Embed Size (px)
Citation preview

American Journal of Medical Genetics 33:336-340 (1989)
Epiphyseal Dysplasia With Coxa Vara, Microcephaly, and Normal Intelligence in Sibs: Expanded Spectrum of LowryWood Syndrome? Lori G. Hankenson, Maer B. Ozonoff, and Suzanne B. Cassidy Department of Pediatrics, Division of Human Genetics, University of Connecticut School of Medicine, Farmington (L.G.H., S.B.C.) and Department of Radiology, Newington Children’s Hospital, Newington (M.B.O.), Connecticut
We report on a brother and sister with epiphy- seal dysplasia and coxa vara, microcephaly, and short stature. This constellation of find- ings is similar to that found in the Lowry- Wood syndrome (Epiphyseal dysplasia, mi- crocephaly, short stature, and mental re- tardation). In the sibs we describe, mental retardation is not apparent, and they have the additional finding of developmental coxa vara. Despite these 2 exceptions, this family prob- ably represents the same disorder described by Lowry and Wood (Clinical Genetics 8:269- 274,1975), and serves to expand the spectrum of the syndrome to include coxa vara. It is also possible that these sibs represent a previously undescribed syndrome, most likely with auto- soma1 recessive inheritance.
KEY WORDS: autosomal recessive inherit- ance, short stature, bone dys- plasia
INTRODUCTION Epiphyseal dysplasia is a nonspecific bony abnormality
which can be seen as an insolated entity [Amir et al., 19851 but has also been described as a part of both autosomal dominant (AD) and autosomal recessive (AR) syndromes: in conjunction with myopia and conductive deafness (AD) [Beighton et al., 19781; early-onset diabe- tes mellitus (AR) [Wolcott and Rollinson, 19721; and short stature, microcephaly, and mental retardation, the Lowry-Wood syndrome (AR) [Lowry and Wood, 1975;
Received for publication July 5, 1988; revision received January 27, 1989.
Address reprint requests to Suzanne B. Cassidy, Department of Pediatrics, Section of Genetics/Dysmorphology, University of Ari- zona Health Sciences Center, 1501 N. Campbell Ave., Tucson, AZ 85724.
0 1989 Alan R. Liss, Inc.
Nevin et al., 19861. Coxa vara is rarely described in association with isolated epiphyseal dysplasia.
We have seen 4 sibs, including a brother and sister who have epiphyseal dysplasia with coxa vara, microce- phaly, and short stature. This constellation of findings is similar to that found in the Lowry-Wood syndrome [Lowry and Wood, 19751 with the notable absence of mental retardation. Additionally, the presence of infan- tile (developmental) coxa vara has not been reported in patients with that disorder.
CLINICAL REPORT Patient 1
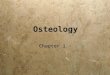
Y.R. is a boy born in Puerto Rico with birth weight of 3.10 kg and length of 48.3 cm (both 25th centile). In infancy he is reported to have had “hip problems,” for which he wore “special boots.” Adductor tenotomies were performed at age 3 to correct gait abnormalities. At age 4, radiographs documented bilateral epiphyseal dysplasia of the femoral heads and bilateral coxa vara (L>R) (Fig. 1A). Additional skeletal amomalies include bilateral pos- terior radial head dislocation with radial hypoplasia and partial fusion of the capitate and hamate bones. A right scoliosis of 17 degrees (supine) from T3 to L5 without congenital anomaly was present. The distal tibia1 and proximal humeral epiphyseal ossification centers were slightly flattened and deformed; the centers at the knee were normal. Bone age was normal.
Examination at 4 6/12 years (Fig. 1B,C) showed his height to be 97 cm ((5th centile), weight to be 12.9 kg ((5th centile), and head circumference (OFC) 47.5 cm (<2nd centile). Arm span was 87 cm and the upper:lower segment ratio was 1.33 (elevated for age). He had ob- viously short limbs, a pectus excavatum/pectus carina- tum, restricted supination of forearms, and imcomplete extension a t the elbows. Toes and fingers were short, and the 5th digit of each hand was especially short with an apparently short metacarpal (not evident radiographi- cally). Gena valga were present and both hips showed increased external rotation and limited internal rotation. The gait was stiff with outward rotation of both legs and feet. Cognitive and motor development were normal.

Expanded Lowry-Wood Syndrome 337
Fig. 1. Affected male. A: Pelvic radiographs. Please note bilateral coxa vara, irregular femoral metaphyseal border and small, irregular metaphyseal ossification centers. B, C: Photographs a t age 4 6/12: B: Front view. C: Side view. Please note disproportionately short limbs, abnormal hip position, lumbar lordosis, and pectus deformity.
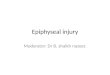
Patient 2 (10-25th centile) and length of 45.7 cm (5-10th centile). Motor and cognitive development were normal. Radio- graphic evaluation at age 3 (Fig. 2A) demonstrated bilat- eral femoral epiphyseal dysplasia (R>L) and bilateral
His sister, Yo.R., was seen at age 3 3/12; she had also been born in Puerto Rico with a birth weight of 2.8 kg

338 Hankenson et al.
coxa vara. There was no radial hypoplasia or dislocation. The proximal humeral ossification centers were unre- markable, but there was slight wedging of the distal tibia1 centers similar to that shown by her brother. Bone age was normal.
Examination a t age 3 years (Fig. 2B,C) showed her weight to be 11.4 kg ( 4 t h centile), height 88.9 cm (-6th
centile), and OFC 46.5 cm (<2nd centile). Her arm span was 82.5 cm and upper:lower segment ratio was 1.22 (above normal for age). She had a 5% decrease in supi- nation of the forearm bilaterally, bilateral gena valga, and abnormal hip rotation (minimal internal rotation and increased external rotation). Fingers and toes were short, and the fifth fingers were very short with appar-
Fig. 2 . Affected female. A: Pelvic radiographs. B,C: Photographs at age 3 years. B: Front view. C: Rear view. Findings are similar to those of the male, with the exception of absence of pectus deformity.

Expanded Lowry-Wood Syndrome 339
ently short metacarpals. Gait was somewhat waddling and stiff with increased lumbar lordosis; femora rotated externally.
Y.R.’s older brother, J.R., was diagnosed as having right congenital hip dislocation with acetabular “dyspla- sia” and was treated with casting at age 2; he also wore “leg braces.” Examination a t age 7 years was unremark- able with height at the 5th centile and normal OFC. Cognitive development was normal.
Y .R.’s youngest sister, L.R., had normal history, phys- ical examination, and cognitive development a t age 15 months. Hips were radiographically normal at age 9 months.
Vision and hearing were grossly normal in all children in this family; nystagmus was not present in any relative.
Y.R.’s mother, C.R., is 147.3 cm tall ( 6 t h centile), her OFC is 53 cm (20th centile), and her upper:lower segment ratio is 0.99 (normal). She has no bony abnormalities apparent on physical examination. Y.R.’s father, Ja.R. is 162.6 cm tall ((5th centile), his OFC is 55 cm (40th centile), and his upper:lower segment ratio is 1.06 (nor- mal). He reports that he suffered from “rickets” as a child and spent 4-5 months in the hospital in Puerto Rico at age 5. Radiographs as an adult showed normal pelvis and legs. He has a markedly short 5th metacarpal, but no other major bone abnormalities. He is partially blind secondary to meningitis as a child.
Mother has a brother with a stature less than 147 cm; there is no history of anyone with recognized bone ab- normalities. Paternal history is negative for short stature or recognized bone abnormalities. Both parents are of Puerto Rican ancestry; there is no known consanguinity.
DISCUSSION A boy and a girl in the family reported here have an
hereditary skeletal dysplasia consisting of femoral epi- physeal dysplasia with bilateral developmental coxa vara, microcephaly (OFC <2nd centile), and disproportionate short stature (upper:lower segment ratio >1.2). An older brother has a “dysplastic” right acetabulum. Acetabular “dysplasia” is an uncommon, but not unknown, finding in multiple epiphyseal dysplasia, although in this case it is a solitary finding and is likely to be a consequence of congenital hip dislocation. The father of the affected sibs has short stature and a vague history of skeletal problems as a child; the mother has short stature only. While the parents are both short, their upper:lower segment ratios are normal (approximately 1.0). Their short stature may be ethnic in origin since they are of Puerto Rican ances- try, although the possibility that it is a heterozygote manifestation cannot be ruled out.
Skeletal changes characteristic of epiphyseal dyspla- sias generally include irregularity and fragmentation of the epiphyseal ossification centers of the long bones. The hip is almost universally affected, particularly the femo- ral heads; the acetabulum is only secondarily involved. Affected individuals present with short stature, abnormal gait, short and broad digits, and early osteoarthritic changes.
Fairbanks [ 19471 reported multiple epiphyseal dyspla- sia with occasional associated coxa vara. Maudsley [ 19551
reported apparently heritable forms of multiple epiphy- seal dysplasia and suggested AD inheritance, again with coxa vara mentioned as only an incidental finding. Fa- milial cases of epiphyseal dysplasia associated with other abnormalities have been described. Both AD and AR disorders which include epiphyseal dysplasia have been reported [Amir et al., 1985; Beighton et al., 1978; Lowry and Wood, 1975; Nevin et al., 1986; Wolcott and Rollison, 19721. Lowry and Wood [1975] described two brothers with multiple epiphyseal dysplasia, short stature, micro- cephaly, and nystagmus, one of whom was mildly men- tally retarded. Nevin et al. [ 19861 subsequently reported a brother and sister with multiple epiphyseal dysplasia, short stature, and microcephaly, but no nystagmus; both were mildly mentally retarded. The disorder seen in these 2 families has been called Lowry-Wood syndrome by Nevin et al. [1986]; inheritance is presumed to be AR.
Coxa vara is a relatively rare orthopedic condition in which there is a decrease in the femoral neck-to-shaft angle to less than 110”, the normal angle ranging from 150” in the newborn to 125” in the adult and 120” in the aged [Pavlov et al., 19801. It is called “developmental” coxa vara when it is not present at birth but evolves within the first few years of life. Isolated coxa vara may be inherited as an AD disorder [Johanning, 19511; it has occasionally been noted in patients with epiphyseal dys- plasia. It has not previously been described in the re- ported families with Lowry-Wood syndrome.
The sibs described in this report are similar in several respects to the children in the 2 previously reported families with Lowry-Wood syndrome, including epiphy- seal dysplasia, disproportionate short stature, and micro- cephaly. The nystagmus reported by Lowry and Wood [ 19751 is not evident, nor is mental retardation or devel- opmental delay as of ages 3 and 4 years. These sibs have the previously unreported finding of coxa vara. The char- acteristics they exhibit overlap sufficiently with the Lowry-Wood syndrome that they most likely represent an additional family with that disorder. If so, then the spectrum of that condition should be expanded to include coxa vara. Mental retardation and nystagmus would not appear to be essential for diagnosis. If these affected children do not have the Lowry-Wood syndrome, then they have a previously unreported disorder, likely to also be an AR trait.
The consistency or inconsistency of coxa vara, mental retardation, and nystagmus in reports of other families with the findings described in this family may help to determine whether the presence of coxa vara distin- guishes their condition as a separate entity or expands the spectrum of manifestations seen in the Lowry-Wood syndrome.
ACKNOWLEDGMENTS
We gratefully acknowledge the secretarial assistance of Liesa LeConche.
REFERENCES Amir D, Mogle P, Weinberg H (1985): Multiple epiphyseal dysplasia in
one family. J Bone Joint Surg [Br] 67:809-813.

340 Hankenson et al.
Beighton P, Goldberg L, Op’t Hof J (1978): Dominant inheritance of multiple epiphyseal dysplasia, myopia and deafness. Clin Genet 14:173-177.
Fairbanks HAT (1947): Dysplasia epiphysialis multiplex. Br J Surg 34:225-232.
Johanning K (1951): Coxa vara infantum I. Clinical appearance and aetiological problems. Acta Orthop Scand 21:273-299.
Lowry RB, Wood BJ (1975): Syndrome of epiphyseal dysplasia, short stature, microcephaly and nystagmus. Clin Genet 8:269-274.
Maudsley RH (1955): Dysplasia epiphysialis multiplex. J Bone Joint Surg [Br] 37:228-240.
Nevin NC, Thomas PS, Hutchinson J (1986): Syndrome of short stature, microcephaly, mental retardation, and multiple epiphyseal dys- plasia - Lowry-Wood syndrome. Am J Med Genet 24:33-39.
Pavlov H, Goldman AB, Freiberger RH (1980): Infantile coxa vara. Radiology 135:631-640.
Wolcott CD, Rollinson ML (1972): Infancy-onset diabetes mellitus and multiple epiphyseal dysplasia. J Pediatr 80:292-297.