Embed Size (px)
Citation preview
Epidemiology of Psychosis
Chris Gale
Otago Registrar Training Group
Feb 2011.
Methodologies used.
● Population surveys.● General population.● High risk populations.● Screener and re-interview.
● Case records (raw or capture | release).● Comprehensive national records● Insurance and prescribing● Admission and outpatient
● Complications of psychosis.
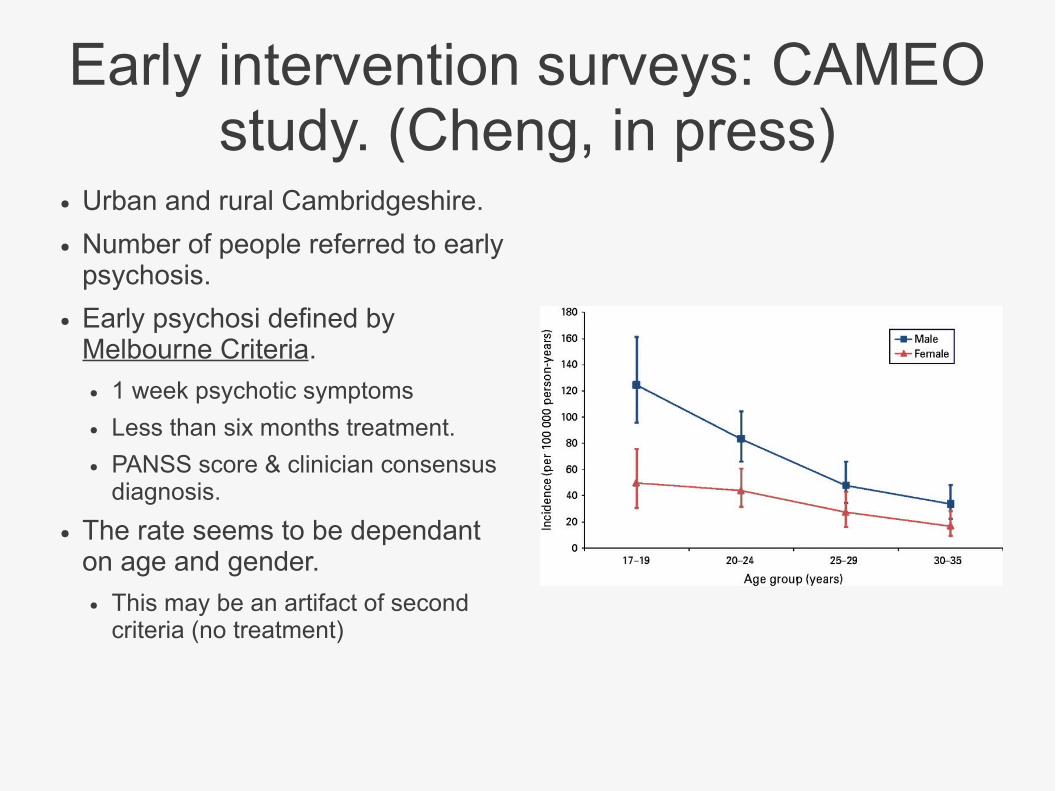
Early intervention surveys: CAMEO study. (Cheng, in press)
● Urban and rural Cambridgeshire.
● Number of people referred to early psychosis.
● Early psychosi defined by Melbourne Criteria.● 1 week psychotic symptoms
● Less than six months treatment.
● PANSS score & clinician consensus diagnosis.
● The rate seems to be dependant on age and gender.● This may be an artifact of second
criteria (no treatment)
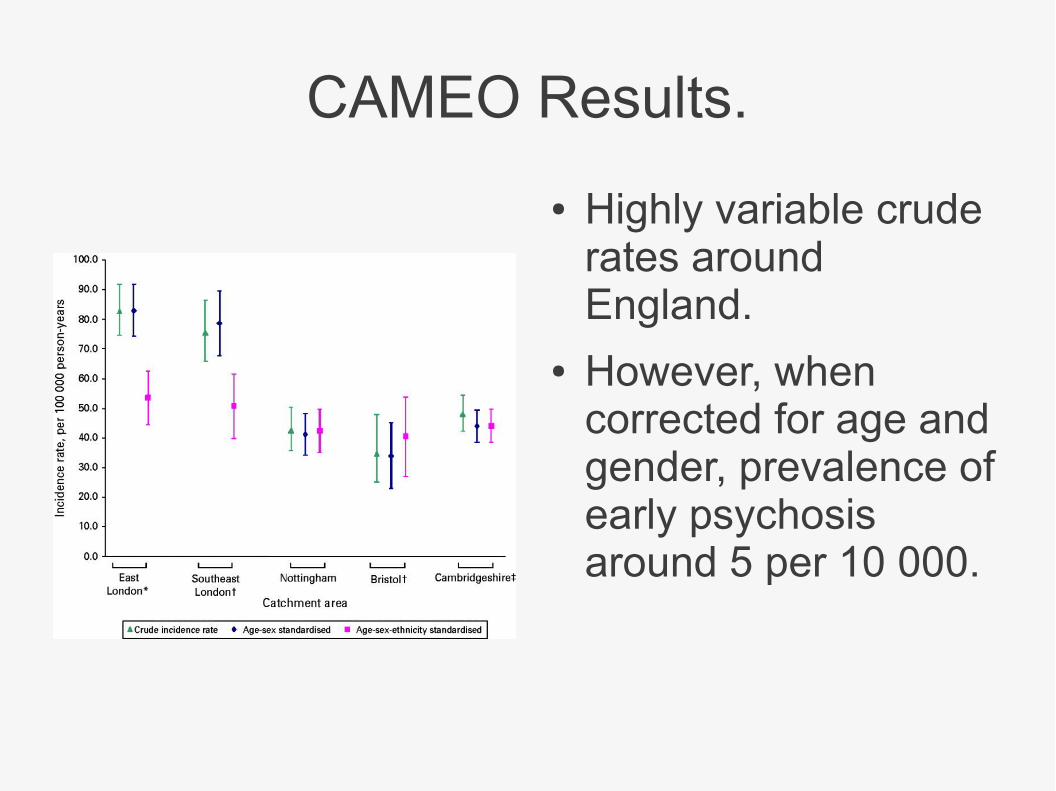
CAMEO Results.
● Highly variable crude rates around England.
● However, when corrected for age and gender, prevalence of early psychosis around 5 per 10 000.
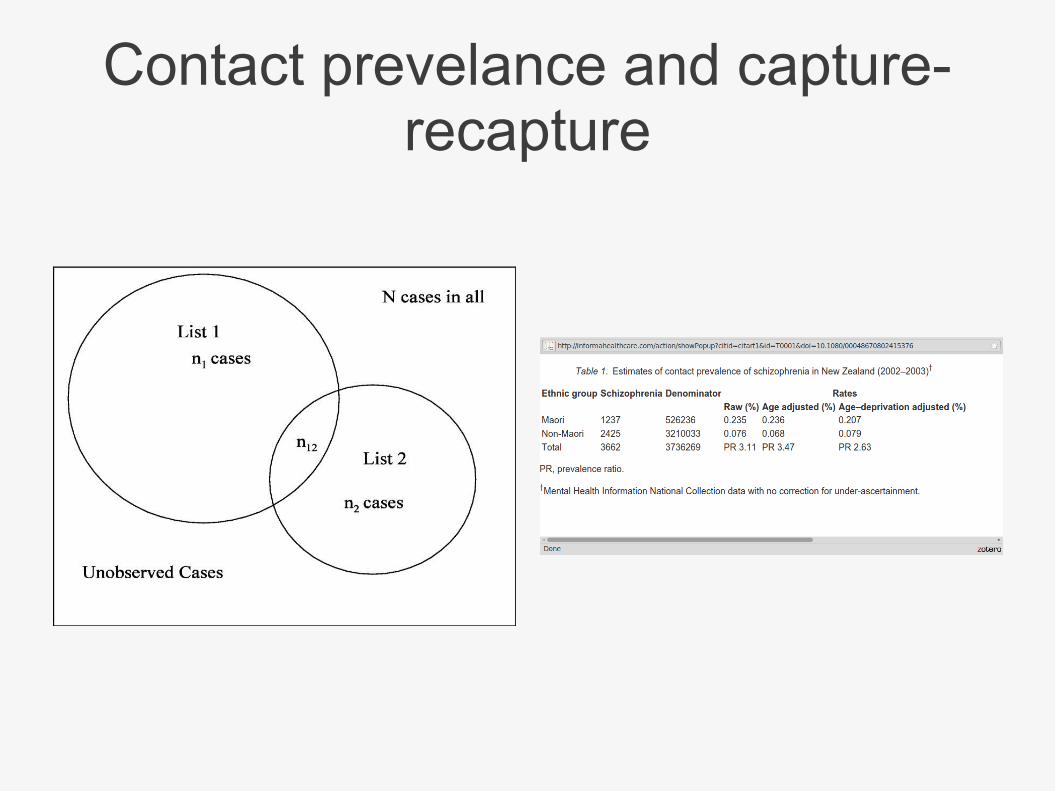
Contact prevelance and capture-recapture

Atypical Metabolic: 6 to 8 Weeks.
● The average weight gain after 6 to 8 weeks taking olanzapine was 5 to 6 kg,18, 26, which was significantly higher than the average weight gained while taking risperidone (4 kg) or haloperidol (3 kg).
● A significant increase in fasting and postprandial blood glucose levels and the incidence of diabetes The largest effects were seen for olanzapine, then risperidone and haloperidol.
● At 8 weeks, there was a significant increase in insulin level, insulin resistance, and glucose, cholesterol, triglyceride, and C peptide levels across clozapine, olanzapine, risperidone, and sulpiride combined but no significant difference between drugs.
Foley, Arch Gen Psychiatry, in press.

Atypical Metabolic: By 3 to 4 Months.
● Increase in cholesterol and fasting insulin levels was found after 3 to 4 months taking olanzapine in 1 study but not another.
● No significant increase was found in fasting triglyceride, glucose,or leptin levels
● A significant increase in absolute fat mass; percentage of body fat and waist to hip ratio, suggesting central deposition of body fat; and C peptide level while taking olanzapine.
Foley, Arch Gen Psychiatry, in press.
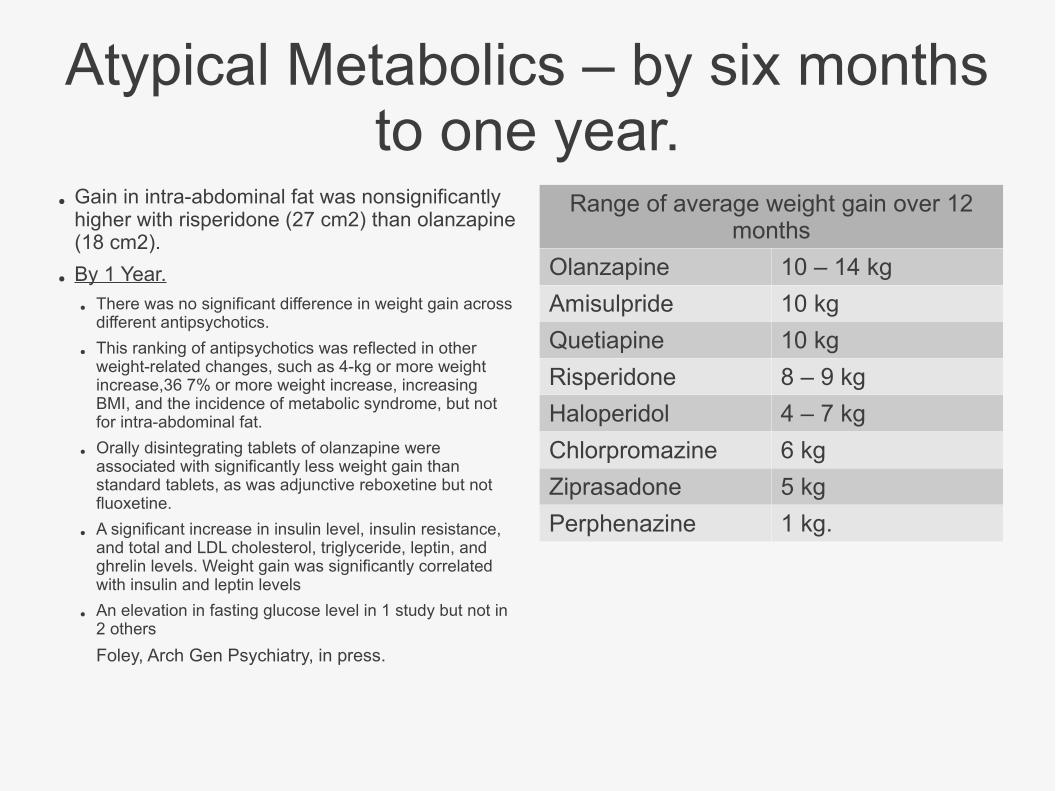
Atypical Metabolics – by six months to one year.
● Gain in intra-abdominal fat was nonsignificantly higher with risperidone (27 cm2) than olanzapine (18 cm2).
● By 1 Year.
● There was no significant difference in weight gain across different antipsychotics.
● This ranking of antipsychotics was reflected in other weight-related changes, such as 4-kg or more weight increase,36 7% or more weight increase, increasing BMI, and the incidence of metabolic syndrome, but not for intra-abdominal fat.
● Orally disintegrating tablets of olanzapine were associated with significantly less weight gain than standard tablets, as was adjunctive reboxetine but not fluoxetine.
● A significant increase in insulin level, insulin resistance, and total and LDL cholesterol, triglyceride, leptin, and ghrelin levels. Weight gain was significantly correlated with insulin and leptin levels
● An elevation in fasting glucose level in 1 study but not in 2 others
Foley, Arch Gen Psychiatry, in press.
Range of average weight gain over 12 months
Olanzapine 10 – 14 kg
Amisulpride 10 kg
Quetiapine 10 kg
Risperidone 8 – 9 kg
Haloperidol 4 – 7 kg
Chlorpromazine 6 kg
Ziprasadone 5 kg
Perphenazine 1 kg.
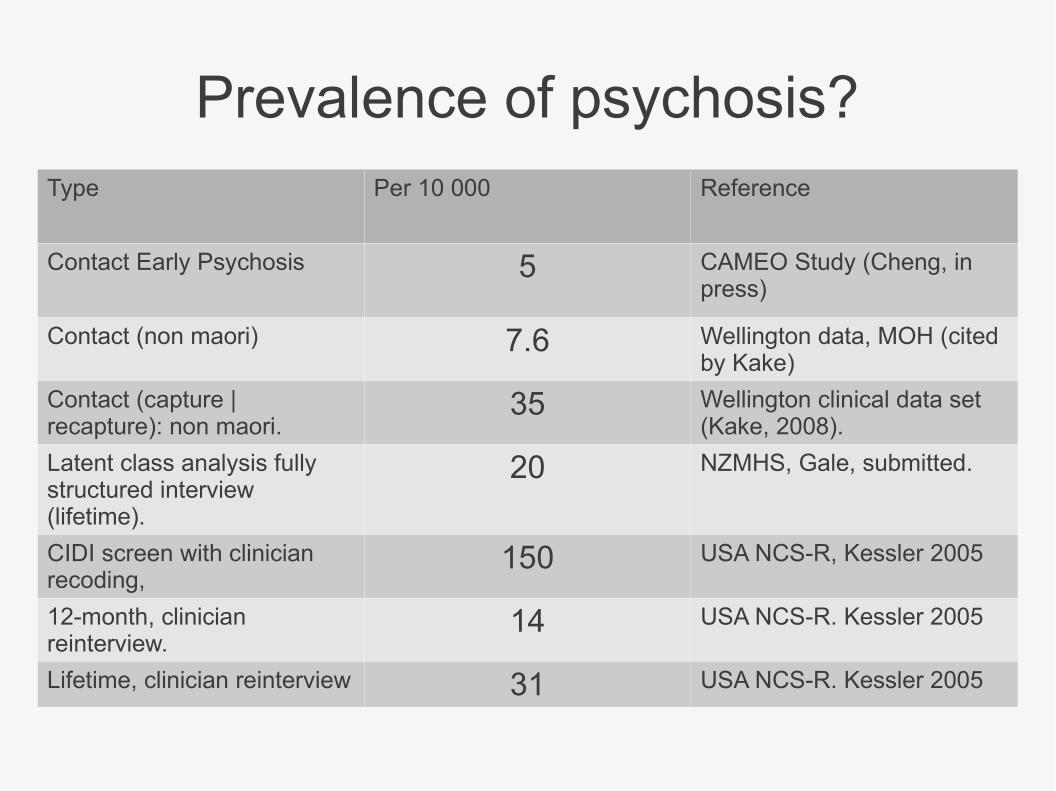
Prevalence of psychosis?Type Per 10 000 Reference
Contact Early Psychosis 5 CAMEO Study (Cheng, in press)
Contact (non maori) 7.6 Wellington data, MOH (cited by Kake)
Contact (capture | recapture): non maori.
35 Wellington clinical data set (Kake, 2008).
Latent class analysis fully structured interview (lifetime).
20 NZMHS, Gale, submitted.
CIDI screen with clinician recoding,
150 USA NCS-R, Kessler 2005
12-month, clinician reinterview.
14 USA NCS-R. Kessler 2005
Lifetime, clinician reinterview 31 USA NCS-R. Kessler 2005
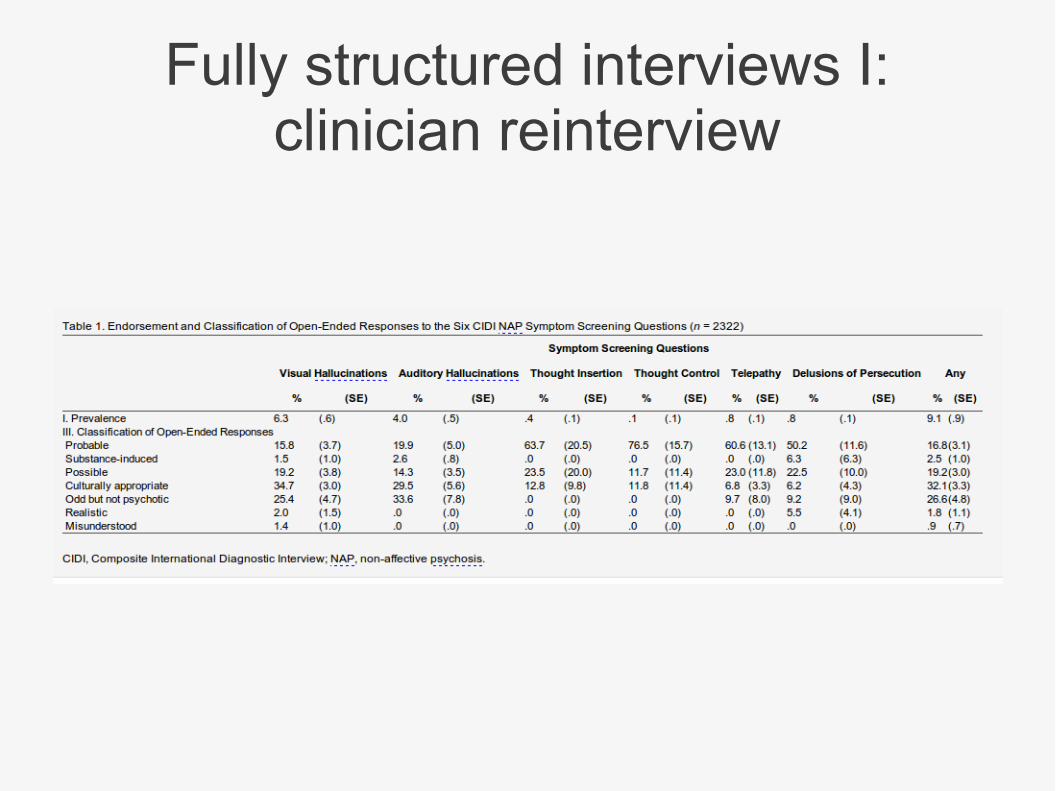
Fully structured interviews I: clinician reinterview
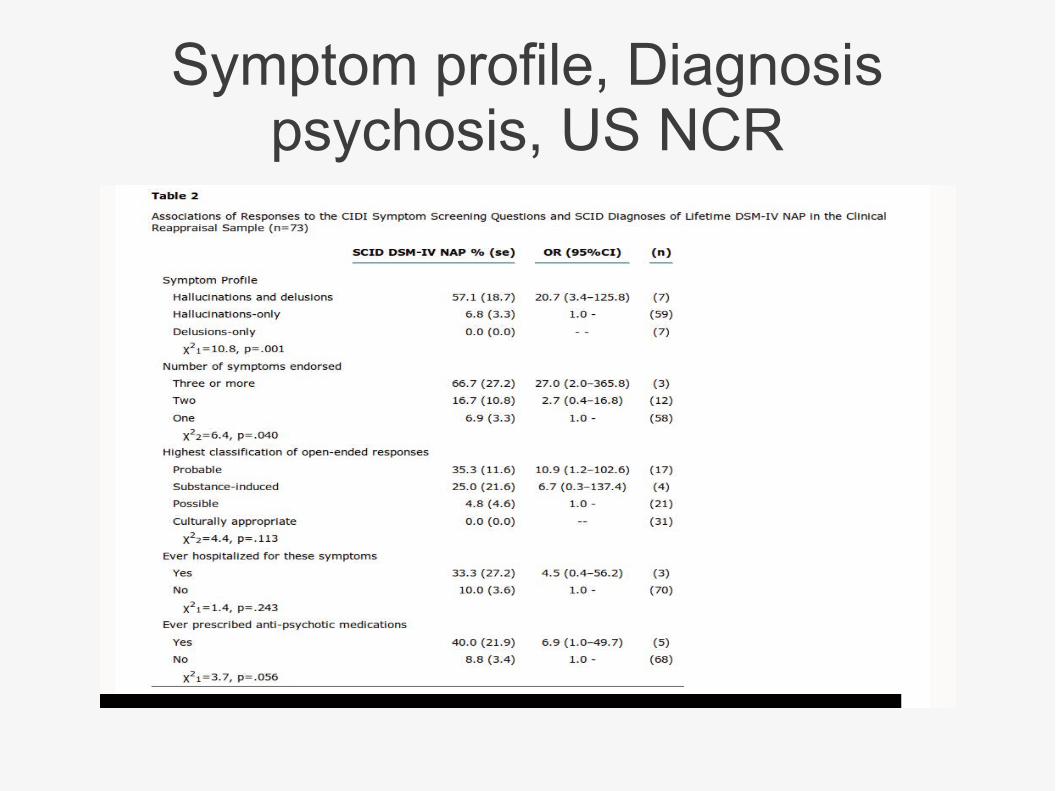
Symptom profile, Diagnosis psychosis, US NCR
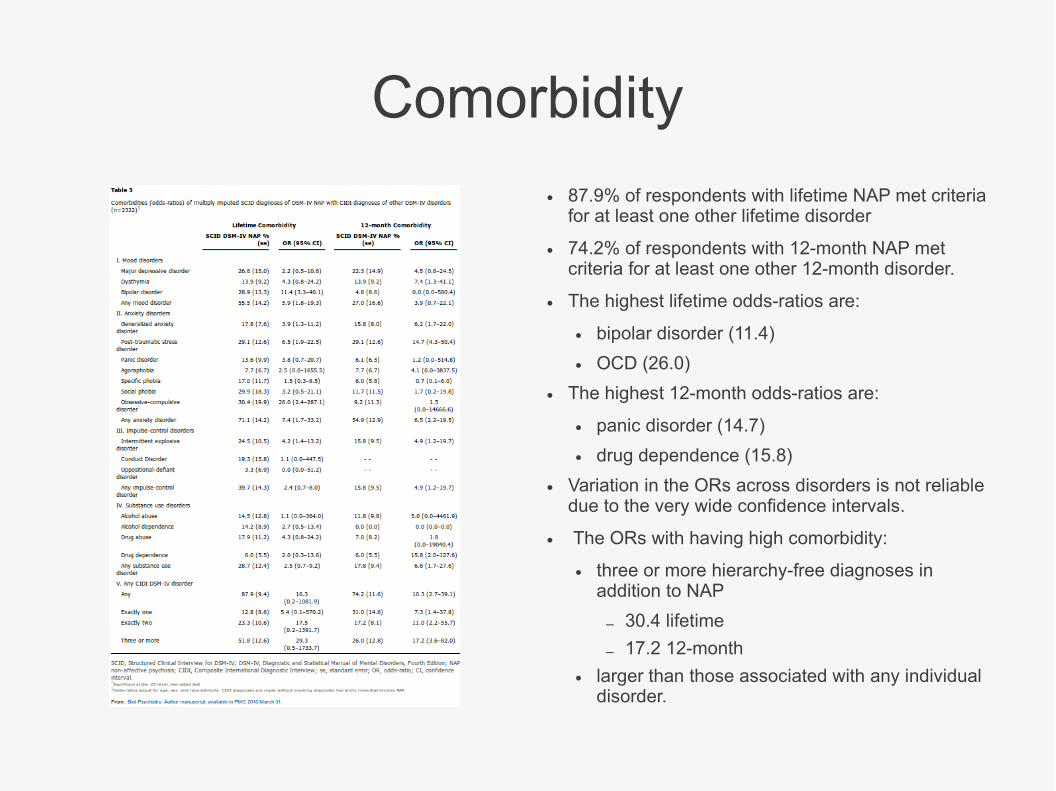
Comorbidity
● 87.9% of respondents with lifetime NAP met criteria for at least one other lifetime disorder
● 74.2% of respondents with 12-month NAP met criteria for at least one other 12-month disorder.
● The highest lifetime odds-ratios are:
● bipolar disorder (11.4)
● OCD (26.0)
● The highest 12-month odds-ratios are:
● panic disorder (14.7)
● drug dependence (15.8)
● Variation in the ORs across disorders is not reliable due to the very wide confidence intervals.
● The ORs with having high comorbidity:
● three or more hierarchy-free diagnoses in addition to NAP
– 30.4 lifetime
– 17.2 12-month
● larger than those associated with any individual disorder.
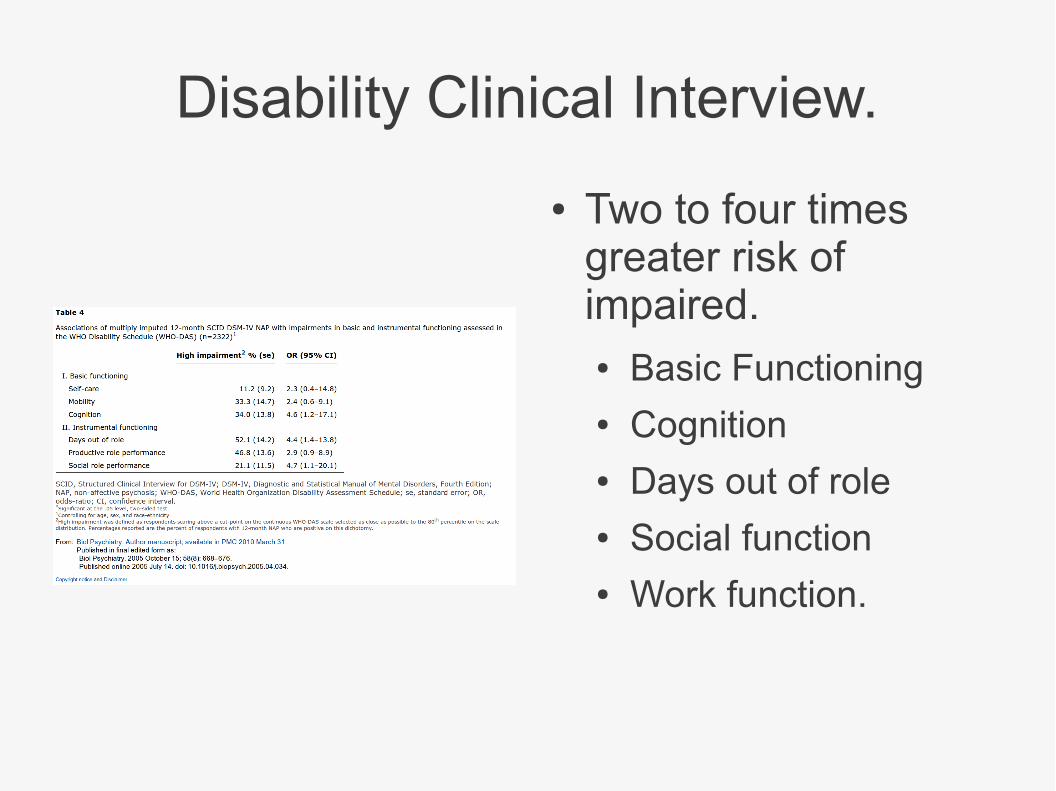
Disability Clinical Interview.
● Two to four times greater risk of impaired.● Basic Functioning● Cognition● Days out of role● Social function● Work function.
Clinician reinterview...
● Estimated rate non affective psychosis 15/1000 from structured interview → 3/1000 with structured clinical interview.
● Non significant correlation of clinician reassignment of screening question text with reinterview results.
● Delusions and Halluncinations most highly correlated with psychosis.
● BUT
● SCID modified to have first question same as screener in CIDI.
● Very expensive project, not replicated.
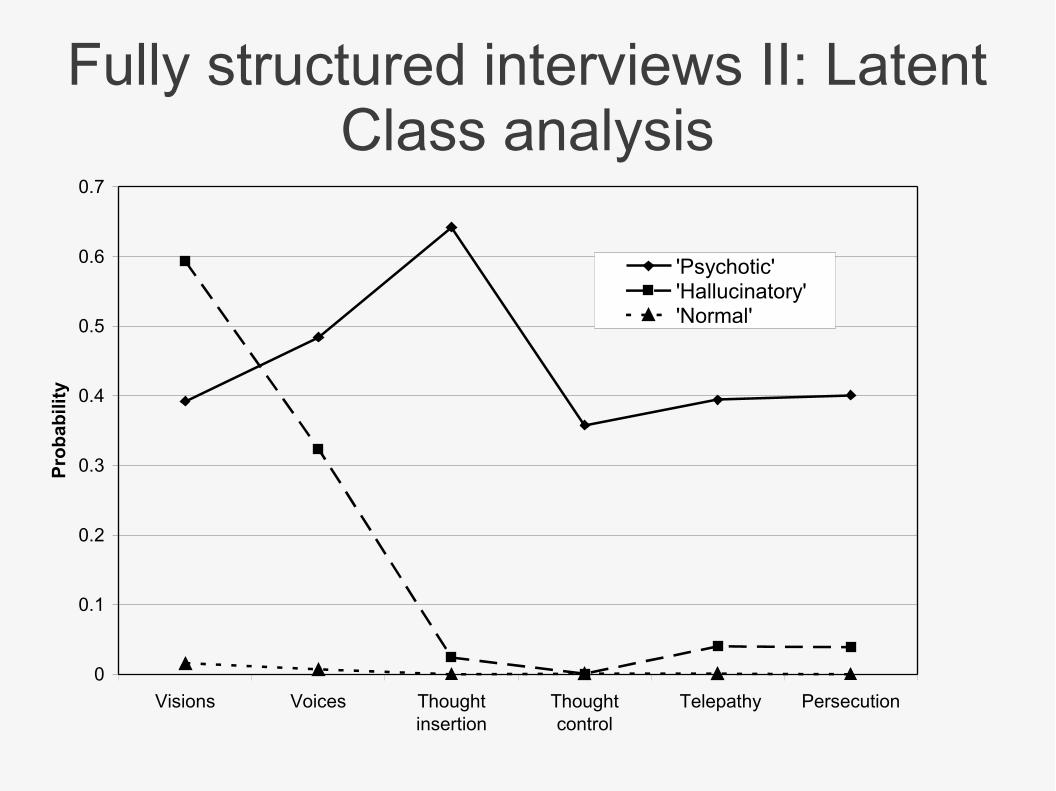
Fully structured interviews II: Latent Class analysis
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Visions Voices Thoughtinsertion
Thoughtcontrol
Telepathy Persecution
Pro
bab
ilit
y
'Psychotic''Hallucinatory''Normal'
Copyright restrictions may apply.
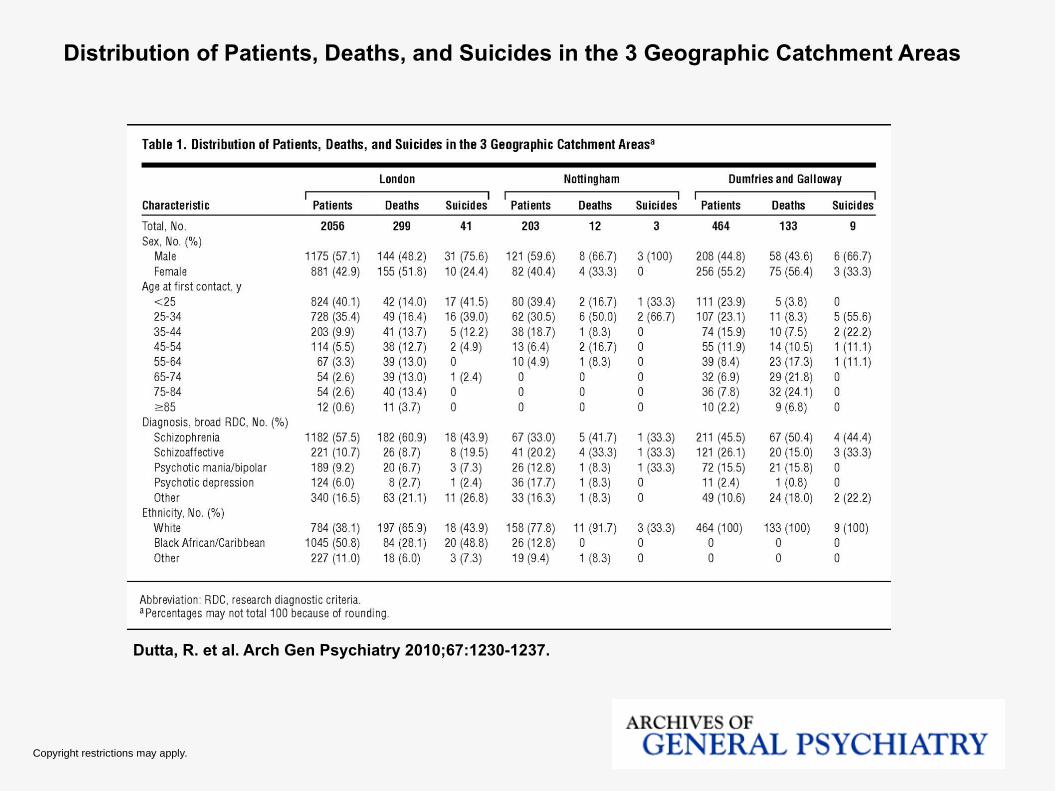
Dutta, R. et al. Arch Gen Psychiatry 2010;67:1230-1237.
Distribution of Patients, Deaths, and Suicides in the 3 Geographic Catchment Areas
Copyright restrictions may apply.
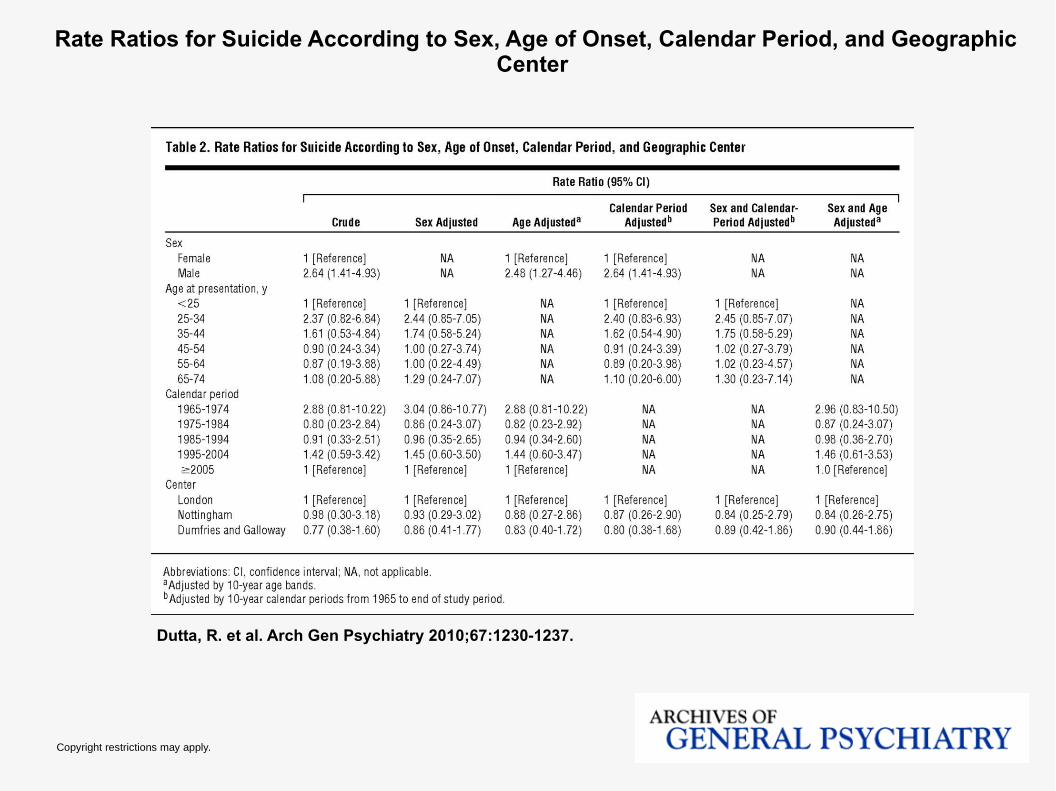
Dutta, R. et al. Arch Gen Psychiatry 2010;67:1230-1237.
Rate Ratios for Suicide According to Sex, Age of Onset, Calendar Period, and Geographic Center
References.● Cheng F, Kirkbride JB, Lennox BR, et al. Administrative incidence of psychosis assessed in an early
intervention service in England: first epidemiological evidence from a diverse, rural and urban setting. Psychol Med. 2010 Dec 23:1-10. [Epub ahead of print]
● Foley DL, Morley KI. Systematic Review of Early Cardiometabolic Outcomes of the First Treated Episode of Psychosis. Arch Gen Psychiatry. 2011 Feb 7. [Epub ahead of print
● Kake TR, Arnold R, Ellis P. Estimating the prevalence of schizophrenia among New Zealand Maori: a capture-recapture approach. Aust N Z J Psychiatry. 2008 Nov;42(11):941-9]





























