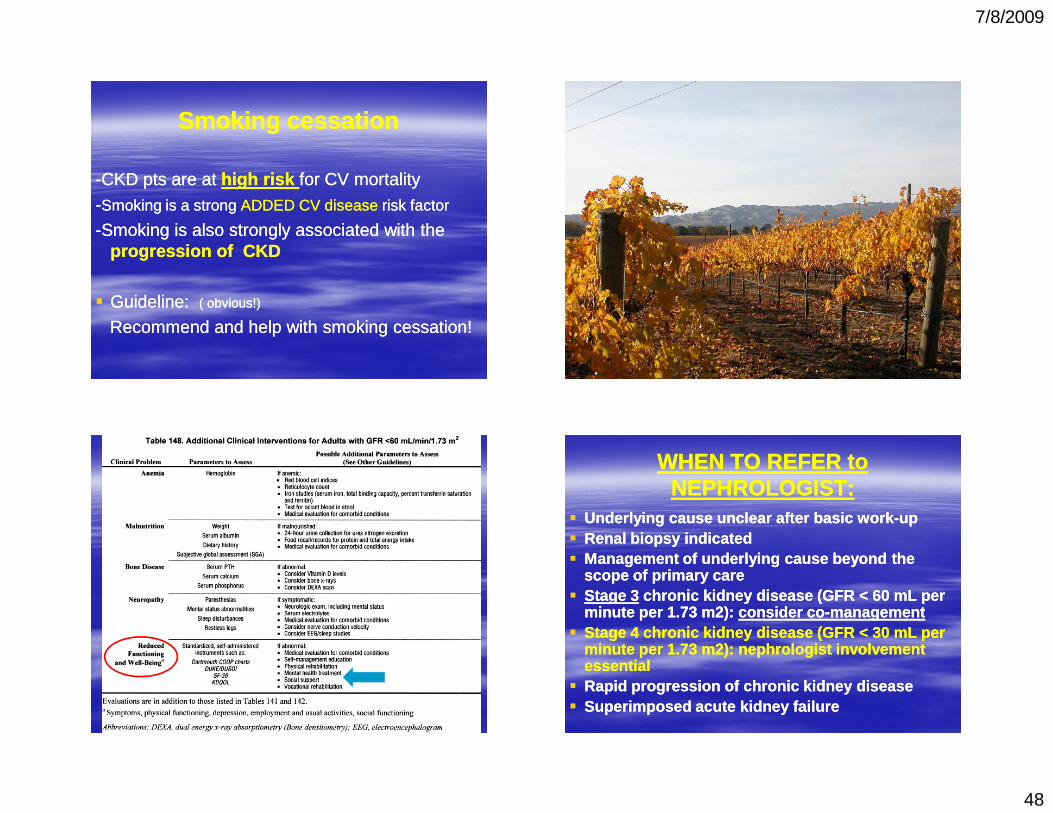
Patients with a GFR below 60 Patients with a GFR below 60 mLmL should have should have monitoring for these complications:monitoring for these complications:
HyperkalemiaHyperkalemiaHyperphosphatemiaHyperphosphatemia, , HypocalcemiaHypocalcemia
(secondary hyperparathyroidism)(secondary hyperparathyroidism)HyponatremiaHyponatremia, Acidosis, AcidosisHypoalbuminemiaHypoalbuminemiaDecreased Decreased immunoglobulinsimmunoglobulins
More Complications in More Complications in Chronic Kidney DiseaseChronic Kidney Disease
DyslipidemiaDyslipidemia, CAD, CADHTNHTNAnemiaAnemiaRenal Renal OsteodystrophyOsteodystrophy ( 2 high PTH)( 2 high PTH)Uremia Uremia ((�� needing dialysis or transplant)needing dialysis or transplant)
7/8/2009
44
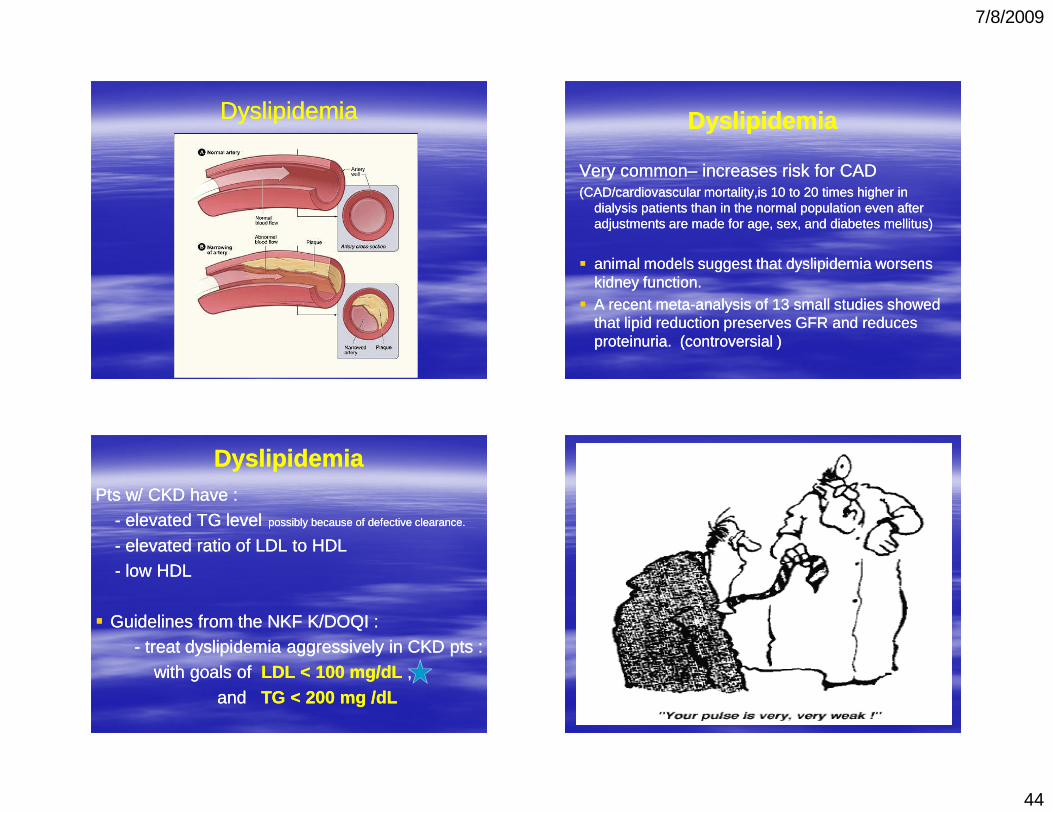
DyslipidemiaDyslipidemia DyslipidemiaDyslipidemia
Very commonVery common–– increases risk for CADincreases risk for CAD(CAD/cardiovascular (CAD/cardiovascular mortality,ismortality,is 10 to 20 times higher in 10 to 20 times higher in
dialysis patients than in the normal population even after dialysis patients than in the normal population even after adjustments are made for age, sex, and diabetes mellitus) adjustments are made for age, sex, and diabetes mellitus)
�� animal models suggest that animal models suggest that dyslipidemiadyslipidemia worsens worsens kidney function. kidney function.
�� A recent metaA recent meta--analysis of 13 small studies showed analysis of 13 small studies showed that lipid reduction preserves GFR and reduces that lipid reduction preserves GFR and reduces proteinuriaproteinuria. (controversial ). (controversial )
DyslipidemiaDyslipidemiaPts w/ CKD have :Pts w/ CKD have :
-- elevated TG levelelevated TG level possibly because of defective clearance.possibly because of defective clearance.
-- elevated ratio of LDL to HDLelevated ratio of LDL to HDL-- low HDLlow HDL
�� Guidelines from the NKF K/DOQI : Guidelines from the NKF K/DOQI : -- treat treat dyslipidemiadyslipidemia aggressively in CKD pts :aggressively in CKD pts :
with goals of with goals of LDL < 100 mg/LDL < 100 mg/dLdL ,,
and and TG < 200 mg /TG < 200 mg /dLdL
7/8/2009
45
HTNHTNHTN leads to direct damage to small blood vessels in HTN leads to direct damage to small blood vessels in the the nephronnephron, loss of regulation of GFR, & , loss of regulation of GFR, & proteinuriaproteinuria..
Several trials prove the benefit of BP control in slowing Several trials prove the benefit of BP control in slowing the progression of kidney disease. the progression of kidney disease.
ACEI s and ARBs ACEI s and ARBs preferentially lower preferentially lower intraglomerularintraglomerularpressure and reduce pressure and reduce proteinuriaproteinuria, and are more , and are more effective than other antihypertensive drugs in effective than other antihypertensive drugs in preventing the progression of kidney diseasepreventing the progression of kidney disease . .
HTNHTN
�� Guidelines: Guidelines: blood pressureblood pressure goal of goal of 130/80130/80 mm Hg is recommended in mm Hg is recommended in patients with normal urinary albumin patients with normal urinary albumin concentrations, and a blood pressure goal concentrations, and a blood pressure goal of of 125/75 mm Hg is recommended in 125/75 mm Hg is recommended in patients with proteinuriapatients with proteinuria equal to or equal to or greater than 1 g per 24 hours.greater than 1 g per 24 hours.
ACE / ARB treatment�� When starting ACEWhen starting ACE--inhibitor, CKD pts often have inhibitor, CKD pts often have
initial decrease in GFR (usually less than 10 mL per initial decrease in GFR (usually less than 10 mL per minute per 1.73 m2) minute per 1.73 m2) �� EXPECT a mild increase in EXPECT a mild increase in creatinine (less than 20creatinine (less than 20--30 % of baseline), and mild 30 % of baseline), and mild increase in K+increase in K+
�� Creatinine and potassium levels should be Creatinine and potassium levels should be monitored 1 to 2 weeks after the initiation of monitored 1 to 2 weeks after the initiation of therapy with ACE inhibitortherapy with ACE inhibitor——COMMON MISTAKE COMMON MISTAKE IS TO IS TO STOPSTOP THE ACE/ARB WHEN Cr increases THE ACE/ARB WHEN Cr increases by <= 30% ! by <= 30% !
�� DO NOT STOP DO NOT STOP �� RECHECK AGAIN IN 1RECHECK AGAIN IN 1--2 WKS2 WKS
7/8/2009
46
AnemiaAnemia
�� normocyticnormocytic , , normochromicnormochromic, , hypoproliferativehypoproliferative
�� due to due to lower erythropoietin production lower erythropoietin production by by the decreased # of functioning renal tubular the decreased # of functioning renal tubular cells.cells.
�� SxsSxs are of decreased quality of life: fatigue, are of decreased quality of life: fatigue, less exercise tolerance, lower immunity & less exercise tolerance, lower immunity & cognition, increased work on heart can lead to cognition, increased work on heart can lead to LVH & LVH & cardiomyopathycardiomyopathy..
AnemiaAnemia
�� correction of anemia correction of anemia maymay slow progression of slow progression of chronic kidney disease, possibly decrease chronic kidney disease, possibly decrease mortality. mortality.
�� NKF K/DOQI guidelines recommend : NKF K/DOQI guidelines recommend : --target hemoglobin concentration of 10 target hemoglobin concentration of 10 -- 12 12 --give Iron supplement if low give Iron supplement if low ferritinferritin(<100 (<100 ngng//mLmL) )
--give Erythropoietin to give Erythropoietin to predialysispredialysis pts w/ pts w/ anemiaanemia--dependent angina or severe dependent angina or severe anemia w/ anemia w/ HbHb <10 <10
Renal Renal OsteodystrophyOsteodystrophy�� In early CKD, In early CKD, hyperphosphatemiahyperphosphatemia leads to increased PTH leads to increased PTH
((secondary hyperparathyroidismsecondary hyperparathyroidism ), which causes ), which causes increased bone turnover, decreased cortical bone and increased bone turnover, decreased cortical bone and decreased bone strengthdecreased bone strength�� causing fracturescausing fractures
�� Can reduce hyperparathyroidism by Can reduce hyperparathyroidism by treating & preventing treating & preventing hyperphosphatemiahyperphosphatemia::
--restrict dietary phosphate intake (e.g., colas, nuts, restrict dietary phosphate intake (e.g., colas, nuts, peas, beans, dairy products)peas, beans, dairy products)--use phosphate bindersuse phosphate binders--vitamin D to suppress parathyroid hormone secretion.vitamin D to suppress parathyroid hormone secretion.
(some patients can have refractory hyperparathyroidism due to (some patients can have refractory hyperparathyroidism due to parathyroid gland hyperplasia, and may require surgical treatment)parathyroid gland hyperplasia, and may require surgical treatment)

7/8/2009
47
NutritionNutrition�� CKD pts are at risk for malnutrition and CKD pts are at risk for malnutrition and hypoalbuminemiahypoalbuminemia, ,
both of which may be associated with poor outcomes both of which may be associated with poor outcomes
�� Question/Subject of debate: Question/Subject of debate:
What amount of protein intake may reduce the risk of CKD What amount of protein intake may reduce the risk of CKD progression and also minimize risk of malnutrition? progression and also minimize risk of malnutrition?
..
NutritionNutrition�� NKF K/DOQI recommendation for preNKF K/DOQI recommendation for pre--dialysis dialysis
CKD: protein intake of 0.8 to 1.0 g per kg per day CKD: protein intake of 0.8 to 1.0 g per kg per day (controversial (controversial ----based on evidence from animal studiesbased on evidence from animal studies
and is NOT first line treatment plan )and is NOT first line treatment plan )
�� CKD pts, especially those requiring dialysis, CKD pts, especially those requiring dialysis, should have albumin and weight monitored, to should have albumin and weight monitored, to prevent malnutrition. prevent malnutrition.
�� CKD pts should be CKD pts should be referred to a nutritionist referred to a nutritionist for for recommendations on optimal protein and caloric recommendations on optimal protein and caloric intake intake
7/8/2009
48
Smoking cessationSmoking cessation
--CKD pts are at CKD pts are at high risk high risk for CV mortalityfor CV mortality
--Smoking is a strong Smoking is a strong ADDED CV disease ADDED CV disease risk factor risk factor
--Smoking is also strongly associated with the Smoking is also strongly associated with the progression of CKD progression of CKD
�� Guideline: Guideline: ( obvious!) ( obvious!)
Recommend and help with smoking cessation! Recommend and help with smoking cessation!
WHEN TO REFER to WHEN TO REFER to NEPHROLOGIST:NEPHROLOGIST:
�� Underlying cause unclear after basic workUnderlying cause unclear after basic work--upup�� Renal biopsy indicatedRenal biopsy indicated�� Management of underlying cause beyond the Management of underlying cause beyond the
scope of primary carescope of primary care�� Stage 3Stage 3 chronic kidney disease (GFR < 60 chronic kidney disease (GFR < 60 mLmL per per
minute per 1.73 m2): minute per 1.73 m2): considerconsider coco--managementmanagement�� Stage 4 chronic kidney disease (GFR < 30 Stage 4 chronic kidney disease (GFR < 30 mLmL per per
minute per 1.73 m2): minute per 1.73 m2): nephrologistnephrologist involvement involvement essentialessential
�� Rapid progression of chronic kidney diseaseRapid progression of chronic kidney disease�� Superimposed acute kidney failureSuperimposed acute kidney failure
7/8/2009
49
NATIONAL KIDNEY NATIONAL KIDNEY FOUNDATIONFOUNDATION
www.kidney.orgwww.kidney.orgGet to know the web site as a reference forGet to know the web site as a reference for
Guidelines and Patient EducationGuidelines and Patient Education
And use: And use: www. mdrd.comwww. mdrd.com
And … isn’t your MOUTH tired too?!
7/8/2009
50
1
4
3
5
2
Gynecology
Psychiatry
PediatricsNeurology
Cardiology
Geriatrics
Nephrology
Neurology





























