Embed Size (px)
Citation preview

Epidemiology of foodborne and emerging infectious diseases in Australia,
2014 to 2015 A thesis submitted for the degree of Master of Philosophy in Applied
Epidemiology (MAE) at the Australian National University
Fiona May
20 November 2015
Zoonoses, Foodborne and Emerging Infectious Diseases section (ZoFE)
Office of Health Protection Australian Government Department of Health
Funded by:
Australian Government Department of Health
Field Supervisor: Ben Polkinghorne NCEPH Supervisor: Emily Fearnley

2
Originality Statement ‘I hereby declare that this submission is my own work and to the best of my knowledge
it contains no materials previously published or written by another person, or
substantial proportions of material which have been accepted for the award of any
other degree or diploma at the Australian National University or any other educational
institution, except where due acknowledgment is made in the thesis. Any contribution
made to the research by others is explicitly acknowledged in the thesis. I also declare
that the intellectual content of this thesis is the product of my own work, except to the
extent that assistance from others in the project’s design and conception or in style,
presentation or linguistic expression is acknowledged’.
Signed ……………………………………………………………..
Date ………………………………………………………………...

3
Abstract My placement was with the Zoonoses, Foodborne and Emerging Infectious Diseases
section in the Office of Health Protection at the Australian Government Department of
Health during 2014-2015. I focused on the following five projects.
I described the epidemiology of bacterial toxin mediated foodborne outbreaks in
Australia and identified risk factors and risk groups, from an analysis of outbreak data
recorded from 2001 to 2013. The main risk factor for bacterial toxin mediated
foodborne outbreaks is temperature abuse (storage between 4°C and 60°C) of solid
masses of foods, such as lasagna. Residents of aged care facilities were the group at
highest risk of illness and death from bacterial toxin mediated foodborne outbreaks.
Few outbreaks were identified with food prepared at home.
As part of the national response to the large outbreak of Ebola virus disease (EVD) in
West Africa (2014-2015), a national surveillance system was established to enable
reporting and to provide information to jurisdictions to assist monitoring of travellers at
risk of contracting EVD. I conducted an evaluation of this system. The system was
considered useful and achieved its aims; however, a coordinated central, online
database would improve reporting and ease of use.
Culture independent diagnostic testing (CIDT) for bacterial causes of gastroenteritis is
becoming commonly used in pathology laboratories in Australia. These tests are rapid,
cheap and require less technical expertise than traditional culture based laboratory
tests. However, these tests do not provide the subtyping information required for public
health surveillance, including outbreak detection. For the time being, laboratories are
continuing culture in addition to CIDT. My project documents this transition in
Queensland.
In May 2014, three cases of bacteraemia caused by Ralstonia species were diagnosed
in South Australia. The only common exposure was propofol, a sedative. An
investigation into the cause of this cluster of cases was led by the Therapeutic Goods
Administration (TGA) as the agency responsible for the regulation of propofol.
Additional cases were identified from Queensland (four cases), and Victoria (one case).
I was part of the epidemiology team assisting and advising the TGA. The investigation
incorporated evidence from the case series, molecular analysis of isolates (including
whole genome sequencing), assessment of causal association and expert consultation
through the Delphi method. The cases of Ralstonia bacteraemia were determined to be
associated with at least two separate exposures. Cases in Queensland were linked to
contaminated bottled water, while cases in South Australia and Victoria were

4
associated with propofol. The mechanism of contamination of the propofol was unable
to be determined.
During a multi-jurisdictional investigation into an outbreak of hepatitis A associated with
consumption of frozen mixed berries in 2015, a national case control study was
conducted. I assisted OzFoodNet Queensland with interviewing controls and
conducted a sub-analysis of cases and controls from Queensland. Frozen mixed
berries were the only food exposure with a statistically significant association with
illness, supporting the implication of frozen mixed berries as the source of the outbreak,
as indicated by traceback and microbiological evidence.

5
Acknowledgements First and foremost, I’d like to thank my wonderful supervisors, Ben Polkinghorne (field)
and Emily Fearnley (academic). Without you guys, this thesis would not be as polished
as I hope it is. I know it got a bit tight towards the end there (I do not recommend
moving interstate within the month before Master of Philosophy in Applied
Epidemiology (MAE) thesis submission!), but we made it.
To the members of the Zoonoses, Foodborne and Emerging Infectious diseases
(ZoFE) section at the Department of Health – thanks for all your help and support over
the not quite two years (and for saying nice things about my cupcakes). Especially Tim
Sloan-Gardner, for your never ending patience for my never ending questions, Katrina
Knope for all your epi help, especially for Ebola, Leroy Trapani and Rachael Corvisy
(yes Rach, I know you aren’t technically ZoFE) for your friendship and many enjoyable
conversations about TV shows, and Amy Burroughs, who shares my first love of
viruses. Thanks also to all the other people I have had the pleasure of working with in
the Office of Health Protection. And thanks to the Department of Health for funding my
placement.
My fellow MAE14 cohort – we were all in this together, and it was great how supportive
everyone was. In particular, Anna-Lena Arnold, my Ralstonia and Chocolateria San
Churro buddy, who was only an instant message away. It was so great having you
nearby for chats about work and life in general!
Everyone else at the National Centre for Epidemiology and Population Health, I learned
so much from all of you. You all have different strengths as epidemiologists and that is
what makes the MAE program so well rounded. I’d like to thank Mahomed Patel in
particular, for teaching me so much during the Ralstonia investigation.
I’ve also been lucky enough to work closely with stakeholders from the Therapeutic
Goods Administration, OzFoodNet and laboratories in Queensland. Everyone was very
helpful and understanding of my status as epidemiologist-in-training.
And of course, I wouldn’t be here without my family. Mum, Dad, Al and Jason, and of
course the wonderful Lara and Lachy, and not to forget Bonnie. I’ve missed you all
while I’ve been in Canberra, but I’m very excited to be back in QLD, and hopefully not
leaving again for a while! And special thanks to Mum for helping me move to Canberra,
and then back again to Brisbane!

6
Table of Contents Originality Statement ................................................................................................. 2
Abstract ........................................................................................................................ 3
Acknowledgements ....................................................................................................... 5
Chapter 1 – Masters of Applied Epidemiology (MAE) experience ................................. 9
Summary of Core Competencies ............................................................................. 11
Chapter 2 – Epidemiology of bacterial toxin mediated foodborne gastroenteritis
outbreaks in Australia, 2001 to 2013 ........................................................................... 13
Table of contents ..................................................................................................... 14
Prologue .................................................................................................................. 16
Abstract ................................................................................................................... 18
Introduction ............................................................................................................. 19
Methods .................................................................................................................. 21
Results .................................................................................................................... 28
Discussion ............................................................................................................... 52
Conclusion .............................................................................................................. 59
Recommendations for the Outbreak Register .......................................................... 59
References .............................................................................................................. 61
Appendix 1: Data dictionary for Outbreak Register fields used ................................ 63
Appendix 2: Tables showing assessments of probable toxin types for suspected
outbreaks ................................................................................................................ 67
Appendix 3: Advanced draft of a paper for publication in Communicable Diseases
Intelligence .............................................................................................................. 73
Appendix 4: Conference presentation, Communicable Diseases Control Conference,
Brisbane 2 June 2015.............................................................................................. 96
Chapter 3 – Establishment and Evaluation of a National Surveillance System for Ebola
Virus Disease .............................................................................................................. 99
Table of contents ................................................................................................... 100
Prologue ................................................................................................................ 102
Abstract ................................................................................................................. 103
Introduction ........................................................................................................... 104
Aim and objectives ................................................................................................ 107

7
Design of surveillance system ............................................................................... 107
Results of national surveillance system ................................................................. 117
Evaluating the surveillance system........................................................................ 125
Discussion ............................................................................................................. 137
Summary of recommendations .............................................................................. 138
Conclusion ............................................................................................................ 139
References ............................................................................................................ 139
Appendix 1: Targeted literature review .................................................................. 142
Appendix 2: Data collection tool for laboratory testing and temperature monitoring148
Appendix 3: Case and contact report forms and data dictionaries ......................... 149
Appendix 4: List of questions for Stakeholders ...................................................... 212
Chapter 4 – The effect of culture independent diagnostic testing on the diagnosis and
reporting of enteric bacterial pathogens in Queensland, 2010 to 2014 ...................... 215
Table of contents ................................................................................................... 216
Prologue................................................................................................................ 217
Abstract ................................................................................................................. 218
Introduction ........................................................................................................... 220
Aim of study .......................................................................................................... 222
Methods ................................................................................................................ 222
Results .................................................................................................................. 225
Discussion ............................................................................................................. 247
References ............................................................................................................ 251
Appendix 1: Laboratory process questionnaire ...................................................... 253
Appendix 2: Data dictionary for analysis* .............................................................. 255
Chapter 5 – Cluster of cases with Ralstonia species bacteraemia potentially associated
with propofol administration ...................................................................................... 259
Table of contents ................................................................................................... 260
Prologue................................................................................................................ 262
Abstract ................................................................................................................. 265
Introduction ........................................................................................................... 266
Objectives ............................................................................................................. 268

8
Methods ................................................................................................................ 268
Results .................................................................................................................. 273
Discussion ............................................................................................................. 300
References ............................................................................................................ 304
Appendix 1: Targeted literature search and synthesis ........................................... 309
Appendix 2: Case report form ................................................................................ 312
Appendix 3: ProMED post requesting information about contamination of propofol317
Appendix 4: TGA testing ........................................................................................ 318
Chapter 6 – A case control study to determine the source of an outbreak of hepatitis A
in Queensland, 2015 ................................................................................................. 323
Table of contents ................................................................................................... 324
Prologue ................................................................................................................ 325
Abstract ................................................................................................................. 327
Introduction ........................................................................................................... 328
Methods ................................................................................................................ 329
Results .................................................................................................................. 331
Discussion ............................................................................................................. 336
References ............................................................................................................ 338
Appendix 1: Lay summary for OzFoodNet website ................................................ 340
Appendix 2: Case questionnaire ............................................................................ 343
Appendix 3: Control questionnaire ......................................................................... 355
Chapter 7 – Teaching experience ............................................................................. 367
Introduction ........................................................................................................... 368
Lessons from the Field .......................................................................................... 369
Lesson for first year MAE students – Measures of test performance ..................... 378

9
Chapter 1 – Masters of Applied Epidemiology (MAE) experience
I was placed within the Zoonoses, Foodborne and Emerging Infectious Diseases
(ZoFE) section in the Office of Health Protection at the Australian Government
Department of Health (Department of Health) in Canberra, Australian Capital Territory,
2014-2015. This was my first real foray into public health and epidemiology after a
career in academia, and I loved it. Being placed in the Department of Health, rather
than a jurisdictional health department, gave me a great overview of how public health
works in Australia. Now I’m looking forward to getting experience from the jurisdictional
side in my future career as an epidemiologist.
During my MAE I had the opportunity to participate in many activities in addition to the
core requirements of the MAE. I was able to attend Rapid Assessment Team (RAT)
and Monitoring and Investigation Team (MIT) meetings for the Australian Government
response to Ebola virus disease (EVD) in West Africa (2014), Middle Eastern
Respiratory Syndrome (MERS) in Korea (2015) and hepatitis A virus associated with
frozen berries in Australia (2015). Two of these responses (EVD in Chapter 3 and
hepatitis A in Chapter 6) formed the basis of two of my core MAE competencies.
My placement in Health also allowed me to be involved in the activities of the National
Incident Room (NIR). In addition to being part of the workforce for NIR activation for the
outbreak of hepatitis A associated with frozen berries (Chapter 6), I was also a Watch
Officer for the NIR. As part of this role, once or twice a month I would be responsible
for responding to any incidents reported through the health emergency phone number.
Incidents usually related to passenger exposures to an infectious disease on
international flights, such as measles and tuberculosis. Responding to incidents
required contacting the airline to obtain passenger manifests, contacting the Australian
Government Department of Immigration and Border Protection to obtain incoming
passenger cards, and sending information on the passengers exposed to their home
jurisdictional health department and international focal points if passengers were from
overseas. This behind the scenes experience was a valuable insight into what happens
in cross jurisdictional incidents.
Another valuable experience I had in my placement was being an associate editor for
Communicable Diseases Intelligence, the peer reviewed, Medline indexed journal
edited and published by members of ZoFE in association with an external editorial
advisory board. I had previously written and reviewed papers for journals, but had
never experienced the inner workings of a journal before. I also wrote the sections on

10
gastrointestinal diseases and zoonoses for the National Notifiable Diseases
Surveillance System 2013 Annual Report, to be published in Communicable Diseases
Intelligence.
Coming from academia, I had no idea about government committees and their
associated secretariats. During my placement I was able to attend meetings, both via
teleconference and face to face, of the Communicable Diseases Network Australia
(CDNA), OzFoodNet and the National Arboviruses and Malaria Advisory Committee
(NAMAC). NAMAC in particular appealed to me due to my previous experience in
arbovirus research. I was able to attend and present at a face to face meeting of
OzFoodNet held in Adelaide in June 2015. At this meeting I also actively participated in
the structured audit (debrief) for the hepatitis A outbreak – another new experience.
I was lucky enough to attend two different scientific meetings during my MAE. I
attended the 2015 Communicable Diseases Control Conference in, Brisbane. I
presented my study findings on bacterial toxin associated foodborne outbreaks
(Chapter 2) at this meeting. I also attended a symposium held in Melbourne about the
introduction of genomics into public health and epidemiology – “Embracing the
genomic revolution – applied microbial genomics in public health and clinical
microbiology”. As a molecular biologist moving into epidemiology, with experience in
next generation sequencing, this was of great interest to me.
My MAE experience has been a varied and wonderful introduction to epidemiology. I
look forward to my career in epidemiology, applying all I have learned during my two
years in Canberra, in my placement and through coursework at the Australian National
University.

11
Sum
mar
y of
Cor
e C
ompe
tenc
ies
MAE
com
pete
ncy
Cha
pter
2:
Bac
teria
l tox
in
med
iate
d fo
odbo
rne
outb
reak
s
Cha
pter
3:
Surv
eilla
nce
of
Ebol
a vi
rus
dise
ase
Cha
pter
4:
Cul
ture
in
depe
nden
t di
agno
stic
test
ing
in Q
ueen
slan
d
Cha
pter
5:
A cl
uste
r of c
ases
of
Ral
ston
ia
bact
erae
mia
Cha
pter
6:
An o
utbr
eak
of
hepa
titis
A
asso
ciat
ed w
ith
froz
en m
ixed
ber
ries
Cha
pter
7:
Teac
hing
Inve
stig
ate
an a
cute
pub
lic
heal
th p
robl
em
Anal
yse
a pu
blic
hea
lth d
atas
et
Eval
uate
a s
urve
illanc
e sy
stem
Des
ign
and
cond
uct a
n ep
idem
iolo
gica
l stu
dy
Lite
ratu
re re
view
Lay
repo
rt
Publ
icat
ion
Ora
l pre
sent
atio
n at
a s
cien
tific
co
nfer
ence
Less
ons
from
the
Fiel
d
Less
on fo
r 1st y
ear M
AE s
tude
nts

12

13
Chapter 2 Epidemiology of bacterial toxin mediated
foodborne gastroenteritis outbreaks in Australia, 2001 to 2013

14
Table of contents Prologue .................................................................................................................. 16
Study rationale ..................................................................................................... 16
My role ................................................................................................................. 16
Lessons learned .................................................................................................. 16
Public health implications of this work .................................................................. 17
Acknowledgements .............................................................................................. 17
Master of Philosophy (Applied Epidemiology) core activity requirement ............... 18
Abstract ................................................................................................................... 18
Introduction ............................................................................................................. 19
Methods .................................................................................................................. 21
Data collection and analysis ................................................................................. 21
Case definitions ................................................................................................ 21
Vehicle attribution ............................................................................................. 24
Other data cleaning .......................................................................................... 25
Data analysis .................................................................................................... 26
Results .................................................................................................................... 28
Descriptive epidemiology ..................................................................................... 28
Symptomology ..................................................................................................... 35
Food vehicle attribution ........................................................................................ 37
Contributing factors .............................................................................................. 40
Food preparation and consumption settings......................................................... 44
Further attribution of suspected aetiologies .......................................................... 50
Discussion ............................................................................................................... 52
Conclusion .............................................................................................................. 59
Recommendations for the Outbreak Register .......................................................... 59
References .............................................................................................................. 61
Appendix 1: Data dictionary for Outbreak Register fields used ................................ 63
Appendix 2: Tables showing assessments of probable toxin types for suspected
outbreaks ................................................................................................................ 67

15
Appendix 3: Advanced draft of a paper for publication in Communicable Diseases
Intelligence .............................................................................................................. 73
Appendix 4: Conference presentation, Communicable Diseases Control Conference,
Brisbane 2 June 2015 ............................................................................................. 96

16
Prologue
Study rationale Bacterial toxin mediated foodborne illnesses are a neglected cause of foodborne
illness. Unlike commonly reported foodborne bacterial pathogens, including Salmonella
and Campylobacter, the epidemiology of bacterial toxins have been less frequently
studied. A single study from the United States (US) focused exclusively on the
epidemiology of bacterial toxin mediated outbreaks in the US (1). Other studies (2, 3)
included bacterial toxin mediated outbreaks in an overall review of foodborne
outbreaks. Data on all foodborne outbreaks in Australia, including those confirmed or
suspected to have been caused by bacterial toxin producing bacteria are collated in the
Outbreak Register by OzFoodNet.
My role I developed (in consultation with my supervisors) and wrote the initial proposal for this
study. I cleaned and analysed the data, provided recommendations to improve the
Outbreak Register and presented my research findings to the national Communicable
Diseases Control Conference in Brisbane, 1-2 June 2015, and the 46th OzFoodNet
face to face meeting in Adelaide, 22-23 June 2015. I am also the first author on a
manuscript on this study submitted to Communicable Diseases Intelligence.
Lessons learned The most important lesson I learned during this study was that even if someone tells
you that the data is complete up to a certain date, check the data by year before you
start the work, and if the numbers look odd, chase it up! Also, Stata “do files” are a
lifesaver when you have to repeat all of the data analysis from the beginning. I learned
so much about using Stata during this analysis. It is such a powerful program, and the
community of Stata users online is very helpful.
Using the Outbreak Register taught me a lot about design of forms and databases. The
huge amount of recoding I had to do, both by hand in Excel and “automatically” through
Stata, made me really appreciate well designed questions with defined responses
rather than free text into which anything and everything could be entered.
Similarly, the symptom questions where “yes” was the only answer (no options for “no”
or missing or unknown) caused problems in recoding and determining the meanings of
the responses – questions should always have no and unknown options! Indeed,
calculating the percent of symptoms was not the simple matter I first thought it would
be. It seems obvious – number of people with the symptom divided by the total number

17
of people ill. However, these outbreaks are difficult to investigate, and often many
people are not interviewed individually. This problem has been acknowledged through
an extra question asking how many were interviewed about the symptom. But again,
this was not straightforward. Missing or inconsistent information (fewer people
interviewed than had the symptom) made this ostensibly simple calculation very
complicated.
Although I haven’t had the opportunity to enter data into the Register myself, through
using the data from the Access-based Register, and using NetEpi and EpiInfo for other
projects, I have gained a real appreciation of the fact that there are other, better options
for databases than Access. An online database would mean that jurisdictions could
enter data directly, rather than waiting to send it. The database would always be up to
date, instead of still missing some 2013 outbreaks in early 2015.
Although the OzFoodNet epidemiologists are always helpful, it took time to chase up
some missing or inconsistent information from the original source; information that
would hopefully have been entered correctly if entered immediately into a centrally
available database.
Public health implications of this work This study has provided OzFoodNet with information about the risk factors associated
with bacterial toxin mediated foodborne outbreaks. This information can be used in the
future to inform changes to public health policy to help prevent these outbreaks.
Suggestions for improvement of the Outbreak Register will result in a more streamlined
and useful tool.
Acknowledgements Big thanks go to my two supervisors, Dr Ben Polkinghorne and Dr Emily Fearnley. And
thanks also to all the members of OzFoodNet who have contributed the data over the
years. Thanks also to John Bates with whom I had a very informative chat about
laboratory testing methods for bacterial toxins.

18
Master of Philosophy (Applied Epidemiology) core activity requirement Analysis of a public health dataset such as surveillance data.
Literature review that demonstrates skills in conducting a targeted literature search and
synthesis.
Preparation of an advanced draft of a paper for publication in a national or international
peer-reviewed journal (Appendix 3).
Abstract and oral presentation of the project at a national or international scientific
conference (Appendix 4).
Abstract Foodborne outbreaks caused by bacterial toxins such as Clostridium perfringens,
Staphylococcus aureus and Bacillus cereus are an often overlooked cause of
morbidity. This study aimed to describe the epidemiology of bacterial toxin mediated
foodborne outbreaks in Australia between 2001 and 2013, and to identify high risk
groups and risk factors to inform prevention measures.
All foodborne and suspected foodborne outbreaks in Australia are collated in the
OzFoodNet Outbreak Register. Data on all confirmed or suspected bacterial toxin
mediated foodborne outbreaks notified to the register and investigated between 2001
and 2013 inclusive were included. Descriptive analyses were undertaken using
StataSE 13.
There were 272 confirmed or suspected toxin mediated outbreaks reported, of which
107 (39%) were laboratory confirmed. These outbreaks affected 4066 people, including
70 hospitalisations and 13 deaths, 12 of which occurred in aged care facility residents.
Clostridium perfringens was suspected or confirmed as the causative agent in 171
(63%) outbreaks. Commercial food service businesses (145 outbreaks, 53%) and aged
care facilities (99 outbreaks, 36%) were the most commonly reported settings for
outbreaks. Only seven outbreaks (3%) were associated with food prepared in private
residences. Inadequate temperature control of pre-cooked foods was reported as a
contributing factor in all confirmed and suspected toxin mediated outbreaks where this
information was available.
Bacterial toxin mediated foodborne outbreaks cause significant preventable morbidity
in Australia, and disproportionately affect residents of aged care facilities, a particularly
vulnerable population. Public health efforts aimed at improving storage and handling

19
practices for pre-cooked and re-heated foods could help to reduce the magnitude of
this problem.
Introduction While many studies have examined the epidemiology of outbreaks of pathogens such
as Salmonella, few have focused on bacterial toxin mediated outbreaks (1). Some
detailed analyses have included the bacterial toxin producers in larger studies of all
causes of gastroenteritis (3), although in these cases, due to the focus on more
common causes of gastroenteritis, such as Salmonella and norovirus, the description
of the epidemiology of the bacterial toxin mediated outbreaks can be less visible. All
infectious causes of gastroenteritis are underestimated in Australia as confirmation
requires at least some of those affected to submit a faecal specimen for testing. The
multiplication factor to account for underestimation depends on numerous factors
including severity of illness and ease of testing (4-6). Outbreaks caused by toxin
producing bacteria are often less severe and have a shorter duration than those
caused by other pathogens making sufferers even less likely to be tested (1). Testing
for bacterial toxin producing bacteria is difficult in both food and faecal samples, and is
only performed at a few laboratories in Australia (John Bates, personal
communication). A recent study estimating underreporting of gastroenteritis in Australia
estimated the multiplier for each of the three bacterial toxin mediated illness to be 104
(5).
Bacterial toxin mediated gastroenteritis can be caused by two different modes of
action. The preformed toxin is, as its name suggests, formed by the bacteria in the food
prior to consumption. Because the toxin has already been formed, onset of illness is
rapid and can be as little as 30 minutes. Vomiting is commonly associated with
intoxication caused by preformed toxin (7). Growth of the bacteria and the production of
toxin occurs before the cooking kill step, and the toxin itself is heat resistant (7, 8)
meaning further heating will not render the food safe to eat. Staphylococcus aureus
and Bacillus cereus can produce preformed toxins (9, 10). Foodborne disease caused
by a pre-formed B. cereus toxin is known as “emetic B. cereus” due to the predominant
symptoms of nausea and vomiting.
In contrast, the in vivo toxin is formed after consumption of contaminated food. The
incubation period of this form of intoxication is longer than that for preformed toxins, but
shorter than many other types of foodborne illness (which are in the order of several
days), and ranges from six to 16 hours (11, 12). Clostridium perfringens and B. cereus
cause this type of intoxication. Foodborne disease caused by in vivo B. cereus toxin is

20
known as “diarrhoeal B. cereus” due to the predominant symptoms of cramping and
watery diarrhoea. The bacteria grow rapidly in food held at ambient temperature (10-
54⁰C), and produce enterotoxin after ingestion (13). Although further cooking can kill
the vegetative cells, both bacteria can produce heat-resistant spores which can then
regerminate after cooking.
All three toxin producing bacteria are ubiquitous in the environment, and in the case of
S. aureus, is a normal component of human flora (14). A third type of foodborne toxin is
the neurotoxin produced by Clostridium botulinum. This toxin is formed in the food
before consumption and causes neurological illness (15). C. botulinum toxin is one of
the most poisonous biological substances known and as such botulism is listed on the
Australian National Notifiable Diseases List. However, few cases of C. botulinum are
reported in Australia, and although a single case of botulism can be considered an
“outbreak”, these single cases are reported via the National Notifiable Diseases
Surveillance System (NNDSS), and are not entered into the OzFoodNet Outbreak
Register and thus are not discussed further in this chapter.
In Australia, infection with S. aureus, B. cereus and C. perfringens are not notifiable
diseases, so cases of gastroenteritis due to these pathogens are only reported in the
OzFoodNet Outbreak Register as part of an outbreak, defined as two or more cases of
the same illness with a common source.
OzFoodNet began entering data into the Outbreak Register in 2001. The Register is a
Microsoft Access database maintained by OzFoodNet Central (located in the Australian
Government Department of Health). Jurisdiction-based OzFoodNet personnel are
responsible for entering the details of their outbreak investigations into their own
jurisdiction-specific Access database, and are required to transmit their data to
OzFoodNet Central quarterly. The Outbreak Register contains information about all
outbreaks of gastroenteritis and other outbreaks that are investigated by OzFoodNet. In
addition to foodborne outbreaks, this includes waterborne, animal-to-person, person-to-
person and environmental outbreaks. The data collected are diverse, and include
information about the illness, possible source, transmission, causes (distal, e.g.
process failures and proximate, e.g. aetiology), and information about the level of
evidence for these categories. Summaries of outbreaks are published in OzFoodNet
quarterly and annual reports, available in the publication Communicable Diseases
Intelligence.

21
The aim of this study was to describe the epidemiology of bacterial toxin mediated
foodborne outbreaks in Australia between 2001 and 2013, and to identify high risk
groups and risk factors to inform prevention measures.
Methods
Data collection and analysis All data were extracted from the Microsoft Access Outbreak Register into a Microsoft
Excel spreadsheet on 2 February 2015. At this date, data entry for outbreaks from
2001 to 2013 inclusive had been completed. Preliminary cleaning (application of
inclusion and exclusion criteria) was performed in Microsoft Excel, while further data
cleaning was performed in StataSE 13 (Stata Corp, College Station, TX, USA). Missing
data, nonsensical data and answers of “unknown” were treated as unknown responses.
Specific data cleaning steps are outlined below. All changes to the data were made on
the data extract only, but the extract and the data cleaning queries used were provided
to OzFoodNet at the end of the process. Completeness for all variables was defined as
useable data, i.e. values other than missing or unknown. A data dictionary for the
variables used in this analysis is included in Appendix 1.
Case definitions Bacterial toxin mediated foodborne or suspected foodborne outbreaks with onset
between 2001 and 2013 were included in the study. To retain only outbreaks caused
by, or suspected to be caused by bacterial toxins, all outbreaks confirmed or suspected
to be caused by a different aetiology were removed. The free text remarks field of all
outbreaks with an unknown aetiology were read and any outbreaks with a suspected
toxin mediated aetiology recorded in the remarks field, and not already recorded in the
aetiology field were entered into the aetiology field in the downloaded data. All
remaining outbreaks with an unknown aetiology were removed. A summary of this
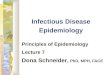
process is shown in Figure 1.

22
Figure 1: Flowchart showing inclusion categories

23
Six aetiology categories were created:
1. “Bacillus cereus” – B. cereus was listed as the sole aetiology
2. “Clostridium perfringens” – C. perfringens was listed as the sole aetiology
3. “Staphylococcus aureus” – S. aureus was listed as the sole aetiology
4. “Preformed toxin” – the aetiology was listed as preformed toxin, or both S.
aureus and B. cereus were listed as possible or confirmed aetiologies
5. “In vivo toxin” – both C. perfringens and B. cereus were listed as possible or
confirmed aetiologies
6. “Toxin” – a bacterial toxin was suspected but no further information was
provided in any field
The aetiology of outbreaks was further categorised as “confirmed” or “suspected”,
based on simplified US Centres for Disease Control and Prevention (CDC) guidelines
(16). In short, the aetiology of the outbreak was considered confirmed if the agent was
isolated or enterotoxin detected in clinical specimens from two or more cases, or at
least 105 organisms were isolated per gram of epidemiologically implicated food.
Suspected outbreaks were those where only a toxin or toxin producing bacteria were
isolated from only one case or at low levels in food, or where symptoms and food
vehicle indicated a toxin mediated aetiology to the investigators, leading to mention in
the remarks field.
The set of outbreaks with unknown aetiology that was removed above was reassessed
for outbreaks with an unknown aetiology that may have been unidentified toxin
mediated outbreaks. Only outbreaks with no known or suggested aetiology were
included in this dataset. The outbreaks with unknown aetiology and an incubation
period less than or equal to 18 hours were suspected to be toxin mediated due to the
short incubation period. These outbreaks were analysed as outbreaks of “unknown”
aetiology. Due to a paucity of information, these outbreaks were not included in most
analyses and were not categorised as above.

24
Vehicle attribution Investigators enter food vehicle information into a dedicated field in the Outbreak
Register database. However, sometimes the food is listed as unknown if the evidence
is weak. In these outbreaks, the suspected food may be entered into the free-text
remarks field. To maximise the amount of information available for food attribution, the
remarks field was examined and any food with a reasonable level of suspicion (i.e. the
only food eaten) was added to the food vehicle field in the downloaded data.
The suspected foods were grouped according to how they were prepared using the
categories proposed by Weingold et al (17). These categories are shown in Table 1.
The best estimate of category was used based on the information provided in the food
vehicle field. Only the information provided by the investigators was used and no
assumptions were made about complementary foods that were not specifically
mentioned, such as rice that is often, but not always, served with curries. Two
additional mutually exclusive food attribution variables were also created; one variable
was based on reporting of rice or noodles as implicated vehicles (yes or no), and the
other was based on the type of meat reported as an implicated vehicle (seafood,
poultry or meat).
The evidence obtained to implicate the food vehicle is entered in five different non-
mutually exclusive fields of the Outbreak Register (see Appendix 1). To create one
variable for analysis, the most robust level of evidence for each outbreak was
determined. The levels of evidence were ranked with laboratory evidence (isolation of
the pathogen from the food) as the highest level, followed by statistical evidence
(analytical study), then compelling descriptive evidence, other evidence and finally no
evidence.

25
Table 1: Description of food categories. Adapted from (17)
Category Description Example foods Foods eaten raw or lightly cooked
Foods that are served without being cooked at a temperature high enough to kill pathogens
Raw oysters, raw egg aioli
Cook/serve foods Limited and rapid (<30 min) preparation steps including a cooking step, at a high enough temperature to kill pathogens
Pizza, steak, chicken pieces, stir fry
Solid masses of potentially hazardous foods
Dense foods that are cooked and may be held hot for a time before serving
Lasagne, casseroles, rice
Roasted meat/poultry
Solid pieces of meat, roasted or baked (cooked >30 min)
Roast beef, whole chicken
Salads with one or more cooked ingredients
One or more of the ingredients in the salad is cooked prior to combining with the salad. Salad is then served cold
Pasta salad, chicken Caesar salad
Salads with raw ingredients
Salad with no cooked component Green salad, fresh tomatoes
Baked goods Baked or cooked, with some cold or hot holding. May be iced, filled etc.
Meat pies, cake, bread, icing
Sandwiches Hot or cold ingredients served between two pieces of bread or other baked goods. This category is selected if investigation suggests that contamination likely occurred during assembly or consumption of the sandwich
Hamburger, hot dog, panini, sandwich
Liquid or semi-solid mixtures of potentially hazardous foods
Combination of multiple ingredients before or during cooking, followed by hot holding and service
Sauce, soup, gravy
Beverages Liquid foods, with or without ice Soft drink, milk, alcohol Commercially processed foods
Food processed in a processing facility Pasteurised milk, precooked meat, canned fruit, ice cream
Multiple foods Multiple foods implicated, do not fit any other category
Buffet
Other Food does not fit any other category Unknown Food vehicle unknown
Other data cleaning Additional data cleaning steps included:
As specified in the data dictionary, for some variables a value containing 9s (i.e.
9, 99, 999, or sometimes 998) is the code for unknown answers. These
responses were recoded as unknown for this analysis.
Nonsensical values in all variables were recoded as unknown.
The setting in which the food was prepared is the most likely location for
contamination with toxin producing bacteria. The Outbreak Register has fields

26
for both the place the food vehicle was prepared (preparation setting) and the
place where the food vehicle was consumed (setting eaten). The data dictionary
recommends a “preparation setting” of “not applicable” only if the outbreak is
not foodborne or suspected foodborne. In outbreaks where the “preparation
setting” was listed as “not applicable”, “preparation setting” was replaced with
the value in “setting eaten” in order to allow analysis of the setting in which
contamination most likely occurred as it is likely that the food was prepared and
eaten in the same setting.
Data analysis Medians and ranges were calculated for all numerical variables including number of
cases, number of hospitalisations, number of deaths, median age, percentage of each
gender, median incubation period and duration and percentage for each symptom.
Since this is aggregated data, this means that the medians presented may be medians
of medians (for example, the median of median incubation periods).
Histograms were constructed in Microsoft Excel using outbreak data aggregated by
year based on onset date of the outbreak. Overall rates for each jurisdiction were
calculated using population data downloaded from the Australian Bureau of Statistics
(18), and compared using Poisson regression. A p-value less than 0.05 was
considered significant for all analyses.
Percent incidence of symptoms was calculated using the number of cases
reporting the illness as the numerator, and the number of cases interviewed
about the symptom as the denominator, with the exception of the following:
o For outbreaks where the number of cases reporting the symptoms was
higher than the number interviewed, the total number ill was used as the
denominator.
o Similarly, if the number of cases reporting a symptom had a value, but
the number of cases interviewed about the symptom was missing, the
total number ill was used as the denominator.
o If an outbreak had no information for any symptom, the percentage of
each symptom for this outbreak was recoded as missing.
Three different questions in the Outbreak Register were used to record the
factors that contributed to an outbreak; “major contaminating factors”, “factors
for microbial growth” and “factors for microbial survival”. The category “major
contaminating factors” refers to the factor that led to contamination of the food
vehicle, and thus to the outbreak. “Factors for bacterial growth” refers to how

27
the pathogen grew in the food after contamination, and “factors for microbial
survival” refers to how the pathogen survived food preparation procedures
(such as cooking) to be consumed by the case. For all three categories of
contributing factor, two different options can be selected, potentially resulting in
percentages adding up to more than 100%. “Unknown” was only used for
outbreaks where no other option was selected.
To assess the role of temperature abuse on growth of the bacteria and
production of toxin, the number of outbreaks that reported at least one growth
factor involving temperature abuse was calculated. These growth factors were:
o delay between preparation and consumption
o foods left at room or warm temperature
o inadequate refrigeration
o slow cooling
o inadequate thawing
o insufficient cooking
To assess the role of temperature abuse on survival of the bacteria and toxin,
the number of outbreaks that reported at least one survival factor involving
temperature abuse was calculated. These survival factors were:
o inadequate thawing and cooking
o insufficient time or temperature during reheating
o insufficient time or temperature during cooking
The number of outbreaks where the food was prepared in a food service setting
(“food service business”) was calculated using those outbreaks where
“preparation setting” was listed as:
o restaurant
o commercial caterer
o fair/festival/mobile service
o take-away
o grocery store/delicatessen
Outbreaks involving aged care facilities were analysed by calculating the
number of outbreaks where “preparation setting” and/or “setting eaten” was
aged care.
For further attribution of B. cereus and other suspected outbreaks, the following
criteria were used for probable case definitions:
o Emetic B. cereus
incubation period ≤ 6 hours
≥ 50% of cases reporting vomiting

28
o Diarrhoeal B. cereus
incubation period ≥ 6 hours
< 50% of cases reporting vomiting
o Preformed toxin
incubation period ≤ 6 hours
≥ 50% of cases reporting vomiting
if incubation period is < 2 hour, and the suspected food vehicle
includes rice, classify as probable emetic B. cereus
o In vivo toxin
incubation period ≥ 6 hours
< 50% of cases reporting vomiting
Results
Descriptive epidemiology A summary of the epidemiology of bacterial toxin mediated foodborne outbreaks in
Australia is shown in Figure 2 and Table 2. A total of 272 outbreaks were confirmed or
suspected to have been caused by a bacterial toxin producing pathogen. Of these, 107
(39%) were laboratory confirmed. A single case was positive for a toxin producing
bacteria in 28 (17%) of the suspected outbreaks. The remaining 137 outbreaks were
considered suspected toxin mediated outbreaks based on investigator suspicion. A
total of 4066 people were ill as a result of bacterial toxin outbreaks, of which 2219
(55%) cases were within laboratory confirmed outbreaks. A total of 13 deaths were
reported during laboratory confirmed outbreaks, 12 (92%) within aged care facilities.
Not all outbreaks had data entered for the number of hospitalisations, number of
deaths, number at risk (used to calculate percent ill), median age or median per cent of
each sex. The symbols in Table 2 represent completeness of each variable, as shown
in the footnote.
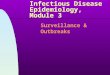
The frequency of outbreaks by year is shown in Figure 3, and a breakdown of the
number of outbreaks per state is shown in Figure 4. An additional 180 outbreaks were
identified as possible toxin mediated outbreaks with unknown aetiology, based on an
incubation period of 18 hours or less. These outbreaks are included for comparison in
Figure 3. There is no obvious trend over time for any of the categories of toxin
mediated outbreaks, although in 2005, 2010 and 2011 more outbreaks were reported
in all categories (Figure 3). The rate of bacterial toxin mediated outbreaks per one
million people reported per jurisdiction is shown in Table 3. If the rates for the

29
jurisdictions with 50 or more outbreaks reported are compared, Victoria (VIC) reported
2.5 times as many bacterial toxin mediated outbreaks than New South Wales (NSW),
and 2 times as many outbreaks as Queensland (QLD) (both comparisons significant
with p-values <0.001).
Figure 2: Flow chart showing inclusion criteria for this study. The number of outbreaks
remaining at each step is shown in brackets.

30
Table 2: Epidemiology of bacterial toxin mediated foodborne outbreaks in Australia, 2001 –
2013
Confirmed Suspected All Number of outbreaks 107 165 272 Total number of cases 2219 1847 4066 Number of cases per outbreak, median (range) 12.0 (2-272) 8.0 (2-125) 9.0 (2-272)
Hospitalisations 47† 23* 70* Deaths 13* 0* 13* Percent of outbreaks associated with one or more deaths
5.7* 0* 2.2*
Ill median percent (range) 20.4 (0.7-100)† 18.2 (2.2-100) ‡ 19.1 (0.7-100) † Age median 63.5† 43.5‡ 52.5†
Sex median percent
Male 37.0† 42.0† 40.0† Female 63.0† 58.0† 60.0†
* ≥90% complete † 75 – 89% complete ‡ 50 – 74% complete
Figure 3: Confirmed and suspected bacterial toxin mediated outbreaks, and outbreaks with an
unknown aetiology and incubation period of 18 hours or less, by year, Australia, 2001 to 2013
0
10
20
30
40
50
Num
ber o
f out
brea
ks
Year of onset
UnknownSuspectedConfirmed

31
Figure 4: Distribution of confirmed and suspected bacterial toxin mediated foodborne outbreaks
by jurisdiction and year, Australia 2001-2013. ACT – Australian Capital Territory; NSW – New
South Wales; NT – Northern Territory; QLD – Queensland; SA – South Australia; TAS –
Tasmania; VIC – Victoria; WA – Western Australia
Table 3: Rate of bacterial toxin mediated outbreaks reported per million people for each
Australian jurisdiction, 2001 to 2013
Jurisdiction* Number of outbreaks
Rate per 1 million people
Incidence rate ratio
95% Confidence Interval p-value
ACT 5 1.11 0.61 0.25 – 1.48 0.27 NSW 67 0.75 0.41 0.30 – 0.55 <0.001 NT 2 0.71 0.39 0.10 – 1.56 0.18
QLD 50 0.93 0.51 0.37 – 0.71 <0.001 SA 4 0.19 0.11 0.04 – 0.29 <0.001
TAS 1 0.16 0.08 0.01 – 0.61 0.014 VIC 124 1.83 reference reference reference WA 19 0.68 0.37 0.23 – 0.60 <0.001
* ACT – Australian Capital Territory; NSW – New South Wales; NT – Northern Territory; QLD – Queensland; SA – South Australia; TAS – Tasmania; VIC – Victoria; WA – Western Australia
Table 4 shows the general epidemiology of bacterial toxin mediated outbreaks,
separated into aetiology categories. Of the laboratory confirmed outbreaks, 76% were
caused by C. perfringens, 15% were caused by S. aureus and 6% were caused by B.
cereus. Only outbreaks associated with S. aureus had more confirmed outbreaks than
suspected (70% confirmed). Outbreaks associated with confirmed S. aureus infection
had fewer cases on average than outbreaks caused by other confirmed aetiologies.
0
5
10
15
20
25
30
35
40
45
Num
ber o
f out
brea
ks
Year of onset
WA VICTAS SAQLD NTNSW ACT

32
Almost all deaths (92%) were associated with confirmed C. perfringens outbreaks.
Completeness of the data was variable, with some fields having less than 50% useable
answers (not unknown). In Figure 5, the frequency of outbreaks each year is divided
into aetiology and confirmation status.

33
Tabl
e 4:
Epi
dem
iolo
gy o
f bac
teria
l tox
in m
edia
ted
outb
reak
s, b
y co
nfirm
ed o
r sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed
toxi
n In
viv
o to
xin
Toxi
n
Num
ber o
f out
brea
ks
Con
firm
ed
16
6 81
2
2 -
Susp
ecte
d 7
11
90
14
10
33
Tota
l num
ber o
f ca
ses
Con
firm
ed
200
114
1533
28
8 84
-
Susp
ecte
d 40
72
11
95
84
122
334
Num
ber o
f cas
es p
er
outb
reak
med
ian
(ran
ge)
Con
firm
ed
8 (2
-38)
18
(3-3
7)
13 (2
-100
) 14
4 (1
6-27
2)
42 (9
-75)
-
Susp
ecte
d 5
(3-1
0)
6 (2
-14)
9
(2-7
5)
5 (2
-14)
12
(3-2
8)
5 (2
-125
)
Hos
pita
lisat
ions
C
onfir
med
18
† 0*
14
† 15
* 0*
-
Susp
ecte
d 0*
3*
10
* 10
* 0*
0*
Dea
ths
Con
firm
ed
1*
0*
12*
0*
0*
- Su
spec
ted
0*
0*
0*
0*
0*
0*
Perc
ent o
f out
brea
ks
with
one
or m
ore
deat
hs
Con
firm
ed
6.3*
0*
6.
2*
0*
0*
-
Susp
ecte
d 0*
0*
0*
0*
0*
0*
Perc
ent i
ll m
edia
n (r
ange
) C
onfir
med
48
(13.
3-88
.9)‡
26 (1
4.8-
32.0
)‡ 19
(0.7
-100
)† 8
(8.4
)‡ 52
(4.1
-100
)*
- Su
spec
ted
56 (2
.2-7
5.0)
§ 56
(5.5
-100
)§ 10
(2.5
-88.
9)†
17 (4
.4-1
00)‡
51 (1
2.6-
100)
* 43
(2.7
-100
)‡
Age
med
ian
Con
firm
ed
31†
36‡
81†
39*
20‡
- Su
spec
ted
36*
31§
82†
39†
30‡
29‡
Sex
med
ian
perc
ent
Mal
e C
onfir
med
39
† 41
‡ 34
† 0§
50‡
- Su
spec
ted
40*
43§
40‡
29†
47†
50†
Fem
ale
Con
firm
ed
62†
59‡
66†
0§ 50
‡ -
Susp
ecte
d 60
* 57
§ 58
‡ 71
† 53
† 50
† * ≥
90%
com
plet
e
† 75
– 89
% c
ompl
ete
‡ 50
– 7
4% c
ompl
ete
§ <
49%
com
plet
e

34
Figu
re 5
: Con
firm
ed a
nd s
uspe
cted
bac
teria
l tox
in m
edia
ted
food
born
e ou
tbre
aks,
by
aetio
logy
and
yea
r, Au
stra
lia 2
001-
2013

35
Symptomology Table 5 shows information about the illness caused by the different toxin producing
bacteria. Similar to the general epidemiology variables, completeness was variable.
S. aureus outbreaks had the shortest median incubation period (3 hours for confirmed
outbreaks, 6 hours for suspected outbreaks) and C. perfringens outbreaks had the
longest (12 hours for both confirmed and suspected outbreaks). The median incubation
period for B. cereus was 8.5 hours. Duration of illness was comparable between
pathogen groups, although both confirmed and suspected S. aureus outbreaks had a
shorter median than the other categories.
Diarrhoea was the most commonly reported symptom in all outbreaks. Vomiting and
nausea were most common in outbreaks associated with S. aureus and in the
preformed toxin category. Fever, bloody diarrhoea, reverse temperature and joint and
muscle pain were infrequently reported. Numbness and tingling, itching, and rash were
not reported in any outbreaks.

36
Tabl
e 5:
Incu
batio
n pe
riod,
dur
atio
n of
illn
ess
and
med
ian
perc
ent o
f sym
ptom
s in
bac
teria
l tox
in m
edia
ted
food
born
e ou
tbre
aks
by c
onfir
med
or s
uspe
cted
aetio
logy
, Aus
tralia
200
1-20
13
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n To
xin
Incu
batio
n pe
riod
hour
s (r
ange
) C
onfir
med
3
(2-7
)*
8.5
(2-1
2)*
12 (6
-17)
± 4
(2-6
)*
12 (1
2-12
)‡ -
Susp
ecte
d 6
(2-8
)*
10 (2
-31)
† 12
(6-5
76)±
4 (1
-15)
* 12
(11-
22)*
8
(1-1
6)†
Dur
atio
n of
illn
ess
hour
s (r
ange
) C
onfir
med
18
(3-7
2)‡
23.5
(0-4
8)‡
24 (3
-204
)† 24
(24-
24)‡
36 (2
4-48
)*
- Su
spec
ted
18 (9
-96)
† 24
(2-4
8)†
24 (4
-300
)† 19
(2-3
9)*
27 (1
0-45
)† 24
(6-7
2)†
Dia
rrho
ea %
(r
ange
) C
onfir
med
82
(0-1
00)†
97 (0
-100
)*
100
(53-
100)
* 86
(72-
100)
* 10
0 (1
00-1
00)*
-
Susp
ecte
d 75
(56-
100)
* 10
0 (3
3-10
0)†
100
(67-
100)
* 57
(0-1
00)*
10
0 (8
9-10
0)*
100
(0-1
00)*
Abdo
min
al p
ain
%
(ran
ge)
Con
firm
ed
67 (0
-100
)† 35
(0-8
8)*
0 (0
-100
)*
88 (7
6-10
0)*
33 (0
-67)
* -
Susp
ecte
d 75
(33-
100)
* 67
(0-1
00)†
0 (0
-100
)*
75 (0
-100
)*
75 (0
-100
)*
80 (0
-100
)*
Vom
iting
% (r
ange
) C
onfir
med
10
0 (4
3-10
0)†
14 (0
-100
)*
0 (0
-74)
* 66
(50-
83)*
0
(0-0
)*
- Su
spec
ted
67 (0
-100
)*
33 (0
-100
)† 0
(0-6
7)*
78 (1
7-10
0)*
0 (0
-31)
* 33
(0-1
00)*
Nau
sea
% (r
ange
) C
onfir
med
83
(0-1
00)†
29 (0
-100
)*
0 (0
-100
)*
87 (7
4-10
0)*
0 (0
-0)*
-
Susp
ecte
d 75
(33-
100)
* 0
(0-1
00)†
0 (0
-100
)*
83 (0
-100
)*
42 (0
-73)
* 40
(0-1
00)*
Feve
r % (r
ange
) C
onfir
med
0
(0-8
3)†
7 (0
-67)
* 0
(0-7
5)*
43 (3
7-50
)*
0 (0
-0)*
-
Susp
ecte
d 50
(0-6
7)*
0 (0
-100
)† 0
(0-4
3)*
0 (0
-80)
* 0
(0-1
00)*
0
(0-1
00)*
Blo
ody
diar
rhoe
a %
(r
ange
) C
onfir
med
0
(0-1
7)†
0 (0
-0)*
0
(0-1
2)*
0 (0
-0)*
0
(0-0
)*
- Su
spec
ted
0 (0
-20)
* 0
(0-0
)† 0
(0-0
)*
0 (0
-0)*
0
(0-0
)*
0 (0
-4)*
R
ever
se
tem
pera
ture
%
(ran
ge)
Con
firm
ed
0 (0
-0)†
0 (0
-0)*
0
(0-6
7)*
0 (0
-0)*
0
(0-0
)*
-
Susp
ecte
d 0
(0-0
)*
0 (0
-0)†
0 (0
-10)
* 0
(0-0
)*
0 (0
-0)*
0
(0-1
00)*
Join
t and
mus
cle
pain
% (r
ange
) C
onfir
med
0
(0-6
7)†
0 (0
-6)*
0
(0-2
9)*
0 (0
-0)*
0
(0-0
)*
- Su
spec
ted
0 (0
-0)*
0
(0-0
)† 0
(0-3
3)*
0 (0
-60)
* 0
(0-2
9)*
0 (0
-100
)*
* ≥90
% c
ompl
ete
† 75
– 89
% c
ompl
ete
‡ 50
– 7
4% c
ompl
ete

37
Food vehicle attribution A wide variety of foods were implicated or suspected to be implicated in bacterial toxin
mediated outbreaks. To simplify analysis, foods were categorised and are shown in
Table 6. A food vehicle was suspected for all confirmed outbreaks caused by S.
aureus, B. cereus, preformed and in vivo formed toxins. In contrast, almost half of the
outbreaks confirmed to be caused by C. perfringens had an unknown or missing food
vehicle. Completeness for suspected outbreaks ranged from 39% for suspected C.
perfringens outbreaks to 91% for suspected B. cereus outbreaks. The category of
“solid masses of potentially hazardous foods” was the most frequently implicated
category for all aetiologies (29%; Table 6), followed by the category of “liquid or semi-
solid mixtures of potentially hazardous foods” (11%).
Of those outbreaks with a food vehicle listed, 26% were confirmed through laboratory
evidence. Another 19% of outbreaks showed a statistical link with the food through an
analytical study such as case control or cohort and 23% had compelling evidence to
implicate the food. Of the outbreaks associated with solid masses of potentially
hazardous foods, in 31% the implicated pathogen was isolated from the food vehicle. In
19%, the investigators were able to obtain statistical evidence that implicated the food
vehicle. In an additional 26% of the outbreaks, the investigators were able to obtain
compelling evidence implicating the food.
The type of meat present in the food vehicle is shown in the top section of Table 7.
Seafood is rarely implicated. Meat (beef, pork and lamb) is reported more frequently
than poultry. Also shown in Table 7 is the presence of a starch containing product such
as rice, noodles or pasta. With the exception of outbreaks of C. perfringens, starch
containing foods are common in all outbreak types.

38
Tabl
e 6:
Foo
d ca
tego
ries
impl
icat
ed in
toxi
n m
edia
ted
outb
reak
s by
con
firm
ed o
r sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
Stap
hylo
cocc
us
aure
us
% (n
)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed
toxi
n %
(n)
In v
ivo
toxi
n %
(n)
Toxi
n %
(n)
Solid
mas
ses
of p
oten
tially
ha
zard
ous
food
s C
onfir
med
43
(7)
50 (3
) 24
(19)
50
(1)
50 (1
) -
Susp
ecte
d 43
(3)
46 (5
) 21
(19)
43
(6)
40 (4
) 33
(11)
Liqu
id o
r sem
i-sol
id m
ixtu
res
of p
oten
tially
haz
ardo
us fo
ods
Con
firm
ed
6 (1
) 33
(2)
16 (1
3)
0 50
(1)
- Su
spec
ted
0 0
11 (1
0)
14 (2
) 0
3 (1
)
Roa
sted
mea
t/pou
ltry/
fish
Con
firm
ed
19 (3
) 0
7 (6
) 0
0 -
Susp
ecte
d 0
18 (2
) 4
(4)
0 10
(1)
3 (1
)
Coo
k/se
rve
food
s C
onfir
med
13
(2)
0 4
(3)
0 0
- Su
spec
ted
14 (1
) 9
(1)
0 0
10 (1
) 12
(4)
Sala
ds p
repa
red
with
one
or
mor
e co
oked
ingr
edie
nts
Con
firm
ed
6 (1
) 0
0 0
0 -
Susp
ecte
d 14
(1)
9 (1
) 0
0 0
3 (1
)
Sala
ds w
ith ra
w in
gred
ient
s C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
0 0
0 3
(1)
Mul
tiple
food
s C
onfir
med
0
17 (1
) 0
50 (1
) 0
- Su
spec
ted
0 0
0 0
0 0
Bak
ed g
oods
C
onfir
med
6
(1)
0 3
(2)
0 0
- Su
spec
ted
0 0
1 (1
) 0
0 0
Sand
wic
hes
Con
firm
ed
0 0
0 0
0 -
Susp
ecte
d 0
9 (1
) 1
(1)
0 10
(1)
6 (2
)
Bev
erag
es
Con
firm
ed
6 (1
) 0
0 0
0 -
Susp
ecte
d 0
0 0
0 0
0
Unk
now
n fo
od v
ehic
le
Con
firm
ed
0 0
47 (3
8)
0 0
- Su
spec
ted
29 (2
) 9
(1)
61 (5
5)
43 (6
) 30
(3)
36 (1
2)

39
Tabl
e 7:
Spe
cific
type
s of
food
impl
icat
ed in
bac
teria
l tox
in m
edia
ted
food
born
e ou
tbre
aks
by c
onfir
med
or s
uspe
cted
aet
iolo
gy, A
ustra
lia 2
001
to 2
013
St
aphy
loco
ccus
au
reus
%
(n)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed to
xin
% (n
) In
viv
o to
xin
% (n
) To
xin
% (n
)
Mea
t C
onfir
med
13
(2)
17 (1
) 28
(23)
0
50 (1
) -
Susp
ecte
d 43
(3)
18 (2
) 16
(14)
0
30 (3
) 18
(6)
Poul
try
Con
firm
ed
31 (5
) 17
(1)
7 (6
) 50
(1)
0 -
Susp
ecte
d 14
(1)
36 (4
) 3
(3)
14 (2
) 30
(3)
9 (3
)
Seaf
ood
Con
firm
ed
6 (1
) 17
(1)
1 (1
) 0
0 -
Susp
ecte
d 0
0 0
7 (1
) 10
(1)
18 (6
)
Noo
dles
, pas
ta
or ri
ce
Con
firm
ed
50 (8
) 50
(3)
6 (5
) 50
(1)
50 (1
) -
Susp
ecte
d 43
(3)
36 (4
) 9
(8)
43 (6
) 20
(2)
30 (1
0)

40
Contributing factors All three of the contributing factor fields were poorly completed, as shown by the high
number of unknown values in Table 8. Only 21% of outbreaks had a major
contaminating factor listed (other than “unknown”). Of those with a response, the most
commonly reported major factor was the generic category “other source of
contamination”. Other categories frequently reported were “person to food to person”,
“food handler contamination”, “cross contamination from raw ingredients”, “inadequate
cleaning of equipment”, “storage in contaminated environment” and “toxic substance or
part of tissue”. Few of these major factors were confirmed; 56% of those with an
answer were assumed or suspected contamination factors. Of those confirmed, 22%
were confirmed with measured evidence, 3% were confirmed verbally during inspection
and 19% were confirmed by observation during inspection.
Factors for microbial growth had the highest rate of completeness of the three
contributing factor variables, with 43% of outbreaks having at least one response
(Table 9). All of these outbreaks reported a factor for microbial growth that can be
considered temperature abuse. The only factor for bacterial growth selected that was
not related to temperature abuse was “anaerobic packaging/modified atmosphere”, and
this was only selected in one outbreak, suspected to have been caused by an in vivo
toxin. The growth factors in this outbreak were confirmed by observation during
inspection. Of those outbreaks with growth factors listed, 48% were assumed or
suspected, 23% were confirmed by observation during inspection, 23% were confirmed
verbally during inspection and 7% were confirmed with measured evidence.
Completeness of the factors for microbial survival was also low; only 28% of outbreaks
had at least one response. Of the outbreaks with a response, 82% of the factors for
microbial survival involved a type of temperature abuse, including “insufficient
time/temperature during cooking”, “insufficient time/temperature during reheating” or
“inadequate thawing and cooking” (Table 10). Of those outbreaks with survival factors
listed, 69% were assumed or suspected, 13% were confirmed by observation during
inspection, 13% were confirmed verbally during inspection and 5% were confirmed with
measured evidence.

41
Tabl
e 8:
Maj
or c
onta
min
atin
g fa
ctor
s co
ntrib
utin
g to
con
tam
inat
ion
of fo
od v
ehic
le, b
y co
nfirm
ed o
r sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
Stap
hylo
cocc
us
aure
us
% (n
)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed
toxi
n %
(n)
In v
ivo
toxi
n %
(n)
Toxi
n %
(n)
Oth
er s
ourc
e of
con
tam
inat
ion
Con
firm
ed
13 (2
) 17
(1)
5 (4
) 50
(1)
50 (1
) -
Susp
ecte
d 14
(1)
9 (1
) 1
(1)
7 (1
) 0
6 (2
)
Food
han
dler
con
tam
inat
ion
Con
firm
ed
25 (4
) 0
1 (1
) 50
(1)
0 -
Susp
ecte
d 14
(1)
0 1
(1)
0 0
15 (5
)
Cro
ss c
onta
min
atio
n fr
om ra
w
ingr
edie
nts
Con
firm
ed
0 0
5 (4
) 50
(1)
0 -
Susp
ecte
d 0
0 0
21 (3
) 10
(1)
6 (2
)
Inad
equa
te c
lean
ing
of
equi
pmen
t C
onfir
med
6
(1)
0 4
(3)
50 (1
) 50
(1)
- Su
spec
ted
0 9
(1)
1 (1
) 7
(1)
10 (1
) 3
(1)
Toxi
c su
bsta
nce
or p
art o
f tis
sue
Con
firm
ed
6 (1
) 0
2 (2
) 0
0 -
Susp
ecte
d 0
0 0
7 (1
) 0
15 (5
)
Pers
on to
food
to p
erso
n C
onfir
med
31
(5)
0 0
0 0
- Su
spec
ted
0 0
0 7
(1)
0 0
Stor
age
in c
onta
min
ated
en
viro
nmen
t C
onfir
med
6
(1)
17 (1
) 2
(2)
0 50
(1)
- Su
spec
ted
0 0
0 0
10 (1
) 0
Inge
stio
n of
con
tam
inat
ed ra
w
prod
ucts
C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
1 (1
) 0
0 6
(2)
Unk
now
n C
onfir
med
25
(4)
67 (4
) 84
(68)
0
0 -
Susp
ecte
d 71
(5)
82 (9
) 96
(86)
64
(9)
80 (8
) 64
(21)

42
Tabl
e 9:
Fac
tors
for m
icro
bial
gro
wth
afte
r con
tam
inat
ion
of fo
od v
ehic
le, b
y co
nfirm
ed o
r sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
Stap
hylo
cocc
us
aure
us
% (n
)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed
toxi
n %
(n)
In v
ivo
toxi
n %
(n)
Toxi
n %
(n)
Food
s le
ft at
room
or w
arm
te
mpe
ratu
re
Con
firm
ed
56 (9
) 33
(2)
16 (1
3)
100
(2)
100
(2)
- Su
spec
ted
43 (3
) 9
(1)
7 (6
) 14
(2)
10 (1
) 21
(7)
Slow
coo
ling
Con
firm
ed
6 (1
) 0
30 (2
4)
0 0
- Su
spec
ted
0 18
(2)
7 (6
) 21
(3)
10 (1
) 21
(7)
Inad
equa
te re
frig
erat
ion
Con
firm
ed
38 (6
) 17
(1)
11 (9
) 50
(1)
0 -
Susp
ecte
d 43
(3)
9 (1
) 4
(4)
7 (1
) 20
(2)
6 (2
)
Del
ay b
etw
een
prep
arat
ion
and
cons
umpt
ion
Con
firm
ed
6 (1
) 17
(1)
12 (1
0)
50 (1
) 50
(1)
- Su
spec
ted
14 (1
) 9
(1)
3 (3
) 0
10 (1
) 15
(5)
Inad
equa
te h
ot h
oldi
ng
tem
pera
ture
C
onfir
med
13
(2)
33 (2
) 2
(2)
0 50
(1)
- Su
spec
ted
14 (1
) 0
6 (5
) 0
0 6
(2)
Insu
ffici
ent c
ooki
ng
Con
firm
ed
0 33
(2)
1 (1
) 0
0 -
Susp
ecte
d 0
0 1
(1)
7 (1
) 10
(1)
3 (1
)
Inad
equa
te th
awin
g C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
0 0
0 3
(1)
Anae
robi
c pa
ckag
ing/
mod
ified
at
mos
pher
e C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
0 0
10 (1
) 0
Oth
er s
ourc
e of
con
tam
inat
ion
Con
firm
ed
0 0
0 0
0 -
Susp
ecte
d 0
9 (1
) 0
0 0
0
Unk
now
n C
onfir
med
19
(3)
17 (1
) 49
(40)
0
0 -
Susp
ecte
d 14
(1)
73 (8
) 80
(72)
64
(9)
50 (5
) 48
(16)

43
Tabl
e 10
: Fac
tors
for m
icro
bial
sur
viva
l afte
r con
tam
inat
ion
of fo
od v
ehic
le, b
y co
nfirm
ed o
r sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
Stap
hylo
cocc
us
aure
us
% (n
)
Bac
illus
cer
eus
% (n
)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed
toxi
n %
(n)
In v
ivo
toxi
n %
(n)
Toxi
n %
(n)
Insu
ffici
ent t
ime/
tem
pera
ture
du
ring
rehe
atin
g C
onfir
med
0
33 (2
) 41
(33)
0
0 -
Susp
ecte
d 0
0 10
(9)
7 (1
) 10
(1)
15 (5
)
Insu
ffici
ent t
ime/
tem
pera
ture
du
ring
cook
ing
Con
firm
ed
6 (1
) 33
(2)
5 (4
) 0
100
(2)
- Su
spec
ted
0 0
2 (2
) 0
10 (1
) 12
(4)
Oth
er s
ourc
e of
con
tam
inat
ion
Con
firm
ed
13 (2
) 17
(1)
2 (2
) 10
0 (2
) 0
- Su
spec
ted
14 (1
) 0
1 (1
) 0
10 (1
) 6
(2)
Inad
equa
te o
r fai
led
disi
nfec
tion
Con
firm
ed
6 (1
) 0
0 0
50 (1
) -
Susp
ecte
d 0
0 0
7 (1
) 0
3 (1
)
Inad
equa
te a
cidi
ficat
ion
Con
firm
ed
0 0
0 0
0 -
Susp
ecte
d 14
(1)
9 (1
) 0
0 0
0
Inad
equa
te th
awin
g an
d co
okin
g C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
0 0
0 3
(1)
Unk
now
n C
onfir
med
75
(12)
33
(2)
56 (4
5)
50 (1
) 0
- Su
spec
ted
71 (5
) 91
(10)
87
(78)
93
(13)
80
(8)
64 (2
1)

44
Food preparation and consumption settings The setting in which contamination of the food vehicle may have occurred is listed in
two categories – the setting in which the food was prepared (Table 11) and the setting
in which the food was consumed (Table 12). For 77% of the outbreaks, the implicated
food was eaten and prepared in the same location. In the other 23% of outbreaks, the
food was prepared in a commercial location such as a take-away shop and eaten at
home.
The types of settings in which bacterial toxin mediated outbreaks occur can be divided
into two dominant types depending on the pathogen involved. Outbreaks caused by C.
perfringens, both confirmed and suspected, were most commonly reported in aged
care facilities (51% and 60% for confirmed and suspected respectively, when both
setting where food was prepared and setting where food was consumed is taken into
account, Table 13). There were no reports of outbreaks caused by the other bacterial
toxin aetiologies in aged care facilities with the exception of two outbreaks suspected to
be due to a toxin, and one outbreak confirmed to involve both C. perfringens and B.
cereus. The other aetiology groups were more likely to be reported in outbreaks where
food was prepared by a commercial enterprise, such as a restaurant, fast food/take
away, grocery store, delicatessen, commercial caterer, fair, festival, mobile service
(Table 13). The food vehicles for few outbreaks (3%) were prepared in a private
residence.

45
Tabl
e 11
: Set
ting
whe
re th
e fo
od w
as p
repa
red,
by
conf
irmed
and
sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
St
aphy
loco
ccus
au
reus
%
(n)
Bac
illus
cer
eus
% (n
) C
lost
ridiu
m
perf
ringe
ns
% (n
) Pr
efor
med
toxi
n %
(n)
In v
ivo
toxi
n %
(n)
Toxi
n %
(n)
Aged
car
e C
onfir
med
0
0 47
(38)
0
50 (1
) -
Susp
ecte
d 0
0 59
(53)
0
0 9
(3)
Res
taur
ant
Con
firm
ed
19 (3
) 33
(2)
19 (1
5)
50 (1
) 0
- Su
spec
ted
57 (4
) 55
(6)
24 (2
2)
64 (9
) 60
(6)
55 (1
8)
Com
mer
cial
cat
erer
C
onfir
med
25
(4)
33 (2
) 11
(9)
0 50
(1)
- Su
spec
ted
0 18
(2)
6 (5
) 0
20 (2
) 6
(2)
Take
-aw
ay
Con
firm
ed
13 (2
) 17
(1)
2 (2
) 0
0 -
Susp
ecte
d 14
(1)
9 (1
) 4
(4)
14 (2
) 10
(1)
21 (7
)
Inst
itutio
n C
onfir
med
0
0 6
(5)
0 0
- Su
spec
ted
0 9
(1)
1 (1
) 7
(1)
0 0
Hos
pita
l C
onfir
med
0
0 6
(5)
0 0
- Su
spec
ted
0 0
2 (2
) 0
0 0
Priv
ate
resi
denc
e C
onfir
med
0
0 2
(2)
0 0
- Su
spec
ted
29 (2
) 9
(1)
0 7
(1)
0 3
(1)
Nat
iona
l fra
nchi
sed
fast
fo
od re
stau
rant
C
onfir
med
13
(2)
17 (1
) 1
(1)
0 0
- Su
spec
ted
0 0
1 (1
) 0
0 0
Oth
er
Con
firm
ed
6 (1
) 0
1 (1
) 0
0 -
Susp
ecte
d 0
0 1
(1)
0 0
3 (1
)
Cam
p C
onfir
med
6
(1)
0 0
0 0
- Su
spec
ted
0 0
0 7
(1)
10 (1
) 0
Fair/
fest
ival
/mob
ile
serv
ice
Con
firm
ed
6 (1
) 0
0 50
(1)
0 -
Susp
ecte
d 0
0 0
0 0
0 G
roce
ry
Con
firm
ed
6 (1
) 0
0 0
0 -

46
St
aphy
loco
ccus
au
reus
%
(n)
Bac
illus
cer
eus
% (n
) C
lost
ridiu
m
perf
ringe
ns
% (n
) Pr
efor
med
toxi
n %
(n)
In v
ivo
toxi
n %
(n)
Toxi
n %
(n)
stor
e/de
licat
esse
n Su
spec
ted
0 0
0 0
0 0
Chi
ld c
are
Con
firm
ed
6 (1
) 0
0 0
0 -
Susp
ecte
d 0
0 0
0 0
0
Com
mer
cial
ly
man
ufac
ture
d C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
0 0
0 3
(1)
Priv
ate
cate
rer
Con
firm
ed
0 0
1 (1
) 0
0 -
Susp
ecte
d 0
0 0
0 0
0
Scho
ol
Con
firm
ed
0 0
0 0
0 -
Susp
ecte
d 0
0 1
(1)
0 0
0
Mili
tary
C
onfir
med
0
0 1
(1)
0 0
- Su
spec
ted
0 0
0 0
0 0
Unk
now
n C
onfir
med
0
0 1
(1)
0 0
- Su
spec
ted
0 0
0 0
0 0

47
Tabl
e 12
: Set
ting
whe
re th
e fo
od w
as c
onsu
med
, by
conf
irmed
and
sus
pect
ed a
etio
logy
, Aus
tralia
200
1 to
201
3
St
aphy
loco
ccus
au
reus
%
(n)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed to
xin
% (n
) In
viv
o to
xin
% (n
) To
xin
% (n
)
Aged
car
e C
onfir
med
0
0 51
(41)
0
50 (1
) -
Susp
ecte
d 0
0 60
(54)
0
0 9
(3)
Res
taur
ant
Con
firm
ed
13 (2
) 33
(2)
17 (1
4)
0 0
- Su
spec
ted
71 (5
) 55
(6)
21 (1
9)
64 (9
) 80
(8)
45 (1
5)
Priv
ate
resi
denc
e C
onfir
med
19
(3)
50 (3
) 5
(4)
0 0
- Su
spec
ted
0 18
(2)
2 (2
) 14
(2)
0 15
(5)
Oth
er
Con
firm
ed
13 (2
) 0
5 (4
) 0
0 -
Susp
ecte
d 29
(2)
9 (1
) 6
(5)
7 (1
) 0
9 (3
)
Com
mer
cial
cat
erer
C
onfir
med
13
(2)
17 (1
) 4
(3)
50 (1
) 50
(1)
- Su
spec
ted
0 9
(1)
3 (3
) 0
10 (1
) 3
(1)
Inst
itutio
n C
onfir
med
0
0 6
(5)
0 0
- Su
spec
ted
0 9
(1)
1 (1
) 7
(1)
0 0
Com
mun
ity
Con
firm
ed
13 (2
) 0
4 (3
) 0
0 -
Susp
ecte
d 0
0 0
0 0
9 (3
)
Cam
p C
onfir
med
6
(1)
0 0
0 0
- Su
spec
ted
0 0
1 (1
) 7
(1)
10 (1
) 0
Fair/
fest
ival
/mob
ile
serv
ice
Con
firm
ed
6 (1
) 0
0 50
(1)
0 -
Susp
ecte
d 0
0 1
(1)
0 0
3 (1
)
Hos
pita
l C
onfir
med
0
0 4
(3)
0 0
- Su
spec
ted
0 0
1 (1
) 0
0 0
Func
tion
Con
firm
ed
6 (1
) 0
0 0
0 -
Susp
ecte
d 0
0 0
0 0
3 (1
) Sc
hool
C
onfir
med
0
0 1
(1)
0 0
-

48
St
aphy
loco
ccus
au
reus
%
(n)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed to
xin
% (n
) In
viv
o to
xin
% (n
) To
xin
% (n
)
Susp
ecte
d 0
0 1
(1)
0 0
0
Nat
iona
l fra
nchi
sed
fast
fo
od re
stau
rant
C
onfir
med
6
(1)
0 0
0 0
- Su
spec
ted
0 0
1 (1
) 0
0 0
Cru
ise/
airli
ne
Con
firm
ed
0 0
1 (1
) 0
0 -
Susp
ecte
d 0
0 0
0 0
0
Picn
ic
Con
firm
ed
0 0
0 0
0 -
Susp
ecte
d 0
0 1
(1)
0 0
0
Hea
lth s
pa/re
sort
C
onfir
med
0
0 0
0 0
- Su
spec
ted
0 0
0 0
0 3
(1)
Chi
ld c
are
Con
firm
ed
6 (1
) 0
0 0
0 -
Susp
ecte
d 0
0 0
0 0
0
Mili
tary
C
onfir
med
0
0 1
(1)
0 0
- Su
spec
ted
0 0
0 0
0 0
Unk
now
n C
onfir
med
0
0 1
(1)
0 0
- Su
spec
ted
0 0
0 0
0 0

49
Tabl
e 13
: Con
tribu
tion
of a
ged
care
faci
litie
s an
d fo
od s
ervi
ce b
usin
esse
s to
bac
teria
l tox
in m
edia
ted
outb
reak
s, b
y co
nfirm
ed a
nd s
uspe
cted
aet
iolo
gy, A
ustra
lia
2001
to 2
013
St
aphy
loco
ccus
au
reus
%
(n)
Bac
illus
ce
reus
%
(n)
Clo
strid
ium
pe
rfrin
gens
%
(n)
Pref
orm
ed to
xin
% (n
) In
viv
o to
xin
% (n
) To
xin
% (n
)
Aged
car
e C
onfir
med
0
0 51
(41)
0
50 (1
) -
Susp
ecte
d 0
0 60
(54)
0
0 9
(3)
Food
ser
vice
bu
sine
sses
C
onfir
med
86
(14)
10
0 (6
) 35
(28)
10
0 (2
) 50
(1)
- Su
spec
ted
71 (5
) 82
(9)
36 (3
2)
77 (1
1)
90 (9
) 85
(28)

50
Further attribution of suspected aetiologies The Outbreak Register does not provide information on the type of toxin produced by
B. cereus. Table 14 attempts to utilise the information available, such as incubation
period and percent of cases reporting vomiting, to assess which outbreaks may have
been caused by the emetic toxin and which ones may have been caused by the
diarrhoeal toxin. One confirmed outbreak was likely to be caused by the emetic toxin,
based on a short incubation period and high rates of vomiting. Five confirmed
outbreaks were likely to be caused by the diarrhoeal toxin based on longer incubation
periods and lower rates of vomiting.
Of the 11 outbreaks suspected to be caused by B. cereus, four had incubation periods
less than six hours. In three of these outbreaks, all cases reported vomiting and these
outbreaks can be considered likely outbreaks of the emetic type. The fourth outbreak
had only 33% of cases reporting vomiting. Three of the remaining seven outbreaks had
median incubation periods between 10 hours and 14 hours. No cases reported
vomiting in any of these outbreaks, and are likely to be diarrhoeal toxin type outbreaks.
Two outbreaks had long incubation periods of 24 and 31 hours. These outbreaks may
not be toxin mediated. The remaining two outbreaks had no data for incubation period
and one had no data for numbers of cases reporting vomiting.

51
Table 14: Informative variables and assessment of probable toxin type for confirmed and
suspected B. cereus outbreaks (emetic or diarrhoeal), Australia 2001 to 2013
Confirmation Incubation (hr)*
Vomiting (%)*
Diarrhoea (%)* Food vehicle Probable
toxin type Confirmed 2 100 0 Fried rice and
honey chicken Emetic
Confirmed 6 0 100 Multiple foods Diarrhoeal
Confirmed 8 16 100 Boiled gefilte fish (fish balls) Diarrhoeal
Confirmed 9 67 67 Mashed Potato & Gravy Diarrhoeal
Confirmed 10 3 97 Rice Diarrhoeal
Confirmed 12 13 96 Rice (and/or beef curry) Diarrhoeal
Suspected 2 100 33 Fried rice Emetic Suspected 4 100 100 Chicken katsu Emetic
Suspected 4 100 100 Chicken teriyaki sushi roll (nori
roll) Emetic
Suspected 4 33 100 Cold chicken salad Diarrhoeal
Suspected 10 0 100 Kebab/hummous Diarrhoeal Suspected 11 0 86 Cooked Chicken Diarrhoeal Suspected 14 0 100 Naan/rice Diarrhoeal Suspected 24 100 84 Rice Unknown Suspected 31 - - Meat Unknown
Suspected - 0 100 Unknown Insufficient information
Suspected - - - Chicken and
bacon/meatlovers pizza
Insufficient information
* - indicates no information provided for variable
Tables showing a similar analysis for all other suspected outbreaks are shown in
Appendix 2, separated by suspected aetiology. Of the seven suspected S. aureus
outbreaks, and 90 suspected C. perfringens outbreaks, 32 had symptoms and
incubation period consistent with the aetiology suspected by investigators (four S.
aureus outbreaks, 28 C. perfringens outbreaks). An additional outbreak suspected by
investigators to be caused by S. aureus was more likely to be caused by an in vivo
toxin. All other outbreaks did not have enough information to allow characterisation, or
had symptoms inconsistent with a bacterial toxin mediated outbreak.
A total of 57 outbreaks were suspected to be caused by an unnamed bacterial
intoxication. Of these outbreaks, two were assessed as likely caused by the B. cereus
emetic toxin, 15 due to a preformed toxin (S. aureus or emetic B. cereus) and 29 due to
an in vivo formed toxin (diarrhoeal B. cereus or C. perfringens). A further 12 outbreaks
had insufficient information supplied, or the details were inconsistent with what is

52
known about bacterial intoxications. All but one (90%) of the outbreaks assessed as
probable in vivo toxin outbreaks by investigators were probable in vivo outbreaks by
the case definition. Only one outbreak had no median incubation period reported,
although symptoms were consistent with an in vivo toxin outbreak. Nine of the 14
outbreaks (64%) assessed as probable preformed toxin outbreaks by investigators met
the probable preformed toxin case definition. Of the remaining five outbreaks, three
met the probable in vivo toxin outbreak case definition, and two were inconsistent with
any probable bacterial toxin case definition. Similarly, 24 of the 33 outbreaks (73%)
identified by investigators as caused by a toxin (type of toxin not specified) fitted the
probable toxin case definition (eight probable preformed toxin outbreaks, 16 probable
in vivo toxin outbreaks). Of the remaining nine outbreaks, two were not consistent with
a bacterial intoxication and seven had insufficient information to allow an assessment.
In total, 87% (82 of 94 outbreaks with complete information) of outbreaks with a
suspected aetiology and a known median incubation period, percent vomiting and
percent diarrhoea were categorised correctly. However, of these, 26% (24 outbreaks)
that were reported as “toxin” outbreaks could have been fully categorised based on
symptomology.
Of the 180 outbreaks with unknown aetiology and incubation periods of 18 hours or
less, 40 outbreaks had incubation periods of seven hours or less, and 50% or more
cases reporting vomiting. These outbreaks are probable preformed toxin outbreaks
according to the case definition. Another 44 outbreaks had incubation periods between
six hours and 18 hours, less than 50% of cases reporting vomiting and 50% or more
cases reporting diarrhoea. These outbreaks are probable in vivo outbreaks. The
remaining 86 outbreaks did not follow this pattern, so no conclusions could be made on
aetiology.
Discussion This analysis was able to establish a greater understanding of the epidemiology of
bacterial toxin mediated foodborne outbreaks in Australia between 2001 and 2013. The
incidence of bacterial toxin mediated foodborne outbreaks during the thirteen-year
period under study was variable. Similarly, there was no obvious trend for any specific
aetiology or confirmation status, although 2010 and 2011 had more C. perfringens
outbreaks than other years. The number of outbreaks per jurisdiction was too small in
most jurisdictions for meaningful calculations of rate, as a single outbreak in a small
jurisdiction makes a big difference to the rate. However, comparing outbreaks in the
larger states, VIC reported more than twice as many outbreaks (adjusted for

53
population) than any other state. While classification of outbreaks as “suspected” rather
than “unknown” may contribute to this higher incidence of toxin mediated outbreaks
(i.e. epidemiologists in VIC may be more willing to assume a toxin aetiology in an
unconfirmed outbreak), VIC also has a higher incidence of confirmed toxin outbreaks
than other jurisdictions. From the data available, it is unclear whether this was due to a
higher incidence of bacterial toxin mediated outbreaks in VIC, or if other unknown
factors were involved.
The median incubation period for the confirmed S. aureus outbreaks was shorter than
for all other aetiologies (median 3 hours, range 2 hours to 7 hours). In contrast, the
median incubation period for C. perfringens outbreaks was 12 hours (range 6 hours to
17 hours). These incubation periods are similar to the expected incubation periods for
these illnesses, one to seven hours for S. aureus (19) and 16 hours for C. perfringens
(11).
The median incubation period for outbreaks suspected to be due to C. perfringens was
the same as that reported for confirmed outbreaks (median 12 hours). However, the
upper bound of the range was much larger (24 days). Completeness of median
incubation periods for suspected C. perfringens outbreaks was poor (33%). Of the 60
outbreaks with no median incubation period listed, 53 occurred in aged care facilities,
highlighting the difficulty investigating outbreaks in this setting (20). Onset of illness can
be difficult to identify in elderly cases due to a higher incidence of diarrhoea from other
causes, such as medication use (21). All but two of the suspected C. perfringens
outbreaks with median incubation periods reported have incubation periods consistent
with that expected for this pathogen (11). The two outbreaks with long incubation
periods (5 and 24 days) both had moderate growth of C. perfringens from a single
case, probably contributing to the investigator’s suspicion that these outbreaks were
caused by C. perfringens. For confirmation, growth is required from at least two cases,
and in these outbreaks the growth of C. perfringens may have been incidental and the
aetiology of the outbreak some other unidentified agent. Indeed, it is common for
elderly people to have elevated levels of C. perfringens in their faeces without
associated illness (22).
The median incubation period and range for confirmed B. cereus outbreaks of 8.5
hours (range 2 hours to 12 hours) is reflective of the inability to separate the emetic
and diarrheal forms of the illness based on the information provided. The emetic
disease is expected to have an incubation period between 30 minutes and six hours,
while the diarrhoeal disease is expected to have an incubation period of six to 15 hours

54
(12). Of the six confirmed B. cereus outbreaks, 83% (5 outbreaks) were likely to have
been caused by the diarrhoeal toxin. The remaining outbreak had a suspected food
vehicle that included rice, consistent with the emetic form of B. cereus as rice is a
commonly reported vehicle for emetic B. cereus (8, 10, 23). Of the eleven suspected B.
cereus outbreaks, 27% (three outbreaks) were likely caused by the emetic toxin and
45% (five outbreaks) were likely diarrhoeal toxin. This distribution of a greater number
of diarrhoeal outbreaks than emetic is consistent with the epidemiology of B. cereus in
North America and Northern Europe, and different to that seen in countries with high
rates of rice consumption such as Japan (10).
A wide variety of foods (confirmed through isolation or epidemiological evidence, or
suspected due to common consumption) were implicated in toxin mediated outbreaks.
The food source for confirmed C. perfringens outbreaks was not identified for 47% of
outbreaks. This is in contrast with other confirmed aetiologies and may be due to the
setting in which these outbreaks occurred. Of these 38 confirmed C. perfringens
outbreaks, 29 occurred in aged care facilities, and six occurred in hospitals or other
institutions. Determining the food eaten in these settings is often difficult due to poor
recall on the part of the cases, contributing to the difficulty investigating outbreaks in
aged care facilities, as discussed above (20).
The food vehicles implicated in bacterial toxin mediated outbreaks most frequently fall
into the two food categories that are likely to spend a longer period of time at
temperatures that promote bacterial growth than other types of foods (“solid masses of
potentially hazardous foods” and “liquids or semi-solid mixtures of potentially
hazardous foods”). This is different from the US study, which reported “roasted meat or
poultry” as the most commonly reported food category for bacterial toxin mediated
outbreaks (1). No other studies of bacterial toxin mediated outbreaks were found that
used food categories to examine food preparation rather than the ingredients
themselves.
The evidence for the implication of these food vehicles varies from isolation of the
pathogen from a sample of the food to no specific evidence other than that the food
was eaten and the investigators suspected it may have been implicated. More than two
thirds of the outbreaks that had a food vehicle listed had evidence to support the
implication of this food. This includes outbreaks where the pathogen was isolated from
the food, an epidemiological link was shown statistically through an analytical study, or
the evidence was “compelling”, such as outbreaks where only one food item was eaten
by a case. Given the difficulty confirming outbreaks caused by the bacterial toxin

55
producing pathogens, especially in food, this level of confidence in the food vehicle is
satisfactory, although there is room for improvement.
The most commonly reported major contamination factor in all outbreaks was the
generic description “other source of contamination”, in 6% of all outbreaks.
Contamination of food directly from a person rather than the environment (person to
food to person or food handler contamination; no outbreak reported both) was most
commonly reported in outbreaks caused by S. aureus (63% of S. aureus outbreaks that
reported a major contributing factor). This is consistent with the ubiquitousness of S.
aureus on human skin, and previous studies showing that S. aureus outbreaks are
commonly associated with contamination from food handlers (1, 7, 9, 24). Surprisingly,
few outbreaks of S. aureus or B. cereus had a major contamination factor of “toxic
substance or part of tissue” (6% of confirmed S. aureus outbreaks, no B. cereus or
suspected S. aureus outbreaks), a category that according to the Outbreak Register
data dictionary includes preformed toxin outbreaks.
All of the outbreaks with a factor for microbial growth listed reported at least one factor
that relates to temperature abuse of the food. Similarly, 82% of outbreaks reporting a
bacterial survival factor included at least one factor relating to temperature abuse.
Temperature abuse of food occurs when the food is held at a temperature between 4°C
and 60°C, the optimal temperature for growth of many microorganisms. Temperature
abuse is a commonly reported contributing factor for bacterial toxin mediated
outbreaks, as this allows the pathogen to grow in the food, and in the case of
preformed toxin or bacterial spores (S. aureus and B. cereus, and B. cereus and C.
perfringens respectively), subsequent cooking of the food does not remove the threat
(7, 10, 13).
Contamination of the food that caused foodborne outbreaks can occur in three main
parts of the food chain: contamination during primary food production (e.g. Salmonella
in eggs), contamination during preparation of food products for consumption, or
contamination at the location where the food is consumed. The latter two categories
are reported in the Outbreak Register and are relevant for bacterial toxin mediated
outbreaks. As the same setting for preparation and consumption was assumed when
“not applicable” was entered as the preparation setting, the analysis may overestimate
the association with these settings as the food may have been prepared elsewhere.
However, this is unlikely, as the food must have been prepared somewhere, and if the
food had been prepared elsewhere the investigator should have entered this
information rather than selecting “not applicable”. More than half of the outbreaks

56
(53%) were associated with preparation of food at food service businesses, such as a
restaurant or commercial caterer. Few outbreaks were associated with preparation of
food in private homes (3%). This is in contrast to that reported in a study in the US,
which found that 16% of outbreaks were associated with private homes (1).
Aged care facilities were implicated, either as the location for food preparation and/or
the location for consumption, in 56% of outbreaks associated with C. perfringens, but
none of the outbreaks caused by S. aureus or B. cereus. However, this is not
necessarily a true reflection of the incidence of these other toxin producing bacteria
and may be due to measurement bias. Indeed, only three of the suspected outbreaks
in the toxin category and none in the in vivo toxin categories were associated with aged
care facilities compared with 54 of the 90 suspected C. perfringens outbreaks,
suggesting that investigators may assume C. perfringens in aged care outbreaks. In
addition, bacterial toxin mediated outbreaks are less likely to be recorded or
investigated in the community (underreporting), as the illness is mild and short
compared with other forms of gastroenteritis, whereas in aged care facilities the illness
may be more severe, leading to greater vigilance, detection and investigation. C.
perfringens is more likely to cause large outbreaks that are noticed and investigated
(1), suggesting that even if small S. aureus or B. cereus outbreaks are occurring in
aged care facilities, they are not necessarily investigated. Completeness of data is
lacking in these investigations, particularly for incubation period and food vehicle.
However, few outbreaks report high rates of vomiting among cases, suggesting that it
is unlikely that these are misattributed S. aureus outbreaks. Aged care was not
reported as a notable risk factor for bacterial toxin mediated outbreaks in US studies,
only included in an “other” category (1, 25).
All but one of the deaths that occurred during bacterial toxin mediated outbreaks
occurred in an aged care facility. It is difficult to know whether these deaths were
caused by the outbreak associated illness or incidental to the outbreak. This is
consistent with other studies showing higher mortality during foodborne outbreaks in
aged care facilities (20, 22, 26, 27). However, improving the investigation of all
outbreaks of gastroenteritis in aged care facilities is an important component of
maintaining the health of this vulnerable group. Community outbreaks of bacterial
toxins are likely to remain underreported.
Many of the outbreaks investigated here were the result of temperature abuse of “solid
masses of potentially hazardous food”, a category of food that can be difficult to heat or
cool appropriately. A simple measure to reduce the incidence of these outbreaks is

57
greater awareness around keeping foods at appropriate temperatures, and promoting
awareness that some types of foods require extra care when heating or cooling.
Although 87% of outbreaks with a suspected aetiology and sufficient information for
categorisation were categorised correctly by investigators, four outbreaks were
incorrectly categorised, based on the criteria used here. Of the 87% of outbreaks, 26%
were toxin outbreaks that could have been further categorised as preformed or in vivo
toxins. The inconsistency between the aetiology suspected by the investigator and the
probable case definitions, and the missed opportunity of further categorising toxin
outbreaks suggests that including these definitions as a guide in the Outbreak Register
would help investigators to suggest a probable aetiology based on their investigation.
Given that bacterial toxin mediated outbreaks are often not confirmed, this will increase
discrimination of outbreaks of unknown cause.
The design of the question in the Outbreak Register asking if a symptom was reported
by any cases is flawed. The only option is to check the box marked “yes” (leading to
additional questions asking the number of cases reporting the symptom), or leave it
unchecked. This second option means that there is no way to distinguish between
outbreaks where the symptom was not reported in any cases, and outbreaks where
cases were not asked about the symptom at all, leading to measurement bias. For this
study, it was assumed that outbreaks where the box was not checked truly had no
cases reporting the symptom, unless no information was entered for any symptom. In
this latter case, the data was treated as missing. This method of analysis potentially
leads to lower median percentages when the data from outbreaks are combined (i.e. by
aetiology), especially for less frequently reported symptoms. The use of median rather
than mean for these calculations attempts to counteract this measurement bias, and
the range allows for an assessment of accuracy.
One of the limitations of this study was choosing which outbreaks to include for
analysis in addition to the confirmed outbreaks. The suspected outbreaks consisted of
a combination of outbreaks in which a toxin producing bacteria was isolated from only
one clinical sample or in low levels from food (i.e. not meeting CDC guidelines) and
outbreaks where the symptomology and incubation periods led the investigators to
suspect a toxin mediated outbreak with enough confidence to mention it in the remarks
section. Without confirmation, it is possible that these outbreaks may have been
caused by a pathogen other than a bacterial toxin, leading to selection bias, and may
reflect differences in the way individual investigators perceive risk and the differences
in the knowledge of investigators (28). This selection bias has been mitigated by

58
separating out the analysis of the outbreaks with a laboratory confirmed aetiology from
the outbreaks with a suspected aetiology, and comparing these analyses. This study
then attempts to assess whether the suspected outbreaks are true bacterial toxin
mediated outbreaks by comparing symptomology of the suspected outbreaks with the
distinctive symptomology of bacterial toxin mediated outbreaks.
In addition to the outbreaks designated as confirmed or suspected bacterial toxin
mediated outbreaks, there were also 180 outbreaks with a median incubation period
less than 18 hours. These outbreaks were not included in the analysis as no suspicion
of a bacterial toxin aetiology was mentioned by the investigators. These outbreaks may
not have been investigated beyond a basic report, or the investigator didn’t feel
comfortable mentioning suspicions in the remarks. At least 94 of these outbreaks could
be considered to fit the pattern for a preformed or in vivo toxin outbreak. A further 86
outbreaks did not have enough information to make an assessment or the
symptomology was incompatible with bacterial toxin mediated outbreaks. These
“unknown” outbreaks were not analysed with the suspected and confirmed outbreaks,
as selecting them based on incubation period rather than aetiology and categorising
them by symptomology may bias the analysis (selection bias). However, given that it is
likely that some of these outbreaks are true bacterial toxin mediated outbreaks, their
absence from the analysis may in turn bias the conclusions drawn away from
characteristics that are unique to bacterial toxin mediated outbreaks.
Analysis of data collected and entered by multiple people over many years, such as the
data in the Outbreak Register, always requires assumptions of what those who entered
the data meant, especially in free text fields. In this analysis, assumptions were made
about the foods implicated in the outbreak, based on what was written in the free text
food vehicle field. Assumptions were kept to a minimum by only including foods listed.
However, this may result in underestimation of foods that are common
accompaniments, such as rice.
Another assumption made for this analysis was that if the food preparation setting was
listed as not applicable, then it was assumed to be the same as the setting in which the
food was eaten. This may result in an overestimation of the proportion for some food
preparation settings. However, for analysis of the two main settings associated with
bacterial toxin mediated foodborne outbreaks (aged care and food service businesses),
both food preparation and food consumption setting were combined, minimising the
effect of misattribution of the food preparation setting.

59
The outbreaks reported here are likely to be only a small proportion of the true
incidence of bacterial toxin mediated outbreaks. Since these outbreaks frequently have
a short incubation period, short duration and comparatively mild illness, they are often
not reported and/or investigated. In addition, testing for these pathogens is only
conducted at a small number of laboratories in Australia, so outbreaks due to bacterial
toxins are often not laboratory confirmed. A limitation of studies into the epidemiology
of bacterial toxin mediated outbreaks is that because these toxins cause a mild and
short lived illness, outbreaks are often not reported and investigated.
Conclusion Bacterial toxin mediated foodborne outbreaks are a completely preventable form of
foodborne illness. Most outbreaks are associated with foods in the category “solid
masses of potentially hazardous food” and improper temperature control was
associated with all outbreaks where contributing factor information was available. The
primary group of people at greater risk of bacterial toxin mediated foodborne disease
outbreaks are those residing in aged care facilities. In this setting, foods are often
prepared in advance and are often in the “solid masses of potentially hazardous foods”
category, a category that includes many foods that are easy to prepare for large groups
of people and often refrigerated and reheated. In addition, deaths from usually mild
gastroenteritis are more likely in elderly people. Public health efforts aimed at
improving pre-cooked food storage habits could help to reduce the magnitude of this
problem, especially by focusing the public health efforts in institutional settings, in
particular aged care facilities.
Recommendations for the Outbreak Register The OzFoodNet Outbreak Register is an extremely useful tool for understanding the
epidemiology of and ultimately preventing gastrointestinal outbreaks in Australia.
However, to reach its full potential, some improvements should be made, mostly in
order to increase completeness and ease of use.
The Outbreak Register is currently an Access database. While Access is a useful tool,
and was the best available option when the Outbreak Register was established in
2001, there are now many other options for a database such as this. Online databases
allow users to enter the data directly, rather than the current method of sending the
jurisdictional databases to OzFoodNet Central for compilation. Online databases are
also more secure than using email to transfer the data and can allow for automated
validation checks.

60
Many fields in the Outbreak Register are free text fields, meaning that investigators can
enter any data they wish. However, many of these fields, such as aetiology, could be
defined categories. By having a set of options from which investigators can select,
misspellings and ambiguous answers can be avoided. This also improves the ease of
use and time taken to enter the data. Including an option of “other”, with a free text field
that follows will permit the entry of novel pathogens or responses. By retaining the
current free text “remarks” field, investigators are still able to enter any extra
information that couldn’t be entered elsewhere.
Food vehicles in outbreaks can vary greatly, and it is important to retain a free text field
to record the confirmed or suspected food involved. However, including additional
questions to categorise these foods would assist in comparison between outbreaks.
The investigators are often aware of more specific information about the meals than
what is entered into the Outbreaks Register, so categorising foods during later
analyses may miss some nuances. Including a food categories question, as used in
this study, along with a question about food types (e.g. eggs, meat, poultry, rice,
legumes, berries) would assist future analyses. This latter question would need to be a
checkbox question, allowing investigators to select multiple options if required.
Some questions are redundant and/or not used correctly. These questions could be
redesigned to improve clarity. For example, the variable “food_evidence” asks what
type of evidence was obtained to implicate the food vehicle. The following five
questions then ask about each of these types of evidence individually as a yes or no
question. As a result, “food_evidence” is frequently not completed. It is not necessary
to include this field in the Register as the same information is entered into the individual
evidence fields.
Well-designed questions should have multiple options, covering all possible responses.
By only allowing a “yes” response for the questions about symptoms, it is impossible to
distinguish between a true no (i.e. no cases reported having the symptom), and a
missing or unknown response.
In conclusion, this study has examined the epidemiology of bacterial toxin mediated
foodborne outbreaks in Australia and assessed the useability of the OzFoodNet
Outbreak Register. The recommendations for improvement of the Outbreak Register
have been shared with the OzFoodNet Outbreak Register Working Group. Future
improvements of the Register will allow easier comparison of outbreaks.

61
References 1. Bennett SD, Walsh KA, Gould LH. Foodborne disease outbreaks caused by Bacillus cereus, Clostridium perfringens, and Staphylococcus aureus--United States, 1998-2008. Clinical Infectious Diseases: an official publication of the Infectious Diseases Society of America. 2013;57(3):425-33. 2. Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA, Roy SL, et al. Foodborne illness acquired in the United States--major pathogens. Emerging Infectious Diseases. 2011;17(1):7-15. 3. Gormley FJ, Little CL, Rawal N, Gillespie IA, Lebaigue S, Adak GK. A 17-year review of foodborne outbreaks: describing the continuing decline in England and Wales (1992-2008). Epidemiology and Infection. 2011;139(5):688-99. 4. Hall G, Kirk MD, Becker N, Gregory JE, Unicomb L, Millard G, et al. Estimating foodborne gastroenteritis, Australia. Emerging Infectious Diseases. 2005;11(8):1257-64. 5. Kirk M, Ford L, Glass K, Hall G. Foodborne illness, Australia, circa 2000 and circa 2010. Emerging Infectious Diseases. 2014;20(11):1857-64. Epub 2014/10/24. 6. Hall G, Yohannes K, Raupach J, Becker N, Kirk M. Estimating community incidence of Salmonella, Campylobacter, and Shiga toxin-producing Escherichia coli infections, Australia. Emerging Infectious Diseases. 2008;14(10):1601-9. 7. Tranter HS. Foodborne staphylococcal illness. Lancet. 1990;336(8722):1044-6. 8. Ehling-Schulz M, Frenzel E, Gohar M. Food-bacteria interplay: pathometabolism of emetic Bacillus cereus. Frontiers in Microbiology. 2015;6:704. 9. Argudin MA, Mendoza MC, Rodicio MR. Food poisoning and Staphylococcus aureus enterotoxins. Toxins. 2010;2(7):1751-73. 10. Stenfors Arnesen LP, Fagerlund A, Granum PE. From soil to gut: Bacillus cereus and its food poisoning toxins. FEMS Microbiology Reviews. 2008;32(4):579-606. 11. Food and Drug Administration. Clostridium perfringens. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed 2012. p. 83-6. 12. Food and Drug Administration. Bacillus cereus. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed 2012. p. 92-5. 13. Lindstrom M, Heikinheimo A, Lahti P, Korkeala H. Novel insights into the epidemiology of Clostridium perfringens type A food poisoning. Food Microbiology. 2011;28(2):192-8. 14. Hennekinne JA, De Buyser ML, Dragacci S. Staphylococcus aureus and its food poisoning toxins: characterization and outbreak investigation. FEMS Microbiology Reviews. 2012;36(4):815-36. 15. Food and Drug Administration. Clostridium botulinum. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed 2012. p. 108-12. 16. Centers for Disease Control and Prevention. Guide to confirming a diagnosis in foodborne disease. 2013 [20/05/15]; Available from: http://www.cdc.gov/foodsafety/outbreaks/investigating-outbreaks/confirming_diagnosis.html. 17. Weingold SE, Guzewich JJ, Fudala JK. Use of Foodborne Disease Data for HACCP Risk Assessment. Journal of Food Protection. 1994;57(9):820-30.

62
18. Australian Bureau of Statistics. Table 4, 3101.0 - Australian Demographic Statistics, Dec 2014. [27/08/2015]; Available from: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3101.0Dec%202014?OpenDocument. 19. Food and Drug Administration. Staphylococcus aureus. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed 2012. p. 87-91. 20. Kirk MD, Veitch MG, Hall GV. Gastroenteritis and food-borne disease in elderly people living in long-term care. Clinical Infectious Diseases: an official publication of the Infectious Diseases Society of America. 2010;50(3):397-404. 21. Trinh C, Prabhakar K. Diarrheal diseases in the elderly. Clinics in Geriatric Medicine. 2007;23(4):833-56, vii. 22. Kirk MD, Lalor K, Raupach J, Combs B, Stafford R, Hall GV, et al. Food- and waterborne disease outbreaks in Australian long-term care facilities, 2001-2008. Foodborne Pathogens and Disease. 2011;8(1):133-9. Epub 2010/11/03. 23. Gilbert RJ, Parry JM. Serotypes of Bacillus cereus from outbreaks of food poisoning and from routine foods. The Journal of Hygiene. 1977;78(1):69-74. 24. Le Loir Y, Baron F, Gautier M. Staphylococcus aureus and food poisoning. Genetics and Molecular Research. 2003;2(1):63-76. 25. Grass JE, Gould LH, Mahon BE. Epidemiology of foodborne disease outbreaks caused by Clostridium perfringens, United States, 1998-2010. Foodborne Pathogens and Disease. 2013;10(2):131-6. 26. Ryan MJ, Wall PG, Adak GK, Evans HS, Cowden JM. Outbreaks of infectious intestinal disease in residential institutions in England and Wales 1992-1994. The Journal of Infection. 1997;34(1):49-54. 27. Levine WC, Smart JF, Archer DL, Bean NH, Tauxe RV. Foodborne disease outbreaks in nursing homes, 1975 through 1987. JAMA: the Journal of the American Medical Association. 1991;266(15):2105-9. 28. Pires SM, Vigre H, Makela P, Hald T. Using outbreak data for source attribution of human salmonellosis and campylobacteriosis in Europe. Foodborne Pathogens and Disease. 2010;7(11):1351-61.

63
Appendix 1: Data dictionary for Outbreak Register fields used Data field Description Example responses
state Jurisdiction reporting the outbreak
ACT NSW NT QLD SA TAS VIC WA
onset_date Date of onset of first case date
aetiology Implicated bacteria or bacterial group
Bacillus cereus Staphylococcus aureus Clostridium perfringens preformed toxin in vivo toxin toxin
confirmation Confirmation of aetiology Confirmed Suspected
ill Number of cases Numeric
hospitalisations Number of cases hospitalised during outbreaks Numeric
deaths Number of deaths of cases Numeric age Median age of cases Numeric male Percent of cases who were male Numeric
female Percent of cases who were female Numeric
incubation Median of the incubation periods reported by cases Numeric
duration Median of the duration of illness reported by cases Numeric
nausea Was nausea reported by any cases? Yes
sym_nausea How many people reported nausea Numeric
nausea_number How many people were interviewed about nausea Numeric
vomiting Was vomiting reported by any cases? Yes
sym_vomit How many people reported vomiting Numeric
vomit_number How many people were interviewed about vomiting Numeric
diarrhoea Was diarrhoea reported by any cases? Yes
sym_diarrhoea How many people reported diarrhoea Numeric
diarrhoea_number How many people were interviewed about diarrhoea Numeric
bloody Was bloody diarrhoea reported by any cases? Yes
sym_bloody How many people reported bloody diarrhoea Numeric
bloody_number How many people were interviewed about bloody diarrhoea
Numeric

64
Data field Description Example responses
fever Was fever reported by any cases? Yes
sym_fever How many people reported fever Numeric
fever_number How many people were interviewed about fever Numeric
abdo Was abdominal pain reported by any cases? Yes
sym_abdo How many people reported abdominal pain Numeric
abdo_number How many people were interviewed about abdominal pain
Numeric
reverse Was reverse temperature reported by any cases? Yes
sym_reverse How many people reported reverse temperature Numeric
reverse_number How many people were interviewed about reverse temperature
Numeric
pain Was joint and muscle pain reported by any cases? Yes
sym_pain How many people reported joint and muscle pain Numeric
pain_number How many people were interviewed about joint and muscle pain
Numeric
numb Was numbness and tingling reported by any cases? Yes
sym_numb How many people reported numbness and tingling Numeric
numb_number How many people were interviewed about numbness and tingling
Numeric
itch Was itching reported by any cases? Yes
sym_itch How many people reported itching Numeric
itch_number How many people were interviewed about itching Numeric
rash Was rash reported by any cases? Yes
sym_rash How many people reported rash Numeric
rash_number How many people were interviewed about rash Numeric
food_vehicle What food was implicated in the outbreak free text
lab_evid Was there any laboratory evidence to implicate the food vehicle? i.e. isolation of pathogen from food
Yes No
stat_evid Was there any statistical evidence to implicate the food vehicle? i.e. analytical study resulting in an OR or RR
Yes No
comp_evid Was there any compelling evidence to implicated the food vehicle? e.g. telltale symptoms, only one food eaten by all cases
Yes No

65
Data field Description Example responses etc
other_evid Was there any other evidence to implicated the food vehicle?
Yes No
cont_factor1 cont_factor2
The major factors contributing to contamination of the food vehicle. Two can be listed
Cross contamination from raw ingredients Food handler contamination Inadequate cleaning of equipment Ingestion of contaminated raw products Other source of contamination person to food to person Storage in contaminated environment Toxic substance or part of tissue Unknown
grow_factor1 grow_factor2
The major factors contributing to growth of the contaminant in the food vehicle. Two can be listed
Foods left at room or warm temperature Slow cooling Inadequate refrigeration Delay between preparation and consumption Insufficient cooking Inadequate thawing Inadequate hot holding temperature Anaerobic packaging/modified atmosphere Other source of contamination Unknown
surv_factor1 surv_factor2
The major factors contributing to survival of the contaminant in the food vehicle. Two can be listed
Insufficient time/temperature during cooking Insufficient time/temperature during reheating Inadequate or failed disinfection Inadequate acidification Inadequate thawing and cooking Other source of contamination Unknown
contevid1 contevid2 growevid1 growevid2 survevid1 survevid2
The level of evidence obtained for the contaminating factor (contevid1 and contevid2), growth factor (growevid1 and growevid2) and survival factor (survevid1 and survevid2)
Assumed/suspected Confirmed by observation during inspection Confirmed verbally during inspection Confirmed with measured evidence Unknown

66
Data field Description Example responses
preparation setting Setting in which the implicated food was prepared
Aged care Camp Child care Commercial caterer Commercially manufactured Fair/festival/mobile service Grocery store/delicatessen Hospital Institution Military National franchised fast food restaurant Other Private caterer Private residence Restaurant School Take-away Unknown
setting eaten Setting in which the implicated food was eaten
Aged care Camp Child care Commercial caterer Community Cruise/airline Fair/festival/mobile service Function Health spa/resort Hospital Institution Military National franchised fast food restaurant Other Picnic Private residence Restaurant School Unknown

67
Appendix 2: Tables showing assessments of probable toxin types for suspected outbreaks Table 15: Informative variables and assessment of probable toxin type for suspected S. aureus
outbreaks
Incubation (hr)*
Vomiting (%)*
Diarrhoea (%)* Food vehicle Probable toxin
2 40 80 Unknown Unknown
3 100 60 Multiple including rice, meat (roast) S. aureus
4 80 100 Vietnamese pork rolls S. aureus 6 0 100 Meatballs, rice, chicken souvlaki in vivo toxin 6 100 75 Unknown S. aureus 6 67 67 Sushi Roll S. aureus 8 67 56 Ham pizza S. aureus
Table 16: Informative variables and assessment of probable toxin type for suspected C.
perfringens outbreaks
Incubation (hr)*
Vomiting (%)*
Diarrhoea (%)* Food vehicle Aged
Care Probable
toxin 6 0 100 Curry No C. perfringens
8 0 100 Beef Rendang and coconut rice No C. perfringens
8 0 100 Pea and ham soup No C. perfringens 9 0 100 Lamb curry No C. perfringens 9 2 100 Curry No C. perfringens
10 0 100 Curried rice and tofu curry No C. perfringens
10 0 100 Curry No C. perfringens 10 4 99 Unknown No C. perfringens 10 4 100 Vegetable and chilli dish No C. perfringens
11 0 93 Lamb curry No C. perfringens
12 0 45 Roast beef No C. perfringens 12 0 100 Unknown No C. perfringens 12 0 100 Unknown Yes C. perfringens 12 0 100 Unknown No C. perfringens
12 4 92
Various Indian dishes - rice, beef madras, butter
chicken, lamb Rogan josh, vegetable curry
No C. perfringens
12 14 100 Chicken curry No C. perfringens 12 30 95 Chicken vol au vents No C. perfringens 13 0 100 Lasagne suspected No C. perfringens
13 10 100 Multiple meat based
foods, solid masses and roast style
No C. perfringens
14 0 100 Chicken curry No C. perfringens 14 0 100 Multiple including curry No C. perfringens

68
Incubation (hr)*
Vomiting (%)*
Diarrhoea (%)* Food vehicle Aged
Care Probable
toxin and rice dishes
14 6 100 Meat curry No C. perfringens 14 19 94 Spaghetti Bolognaise No C. perfringens 14 - - Unknown No C. perfringens 15 0 80 Potato & Gravy No C. perfringens 15 0 100 Stews and curries No C. perfringens
17 0 90 Roast meats, salads, desserts No C. perfringens
17 67 100 Gravy No C. perfringens 120 0 100 Unknown No not a toxin 576 0 100 Unknown No not a toxin
- 0 67 Unknown Yes insufficient information
- 0 79 Yellow rice No insufficient information
- 0 81 Unknown No insufficient information
- 0 90 Unknown No insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Roast beef Yes insufficient information
- 0 100 Unknown No insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient

69
Incubation (hr)*
Vomiting (%)*
Diarrhoea (%)* Food vehicle Aged
Care Probable
toxin information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Lamb chops and roast beef Yes insufficient
information
- 0 100 Beef/lamb kebab No insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Pork and gravy No insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Vitamised food Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Vitamised food Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Unknown Yes insufficient information
- 0 100 Vitamised food Yes insufficient information
- 5 100 Vitamised food Yes insufficient information
- 6 100 Vitamised food Yes insufficient information
- 7 86 Unknown Yes insufficient information
- 8 100 Unknown Yes insufficient information
- 10 90 Unknown Yes insufficient information
- 10 100 Unknown Yes insufficient information
- 11 96 Unknown Yes insufficient information
- 11 100 Unknown Yes insufficient information
- 11 100 Unknown Yes insufficient information
- 11 100 Unknown Yes insufficient

70
Incubation (hr)*
Vomiting (%)*
Diarrhoea (%)* Food vehicle Aged
Care Probable
toxin information
- 12 100 Unknown Yes insufficient information
- 13 100 Unknown Yes insufficient information
- 13 100 Unknown Yes insufficient information
- 14 100 Unknown Yes insufficient information
- 17 92 Unknown Yes insufficient information
- 17 100 Unknown Yes insufficient information
- 17 100 Vitamised food Yes insufficient information
- 20 100 Lasagne Yes insufficient information
- 20 100 Unknown Yes insufficient information
- 25 86 Unknown Yes insufficient information
- 25 100 Unknown Yes insufficient information
- - - Unknown No insufficient information
Table 17: Informative variables and assessment of possible toxin type for suspected preformed
toxin, in vivo toxin and toxin groups
Category Incubation (hr)
Vomiting (%)*
Diarrhoea (%)* Food vehicle Probable toxin
type preformed
toxin 1 100 0 Fried rice or Singapore noodles B.cereus
preformed toxin 2 86 86 Fried rice, pipis B.cereus
preformed toxin 2 100 50
Crumbed chicken pieces, sweet corn and chicken soup
preformed toxin
preformed toxin 4 21 64 Lasagne Unknown
preformed toxin 4 50 0
Japanese food including tempura,
rice, yakitori
preformed toxin
preformed toxin 4 80 0 Unknown preformed
toxin preformed
toxin 4 100 100 Unknown preformed toxin
preformed toxin 4 100 25 Cooked pasta preformed
toxin preformed
toxin 5 71 71 Mango sticky rice preformed toxin
preformed toxin 6 75 75 Unknown preformed
toxin preformed 7 17 50 Gravy in vivo toxin

71
Category Incubation (hr)
Vomiting (%)*
Diarrhoea (%)* Food vehicle Probable toxin
type toxin
preformed toxin 7 40 80 Unknown in vivo toxin
preformed toxin 12 100 0 Unknown Unknown
preformed toxin 15 50 100 Unknown in vivo toxin
in vivo toxin 11 12 100 Seafood mornay and rice dish in vivo toxin
in vivo toxin 12 0 100 Unknown in vivo toxin
in vivo toxin 12 0 100 Butter chicken or boiled rice in vivo toxin
in vivo toxin 12 0 100 Unknown in vivo toxin
in vivo toxin 12 4 100 Potato bake and BBQ chicken in vivo toxin
in vivo toxin 14 0 89 Chicken stirfry or beef massaman in vivo toxin
in vivo toxin 16 0 100 Raw capsicum,
onions, fresh herbs, chicken and/or beef
in vivo toxin
in vivo toxin 16 0 100 Roast chicken and/or stuffing in vivo toxin
in vivo toxin 22 25 100 Beef or lamb kebab in vivo toxin
in vivo toxin - 31 92 Unknown insufficient information
toxin 1 25 50 Pasta with tomato sauce Unknown
toxin 2 67 0 Fish and chips and salad
preformed toxin
toxin 2 100 100 Unknown preformed toxin
toxin 4 60 80 Unknown preformed toxin
toxin 4 67 67 Potato salad preformed toxin
toxin 4 80 40 Feta preformed toxin
toxin 4 100 100 Special fried rice preformed toxin
toxin 4 100 100 Fish preformed toxin
toxin 5 33 67 Sashimi Unknown
toxin 6 100 100 Rice preformed toxin
toxin 6 - - Karaage chicken and rice
Insufficient information
toxin 7 0 100 Pork belly, polenta, shallot tart in vivo toxin
toxin 8 0 100 Beef taco in vivo toxin toxin 8 0 100 Thai fish dish with rice in vivo toxin toxin 9 0 100 Chicken and aioli roll in vivo toxin toxin 10 0 100 Fried rice in vivo toxin

72
Category Incubation (hr)
Vomiting (%)*
Diarrhoea (%)* Food vehicle Probable toxin
type
toxin 10 40 100 Beef, chicken, bean and rice dishes in vivo toxin
toxin 11 0 100 Unknown in vivo toxin toxin 12 0 83 Unknown in vivo toxin toxin 12 0 100 Lamb curry and rice in vivo toxin toxin 12 33 67 Unknown in vivo toxin
toxin 12 100 60 Pizza (meat lovers or chicken) in vivo toxin
toxin 13 9 94 Curried Prawns in vivo toxin toxin 13 50 50 Unknown in vivo toxin toxin 14 0 100 Mushroom sauce in vivo toxin toxin 15 100 100 Chicken doner kebab in vivo toxin toxin 16 80 100 Unknown in vivo toxin
toxin - 0 - Unknown Insufficient information
toxin - 0 100 Unknown Insufficient information
toxin - 17 100 Unknown Insufficient information
toxin - 31 46 Smorgasbord with seafood
Insufficient information
toxin - 54 77 Unknown Insufficient information
toxin - - - Sweet and sour pork or chow mein beef
Insufficient information

73
Appendix 3: Advanced draft of a paper for publication in Communicable Diseases Intelligence Epidemiology of bacterial toxin mediated foodborne gastroenteritis outbreaks in Australia, 2001 to 2013
Dr Fiona J May1, Dr Benjamin G Polkinghorne2 and Dr Emily J Fearnley3
1 Master of Philosophy in Applied Epidemiology Scholar, National Centre for
Epidemiology and Population Health, Research School of Population Health, College of
Medicine, Biology and Environment, Australian National University and Australian
Government Department of Health
2 OzFoodNet Coordinating Epidemiologist, Australian Government Department of
Health
3 Research Fellow, National Centre for Epidemiology and Population Health, Research
School of Population Health, College of Medicine, Biology and Environment, Australian
National University
Corresponding author:
Dr Fiona J May
Queensland Health
PO Box 2368
Fortitude Valley BC QLD 4006
Phone: 07 3328 9077
Email: [email protected]
Word count:
Abstract: 249
Main text: 2964

74
Abstract Bacterial toxin mediated foodborne outbreaks, such as those caused by Clostridium
perfringens, Staphylococcus aureus and Bacillus cereus, are an important and
preventable cause of morbidity and mortality. Due to the short incubation period and
duration of illness, these outbreaks are often underreported. This is the first study to
describe the epidemiology of bacterial toxin mediated outbreaks in Australia. Using
data collected between 2001 and 2013, we identify high risk groups and risk factors to
inform prevention measures.
Descriptive analyses of confirmed bacterial toxin mediated outbreaks between 2001
and 2013 were undertaken using data extracted from the OzFoodNet Outbreak
Register, a database of all outbreaks of gastrointestinal disease investigated by public
health authorities in Australia.
A total of 107 laboratory confirmed bacterial toxin mediated outbreaks were reported
between 2001 and 2013, affecting 2219 people, including 47 hospitalisations and 13
deaths. Twelve deaths occurred in residents of aged care facilities. Clostridium
perfringens was the most commonly reported aetiological agent (81 outbreaks, 76%).
The most commonly reported food preparation settings were commercial food
preparation services (51 outbreaks, 48%) and aged care facilities (42 outbreaks, 39%).
Bacterial toxin outbreaks were rarely associated with food preparation in the home (two
outbreaks, 2%). In all outbreaks, the primary factor contributing to the outbreak was
inadequate temperature control of the food.
Public health efforts aimed at improving storage and handling practices for pre-cooked
and re-heated foods, especially in commercial food preparation services and aged care
facilities, could help to reduce the magnitude of bacterial toxin outbreaks.
Introduction
Two different types of bacterial toxins can cause gastroenteritis. Preformed toxins are
produced by Staphylococcus aureus and Bacillus cereus (emetic toxin). (1, 2) These
toxins are formed in the food and are resistant to heat, so the risk of illness is not
removed by cooking. (3, 4) Onset of illness is rapid, between 30 minutes and six hours,
and vomiting is the most commonly reported symptom. (3) In vivo toxins are produced
by Clostridium perfringens and B. cereus (diarrhoeal toxin), and are formed in the
digestive tract after food containing the bacteria is consumed. While adequately
cooking food can kill the bacteria, both C. perfringens and B. cereus produce heat-
resistant spores which can survive cooking and subsequently regerminate after

75
cooking. Onset of illness is between six and 16 hours. Diarrhoea is commonly reported
and vomiting is not common. (5, 6) All three toxin producing bacteria are ubiquitous in
the environment, and S. aureus is a normal component of human flora. (7)
Individual cases of S. aureus, B. cereus and C. perfringens gastroenteritis are not
notifiable diseases in Australia, so gastroenteritis caused by these pathogens are only
reported if they are part of an outbreak, defined as two or more cases of the same
illness with a common source. Gastrointestinal outbreaks are collated in the national
OzFoodNet Outbreak Register.
OzFoodNet was established in 2000 by the Australian Government as a network of
epidemiologists with representatives in every state and territory. OzFoodNet focuses
on enhanced surveillance for foodborne illnesses. (8) The OzFoodNet Outbreak
Register is a Microsoft Access database maintained by OzFoodNet Central (at the
Australian Government Department of Health), and has been in use since 2001. State
and territory-based OzFoodNet epidemiologists collect and provide summary data
quarterly to OzFoodNet Central on all gastrointestinal outbreaks investigated in their
jurisdiction. Summaries of outbreaks are published in OzFoodNet quarterly and annual
reports (9, 10).
The aim of this study was to describe the epidemiology of bacterial toxin mediated
foodborne outbreaks in Australia between 2001 and 2013, and to identify high risk
groups and risk factors to inform prevention measures.
Methods
Data collection
Outbreak Register data were extracted on 2 February 2015. Variables analysed
included aetiology, laboratory confirmation of aetiology, food vehicle, state or territory
of outbreak, year of outbreak, number of cases, number hospitalised, number of
deaths, median age of cases, percent of cases for each gender, median incubation
period and duration, number of cases reporting each symptom, factors contributing to
the outbreak (microbial growth and microbial survival), the setting in which food was
prepared, the consumption setting and the free text remarks variable. Application of
inclusion and exclusion criteria was performed in Microsoft Excel, and data cleaning
and analysis was performed in StataSE 13 (Stata Corp, College Station, TX, USA).
Missing data, nonsensical data and answers of “unknown” were treated as unknown
responses. Completeness for all variables was defined as useable data, i.e. values
other than missing or unknown.

76
Case definitions
OzFoodNet defines an outbreak as foodborne if there was microbiological evidence
(isolation of the pathogen in the food) and/or analytical epidemiological evidence that
implicated the meal or food as the source of the outbreak. A suspected foodborne
outbreak is defined as an outbreak where descriptive epidemiological evidence
implicated a meal or food as the source of the outbreak. Foodborne and suspected
foodborne outbreaks were included in this study.
All confirmed bacterial toxin outbreaks included in this analysis were laboratory
confirmed according to simplified Centers for Disease Control and Prevention (CDC)
guidelines for bacterial toxin outbreaks. (11) Outbreaks were classified as laboratory
confirmed if the aetiological agent was isolated or enterotoxin was detected in clinical
specimens from two or more cases, or at least 105 organisms were isolated per gram of
epidemiologically implicated food. (11) Confirmed bacterial toxin mediated foodborne or
suspected foodborne outbreaks with onset between 2001 and 2013 were included.
Five aetiology categories were created for analysis:
1. “Bacillus cereus” – B. cereus was listed as the sole aetiology.
2. “Clostridium perfringens” – C. perfringens was listed as the sole aetiology.
3. “Staphylococcus aureus” – S. aureus was listed as the sole aetiology.
4. “Preformed toxin” – both S. aureus and B. cereus were listed as the confirmed
aetiology.
5. “In vivo toxin” – both C. perfringens and B. cereus were listed as the confirmed
aetiology.
For further attribution of outbreaks caused by B. cereus, the following criteria based on
the known characteristics of B. cereus illness were used as probable case definitions
(2):
a. Emetic B. cereus
i. incubation period ≤ 6 hours and
ii. ≥ 50% of cases reporting vomiting
b. Diarrhoeal B. cereus
i. incubation period ≥ 6 hours and
ii. < 50% of cases reporting vomiting
Vehicle attribution
Confirmed or suspected food vehicles with a reasonable level of suspicion (for example
the implicated food was the only food that was eaten by most or all cases) that were
detailed in the Outbreak Register in either the food vehicle variable or in the free-text

77
remarks variable were retained for analysis. To simplify analysis, the food vehicles
were categorised according to the method of food preparation as proposed by
Weingold et al. (12) Only the information provided in the Outbreak Register was used
to apply categories and no assumptions were made about foods commonly served
together. An additional food variable was created to record if a high starch food, such
as rice or pasta, was reported. The number and percentage of outbreaks reporting
each food category are reported.
Data analysis
Median values and ranges were calculated for numerical variables including number of
cases, number of hospitalisations, number of deaths, median age, percentage of each
gender, median incubation period and duration and percentage for each symptom.
Histograms were constructed in Microsoft Excel using outbreak data aggregated by
year based on onset date of the outbreak. Overall rates for each state and territory
were calculated using population data from the Australian Bureau of Statistics (13), and
compared using Poisson regression using StataSE 13. A p-value less than 0.05 was
considered significant.
The percent incidence of symptoms was calculated using the number of cases
reporting the illness as the numerator, and the number of cases interviewed about the
symptom as the denominator, where possible. For outbreaks where the number of
cases reporting the symptoms was higher than the number interviewed, or the number
interviewed was missing, the total number ill was used as the denominator. If an
outbreak had no information for any symptom, the percentage of each symptom was
reported as missing.
Results
A total of 107 confirmed bacterial toxin mediated outbreaks were reported during the
period 2001 to 2013, affecting 2219 people across all states and territories with the
exception of Tasmania. Of these people, 47 were hospitalised and 13 died; 12 deaths
(92%) were in residents of aged care facilities. The number of outbreaks per year by
jurisdiction is shown in Figure 1. Victoria (VIC) had more outbreaks than any other
state (46 outbreaks, 43%), followed by Queensland (QLD; 29 outbreaks, 27%) and
New South Wales (NSW; 22 outbreaks 21%). The rate of bacterial toxin mediated
outbreaks reported per ten million people for each state or territory is shown in Table 1.
Comparing the rates for the states with 20 or more outbreaks, VIC (6.8 outbreaks per
ten million) reported 2.8 times as many bacterial toxin mediated outbreaks than NSW
(2.5 outbreaks per ten million), and 1.3 times as many outbreaks as QLD (5.4

78
outbreaks per ten million). Only the comparison between NSW and VIC was significant
(p-value <0.001).
Figure 1: Laboratory confirmed bacterial toxin mediated outbreaks by year and state or territory,
Australia, 2001 to 2013. ACT – Australian Capital Territory; NSW – New South Wales; NT –
Northern Territory; QLD – Queensland; SA – South Australia; TAS – Tasmania; VIC – Victoria;
WA – Western Australia
Table 1: Rate of laboratory confirmed bacterial toxin mediated outbreaks reported per ten million people for each Australian state and territory, 2001 to 2013
State or Territory*
Number of outbreaks
Rate per 10 million people
Incidence rate ratio
95% Confidence Interval
p-value
VIC 46 6.8 reference reference reference QLD 29 5.4 0.78 0.50 – 1.27 0.34 NT 1 3.5 0.52 0.07 – 3.77 0.52
NSW 22 2.5 0.36 0.22 – 0.60 <0.001 WA 7 2.5 0.15 0.17 – 0.82 0.014 ACT 1 2.2 0.33 0.05 – 2.37 0.27 SA 1 0.5 0.07 0.01 – 0.52 0.01
TAS 0 0 0.00 0 0.996 * ACT – Australian Capital Territory; NSW – New South Wales; NT – Northern Territory; QLD – Queensland; SA – South Australia; TAS – Tasmania; VIC – Victoria; WA – Western Australia Figure 2 shows the number of outbreaks reported each year, by aetiology. Outbreaks
caused by C. perfringens were the most frequently reported cause of bacterial toxin
mediated outbreaks (81 outbreaks, 76%; Figure 2, Table 2). All but one of the deaths

79
associated with a bacterial toxin mediated outbreak was during an outbreak caused by
C. perfringens (12 deaths, 92%).
Figure 2: Laboratory confirmed bacterial toxin mediated foodborne outbreaks, by aetiology and year, Australia 2001-2013

80
Tabl
e 2:
Epi
dem
iolo
gy o
f bac
teria
l tox
in m
edia
ted
outb
reak
s, b
y co
nfirm
ed o
r sus
pect
ed a
etio
logy
, Aus
tralia
, 200
1 to
201
3
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n
Num
ber o
f out
brea
ks
16
6 81
2
2 To
tal n
umbe
r of c
ases
20
0 11
4 15
33
288
84
Med
ian
num
ber o
f cas
es p
er o
utbr
eak
(rang
e)
8 (2
-38)
18
(3-3
7)
13 (2
-100
) 14
4 (1
6-27
2)
42 (9
-75)
H
ospi
talis
atio
ns
18†
0*
14†
15*
0*
Dea
ths
1*
0*
12*
0*
0*
Perc
ent o
f out
brea
ks w
ith o
ne o
r mor
e de
aths
6.
3*
0*
6.2*
0*
0*
M
edia
n pe
rcen
t ill
(rang
e)
48 (1
3.3-
88.9
)‡ 26
(14.
8-32
.0)‡
19 (0
.7-1
00)†
8 (8
.4)‡
52 (4
.1-1
00)*
M
edia
n ag
e 31
† 36
‡ 81
† 39
* 20
‡
Med
ian
perc
ent s
ex
Mal
e 39
† 41
‡ 34
† 0§
50‡
Fem
ale
62†
59‡
66†
0§ 50
‡ * ≥
90%
com
plet
e
† 75
– 89
% c
ompl
ete
‡ 50
– 7
4% c
ompl
ete

81
Symptomology
Outbreaks caused by S. aureus had the shortest median incubation period (three hours) of
the three types of bacterial infection (Table 3), while outbreaks caused by C. perfringens had
the longest median incubation period (12 hours). Duration of illness was comparable
between outbreaks caused by the different pathogens. Diarrhoea was the most commonly
reported symptom in all outbreaks. Vomiting and nausea were most common in outbreaks
caused by S. aureus.

82
Tabl
e 3:
Incu
batio
n pe
riod,
dur
atio
n of
illn
ess
and
med
ian
perc
ent o
f com
mon
ly re
porte
d sy
mpt
oms
in b
acte
rial t
oxin
med
iate
d fo
odbo
rne
outb
reak
s by
ae
tiolo
gy, A
ustra
lia 2
001-
2013
Stap
hylo
cocc
us a
ureu
s B
acill
us c
ereu
s C
lost
ridiu
m p
erfr
inge
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n m
edia
n ra
nge
med
ian
rang
e m
edia
n ra
nge
med
ian
rang
e m
edia
n ra
nge
Incu
batio
n pe
riod
(hou
rs)
3*
2-7
8.5*
2-
12
12±
6-17
4*
2-
6 12
‡ 12
-12
Dur
atio
n of
illn
ess
(hou
rs)
18‡
3-72
23
.5‡
0-48
24
† 3-
204
24‡
24-2
4 36
* 24
-48
Dia
rrhoe
a (%
) 82
† 0-
100
97*
0-10
0 10
0*
53-1
00
86*
72-1
00
100*
10
0-10
0 Ab
dom
inal
pai
n (%
) 67
† 0-
100
35*
0-88
0*
0-
100
88*
76-1
00
33*
0-67
Vo
miti
ng (%
) 10
0† 43
-100
14
* 0-
100
0*
0-74
66
* 50
-83
0*
0-0
Nau
sea
(%)
83†
0-10
0 29
* 0-
100
0*
0-10
0 87
* 74
-100
0*
0-
0 * ≥
90%
com
plet
e † 7
5 –
89%
com
plet
e ‡ 50
– 7
4% c
ompl
ete

83
Food vehicle attribution
The most frequently reported category of food associated with bacterial toxin mediated
foodborne outbreaks was the category of “solid masses of potentially hazardous foods”,
such as lasagne, which was reported in 31 outbreaks (29%) (Table 4). An additional 17
outbreaks (16%) were associated with “liquid or semi-solid mixtures of potentially hazardous
foods”, such as gravy. Half of the outbreaks (13 outbreaks) caused by S. aureus, B. cereus,
preformed toxin and in vivo toxin had a starch-based food such as rice, pasta or noodles
listed as part of the implicated food vehicle, whereas only five outbreaks (6%) caused by C.
perfringens had starch as part of the food vehicle.

84
Tabl
e 4:
Foo
d ca
tego
ries
impl
icat
ed in
toxi
n m
edia
ted
outb
reak
s, A
ustra
lia 2
001
to 2
013
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n
%
n %
n
%
n %
n
%
n So
lid m
asse
s of
pot
entia
lly h
azar
dous
fo
ods
43
7 50
3
24
19
50
1 50
1
Liqu
id o
r sem
i-sol
id m
ixtu
res
of
pote
ntia
lly h
azar
dous
food
s 6
1 33
2
16
13
0 0
50
1
Roa
sted
mea
t/pou
ltry/
fish
19
3 0
0 7
6 0
0 0
0 C
ook/
serv
e fo
ods
13
2 0
0 4
3 0
0 0
0 Sa
lads
pre
pare
d w
ith o
ne o
r mor
e co
oked
ingr
edie
nts
6 1
0 0
0 0
0 0
0 0
Sala
ds w
ith ra
w in
gred
ient
s 0
0 0
0 0
0 0
0 0
0 M
ultip
le fo
ods
0 0
17
1 0
0 50
1
0 0
Bake
d go
ods
6 1
0 0
3 2
0 0
0 0
Sand
wic
hes
0 0
0 0
0 0
0 0
0 0
Beve
rage
s 6
1 0
0 0
0 0
0 0
0 U
nkno
wn
food
veh
icle
0
0 0
0 47
38
0
0 0
0

85
Contributing factors
All bacterial toxin mediated outbreaks that had a contributing factor for microbial growth
recorded (63 outbreaks) had at least one contributing factor for microbial growth that can be
categorised as temperature abuse, including “slow cooling”, “inadequate refrigeration”,
“delay between preparation and consumption”, “insufficient cooking”, “inadequate thawing”
or “inadequate hot holding temperature” (Table 5). Similarly, 85% of outbreaks that had a
contributing factor for microbial survival (40 of 47 outbreaks) had a contributing factor for
microbial survival that can be categorised as temperature abuse, including “insufficient
time/temperature during cooking”, “insufficient time/temperature during reheating” or
“inadequate thawing and cooking” (Table 6).

86
Tabl
e 5:
Con
tribu
ting
fact
ors
for m
icro
bial
gro
wth
afte
r con
tam
inat
ion
of fo
od v
ehic
le, A
ustra
lia 2
001
to 2
013
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n
%
n %
n
%
n %
n
%
n Fo
ods
left
at ro
om o
r war
m
tem
pera
ture
56
9
33
2 16
13
10
0 2
100
2
Inad
equa
te re
frige
ratio
n 38
6
17
1 11
9
50
1 0
0 Sl
ow c
oolin
g 6
1 0
0 30
24
0
0 0
0 D
elay
bet
wee
n pr
epar
atio
n an
d co
nsum
ptio
n 6
1 17
1
12
10
50
1 50
1
Inad
equa
te h
ot h
oldi
ng
tem
pera
ture
13
2
33
2 2
2 0
0 50
1
Insu
ffici
ent c
ooki
ng
0 0
33
2 1
1 0
0 0
0 In
adeq
uate
thaw
ing
0 0
0 0
0 0
0 0
0 0
Anae
robi
c pa
ckag
ing/
mod
ified
at
mos
pher
e 0
0 0
0 0
0 0
0 0
0
Oth
er s
ourc
e of
con
tam
inat
ion
0 0
0 0
0 0
0 0
0 0
Unk
now
n 19
3
17
1 49
40
0
0 0
0

87
Tabl
e 6:
Con
tribu
ting
fact
ors
for m
icro
bial
sur
viva
l afte
r con
tam
inat
ion
of fo
od v
ehic
le, A
ustra
lia 2
001
to 2
013
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n
%
n %
n
%
n %
n
%
n In
suffi
cien
t tim
e/te
mpe
ratu
re
durin
g re
heat
ing
0 0
33
2 41
33
0
0 0
0
Insu
ffici
ent t
ime/
tem
pera
ture
du
ring
cook
ing
6 1
33
2 5
4 0
0 10
0 2
Oth
er s
ourc
e of
con
tam
inat
ion
13
2 17
1
2 2
100
2 0
0 In
adeq
uate
or f
aile
d di
sinf
ectio
n 6
1 0
0 0
0 0
0 50
1
Inad
equa
te a
cidi
ficat
ion
0 0
0 0
0 0
0 0
0 0
Inad
equa
te th
awin
g an
d co
okin
g 0
0 0
0 0
0 0
0 0
0
Unk
now
n 75
12
33
2
56
45
50
1 0
0

88
Food preparation and consumption settings
The food implicated in bacterial toxin foodborne outbreaks was prepared and eaten in the
same location for 78 outbreaks (73%). The implicated food in the remaining 29 outbreaks
(27%) was prepared in a commercial location before being eaten in the home, for example
eating a take-away meal from a restaurant at home. The most commonly reported food
preparation locations for all aetiologies were restaurants (21 outbreaks, 20%) and
commercial caterers (16 outbreaks, 15%; Table 7). Only two outbreaks (2%) were due to
food prepared in a private home. Food preparation businesses (including restaurants,
commercial caterers, take-away locations, grocery stores, delicatessens, fairs, festivals and
mobile food services) were the most commonly reported food preparation setting associated
with bacterial toxin mediated foodborne outbreaks, (51 outbreaks, 48%). A total of 42
outbreaks (39%), all caused by C. perfringens (alone or with B. cereus in the in vivo toxin
category), were associated with meals prepared and/or consumed in aged care facilities
(Table 8). The incidence of aged care associated outbreaks varies from year to year, ranging
from no aged care outbreaks in 2001 to 75% of outbreaks in 2013 and a median of 25% of
outbreaks per year. Restaurants were the second most frequently reported location for
consumption of food (21 outbreaks, 20%; Table 8).

89
Tabl
e 7:
Set
ting
whe
re th
e fo
od w
as p
repa
red,
Aus
tralia
200
1 to
201
3
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n
%
n %
n
%
n %
n
%
n Ag
ed c
are
0 0
0 0
47
38
0 0
50
1 R
esta
uran
t 19
3
33
2 19
15
50
1
0 0
Com
mer
cial
cat
erer
25
4
33
2 11
9
0 0
50
1 Ta
ke-a
way
13
2
17
1 2
2 0
0 0
0 H
ospi
tal
0 0
0 0
6 5
0 0
0 0
Inst
itutio
n 0
0 0
0 6
5 0
0 0
0 N
atio
nal f
ranc
hise
d fa
st
food
rest
aura
nt
13
2 17
1
1 1
0 0
0 0
Fair/
fest
ival
/mob
ile s
ervi
ce
6 1
0 0
0 0
50
1 0
0 Pr
ivat
e re
side
nce
0 0
0 0
2 2
0 0
0 0
Oth
er
6 1
0 0
1 1
0 0
0 0
Cam
p 6
1 0
0 0
0 0
0 0
0 C
hild
car
e 6
1 0
0 0
0 0
0 0
0 G
roce
ry s
tore
/del
icat
esse
n 6
1 0
0 0
0 0
0 0
0 M
ilitar
y 0
0 0
0 1
1 0
0 0
0 Pr
ivat
e ca
tere
r 0
0 0
0 1
1 0
0 0
0 U
nkno
wn
0 0
0 0
1 1
0 0
0 0

90
Tabl
e 8:
Set
ting
whe
re th
e fo
od w
as c
onsu
med
, Aus
tralia
, 200
1 to
201
3
St
aphy
loco
ccus
au
reus
B
acill
us c
ereu
s C
lost
ridiu
m
perf
ringe
ns
Pref
orm
ed to
xin
In v
ivo
toxi
n
%
n %
n
%
n %
n
%
n Ag
ed c
are
0 0
0 0
51
41
0 0
50
1 R
esta
uran
t 13
2
33
2 17
14
0
0 0
0 Pr
ivat
e re
side
nce
19
3 50
3
5 4
0 0
0 0
Com
mer
cial
cat
erer
13
2
17
1 4
3 50
1
50
1 O
ther
13
2
0 0
5 4
0 0
0 0
Inst
itutio
n 0
0 0
0 6
5 0
0 0
0 C
omm
unity
13
2
0 0
4 3
0 0
0 0
Hos
pita
l 0
0 0
0 4
3 0
0 0
0 Fa
ir/fe
stiv
al/m
obile
ser
vice
6
1 0
0 0
0 50
1
0 0
Milit
ary
0 0
0 0
1 1
0 0
0 0
Nat
iona
l fra
nchi
sed
fast
food
re
stau
rant
6
1 0
0 0
0 0
0 0
0
Chi
ld c
are
6 1
0 0
0 0
0 0
0 0
Func
tion
6 1
0 0
0 0
0 0
0 0
Cam
p 6
1 0
0 0
0 0
0 0
0 C
ruis
e/ai
rline
0
0 0
0 1
1 0
0 0
0 Sc
hool
0
0 0
0 1
1 0
0 0
0 U
nkno
wn
0 0
0 0
1 1
0 0
0 0

91
Further attribution of B. cereus outbreaks
Using the probable case definition, in particular the percentage of cases that reported
vomiting, one outbreak caused by B. cereus (17%) was likely to have been caused by
the emetic toxin (incubation period 2 hours, 100% of cases reported vomiting), while
the remaining five outbreaks were likely to have been caused by the diarrhoeal toxin
(Table 9).
Table 9: Informative variables and assessment of probable toxin type for confirmed and suspected B. cereus outbreaks (emetic or diarrhoeal), Australia 2001 to 2013 Probable B. cereus toxin type
Incubation (hours)
Symptoms Food vehicle
Vomiting (%) Diarrhoea (%)
Emetic 2 100 0 Fried rice and honey chicken Diarrhoeal 6 0 100 Multiple foods Diarrhoeal 8 16 100 Boiled gefilte fish (fish balls) Diarrhoeal 9 67 67 Mashed Potato & Gravy Diarrhoeal 10 3 97 Rice Diarrhoeal 12 13 96 Rice (and/or beef curry)
Discussion This study was the first to examine the epidemiology of bacterial toxin mediated
foodborne outbreaks in Australia. The incidence of bacterial toxin mediated foodborne
outbreaks fluctuated over the 13 year analysis period (2001 to 2013), but there was no
overall trend in the change in incidence. Victoria reported more outbreaks per 100,000
people caused by bacterial toxins than any other jurisdiction. From the data available, it
is unclear whether this was due to a higher incidence of bacterial toxin mediated
outbreaks in Victoria, or if other factors are involved.
The median incubation periods and symptomology of S. aureus (14), B. cereus (6) and
C. perfingens (5) in Australian outbreaks were similar to that observed elsewhere. Only
one outbreak caused by B. cereus was likely to have been caused by the emetic toxin
(17%). The food vehicle for this outbreak included rice (fried rice and honey chicken),
consistent with findings that the B. cereus emetic toxin is associated with rice. (2, 3, 15)
This distribution of a greater number of diarrhoeal outbreaks than emetic is consistent
with the epidemiology of B. cereus in North America and Northern Europe, and
different to that seen in countries with high rates of rice consumption such as Japan.
(2)
The two most commonly reported food vehicle categories were “solid masses of
potentially hazardous foods” and “liquids or semi-solid mixtures of potentially
hazardous foods”. Without careful temperature control, both of these categories of
foods can spend a long period of time at temperatures that promote microbial growth

92
due to the density of the food. This finding is in contrast with a study examining
bacterial toxin mediated foodborne outbreaks in the United States, which found that
“roasted meat and poultry” was the most commonly reported food category. (16)
All outbreaks that reported a contributing factor for microbial growth and 85% of
outbreaks that reported a contributing factor for microbial survival, reported at least one
factor that was associated with temperature abuse of the food. Temperature abuse
refers to inappropriate holding of food products between 4°C and 60°C, which is the
optimal temperature for growth of most pathogenic microorganisms. (17) This is a
particular problem with toxin producing bacteria, as even reheating or cooking the food
does not remove the preformed toxin (S. aureus and emetic B. cereus) or the bacterial
spores (C. perfringens and diarrhoeal B. cereus). (2, 4, 18)
The most commonly reported location for preparation of the food vehicle that was
implicated in bacterial toxin mediated foodborne outbreaks was at food preparation
businesses such as restaurants and commercial caterers (48%), while the implicated
food was prepared in private homes in only 2% of the outbreaks. This is in contrast to a
study in the United States, which found that 16% of bacterial toxin mediated outbreaks
were associated with food prepared in the home. (16) Similarly, a study in the
European Union found that homes were the most commonly reported setting for
outbreaks of S. aureus and third most commonly reported setting for outbreaks of C.
perfringens. (19) However, this study did not distinguish between preparation and
consumption settings. Education of all food preparation services on safe food practices,
with a focus on increased awareness of temperature abuse of foods that are difficult to
cool or warm rapidly, including high risk dishes would reduce the incidence of bacterial
toxin mediated foodborne outbreaks in food preparation businesses.
The most commonly reported location for preparation and consumption of the food
implicated in C. perfringens outbreaks was aged care facilities (39% of all outbreaks,
51% of C. perfringens outbreaks). Foods in aged care facilities are often prepared in
bulk and stored for a period of time before serving, increasing the risk of bacterial toxin
outbreaks. (20) Food prepared in aged care facilities was not reported as a major risk
factor for bacterial toxin mediated foodborne outbreaks in the United States. (16, 21)
The short duration and mild symptoms associated with bacterial toxin mediated illness
means that cases and outbreaks in the general community are less likely to be
detected and investigated than cases and outbreaks in aged care facilities. However,
residents of aged care facilities are a vulnerable population, and the outcome of
bacterial toxin mediated illnesses may be more severe in the aged care population and
as such, staff are trained to be particularly observant of symptoms of gastroenteritis.

93
(22) Indeed, almost all deaths were associated with bacterial toxin mediated outbreaks
occurred in aged care facilities (92%), consistent with studies showing higher mortality
during foodborne outbreaks in aged care facilities. (20, 23-25) Prevention of bacterial
toxin mediated foodborne outbreaks in aged care facilities through education and
awareness of ways to avoid temperature abuse of food served in aged care facilities is
important in protecting this vulnerable population. Food safety in aged care facilities is
regulated by Food Standards Australia New Zealand Standard 3.3.1 “Food Safety
Programs for Food Service to Vulnerable Persons”
(https://www.comlaw.gov.au/Series/F2012L00290). This standard was introduced in
2008 and requires implementation of a food safety program by food businesses that
prepare food for vulnerable people, including the elderly. However, despite the
introduction of this Standard during the period of this study, there has been no
decrease in the frequency of bacterial toxin mediated outbreaks in aged care facilities.
Only outbreaks that were laboratory confirmed to be caused by a bacterial toxin were
included in this study. As it can be difficult to confirm the causative agent in bacterial
toxin mediated outbreaks, and few laboratories in Australia are able to test for these
pathogens, many outbreaks that were possibly caused by bacterial toxins but not
laboratory confirmed have not been included in this study. This may have biased the
analysis towards outbreaks that were more likely to be confirmed, such as larger
outbreaks, outbreaks in vulnerable populations such as aged care or commercial
enterprises complying with regulations; the results of this study should be considered in
this context. However, a larger study that incorporated suspected outbreaks showed no
differences in the epidemiology of confirmed bacterial toxin mediated outbreaks and
suspected bacterial toxin mediated outbreaks. (26) Similarly, the outbreaks reported in
the OzFoodNet Outbreak Register are likely to be only a proportion of the total number
of outbreaks caused by bacterial toxins, as these outbreaks are often not reported or
investigated due to the short duration and relatively mild symptoms in healthy adults
compared with other infectious causes of foodborne gastroenteritis such as
Salmonella. (27)
In conclusion, bacterial toxin mediated foodborne outbreaks are most frequently
reported to be associated with dense large volume foods prepared by food preparation
businesses such as restaurants, and in aged care facilities. As bacterial toxin mediated
outbreaks disproportionately affect the vulnerable residents of aged care facilities,
education and training of food handlers in these facilities should be a priority.

94
Acknowledgements
The authors would like to thank all the OzFoodNet epidemiologists and the public
health and laboratory staff for their hard work investigating these outbreaks and
providing data to the Outbreak Register, interviewing patients, testing specimens,
typing isolates and investigating outbreaks.
References
1. Argudin MA, Mendoza MC, Rodicio MR. Food poisoning and Staphylococcus aureus enterotoxins. Toxins. 2010;2(7):1751-73. 2. Stenfors Arnesen LP, Fagerlund A, Granum PE. From soil to gut: Bacillus cereus and its food poisoning toxins. FEMS microbiology reviews. 2008;32(4):579-606. 3. Ehling-Schulz M, Frenzel E, Gohar M. Food-bacteria interplay: pathometabolism of emetic Bacillus cereus. Frontiers in microbiology. 2015;6:704. 4. Tranter HS. Foodborne staphylococcal illness. Lancet. 1990;336(8722):1044-6. 5. Food and Drug Administration. Clostridium perfringens. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed2012. p. 83-6. 6. Food and Drug Administration. Bacillus cereus. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed2012. p. 92-5. 7. Hennekinne JA, De Buyser ML, Dragacci S. Staphylococcus aureus and its food poisoning toxins: characterization and outbreak investigation. FEMS microbiology reviews. 2012;36(4):815-36. 8. Kirk MD, McKay I, Hall GV, Dalton CB, Stafford R, Unicomb L, et al. Food safety: foodborne disease in Australia: the OzFoodNet experience. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2008;47(3):392-400. 9. OzFoodNet Working G. Monitoring the incidence and causes of diseases potentially transmitted by food in Australia: Annual report of the OzFoodNet network, 2011. Communicable diseases intelligence quarterly report. 2015;39(2):E236-64. 10. OzFoodNet Working G. OzFoodNet quarterly report, 1 October to 31 December 2013. Communicable diseases intelligence quarterly report. 2015;39(3):E478-84. 11. Centers for Disease Control and Prevention. Guide to confirming a diagnosis in foodborne disease 2013 [20/05/15]. Available from: http://www.cdc.gov/foodsafety/outbreaks/investigating-outbreaks/confirming_diagnosis.html. 12. Weingold SE, Guzewich JJ, Fudala JK. Use of Foodborne Disease Data for HACCP Risk Assessment. Journal of food protection. 1994;57(9):820-30. 13. Australian Bureau of Statistics. Table 4, 3101.0 - Australian Demographic Statistics, Dec 2014 [27/08/2015]. Available from: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/3101.0Dec%202014?OpenDocument. 14. Food and Drug Administration. Staphylococcus aureus. Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins. 2nd ed2012. p. 87-91. 15. Gilbert RJ, Parry JM. Serotypes of Bacillus cereus from outbreaks of food poisoning and from routine foods. The Journal of hygiene. 1977;78(1):69-74. 16. Bennett SD, Walsh KA, Gould LH. Foodborne disease outbreaks caused by Bacillus cereus, Clostridium perfringens, and Staphylococcus aureus--United States, 1998-2008. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2013;57(3):425-33. 17. Food Standards Australia New Zealand. Australia New Zealand Food Standards Code - Standard 3.2.2 - Food Safety Practices and General Requirements (Australia Only). 2014.

95
18. Lindstrom M, Heikinheimo A, Lahti P, Korkeala H. Novel insights into the epidemiology of Clostridium perfringens type A food poisoning. Food microbiology. 2011;28(2):192-8. 19. EFSA (European Food Safety Authority). The European Union summary report on trends and sources of zoonoses, zoonotic agents and food-borne outbreaks in 2014. EFSA Journal 2015. 2015;13(12):4329. 20. Kirk MD, Veitch MG, Hall GV. Gastroenteritis and food-borne disease in elderly people living in long-term care. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2010;50(3):397-404. 21. Grass JE, Gould LH, Mahon BE. Epidemiology of foodborne disease outbreaks caused by Clostridium perfringens, United States, 1998-2010. Foodborne pathogens and disease. 2013;10(2):131-6. 22. Australian Government Department of Social Services. Gastro-Info gastroenteritis kit for aged care: resources to assist residential aged care homes in preventing, identifying and managing outbreaks of gastroenteritis 2014 [16 November 2015]. Available from: https://www.dss.gov.au/our-responsibilities/ageing-and-aged-care/publications-articles/resources-learning-training/gastro-info-gastroenteritis-kit-for-aged-care-resources-to-assist-residential-aged-care-homes-in-preventing-identifying-managing-outbreaks-of-gastroenteritis. 23. Kirk MD, Lalor K, Raupach J, Combs B, Stafford R, Hall GV, et al. Food- and waterborne disease outbreaks in Australian long-term care facilities, 2001-2008. Foodborne pathogens and disease. 2011;8(1):133-9. 24. Levine WC, Smart JF, Archer DL, Bean NH, Tauxe RV. Foodborne disease outbreaks in nursing homes, 1975 through 1987. JAMA : the journal of the American Medical Association. 1991;266(15):2105-9. 25. Ryan MJ, Wall PG, Adak GK, Evans HS, Cowden JM. Outbreaks of infectious intestinal disease in residential institutions in England and Wales 1992-1994. The Journal of infection. 1997;34(1):49-54. 26. May FJ. Epidemiology of foodborne and emerging infectious diseases in Australia, 2014 to 2015: Australian National University; 2015. 27. Kirk M, Ford L, Glass K, Hall G. Foodborne illness, Australia, circa 2000 and circa 2010. Emerging infectious diseases. 2014;20(11):1857-64.

96
Appendix 4: Conference presentation, Communicable Diseases Control Conference, Brisbane 2 June 2015

97

98

99
Chapter 3 Establishment and Evaluation of a National
Surveillance System for Ebola Virus Disease

100
Table of contents Prologue ................................................................................................................ 102
Study rationale ................................................................................................... 102
My Role ............................................................................................................. 102
Lessons learned ................................................................................................ 102
Public health implications of this work ................................................................ 103
Acknowledgements ............................................................................................ 103
Master of Philosophy (Applied Epidemiology) core activity requirement ............. 103
Abstract ................................................................................................................. 103
Introduction ........................................................................................................... 104
Aim and objectives ................................................................................................ 107
Design of surveillance system ............................................................................... 107
Case definition ................................................................................................... 107
Stakeholders ...................................................................................................... 110
System design ................................................................................................... 111
Data collection and analysis ............................................................................... 113
Border surveillance ......................................................................................... 114
Laboratory testing and temperature monitoring .............................................. 114
Case data management system (NetEpi) ....................................................... 115
Other issues and data sources........................................................................... 116
Dissemination .................................................................................................... 117
Results of national surveillance system ................................................................. 117
Methods ............................................................................................................. 117
Border surveillance ............................................................................................ 117
Laboratory testing for EVD infection ................................................................... 122
Temperature monitoring of returned travellers ................................................... 122
Case data management ..................................................................................... 125
Evaluating the surveillance system ........................................................................ 125
Methods ............................................................................................................. 125
Usefulness ......................................................................................................... 128

101
System attributes ............................................................................................... 129
Simplicity ........................................................................................................ 129
Flexibility ........................................................................................................ 131
Data quality .................................................................................................... 131
Acceptability ................................................................................................... 133
Sensitivity ....................................................................................................... 134
Positive predictive value ................................................................................. 135
Representativeness ....................................................................................... 135
Timeliness ...................................................................................................... 135
Stability .......................................................................................................... 137
Discussion ............................................................................................................. 137
Summary of recommendations .............................................................................. 138
Conclusion ............................................................................................................ 139
References ............................................................................................................ 139
Appendix 1: Targeted literature review .................................................................. 142
Appendix 2: Data collection tool for laboratory testing and temperature monitoring148
Appendix 3: Case and contact report forms and data dictionaries ......................... 149
Appendix 4: List of questions for Stakeholders ...................................................... 212

102
Prologue
Study rationale Ebola virus disease (EVD) is a nationally notifiable disease under the disease grouping
of “viral haemorrhagic fever”. In response to the increasing number of cases of EVD in
West Africa in 2014, a variety of additional enhanced active surveillance measures
were implemented across Australia, at national and jurisdictional levels, from August
2014. At the national level, three main components were implemented to provide early
warning to jurisdictions about possible cases, to prevent potential secondary
transmission and to facilitate coordinated national reporting. These three components
were border surveillance and reporting, reporting of jurisdictional laboratory testing and
temperature monitoring, and an outbreak management system for case reporting.
My Role I designed and developed the NetEpi online outbreak management system for
recording cases of EVD and their contacts. I was the Australian Government
Department of Health contact point for jurisdictional representatives to send weekly
EVD laboratory testing and temperature monitoring data to. I then collated the testing
and monitoring data, and prepared and distributed the testing and monitoring reports. I
also distributed the border monitoring reports. In addition, I conducted an evaluation of
all three components of the national EVD surveillance system.
Lessons learned Establishing a surveillance system that involves several different government agencies
and all jurisdictions during the peak of a large and politically sensitive outbreak
provided many lessons. The biggest lesson I learned was that having a basic plan for
what to do in the event of an outbreak would streamline the response. Hopefully the
lessons learned during this outbreak will be applied to future outbreaks.
Through using the system and analysing the data, I also learned a lot about design of
questionnaires and other data collection tools. For example, while it may look nice and
convenient to list all the reporting periods in which a person is being monitored in a
single cell in Excel, when it comes to analysing the absolute number of people being
monitored in a given week, this becomes less convenient (and requires a lot of fiddling
in Stata). Excel doesn’t really provide a better way to record these data – an online
database system would handle this kind of data a lot better due to the ability to handle
complex and interrelated data.
Although feedback on a questionnaire is useful, nothing compares with actually piloting
the questionnaire – even if that means entering some dummy data. During entering of

103
dummy data into both the case and contacts form in NetEpi, I became aware of a few
things that just didn’t work quite right, including requiring additional questions or options
within existing questions to clarify meaning, and was able to fix them.
Public health implications of this work By implementing the EVD national surveillance system, Australia is well prepared for
the public health response associated with a possible importation of a case of EVD. In
addition, the lessons learned from responding to this outbreak and from the evaluation
of the national surveillance system can be applied to future outbreaks of a similar
nature (i.e. where transmission occurs only after symptom onset, so enhanced border
screening and symptom monitoring is useful) that threaten Australia.
Acknowledgements Thanks to everyone who had input into setting up this surveillance system. Katrina
Knope, Julia Mansour, Jenny Firman, Tim Sloan-Gardner, Rob Boseski and everyone
in CDNA. Thanks to all the stakeholders who provided such useful feedback. And of
course, many thanks to my supervisors, Ben Polkinghorne and Emily Fearnley.
Master of Philosophy (Applied Epidemiology) core activity requirement Establish and evaluate a surveillance system.
Literature review that demonstrates skills in conducting a targeted literature search and
synthesis (Appendix 1).
Abstract In response to the large outbreak of Ebola virus disease (EVD) in West Africa during
2014, the Communicable Diseases Network of Australia (CDNA) sought to implement a
nationally coordinated surveillance system for detection and monitoring of people at
risk of developing EVD (i.e. returned travellers from countries with transmission of
EVD) and reporting of those being monitored or laboratory tested.
Screening of returned travellers at the border was initiated in August 2014, with
enhanced screening added on 24 November 2014. Border screening was conducted
by the Department of Agriculture and Water Resources (Department of Agriculture),
with line lists of those screened provided to jurisdictional health departments via the
Australian Government Department of Health. The number of people under monitoring
or tested for EVD infection was reported to the Australian Government Department of
Health by jurisdictions weekly, beginning on 10 October 2014. An online case and
contact data management system was designed for use if a case was detected in
Australia.

104
Evaluation of the national surveillance system was conducted during the second half of
2015 using the Centers for Disease Control and Prevention (CDC) guidelines for
evaluating public health surveillance systems. Assessment of each of the system
attributes utilised discussions with stakeholders and analysis of the data in the system.
In the absence of a case, dummy data were entered into the data management
system.
The three components of the system were designed separately, and as a result the
different components didn’t integrate as seamlessly as a centrally managed online
database. However, most users agreed that the system achieved the goals of
coordination and reporting of enhanced border screening and monitoring for EVD
compatible symptoms in returned travellers in order to detect and prevent
autochthonous transmission of EVD in Australia.
Introduction On 22 March 2014, what has subsequently become the largest outbreak of Ebola virus
disease (EVD) in history was first notified to the World Health Organization (WHO) by
the Ministry of Health, Guinea, as a requirement of the International Health Regulations
(IHR) 2005. At this point, 49 cases including 29 deaths had been reported (1). Thought
to have originated from a child in rural Guinea in December 2013 (2), the outbreak
spread rapidly throughout the West African countries of Guinea, Sierra Leone and
Liberia. The outbreak was declared a Public Health Emergency of International
Concern (PHEIC) by the WHO on 8 August 2014, with 1711 cases including 932
deaths (3). More than 28 600 cases have been reported, including more than 11 300
deaths as at 1 November 2015 (4). The largest previously reported outbreak of EVD
occurred in Uganda in 2000, with 425 cases and 224 deaths (5).
EVD is an illness of humans and primates caused by a group of five viruses in the
genus Ebolavirus, family Filoviridae. Four of the five species of ebolavirus cause
human disease, with case fatality rates varying between 50% and 90% depending on
the species and the outbreak (6). The incubation period can be between two and 21
days, and symptom onset begins with non-specific symptoms including fever,
weakness, diarrhoea, headache, muscle pain, joint pain, vomiting and abdominal pain,
progressing to loss of alertness, kidney failure, shock and rapid breathing in the later
stages (7-10). The most well-known symptom of EVD, bleeding, occurs in less than
45% of patients, and this number is around 26% in the current outbreak in West Africa
(10). All outbreaks to date have been confined to Africa. However, with the increase in
the number of cases of EVD in West Africa, the possibility of importation of a case into
other countries and subsequent autochthonous transmission increased.

105
Epidemiological studies have shown that transmission of EVD occurs only by direct
contact with symptomatic patients (11-17), with infectiousness increasing over the
course of the disease (13, 18), suggesting that early intervention (via monitoring of
contacts and rapid identification and isolation of cases) can prevent ongoing
transmission.
By early 2015, importations and secondary transmission of EVD outside of Africa had
occurred in Spain, United Kingdom and the United States of America (USA),
highlighting the possibility of importation into any country worldwide. EVD is currently
notifiable in Australia as viral haemorrhagic fever through the National Notifiable
Diseases Surveillance System (NNDSS) under the National Health Security Act 2007.
However, a need for coordinated enhanced surveillance in Australia was identified by
the Chief Medical Officer at a Communicable Diseases Network Australia (CDNA)
meeting on 8 October 2014. Enhanced surveillance allows rapid detection, treatment
and follow up of cases, including case finding, education and monitoring of contacts,
with the aim of preventing ongoing transmission of EVD within Australia. Table 1 shows
surveillance actions relevant to enhanced EVD surveillance arising from the Australian
Government Department of Health (Department of Health) internal EVD Response
Plan (19). As of the time the need for a national surveillance system was identified, we
were in “Standby” and will move to “Response” if a case of EVD is reported in
Australia. As of 13 November 2015, we have moved down to “Preparedness” in
response to the decline in cases of EVD in West Africa.

106
Table 1: Sections from the Australian Government Department of Health internal EVD Response Plan relevant to the enhanced EVD surveillance system*
Response level Surveillance Actions
Preparedness Review existing case definition and testing protocol with CDNA
Consider activation of surveillance systems to collect enhanced case and contact data
Standby Review and refine existing case definition and testing protocol with CDNA
Implement data collection system
Adapt and implement case notification system
Assess and prepare sentinel and syndromic surveillance systems and studies
Prepare to detect cases in Australia
Consider the need for co-ordinated national collection of data on monitoring of health care workers and others returning from affected areas overseas
Response Maintain and refine enhanced data collection for cases and controls:
Adapt and implement case notification system
Enhanced data on all cases and contacts
Maintain and refine case definition and testing protocol
Analyse and report Australian data
Consider the need for co-ordinated national collection of data on monitoring of health care workers and others returning from affected areas overseas
Stand Down Assess summary data from all surveillance systems to determine when virus no longer presents a significant health risk and assess when to cease data collection
Advise final summary epidemiology, severity and virology
Review effectiveness of all systems
* EVD – Ebola virus disease; CDNA – Communicable Diseases Network Australia

107
Aim and objectives The aim of this project was to establish and evaluate an active enhanced national
surveillance system for EVD in Australia. The surveillance system was established in
order to:
Provide information to jurisdictions about incoming passengers from areas of
ongoing EVD transmission who may have been exposed to EVD. This
information was used by the jurisdictions to monitor these people for symptoms
of EVD.
Record and provide data to stakeholders about national numbers of people
screened at the border, tested for EVD and monitored for symptoms of EVD.
Provide a central database for recording cases of EVD, and for management of
contacts of cases of EVD in Australia.
Design of surveillance system
Case definition The case definitions are defined in the EVD Series of National Guidelines (SoNG), and
are under revision to respond to the evolving situation. The current version of the
SoNG, dated 26 June 2015, is available from the Department of Health website at
http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-
ebola.htm/$File/EVD-SoNG.pdf (20). Cases of EVD are classified as “suspected”,
“probable” and “confirmed” based on symptoms, epidemiology and testing as shown in
Table 2. The definitions shown in Table 2 were current as of the latest revision.
“Contacts” were people who were under temperature monitoring by jurisdictional
departments of health due to a higher or lower risk of exposure to EVD, either in
Australia or overseas. People with a risk category of casual contact were monitored in
some jurisdictions, but these people were not reported in the national temperature
monitoring report. Assessment of risk category used the guidelines included in the EVD
SoNG and are summarised in Table 3.

108
Table 2: Summary of case definitions as per the EVD SoNG*
Category
Clinical evidence:
Fever (≥38°C) or history of fever in the past 24 hours. Unexplained haemorrhage or bruising, severe headache, muscle pain, marked vomiting, marked diarrhoea or abdominal pain should also be considered
Epidemiological evidence:
Limited epidemiological evidence requires travel to an EVD affected area (country/region) in the 21 days prior to onset. A full list of the lower risk and higher risk exposures are defined in table 3
Laboratory evidence:
Isolation of virus, detection of virus (by nucleic acid testing, antigen detection or electron microscopy), IgG seroconversion or detection of EVD IgM. Suggestive evidence refers to testing in jurisdiction-based labs. Confirmation requires testing at Victorian Infectious Diseases Reference Laboratory
Contact No Limited epidemiological evidence or lower or higher risk exposure
No
Suspected case Yes Lower or higher risk
exposure No
Probable case Yes Lower or higher risk
exposure Suggestive
Confirmed case Not required Not required Yes
* EVD – Ebola virus disease; SoNG – Series of National Guidelines

109
Table 3: Guidelines for assessment of risk category for cases and contacts of EVD*
Risk category
Criteria
Casual contact
No direct contact with an EVD case or body fluids of an EVD case, but who may have been in the vicinity of an EVD case or fluids
Lower risk Household contact with a confirmed EVD case
Worked in a medical or nursing capacity caring directly for confirmed EVD cases in an EVD affected area
Inadequate PPE or touched skin or body with no visible body fluid of a confirmed EVD case (alive)
No PPE and potential droplet exposure to a confirmed EVD case (case actively vomiting/diarrhoea/cough/aerosol generating procedure – downgrade to casual if in a large room and very distant)
Direct contact with an ill person or body fluids of a person of unknown health status in an EVD affected area
Worked in a mine or cave inhabited by bat colonies in an EVD endemic region
Higher risk Received a needle stick injury from a confirmed case
Had inadequate PPE and blood or fluid splash to mucous membrane from a confirmed case
Had inadequate PPE and skin touched blood, vomit, diarrhoea, urine, saliva or semen from a confirmed case
Had inadequate PPE and processed blood or body fluids from a confirmed case in a laboratory
Had inadequate PPE and direct contact with a dead body or fluid from a dead body with confirmed EVD, or suspected EVD and unknown cause of death in an EVD affected area
Had direct contact with sick or dead wild animals in an EVD endemic region
* EVD – Ebola virus disease; PPE – personal protective equipment

110
Stakeholders The stakeholders involved in national EVD surveillance are shown in Table 4. The
relevant stakeholders were consulted throughout establishment and use of the system,
and during the evaluation. For example, CDNA and jurisdictional departments of health
were asked for feedback about the case and contact report forms in the establishment
phase. All feedback was assessed and forms were adjusted as required.
Table 4: Stakeholders of EVD enhanced surveillance*
Stakeholder Stake held
Department of Health (Ebola Response Task Force)
Coordination
Administration
Dissemination
Communicable Diseases Network Australia (CDNA)
Coordination between Commonwealth and jurisdictional health departments
Planning
Australian Health Protection Principal Committee (AHPPC)
Oversight of response to EVD
State and territory departments of health
Coordination of state-based response to cases (including contact tracing and monitoring)
Reporting to NNDSS and NetEpi
Public Health Laboratory Network (PHLN)
Coordination of laboratory testing
Victorian Infectious Diseases Reference Laboratory (VIDRL)
Testing of patient samples
Department of Agriculture Coordination of border surveillance
Aid organisations† Reporting of returning aid workers to the Department of Health
* EVD – Ebola virus disease; NNDSS – National Notifiable Diseases Surveillance System † Médecins Sans Frontières, the Red Cross, the World Health Organization, the Global Outbreak Alert and Response Network and Aspen

111
System design Surveillance of people deemed to be at risk of developing EVD in Australia occurred
through a multi-pronged approach at various points after entry into Australia following
travel to countries with EVD transmission. This approach was used to detect cases of
EVD sufficiently early to provide treatment and prevent further transmission within
Australia through public health action. The decisions and processes involved in
development of the national EVD surveillance system are shown in Figure 1. The three
components were:
1. Border surveillance – enhanced screening of travellers returned from countries
identified as having ongoing and intense transmission of EVD as they pass
through international airports or seaports. This component was designed and
managed by the Department of Agriculture, in consultation with other
stakeholders, and began on 14 November 2014.
2. Laboratory testing and temperature monitoring – jurisdictions reported the
number of people they were monitoring each week (lower and higher risk
exposures only) and the number of laboratory tests for EVD performed. This
component was designed by Katrina Knope and Tim Sloan-Gardner in the
Department of Health, in collaboration with CDNA, after the AHPPC decision on
10 October 2014 to begin formal collection of testing and monitoring data.
3. Case data management system – a centrally managed online database for
recording and managing data for cases of EVD and for monitoring of contacts.
This component was designed and implemented by the author, in consultation
with other stakeholders, in October and November 2014.
The border screening line list, laboratory testing data and data for temperature
monitoring of people with higher and lower risk exposures were collated using
Microsoft Excel. The case data management system utilised NetEpi, an open source
online surveillance tool and database (http://sourceforge.net/projects/netepi/)
administered by the Department of Health. The website is password protected and
access for relevant national and jurisdictional government staff can be arranged
through the administrators at the Department of Health via
http://outbreak.health.gov.au. This component was designed for recording and
monitoring of both cases and contacts by all jurisdictions. However, some jurisdictions
chose to use their own surveillance systems for monitoring of contacts. All jurisdictions
agreed to use NetEpi for case management if there had been a case reported in
Australia.

112
Figure 1: Timeline of national enhanced EVD surveillance events. Laboratory testing and
temperature monitoring events are shown in light green, case management system events are
shown in blue and border surveillance events are shown in purple. Evaluation events are shown
in red. EVD – Ebola virus disease; WHO – World Health Organization; CMO – Chief Medical
Officer; AHPPC – Australian Health Protection Principal Committee; GP – General Practitioner;
SoNG – Series of National Guidelines; CDNA – Communicable Diseases Network Australia

113
Data collection and analysis Collection and reporting of data by the Department of Health is summarised in Figure
2.
Figure 2: Data collected, collated and reported by the Department of Health as part of EVD
enhanced surveillance. Orange boxes show the progress of a returned traveller through the
system. Purple boxes show border surveillance data collection and reporting, green boxes show
laboratory testing and temperature monitoring data collection and reporting, and blue boxes
show the case data management system. Activities performed by jurisdictional departments of
health are shown in red. EVD – Ebola virus disease; HQO – Health Quarantine Officer; PHU –
Public Health Unit

114
Border surveillance All people who reported that they had been in an area of EVD transmission within the
past 21 days (Guinea and Sierra Leone as of 1 November 2015) were screened for risk
factors via a questionnaire and their temperature taken by agents from the Department
of Agriculture on arrival in Australia at both airports and seaports (screening at
seaports began on 1 December 2014). Travellers were asked three questions:
1. Have you had close contact with someone who has had Ebola or was suspected of
having the disease?
2. Have you participated in a funeral which involved direct contact with the deceased
body?
3. Have you had a fever in the last 24 hours?
A response of “yes” to any question or a temperature measured at the time of border
screening equal to or higher than 37.5°C resulted in referral to a Human Quarantine
Officer (HQO). A slightly lower temperature than that recommended in the SoNG
(38°C) was used due to potential inaccuracies in the thermometers used at the border.
Line listed data from this screening was passed daily to the Department of Health and
on to jurisdictional departments of health after cleaning. These data were collated and
reported weekly to the AHPPC and CDNA. The border screening summary was not for
further distribution.
Laboratory testing and temperature monitoring A risk assessment was performed by jurisdictional representatives, and those people
assessed as having a lower or higher risk exposure (as outlined in the EVD SoNG and
summarised in Table 3) were monitored for a temperature equal to or higher than 38°C
and other symptoms compatible with EVD. Some jurisdictions also monitored people
assessed as casual risk, but these people were not reported to the Department of
Health. Monitoring continued twice daily until 21 days after leaving the EVD affected
country, in some jurisdictions using the “contact” form in NetEpi. These data were de-
identified and sent weekly via email, along with data on laboratory specimen testing for
EVD, to the Department of Health. The format of the data collection email is shown in
Appendix 2. Data were then collated for distribution to AHPPC and CDNA members,
and made available to the media and public as needed. Additional analysis of the data
from both these sources was performed on an as needs basis.

115
Case data management system (NetEpi) In the event of a case, jurisdictions agreed that enhanced information for cases
(suspected, probable or confirmed as per the EVD SoNG, herein referred to as “cases”,
see Table 2) would be entered into NetEpi, either directly by jurisdictional staff
(nominated by jurisdictions) or via importation of data exported from jurisdiction-specific
databases. Case reporting forms (Appendix 3), containing the minimum national
dataset were available on NetEpi. For those jurisdictions with their own Ebola
surveillance database in place (as at 1 November 2015, Queensland, New South
Wales, Tasmania, Western Australia, Australian Capital Territory and Victoria), case
data would be emailed to the Department of Health “epi inbox” ([email protected]) as
required (or weekly if cases become frequently identified). “Rules” defining which field
in the jurisdiction based database corresponds to the fields in NetEpi would allow direct
upload of the data to the NetEpi database by the Department of Health EVD
surveillance team and data managers. Forms for use with contacts, including risk
assessment and temperature monitoring were also produced and were available on
NetEpi. These forms were produced for use by jurisdictions, although jurisdictions were
unable to share the data collected using these forms with the Department of Health, as
sharing of identifiable details of well people is not covered under public health
legislation. Both forms shared the same questions covering demographics, exposure
history and exposure risk assessment. Figure 3 depicts the flow of information through
the EVD surveillance system for cases. Forms were finalised and data were able to be
entered from 27 November 2014.

116
Figure 3: Chart showing the flow of case data information through the NetEpi EVD Surveillance
system
Data entered in the NetEpi database was analysed by the EVD surveillance manager
at the Department of Health on an as needs basis (regularity depended on
requirements, for example reporting of a case). Jurisdictions were able to access their
own data for analysis as desired. Data was analysed using StataSE 13.
Other issues and data sources Information from some international aid organisations was provided to jurisdictions in
advance of the aid worker’s return. The Department of Health and other jurisdictions
planned to provide assistance with contact tracing and monitoring to jurisdictions if
numbers exceed jurisdictional capacity. The requirement for assistance was monitored
and would be provided through discussions with CDNA.

117
Dissemination Summary reports were prepared for CDNA and AHPPC on a weekly basis and for
other stakeholders as required. Current reporting of border screening and EVD testing
and monitoring will continue until the end of the outbreak in West Africa, or upon advice
from AHPPC to end active surveillance for EVD.
Results of national surveillance system
Methods Descriptive analysis of data in all components of the national surveillance system was
conducted. Border surveillance data and laboratory testing and temperature monitoring
data as of 30 September 2015 were used for analysis. All data were analysed using
Excel and StataSE 13.
Border surveillance Although border screening was initiated on 9 August 2014, the current system of
enhanced screening was implemented on 14 November 2014. Therefore, only data
from 14 November 2014 was available for analysis. Screening was initially conducted
on travellers from Sierra Leone, Guinea, Liberia, the Democratic Republic of Congo
(DRC) and Nigeria. Screening of travellers from Nigeria was terminated on 15
November 2014, the DRC on 24 November 2014 and Liberia on 15 May 2015 due to
the end of intense transmission of EVD in these countries. A total of 733 people were
screened between 14 November 2014 and 30 September 2015. Figure 4 shows the
number of people screened, by week. The weeks in which screening ended for
travellers from each country are shown. Termination of screening of travellers from the
DRC dramatically reduced the number of travellers being screened. The timing of this
was fortuitous as the number of travellers returning from Liberia, Sierra Leone and
Guinea increased from the following week, although not to the same level.
Most travellers screened had returned from Sierra Leone (348 people). Only three
travellers had returned from Nigeria. However, travellers from Nigeria were only
screened on the first week of enhanced screening.

118
Figu
re 4
: Num
ber o
f peo
ple
scre
ened
per
wee
k by
cou
ntry
vis
ited.
DR
C –
Dem
ocra
tic R
epub
lic o
f Con
go

119
The responses to screening questions and the temperature recorded reflect activities
undertaken in the country the traveller is returning from, and are shown in Table 5.
Only one traveller returning from Guinea reported close contact with someone who had
EVD, and none reported attending a funeral. In contrast, 22% of travellers returning
from Sierra Leone reported close contact with an EVD patient, and 3% reported
attending a funeral. Reason for travel is not recorded in the border screening line list,
so an analysis of why more people had travelled to Sierra Leone was not possible.
Table 5: Positive traveller responses to airport health screening questions by destination
jurisdiction and country visited
Sierra Leone
(n=348) Guinea (n=207)
Liberia (n=115)
DRC† (n=64)
Nigeria (n=3)
Screening questions
Close contact (%) 75 (22) 1 (0.5) 14 (12) 0 0
Funeral (%) 9 (3) 0 0 1 (2) 0 Fever in last 24 hours (%) 0 0 0 0 -
Temperature (average) 36.5 36.4 36.5 36.3 0
* “Close contact” – Have you had close contact with someone who has had Ebola or was suspected of having the disease?; “Funeral” – Have you participated in a funeral which involved direct contact with the deceased body?; “Fever” – Have you had a fever in the last 24 hours? † DRC – Democratic Republic of Congo
Eight airports and no seaports reported screening travellers from areas of EVD
transmission (Table 6). While the information about country of origin and destination
jurisdiction is complete, 25% of records were missing information about whether an
HQO was contacted. An HQO was contacted for 118 travellers, most frequently in
Sydney (74 times, 30% of travellers). The most common reason for contacting an HQO
was due to an answer of “yes” to the question about close contact with someone who
had Ebola or was suspected of having the disease (74 referrals). The second most
common reason for an HQO referral was a high temperature (26 referrals). No-one
reported a fever within the last 24 hours, so this category was not included in the
analysis.
The final destination for most travellers was the same state where they were screened,
although both Sydney and Melbourne airports screened the highest number of
travellers who were travelling on to a second jurisdiction.

120
Tabl
e 6:
Out
com
e of
Dep
artm
ent o
f Agr
icul
ture
and
Wat
er R
esou
rces
EVD
bor
der s
cree
ning
by
airp
ort,
Aust
ralia
(14
Nov
embe
r 201
4 to
30
Sept
embe
r 201
5)
Adel
aide
B
risba
ne
Bro
ome
Dar
win
M
elbo
urne
Pe
rth
Sydn
ey
Tow
nsvi
lle
Num
ber o
f peo
ple
scre
ened
per
ai
rpor
t 9
98
1 3
153
220
248
1
Num
ber o
f tim
es H
QO
ca
lled
(%)
Unk
now
n 3
(33)
26
(27)
0
2 (6
7)
31 (2
0)
58 (2
6)
64 (2
6)
0 N
o 5
(56)
66
(67)
1
(100
) 1
(33)
92
(60)
15
5 (7
0)
110
(44)
1
(100
) Ye
s 1
(11)
6
(6)
0 0
30 (2
0)
7 (3
) 74
(30)
0
If H
QO
ca
lled,
nu
mbe
r re
spon
ding
ye
s to
eac
h qu
estio
n (%
)
Hig
h te
mpe
ratu
re
0 1
(17)
0
0 9
(30)
1
(14)
15
(20)
0
Clo
se c
onta
ct
1 (1
00)
5 (8
3)
0 0
18 (6
0)
4 (2
9)
46 (6
2)
0 Fu
nera
l 0
0 0
0 0
1 (1
4)
0 0
Hig
h te
mpe
ratu
re
and
clos
e co
ntac
t 0
0 0
0 0
0 7
(9)
0
Hig
h te
mpe
ratu
re
and
fune
ral
0 0
0 0
0 0
0 0
Clo
se c
onta
ct a
nd
fune
ral
0 0
0 0
3 (1
0)
0 6
(8)
0
All t
hree
0
0 0
0 0
0 0
0 N
umbe
r of
peop
le
repo
rting
tra
vel t
o ea
ch
coun
try*
(%)
Sier
ra L
eone
4
(44)
49
(50)
0
2 (6
7)
75 (4
9)
86 (3
9)
132
(53)
0
Libe
ria
2 (2
2)
17 (1
7)
0 0
27 (1
8)
18 (8
) 51
(21)
0
Gui
nea
3 (3
3)
30 (3
1)
1 (1
00)
0 44
(29)
84
(38)
44
(18)
1
(100
) N
iger
ia
0 0
0 0
1 (1
) 2
(1)
0 0
DR
C
2 (2
2)
2 (2
) 0
1 (3
3)
8 (5
) 29
(13)
22
(9)
0

121
* So
me
trave
llers
vis
ited
mor
e th
an o
ne c
ount
ry. D
RC
– D
emoc
ratic
Rep
ublic
of C
ongo
Adel
aide
B
risba
ne
Bro
ome
Dar
win
M
elbo
urne
Pe
rth
Sydn
ey
Tow
nsvi
lle
Num
ber o
f pe
ople
re
porti
ng
each
ju
risdi
ctio
n as
a fi
nal
dest
inat
ion
(%)
Ove
rsea
s 0
1 (1
) 0
0 1
(1)
1 (0
) 4
(2)
0 AC
T 0
1 (1
) 0
0 3
(2)
0 30
(12)
0
NSW
0
6 (6
) 0
0 6
(4)
1 (0
) 15
4 (6
2)
1 (1
00)
NT
0 0
0 3
(100
) 0
1 (0
) 6
(2)
0 Q
LD
1 (1
1)
88 (9
0)
1 (1
00)
0 6
(4)
9 (4
) 13
(5)
0 SA
8
(89)
0
0 0
13 (8
) 0
5 (2
) 0
TAS
0 0
0 0
7 (5
) 0
4 (2
) 0
VIC
0
0 0
0 11
6 (7
6)
3 (1
) 26
(10)
0
WA
0 2
(2)
0 0
1 (1
) 20
5 (9
3)
6 (2
) 0

122
Laboratory testing for EVD infection Formalised reporting of laboratory testing for EVD infection began on 10 October 2014.
Prior to this time, testing information was shared informally between the Chief Health
Officer in the jurisdiction doing the testing, and the Chief Medical Officer. Testing
performed prior to implementation of formal reporting was reported retrospectively.
Between 10 April 2014 and 30 September 2015, 25 people were tested for EVD in
Australia. Figure 5 shows the number of laboratory tests for EVD by month of testing.
Testing was sporadic, with four tests performed in some months and no tests in others.
Figure 5: Number of people tested for EVD by jurisdiction, month and year of test. ACT –
Australian Capital Territory; NSW – New South Wales; QLD – Queensland; SA – South
Australia; VIC – Victoria; WA – Western Australia
Temperature monitoring of returned travellers From the beginning of reporting on 10 October 2014 until 30 September 2015, 248
people were under monitoring for a raised temperature and symptoms compatible with
EVD. This included at least nine people who were monitored in two different
jurisdictions during a single 21-day monitoring period, making a total of 239 individual
people under temperature monitoring.
A summary of the number of people monitored in each jurisdiction and reason for travel
is shown in Table 7. Victoria monitored more people than any other jurisdiction (139
people), while NT monitored the least (five people). Most people under monitoring were
aid workers or health care workers.
0
1
2
3
4
Mar Ap
r
May Jun
July
Aug
Sep
Oct
Nov
Dec Jan
Feb
Mar Ap
r
May Jun
Jul
Aug
Sep
2014 2015
Num
ber o
f peo
ple
test
ed
Month of test
WAVICSAQLDNSWACT

123
Table 7: Category of traveller under monitoring for EVD, by jurisdiction, Australia 10 October
2014 to 30 September 2015
Jurisdiction* Aid or Health Care
Worker Work
Refugee or
migrant Visitor to Australia
Traveller or visitor Unknown Total
ACT 6 0 0 0 0 0 6 NSW 45 5 0 0 0 0 50 NT 4 0 0 0 1 0 5
QLD 9 0 0 0 0 0 9 SA 6 4 0 0 7 1 18
TAS 11 0 0 1 2 0 14 VIC 74 0 10 0 50 5 139 WA 5 1 0 0 1 0 7
Total 160 10 10 1 61 5 248
* ACT – Australian Capital Territory; NSW – New South Wales; NT – Northern Territory; QLD – Queensland; SA – South Australia; TAS – Tasmania; VIC – Victoria; WA – Western Australia
Figure 6 shows the number of people being monitored in each jurisdiction during each
reporting period (ending on Wednesday). Reporting on 7 January 2015 was for a
period of two weeks due to the Christmas break. As people were monitored for up to 21
days, each individual appears in the graph for up to four consecutive reporting weeks
depending on how many days passed between leaving a country with EVD
transmission and beginning monitoring in Australia. Victoria monitored the largest
number of people in every monitoring period since December 2014. In contrast, the
number of people being monitored in New South Wales has decreased over time.

124
Figu
re 6
: Num
ber o
f peo
ple
bein
g ac
tivel
y te
mpe
ratu
re m
onito
red
durin
g th
e w
eek
prec
edin
g ea
ch W
edne
sday
, by
Aust
ralia
n ju
risdi
ctio
n, 1
0 O
ctob
er 2
014
to 3
0
Sept
embe
r 201
5. *
Not
e th
at d
ata
colle
cted
on
7 Ja
nuar
y 20
15 w
as fo
r a tw
o-w
eek
perio
d du
e to
Chr
istm
as b
reak
. AC
T –
Aust
ralia
n C
apita
l Ter
ritor
y; N
SW –
New
Sout
h W
ales
; NT
– N
orth
ern
Terri
tory
; QLD
– Q
ueen
slan
d; S
A –
Sout
h Au
stra
lia; T
AS –
Tas
man
ia; V
IC –
Vic
toria
; WA
– W
este
rn A
ustra
lia
05101520253015 Oct22 Oct29 Oct05 Nov12 Nov19 Nov26 Nov03 Dec10 Dec17 Dec23 Dec07 Jan*14 Jan21 Jan28 Jan04 Feb11 Feb18 Feb25 Feb04 Mar11 Mar18 Mar25 Mar01 Apr08 Apr15 Apr22 Apr29 Apr
06 May13 May20 May27 May03 Jun10 Jun17 Jun24 Jun01 Jul08 Jul15 Jul22 Jul29 Jul
05 Aug12 Aug19 Aug26 Aug02 Sep09 Sep16 Sep23 Sep30 Sep
2014
2015
Number of people under temperature monitoring
Dat
e of
end
of r
epor
ting
perio
d
WA
VIC
TAS
SAQ
LDN
TN
SWAC
T

125
No specific field asks jurisdictions to specify if a person is lower or higher risk. Many,
but not all jurisdictions include this information in the comments field. Only one person
was reported to have higher risk exposures.
Case data management As no cases of EVD were reported in Australia to 1 November 2015, no data were
available for analysis. Dummy data for cases and contacts were entered between 8
July 2015 and 21 September 2015 in order to validate and improve the questionnaires
and for the evaluation of this component of the system. These data are not a true
representation of the data entered during the outbreak, and thus will not be presented
here.
Evaluating the surveillance system
Methods Public health surveillance systems should be evaluated regularly to ensure that the
aims are being achieved efficiently and effectively. The Centers for Disease Control
and Prevention (CDC) Updated Guidelines for Evaluating Public Health Surveillance
Systems (21) are a valuable source of strategies for optimising the quality of any
surveillance system being established and were used to conduct the evaluation. The
evaluation examines the characteristics and attributes of the system using both
quantitative (analysis of surveillance data) and qualitative methods (interviews with
stakeholders) as below.
Border screening data, and laboratory testing and temperature monitoring data as of 30
September 2015 was used for this evaluation. In the absence of a case of EVD in
Australia, dummy data was entered by Master of Philosophy in Applied Epidemiology
students and Department of Health staff enlisted for the purpose into a specially
designated test area of NetEpi. Attributes of the system were assessed using these
data, as outlined in Table 9. All data were analysed using Excel and StataSE 13.
Interviews with CDNA, AHPPC and Department of Agriculture representatives,
jurisdictional users, Ebola Response Taskforce members, representatives from the
laboratories and the surveillance data managers at the Department of Health were
conducted in order to assess the attributes of the three components of the surveillance
system. Table 8 lists the stakeholders and the method of consultation. Although aid
agencies were stakeholders of the national EVD surveillance system, they were not
consulted as the information provided to the Department of Health by aid agencies was
treated as separate from the national EVD surveillance system. Table 9 summarises

126
the method of evaluation and stakeholder interviewed to address each attribute. A full
list of the questions asked of stakeholders is available in Appendix 4.
Table 8: Stakeholders of EVD enhanced surveillance in Australia and method of consultation
for evaluation, 2014 and 2015*
Stakeholder Method of consultation for evaluation
Department of Health (Ebola Response Task Force and surveillance data managers)
Face to face interviews with structured and semi-structured questions
Communicable Diseases Network Australia (CDNA)
Semi-structured survey via email and online
Australian Health Protection Principal Committee (AHPPC)
Feedback provided via CDNA
State and territory departments of health Semi-structured telephone interviews with state representatives
Public Health Laboratory Network (PHLN)
Structured questionnaire via email with PHLN representative
Victorian Infectious Diseases Reference Laboratory (VIDRL)
Structured questionnaire via email with VIDRL representative
Department of Agriculture Structured questionnaire via email with Department of Agriculture representative
Aid organisations including MSF, Red Cross, WHO/GOARN, Aspen
Not consulted
* EVD – Ebola virus disease; NNDSS – National Notifiable Diseases Surveillance System; MSF – Médecins Sans Frontières; WHO – World Health Organization; GOARN – Global Outbreak Alert and Response Network

127
Tabl
e 9:
Met
hod
for a
sses
smen
t of a
ttrib
utes
of s
urve
illanc
e of
EVD
, Aus
tralia
201
5
Attr
ibut
e As
sess
men
t met
hod
Who
was
con
sulte
d or
wha
t dat
a w
as u
sed
to a
ddre
ss a
ttrib
ute
Use
fuln
ess
Qua
litat
ive
(inte
rvie
w)
Juris
dict
iona
l use
rs, C
DN
A re
pres
enta
tives
, Ebo
la R
espo
nse
Task
forc
e
Sim
plic
ity
Qua
litat
ive
Juris
dict
iona
l use
rs, D
epar
tmen
t of A
gric
ultu
re
Flex
ibili
ty
Qua
ntita
tive
(dat
a an
alys
is)
Dum
my
data
from
cas
e m
anag
emen
t sys
tem
, bor
der s
urve
illanc
e da
ta, w
eekl
y m
onito
ring
and
test
ing
data
Dat
a qu
ality
Q
uant
itativ
e D
umm
y da
ta fr
om c
ase
man
agem
ent s
yste
m, b
orde
r sur
veilla
nce
data
, wee
kly
mon
itorin
g an
d te
stin
g da
ta
Acce
ptab
ility
Q
ualit
ativ
e Ju
risdi
ctio
nal u
sers
, CD
NA
repr
esen
tativ
es
Sens
itivi
ty
Qua
ntita
tive
Dat
a fro
m c
ase
man
agem
ent s
yste
m, b
orde
r sur
veilla
nce
data
, wee
kly
mon
itorin
g an
d te
stin
g da
ta
Posi
tive
pred
ictiv
e va
lue
Qua
ntita
tive
Dat
a fro
m c
ase
man
agem
ent s
yste
m, b
orde
r sur
veilla
nce
data
, wee
kly
mon
itorin
g an
d te
stin
g da
ta
Rep
rese
ntat
iven
ess
Qua
ntita
tive
Dum
my
data
from
cas
e m
anag
emen
t sys
tem
, bor
der s
urve
illanc
e da
ta, w
eekl
y m
onito
ring
and
test
ing
data
Ti
mel
ines
s Q
uant
itativ
e an
d Q
ualit
ativ
e Ju
risdi
ctio
nal u
sers
, Ebo
la R
espo
nse
Task
forc
e, V
IDR
L, D
epar
tmen
t of A
gric
ultu
re
Dum
my
data
from
cas
e m
anag
emen
t sys
tem
, bor
der s
urve
illanc
e da
ta, w
eekl
y m
onito
ring
and
test
ing
data
St
abili
ty
Qua
litat
ive
Dep
artm
ent o
f Hea
lth s
urve
illanc
e da
ta m
anag
ers

128
Usefulness The usefulness of a surveillance system refers to the contribution of the system to the
prevention and control of the disease. EVD is a severe disease with a high mortality
rate (6), but with good management it can be easily controlled as it is only
transmissible by direct contact after onset of symptoms (11-17). Identification and
isolation of cases soon after symptom onset is essential for prevention and control of
transmission of EVD. A useful surveillance system for EVD provides efficient case data
management and contract tracing through a properly managed national surveillance
system. By monitoring people from when they entered Australia until 21 days after they
left a country with known transmission of EVD, the three components in the national
EVD surveillance system aimed to assist public health units to identify cases of EVD
early enough to prevent transmission of EVD. However, as there were no cases of
EVD reported in Australia at 1 November 2015, the system has not been truly tested.
Consultation with CDNA during the preliminary stages of this project suggested that a
nationally coordinated surveillance system for EVD was useful and desired, especially
with the escalation of the EVD outbreak in West Africa and the increasing possibility of
an imported case in Australia. Consultation with stakeholders after the system had
been in use for nearly a year showed that all three components had varying levels of
usefulness to different stakeholders.
The border screening line list was universally considered the most useful component
by jurisdictional users and CDNA representatives. The contact information provided
within the line list allowed the jurisdictional public health units to contact people and
arrange for monitoring.
“As border protection is managed by the Commonwealth, there would have
been no other way for States to know who has recently entered”
“It has been useful for us to be able to tell Emergency Departments and
ambulance services that we are aware of ‘all’ people coming from an EVD-
affected area…”
However, a frequent comment from both CDNA and jurisdictional users was that the
border screening line lists should have been separated by jurisdiction and details only
sent to the jurisdiction where the person was staying and was assessed and monitored.
Reporting of the border screening summary was not considered useful for public health
purposes by jurisdictional users or CDNA representatives beyond occasional interest
for comparison with other jurisdictions or briefings early in the outbreak response.

129
“We didn’t use this for much other than political purposes and once the
media lost interest, we really didn’t use it at all”
However, the Ebola Response Taskforce at the Department of Health used the border
screening summary for updating Question Time Briefs (QTBs) and other government
products.
“From a national perspective it is important that States have a more global
view”
Similarly, reporting of the laboratory testing and temperature monitoring summary was
not considered useful for public health purposes by jurisdictional users and CDNA
representatives beyond a comparison with other jurisdictions, but was useful to the
Ebola Response Taskforce for updating QTBs. Indeed, one jurisdiction considered that:
“(testing and monitoring reporting was) burdensome on jurisdictions.
Limited in usefulness as reports only some risk groups”
For the two jurisdictions that used the NetEpi case data management system (SA and
NT), having the online system available was useful. However, usefulness of the case
data management system would have been increased from a national perspective if all
jurisdictions had used it and the data for testing and monitoring was able to be
extracted by the Department of Health without having to request the data from
jurisdictions weekly.
System attributes Simplicity Simplicity of a surveillance system is assessed by examining the simplicity of the
structure of the surveillance system and the ease of its operation. In evaluating the
simplicity of national EVD surveillance, each component was assessed separately in
addition to the system as a whole.
Both the border surveillance and the testing and monitoring components utilised
Microsoft Excel spreadsheets containing line lists of people being reported. Considered
as standalone components, they required few fields of data and Excel was the simplest
way to collate and share these data. All jurisdictions agreed that sharing de-identified
laboratory testing and temperature monitoring data by email was the simplest way to
provide these data in the absence of a central data management system.
Simplicity of the EVD surveillance system for case data management was optimised
during implementation for both methods of entering data i.e. direct entry into NetEpi
and import of data exported from a jurisdictional system. NetEpi is a web-based system
for epidemiological records management, administered by the data management team

130
in the Department of Health. It is also used for ongoing enhanced data collection for
listeriosis, for time limited multi-jurisdictional outbreak investigations such as the 2015
hepatitis A outbreak (Chapter 6) and to record usage of post-exposure prophylaxis
(hRIg – human rabies virus immunoglobulin) for possible rabies and Australian bat
lyssavirus exposures. While not user friendly for an inexperienced user, there are many
staff members in different jurisdictional public health units around the country and in the
Department of Health with experience using NetEpi.
The case report form was optimised to keep it as simple as possible while still
collecting the minimum data required. Because the forms were designed for collecting
information for the national dataset, as well as allowing the jurisdictions to collect the
data required for public health action, the case report form was necessarily long. To
simplify use of the form, fields were marked as either required (national dataset) or not
required (public health action not required for national data analysis).
Direct entry of data into NetEpi by jurisdictions was the simplest use of the national
EVD surveillance system. As NetEpi is used routinely by staff at the Commonwealth
Department of Health, it was familiar to the staff involved in development of national
EVD surveillance and was considered the simplest format for hosting the
questionnaires. However, some jurisdictions had their own systems for recording case
data and preferred to use their established systems for their own data management.
These jurisdictions agreed to share their exported data for upload to NetEpi. This mode
of entry was unavoidably more complex than direct entry. This complexity can be
minimised by creating import rules based on the data fields of each jurisdiction in order
to simplify upload of data. However, import rules were not able to be created, as
jurisdictional case report forms were not made available. The jurisdictions that used
NetEpi for recording the details of EVD contacts described it as
“very simple to use”
“(data was) easy to enter into forms”.
The system as a whole was complicated by using different formats for the different
components (i.e. Excel for border surveillance, laboratory testing and temperature
monitoring, NetEpi for case data management). This was a result of the ad hoc way in
which the system was assembled in response to the changing priorities during the
outbreak. If there had been time to plan the system, a single platform could have been
used. This would have allowed each person in the system to be given a single unique
identifier, allowing linkage throughout the system. This was also suggested as a way to
improve the system during almost all interviews with jurisdictional users, CDNA
representatives and the Ebola Response Taskforce. Optimising surveillance through

131
use of a single national system is a key priority in the National Framework for
Communicable Disease Control (22).
Flexibility Flexibility of a surveillance system refers to adaptability of the system to changing
information needs and operating conditions. Using Microsoft Excel and NetEpi as the
base for the components of the EVD surveillance system allows flexibility. NetEpi was
designed to accommodate different types of outbreaks and case reporting, and forms
can be easily changed as required. Adding the enhanced reporting forms for the
current EVD outbreak to NetEpi required only to make an EVD specific “instance” and
prepare the questionnaires. Changing the forms for all jurisdictional instances (if
required) was simply a matter of changing it once as the form was shared. In addition,
data were able to be imported and exported as a standard comma-separated values
(.csv) file, allowing data exported from other systems (such as jurisdictional
surveillance systems) to be imported, and data can be exported for further analysis of
the data in any program that can read a csv file, including Excel and Stata. However,
once data had been entered, forms could only be changed in minor ways or there was
a risk of losing access to data previously entered. New questions and new options
within questions could be added but more complicated changes may result in loss of
data. However, by exporting data before changes were made, the data could be re-
entered using the upload feature. Indeed, flexibility of NetEpi was shown through
changes made to the forms as a result of suggestions made by users during entry of
dummy data and use of the forms for contact monitoring by SA and NT.
Although the components themselves were flexible to change, as a national system, all
proposed changes were required to be cleared through several different bodies,
including CDNA and AHPPC, leading to reduced flexibility for making changes.
Data quality Data quality of a surveillance system is assessed by examining the completeness and
validity of the data. The Excel line lists and NetEpi case report forms were designed to
maximise completeness. Some strategies that were used included keeping the
required fields to a minimum, and making it obvious these fields were required by using
the “required fields” option in NetEpi to force a response, and by marking the required
fields clearly in the data dictionary. In addition, responses to questions were formatted,
where possible, as check box inputs requiring a single response in order to improve
validity.
A snapshot of the data in both the border screening line list and the testing and
monitoring spreadsheet was made on 30 September 2015. The border screening line

132
list was extracted from an internal database maintained by the Department of
Agriculture. Jurisdictional representatives reported that contact information for the
travellers was often wrong or incomplete. In addition, seven fields were empty or poorly
completed and were excluded from the analysis. Of these fields, most recorded data
specifically for use by Agriculture (such as number of people travelling together and
additional comments) and were not required for analysis of data related to public
health.
The field recording the action taken was poorly completed; 27% of responses were
missing. Of those with a response, there was no standard response, and as a result
responses had different phrasing. However, even after cleaning, the responses implied
that 70% of people received a leaflet and only 2% of people received a health pack.
This was in contrast to the endorsed protocol that all travellers were given a pack
containing information about EVD symptoms and a thermometer, suggesting this field
was not accurately completed by border officers.
The triggers for calling an HQO were considered appropriate, although one
jurisdictional representative described the thermometers used as “random number
generators” and that nurses called to the airport would ask the traveller to check their
temperature using the thermometer provided in the pack. Another jurisdictional
representative suggested that a time frame should be included in the close contact and
funeral questions, as some travellers had not been near an EVD case in the previous
21 days.
All fields in the testing data were 100% complete, with the exception of the “category of
traveller” field and information about subsequent tests. As most people were tested
only once or twice, it was not unexpected that information about the second and third
tests was incomplete. However, the “category of traveller” (e.g. health care worker,
refugee) field was not well defined and as a result responses required cleaning to
categorise the responses before analysis. Similarly, all fields in the monitoring data
were 100% complete with the exception of “country of travel” and “category of traveller”
as with the testing data. As the data for these Excel spreadsheets were obtained from
the text of an email and copied into the large spreadsheet maintained at the
Department of Health, it was difficult to restrict responses to defined categories.
Suggestions for categories were included in the heading of the table in the email (See
Appendix 2). Assessed risk category (i.e. lower or higher risk) was often entered into
either the “category of traveller” field or the “comments” field. However, the risk
assessment was not always included. A separate field for reporting risk category would
ensure that this information would be available. The field for “country of travel” was not
included in the suggested table format in the email. As a result, this field was very

133
poorly completed and with no consistent identifying information, a comparison between
border screening and monitoring could not be conducted.
While there were no cases of EVD in Australia during the evaluation period to 1
November 2015, and as a consequence no real cases were entered into NetEpi,
dummy data were entered for both cases and contacts. These data were entered by
several different volunteers, testing the interpretation of the questions by different
people. Some data for questions that were not marked as required were missing.
However, this is acceptable as completing these fields was optional.
The design of the case data management form required calculations of 21 days from a
given date (the incubation period of EVD) in order to know what period to ask people
about their exposures. Some users did not calculate this correctly, resulting in
inaccurate estimates of exposure or infectious periods. Although it was not available in
NetEpi, an automatically performed calculation would prevent this. In addition, users
were asked to select the appropriate risk category based on answers to some previous
questions. Despite clear instructions on how to select the risk category, some users
selected the wrong category. Again, an automatic assessment of risk category based
on responses to risk questions would have prevented misallocation.
Acceptability The acceptability of a surveillance system refers to the willingness of people to be
involved and use the surveillance system. The national EVD surveillance systems and
forms were designed in consultation with jurisdictions through CDNA and Chief Health
Officers through AHPPC. Enhanced border surveillance began on 14 November 2014
and was coordinated by the Department of Agriculture in collaboration with CDNA.
Reporting of testing and monitoring data was agreed by AHPPC and CDNA on 10
October 2014. Verbal agreement was obtained on 22 October 2014 from all
jurisdictions via CDNA to either use NetEpi for EVD case data management directly or
via importing data from their own surveillance databases. A summary of the case data
management system was sent to members of CDNA on 12 November 2014 along with
the forms and data dictionary for feedback, and feedback was received from four
jurisdictions.
EVD is a rare, but important disease with a high level of public awareness and a high
case fatality rate. As a consequence, acceptability for a nationally coordinated EVD
surveillance system was high. There has been some suggestion that increasing human
encroachment into formerly forested areas has resulted in an increase in the number of
EVD outbreaks reported (23). This suggests that the possibility of importation of EVD
into Australia will not end when this outbreak ends. In the event of another outbreak of
EVD or a disease with similar epidemiology, the lessons learned through developing

134
and testing the current enhanced surveillance system for EVD will allow surveillance to
be rapidly implemented.
Acceptability of the system was high among jurisdictional users and CDNA
representatives as discussed during interviews.
“It did the communication job it needed to do in a really timely manner”
“Probably the best way we’ve got at the moment”
This reflects the high level of public and political interest in this outbreak. As the
outbreak has diminished and fallen from the public consciousness, acceptability has
decreased, especially for the weekly email of people tested and monitored. Some
jurisdictional users expressed interest in decreasing reporting to fortnightly or monthly.
Use of a national centralised online database that allows automated reporting of
numbers tested and monitored would increase acceptability. The most commonly
reported reason for jurisdictions not using the NetEpi case management system for
contact management was that they were already using their own surveillance system
and did not want to enter data twice.
Sensitivity Sensitivity refers to the proportion of true cases that were correctly identified as cases.
Sensitivity also refers to the ability of the system to detect an outbreak and monitor
changes in the number of cases. A surveillance system with high sensitivity means that
most true cases are detected, although it gives no information about how many non-
cases were falsely detected as cases (false positives). As EVD is not endemic in
Australia, active monitoring at the airports and seaports, and surveillance at the border
(via border surveillance) and within jurisdictions (via laboratory testing and temperature
monitoring) enables early identification and monitoring of possible imported cases. The
case definition for EVD, as defined in the EVD SoNG (20), is comprehensive and has a
high level of sensitivity. It has three different levels of suspicion, “suspected”,
“probable” and “confirmed”, allowing the capture of all cases of EVD. Although the
initial stages of EVD are non-specific and similar to many other diseases, the inclusion
of epidemiological evidence increases the specificity without affecting the sensitivity of
the case definition. Specificity refers to the proportion of true non-cases that are
correctly identified as non-cases. An outbreak surveillance system should optimise
sensitivity preferentially over specificity, especially for outbreaks of diseases with a high
case fatality rate such as EVD, as detecting all cases is more important than all
identified cases being true cases. However, if specificity can be improved without
affecting sensitivity, the burden on public health can be reduced. Monitoring for clinical
signs of EVD in all people with an epidemiological link to a case (people with a lower or

135
higher risk of EVD) increases the sensitivity of the system to detect a case of EVD
before extensive transmission occurs.
A true calculation of the sensitivity of the national EVD surveillance system was not
able to be done as there have been no cases of EVD in Australia as of 1 November
2015.
Positive predictive value Positive predictive value (PPV) refers to the proportion of detected positive cases that
are truly positive. Unlike sensitivity, PPV does tell us the proportion of non-cases that
are detected as cases. Due to the severe nature of EVD and the high potential of
transmission of EVD if undetected, high sensitivity is more important than high PPV.
The surveillance case definition is designed to minimise the probability of missing any
cases, and as a result can be expected to have a low PPV. However, given the small
numbers of people who met the case definition, the extra burden on the public health
system due to a low PPV is acceptable. As of 30 September 2015, no cases have been
reported, but 25 people have been tested for EVD (all negative) and 248 people have
been monitored. If we consider the 25 tested people as false positives based on
symptoms and epidemiology (i.e. before the test result was obtained), the PPV was
0%.
Representativeness Representativeness of a surveillance system refers to the ability of the system to
accurately characterise the epidemiology of the disease. The national EVD surveillance
system was designed for maximum representativeness as it was designed to capture
all people at risk of developing EVD in Australia through recording and following up all
passengers returning from EVD affected areas. However, this method relies on self-
reporting of travel history by returning travellers, potentially missing travellers who are
unwilling to mention travel to these countries.
An additional comment on representativeness was mentioned during jurisdictional
interviews. The risk assessment questions (which are based on the risk assessment in
the EVD SoNG and are shown in Table 3) were skewed towards health care workers,
and as a result may miss community based exposures, where people were less likely
to wear personal protective equipment. This may result in non-health care workers
being categorised as low or casual risk and not being recorded in the national
surveillance system.
Timeliness The timeliness of a surveillance system depends on the purpose the data is being
collected. In this case, it can be defined as the time taken to provide data for public

136
health action and can be measured by the time lapse between the different steps of the
system. As Australia had no cases of EVD in the evaluation period, and direct data
entry was limited, no mean time lapse can be calculated. However, general comments
can be made on the different components of the system.
The inclusion of contact monitoring as a component of this system, along with other
measures including border monitoring, was designed to capture cases of EVD before
they develop symptoms. Data collected at the border by Department of Agriculture
agents could be
“entered in real time using a tablet or by entering the data manually on a
regular PC shortly after screening the passenger”
Referral to an HQO was immediate upon a response of “yes” to any question or
measurement of temperature equal to or higher than 37.5°C. The border surveillance
data were shared with Department of Health and on to jurisdictional departments of
health daily, allowing temperature monitoring to begin immediately.
Whether jurisdictions were using NetEpi or their own databases for contact monitoring,
monitoring data (including daily temperature monitoring) were entered in real time. In
this way, jurisdictions knew immediately if a contact developed EVD or symptoms
compatible with EVD. As such, the recording of cases of EVD should be timely, and
reporting would be daily in the event of an outbreak.
As suspected EVD cases require isolation and there was a high level of public concern
around EVD, ruling out non-cases was almost as important as confirming actual cases.
A change to the SoNG on 6 November 2014 added VIDRL in Melbourne as a
confirmatory laboratory (previously only laboratories in South Africa and USA could
confirm EVD cases), significantly improving the potential timeliness of confirmation of
cases and ruling out of non-cases. Laboratory confirmation was prioritised and results
were returned rapidly. Testing at VIDRL in Victoria for EVD was made available 24
hours a day and took under three hours from sample receipt to result. Testing in other
jurisdictions was slower, but a negative result to rule out EVD was able to be obtained
within a day from sample collection. Positive tests at laboratories other than VIDRL will
require confirmation of EVD infection at VIDRL. However, as no tests were positive for
EVD during the course of this evaluation, timeliness could not be directly assessed. All
jurisdictions that performed laboratory testing for EVD in people being monitored
reported that isolation and testing of the patient occurred within hours of notification of
symptoms compatible with EVD.

137
Stability The stability of a surveillance system is assessed by determining how often the system
is unavailable for use. The border surveillance, laboratory testing and temperature
monitoring components of the surveillance system utilised regular transmission of data
via email. This system of data transmission is stable, but relies on prompt sending of
data when requested. During the period of evaluation of the system there were no
weeks in which data was not received prior to weekly reporting. However, follow up
emails and phone calls were often required before data was received.
The Microsoft Excel border surveillance and testing and monitoring data files were
accessible only from within the password protected Department of Health computer
system. However, Microsoft Excel is a stable platform and data saved on the
Department of Health computer system were constantly backed up to servers.
NetEpi is a web based system that is accessible from anywhere with an internet
connection. Each jurisdiction using NetEpi had their own section within NetEpi in which
to enter their data. Access to this section was password protected and access was
available to any number of relevant government employees required to gather and
enter these data, as long as an internet connection was available.
NetEpi has never had an outage since it has been in use by the Department of Health
(established in 2004). However, the system is not currently undergoing further
development and upgrading is not possible. The servers are physically located within
data centres in Canberra, including a backup of the system at a second location.
Discussion This newly established surveillance system was developed in response to a
surveillance gap identified during the 2014-2015 EVD outbreak in West Africa, in
particular after autochthonous transmission of EVD occurred in two non-African
countries. It was established during an outbreak situation, but if maintained, could be
used to collect enhanced data on all viral haemorrhagic fevers and other acute
diseases. The current outbreak of EVD has reminded the international community that
in the modern world of increased globalisation and air travel, introduction and potential
transmission of severe diseases such as viral haemorrhagic fevers is only a flight
away. In light of this, evaluation of the newly established national EVD surveillance
system was essential to learn from experience and be prepared for the next big
outbreak.
The national EVD surveillance system was designed over a period of months by
different people and agencies for different purposes. As a result, the three components
were not well integrated and there was no linkage between the three components.

138
People were given different identifying numbers in each component, and in different
jurisdictions. This meant it was not clear when the same person was monitored by two
different jurisdictions, and border screening data couldn’t be linked to monitoring data.
Due to privacy concerns, personal information should be restricted in a national
system, but a single unique identifier would have allowed linkage between the national
system and individual jurisdictional systems. A single centralised system, where each
person is entered into the system and given an identifying number immediately upon
screening at the airport would have allowed easier tracking of the person through to
jurisdictional screening and reporting back to the Department of Health. In addition, a
centralised system could have allowed downloading of summary reports without
sending weekly emails to jurisdictional representatives, relieving the burden of weekly
reporting from jurisdictions. Indeed, a web-based system designed for monitoring
returnees for EVD symptoms in Georgia, USA, can automatically notify epidemiologists
if someone reports a symptom, misses a scheduled monitoring time or if an error is
reported. This saved the epidemiologists time and allowed just two epidemiologists to
monitor up to 100 people at a time (24). A similar system used for monitoring of
returnees in WA, EbolaTracks, utilises automatic messages sent to mobile phones (25)
allowing WA to monitor large numbers of people with relative ease.
The most useful component of the national surveillance system were the data collected
during border screening. These data were the primary source of information used by
jurisdictions for finding and contacting people for monitoring. The information collected
by the surveillance system also formed a major component of responses to media
requests and other reporting to government and the public.
Summary of recommendations The general recommendations for improvement of the national EVD surveillance
system are as follows:
Use of a centralised, online database (such as NetEpi or a system similar to
that used in Georgia (24)) that can accommodate multiple components,
including border screening, reporting of laboratory testing and temperature
monitoring, and case data management.
Prepare a generic plan for national communicable disease outbreak
surveillance that can be adapted for any public health response as required.
This plan should include guidelines for centralised data management and
reporting, and was a key priority identified in the National Framework for
Communicable Disease Control (22).
Recommendations specific for the components as they are currently implemented are
as follows:

139
Ensure accuracy of data collected, especially contact details collected at the
border by incorporating checks on the data, such as ensuring phone numbers
have the correct number of digits and addresses exist.
Include a “risk category” field in testing and monitoring data.
Provide set definitions of reason for travel categories in testing and monitoring
data collection tool.
Redesign the reporting period field in the central Excel database for
temperature monitoring data by separating out each week the person is
monitored into separate cells.
Specify that the ‘end of monitoring date’ field in monitoring data refers to the
end of monitoring by the reporting jurisdiction. This field may need to be
updated if a person unexpectedly relocates to a different jurisdiction or country
during monitoring.
Retain a single unique ID in all systems to allow tracking when a person
relocates during monitoring.
Conclusion Although there may never be a case of EVD in Australia, there was a need for
preparedness, including establishment of a coordinated enhanced surveillance system.
While this surveillance system was useful and provided the surveillance necessary for
monitoring potentially exposed contacts, the suggested improvements would ensure
the system would be able to handle the rapid entry of large numbers of actual cases
and their contacts if required in the future. Application of the recommendations in this
evaluation to improve this surveillance system, as well as those implemented for future
outbreaks of a similar nature, will ensure Australia is ready for an infectious disease
outbreak incident caused by a similar haemorrhagic virus.
References 1. World Health Organization. Ebola virus disease in Guinea. 2014 [updated 2014; cited 21/04/15]; Available from: http://www.who.int/csr/don/2014_03_23_ebola/en/. 2. Baize S, Pannetier D, Oestereich L, Rieger T, Koivogui L, Magassouba N, et al. Emergence of Zaire Ebola virus disease in Guinea. The New England journal of medicine. 2014 Oct 9;371(15):1418-25. 3. World Health Organization. Statement on the 1st meeting of the IHR Emergency Committee on the 2014 Ebola outbreak in West Africa. 2014 [updated 2014; cited 21/04/15]; Available from: http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/. 4. World Health Organization. Ebola situation report - 4 November 2015. 2015 [updated 2015; cited 5 November 2015]; Available from: http://apps.who.int/ebola/current-situation/ebola-situation-report-4-november-2015.

140
5. Okware SI, Omaswa FG, Zaramba S, Opio A, Lutwama JJ, Kamugisha J, et al. An outbreak of Ebola in Uganda. Tropical medicine & international health: TM & IH. 2002 Dec;7(12):1068-75. 6. Chippaux JP. Outbreaks of Ebola virus disease in Africa: the beginnings of a tragic saga. The journal of venomous animals and toxins including tropical diseases. 2014;20(1):44. 7. Heymann DL. Control of Communicable Diseases Manual. 19 ed.; 2008. 8. Bah EI, Lamah MC, Fletcher T, Jacob ST, Brett-Major DM, Sall AA, et al. Clinical Presentation of Patients with Ebola Virus Disease in Conakry, Guinea. The New England Journal of Medicine. 2014 Nov 5. 9. Bwaka MA, Bonnet MJ, Calain P, Colebunders R, De Roo A, Guimard Y, et al. Ebola hemorrhagic fever in Kikwit, Democratic Republic of the Congo: clinical observations in 103 patients. The Journal of Infectious Diseases. 1999 Feb;179 Suppl 1:S1-7. 10. Barry M, Traore FA, Sako FB, Kpamy DO, Bah EI, Poncin M, et al. Ebola outbreak in Conakry, Guinea: Epidemiological, clinical, and outcome features. Medecine et Maladies Infectieuses. 2014 Dec;44(11-12):491-4. 11. Wamala JF, Lukwago L, Malimbo M, Nguku P, Yoti Z, Musenero M, et al. Ebola hemorrhagic fever associated with novel virus strain, Uganda, 2007-2008. Emerging Infectious Diseases. 2010 Jul;16(7):1087-92. 12. Francesconi P, Yoti Z, Declich S, Onek PA, Fabiani M, Olango J, et al. Ebola hemorrhagic fever transmission and risk factors of contacts, Uganda. Emerging Infectious Diseases. 2003 Nov;9(11):1430-7. 13. Dowell SF, Mukunu R, Ksiazek TG, Khan AS, Rollin PE, Peters CJ. Transmission of Ebola hemorrhagic fever: a study of risk factors in family members, Kikwit, Democratic Republic of the Congo, 1995. The Journal of Infectious Diseases. 1999 Feb;179 Suppl 1:S87-91. 14. Roels TH, Bloom AS, Buffington J, Muhungu GL, Mac Kenzie WR, Khan AS, et al. Ebola hemorrhagic fever, Kikwit, Democratic Republic of the Congo, 1995: risk factors for patients without a reported exposure. The Journal of Infectious Diseases. 1999 Feb;179 Suppl 1:S92-7. 15. Baron RC, McCormick JB, Zubeir OA. Ebola virus disease in southern Sudan: hospital dissemination and intrafamilial spread. Bulletin of the World Health Organization. 1983;61(6):997-1003. 16. Ebola haemorrhagic fever in Sudan, 1976. Report of a WHO/International Study Team. Bulletin of the World Health Organization. 1978;56(2):247-70. 17. Ebola haemorrhagic fever in Zaire, 1976. Bulletin of the World Health Organization. 1978;56(2):271-93. 18. Yamin D, Gertler S, Ndeffo-Mbah ML, Skrip LA, Fallah M, Nyenswah TG, et al. Effect of Ebola Progression on Transmission and Control in Liberia. Annals of Internal Medicine. 2014 Oct 28. 19. Department of Health. Ebola virus disease response plan. 2014. 20. Department of Health. Ebola Virus Disease (EVD) CDNA National Guidelines for Public Health Units. 2015 [updated 2015; cited 15 November 2015]; Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-ebola.htm/$File/EVD-SoNG.pdf. 21. German RR, Lee LM, Horan JM, Milstein RL, Pertowski CA, Waller MN, et al. Updated guidelines for evaluating public health surveillance systems:

141
recommendations from the Guidelines Working Group. MMWR Recomm Rep. 2001 Jul 27;50(RR-13):1-35; quiz CE1-7. 22. Williams S, Armstrong P, Cheng A, Firman J, Kaldor J, Kirk M, et al. National Framework for Communicable Disease Control. 2014 [updated 2014; cited 15 October 2015]; Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-nat-frame-communic-disease-control.htm. 23. Muyembe-Tamfum JJ, Mulangu S, Masumu J, Kayembe JM, Kemp A, Paweska JT. Ebola virus outbreaks in Africa: past and present. The Onderstepoort Journal of Veterinary Research. 2012;79(2):451. 24. Parham M, Edison L, Soetebier K, Feldpausch A, Kunkes A, Smith W, et al. Ebola active monitoring system for travelers returning from West Africa-Georgia, 2014-2015. MMWR Morbidity and Mortality Weekly Report. 2015 Apr 10;64(13):347-50. 25. Tracey LE, Regan AK, Armstrong PK, Dowse GK, Effler PV. EbolaTracks: an automated SMS system for monitoring persons potentially exposed to Ebola virus disease. Euro surveillance: European communicable disease bulletin. 2015;20(1).

142
Appendix 1: Targeted literature review Introduction
With the rapidly increasing number of cases of Ebola virus disease (EVD) in West
Africa, and the possibility of importation of a case into western countries, the
Commonwealth Department of Health is currently implementing an enhanced
surveillance system to monitor contacts and returned health care workers, and to
collect information about cases of EVD. Currently all messages (media and
government) state that transmission of Ebola virus (EBOV) only occurs through close
physical contact with a symptomatic case of EVD. None of these statements reference
primary articles validating this statement.
Focused research question
Are the current Australian guidelines for prevention of transmission of Ebola virus
disease based on epidemiological evidence of risk of infection and modes of
transmission?
Methods for conducting literature search
PubMed was searched using the search terms shown in Figure 1. The term “ebola*”
was included in order to find papers that referred to both “ebola” and “ebolavirus”, as
the terms are interchangeable and vary over time. Only the epidemiology of EBOV in
humans (not animals) was relevant to the research question. The term “outbreak” was
chosen over “human” in order to remove experimental studies on animals from the
search without losing papers that don’t specify “human” as the source of the outbreak.
“Transmission” and “risk” were both included to restrict the articles to only those that
examined transmission of EBOV in terms of the risk to contacts.
Figure 1. Flowchart of search terms showing number of hits for each search term
No restriction was placed on time, as EBOV has only been known since 1976, and
there have been few large outbreaks allowing epidemiological study since that time.
Reviews were excluded (although recent comprehensive reviews were checked to

143
ensure no important papers had been missed with the chosen search terms) and only
articles that specifically examined different risk factors were included. Articles on
transmission in animals and primary transmission from the zoonotic source to the initial
case were excluded since the research question focuses on transmission between
human cases in an outbreak setting.
From the final search of “ebola* AND outbreak AND transmission AND risk”, five
papers remained relevant to the research question after reading the abstract, and two
additional papers were found by “snowballing” from these papers. These two
snowballed papers were referenced in almost all of the papers found through the
primary search as they are the definitive epidemiological studies of the original two
outbreaks of EBOV in 1976. See Table 1 for details of papers.
Synthesis
Some of the articles are comprehensive discussions of all aspects of the outbreak in
question. Only results relevant to the research question are discussed.
The two studies published in 1978 (1, 2) were done when EBOV was a newly
discovered virus and EVD a newly discovered disease. Although the outbreaks
occurred concurrently, they were later found to be caused by different strains of EBOV
(Zaire strain and Sudan strain), and each had slightly differing epidemiology. Both
studies used a case control design to examine risk factors for transmission. Neither
study calculated odds ratios (OR), instead basing their conclusions on attack rates
(AR) alone.
The outbreak in Zaire (now Democratic Republic of the Congo) was unique of all the
outbreaks reported in that the primary mode of transmission, particularly during the
early part of the outbreak, was due to reuse of needles within the hospital. No specific
calculations of risk due to injection are presented in the article, although they state that
85 of the 288 cases had received at least one injection at the hospital. Following
closure of the hospital, transmission was associated primarily with contact with EVD
patients. When comparing those cases with no hospital-associated needle
transmission with controls (age and sex matched, selected from the same village), only
aiding delivery of a child born to an EVD patient showed a higher attack rate in cases
compared to controls (case AR = 18.3%, family control AR = 9.5%, village control AR =
4.5%) (2). During the concurrent outbreak in Sudan, the authors concluded that close
and prolonged contact, especially nursing a case (AR = 81%), was required for
transmission, whereas merely being in the same room had a lower risk (AR = 23%)
and noted that no cases were reported in people with only casual contact (1).

144
The article by Baron et al. (3) utilised a case control study to examine risk factors
during the 1979 EVD outbreak in Sudan (Sudan strain). Controls in this study were
asymptomatic family members. However, they state that 21 of the 103 controls had
antibody to EBOV. Whether these antibodies were due to infection during this outbreak
or due to previous exposure to EBOV is unknown. Despite these limitations, they found
that providing nursing care to an EVD case had the highest risk of transmission (OR =
5.1, 95% Confidence Interval (CI) = 1.31-15.48), followed by physical contact with no
nursing care (OR not reported) (3).
Two papers examined transmission during the large 1995 outbreak in Kikwit,
Democratic Republic of the Congo (Zaire strain). The first, by Dowell et al (4) is a
comprehensive cross sectional study of 27 households with at least one primary case
of EVD. All surviving members of the household were interviewed about their own risk
factors, and were also asked about the risk factors of deceased family members. The
questionnaire used was standardised and delivered, via a translator, in Kikongo, the
local language. Risk factors for each secondary were examined for four different
periods of possible exposure to a primary case, including the incubation period (when
cases are not thought to be infectious), home care, hospital care (considered late
infection) and after death. Crude prevalence rate ratios (PRR) were calculated,
analogous to relative risk, and adjusted PRR were calculated after stratification and
logistic regression. Direct physical contact with an EVD case (all cases reported direct
physical contact with cases so the PRR is undefined) or their body fluids (PRR = 3.6,
95% CI = 1.9-6.8) remained significant after adjusting for other exposures, and the
PRR became higher as the disease progressed, whereas there was no exposure
during the incubation period that was associated with an increased risk of illness. In
addition, none of the non-cases reported physical contact with symptomatic cases (4).
The second study of transmission risk factors using data collected during the 1995
Kikwit outbreak aimed to delve deeper to find a source of infection for 55 patients (5). A
previous study had traced the outbreak using an assumption of direct person to person
contact, but had been unable to find the link for these 55 cases (6). This article is not
included in this review due to this assumption of a risk factor. Roels et al (5) used a
matched case control study design to elucidate risk factors for 44 of these cases (the
remaining 11 patients either refused to participate or could not be located). The
questionnaire was identical for cases (or their proxies) and controls, and made no
assumptions about risk factors, including factors such as dietary habits and social
customs. Analysis of the data included exact conditional logistic regression for
multivariate analysis. In their final model, admission to hospital for an unrelated illness
(OR = 12, 95% CI = 2.7-76.8) and visiting a person with fever and bleeding (OR = 10,

145
95% CI = 3.2-38.9) remained significant (5). After taking into consideration these two
risk factors, only 12 cases with an unknown transmission remained from this outbreak
(out of 316 cases in total). The authors suggest that these cases may have been due to
transmission via droplets or fomites (5). However, these cases were not confirmed by
serologic testing, so may not be true cases of EVD, and limitations of the study
including use of proxies may have missed unrecorded contact with other cases of EVD.
The largest outbreak of EVD prior to the current outbreak in West Africa occurred in
Uganda, in 2000-2001 (Sudan strain). A comprehensive study of the risk factors of this
outbreak was conducted by Francesconi et al (7). The authors traced the outbreak
back to the primary cases, and then used this information on cases and contacts to
conduct a case control study, using healthy contacts of cases as controls. All but one
case reported direct contact with an EVD patient’s body fluids (prevalence proportion
ratio (PPR) = 4.61%, 95% CI = 1.73-12.29). The remaining case reported only sleeping
in a blanket belonging to an EVD case. Unique to this study, risk of transmission after
sharing meals or sleeping on the same mat as a case (commonly considered “casual
contact”) remained significant after controlling for direct contact. The risk through
different stages of the course of illness showed that risk of transmission through
contact with body fluids increased during the later stages of illness and risk increased
with each additional type of direct contact, i.e. two different types of direct contact was
associated with a higher risk than only having one type of direct contact (7).
Wamala et al (8) reported on a case control study conducted during an outbreak in
Uganda during 2007-2008. This outbreak was the only outbreak of a novel strain of
EBOV, Bundibugyo. Controls were patients in hospital with negative EVD test results.
Similarly to the previous studies, contact with cases of EVD was the primary risk factor
(OR = 2.66, 95% CI = 1.35-5.24), specifically visiting sick people, visiting the hospital or
participating in funeral rituals (8).
All studies were conducted under the extreme conditions of an active outbreak of EVD,
and as a result, all have limitations on the data collected. Most notably, the high case
fatality rate of EVD and rapid onset of illness required extensive use of proxies in order
to obtain information about potential exposures, and selection of appropriate controls
relied more on availability and ease than the robust control selection techniques
available in other case control studies. Quality of the articles chosen improved over
time, with the addition of measures of association (the different types of odds ratios)
instead of attack rates only, but all were applicable to the research question. Despite
the varying quality of the studies involved, all seven came to the same basic
conclusion: transmission of EBOV requires contact with a case of EVD. No study found
evidence of airborne transmission.

146
Conclusion
The articles reviewed here support the commonly held belief that EVD is transmitted
via direct contact with actively symptomatic patients. Thus, the current Australian
guidelines are consistent with the evidence from previous outbreaks. However, there
has recently been some suggestion of other modes of transmission in the grey
literature (news articles and blog posts), specifically around infection of nurses in the
US and Spain while wearing PPE. These suggestions are based on few cases, recall
bias and are not supported by solid investigations, but if new evidence for alternative
modes of transmission of EVD becomes proven, the guidelines should be adapted to
reflect these changes. The epidemiology of EVD if introduced into western countries is
unknown, but if cases do occur good surveillance systems are required to track and
manage cases and to understand the differences compared with what is known about
EVD epidemiology in Africa.
References
1. Ebola haemorrhagic fever in Sudan, 1976. Report of a WHO/International Study Team. Bulletin of the World Health Organization. 1978;56(2):247-270. Epub 1978/01/01.
2. Ebola haemorrhagic fever in Zaire, 1976. Bulletin of the World Health Organization. 1978;56(2):271-293. Epub 1978/01/01.
3. Baron RC, McCormick JB, Zubeir OA. Ebola virus disease in southern Sudan: hospital dissemination and intrafamilial spread. Bulletin of the World Health Organization. 1983;61(6):997-1003. Epub 1983/01/01.
4. Dowell SF, Mukunu R, Ksiazek TG, et al. Transmission of Ebola hemorrhagic fever: a study of risk factors in family members, Kikwit, Democratic Republic of the Congo, 1995. Commission de Lutte contre les Epidemies a Kikwit. The Journal of Infectious Diseases. 1999;179 Suppl 1:S87-91. Epub 1999/02/13.
5. Roels TH, Bloom AS, Buffington J, et al. Ebola hemorrhagic fever, Kikwit, Democratic Republic of the Congo, 1995: risk factors for patients without a reported exposure. The Journal of Infectious Diseases. 1999;179 Suppl 1:S92-97. Epub 1999/02/13.
6. Khan AS, Tshioko FK, Heymann DL, et al. The reemergence of Ebola hemorrhagic fever, Democratic Republic of the Congo, 1995. Commission de Lutte contre les Epidemies a Kikwit. The Journal of Infectious Diseases. 1999;179 Suppl 1:S76-86. Epub 1999/02/13.
7. Francesconi P, Yoti Z, Declich S, et al. Ebola hemorrhagic fever transmission and risk factors of contacts, Uganda. Emerging Infectious Diseases. 2003;9(11):1430-1437. Epub 2004/01/14.
8. Wamala JF, Lukwago L, Malimbo M, et al. Ebola hemorrhagic fever associated with novel virus strain, Uganda, 2007-2008. Emerging Infectious Diseases. 2010;16(7):1087-1092. Epub 2010/07/01.

147
Table 1: Table of studies used for targeted review
Authors Year of outbreak
Country Study objectives Study type
Key risk factor
Wamala et al. 2010 (8)
2007-2008
Uganda To determine the risks for transmission
of EVD during the 2007-2008 outbreak
in Uganda
Case control
Handling dead bodies without
PPE
Francesconi et al. 2003
(7)
2000-2001
Uganda To determine the risks for transmission
of EVD during the 2000-2001 outbreak
in Uganda
Case control
Contact with an EVD patient's
body fluids
Dowell et al. 1999 (4)
1995 Democratic Republic of
Congo
To determine the risks for transmission
of EVD during the 1995 outbreak in
Congo
Cross sectional
All secondary cases had
direct physical contact with a case of EVD
Roels et al. 1999 (5)
1995 Democratic Republic of
Congo
To determine the source of exposure for 55 patients with
unknown transmission in
Dowell et al.
Matched case
control
Admission to hospital and
vising a person with fever and
bleeding
Baron et al. 1983 (3)
1979 Sudan To determine the risks for transmission
of EVD during the 1979 outbreak in
Sudan
Case control
Providing nursing care
WHO/ International study team,
1978 (1)
1976 Sudan To establish the epidemiology of the
newly identified disease, EVD, during the 1976 outbreak in
Sudan
Case control
Close and prolonged
contact
International Commission,
1978 (2)
1976 Zaire (now Democratic Republic of the Congo)
To establish the epidemiology of the
newly identified disease, EVD, during the 1976 outbreak in
Zaire
Matched case
control
Injection in hospital
(needle reuse) or close
contact with another case in
community

148
Appendix 2: Data collection tool for laboratory testing and temperature monitoring As per the AHPPC decision on 10 October 2014, the Department of Health are collecting and collating weekly EVD testing and monitoring data for public dissemination. Case Definitions for weekly testing and monitoring data
•Tested suspected/probable/confirmed EVD cases: a person with clinical, epidemiological and/or laboratory evidence who has been tested in Australia for EVD during the reporting period.
•Persons being actively monitored for signs and symptoms of Ebolavirus disease (EVD), following potential exposure to the disease while overseas: a person with a higher or lower risk exposure (as define by the Ebolavirus SoNG) for which monitoring was initiated or continued by a public health unit or health department during the reporting period.
•Please use only one unique identifier per person (i.e. same identifier for monitoring and testing where applicable)
Could jurisdictions please supply linelisted data using the following templates by COB Wednesday 30 September 2015: Data collection templates for weekly testing and monitoring data Tested suspected/probable/confirmed EVD cases 24/9/15 to 30/9/15 Date notified
Unique Identifier
Jurisdiction Category - e.g. HCW, returned traveller
Test Date 1* & Result
Test Date 2* & Result
Test Date 3* & Result
Comments
*Only enter multiple test dates if applicable Persons being actively monitored for signs and symptoms of Ebolavirus disease (EVD), following potential exposure to the disease while overseas 24/9/15 to 30/9/15 Date person left ebola affected country
End of monitoring Date
Unique Identifier
Jurisdiction Category - e.g. HCW, returned traveller
Comments

149
Appendix 3: Case and contact report forms and data dictionaries Case report form
Ebola - dummy data Demographics/Identification
1 This is an environment for collection of dummy data to assist with evaluation of NetEpi EVD surveillance
2 Surname
3 Given names
4 Notifying state (Mark only one box) Unknown Australian Capital Territory New South Wales Northern Territory Queensland South Australia Tasmania Victoria Western Australia
= Ebolavirus Disease (EVD) Case Form = (Version 88)
1. == This form is for suspected, probable and confirmed cases only ==
1.1. Status of caseDefinitions from Ebolavirus SoNG Person under investigation Requires clinical evidence and limited epidemiological evidence. Note: If a risk assessment determines that a person under investigation should be tested for Ebola Virus, the person should be managed as a suspected case from that point forward regardless of clinical and epidemiological evidence. Suspected case Requires clinical evidence and epidemiological evidence. Probable case Requires clinical evidence and epidemiological evidence, AND, laboratory suggestive evidence of EVD. Confirmed case Requires laboratory definitive evidence only. For surveillance purposes, only probable and confirmed cases are submitted to NNDSS Definitions Clinical evidence requires fever of greater than 38C or history of fever in the past 24 hours. Additional symptoms such as unexplained haemorrhage or bruising, severe headache, muscle pain, marked vomiting, marked diarrhoea, abdominal pain should also be considered. Limited epidemiological evidence requires only travel to an EVD affected area (country/region) in the 21 days prior to onset.

150
Epidemiological evidence requires a lower risk exposure or higher risk exposure as defined below in the 21 days prior to onset. Lower risk exposures:
household contact with an EVD case (in some circumstances this might be classified as higher risk such where the household was in a resource poor setting),
being within approximately 1 metre of an EVD case or within the case’s room or care area for a prolonged period of time (e.g., healthcare workers, household members) while not wearing recommended personal protective equipment ,
having direct brief contact (e.g., shaking hands) with an EVD patient while not wearing recommended personal protective equipment.
Higher risk exposures: percutaneous (e.g. needle stick) or mucous membrane exposure to
blood or body fluids of an EVD patient (either suspected or confirmed) direct skin contact with blood or body fluids of an EVD case without
appropriate personal protective equipment (PPE), laboratory processing of body fluids of suspected, probable, or confirmed
EVD cases without appropriate PPE or standard biosafety precautions, direct contact with a dead body without appropriate PPE in a country
where an EVD outbreak is occurring, direct handling of sick or dead animals from disease-endemic areas,
consumption of “bushmeat” in country where EVD is known to occur. Note: The presence of higher versus lower risk exposures, and the patient’s clinical condition may influence decisions about the need to transfer the patient. Note: Exposure to an EVD case in an Australian setting would require the case is probable or confirmed EVD according to laboratory criteria.
Laboratory suggestive evidence includes: Isolation of virus pending confirmation by Victorian Infectious Diseases Reference Laboratory (VIDRL), Melbourne, or the Special Pathogens Laboratory, CDC, Atlanta or Special Pathogens Laboratory, National Institute of Virology (NIV), Johannesburg; OR
Detection of specific virus by nucleic acid testing, antigen detection assay, or electron microscopy pending confirmation by VIDRL, Melbourne, or CDC, Atlanta or NIV, Johannesburg; OR
IgG seroconversion or a significant increase in antibody level or a fourfold or greater rise in titre to specific virus pending confirmation by VIDRL, Melbourne, or CDC, Atlanta or NIV, Johannesburg; OR
Detection of IgM to a specific virus pending confirmation by VIDRL, Melbourne, or CDC, Atlanta or NIV, Johannesburg.
Laboratory definitive evidence requires confirmation of EVD infection by VIDRL, Melbourne, or CDC, Atlanta, or NIV, Johannesburg
Isolation of a specific virus; OR Detection of specific virus by nucleic acid testing or antigen detection
assay; OR IgG seroconversion or a significant increase in antibody level or a fourfold or

151
greater rise in titre to specific virus.
(Mark only one box) Suspected case - requires clinical evidence and epidemiological evidence. Probable case - requires clinical evidence and epidemiological evidence,
AND, laboratory suggestive evidence of EVD Confirmed case - requires laboratory definitive evidence only Contact - Do not use this form, please use form for contacts Confirmed negative (not a case of EVD)
For more information on definitions please click on the information button
2. == Case information ==
2.1. Date of birth
2.2. Gender (Mark only one box) Male Female
Other
Unknown
2.3. State in which case resides or is primarily staying while in Australia
(Mark only one box) Australian Capital Territory New South Wales Northern Territory Queensland South Australia Tasmania Victoria Western Australia Unknown
2.4. Residency status (Mark only one box) Australian resident Migrant Short term visitor Long term visitor Unknown
2.5. Is the case alive or dead? (Mark only one box) Alive Deceased
If you selected Alive, skip the remaining parts of this question.
2.6. Date of death
3. == Clinical Symptoms ==
3.1. Did/does the case have a fever? (Mark only one box) Yes
No Unknown

152
If Yes write the maximum recorded temperature below
3.2. Maximum temperature recorded in degrees C to one decimal place
Degrees C
3.3. Did/does the case have abdominal pain?
(Mark only one box) Yes
No Unknown
3.4. Did/does the case have diarrhoea? (Mark only one box) Yes
No Unknown
3.5. Did/does the case have fatigue? (Mark only one box) Yes
No Unknown
3.6. Did/does the case have joint and muscle pain?
(Mark only one box) Yes
No Unknown
3.7. Did/does the case have severe headache?
(Mark only one box) Yes
No Unknown
3.8. Was/is the case vomiting? (Mark only one box) Yes
No Unknown
3.9. Did/does the case have unexplained bleeding or bruising?
(Mark only one box) Yes
No Unknown
3.10. Did/does the case have other symptoms or complications?
(Mark only one box) Yes
No Unknown
If yes please specify below
3.11. Other symptoms such as neurologic, multi-organ failure, oedema, hypotension/shock (please specify)
4. == Exposure period ==
4.1. Symptom dates
4.1.1. Date of onset of symptoms
4.1.2. Start of exposure period (21 days prior to onset of symptoms)
4.2. Travel exposure

153
4.2.1. Did the case travel to an area in West Africa with active Ebola disease/outbreak during the exposure period?
(Mark only one box) Yes No Unknown If you did not select Yes, skip the remaining parts of this question. If yes, specify area/s below.
4.2.2. Name of first region visited City Country
4.2.3. Date arrived in first region
4.2.4. Date departed first region
4.2.5. Name of second region visited City Country
4.2.6. Date arrived in second region
4.2.7. Date departed second region
4.2.8. Name of third region visited City Country
4.2.9. Date arrived in third region
4.2.10 Date departed third region
4.2.11 Provide information on additional regions visited.
4.3. EVD case exposures
4.3.1. During the exposure period, did the case have contact with any known EVD case/s in Australia or overseas?
(Mark only one box) Yes - Overseas Yes - Australia No Unknown If you did not select Yes - Overseas or Yes - Australia, skip the remaining parts of this question.
4.3.2. At the time of contact, were any of the cases deceased?
(Mark only one box) Yes
No Unknown
4.3.3. In what setting/s did contact occur? Household Health care School Aeroplane Unknown

154
Burial/body disposal Other - please specify Select all that apply
4.3.4. Specify other exposure setting
4.3.5. What type of contact was it? Visit sick patient Care for sick patient - specify type of care below Bury deceased patient Exposed to blood, saliva, urine, vomit or faeces of sick patient Exposed to blood, saliva, urine, vomit or faeces of deceased patient Live with sick patient Other - please specify Unknown Select all that apply
4.3.6. Specify other information about type of contact
5. == **Exposure risk assessment** ==
5.1. HIGHER RISK A person is "higher risk" if any of the following are present:
5.1.1. Did the case receive a needle stick injury from a confirmed case?
(Mark only one box) Yes
No Unknown
5.1.2. Did the case have inadequate PPE and blood or fluid splash to mucous membrane from a confirmed case?
(Mark only one box) Yes
No Unknown
5.1.3. Did the case have inadequate PPE and their skin touched blood, vomit, diarrhoea, urine, saliva, semen from a confirmed case?
(Mark only one box) Yes
No Unknown
5.1.4. Did the case have inadequate PPE and processed blood or body fluids from a confirmed case in laboratory?
(Mark only one box) Yes
No Unknown
5.1.5. Did the case have inadequate PPE and direct contact with dead body or fluid from a dead body with confirmed EVD, or suspected to have EVD, outcome not known or cause of death unknown in an EVD affected area?
(Mark only one box) Yes
No Unknown
5.1.6. Did the case have direct contact with sick or dead wild animals in an EVD endemic region?
(Mark only one box) Yes
No Unknown

155
5.2. LOWER RISK A person is considered "lower risk" if no higher risks are present and they answer yes to any of the following:
5.2.1. Is the case a household member of a confirmed case?
(Mark only one box) Yes
No Unknown
5.2.2. Did the case work in a medical or nursing capacity caring directly for confirmed EVD cases in an EVD affected area?
(Mark only one box) Yes
No Unknown
5.2.3. Did the case have inadequate PPE and touched skin or body of alive confirmed EVD case with no visible body fluid?
(Mark only one box) Yes
No Unknown
5.2.4. Was there potential droplet exposure to a confirmed EVD case, meaning no PPE and in same room with confirmed EVD case actively vomiting / diarrhoea / cough / aerosol generating procedure (downgrade to casual if large room and very distant, such as in a hall at other end, or briefly at the other end of train carriage)?
(Mark only one box) Yes
No Unknown
5.2.5. Did the case have direct contact with an ill person or body fluids from a person of unknown health status in a EVD affected area?
(Mark only one box) Yes
No Unknown
5.2.6. Did the case work in a mine / cave inhabited by bat colonies in an EVD endemic region?
(Mark only one box) Yes
No Unknown
5.3. CASUAL CONTACT A person is considered a "casual contact" if no high or low risks are present and they have any of the following: (Note to interviewer: brief interactions such as walking by a person or moving through a hospital do not constitute close/casual contact)
5.3.1. Did the case have inadequate PPE and had been within 1 metre or within the room or care area of an EVD case for a prolonged period of time?
(Mark only one box) Yes
No Unknown
5.3.2. Did the case have inadequate PPE and had direct contact (e.g. shaking hands) with an EVD case?
(Mark only one box) Yes
No Unknown
5.3.3. Did the case have inadequate PPE and potentially touched a non-visibly stained surface in a room occupied by a confirmed case of EVD (e.g. was in waiting room with a case, was
(Mark only one box) Yes
No Unknown

156
on a ward round of a case and did not touch case)?
5.3.4. Did the case work in a medical or nursing capacity in Australia and cared directly for a confirmed EVD case using adequate PPE?
(Mark only one box) Yes
No Unknown
5.3.5. Was the case a cleaner on a ward with a confirmed case and wore adequate PPE when cleaning room?
(Mark only one box) Yes
No Unknown
5.4. NO RISK A person is considered to have no risk if there is an absence of high, low or casual risk exposures.
6. == Assessed Risk Categorisation ==
6.1. Based on the risk assessment criteria, please select the appropriate risk category
(Mark only one box) Higher Risk Lower Risk Casual Risk No Risk If there are multiple exposures in different categories, consider the higher risk exposure as the case’s risk category.
7. == Hospital presentation ==
7.1. Did the case present at a hospital? (Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
7.2. Date of hospital presentation
7.3. Name, address and phone number of hospital
7.4. Was the case admitted to hospital? (Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
7.5. Date of admission
7.6. Date of discharge or death
7.7. Name, address and phone number of hospital, if different from above
7.8. Isolated in single room (Mark only one box) Yes No Unknown

157
7.9. Admitted to ICU/HDU (Mark only one box) Yes
No Unknown
7.10. Date admitted to ICU/HDU
7.11. Date discharged from ICU/HDU
7.12. Were antivirals administered? (Mark only one box) Yes
No Unknown
7.13. If yes, specify antiviral
7.14. Date hospital information collected
7.15. Name and contact details for treating doctor or team
7.16. Was the infection thought to be hospital acquired?
(Mark only one box) Yes
No Unknown
7.17. Was an infection control consultant notified if infection thought to be hospital acquired?
(Mark only one box) Yes
No Unknown
7.18. Name and contact details of infection control consultant, if yes
8. == Laboratory evidence ==
8.1. Has a specimen been collected? (Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
8.2. Were any of the samples positive for EVD?
(Mark only one box) Yes
No Unknown Pending
8.3. Blood or serum collected (Mark only one box) Yes
No Unknown
8.4. If yes, date blood or serum collected
8.5. Result of EVD testing on blood/serum sample
(Mark only one box) Positive Negative
Pending
8.6. Throat swab collected (Mark only one box)

158
Yes
No Unknown
8.7. If yes, date throat swab collected
8.8. Result of EVD testing on throat swab (Mark only one box) Positive Negative
Pending
8.9. Urine collected (Mark only one box) Yes
No Unknown
8.10. If yes, date urine collected
8.11. Result of EVD testing on urine sample
(Mark only one box) Positive Negative
8.12. Other specimen collected (Mark only one box) Yes
No Unknown Pending
8.13. If yes, specify type of specimen collected
8.14. Date other specimen collected
8.15. Result of EVD testing on other sample
(Mark only one box) Positive Negative
Pending
8.16. Name and address of laboratory specimens sent to
8.17. Were any samples sent for confirmatory testing at VIDRL?
(Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
8.18. Were any of the samples sent to VIDRL positive for EVD?
(Mark only one box) Yes
No Unknown Pending
If you did not select Yes, skip the remaining parts of this question.
8.19. What specimens were confirmed positive for EVD at VIDRL?
Blood/serum Throat swab Urine Other specimen
8.20. Specify other tests Specify other tests
9. == Log of case movements during infectious period == Note: EVD cases

159
are deemed infectious from the day of symptoms onset for three weeks
9.1. Infectious period
9.1.1. Start of infectious period. Use the same date as recorded in "symptom onset" (question 4.1.1)
9.1.2. End of infectious period. Calculate as 21 days after symptom onset
9.2. Travel
9.2.1. Did the case travel away from home (including return from overseas) during the infectious period?
(Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
9.2.2. Where did the case travel? Within state Interstate
Overseas
9.2.3. Provide details of travel, including location, arrival and departure dates, mode of travel, flight/train/bus number and accommodation details
9.3. Occupation
9.3.1. Did the case work in any of these occupations during the infectious period?
(Mark only one box) Health care facility Residential care facility Assisted living Military base Correctional facility Educational facility Other - please specify Unknown None of the above
9.3.2. Specify other occupation
9.3.3. Details of work location, including address and phone number
9.4. Childcare
9.4.1. Did the case attend a childcare centre?
(Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.

160
9.4.2. Details of childcare centre attended, including address and phone number
9.5. Preschool/school
9.5.1. Did the case attend a Preschool or school?
(Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
9.5.2. Details of preschool or school attended, including address and phone number
9.6. Educational/residential facility
9.6.1. Did the case attend another educational or residential facility?
(Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
9.6.2. Details of other educational or residential facility attended, including address and phone number
9.7. Health service or facility
9.7.1. Did the case attend a health service or facility?
(Mark only one box) Yes
No Unknown
If you did not select Yes, skip the remaining parts of this question.
9.7.2. Details of first health facility, including name, address and contact number, date attended, time stayed and section visited/stayed.
9.7.3. Details of second health facility, including name, address and contact number, date attended, time stayed and section visited/stayed.
9.7.4. Details of third health facility, including name, address and contact number, date attended, time stayed and section visited/stayed.
9.8. Household contacts
9.8.1. What type of accommodation does the case live in?
(Mark only one box) Private residence Correctional facility

161
Hospital Hostel/boarding/hotel Aged care Psych facility Other - please specify Unknown
9.8.2. Specify other accommodation type
9.8.3. Number of household contacts
9.8.4. Contact information for the other contacts in the household
9.9. Other locations
9.9.1. Provide information on places such as cinemas, cafes, restaurants, etc not covered above. Go through each day sequentially to assist memory
List other locations, dates and contacts (if known)
9.10. Pets
9.10.1.
Has the case been in close contact with any animal, for example pets?
(Mark only one box) Yes
No Unknown
If yes, specify pet type below
9.10.2 Specify types of pets/animals
10. == Contacts identified ==
10.1. Have any contacts been identified for this case? (Mark only one box) Yes - If yes, please use Ebola Contacts form for these contacts if this person becomes a case No Unknown
11. == Data entry ==
11.1. Contact details for person who entered data
Paste in email signature block

162
CAS
E FO
RM
DAT
A D
ICTI
ON
ARY
Sect
ion
Varia
ble
nam
e Q
uest
ion
num
ber
Varia
ble
type
Po
ssib
le re
spon
ses
Des
crip
tion
Req
uire
d fie
ld
Dem
ogra
phic
s
case
_id
D1
strin
g te
xt
Uni
que
ID a
utom
atic
ally
gen
erat
ed
by N
etEp
i X
loca
l_ca
se_i
d D
2 st
ring
text
U
niqu
e ID
use
d by
repo
rting
sta
te
X
surn
ame
D3
strin
g te
xt
Surn
ame
of c
ase
X
give
n_na
mes
D
4 st
ring
text
G
iven
nam
es o
f cas
e X
stat
e D
5 st
ring
ACT
= Au
stra
lian
Cap
ital
Terri
tory
N
SW =
New
Sou
th W
ales
N
T =
Nor
ther
n Te
rrito
ry
QLD
= Q
ueen
slan
d SA
= S
outh
Aus
tralia
TA
S =
Tasm
ania
VI
C =
Vic
toria
W
A =
Wes
tern
Aus
tralia
. =
Unk
now
n
Not
ifyin
g st
ate
X

163
Asse
ssm
ent o
f sta
tus
stat
us
1.1
num
eric
1 =
Susp
ecte
d ca
se -
requ
ires
clin
ical
evi
denc
e an
d ep
idem
iolo
gica
l ev
iden
ce.
2 =
Prob
able
cas
e -
requ
ires
clin
ical
evi
denc
e an
d ep
idem
iolo
gica
l ev
iden
ce, A
ND
, lab
orat
ory
sugg
estiv
e ev
iden
ce o
f EV
D
3 =
Con
firm
ed c
ase
- re
quire
s la
bora
tory
de
finiti
ve e
vide
nce
only
0
= C
onta
ct -
Do
not u
se
this
form
, ple
ase
use
form
fo
r con
tact
s
Stat
us o
f the
cas
e as
per
EVD
So
NG
X
Cas
e In
form
atio
n
dob
2.1
num
eric
da
te (D
D/M
M/Y
YYY)
D
ate
of b
irth
of c
ase
X
gend
er
2.2
num
eric
1 =
Mal
e 2
= Fe
mal
e 3
= O
ther
9
= U
nkno
wn
Gen
der o
f cas
e X
stat
e_re
side
2.
3 nu
mer
ic
1 =
Aust
ralia
n C
apita
l Te
rrito
ry
2 =
New
Sou
th W
ales
3
= N
orth
ern
Terri
tory
4
= Q
ueen
slan
d 5
= So
uth
Aust
ralia
6
= Ta
sman
ia
7 =
Vict
oria
8
= W
este
rn A
ustra
lia
9 =
Unk
now
n
Stat
e in
whi
ch c
ase
resi
des
or is
pr
imar
ily s
tayi
ng w
hile
in A
ustra
lia
X

164
resi
denc
y 2.
4 nu
mer
ic
1 =
Aust
ralia
n re
side
nt
2 =
Mig
rant
3
= Sh
ort t
erm
vis
itor
4 =
Long
term
vis
itor
9 =
Unk
now
n
Res
iden
cy s
tatu
s X
died
2.
5 bi
nary
1
= Al
ive
0 =
Dec
ease
d Is
the
case
aliv
e or
dea
d?
X
date
_dea
th
2.6
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
of d
eath
if c
ase
is d
ecea
sed
X
Clin
ical
sym
ptom
s
feve
r 3.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n D
id/d
oes
the
case
hav
e a
feve
r?
X
feve
r_te
mp
3.2
num
eric
nu
mbe
r bet
wee
n 20
and
50
If th
e ca
se h
as/h
ad a
feve
r, w
hat
was
the
tem
pera
ture
reco
rded
, in
C
X
abdo
_pai
n 3.
3 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
/doe
s th
e ca
se h
ave
abdo
min
al
pain
X
diar
rhoe
a 3.
4 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n D
id/d
oes
the
case
hav
e di
arrh
oea
X
fatig
ue
3.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
/doe
s th
e ca
se h
ave
fatig
ue
X
join
t_m
uscl
e 3.
6 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
/doe
s th
e ca
se h
ave
join
t and
m
uscl
e pa
in?
X

165
sev_
head
ache
3.
7 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
/doe
s th
e ca
se h
ave
seve
re
head
ache
? X
vom
it 3.
8 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n W
as/is
the
case
vom
iting
? X
blee
d 3.
9 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
/doe
s th
e ca
se h
ave
unex
plai
ned
blee
ding
or b
ruis
ing?
X
othe
r_sy
mp
3.10
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
/doe
s th
e ca
se h
ave
othe
r sy
mpt
oms
or c
ompl
icat
ions
? X
othe
r_sy
mp_
det
3.11
st
ring
text
Spec
ify "o
ther
" sym
ptom
s or
co
mpl
icat
ions
, inc
ludi
ng
neur
olog
ic, m
ulti-
orga
n fa
ilure
, oe
dem
a, h
ypot
ensi
on/s
hock
Expo
sure
pe
riod
Dat
es
sym
p_on
set
4.1.
1 st
ring
date
(DD
/MM
/YYY
Y)
Dat
e of
ons
et o
f sym
ptom
s.
X
exp_
perio
d 4.
1.2
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
of s
tart
of e
xpos
ure
perio
d.
This
sho
uld
be c
alcu
late
d as
21
days
prio
r to
onse
t of s
ympt
oms
X
Trav
el e
xpos
ures
waf
r_tra
vel
4.2.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
trav
el to
an
area
in
Wes
t Afri
ca w
ith a
n ac
tive
EVD
ou
tbre
ak
X
regi
on1_
nam
e 4.
2.2
strin
g te
xt
Nam
e of
the
first
regi
on tr
avel
led
to
with
in th
e ac
tive
EVD
zon
e in
Wes
t Af
rica
regi
on1_
arriv
al
4.2.
3 st
ring
date
(DD
/MM
/YYY
Y)
Dat
e ar
rived
in th
e fir
st E
VD a
ctiv
e re
gion

166
regi
on1_
depa
rt 4.
2.4
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
depa
rted
from
the
first
EVD
ac
tive
regi
on
regi
on2_
nam
e 4.
2.5
strin
g te
xt
Nam
e of
of t
he s
econ
d re
gion
tra
velle
d to
with
in th
e ac
tive
EVD
zo
ne in
Wes
t Afri
ca
regi
on2_
arriv
al
4.2.
6 st
ring
date
(DD
/MM
/YYY
Y)
Dat
e ar
rived
in th
e se
cond
EVD
ac
tive
regi
on
regi
on2_
depa
rt 4.
2.7
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
depa
rted
from
the
seco
nd
EVD
act
ive
regi
on
regi
on3_
nam
e 4.
2.8
strin
g te
xt
Nam
e of
of t
he th
ird re
gion
tra
velle
d to
with
in th
e ac
tive
EVD
zo
ne in
Wes
t Afri
ca
regi
on3_
arriv
al
4.2.
9 st
ring
date
(DD
/MM
/YYY
Y)
Dat
e ar
rived
in th
e th
ird E
VD a
ctiv
e re
gion
regi
on3_
depa
rt 4.
2.10
st
ring
date
(DD
/MM
/YYY
Y)
Dat
e de
parte
d fro
m th
e th
ird E
VD
activ
e re
gion
extra
_reg
ions
4.
2.11
st
ring
text
Pr
ovid
e in
form
atio
n on
add
ition
al
regi
ons
visi
ted.
EVD
cas
e ex
posu
res
evd_
case
_exp
4.
3.1
num
eric
1 =
Yes
- Ove
rsea
s 2
= Ye
s - A
ustra
lia
0 =
No
9 =
Unk
now
n
Dur
ing
the
expo
sure
per
iod,
did
the
case
hav
e co
ntac
t with
any
kno
wn
EVD
cas
e/s
in A
ustra
lia o
r ov
erse
as?
X
cont
act_
outc
ome
4.3.
2 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
At th
e tim
e of
con
tact
, wer
e an
y of
th
e ca
ses
dece
ased
? X

167
exp_
setti
ng
4.3.
3 nu
mer
ic
1 =
Hou
seho
ld
2 =
Hea
lth c
are
3 =
Scho
ol
4 =
Aero
plan
e 5
= Bu
rial/b
ody
disp
osal
6
= O
ther
- pl
ease
spe
cify
9
= U
nkno
wn
In w
hat s
ettin
g/s
did
cont
act o
ccur
? Se
lect
all
that
app
ly
X
exp_
othe
r 4.
3.4
strin
g te
xt
Spec
ify "o
ther
" exp
osur
e se
tting
X
cont
act_
type
4.
3.5
num
eric
1 =
Visi
t sic
k pa
tient
2
= C
are
for s
ick
patie
nt
3 =
Bury
dec
ease
d pa
tient
4
= Ex
pose
d to
blo
od,
saliv
a, u
rine,
vom
it or
fa
eces
of s
ick
patie
nt
5 =
Expo
sed
to b
lood
, sa
liva,
urin
e, v
omit
or
faec
es o
f dec
ease
d pa
tient
6
= O
ther
- pl
ease
spe
cify
9
= U
nkno
wn
Wha
t typ
e of
con
tact
was
it?
Sele
ct
all t
hat a
pply
X
cont
act_
type
_inf
o 4.
3.6
strin
g te
xt
Spec
ify "o
ther
" con
tact
type
X
Expo
sure
ris
k as
sess
men
t H
ighe
r ris
k
high
_nee
dle
5.1.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
rece
ive
a ne
edle
stic
k in
jury
from
a c
onfir
med
cas
e X
high
_flu
id
5.1.
2 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
hav
e in
adeq
uate
PPE
an
d bl
ood
or fl
uid
spla
sh to
m
ucou
s m
embr
ane
from
a
conf
irmed
cas
e?
X
high
_ski
n 5.
1.3
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
hav
e in
adeq
uate
PPE
an
d th
eir s
kin
touc
hed
bloo
d,
vom
it, d
iarrh
oea,
urin
e, s
aliv
a,
sem
en fr
om a
con
firm
ed c
ase?
X

168
high
_pro
cess
ed
5.1.
4 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
hav
e in
adeq
uate
PPE
an
d pr
oces
sed
bloo
d or
bod
y flu
ids
from
a c
onfir
med
cas
e in
la
bora
tory
?
X
high
_dea
d 5.
1.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
hav
e in
adeq
uate
PPE
an
d di
rect
con
tact
with
dea
d bo
dy
or fl
uid
from
a d
ead
body
with
co
nfirm
ed E
VD, o
r sus
pect
ed to
ha
ve E
VD, o
utco
me
not k
now
n or
ca
use
of d
eath
unk
now
n in
an
EVD
af
fect
ed a
rea?
X
high
_ani
mal
s 5.
2.6
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
hav
e di
rect
con
tact
w
ith s
ick
or d
ead
wild
ani
mal
s in
an
EVD
end
emic
regi
on?
X
Low
er ri
sk
low
_hou
seho
ld
5.2.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Is th
e ca
se a
hou
seho
ld m
embe
r of
a co
nfirm
ed c
ase?
X
low
_hcw
5.
2.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
wor
k in
a m
edic
al o
r nu
rsin
g ca
paci
ty c
arin
g di
rect
ly fo
r co
nfirm
ed E
VD c
ases
in a
n EV
D
affe
cted
are
a?
X
low
_ski
n_flu
id
5.2.
3 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
hav
e in
adeq
uate
PPE
an
d to
uche
d sk
in o
r bod
y of
aliv
e co
nfirm
ed E
VD c
ase
with
no
visi
ble
body
flui
d?
X
low
_dro
plet
5.
2.4
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Was
ther
e po
tent
ial d
ropl
et
expo
sure
to a
con
firm
ed E
VD
case
, mea
ning
no
PPE
and
in
sam
e ro
om w
ith c
onfir
med
EVD
ca
se a
ctiv
ely
vom
iting
/ di
arrh
oea
/ co
ugh
/ AG
P (d
owng
rade
to c
asua
l if
larg
e ro
om a
nd v
ery
dist
ant,
such
as
in a
hal
l at o
ther
end
, or b
riefly
at
the
othe
r end
of t
rain
car
riage
)?
X

169
low
_illc
onta
ct
5.2.
5 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
hav
e di
rect
con
tact
w
ith a
n ill
pers
on o
r bod
y flu
ids
from
a p
erso
n of
unk
now
n he
alth
st
atus
in a
EVD
affe
cted
are
a?
X
low
_min
e 5.
2.7
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
wor
k in
a m
ine
/ cav
e in
habi
ted
by b
at c
olon
ies
in a
n EV
D e
ndem
ic re
gion
? X
Cas
ual
casu
al_3
feet
5.
3.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
hav
e in
adeq
uate
PPE
an
d ha
d be
en w
ithin
1 m
etre
or
with
in th
e ro
om o
r car
e ar
ea o
f an
EVD
cas
e fo
r a p
rolo
nged
per
iod
of
time?
X
casu
al_d
irect
cont
act
5.3.
2 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
hav
e in
adeq
uate
PPE
an
d ha
d di
rect
con
tact
(e.g
. sh
akin
g ha
nds)
with
an
EVD
cas
e?
X
casu
al_t
ouch
5.
3.3
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
hav
e in
adeq
uate
PPE
an
d po
tent
ially
touc
hed
a no
n -vi
sibl
y st
aine
d su
rface
in a
room
oc
cupi
ed b
y a
conf
irmed
cas
e of
EV
D (e
.g. w
as in
wai
ting
room
with
a
case
, was
on
a w
ard
roun
d of
a
case
and
did
not
touc
h ca
se)?
X
casu
al_h
cw
5.3.
4 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
wor
k in
a m
edic
al o
r nu
rsin
g ca
paci
ty in
Aus
tralia
and
ca
red
dire
ctly
for a
con
firm
ed E
VD
case
usi
ng a
dequ
ate
PPE?
X
casu
al_c
lean
er
5.3.
5 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
the
case
a c
lean
er o
n a
war
d w
ith a
con
firm
ed c
ase
and
wor
e ad
equa
te P
PE w
hen
clea
ning
ro
om?
X

170
No
risk
NA
5.4
NA
NA
Info
rmat
iona
l sec
tion
abou
t "N
o R
isk"
cat
egor
y
Asse
ssed
Ris
k C
ateg
oris
atio
n ris
k_ca
t 6.
1 nu
mer
ic
1 =
Hig
her r
isk
2 =
Low
er ri
sk
3 =
Cas
ual r
isk
4 =
No
risk
Base
d on
the
risk
asse
ssm
ent
crite
ria, p
leas
e se
lect
the
appr
opria
te ri
sk c
ateg
ory.
If th
ere
are
mul
tiple
exp
osur
es in
diff
eren
t ca
tego
ries,
con
side
r the
hig
her r
isk
expo
sure
as
the
case
’s ri
sk
cate
gory
.
X
Hos
pita
l pr
esen
tatio
n
Initi
al h
ospi
tal
pres
enta
tion
hosp
_pre
sent
7.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
pre
sent
with
sy
mpt
oms
to a
ny h
ospi
tal?
Thi
s in
clud
es s
ituat
ions
in w
hich
the
case
was
not
adm
itted
.
X
hosp
_pre
sent
_dat
e 7.
2 st
ring
date
(DD
/MM
/YYY
Y)
Wha
t dat
e di
d th
e ca
se fi
rst
pres
ent a
t the
hos
pita
l X
hosp
_pre
sent
_inf
o 7.
3 st
ring
text
Prov
ide
all i
nfor
mat
ion
abou
t the
ho
spita
l the
cas
e pr
esen
ted
at,
incl
udin
g na
me,
add
ress
and
ph
one
num
ber
X
Hos
pita
l ad
mis
sion
hosp
_adm
7.
4 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
the
case
adm
itted
to h
ospi
tal
for t
reat
men
t? If
no,
the
rest
of t
his
ques
tion
can
be s
kipp
ed.
X
adm
_dat
e 7.
5 st
ring
date
(DD
/MM
/YYY
Y)
Wha
t dat
e w
as th
e ca
se a
dmitt
ed
to h
ospi
tal?
disc
harg
e_da
te
7.6
strin
g da
te (D
D/M
M/Y
YYY)
W
hat d
ate
was
the
case
di
scha
rged
from
hos
pita
l (if
avai
labl
e)

171
hosp
_inf
o 7.
7 st
ring
text
Prov
ide
all i
nfor
mat
ion
abou
t the
ho
spita
l the
cas
e pr
esen
ted
at,
incl
udin
g na
me,
add
ress
and
ph
one
num
ber,
if di
ffere
nt fr
om th
at
prov
ided
in Q
uest
ion
9.1.
If s
ame,
w
rite
"as
abov
e"
sing
le_r
oom
7.
8 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
the
case
isol
ated
in a
room
by
them
selv
es?
icu
7.9
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Was
the
case
adm
itted
to IC
U o
r H
DU
?
icu_
adm
_dat
e 7.
10
strin
g da
te (D
D/M
M/Y
YYY)
If
the
case
was
adm
itted
to IC
U o
r H
DU
, wha
t dat
e w
ere
they
ad
mitt
ed?
icu_
dis_
date
7.
11
strin
g da
te (D
D/M
M/Y
YYY)
If
the
case
was
dis
char
ged
from
IC
U o
r HD
U, w
hat d
ate
wer
e th
ey
disc
harg
ed?
antiv
irals
7.
12
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Wer
e an
tivia
ls a
dmin
iste
red
to th
e ca
se?
antiv
iral_
type
7.
13
strin
g te
xt
If an
tivira
ls w
ere
adm
inis
tere
d,
wha
t is/
are
the
nam
e/s
of th
e an
tivira
l/s?
hosp
_inf
o_da
te
7.14
st
ring
date
(DD
/MM
/YYY
Y)
Wha
t dat
e w
as th
is in
form
atio
n re
gard
ing
hosp
italis
atio
n co
llect
ed?
treat
er_i
nfo
7.15
st
ring
text
Pr
ovid
e th
e na
me
and
cont
act
deta
ils fo
r the
doc
tor o
r tea
m
treat
ing
the
case

172
hosp
_acq
7.
16
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Was
the
infe
ctio
n th
ough
t to
be
hosp
ital a
cqui
red?
X
icc
7.17
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
an
infe
ctio
n co
ntro
l con
sulta
nt
notif
ied,
if th
e in
fect
ion
was
thro
ugh
to b
e ho
spita
l acq
uire
d?
icc_
cont
act
7.18
st
ring
text
C
onta
ct in
form
atio
n fo
r the
in
fect
ion
cont
rol c
onsu
ltant
Labo
rato
ry e
vide
nce
spec
imen
8.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
a s
peci
men
col
lect
ed fr
om th
e ca
se?
X
pos_
sam
ple
8.2
num
eric
1 =
Yes
0 =
No
7 =
pend
ing
9 =
Unk
now
n
Wer
e an
y of
the
sam
ples
pos
itive
fo
r EVD
? X
bloo
d 8.
3 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
a b
lood
or s
erum
sam
ple
colle
cted
?
bloo
d_da
te
8.4
strin
g da
te (D
D/M
M/Y
YYY)
W
hat d
ate
was
the
bloo
d or
ser
um
sam
ple
colle
cted
?
bloo
d_re
sult
8.5
num
eric
1
= po
sitiv
e 0
= ne
gativ
e 7
= pe
ndin
g
Was
the
bloo
d or
ser
um s
ampl
e po
sitiv
e fo
r EVD
?
thro
at_s
wab
8.
6 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n W
as a
thro
at s
wab
col
lect
ed?
thro
at_d
ate
8.7
strin
g da
te (D
D/M
M/Y
YYY)
W
hat d
ate
was
the
thro
at s
wab
co
llect
ed?

173
thro
at_r
esul
t 8.
8 nu
mer
ic
1 =
posi
tive
0 =
nega
tive
7 =
pend
ing
Was
the
thro
at s
wab
pos
itive
for
EVD
?
urin
e 8.
9 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n W
as a
urin
e sa
mpl
e co
llect
ed?
urin
e_da
te
8.10
st
ring
date
(DD
/MM
/YYY
Y)
Wha
t dat
e w
as th
e ur
ine
sam
ple
colle
cted
?
urin
e_re
sult
8.11
nu
mer
ic
1 =
posi
tive
0 =
nega
tive
7 =
pend
ing
Was
the
urin
e sa
mpl
e po
sitiv
e fo
r EV
D?
othe
r 8.
12
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Was
any
oth
er s
peci
men
col
lect
ed
for t
estin
g?
othe
r_sp
ec
8.13
st
ring
text
W
hat w
ere
the
othe
r spe
cim
ens
colle
cted
?
othe
r_da
te
8.14
st
ring
date
(DD
/MM
/YYY
Y)
Wha
t dat
e w
as th
e ot
her s
ampl
e co
llect
ed?
othe
r_re
sult
8.15
nu
mer
ic
1 =
posi
tive
0 =
nega
tive
7 =
pend
ing
Was
the
othe
r sam
ple
posi
tive
for
EVD
?
lab_
info
8.
16
strin
g te
xt
Prov
ide
the
nam
e an
d ad
dres
s of
th
e la
bora
tory
the
spec
imen
s w
ere
sent
to
vidr
l 8.
17
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Wer
e an
y sa
mpl
es s
ent f
or
conf
irmat
ory
test
ing
at V
IDR
L?
X

174
vidr
l_po
s 8.
18
num
eric
1 =
Yes
0 =
No
7 =
pend
ing
9 =
Unk
now
n
Wer
e an
y of
the
sam
ples
that
wer
e se
nt fo
r con
firm
ator
y te
stin
g at
VI
DR
L po
sitiv
e fo
r EVD
? X
vidr
l_sp
ecim
ens
8.19
nu
mer
ic
1 =
Bloo
d/se
rum
2
= Th
roat
sw
ab
3 =
Urin
e 4
= O
ther
spe
cim
en
Wha
t spe
cim
ens
wer
e co
nfirm
ed
posi
tive
for E
VD a
t VID
RL?
X
vidr
l_ot
her
8.20
st
ring
text
Sp
ecify
wha
t oth
er te
sts
wer
e do
ne
by V
IDR
L X
Infe
ctio
us
perio
d
Dat
es
date
_sta
rt 9.
1.1
strin
g da
te (D
D/M
M/Y
YYY)
St
art o
f the
infe
ctio
us p
erio
d. C
opy
this
dat
e fro
m d
ate
of s
ympt
om
onse
t
date
_end
9.
1.2
strin
g da
te (D
D/M
M/Y
YYY)
Cal
cula
te th
e en
d of
the
infe
ctio
us
perio
d. T
his
is c
urre
ntly
con
side
red
to b
e 21
day
s af
ter s
ympt
om o
nset
. H
owev
er, s
ome
stud
ies
have
sh
own
the
pres
ence
of i
nfec
tious
vi
rus
in s
ome
fluid
s (s
uch
as
sem
en) u
p to
80
days
afte
r sy
mpt
om o
nset
Trav
el
trave
l 9.
2.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
trav
el a
way
from
ho
me
durin
g th
e in
fect
ious
per
iod?
trave
l_lo
catio
n 9.
2.2
num
eric
1
= w
ithin
sta
te
2 =
inte
rsta
te
3 =
over
seas
Whe
re d
id th
e ca
se tr
avel
dur
ing
the
infe
ctio
us p
erio
d?

175
trave
l_de
tails
9.
2.3
strin
g te
xt
Prov
ide
deta
ils o
f tra
vel,
incl
udin
g lo
catio
n, a
rriva
l and
dep
artu
re
date
s, m
ode
of tr
avel
, fli
ght/t
rain
/bus
num
ber a
nd
acco
mm
odat
ion
deta
ils
Occ
upat
ion
high
_ris
k_oc
cupa
tion
9.3.
1 nu
mer
ic
1 =
Hea
lth c
are
faci
lity
2 =
Res
iden
tial c
are
faci
lity
3 =
Assi
sted
livi
ng
4 =
Milit
ary
base
5
= C
orre
ctio
nal f
acilit
y 6
= Ed
ucat
iona
l fac
ility
7 =
Oth
er -
plea
se s
peci
fy
9 =
Unk
now
n 0
= N
one
of th
e ab
ove
Did
the
case
wor
k in
any
of t
hese
hi
gh ri
sk o
ccup
atio
ns d
urin
g th
e in
fect
ious
per
iod?
occu
patio
n_de
tails
9.
3.2
strin
g te
xt
Det
ails
of w
ork
loca
tion,
incl
udin
g ad
dres
s an
d ph
one
num
ber
Chi
ldca
re
child
care
9.
4.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
atte
nd a
chi
ldca
re
cent
re d
urin
g th
e in
fect
ious
per
iod?
child
care
_det
ails
9.
4.2
strin
g te
xt
Det
ails
of c
hild
care
cen
tre
atte
nded
, inc
ludi
ng a
ddre
ss a
nd
phon
e nu
mbe
r
Scho
ol
scho
ol
9.5.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
atte
nd a
Pre
scho
ol o
r sc
hool
dur
ing
the
infe
ctio
us
perio
d?
scho
ol_d
etai
ls
9.5.
2 st
ring
text
D
etai
ls o
f pre
scho
ol o
r sch
ool
atte
nded
, inc
ludi
ng a
ddre
ss a
nd
phon
e nu
mbe
r

176
Oth
er e
duca
tiona
l in
stitu
tion
othe
r_ed
u 9.
6.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
atte
nd a
noth
er
educ
atio
nal o
r res
iden
tial f
acilit
y du
ring
the
infe
ctio
us p
erio
d?
othe
r_ed
u_de
tails
9.
6.2
strin
g te
xt
Det
ails
of o
ther
edu
catio
nal o
r re
side
ntia
l fac
ility
atte
nded
, in
clud
ing
addr
ess
and
phon
e nu
mbe
r
Hea
lth c
are
heal
th
9.7.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
case
atte
nd a
hea
lth
serv
ice
or fa
cilit
y du
ring
the
infe
ctio
us p
erio
d?
heal
th1_
deta
ils
9.7.
2 st
ring
text
Det
ails
of f
irst h
ealth
faci
lity,
in
clud
ing
nam
e, a
ddre
ss a
nd
cont
act n
umbe
r, da
te a
ttend
ed,
time
stay
ed a
nd s
ectio
n vi
site
d/st
ayed
.
heal
th2_
deta
ils
9.7.
3 st
ring
text
Det
ails
of s
econ
d he
alth
faci
lity,
in
clud
ing
nam
e, a
ddre
ss a
nd
cont
act n
umbe
r, da
te a
ttend
ed,
time
stay
ed a
nd s
ectio
n vi
site
d/st
ayed
.
heal
th3_
deta
ils
9.7.
4 st
ring
text
Det
ails
of t
hird
hea
lth fa
cilit
y,
incl
udin
g na
me,
add
ress
and
co
ntac
t num
ber,
date
atte
nded
, tim
e st
ayed
and
sec
tion
visi
ted/
stay
ed.

177
Hou
seho
ld
acco
m_t
ype
9.8.
1 nu
mer
ic
1 =
Priv
ate
resi
denc
e 2
= C
orre
ctio
nal f
acilit
y 3
= H
ospi
tal
4 =
Hos
tel/b
oard
ing/
hote
l 5
= Ag
ed c
are
6 =
Psyc
h fa
cilit
y 7
= O
ther
- pl
ease
spe
cify
9
= U
nkno
wn
Wha
t typ
e of
acc
omm
odat
ion
does
th
e ca
se li
ve in
? X
acco
m_o
ther
9.
8.2
strin
g te
xt
Spec
ify "o
ther
" typ
e of
ac
com
mod
atio
n
hous
ehol
d 9.
8.3
num
eric
W
hole
num
ber
Num
ber o
f peo
ple
livin
g in
the
sam
e ho
useh
old
hous
ehol
d_in
fo
9.8.
4 st
ring
text
C
onta
ct in
form
atio
n fo
r the
oth
er
cont
acts
in th
e ho
useh
old
Oth
er
othe
r_m
ovem
ent
9.9.
1 st
ring
text
List
oth
er lo
catio
ns, d
ates
and
co
ntac
ts w
here
tran
smis
sion
may
ha
ve o
ccur
red
durin
g th
e in
fect
ious
pe
riod
Pets
pe
t 9.
10.1
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Has
the
case
bee
n in
clo
se c
onta
ct
with
any
ani
mal
, for
exa
mpl
e pe
ts?
pet_
type
9.
10.2
st
ring
text
Sp
ecify
type
s of
pet
s/an
imal
s
Con
tact
s co
ntac
ts
10.1
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Hav
e an
y po
ssib
le c
onta
cts
been
id
entif
ied
usin
g th
is fo
rm?
If so
, the
Eb
ola
Con
tact
form
sho
uld
be u
sed
to o
btai
n th
e de
tails
of t
hese
pe
ople
, and
cas
e/co
ntac
t for
ms
shou
ld b
e lin
ked
as a
ssoc
iatio
ns in
N
etEp
i
X
Dat
a en
try
inte
rvie
wer
_det
ails
11
.1
strin
g te
xt
Past
e in
em
ail s
igna
ture
blo
ck o
f in
terv
iew
er
X

178
Contact report form
Ebola – dummy data Demographics/Identification
1 This is an environment for collection of dummy data to assist with evaluation of NetEpi EVD surveillance cases of EVD.
2 Surname
3 Given names
4 Notifying State (Mark only one box) Unknown Australian Capital Territory New South Wales Northern Territory Queensland South Australia Tasmania Victoria Western Australia
= Ebolavirus Disease (EVD) Contacts Form = (Version 44)
1. == This form is used to evaluate and monitor all people who have had contact with a case (suspected, confirmed or probable) of EVD, including returning health care workers ==
1.1. What type of contact has the person had with a case of EVD?
Health care worker in a region of current EVD activity Health care of EVD case in Australia Contact of EVD case in a region of current EVD activity Contact of EVD case in Australia Travel or lived in a region of current EVD activity Other - please specify Check all that apply
1.2. Specify type of "other" contact

179
1.3. Has the person been tested for EVD
(Mark only one box) Yes No Unknown
If yes is selected, please use EVD case form instead. As per the Ebolavirus SoNG, if a risk assessment determines that a person should be tested for Ebola virus, the person should be managed as a suspected case. If the test is negative for EVD, the person should return to monitoring as a contact for the remainder of the incubation period (21 days after last exposure to an EVD case or leaving region of current EVD activity)
2. == General information ==
2.1. Date of birth
2.2. Gender (Mark only one box) Male Female Other Unknown
2.3. State in which person resides or is primarily staying while in Australia
(Mark only one box) Australian Capital Territory New South Wales Northern Territory Queensland South Australia Tasmania Victoria Western Australia Unknown
2.4. Residency status (Mark only one box) Australian resident Migrant Short term visitor Long term visitor Unknown
3. == Exposure information ==
3.1. Date of first exposure
3.2. Date of last exposure

180
3.3. Exposure setting (Mark only one box) Travel/work in region of EVD activity Health care overseas Health care in Australia Household School Aeroplane Other - please specify Unknown
3.4. Specify "other" exposure setting
3.5. In which country did exposure occur? Use Standard Australian Classification of Countries (SACC). http://www.abs.gov.au/ausstats/[email protected]/mf/1269.0
4. == Travel exposure ==
4.1. Did the person travel to an area of West Africa with active Ebola disease/outbreak during the exposure period?
(Mark only one box) Yes No Unknown
4.2. Name of the first region visited
4.3. Date arrived in the first region
4.4. Date departed first region
4.5. Name of the second region visited
4.6. Date arrived in the second region
4.7. Date departed second region
4.8. Name of the third region visited
4.9. Date arrived in the third region
4.10. Date departed third region
5. == *Exposure risk assessment* ==
5.1. HIGHER RISK A person is "higher risk" if any of the following are present:
5.1.1. Did the person receive a needle stick injury from a confirmed case?
(Mark only one box) Yes No Unknown
5.1.2. Did the person have inadequate PPE and blood or fluid splash to mucous membrane from a confirmed case?
(Mark only one box) Yes No Unknown

181
5.1.3. Did the person have inadequate PPE and their skin touched blood, vomit, diarrhoea, urine, saliva, semen from a confirmed case?
(Mark only one box) Yes No Unknown
5.1.4. Did the person have inadequate PPE and processed blood or body fluids from a confirmed case in laboratory?
(Mark only one box) Yes No Unknown
5.1.5. Did the person have inadequate PPE and direct contact with dead body or fluid from a dead body with confirmed EVD, or suspected to have EVD, outcome not known or cause of death unknown in an EVD affected area?
(Mark only one box) Yes No Unknown
5.1.6. Did the person have direct contact with sick or dead wild animals in an EVD endemic region?
(Mark only one box) Yes No Unknown
5.2. LOWER RISK A person is considered "lower risk" if no high risks are present and they answer yes to any of the following:
5.2.1. Is the person a household member of a confirmed case?
(Mark only one box) Yes No Unknown
5.2.2. Did the person work in a medical or nursing capacity caring directly for confirmed EVD cases in an EVD affected area?
(Mark only one box) Yes No Unknown
5.2.3. Did the person have inadequate PPE and touched skin or body of alive confirmed EVD case with no visible body fluid?
(Mark only one box) Yes No Unknown
5.2.4. Was there potential droplet exposure to a confirmed EVD case, meaning no PPE and in same room with confirmed EVD case actively vomiting / diarrhoea / cough / aerosol generating procedure (downgrade to casual if large room and very distant, such as in a hall at other end, or briefly the other end of train carriage)?
(Mark only one box) Yes No Unknown
5.2.5. Did the person have direct contact with an ill person or body fluids from a person of unknown health status in a EVD affected area?
(Mark only one box) Yes No Unknown
5.2.6. Did the person work in a mine/cave inhabited by bat colonies in an EVD endemic region?
(Mark only one box) Yes No Unknown
5.3. CASUAL CONTACT A person is considered a "casual contact" if no high or low risks are present and they have any of the following: Note to interviewer: brief interactions such as walking by a person or moving through a hospital do not constitute close/casual contact

182
5.3.1. Did the person have inadequate PPE and had been within 1 metre or within the room or care area of an EVD case for a prolonged period of time?
(Mark only one box) Yes No Unknown
5.3.2. Did the person have inadequate PPE and had direct contact (e.g. shaking hands) with an EVD case?
(Mark only one box) Yes No Unknown
5.3.3. Did the person have inadequate PPE and potentially touched a non-visibly stained surface in a room occupied by a confirmed case of EVD (e.g. was in waiting room with a case, was on a ward round of a case and did not touch case)?
(Mark only one box) Yes No Unknown
5.3.4. Did the person work in a medical or nursing capacity in Australia and cared directly for a confirmed EVD case using adequate PPE?
(Mark only one box) Yes No Unknown
5.3.5. Was the person a cleaner on a ward with a confirmed case and wore adequate PPE when cleaning room?
(Mark only one box) Yes No Unknown
5.4. NO RISK A person is considered to have no risk if there is an absence of higher, lower or casual risk exposures
6. == Assessed Risk Categorisation ==
6.1. Based on the risk assessment criteria, please select the appropriate risk category
(Mark only one box) Higher Risk Lower Risk Casual Risk No Risk If there are multiple exposures in different categories, consider the higher risk exposure as the contact’s risk category.
7. == Clinical Symptoms == If the person answers yes to any of these symptoms in combination with a lower or higher risk of exposure, a case report form should be completed instead and the local Public Health Unit should be notified.
7.1. Did/does the person have a fever or history of fever in the past 24 hours, abdominal pain, diarrhoea, fatigue, joint or muscle pain, severe headache, vomiting or unexplained bleeding?
(Mark only one box) Yes No Unknown
8. == Temperature logging == If the person records a fever (>37.5C), notify the local Public Health Unit
8.1. Day 0 Record as the same date as "date last exposed"

183
8.1.1. Day 0 date and AM time
8.1.2. Day 0 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.1.3. Record temperature AM Degrees C
8.1.4. Day 0 date and PM time
8.1.5. Day 0 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.1.6. Record temperature PM Degrees C
8.2. Day 1
8.2.1. Day 1 date and AM time
8.2.2. Day 1 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.2.3. Record temperature AM Degrees C
8.2.4. Day 1 date and PM time
8.2.5. Day 1 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.2.6. Record temperature PM Degrees C
8.3. Day 2
8.3.1. Day 2 date and AM time
8.3.2. Day 2 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.3.3. Record temperature AM Degrees C
8.3.4. Day 2 date and PM time

184
8.3.5. Day 2 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.3.6. Record temperature PM Degrees C
8.4. Day 3
8.4.1. Day 3 date and AM time
8.4.2. Day 3 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.4.3. Record temperature AM Degrees C
8.4.4. Day 3 date and PM time
8.4.5. Day 3 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.4.6. Record temperature PM Degrees C
8.5. Day 4
8.5.1. Day 4 date and AM time
8.5.2. Day 4 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.5.3. Record temperature AM Degrees C
8.5.4. Day 4 date and PM time
8.5.5. Day 4 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.5.6. Record temperature PM Degrees C
8.6. Day 5
8.6.1. Day 5 date and AM time

185
8.6.2. Day 5 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.6.3. Record temperature AM Degrees C
8.6.4. Day 5 date and PM time
8.6.5. Day 5 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.6.6. Record temperature PM Degrees C
8.7. Day 6
8.7.1. Day 6 date and AM time
8.7.2. Day 6 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.7.3. Record temperature AM Degrees C
8.7.4. Day 6 date and PM time
8.7.5. Day 6 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.7.6. Record temperature PM Degrees C
8.8. Day 7
8.8.1. Day 7 date and AM time
8.8.2. Day 7 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.8.3. Record temperature AM Degrees C
8.8.4. Day 7 date and PM time

186
8.8.5. Day 7 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.8.6. Record temperature PM Degrees C
8.9. Day 8
8.9.1. Day 8 date and AM time
8.9.2. Day 8 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.9.3. Record temperature AM Degrees C
8.9.4. Day 8 date and PM time
8.9.5. Day 8 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.9.6. Record temperature PM Degrees C
8.10. Day 9
8.10.1. Day 9 date and AM time
8.10.2. Day 9 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.10.3. Record temperature AM Degrees C
8.10.4. Day 9 date and PM time
8.10.5. Day 9 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.10.6. Record temperature PM Degrees C
8.11. Day 10
8.11.1. Day 10 date and AM time

187
8.11.2. Day 10 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.11.3. Record temperature AM Degrees C
8.11.4. Day 10 date and PM time
8.11.5. Day 10 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.11.6. Record temperature PM Degrees C
8.12. Day 11
8.12.1. Day 11 date and AM time
8.12.2. Day 11 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.12.3. Record temperature AM Degrees C
8.12.4. Day 11 date and PM time
8.12.5. Day 11 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.12.6. Record temperature PM Degrees C
8.13. Day 12
8.13.1. Day 12 date and AM time
8.13.2. Day 12 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.13.3. Record temperature AM Degrees C
8.13.4. Day 12 date and PM time

188
8.13.5. Day 12 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.13.6. Record temperature PM Degrees C
8.14. Day 13
8.14.1. Day 13 date and AM time
8.14.2. Day 13 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.14.3. Record temperature AM Degrees C
8.14.4. Day 13 date and PM time
8.14.5. Day 13 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.14.6. Record temperature PM Degrees C
8.15. Day 14
8.15.1. Day 14 date and AM time
8.15.2. Day 14 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.15.3. Record temperature AM Degrees C
8.15.4. Day 14 date and PM time
8.15.5. Day 14 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.15.6. Record temperature PM Degrees C
8.16. Day 15
8.16.1. Day 15 date and AM time

189
8.16.2. Day 15 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.16.3. Record temperature AM Degrees C
8.16.4. Day 15 date and PM time
8.16.5. Day 15 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.16.6. Record temperature PM Degrees C
8.17. Day 16
8.17.1. Day 16 date and AM time
8.17.2. Day 16 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.17.3. Record temperature AM Degrees C
8.17.4. Day 16 date and PM time
8.17.5. Day 16 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.17.6. Record temperature PM Degrees C
8.18. Day 17
8.18.1. Day 17 date and AM time
8.18.2. Day 17 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.18.3. Record temperature AM Degrees C
8.18.4. Day 17 date and PM time

190
8.18.5. Day 17 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.18.6. Record temperature PM Degrees C
8.19. Day 18
8.19.1. Day 18 date and AM time
8.19.2. Day 18 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.19.3. Record temperature AM Degrees C
8.19.4. Day 18 date and PM time
8.19.5. Day 18 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.19.6. Record temperature PM Degrees C
8.20. Day 19
8.20.1. Day 19 date and AM time
8.20.2. Day 19 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.20.3. Record temperature AM Degrees C
8.20.4. Day 19 date and PM time
8.20.5. Day 19 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.20.6. Record temperature PM Degrees C
8.21. Day 20
8.21.1. Day 20 date and AM time

191
8.21.2. Day 20 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.21.3. Record temperature AM Degrees C
8.21.4. Day 20 date and PM time
8.21.5. Day 20 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.21.6. Record temperature PM Degrees C
8.22. Day 21
8.22.1. Day 21 date and AM time
8.22.2. Day 21 AM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.22.3. Record temperature AM Degrees C
8.22.4. Day 21 date and PM time
8.22.5. Day 21 PM Did the person have a fever? (Mark only one box) Yes No Unknown
Record temperature below
8.22.6. Record temperature PM Degrees C
9. == **Data Entry** ==
9.1. Contact details for person who entered data
Paste in email signature block

192
CO
NTA
CT
FOR
M D
ATA
DIC
TIO
NAR
Y
Sect
ion
Varia
ble
nam
e Q
uest
ion
num
ber
Varia
ble
type
Po
ssib
le re
spon
ses
Des
crip
tion
Req
uire
d fie
ld
Dem
ogra
phic
s
case
_id
D1
strin
g te
xt
Uni
que
ID a
utom
atic
ally
gen
erat
ed b
y N
etEp
i X
loca
l_ca
se_i
d D
2 st
ring
text
U
niqu
e ID
use
d by
repo
rting
sta
te
X su
rnam
e D
3 st
ring
text
Su
rnam
e of
cas
e X
give
n_na
mes
D
4 st
ring
text
G
iven
nam
es o
f cas
e X
stat
e D
5 st
ring
ACT
= Au
stra
lian
Cap
ital
Terri
tory
N
SW =
New
Sou
th W
ales
N
T =
Nor
ther
n Te
rrito
ry
QLD
= Q
ueen
slan
d SA
= S
outh
Aus
tralia
TA
S =
Tasm
ania
VI
C =
Vic
toria
W
A =
Wes
tern
Aus
tralia
. =
Unk
now
n
Not
ifyin
g st
ate
X

193
Asse
ssm
ent o
f sta
tus
cont
act_
type
1.
1 nu
mer
ic
1 =
Hea
lth c
are
wor
ker i
n a
regi
on o
f cur
rent
EVD
ac
tivity
2
= H
ealth
car
e of
EVD
ca
se in
Aus
tralia
3
= C
onta
ct o
f EVD
cas
e in
a re
gion
of c
urre
nt
EVD
act
ivity
4
= C
onta
ct o
f EVD
cas
e in
Aus
tralia
5
= Tr
avel
or l
ived
in
regi
on o
f cur
rent
EVD
ac
tivity
6
= O
ther
- pl
ease
spe
cify
Wha
t typ
e of
con
tact
has
the
pers
on h
ad w
ith a
ca
se o
f EVD
? X
cont
act_
type
_spe
c 1.
2 st
ring
text
Sp
ecify
"oth
er" t
ype
of c
onta
ct
X
test
ed
1.3
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Has
the
pers
on b
een
test
ed fo
r EVD
? If
yes
is
sele
cted
, ple
ase
use
EVD
cas
e fo
rm in
stea
d. A
s pe
r the
Ebo
lavi
rus
SoN
G, i
f a ri
sk a
sses
smen
t de
term
ines
that
a p
erso
n sh
ould
be
test
ed fo
r Eb
ola
viru
s, th
e pe
rson
sho
uld
be m
anag
ed a
s a
susp
ecte
d ca
se. I
f the
test
is n
egat
ive
for E
VD,
the
pers
on s
houl
d re
turn
to m
onito
ring
as a
con
tact
fo
r the
rem
aind
er o
f the
incu
batio
n pe
riod
(21
days
af
ter l
ast e
xpos
ure
to a
n EV
D c
ase
or le
avin
g re
gion
of c
urre
nt E
VD a
ctiv
ity)
X
Info
rmat
ion
dob
2.1
num
eric
da
te (D
D/M
M/Y
YYY)
D
ate
of b
irth
of c
ase
X
gend
er
2.2
num
eric
1 =
Mal
e 0
= Fe
mal
e 3
= O
ther
9
= U
nkno
wn
Gen
der o
f cas
e X

194
stat
e_re
side
2.
3 nu
mer
ic
1 =
Aust
ralia
n C
apita
l Te
rrito
ry
2 =
New
Sou
th W
ales
3
= N
orth
ern
Terri
tory
4
= Q
ueen
slan
d 5
= So
uth
Aust
ralia
6
= Ta
sman
ia
7 =
Vict
oria
8
= W
este
rn A
ustra
lia
9 =
Unk
now
n
Stat
e in
whi
ch p
erso
n re
side
s or
is p
rimar
ily
stay
ing
X
resi
denc
y 2.
4 nu
mer
ic
1 =
Aust
ralia
n re
side
nt
2 =
Mig
rant
3
= Sh
ort t
erm
vis
itor
4 =
Long
term
vis
itor
9 =
Unk
now
n
Res
iden
cy s
tatu
s X
Expo
sure
info
rmat
ion
date
_1st
_exp
3.
1 st
ring
date
(DD
/MM
/YYY
Y)
Dat
e of
firs
t kno
wn
expo
sure
to a
n EV
D c
ase
X la
st_e
xp
3.2
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
of la
st k
now
n ex
posu
re to
an
EVD
cas
e X
exp_
setti
ng
3.3
num
eric
1 =
Trav
el/w
ork
in re
gion
of
EVD
act
ivity
2
= H
ealth
car
e ov
erse
as
3 =
Hea
lth c
are
in
Aust
ralia
4
= H
ouse
hold
5
= Sc
hool
6
= Ae
ropl
ane
7 =
Oth
er -
plea
se s
peci
fy
9 =
Unk
now
n
Type
of s
ettin
g in
whi
ch e
xpos
ure
to a
n EV
D c
ase
occu
rred
X
othe
r_ex
p 3.
4 st
ring
text
Sp
ecify
"oth
er" e
xpos
ure
setti
ng
X

195
exp_
coun
try
3.5
strin
g te
xt (4
cha
ract
ers)
In w
hich
cou
ntry
did
exp
osur
e oc
cur?
Use
St
anda
rd A
ustra
lian
Cla
ssifi
catio
n of
Cou
ntrie
s (S
ACC
). ht
tp://
ww
w.a
bs.g
ov.a
u/au
ssta
ts/a
bs@
.nsf
/mf/1
269.
0
X
Trav
el e
xpos
ures
waf
r_tra
vel
4.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
case
trav
el to
an
area
in W
est A
frica
with
an
act
ive
EVD
out
brea
k X
regi
on1_
nam
e 4.
2 st
ring
text
N
ame
of th
e fir
st re
gion
trav
elle
d to
with
in th
e ac
tive
EVD
zon
e in
Wes
t Afri
ca
regi
on1_
arriv
al
4.3
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
arriv
ed in
the
first
EVD
act
ive
regi
on
re
gion
1_de
part
4.4
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
depa
rted
from
the
first
EVD
act
ive
regi
on
regi
on2_
nam
e 4.
5 st
ring
text
N
ame
of o
f the
sec
ond
regi
on tr
avel
led
to w
ithin
th
e ac
tive
EVD
zon
e in
Wes
t Afri
ca
regi
on2_
arriv
al
4.6
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
arriv
ed in
the
seco
nd E
VD a
ctiv
e re
gion
regi
on2_
depa
rt 4.
7 st
ring
date
(DD
/MM
/YYY
Y)
Dat
e de
parte
d fro
m th
e se
cond
EVD
act
ive
regi
on
regi
on3_
nam
e 4.
8 st
ring
text
N
ame
of o
f the
third
regi
on tr
avel
led
to w
ithin
the
activ
e EV
D z
one
in W
est A
frica
regi
on3_
arriv
al
4.9
strin
g da
te (D
D/M
M/Y
YYY)
D
ate
arriv
ed in
the
third
EVD
act
ive
regi
on
re
gion
3_de
part
4.10
st
ring
date
(DD
/MM
/YYY
Y)
Dat
e de
parte
d fro
m th
e th
ird E
VD a
ctiv
e re
gion
extra
_reg
ions
4.
11
strin
g te
xt
Prov
ide
info
rmat
ion
on a
dditi
onal
regi
ons
visi
ted.
Expo
sure
ris
k as
sess
men
t
Hig
her
risk
high
_nee
dle
5.1.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on re
ceiv
e a
need
le s
tick
inju
ry fr
om a
co
nfirm
ed c
ase
X
high
_flu
id
5.1.
2 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd b
lood
or
fluid
spl
ash
to m
ucou
s m
embr
ane
from
a
conf
irmed
cas
e?
X

196
high
_ski
n 5.
1.3
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd th
eir
skin
touc
hed
bloo
d, v
omit,
dia
rrhoe
a, u
rine,
sal
iva,
se
men
from
a c
onfir
med
cas
e?
X
high
_pro
cess
ed
5.1.
4 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd
proc
esse
d bl
ood
or b
ody
fluid
s fro
m a
con
firm
ed
case
in la
bora
tory
? X
high
_dea
d 5.
1.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd d
irect
co
ntac
t with
dea
d bo
dy o
r flu
id fr
om a
dea
d bo
dy
with
con
firm
ed E
VD, o
r sus
pect
ed to
hav
e EV
D,
outc
ome
not k
now
n or
cau
se o
f dea
th u
nkno
wn
in
an E
VD a
ffect
ed a
rea?
X
high
_ani
mal
s 5.
2.6
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
dire
ct c
onta
ct w
ith s
ick
or
dead
wild
ani
mal
s in
an
EVD
end
emic
regi
on?
X
Low
er
risk
low
_hou
seho
ld
5.2.
1 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Is th
e pe
rson
a h
ouse
hold
mem
ber o
f a c
onfir
med
ca
se?
X
low
_hcw
5.
2.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on w
ork
in a
med
ical
or n
ursi
ng
capa
city
car
ing
dire
ctly
for c
onfir
med
EVD
cas
es in
an
EVD
affe
cted
are
a?
X
low
_ski
n_flu
id
5.2.
3 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd to
uche
d sk
in o
r bod
y of
aliv
e co
nfirm
ed E
VD c
ase
with
no
visi
ble
body
flui
d?
X

197
low
_dro
plet
5.
2.4
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Was
ther
e po
tent
ial d
ropl
et e
xpos
ure
to a
co
nfirm
ed E
VD c
ase,
mea
ning
no
PPE
and
in
sam
e ro
om w
ith c
onfir
med
EVD
cas
e ac
tivel
y vo
miti
ng /
diar
rhoe
a / c
ough
/ AG
P (d
owng
rade
to
casu
al if
larg
e ro
om a
nd v
ery
dist
ant,
such
as
in a
ha
ll at
oth
er e
nd, o
r brie
fly th
e ot
her e
nd o
f tra
in
carri
age)
?
X
low
_illc
onta
ct
5.2.
5 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
dire
ct c
onta
ct w
ith a
n ill
pers
on o
r bod
y flu
ids
from
a p
erso
n of
unk
now
n he
alth
sta
tus
in a
EVD
affe
cted
are
a?
X
low
_min
e 5.
2.7
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on w
ork
in a
min
e / c
ave
inha
bite
d by
ba
t col
onie
s in
an
EVD
end
emic
regi
on?
X
Cas
ual
casu
al_3
feet
5.
3.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd h
ad
been
with
in 1
met
re o
r with
in th
e ro
om o
r car
e ar
ea
of a
n EV
D c
ase
for a
pro
long
ed p
erio
d of
tim
e?
X
casu
al_d
irect
cont
act
5.3.
2 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd h
ad
dire
ct c
onta
ct (e
.g. s
haki
ng h
ands
) with
an
EVD
ca
se?
X
casu
al_t
ouch
5.
3.3
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
inad
equa
te P
PE a
nd
pote
ntia
lly to
uche
d a
non -
visi
bly
stai
ned
surfa
ce in
a
room
occ
upie
d by
a c
onfir
med
cas
e of
EVD
(e.g
. w
as in
wai
ting
room
with
a c
ase,
was
on
a w
ard
roun
d of
a c
ase
and
did
not t
ouch
cas
e)?
X
casu
al_h
cw
5.3.
4 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on w
ork
in a
med
ical
or n
ursi
ng
capa
city
in A
ustra
lia a
nd c
ared
dire
ctly
for a
co
nfirm
ed E
VD c
ase
usin
g ad
equa
te P
PE?
X

198
casu
al_c
lean
er
5.3.
5 nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Was
the
pers
on a
cle
aner
on
a w
ard
with
a
conf
irmed
cas
e an
d w
ore
adeq
uate
PPE
whe
n cl
eani
ng ro
om?
X
No
risk
NA
5.4
NA
NA
Info
rmat
iona
l sec
tion
abou
t "N
o R
isk"
cat
egor
y
Asse
ssed
Ris
k C
ateg
oris
atio
n ris
k_ca
t 6.
1 nu
mer
ic
1 =
Hig
her r
isk
2 =
Low
er ri
sk
3 =
Cas
ual r
isk
4 =
No
risk
Base
d on
the
risk
asse
ssm
ent c
riter
ia, p
leas
e se
lect
the
appr
opria
te ri
sk c
ateg
ory.
If th
ere
are
mul
tiple
exp
osur
es in
diff
eren
t cat
egor
ies,
con
side
r th
e hi
gher
risk
exp
osur
e as
the
case
’s ri
sk
cate
gory
.
X
Clin
ical
Sym
ptom
s sy
mpt
oms
7.1
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
/doe
s th
e pe
rson
hav
e a
feve
r or h
isto
ry o
f fe
ver i
n th
e pa
st 2
4 ho
urs,
abd
omin
al p
ain,
di
arrh
oea,
fatig
ue, j
oint
or m
uscl
e pa
in, s
ever
e he
adac
he, v
omiti
ng o
r une
xpla
ined
ble
edin
g?
X
Tem
pera
ture
lo
ggin
g D
ay 0
day0
_am
date
8.
1.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
of l
ast e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day0
_am
feve
r 8.
1.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 0?
day0
_am
tem
p 8.
1.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 0
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day0
_pm
date
8.
1.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
of l
ast e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day0
_pm
feve
r 8.
1.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
0?

199
day0
_pm
tem
p 8.
1.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 0
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
1
day1
_am
date
8.
2.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
1 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
_am
feve
r 8.
2.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 1?
day1
_am
tem
p 8.
2.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
_pm
date
8.
2.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
1 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
_pm
feve
r 8.
2.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
1?
day1
_pm
tem
p 8.
2.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
2
day2
_am
date
8.
3.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
2 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day2
_am
feve
r 8.
3.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 2?
day2
_am
tem
p 8.
3.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 2
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.

200
day2
_pm
date
8.
3.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
2 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day2
_pm
feve
r 8.
3.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
2?
day2
_pm
tem
p 8.
3.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 2
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
3
day3
_am
date
8.
4.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
3 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day3
_am
feve
r 8.
4.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 3?
day3
_am
tem
p 8.
4.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 3
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day3
_pm
date
8.
4.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
3 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day3
_pm
feve
r 8.
4.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
3?
day3
_pm
tem
p 8.
4.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 3
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
4
day4
_am
date
8.
5.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
4 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken

201
day4
_am
feve
r 8.
5.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 4?
day4
_am
tem
p 8.
5.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 4
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day4
_pm
date
8.
5.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
4 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day4
_pm
feve
r 8.
5.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
4?
day4
_pm
tem
p 8.
5.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 4
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
5
day5
_am
date
8.
6.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
5 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day5
_am
feve
r 8.
6.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 5?
day5
_am
tem
p 8.
6.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 5
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day5
_pm
date
8.
6.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
5 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day5
_pm
feve
r 8.
6.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
5?

202
day5
_pm
tem
p 8.
6.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 5
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
6
day6
_am
date
8.
7.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
6 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day6
_am
feve
r 8.
7.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 6?
day6
_am
tem
p 8.
7.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 6
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day6
_pm
date
8.
7.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
6 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day6
_pm
feve
r 8.
7.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
6?
day6
_pm
tem
p 8.
7.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 6
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
7
day7
_am
date
8.
8.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
7 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day7
_am
feve
r 8.
8.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 7?
day7
_am
tem
p 8.
8.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 7
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.

203
day7
_pm
date
8.
8.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
7 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day7
_pm
feve
r 8.
8.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
7?
day7
_pm
tem
p 8.
8.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 7
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
8
day8
_am
date
8.
9.1
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
mor
ning
tim
e on
day
8 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day8
_am
feve
r 8.
9.2
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 8?
day8
_am
tem
p 8.
9.3
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 8
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day8
_pm
date
8.
9.4
num
eric
da
te (D
D/M
M/Y
YYY)
and
tim
e D
ate
and
afte
rnoo
n tim
e on
day
8 p
ost-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day8
_pm
feve
r 8.
9.5
num
eric
1
= Ye
s 0
= N
o 9
= U
nkno
wn
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
8?
day8
_pm
tem
p 8.
9.6
num
eric
nu
mbe
r bet
wee
n 20
and
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 8
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
9
day9
_am
date
8.
10.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 9
pos
t-exp
osur
e at
w
hich
tem
pera
ture
was
take
n

204
day9
_am
feve
r 8.
10.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 9?
day9
_am
tem
p 8.
10.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 9
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day9
_pm
date
8.
10.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 9
pos
t-exp
osur
e at
w
hich
tem
pera
ture
was
take
n
day9
_pm
feve
r 8.
10.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
9?
day9
_pm
tem
p 8.
10.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 9
? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
10
day1
0_am
date
8.
11.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
0 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
0_am
feve
r 8.
11.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 10
?
day1
0_am
tem
p 8.
11.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
0? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
0_pm
date
8.
11.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
0 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
0_pm
feve
r 8.
11.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
10?

205
day1
0_pm
tem
p 8.
11.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
0? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
11
day1
1_am
date
8.
12.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
1 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
1_am
feve
r 8.
12.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 11
?
day1
1_am
tem
p 8.
12.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
1? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
1_pm
date
8.
12.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
1 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
1_pm
feve
r 8.
12.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
11?
day1
1_pm
tem
p 8.
12.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
1? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
12
day1
2_am
date
8.
13.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
2 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
2_am
feve
r 8.
13.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 12
?
day1
2_am
tem
p 8.
13.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
2? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.

206
day1
2_pm
date
8.
13.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
2 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
2_pm
feve
r 8.
13.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
12?
day1
2_pm
tem
p 8.
13.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
2? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
13
day1
3_am
date
8.
14.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
3 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
3_am
feve
r 8.
14.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 13
?
day1
3_am
tem
p 8.
14.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
3? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
3_pm
date
8.
14.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
3 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
3_pm
feve
r 8.
14.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
13?
day1
3_pm
tem
p 8.
14.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
3? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
14
day1
4_am
date
8.
15.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
4 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken

207
day1
4_am
feve
r 8.
15.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 14
?
day1
4_am
tem
p 8.
15.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
4? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
4_pm
date
8.
15.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
4 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
4_pm
feve
r 8.
15.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
14?
day1
4_pm
tem
p 8.
15.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
4? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
15
day1
5_am
date
8.
16.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
5 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
5_am
feve
r 8.
16.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 15
?
day1
5_am
tem
p 8.
16.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
5? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
5_pm
date
8.
16.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
5 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
5_pm
feve
r 8.
16.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
15?

208
day1
5_pm
tem
p 8.
16.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
5? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
16
day1
6_am
date
8.
17.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
6 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
6_am
feve
r 8.
17.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 16
?
day1
6_am
tem
p 8.
17.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
6? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
6_pm
date
8.
17.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
6 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
6_pm
feve
r 8.
17.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
16?
day1
6_pm
tem
p 8.
17.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
6? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
17
day1
7_am
date
8.
18.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
7 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
7_am
feve
r 8.
18.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 17
?
day1
7_am
tem
p 8.
18.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
7? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.

209
day1
7_pm
date
8.
18.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
7 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
7_pm
feve
r 8.
18.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
17?
day1
7_pm
tem
p 8.
18.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
7? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
18
day1
8_am
date
8.
19.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
8 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day1
8_am
feve
r 8.
19.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 18
?
day1
8_am
tem
p 8.
19.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
8? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
8_pm
date
8.
19.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
8 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
8_pm
feve
r 8.
19.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
18?
day1
8_pm
tem
p 8.
19.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
8? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
19
day1
9_am
date
8.
20.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 1
9 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken

210
day1
9_am
feve
r 8.
20.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 19
?
day1
9_am
tem
p 8.
20.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 1
9? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day1
9_pm
date
8.
20.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 1
9 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day1
9_pm
feve
r 8.
20.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
19?
day1
9_pm
tem
p 8.
20.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 1
9? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
20
day2
0_am
date
8.
21.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 2
0 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day2
0_am
feve
r 8.
21.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 20
?
day2
0_am
tem
p 8.
21.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 2
0? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day2
0_pm
date
8.
21.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 2
0 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day2
0_pm
feve
r 8.
21.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
20?

211
day2
0_pm
tem
p 8.
21.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 2
0? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Day
21
day2
1_am
date
8.
22.1
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d m
orni
ng ti
me
on d
ay 2
1 po
st-e
xpos
ure
at
whi
ch te
mpe
ratu
re w
as ta
ken
day2
1_am
feve
r 8.
22.2
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e m
orni
ng o
n da
y 21
?
day2
1_am
tem
p 8.
22.3
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e m
orni
ng
on d
ay 2
1? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pr
esen
t.
day2
1_pm
date
8.
22.4
nu
mer
ic
date
(DD
/MM
/YYY
Y) a
nd
time
Dat
e an
d af
tern
oon
time
on d
ay 2
1 po
st-e
xpos
ure
at w
hich
tem
pera
ture
was
take
n
day2
1_pm
feve
r 8.
22.5
nu
mer
ic
1 =
Yes
0 =
No
9 =
Unk
now
n
Did
the
pers
on h
ave
a fe
ver i
n th
e af
tern
oon
on
day
21?
day2
1_pm
tem
p 8.
22.6
nu
mer
ic
num
ber b
etw
een
20 a
nd
50
Wha
t was
the
tem
pera
ture
reco
rded
in th
e af
tern
oon
on d
ay 2
1? R
ecor
d te
mpe
ratu
re e
ven
if no
feve
r pre
sent
.
Dat
a en
try
inte
rvie
wer
_det
ails
9.
1 st
ring
text
Pa
ste
in e
mai
l sig
natu
re b
lock
of i
nter
view
er
X

212
Appendix 4: List of questions for Stakeholders
Questions for Ebola Response Taskforce – face to face discussion
1. Do you consider the EVD surveillance system to be simple to use and
understand?
2. How could it be simplified or streamlined?
3. How well do you feel our surveillance measures achieved the objectives of
prevention and control?
4. Were the reports (border surveillance/testing and monitoring) useful?
5. Did the information contained in the reports provide the information the EVD
taskforce required?
6. What other information would have been useful?
7. Was there any information gathered that was unnecessary?
8. Was the information shared in a timely manner?
9. How could this have been improved?
10. Do you have any other comments?
Questions for CDNA members – Out of session item and SurveyMonkey survey
1. On a scale of 1 to 5, where 1 is poor and 5 is excellent, how would you rate the
overall usefulness of the following and why?
a. Reporting to jurisdictions of people identified at the border as having
been in an EVD epidemic area
b. Weekly reporting of border surveillance summary
c. Weekly reporting of testing and monitoring summary
d. NetEpi EVD instance for case reporting (for those who are using it)
2. What specific information provided by each of the enhanced active surveillance
measures was the most useful from the jurisdictional perspective, and why?
a. Reporting to jurisdictions of people identified at the border as having
been in an EVD epidemic area
b. Weekly reporting of border surveillance
c. Weekly reporting of testing and monitoring (national)
3. How did you use the data from each of the additional components? For
example for planning, briefings, assignment of rosters for on call work.
a. Reporting to jurisdictions of people identified at the border as having
been in an EVD epidemic area
b. Weekly reporting of border surveillance
c. Weekly reporting of testing and monitoring (national)

213
d. NetEpi EVD instance for case reporting (for those who are using it)
4. How could each component be improved (if at all)?
a. Reporting to jurisdictions of people identified at the border as having
been in an EVD epidemic area
b. Weekly reporting of border surveillance
c. Weekly reporting of testing and monitoring (national)
d. NetEpi EVD instance for case reporting (for those who are using it)
5. Is weekly reporting of border and testing/monitoring data the best frequency of
reporting? If not, why not and what would you suggest?
6. Who would be best for me to talk to in your jurisdiction about day to day use of
the system? For example, would contacting the person who sends the testing
and monitoring email be best?
Questions for Jurisdictional users – telephone conversation Case data management - NetEpi – SA and NT
1. On a scale of 1 to 5 where 1 is hard and 5 is simple, how easy is it to enter data
into NetEpi? – SA and NT only
2. Why did you provide that rating? How could it be improved?
3. Was having the control form in NetEpi useful to you? Scale of 1 to 5
4. What was or wasn’t useful about it – how could it be improved?
5. Was using NetEpi acceptable?
6. How could it be made more acceptable?
7. Do you initially collect the information on paper, and how long between
collecting the information and entering it into NetEpi?
NetEpi – all other states 1. Why did you decide not to use NetEpi for contact management?
Laboratory testing and temperature monitoring 1. On a scale of 1 to 5 where 1 is hard and 5 is simple, how easy is it to extract the
data you are required to email to me weekly?
2. Why? And how could it be improved?
3. Are the fields easy to interpret?
4. Is the method of sharing testing and monitoring data easy? i.e. email
5. What would make it easier or simpler?
6. Is weekly reporting of testing and monitoring enough? Too much?
7. Do you receive the weekly summary?
8. Do you use the information in the summary?
a. Is it useful?

214
9. What was the time between onset of symptoms compatible with EVD and
testing and/or isolation?
Border surveillance 1. Is the information provided through border screening useful to you?
2. Why or why not?
3. What information that is provided is most useful?
4. Is there any information that is not provided that would be useful?
5. How do you use the provided data? E.g planning, briefings, assignment of
rosters etc
6. Do you receive the weekly border summary?
a. Is it useful?
Overall 1. Is this system the best way to manage the national side of the outbreak and
surveillance?
2. Do you have any suggestions that would improve it?
3. Do you have any other comments?
Questions for Department of Agriculture 1. How easy is it (on a scale of 1 to 5 where 1 is hard and 5 is easy) to enter data into
the Ag run database?
2. Why did you give this rating and do you have any suggestions on how it could be
improved?
3. Is the method of downloading and sharing this data to Health simple? Use the 1 to
5 scale again.
4. Why did you give this rating and do you have any suggestions on how it could be
improved?
5. Is this system the best way to manage the response to the outbreak? If not, what
would have been better?
6. What is the time lag between screening a passenger and entering the data into the
database?
7. Do you have any other comments?

215
Chapter 4 The effect of culture independent
diagnostic testing on the diagnosis and reporting of enteric bacterial pathogens in
Queensland, 2010 to 2014

216
Table of contents Prologue ................................................................................................................ 217
Study rationale ................................................................................................... 217
My role ............................................................................................................... 217
Lessons learned ................................................................................................ 217
Public health implications of this work ................................................................ 218
Acknowledgements ............................................................................................ 218
Master of Philosophy (Applied Epidemiology) core activity requirement ............. 218
Abstract ................................................................................................................. 218
Introduction ........................................................................................................... 220
Aim of study .......................................................................................................... 222
Methods ................................................................................................................ 222
Ethics approval .................................................................................................. 222
Laboratory processes ........................................................................................ 222
Data collection ................................................................................................... 222
Data analysis ..................................................................................................... 223
Testing for enteric bacteria at primary pathology laboratories ......................... 223
Community outbreaks of enteric bacteria ....................................................... 225
Results .................................................................................................................. 225
Laboratory process ............................................................................................ 225
Testing for enteric bacteria at primary pathology laboratories ............................ 228
Referral of enteric bacteria to QHFSS ................................................................ 242
Community outbreaks of enteric bacteria ........................................................... 246
Discussion ............................................................................................................. 247
References ............................................................................................................ 251
Appendix 1: Laboratory process questionnaire ...................................................... 253
Appendix 2: Data dictionary for analysis*............................................................... 255

217
Prologue
Study rationale Over the last few years, public health laboratories across Australia have been
introducing culture independent diagnostic techniques for testing of clinical samples for
the presence of pathogens causing disease. In Queensland (QLD), both private
pathology laboratories (Queensland Medical Laboratory (QML) and Sullivan Nicolaides
Pathology (SNP)) introduced culture independent diagnostic testing (CIDT) for bacterial
enteric pathogens in late 2013, while the public pathology laboratory, Pathology QLD
introduced CIDT in late 2015. As with any change in diagnostic methods, it is important
to understand the effect of the change from culture-based tests to culture independent
tests on the diagnosis and surveillance of enteric diseases.
My role I designed and conducted this study, including preparing the proposal, applying for
ethics approval, liaising with stakeholders, coordinating data collation and analysing the
data.
Lessons learned This project required coordination of stakeholders from several different locations, most
of which were in a different part of the country from me. I hadn’t met many of them
before, so it was useful to organise a meeting with everyone when I was in Brisbane for
a conference. Meeting people face to face helps with communication down the track,
especially when you have to ask people for something.
Although I had applied for animal ethics approval before, this was my first time applying
for human ethics approval. Obtaining human ethics approval is more complicated than
applying for animal ethics approval. While the experience was useful, in the end it
turned out that I probably didn’t need to obtain ethics approval for this study since it
used only de-identified data. It is a good idea to talk to the staff at the ethics office
before you apply – these people know best what types of studies require ethics
approval.
The data for this project was provided by several different laboratories, and as a result
was in different formats, requiring a lot of cleaning before the data could be combined.
String functions in Stata were a lifesaver, in particular the function ‘strpos’ – which finds
a particular part of a string within a variable. From there you can generate new
variables or replace values using the information, or list, table or count only those with
the string.

218
Public health implications of this work Laboratory notifications of enteric pathogens such as Salmonella increased in 2014
and 2015. This increase coincided with the introduction of CIDT at QML and SNP. As a
result, it was unclear if the increase in laboratory notifications of enteric pathogens was
a real increase in disease incidence or was an artefact of the change in testing
practices due to more sensitive tests detecting cases that were previously undetected.
Time and effort in public health surveillance units may be needlessly expended on
investigating what was thought to be an increase in disease incidence only to find it
was an artefact of changed sensitivity of laboratory testing practices. This study
determined that the increase in notifications of Salmonella in QLD during 2014 was a
true increase in the incidence of the disease. However, the increase in notifications of
Campylobacter, Shigella and Yersinia was likely to be a combination of increased
incidence and the increased sensitivity of the testing methods used (CIDT). This
information can be used to plan public health surveillance and policy. In addition, this
study documented for the first time the laboratory testing procedures for Salmonella,
Campylobacter, Shigella and Yersinia in use at all pathology laboratories in QLD to
enable coordinated planning of testing practices in QLD and incorporate advances in
diagnostic technologies without losing the information required for public health
surveillance.
Acknowledgements Thanks to all those involved in every step of this project. Ben Polkinghorne from the
Australian Government Department of Health (OzFoodNet), Emily Fearnley and Martyn
Kirk from the National Centre for Epidemiology and Population Health, Russell Stafford
and Heidi Carroll from QLD Health, John Bates from QLD Health Forensic and
Scientific Services, Renu Vohra from QML, Jenny Robson from SNP and Graeme
Nimmo from Pathology QLD.
Master of Philosophy (Applied Epidemiology) core activity requirement Design and conduct an epidemiological study.
Abstract Culture-independent diagnostic testing (CIDT) for testing of samples for the presence
of enteric pathogens has been introduced to all three primary pathology laboratories in
Queensland, as of November 2015. Changes in testing methods for pathogens should
be assessed to determine their impact on public health surveillance through changed
sensitivity of testing. Changes in testing sensitivity can affect the apparent incidence of
the disease by diagnosing cases that would otherwise have remained undiagnosed

219
using the previously used test if the new test is more sensitive than the old test, or may
miss cases that would have been diagnosed if the new test is less sensitive. This study
aimed to assess the impact of the introduction of CIDT on testing for four enteric
pathogens in Queensland and to document the current testing protocol in each primary
laboratory and the Queensland reference laboratory.
Laboratory process data was obtained from the laboratories by questionnaire. Primary
testing and demographic data was obtained from Queensland Medical Laboratory
(QML), Sullivan Nicolaides Pathology (SNP) and Pathology Queensland (the primary
laboratories) and subtyping data was obtained from Queensland Health Forensic and
Scientific Services (the reference laboratory). Tests that were positive for Salmonella,
Campylobacter, Shigella and Yersinia between 2010 and 2014, inclusive, were
analysed by type of test performed. The percent of tests positive was calculated using
the total number of tests for gastroenteritis performed by each laboratory as the
denominator. The incidence of positive tests after the introduction of CIDT was
compared with positive tests before the introduction of CIDT. Information about
outbreaks of Salmonella, Campylobacter, Shigella and Yersinia between 2010 and
2014, inclusive, were extracted from the Queensland OzFoodNet Outbreak Register,
and assessed for whether they would have been identified without subtyping
information on isolates from the cases and source.
Only QML and SNP introduced CIDT during the study period (August 2013 and
November 2013 respectively) and both laboratories continue to culture samples, either
concurrently with CIDT or reflexively for samples positive by CIDT. The number of tests
positive for all four pathogens increased in 2014, after introduction of CIDT at QML and
SNP. The increase in the number of tests positive for Salmonella was likely to be due
to a real increase in the incidence of the pathogen, but the reason for the increase in
the number of tests positive for Campylobacter, Shigella and Yersinia was less clear
and was likely to be a combination of a true increase in incidence and the increased
sensitivity of CIDT. After testing, 38% of samples positive for these four pathogens
were positive by CIDT only. Ten outbreaks of Salmonella between 2010 and 2014 did
not have a single point source and were identified based on subtyping information.
The introduction of CIDT in QLD has had an impact on the apparent incidence of the
enteric pathogens in this study due to increased sensitivity of the CIDT test, in
particular for Campylobacter, Shigella and Yersinia. This increased sensitivity of case
detection must be considered when assessing disease trends and the burden of
disease. Continued culture of samples will ensure the availability of isolates for
outbreak detection and public health surveillance.

220
Introduction Recent advances in laboratory technologies have made techniques that were once
only in the realm of research cheap and simple enough for routine use in diagnostic
pathology laboratories (1). Until late 2013, growth of organisms by culture and
characterisation of the cultured isolates was the predominant form of identification for
enteric bacterial pathogens in Queensland (QLD), but culture-independent diagnostic
testing (CIDT) has become widely used across the state since late 2013. Any change
in testing procedures may impact on public health surveillance and detection of
common source outbreaks. This project aims to investigate how changes in testing
methods, specifically the move from culture-based methods to CIDT, have affected
public health surveillance of enteric pathogens in QLD.
In addition to information about the identity of the causative agent, the information from
pathology testing data that is required for public health action is different from that
required for clinical treatment. At the level of the individual, the identity of the pathogen
and antibiotic sensitivity for some pathogens is often all that is required to inform
clinical treatment and prevention of transmission. In some cases, such as for most
enteric pathogens, even identity is not needed for clinical management as in most
cases, treatment involves rehydration and management of the symptoms (2). However,
for public health surveillance purposes, including examining trends in disease and
detection of outbreaks, additional information about the pathogen strain or serotype is
essential. Traditional methods of culture and further characterisation of the isolates
provides information for both these purposes. However, this relies on the ability to
culture the infectious agent. Unless information is available implicating a specific
pathogen, stool samples are plated on multiple selective (allows the growth of only
certain types of bacteria) or differential (incorporates chemicals that change colour
depending on the metabolites produced by certain types of bacteria) agar plates in
order to grow the pathogen present in the sample while minimising the growth of the
normal flora present in the sample. Some agents, such as Campylobacter (3) and
Shigella (4) are fastidious and difficult to culture, meaning that they may be
underdiagnosed as a cause of diarrhoeal illness using traditional culture diagnostic
methods. Introduction of CIDT for difficult to culture pathogens may result in an
increase in the number of cases identified.
Culture-independent technologies include any test that does not require the agent to be
cultured prior to identification. CIDT currently used by pathology laboratories worldwide
include tests that amplify and/or detect nucleic acid (most commonly polymerase chain
reaction [PCR]) and tests that detect antigens (such as enzyme immunoassays) (1).
These tests are fast, easy, sensitive and reliable, but are unable to identify antibiotic

221
sensitivity (required to inform treatment for some diseases) or serotypes (required to
link cases in an outbreak) (5-7). The improvement in sensitivity will provide a more
accurate estimate of the burden of disease, and the ability of multiplex PCR to detect
polymicrobial infections will provide new insight into diseases and disease interactions
(1). However, the change in sensitivity will need to be considered when interpreting
disease trends over time (1). The currently recommended method to avoid this loss of
information is to concurrently culture all samples that undergo CIDT, or reflexively
culture all CIDT positive samples (6). This doubling up of testing methods is time and
resource intensive, thus hoped to be temporary. Newer technologies, such as
metagenomics, are currently gaining popularity in the research setting, and will provide
molecular characterisation that will replace the need for culture and culture dependent
characterisation. The introduction of CIDT will have immediate impacts on the
laboratories themselves, both primary pathology laboratories and public health
reference laboratories, including on-cost, storage and human resources (including
training). CIDT will also have an impact on the public health surveillance system,
especially if the greater sensitivity of CIDT results in an increase in the numbers of
cases of disease identified, leading to additional workload for public health staff.
Current CIDT techniques also result in a loss of serotyping and molecular
characterisation, which may lead to a decrease in the number of outbreaks identified.
A study conducted on data collected between 2012 and 2014 by the Centers for
Disease Control and Prevention (CDC) Foodborne Diseases Active Surveillance
Network (FoodNet) assessed the impact of CIDT on public health surveillance of
enteric pathogens in the United States (US). FoodNet reported that 46% of CIDT
positive samples were not confirmed by culture, where 22% were culture negative, and
culture was not attempted for 24% (8). It is difficult to know whether the culture
negative samples were falsely positive by CIDT, or were true positives that would have
remained undiagnosed had they been tested by culture alone. Not all laboratories
surveyed were using CIDT, and CIDT methods were most commonly used to identify
Campylobacter (8).
Clinical pathology in QLD is dominated by two private primary pathology laboratories
(Queensland Medical Laboratory [QML] and Sullivan Nicolaides Pathology [SNP]) and
one public primary laboratory (Pathology QLD), and one reference laboratory
(Queensland Health Forensic and Scientific Services [QHFSS]). Approximately 8000
cases of foodborne illness are reported annually in QLD. Salmonella (other than
Typhoid or Paratyphoid) and Campylobacter together contribute more than 90% of the
foodborne illnesses notified to Queensland Health every year. Shigella and Yersinia

222
have the next two highest numbers of yearly notifications (~1% of notifications each)
(9). Therefore, these four pathogens were selected to be included in this study.
Aim of study The aim of this study was to document the move from traditional culture based
methods to culture independent methods for identification of bacterial enteric
pathogens in QLD by comparing testing practices at the three primary diagnostic
laboratories and one reference laboratory, and identifying changes in numbers of
positive tests for Salmonella, Campylobacter, Shigella and Yersinia.
Methods
Ethics approval Human research ethics approval for the study was obtained through both the Australian
National University Research Ethics Committee (reference number 2015/429) and the
Royal Brisbane and Women’s Hospital Human Research Ethics Committee (reference
number HREC/15/QRBW/404).
Laboratory processes In order to establish the routine procedure for testing clinical samples for enteric
bacteria for each QLD pathology laboratory, process data for samples tested for
Salmonella, Campylobacter, Shigella and Yersinia were collected from all four
laboratories (QML, SNP, Pathology QLD and QHFSS) through a questionnaire sent to
co-investigators on 8 September 2015 (Appendix 1). Data collected included
information about when the laboratory introduced CIDT, whether they routinely test for
each pathogen, what they do when CIDT and culture results are discordant and
whether they refer the pathogen to the reference laboratory for further subtyping. The
questionnaire was designed as a Microsoft Excel spreadsheet with set response
options where possible to limit the answers available. This qualitative data was collated
and summarised using Microsoft Excel.
Data collection The data provided by the laboratories included all testing results for stool samples that
were positive for Salmonella, Campylobacter, Shigella or Yersinia performed between
2010 and 2014, inclusive. Each laboratory provided the data as a line list, with the
minimum fields of laboratory identification number, date the sample was received by
the laboratory, the age or date of birth of the patient, the postcode of the patient, the
organisms identified by culture, and the results of PCR testing where applicable. In
addition, QML provided the date the pathogen was identified, allowing a calculation of

223
time from receipt of the sample to identification of the pathogen. QML also provided
information about what type of test was requested. QHFSS provided data on subtyping
and biotyping of the pathogens isolated. QHFSS also provided laboratory reference
numbers allowing linkage of samples with the primary referring laboratory.
Data analysis Testing for enteric bacteria at primary pathology laboratories All data was cleaned and analysed using StataSE 13 (Stata Corp, College Station, TX,
USA). The data provided by each laboratory was cleaned and prepared separately to
obtain common variable names and formats. If a date of birth was provided, the age at
the time of sample collection or receipt of the sample by the laboratory was calculated.
The data from QML, SNP and Pathology QLD were combined into a single data set
using the STATA append command. As Pathology QLD had not introduced PCR during
the period of this study, it is used as a baseline comparison of the change in incidence
during 2014 in a laboratory without PCR.
All samples that did not identify at least one of Salmonella, Campylobacter, Shigella or
Yersinia by culture or PCR at the primary laboratory or after referral to QHFSS were
excluded from the analysis, even if a different pathogen was identified. Thus a negative
value for a variable such as Salmonella PCR means only that the sample was negative
by that test method for that pathogen, and was not negative for all pathogens included
in this study. Samples positive only for Salmonella Typhi or Salmonella Paratyphi were
excluded as the public health response for these two pathogens is different from the
public health response for other Salmonella serovars.
The median number of tests positive and the percent of tests positive (percent
positivity) were calculated for each pathogen by month of sample receipt. The
denominator data used to calculate the percent positivity was obtained from the
laboratories, and was the total number of tests for bacterial enteric pathogens
conducted during each month. Graphs of the median number of tests positive and
percent positivity were produced using Microsoft Excel.
Median counts and percent positivity before the introduction of CIDT (data from 2010 to
2012) and after the introduction of CIDT (data from 2014) were compared for all
laboratories whether they had introduced CIDT or not. Data from 2013 was not
included in the comparison as QML and SNP introduced CIDT in different months
during 2013 (August and November respectively). Significance was assessed using the
Wilcoxon rank-sum test. The difference in medians was considered significant if the p-
value was less than 0.05.

224
The time from sample receipt to identification of the pathogen was calculated for
samples tested by QML. The median time to identification before the introduction of
CIDT (data from 2010 to 2012) was compared with the median time to identification
after the introduction of CIDT (data from 2014). The significance of the difference in
medians was assessed using the Wilcoxon rank-sum test. A p-value less than 0.05
was considered significant.
A data set categorising postcodes into Australian Bureau of Statistics Remoteness
Areas was obtained from the Australian Government Department of Health Office of
Health Protection Data Managers. For the purposes of this study, the “Inner Regional
Australia” and “Outer Regional Australia” categories were combined into a single
category of “Regional Australia”. Similarly, “Remote Australia” and “Very Remote
Australia” were combined into a category of “Remote Australia”. The Remoteness Area
data set was merged with the laboratory testing data set using the postcode of the
patient.
QML offers three different options for testing of samples for enteric pathogens: CIDT
(PCR), culture alone, or culture and microscopy. Two types of tests (e.g. CIDT and
culture) can be requested on the same sample. The categories of “culture” and “culture
and microscopy” were combined for analysis, resulting in three testing options: CIDT
only, CIDT and culture and culture only. The type of test requested was compared by
Remoteness Area and age group of the patient using the chi-squared test.
Referral of enteric bacteria to QHFSS Data cleaning and analysis was performed using StataSE 13. The median number of
tests performed per month was compared using the Wilcoxon rank-sum test. The
difference in medians was considered significant if the p-value was less than 0.05.
The data provided by QHFSS was merged into the primary laboratory data set using
the laboratory numbers provided by the primary laboratory. Samples that were referred
from a laboratory other than QML, SNP or Pathology QLD were removed from the
subsequent analysis. Where names of towns were entered in the postcode field, they
were converted to postcodes using the Australia Post postcode finder
(http://auspost.com.au/apps/postcode.html). Duplicate entries were removed if all fields
were the same or combined if different results were entered for the same patient.
Samples that were identified as Salmonella at the primary laboratory but identified as
Salmonella Typhi or Salmonella Paratyphi at QHFSS were excluded from the analysis
of referral data if no other species of Salmonella was identified and if the sample was
negative for Campylobacter, Shigella and Yersinia.

225
Median counts and percent positivity were calculated and compared as for primary
laboratories. As QHFSS is the reference laboratory, the data form a subset of the tests
performed at the primary laboratories. The denominator number for QHFSS data was
the number of tests that were referred to QHFSS by the primary laboratories and were
positive for at least one of Salmonella, Campylobacter, Shigella and Yersinia at the
primary laboratory, QHFSS or both.
Community outbreaks of enteric bacteria Data for outbreaks caused by Salmonella, Campylobacter, Shigella and Yersinia in
QLD that were reported between 2010 and 2014 were extracted from the Microsoft
Access OzFoodNet Outbreak Register. Community based outbreaks (i.e. those that did
not have an obvious point source, such as a single restaurant or event) were
determined by analysing the setting in which the implicated food was prepared and
eaten, the case definition and other information about case finding that was entered in
the free-text remarks field of the Register. Information on subtyping of isolates that was
used to link cases and the source of the outbreak (food or water) was analysed.
Results
Laboratory process The routine procedure for all four laboratories in QLD is similar, with only minor
differences (Table 1).
QML culture stool samples for the bacterial pathogens of Salmonella, Campylobacter,
Shigella. Stools are only cultured for and Yersinia when requested. They introduced
PCR in August 2013 and use a Roche brand multiplex PCR test for all four bacteria.
They only perform CIDT if the test is requested, and when requested, they concurrently
perform culture on the sample. In the event of a discordant result, where the sample
was PCR positive but culture negative, the result is reported as positive for Salmonella,
Campylobacter and Shigella without additional testing, but reflex culture is attempted
for samples that were PCR positive for Yersinia. They refer cultured isolates of
Salmonella, Shigella and Yersinia but not Campylobacter to QHFSS for further
characterisation. Stool samples positive for Salmonella and Shigella only by PCR are
referred to QHFSS for further culture.
SNP routinely culture stool samples for the bacterial pathogens of Salmonella,
Campylobacter and Shigella, but only culture stool samples for the bacterial pathogen
of Yersinia on request. They introduced PCR in November 2013 and use the same
Roche brand multiplex PCR test used by QML. They test the samples for the presence
of Salmonella, Campylobacter and Shigella concurrently with PCR. As the PCR also
includes primers for Yersinia, they attempt to culture Yersinia if the PCR test is positive

226
for Yersinia (reflex testing). They refer isolates of Salmonella, Shigella and Yersinia but
not Campylobacter to QHFSS for further characterisation. They discard PCR
positive/culture negative samples after seven days without referral to QHFSS. These
samples are reported as positive for the pathogen detected.
Pathology QLD introduced an in-house designed multiplex PCR test for enteric
pathogens in September 2015 and reflexively culture only those samples that are
positive by PCR. However, during the period of data collection for this study (2010 to
2014) Pathology QLD had not yet introduced CIDT. They refer isolates of Salmonella,
Shigella and Yersinia to QHFSS for further typing.
QHFSS are the reference laboratory for QLD. They have not introduced any CIDT
methods to date (as of 1 November 2015).

227
Table 1: Routine procedures for Salmonella, Campylobacter, Shigella and Yersinia as reported
by Queensland laboratories in September and October 2015
Salmonella Campylobacter Shigella Yersinia
Routinely test
QML Yes Yes Yes Yes SNP Yes Yes Yes If requested
Pathology QLD Yes Yes Yes Yes
QHFSS Yes Yes Yes Yes
Use culture
QML If requested If requested If requested If requested SNP Yes Yes Yes Yes
Pathology QLD Yes Yes Yes Yes
QHFSS Yes Yes Yes Yes
Use CIDT
QML If requested If requested If requested If requested SNP Yes Yes Yes Yes
Pathology QLD Yes No Yes Yes
QHFSS No No No No
Type and brand of
CIDT
QML Roche PCR Roche PCR Roche PCR Roche PCR SNP Roche PCR Roche PCR Roche PCR Roche PCR
Pathology QLD
In house PCR Not done In house
PCR In house
PCR QHFSS Not done Not done Not done Not done
Timing of culture
with CIDT
QML Concurrent Concurrent Concurrent (reflexive if
unsuccessful) Concurrent
SNP Concurrent Concurrent Concurrent Reflexive Pathology
QLD Reflexive Not done Reflexive Reflexive
QHFSS Not done Not done Not done Not done
Referral of isolates to
QHFSS
QML Yes No Yes No SNP Yes No Yes Yes
Pathology QLD Yes No Yes Yes
QHFSS Not done Not done Not done Not done
Referral of CIDT
positive stool to QHFSS
QML Yes No Yes No SNP No No No No
Pathology QLD No Not done No No
QHFSS Not done Not done Not done Not done
Date CIDT introduce
d
QML August 2013 SNP November 2013
Pathology QLD September 2015*
QHFSS Not introduced (as of November 2015) * CIDT was introduced at Pathology QLD after the period of data collection for this study. During the period of data collection for this study (2010 to 2014), Pathology QLD used on culture for all four pathogens and referred all but Campylobacter to QHFSS. QML – Queensland Medical Laboratory; SNP – Sullivan Nicolaides Pathology; QHFSS – Queensland Health Forensic and Scientific Services; QLD - Queensland

228
Testing for enteric bacteria at primary pathology laboratories In Figure 1 (Salmonella), Figure 2 (Campylobacter), Figure 3 (Shigella) and Figure 4
(Yersinia), the type of test that resulted in the positive identification of the pathogen is
shown by year and month of test. Prior to the introduction of CIDT at QML in August
2013, all pathogens were identified by culture alone. With the introduction of CIDT, first
at QML in August 2013, and then at SNP in November 2013, the number of tests
positive by CIDT and culture or CIDT alone increased. After the introduction of CIDT,
most samples positive for Shigella (Figure 3) and Yersinia (Figure 4) were positive by
CIDT alone.

229
Figu
re 1
: Typ
e of
test
or t
ests
pos
itive
for S
alm
onel
la a
t the
thre
e pr
imar
y pa
thol
ogy
labo
rato
ries
in Q
ueen
slan
d be
twee
n 20
10 a
nd 2
014
by y
ear a
nd m
onth
of t
est.
CID
T –
cultu
re in
depe
nden
t dia
gnos
tic te
st
0
100
200
300
400
500
600
700
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Number of tests positive for Salmonella
Year
and
mon
th o
f tes
t
Cul
ture
CID
T an
d cu
lture
CID
T

230
Figu
re 2
: Typ
e of
test
or t
ests
pos
itive
for C
ampy
loba
cter
at t
he th
ree
prim
ary
path
olog
y la
bora
torie
s in
Que
ensl
and
betw
een
2010
and
201
4 by
yea
r and
mon
th o
f
test
. CID
T –
cultu
re in
depe
nden
t dia
gnos
tic te
st
0
100
200
300
400
500
600
700
800
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Number of tests positive for Campylobacter
Year
and
mon
th o
f tes
t
Cul
ture
CID
T an
d cu
lture
CID
T

231
Figu
re 3
: Typ
e of
test
or t
ests
pos
itive
for S
hige
lla a
t the
thre
e pr
imar
y pa
thol
ogy
labo
rato
ries
in Q
ueen
slan
d be
twee
n 20
10 a
nd 2
014
by y
ear a
nd m
onth
of t
est.
CID
T –
cultu
re in
depe
nden
t dia
gnos
tic te
st
0102030405060Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Number of tests positive for Shigella
Year
and
mon
th o
f tes
t
Cul
ture
CID
T an
d cu
lture
CID
T

232
Figu
re 4
: Typ
e of
test
or t
ests
pos
itive
for Y
ersi
nia
at th
e th
ree
prim
ary
path
olog
y la
bora
torie
s in
Que
ensl
and
betw
een
2010
and
201
4 by
yea
r and
mon
th o
f tes
t.
CID
T –
cultu
re in
depe
nden
t dia
gnos
tic te
st
01020304050607080Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Number of tests positive for Yersinia
Year
and
mon
th o
f tes
t
Cul
ture
CID
T an
d cu
lture
CID
T

233
The number of tests for enteric pathogens that were performed by each primary
laboratory (denominator) increased over time (Figure 5). The increase in the number of
tests performed at QML exceeded the increase at SNP, and the increase at both
exceeded the increase at Pathology QLD. The number of tests positive per month at
each laboratory is shown in Figure 6 (Salmonella), Figure 7 (Campylobacter), Figure 8
(Shigella) and Figure 9 (Yersinia) by each pathogen of interest.
Salmonella shows seasonality and an increase in the number of tests positive and
percent positivity at all laboratories during the summer of 2013-2014, whether they had
introduced CIDT or not (Figure 6). Pathology QLD has a higher rate of detection of
Salmonella than QML and SNP, but lower overall numbers.
The number of tests positive and the percent positivity for Campylobacter at all
laboratories decreased in early 2012 and has remained stable at Pathology QLD since
this time (Figure 7). In contrast, both the number of tests positive and the percent
positivity for Campylobacter at QML increased from September 2013. Testing for
Campylobacter at SNP also decreased in early 2012, but decreased again in mid-2013
to levels lower than QML and Pathology QLD. The median number of tests positive and
percent positivity at SNP increased back to 2012 levels beginning December 2013.
The number of tests positive and the percent positivity for Shigella increased
dramatically for both QML and SNP after introduction of CIDT. In contrast, the number
of tests positive and percent positivity at Pathology QLD remained constant between
2010 and 2014 (Figure 8).
Similarly, the number of tests positive and the percent positivity for Yersinia also
increased dramatically at QML and SNP after introduction of CIDT (Figure 9). In
contrast, the number of tests positive and the percent positivity remained constant at
Pathology QLD in 2014.

234
Figu
re 5
: Num
ber o
f tes
ts fo
r ent
eric
pat
hoge
ns p
erfo
rmed
by
each
labo
rato
ry, b
y m
onth
of t
est,
2010
- 20
14. C
IDT
was
intro
duce
d to
QM
L in
Sep
tem
ber 2
013
and
SNP
in N
ovem
ber 2
013.
QM
L –
Que
ensl
and
Med
ical
Lab
orat
ory;
SN
P –
Sulliv
an N
icol
aide
s Pa
thol
ogy;
QLD
– Q
ueen
slan
d
0
1,00
0
2,00
0
3,00
0
4,00
0
5,00
0
6,00
0
7,00
0
8,00
0
9,00
0Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Number of tests performed
Year
and
mon
th o
f tes
t
QM
LSN
PPa
thol
ogy
QLD

235
Figu
re 6
: Num
ber o
f tes
ts p
ositi
ve fo
r Sal
mon
ella
(bar
s) a
nd th
e pe
rcen
t of a
ll te
sts
that
wer
e po
sitiv
e fo
r Sal
mon
ella
(lin
es) b
y m
onth
, 201
0 - 2
014.
CID
T w
as
intro
duce
d to
QM
L in
Sep
tem
ber 2
013
and
SNP
in N
ovem
ber 2
013.
QM
L –
Que
ensl
and
Med
ical
Lab
orat
ory;
SN
P –
Sulliv
an N
icol
aide
s Pa
thol
ogy;
QLD
-
Que
ensl
and
-0.5
0
0.50
1.50
2.50
3.50
4.50
5.50
050100
150
200
250
300
350
400
450
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Percent of samples tested positive for Salmonella
Number of positive tests
Year
and
mon
th o
f tes
t
QM
L (n
)SN
P (n
)Pa
thol
ogy
QLD
(n)
QM
L (%
)SN
P (%
)Pa
thol
ogy
QLD
(%)

236
Figu
re 7
: Num
ber o
f tes
ts p
ositi
ve fo
r Cam
pylo
bact
er (b
ars)
and
the
perc
ent o
f all
test
s th
at w
ere
posi
tive
for C
ampy
loba
cter
(lin
es) b
y m
onth
, 201
0 - 2
014.
CID
T
was
intro
duce
d to
QM
L in
Sep
tem
ber 2
013
and
SNP
in N
ovem
ber 2
013.
QM
L –
Que
ensl
and
Med
ical
Lab
orat
ory;
SN
P –
Sulliv
an N
icol
aide
s Pa
thol
ogy;
QLD
-
Que
ensl
and
0.00
1.00
2.00
3.00
4.00
5.00
6.00
050100
150
200
250
300
350
400
450
500
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Percent of samples tested positive for Campylobacter
Number of positive tests
Year
and
mon
th o
f tes
t
QM
L (n
)SN
P (n
)Pa
thol
ogy
QLD
(n)
QM
L (%
)SN
P (%
)Pa
thol
ogy
QLD
(%)

237
Figu
re 8
: Num
ber o
f tes
ts p
ositi
ve fo
r Shi
gella
(bar
s) a
nd th
e pe
rcen
t of a
ll te
sts
that
wer
e po
sitiv
e fo
r Shi
gella
(lin
es) b
y m
onth
, 201
0 - 2
014.
CID
T w
as in
trodu
ced
to Q
ML
in S
epte
mbe
r 201
3 an
d SN
P in
Nov
embe
r 201
3. Q
ML
– Q
ueen
slan
d M
edic
al L
abor
ator
y; S
NP
– Su
llivan
Nic
olai
des
Path
olog
y; Q
LD -
Que
ensl
and
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
05101520253035Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Percent of samples tested positive for Shigella
Number of positive tests
Year
and
mon
th o
f tes
t
QM
L (n
)SN
P (n
)Pa
thol
ogy
QLD
(n)
QM
L (%
)SN
P (%
)Pa
thol
ogy
QLD
(%)

238
Figu
re 9
: Num
ber o
f tes
ts p
ositi
ve fo
r Yer
sini
a (b
ars)
and
the
perc
ent o
f all
test
s th
at w
ere
posi
tive
for Y
ersi
nia
(line
s) b
y m
onth
, 201
0 - 2
014.
CID
T w
as in
trodu
ced
to Q
ML
in S
epte
mbe
r 201
3 an
d SN
P in
Nov
embe
r 201
3. Q
ML
– Q
ueen
slan
d M
edic
al L
abor
ator
y; S
NP
– Su
llivan
Nic
olai
des
Path
olog
y; Q
LD –
Que
ensl
and
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0102030405060Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Percent of samples tested positive for Yersinia
Number of positive tests
Year
and
mon
th o
f tes
t
QM
L (n
)SN
P (n
)Pa
thol
ogy
QLD
(n)
QM
L (%
)SN
P (%
)Pa
thol
ogy
QLD
(%)

239
Table 2 shows the median number of samples that tested positive per month and the
percent positivity per month for each pathogen, by laboratory. The denominator data
(total number of tests performed for enteric pathogens) is also shown. The median
number of tests for enteric pathogens performed per month at each laboratory
increased significantly in 2014 (p-value <0.05).
The median number of tests positive for each of the four pathogens per month was
larger after the introduction of CIDT than before at the two laboratories that have
introduced CIDT (QML and SNP, p-value <0.05; Table 2). The number of tests positive
for Salmonella and Campylobacter doubled, while the number of tests positive for
Shigella and Yersinia increased between ten and twenty fold. In contrast, although the
median number of tests for Salmonella, Shigella and Yersinia has increased over time
at Pathology QLD (which had not introduced CIDT at the time this data was collected),
this difference was not significant with the exception of tests positive for Yersinia. The
number of tests positive for Campylobacter at Pathology QLD decreased in 2014,
although this decrease was not significant.
The difference in percent positivity before and after introduction of CIDT was significant
for all bacterial pathogens under study at both QML and SNP, with the exception of
Salmonella at QML. All changes in percent positivity at QML and SNP were an
increase with the exception of percent positivity for Campylobacter at SNP which
decreased in 2014 (p <0.05). The change in percent positivity for Campylobacter at
Pathology QLD, a decrease, was significant while the change in the percent positivity
for the other three pathogens (an increase) was not significant for tests at Pathology
QLD.
The increase in testing at the primary laboratories was reflected in an increase in
referrals and testing at the reference laboratory, QHFSS, for Salmonella, Shigella and
Yersinia. No laboratories routinely refer samples positive for Campylobacter to QHFSS.
The increase in percent positivity was significant (p < 0.05) for Shigella and Yersinia.

240
Tabl
e 2:
Med
ian
num
ber o
f pos
itive
test
s pe
r mon
th, p
erce
nt p
ositi
vity
and
the
tota
l num
ber o
f tes
ts p
erfo
rmed
for e
nter
ic p
atho
gens
by
labo
rato
ry, i
n pe
riod
of
test
ing
by c
ultu
re (2
010
to 2
012)
com
pare
d to
CID
T pe
riod
(201
4). T
he m
edia
n nu
mbe
r and
per
cent
pos
itivi
ty fo
r the
prim
ary
labo
rato
ries
com
bine
d is
sha
ded
Salm
onel
la
Cam
pylo
bact
er
Shig
ella
Ye
rsin
ia
Den
omin
ator
20
10
to
2012
20
14
p-va
lue
2010
to
20
12
2014
p-
valu
e 20
10
to
2012
20
14
p-va
lue
2010
to
20
12
2014
p-
valu
e 20
10 to
20
12
2014
p-
valu
e
Med
ian
num
ber
of
sam
ples
po
sitiv
e pe
r m
onth
QM
L 85
19
0 <0
.001
16
7 31
9 <0
.001
0
22
<0.0
01
2 35
<0
.001
42
29
7097
<0
.001
SN
P 82
14
4 <0
.001
15
9 19
2 0.
04
2 18
<0
.001
1
14
<0.0
01
4221
55
41
<0.0
01
Path
olog
y Q
LD
77
95
0.11
10
3 88
0.
12
3 4
0.49
2
3 0.
02
2744
29
63
<0.0
01
Tota
l 24
5 45
0 <0
.001
43
6 58
4 <0
.001
6
45
<0.0
01
6 48
<0
.001
11
288
1559
8 <0
.001
Q
HFS
S 20
6 34
1 0.
009
6 1
<0.0
01
5 15
<0
.001
5
20
<0.0
01
261
354
0.02
Perc
ent
of a
ll sa
mpl
es
test
ed
that
wer
e po
sitiv
e
QM
L 1.
91
2.51
0.
06
3.83
4.
40
0.01
0
0.33
<0
.001
0.
05
0.48
<0
.001
SNP
2.01
2.
72
0.02
3.
84
3.57
0.
04*
0.05
0.
33
<0.0
01
0.01
0.
25
<0.0
01
Pa
thol
ogy
QLD
2.
71
3.15
0.
19
3.76
3.
02
0.00
3*
0.11
0.
12
0.88
0.
06
0.11
0.
06
Tota
l 2.
03
2.78
0.
04
3.89
3.
97
0.81
0.
06
0.29
<0
.001
0.
05
0.33
<0
.001
QH
FSS
92.9
89
.8
0.54
2.
58
0.3
<0.0
01
2.28
3.
59
0.00
3 1.
96
6.26
<0
.001
* Rat
e de
crea
sed
in 2
014
† Not
e th
at Q
HFS
S is
the
refe
renc
e la
bora
tory
, so
form
s a
subs
et o
f the
test
s pe
rform
ed a
t the
prim
ary
labo
rato
ries.
The
den
omin
ator
num
ber f
or Q
HFS
S is
the
num
ber o
f tes
ts th
at w
ere
posi
tive
for a
t lea
st o
ne o
f Sal
mon
ella
, Cam
pylo
bact
er, S
hige
lla a
nd Y
ersi
nia
and
refe
rred
to Q
HFS
S by
the
prim
ary
labo
rato
ries.

241
Table 3 shows the number and percentage of results that were concordant and
discordant for CIDT and culture and were performed during 2014 at the two
laboratories that had introduced CIDT (QML and SNP). During 2014, the type of test
positive for more than half of samples that were positive for Salmonella and
Campylobacter included culture of the pathogen (81% and 56% respectively).
However, only 17% of samples positive for Shigella and 22% of samples positive for
Yersinia yielded an isolate.
Table 3: Percent and number of positive samples at laboratories that had introduced CIDT* by
concordance or discordance and test result (culture independent diagnostic tests (CIDT) and
culture-based tests), 2014
CIDT Culture Salmonella n = 3881
Campylobacter n = 6057
Shigella n = 477
Yersinia n = 588
Concordant results % (n) + + 43 (1651) 37 (2239) 10 (48) 21 (123)
Discordant results % (n)
+ - 12 (483) 36 (2176) 74 (352) 65 (379) - + 5 (193) 0 (12) 0 (0) 0 (1) + ND** 6 (239) 8 (476) 9 (42) 14 (80)
ND** + 34 (1315) 19 (1154) 7 (35) 1 (5) Total culture positive % (n) 81 (3159) 56 (3405) 17 (83) 22 (129)
* Queensland Medical Laboratory and Sullivan Nicolaides Laboratory
** ND – Not done
The median time to identification for all four pathogens at QML was three days during
the pre-CIDT period (2010 to 2012). The time to identification reduced to one day in
2014 after the introduction of CIDT. The difference between the time to identification
before introduction of CIDT and after introduction of CIDT was significant (p-value
<0.001).
Table 4 shows how test requests at QML differed by remoteness in the post CIDT
period (2014). During 2014 in all Remoteness Area categories, CIDT and culture was
the most frequently ordered test type, although the number of clinicians requesting
culture only (no CIDT) was higher in remote and regional areas of Australia than in
major cities (p-values <0.05). Conversely, clinicians in major cities were more likely to
order both CIDT and culture than those in regional or remote areas (p-values <0.05).
Table 4: Type of test requested compared by Remoteness Area, QML, 2014
Major Cities of
Australia % (n)
Regional Australia
% (n)
Remote Australia
% (n) p-value
CIDT only 12 (522) 14 (292) 15 (13) 0.14 CIDT and culture 76 (3268) 69 (1471) 65 (57) <0.001
Culture only 12 (526) 17 (359) 20 (18) <0.001

242
Table 5 shows how the type of test requested differs by the age group of the patient. In
2014 at QML, CIDT and culture was the most frequently requested test for all age
groups. The type of test requested differed significantly by age group (p-value for trend
<0.05 for all test types; Table 5). CIDT alone was less likely to be ordered for children
(0 to 17 years) than for adults (pairwise p-values <0.05), while CIDT and culture was
less likely to be ordered for patients aged over 55 than for any other group (pairwise p-
values <0.05). Similarly, culture alone was less likely to be ordered for people aged 18
to 54 years than for any other age group (pairwise p-values <0.05).
Table 5: Type of test requested compared by age group, QML, 2014
0 to 4 years
% (n) 5 to 17 years
% (n) 18 to 54 years
% (n) ≥55 years
(% n) p-value
for trend CIDT only 11 (132) 10 (70) 13 (394) 14 (233) 0.005 CIDT and culture 74 (918) 74 (505) 75 (2242) 70 (1138) <0.001 Culture only 16 (196) 16 (107) 11 (336) 16 (264) <0.001
Referral of enteric bacteria to QHFSS The total number of tests performed per month at QHFSS during the period of data
collection for the study (2010 to 2014), regardless of outcome (positive or negative for
all pathogens) or referring laboratory is shown in Figure 10. The median number of
tests performed at QHFSS before CIDT was introduced at two of the referring primary
laboratories (QML and SNP, 2010 to 2012) was 297 tests per month. The median
number of tests performed at QHFSS after CIDT was introduced at QML and SNP
(2014) was 488. This increase was significant (p-value = 0.003).

243
Figu
re 1
0: T
otal
num
ber o
f tes
ts p
erfo
rmed
at Q
ueen
slan
d H
ealth
For
ensi
c an
d Sc
ient
ific
Serv
ices
, reg
ardl
ess
of o
utco
me
and
refe
rring
labo
rato
ry, b
y ye
ar a
nd
mon
th o
f tes
t.
0
100
200
300
400
500
600
700
800
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
Jan
Mar
May
Jul
Sep
Nov
2010
2011
2012
2013
2014
Number of tests done
Year
and
mon
th o
f tes
t

244
Only QML routinely refers stool samples to QHFSS that were CIDT positive for
Salmonella and Shigella but were negative by culture, or culture was not done (Table
1). However, the data set included 440 stool samples (412 from QML and 28 from
SNP) that were CIDT positive (all four pathogens) and culture negative or not cultured
that were referred to QHFSS. After referral of these 440 stool samples to QHFSS for
reflex culture, 383 (87%) of stool samples yielded an isolate of Salmonella, Shigella or
Yersinia (Table 6). This increased the total number of samples with an isolate available
for subtyping for these three pathogens to 88%, 26% and 37% respectively. No
additional isolates of Campylobacter were cultured after referral to QHFSS despite
referral of 39 stool samples to QHFSS for further testing. All samples and isolates that
were referred to QHFSS and yielded an isolate were further typed to species, subtype
or biotype.
Table 6: Outcome of referral to QHFSS of samples positive by CIDT but with no isolate
obtained compared with the total number of samples culture positive at a primary laboratory
before referral, 2014. The final percent and total count of samples with an isolate obtained after
referral is shaded
Salmonella
% (n) Campylobacter
% (n) Shigella
% (n) Yersinia
% (n) Total culture positive at primary laboratory 81 (3159) 56 (3405) 17 (83) 22 (129)
CIDT positive, no isolate at primary laboratory 19 (720) 44 (2652) 83 (394) 78 (459)
CIDT positive (no isolate) sent to reference laboratory 7 (254) 1 (39) 11 (52) 16 (95)
Isolate obtained from CIDT positive sample at QHFSS 7 (253) 0 9 (42) 15 (88)
Total culture positive (primary and QHFSS) 88 (3412) 56 (3405) 26 (125) 37 (217)
The outcome (positive or negative) for each sample that tested positive by any method
at the initial primary laboratory (QML, SNP and Pathology QLD) or after referral testing
at the reference laboratory (QHFSS) is shown in Table 7 (Salmonella), Table 8
(Campylobacter), Table 9 (Shigella) and Table 10 (Yersinia) by year. Four different
outcomes were observed:
1. The sample was positive for the pathogen at the primary laboratory but was not
sent to QHFSS for further subtyping.
2. The sample was positive for the pathogen at both the primary laboratory and
QHFSS.
3. The sample was positive for the pathogen at the primary laboratory but was
negative at QHFSS.
4. The sample was negative for the pathogen at the primary laboratory (the
sample may have been positive for a different pathogen, or may have been

245
negative for all pathogens), but was sent to QHFSS, and was positive for the
pathogen at QHFSS.
Most samples positive for Salmonella (84%) were positive at both the primary
laboratory and QHFSS (Table 7). Prior to the introduction of CIDT, samples that were
negative were not sent to QHFSS for further attempts at obtaining an isolate
suggesting that most samples in Table 7 that were negative at the primary laboratory
for Salmonella were positive at the primary laboratory for a different pathogen. The
number of samples positive for Salmonella at the primary laboratory that were not sent
to QHFSS for subtyping increased in 2014.
Table 7: Samples positive for Salmonella by outcome at primary laboratory (Queensland
Medical Laboratory, Sullivan Nicolaides Pathology and Pathology Queensland) and reference
laboratory (Queensland Health Forensic and Scientific Services), by year
Salmonella results at laboratory % (n) Primary laboratory + - + +
QHFSS* + + - Not done
Year
2010 92.0 (2822) 0.2 (5) 0.2 (6) 7.7 (235) 2011 88.4 (2668) 0.1 (3) 0.2 (5) 11.3 (342) 2012 85.6 (2536) 0.1 (4) 0.3 (9) 14.0 (414) 2013 83.5 (2746) 0.1 (2) 0.2 (7) 16.3 (535) 2014 75.2 (3832) 0.0 (2) 0.2 (10) 24.6 (1253)
* QHFSS – Queensland Health Forensic and Scientific Services
In contrast, most samples positive for Campylobacter at the primary laboratory were
not sent to QHFSS for additional testing (96%; Table 8). During 2011 and 2012, the
number of samples referred to QHFSS increased dramatically before returning to low
levels in late 2012. This increase in isolates referred to QHFSS may have affected the
median counts and percent positivity for Campylobacter at QHFSS in Table 2.
Table 8: Samples positive for Campylobacter by outcome at primary laboratory (Queensland
Medical Laboratory, Sullivan Nicolaides Pathology and Pathology Queensland) and reference
laboratory (Queensland Health Forensic and Scientific Services), by year
Campylobacter results at laboratory % (n) Primary laboratory + - + +
QHFSS* + + - Not done
Year
2010 0.3 (16) 0.0 (0) 0.7 (38) 98.9 (5054) 2011 6.6 (381) 0.0 (0) 1.0 (59) 92.4 (5333) 2012 11.0 (516) 0.0 (0) 1.3 (61) 87.7 (4125) 2013 0.5 (19) 0.0 (0) 0.6 (22) 99.0 (3947) 2014 0.2 (11) 0.0 (0) 0.9 (67) 98.9 (7066)
* QHFSS – Queensland Health Forensic and Scientific Services

246
Although the total number of samples that tested positive for Shigella increased in
2014, most of these samples were not referred to QHFSS for further testing (53%; Table 9). Similarly, although the number of Yersinia positive samples referred to
QHFSS increased in 2014 (Table 10), there was also an increase in samples positive
for Yersinia that were not referred to QHFSS.
Table 9: Samples positive for Shigella by outcome at primary laboratory (Queensland Medical
Laboratory, Sullivan Nicolaides Pathology and Pathology Queensland) and reference laboratory
(Queensland Health Forensic and Scientific Services), by year
Shigella results at laboratory % (n) Primary laboratory + - + +
QHFSS* + + - Not done
Year
2010 93.1 (94) 0.0 (0) 1.0 (1) 5.9 (6) 2011 89.3 (50) 0.0 (0) 0.0 (0) 10.7 (6) 2012 82.1 (64) 0.0 (0) 1.3 (1) 16.7 (13) 2013 33.7 (63) 0.5 (1) 1.6 (3) 64.2 (120) 2014 29.6 (157) 0.6 (3) 1.9 (10) 68.0 (361)
* QHFSS – Queensland Health Forensic and Scientific Services
Table 10: Samples positive for Yersinia by outcome at primary laboratory (Queensland Medical
Laboratory, Sullivan Nicolaides Pathology and Pathology Queensland) and reference laboratory
(Queensland Health Forensic and Scientific Services), by year
Yersinia results at laboratory % (n) Primary laboratory + - + +
QHFSS* + + - Not done
Year
2010 88.4 (114) 2.3 (3) 2.3 (3) 7.0 (9) 2011 86.3 (44) 0.0 (0) 0.0 (0) 13.7 (7) 2012 80.3 (57) 0.0 (0) 0.0 (0) 19.7 (14) 2013 48.0 (96) 0.0 (0) 2.5 (5) 49.5 (99) 2014 38.6 (242) 0.0 (0) 1.1 (7) 60.3 (378)
* QHFSS – Queensland Health Forensic and Scientific Services
Community outbreaks of enteric bacteria During the period 2010 to 2014, 56 outbreaks caused by Salmonella, 11 outbreaks
caused by Campylobacter and one outbreak caused by Shigella were reported. Of
these outbreaks, ten (all caused by Salmonella) were assessed as unlikely, based on
the setting of the outbreak, to have been identified as outbreaks without subtyping
information. None of these outbreaks had an obvious point source, such as a
restaurant. Four outbreaks were associated with bakery chains, with cases purchasing
products from different locations. One outbreak was associated with a “meals on
wheels” provider, with clients in different locations becoming ill. One outbreak was
associated with a single catering company, but many different events were catered by

247
the company on the day in question. One outbreak was associated with bore water and
the other three outbreaks did not have a clearly defined source. The cases in all of
these outbreaks were identified as connected due to multiple locus variable number
tandem repeat analysis (MLVA) of the Salmonella isolates from the cases, and in some
outbreaks the source. Three of these outbreaks occurred in 2014, after CIDT had been
introduced at QML and SNP. However, during this time, concurrent culture had
continued for Salmonella, making an isolate available for subtyping. All three outbreaks
in 2014 were associated with bakery franchises.
Discussion The introduction of CIDT into the primary laboratories in QLD has increased the
apparent incidence of the enteric pathogens in this study, in particular Shigella and
Yersinia. During the period of data collection for this study (2010 to 2014), only QML
and SNP had introduced CIDT for enteric pathogens, both in 2013 (August and
November respectively). Prior to the introduction of CIDT, identification of enteric
bacterial pathogens occurred through the use of culture to obtain an isolate. After CIDT
was introduced, identification of enteric bacterial pathogens occured one of three ways:
culture (as for before introduction of CIDT), CIDT, or culture and CIDT together. All
laboratories attempt to obtain an isolate through concurrent or reflexive culture.
However, even with continued culture of samples, during 2014, 38% of all samples
positive for one of the four pathogens did not yield an isolate. Of samples positive by
CIDT (either alone or with a positive culture), 50% of samples did not yield an isolate.
This included 29% of samples positive for Salmonella, 54% of samples positive for
Campylobacter, 87% of samples positive for Shigella and 76% of samples positive for
Yersinia. This is similar to a FoodNet study in the US which examined testing for
Salmonella, Campylobacter, Shigella and Yersinia, in addition to Shiga-toxin producing
E. coli and Vibrio, found that 46% of positive samples did not have an associated
isolate (8). With the CIDT methods currently in use, these samples were unable to be
further characterised to subtype, biotype and in some cases even species. Without this
information, defining epidemiologically linked samples is difficult, with negative
implications for public health surveillance.
There was a significant increase in the median number of tests requested per month
for enteric pathogens at all laboratories when 2014 (post CIDT) was compared with the
pre-CIDT period, 2010 to 2012. This may have been due to a change in clinician
behaviour, where clinicians may be more likely to request testing for bacterial causes of
gastroenteritis in 2014 due to a perceived decrease in time to receipt of test results (1).
However, the number of tests performed increased regardless of whether the
laboratory had introduced CIDT during the study period, suggesting a true increase in

248
the incidence of gastroenteritis in QLD. Similarly, the median number of tests per
month positive for each of the pathogens in this study (Salmonella, Campylobacter,
Shigella and Yersinia) increased over the same time period.
The increase in the detection of Salmonella is likely to be due to a true increase in the
incidence of disease as the median number of tests positive for Salmonella increased
for all laboratories, regardless of the introduction of CIDT. Indeed, while the percent
positivity increased slightly, the total number of samples that tested positive for
Salmonella increased dramatically from the summer of 2013/2014. This is consistent
with the increase in cases of Salmonella in other Australian jurisdictions in 2014,
including New South Wales (10) and South Australia (11). Indeed, the incidence of
Salmonella in Australia has been increasing since 2000 (12). The higher percent
positivity reported by Pathology QLD, when compared with the private pathology
laboratories, is likely to be due to the role of Pathology QLD in testing samples taken
from people admitted to hospital. These people have a more serious illness than those
in the community, and are therefore more likely to have a serious gastroenteritis illness
such as Salmonella rather than a milder illness like those caused by a bacterial toxin.
The incidence of Campylobacter in Australia decreased nationwide during 2012. This
decrease has been attributed by OzFoodNet epidemiologists to the introduction of the
Primary Production and Processing Standard for Poultry Meat (Standard 4.2.2) in 2012
(13). However, both the median number of tests positive per month and the percent
positivity for Campylobacter increased significantly at both QML and SNP after the
introduction of CIDT. In contrast, the median number of tests positive per month and
the percent positivity for Campylobacter decreased at Pathology QLD suggesting that
the apparent increase in cases of Campylobacter is due to the increased sensitivity of
detection of Campylobacter infection by PCR. Campylobacter is difficult to culture as it
requires specific environmental conditions (microaerophilic) and fresh stool samples in
order to grow (3). As a result, many cases of Campylobacter remain undiagnosed
when only culture is used for testing. This difficulty obtaining a culture is reflected in
testing at the reference laboratory, where no samples that were CIDT positive for
Campylobacter and were referred to QHFSS for further testing yielded an isolate at
QHFSS.
The median number of tests positive per month and the percent positivity for Shigella
increased dramatically after the introduction of CIDT at QML and SNP. In contrast, the
median number of tests positive and the percent positivity remained constant at
Pathology QLD during 2014. Current PCR methods for testing for the presence of
Shigella are unable to distinguish between Shigella and enteroinvasive Escherichia coli
(EIEC) as Shigella and EIEC are genetically closely related species within the same

249
genus (E. coli) (14, 15). However, EIEC causes a milder illness than Shigella (16) and
is not notifiable in Australia. Some of this increase in the median number of tests
positive for Shigella may be due to cases of EIEC being detected by the Shigella PCR,
although since Shigella can be difficult to culture (4), the possibility that the CIDT
positive samples are true cases of Shigella can’t be discounted. The case definition for
Shigella in QLD requires isolation of the pathogen, so only those samples with an
associated isolate are notified to the National Notifiable Diseases Surveillance System
(17). Nevertheless, although these possibly false positive samples will become de-
notified when an isolate is unable to be obtained, they have already resulted in an
increase in workload at both primary and reference laboratories.
SNP only tests for Yersinia if requested. However, as Yersinia is included in the
multiplex PCR test used at SNP, Yersinia is detected by this method even when it is
not specifically requested. This may explain some of the increase in the median
number of tests positive for Yersinia after introduction of CIDT. In contrast, although
QML and Pathology QLD routinely culture for Yersinia, the number of tests positive for
Yersinia at QML and Pathology QLD has also increased despite Pathology QLD not
introducing CIDT during the study period. The increase in the number of tests positive
for Yersinia at Pathology QLD was small (from a median of two positive samples per
month to three positive samples per month). It is likely that the increase in tests positive
for Yersinia during 2014 is a combination of a real but small increase in cases and an
artefact of the change in the sensitivity of the laboratory testing method.
Clinicians in remote and regional areas of QLD were less likely to request both CIDT
and culture than their major city counterparts during 2014. The QML information for
clinicians recommends requesting both PCR and culture (18), suggesting that outside
of the major cities this recommendation is not followed as well as in the cities. The
postcode used for analysis in this study was that of the patient not the clinician.
However, people are unlikely to travel far for an ailment such as gastroenteritis (19), so
using patient postcodes should be an appropriate substitute for clinician locations.
Clinicians for patients in all age groups ordered both CIDT and culture more frequently
than CIDT or culture alone. However, clinicians were less likely to order CIDT and
culture for patients over 55 years of age, so focusing awareness on clinicians who treat
this age group should improve this.
Obtaining an isolate to enable subtyping of the pathogen is important for public health
surveillance (5-7). Due to the increased sensitivity of PCR testing (1), it is inevitable
that some samples will be positive by CIDT only, especially for those pathogens that
are difficult to culture, like Campylobacter and Shigella. By sending these samples to
the reference laboratory (QHFSS), the probability of obtaining an isolate for subtyping

250
is improved. With the exception of CIDT positive samples referred to QHFSS for culture
of Campylobacter, referral of stool samples to QHFSS that were culture negative at the
primary laboratory increased the number of samples with an isolate available for
subtyping. Despite the resulting increase in workload at QHFSS, this practice should
continue until culture independent subtyping is available so that outbreak detection and
public health surveillance can continue.
Outbreak detection and case finding for diseases with a high level of baseline activity
occurs through epidemiological linking of cases (e.g. the cases attended the same
event or restaurant). When an epidemiological link isn’t obvious, cases can be linked if
the isolates have the same subtype. Not having subtyping information will impact
outbreak detection (5, 6). Ten outbreaks during the study period, three of which were in
2014, after CIDT was introduced at QML and SNP, may not have been identified as
outbreaks without the subtyping information that demonstrated a link between the
cases, showing the importance of continued culture and subtyping of samples from
cases of bacterial gastroenteritis.
A limitation of this study is that only one year of data was available after the
introduction of CIDT at QML and SNP. Comparison of multiple years of data would
ensure the incidence of the pathogens in 2014 was not an anomaly. In addition, only
QLD data was compared, and only for four enteric pathogens. This study should be
extended in the future to other jurisdictions across Australia, and for other pathogens.
However, the results of this study can be used by laboratories and public health units in
QLD to inform the way forward for diagnosis, referral and subtyping of enteric
pathogens.
This study provided an overview of the current testing procedures for Salmonella,
Campylobacter, Shigella and Yersinia at all QLD laboratories and examined the
incidence of the four pathogens. While the number of tests positive for all four
pathogens has increased over the period of the study, only Salmonella has increased
in incidence. The increase in the number of tests positive for Campylobacter, Shigella
and Yersinia is likely to be predominantly due to the change in testing resulting in an
increase in the sensitivity of the tests and subsequently the ability to detect these three
pathogens. However, the possibility of an increase in incidence cannot be discounted
for these pathogens. The increase in the sensitivity of case detection by CIDT must be
accounted for when assessing trends and the burden of disease, especially for
Campylobacter, Shigella and Yersinia. Continuing attempts to obtain an isolate, either
through concurrent culture or reflexive culture of samples positive by CIDT, is
recommended in order to obtain the isolates required for typing as typing information is
necessary for outbreak detection and public health surveillance.

251
References 1. Langley G, Besser J, Iwamoto M, Lessa FC, Cronquist A, Skoff TH, et al. Effect of Culture-Independent Diagnostic Tests on Future Emerging Infections Program Surveillance. Emerging Infectious Diseases. 2015;21(9):1582. 2. Queensland Health. Gastroenteritis. 2014 [updated 2014; cited 13 November 2015]; Available from: http://conditions.health.qld.gov.au/HealthCondition/condition/14/33/60/Gastroenteritis. 3. Bessede E, Delcamp A, Sifre E, Buissonniere A, Megraud F. New methods for detection of campylobacters in stool samples in comparison to culture. Journal of clinical microbiology. 2011 Mar;49(3):941-4. 4. Dutta S, Chatterjee A, Dutta P, Rajendran K, Roy S, Pramanik KC, et al. Sensitivity and performance characteristics of a direct PCR with stool samples in comparison to conventional techniques for diagnosis of Shigella and enteroinvasive Escherichia coli infection in children with acute diarrhoea in Calcutta, India. Journal of Medical Microbiology. 2001 Aug;50(8):667-74. 5. Atkinson R, Maguire H, Gerner-Smidt P. A challenge and an opportunity to improve patient management and public health surveillance for food-borne infections through culture-independent diagnostics. Journal of Clinical Microbiology. 2013 Aug;51(8):2479-82. 6. Cronquist AB, Mody RK, Atkinson R, Besser J, Tobin D'Angelo M, Hurd S, et al. Impacts of culture-independent diagnostic practices on public health surveillance for bacterial enteric pathogens. Clinical Infectious Diseases. 2012 Jun;54 Suppl 5:S432-9. 7. Jones TF, Gerner-Smidt P. Nonculture diagnostic tests for enteric diseases. Emerging Infectious Diseases. 2012 Mar;18(3):513-4. 8. Iwamoto M, Huang JY, Cronquist AB, Medus C, Hurd S, Zansky S, et al. Bacterial Enteric Infections Detected by Culture-Independent Diagnostic Tests - FoodNet, United States, 2012-2014. MMWR Morbidity and Mortality Weekly Report. 2015 Mar 13;64(9):252-7. 9. OzFoodNet Queensland. OzFoodNet - Enhancing Foodborne Disease Surveillance Across Australia, Annual Report 2010, Queensland. 2010. 10. Ward K, Franklin N, Furlong C, Hope K, Flint J. OzFoodNet New South Wales annual report 2014. In: Communicable Diseases Branch HPN, editor.; 2014. 11. Miller M, Halliday J, Denehy E, Koehler A. OzFoodNet South Australia Annual Report 2014. In: Communicable Disease Control Branch SH, editor.; 2014. 12. Kirk M, Ford L, Glass K, Hall G. Foodborne illness, Australia, circa 2000 and circa 2010. Emerging Infectious Diseases. 2014 Nov;20(11):1857-64. 13. Food Standards Australia New Zealand. Poultry Standards. [cited 17 November 2015]; Available from: http://www.foodstandards.gov.au/code/primaryproduction/poultry/pages/default.aspx 14. Sahl JW, Morris CR, Emberger J, Fraser CM, Ochieng JB, Juma J, et al. Defining the phylogenomics of Shigella species: a pathway to diagnostics. Journal of Clinical Microbiology. 2015 Mar;53(3):951-60. 15. Lan R, Reeves PR. Escherichia coli in disguise: molecular origins of Shigella. Microbes Infect. 2002 Sep;4(11):1125-32. 16. Food and Drug Administration. Enteroinvasive Escherichia coli (EIEC). Bad Bug Book, Foodborne Pathogenic Microorganisms and Natural Toxins; 2012. p. 80-1. 17. Queensland Health. Shigella infection (Shigellosis) - Queensland Health Guidelines for Public Health Units. 2010.

252
18. Queensland Medical Laboratory. Faecal Multiplex PCR testing. 2013 [updated 2013; cited 17 November 2015]; Available from: http://www.qml.com.au/Portals/0/PDF/FaecalMultiplexPCR_1177.pdf. 19. Ward B, Humphreys J, McGrail M, Wakerman J, Chisholm M. Which dimensions of access are most important when rural residents decide to visit a general practitioner for non-emergency care? Aust Health Rev. 2015 Apr;39(2):121-6.

253
Appe
ndix
1: L
abor
ator
y pr
oces
s qu
estio
nnai
re
Sa
lmon
ella
C
ampy
loba
cter
Sh
igel
la
Yers
inia
1
a D
o yo
u te
st s
tool
/blo
od s
peci
men
s fo
r eac
h of
thes
e pa
thog
ens
in y
our l
abor
ator
y? Y
es/N
o
b If
no, d
o yo
u se
nd th
e sp
ecim
en fo
r tes
ting
for e
ach
of
thes
e pa
thog
ens
to a
noth
er la
bora
tory
? Ye
s/N
o
c If
yes
to 1
b, w
hich
labo
rato
ry d
o yo
u se
nd th
e sp
ecim
ens
to?
(ski
p to
que
stio
n 6a
)
2 D
o yo
u ro
utin
ely
use
cultu
re to
iden
tify
each
of t
hese
pa
thog
ens?
Yes
/No/
only
if re
ques
ted
3
a D
o yo
u ro
utin
ely
use
a cu
lture
inde
pend
ent t
est (
CID
T) to
id
entif
y ea
ch o
f the
se p
atho
gens
? Ye
s/N
o/on
ly if
re
ques
ted
b If
yes
to 3
a, w
hat t
ype
of C
IDT
do y
ou u
se?
e.g.
PC
R,
rapi
d di
agno
stic
test
c
If ye
s to
3a,
wha
t bra
nd o
f CID
T do
you
use
?
4
a D
o yo
u us
e bo
th c
ultu
re a
nd C
IDT
for e
ach
of th
ese
path
ogen
s?
b If
yes
to 4
a, d
o yo
u do
bot
h co
ncur
rent
ly b
efor
e yo
u kn
ow
the
resu
lt ("
conc
urre
nt")
or d
o yo
u on
ly c
ultu
re s
ampl
es
that
wer
e po
sitiv
e by
CID
T ("r
efle
xive
") o
r do
you
have
a
diffe
rent
rout
ine
("ot
her"
)?
c Pl
ease
des
crib
e yo
ur "o
ther
" rou
tine
5 W
hat d
o yo
u do
with
spe
cim
ens
that
are
pos
itive
by
CID
T bu
t neg
ativ
e by
cul
ture
?

254
6
a D
o yo
u re
fer c
ultu
re p
ositi
ve is
olat
es to
a re
fere
nce
labo
rato
ry fo
r fur
ther
typi
ng?
b If
cultu
re w
as n
egat
ive
or y
ou u
se C
IDT
only
, do
you
refe
r st
ool/b
lood
spe
cim
ens
that
are
CID
T po
sitiv
e to
a
refe
renc
e la
bora
tory
for f
urth
er ty
ping
?
7 If
you
use
CID
T, w
hen
did
your
labo
rato
ry in
trodu
ce th
ese
met
hods
for e
ach
path
ogen
?
8 a
Wha
t is
the
nam
e of
you
r pat
holo
gy la
bora
tory
?
b W
hat s
tate
are
you
loca
ted
in?

255
Appendix 2: Data dictionary for analysis* Field Stata variable name Description Example input Specimen ID labnumber Unique ID Text Laboratory lab Name of the
laboratory doing the testing
QML, SNP, Pathology QLD, QHFSS
Age group age_grp Age group of patient
0-4 years 5-17 years 18-54 years ≥55 years
Sex† gender Gender of patient 1 = Female 0 = Male 3 = Other 9 = Unknown
Postcode postcode Residential postcode of patient
Queensland postcodes only
Remoteness area
ra What was the remoteness area classification of the patient?
Text
Year year Year of testing dd/mm/yyyy Month month Month and year of
test request YYYYmmm
Date of receipt receipt_date Date the request was received
Date
Test/s requested†
test_request What tests were requested?
Culture, PCR or both
Date of identification result†
id_date Date the result was disseminated
Date
Pathogen identified - Salmonella
salmonella Was Salmonella identified in the sample?
Yes = 1 No = 0 Unknown = .
Pathogen identified - Campylobacter
campylobacter Was Campylobacter identified in the sample?
Yes = 1 No = 0 Unknown = .
Pathogen identified - Shigella
shigella Was Shigella identified in the sample?
Yes = 1 No = 0 Unknown = .
Pathogen identified - Yersinia
yersinia Was Yersinia identified in the sample?
Yes = 1 No = 0 Unknown = .
Culture culture Was the culture positive? Negative? Not done? If not done, skip the pathogen specific culture questions
Positive = 1 Negative = 0 Test not performed = .

256
Salmonella culture
salmonella_culture Was Salmonella detected by culture?
Yes = 1 No = 0 Unknown = .
Campylobacter culture
campylobacter_culture Was Campylobacter detected by culture?
Yes = 1 No = 0 Unknown = .
Shigella culture shigella_culture Was Shigella detected by culture?
Yes = 1 No = 0 Unknown = .
Yersinia culture yersinia_culture Was Yersinia detected by culture?
Yes = 1 No = 0 Unknown = .
PCR pcr Was PCR positive? Negative? Not done? If not done, skip the pathogen specific PCR questions
Positive = 1 Negative = 0 Test not performed = .
Salmonella PCR salmonella_pcr Was Salmonella detected by PCR (positive), not detected (negative) or was PCR not done
Positive = 1 Negative = 0 Test not performed = .
Campylobacter PCR
campylobacter_pcr Was Campylobacter detected by PCR (positive), not detected (negative) or was PCR not done
Positive = 1 Negative = 0 Test not performed = .
Shigella PCR shigella_pcr Was Shigella detected by PCR (positive), not detected (negative) or was PCR not done
Positive = 1 Negative = 0 Test not performed = .
Yersinia PCR yersinia_pcr Was Yersinia detected by PCR (positive), not detected (negative) or was PCR not done
Positive = 1 Negative = 0 Test not performed = .
Time to ID† time_to_id Time between receipt of the sample and identification of pathogen
Number of days
Sent to QHFSS?†
qhfss Was the sample sent to QHFSS for further investigation, as indicated by the primary lab?
Yes = 1 No = 0 Unknown = .

257
QHFSS request date
qhfss_request Date the request received by QHFSS
dd/mm/yyyy
QHFSS receipt date
qhfss_receipt Date the sample was received by QHFSS
dd/mm/yyyy
Pathogen identified by QHFSS - Salmonella
qhfss_salmonella Was Salmonella identified in the sample provided to QHFSS?
Yes = 1 No = 0 Unknown = .
Pathogen identified by QHFSS - Campylobacter
qhfss_campylobacter Was Campylobacter identified in the sample provided to QHFSS?
Yes = 1 No = 0 Unknown = .
Pathogen identified by QHFSS - Shigella
qhfss_shigella Was Shigella identified in the sample provided to QHFSS?
Yes = 1 No = 0 Unknown = .
Pathogen identified by QHFSS - Yersinia
qhfss_yersinia Was Yersinia identified in the sample provided to QHFSS?
Yes = 1 No = 0 Unknown = .
Culture - QHFSS
qhfss_culture Was the culture positive when tested by QHFSS? Negative? Not done? If not done, skip the pathogen specific culture questions
Positive = 1 Negative = 0 Test not performed = .
Salmonella culture - QHFSS
qhfss_salmonella_culture Was Salmonella detected by culture at QHFSS?
Yes = 1 No = 0 Unknown = .
Campylobacter culture - QHFSS
qhfss_campylobacter_culture Was Campylobacter detected by culture at QHFSS?
Yes = 1 No = 0 Unknown = .
Shigella culture - QHFSS
qhfss_shigella_culture Was Shigella detected by culture at QHFSS?
Yes = 1 No = 0 Unknown = .
Yersinia culture - QHFSS
qhfss_yersinia_culture Was Yersinia detected by culture at QHFSS?
Yes = 1 No = 0 Unknown = .
Subtyping done? subtyping Was subtyping done on the sample
Yes = 1 No = 0 Unknown = .
MLVA done? mlva Was MLVA done? Yes = 1 No = 0 Unknown = .
MLVA result mlva_result What was MLVA of the sample?
An MLVA number

258
Biotyping done? biotype Was biotyping done?
Yes = 1 No = 0 Unknown = .
Other subtyping subtype Was another subtyping method done
Yes = 1 No = 0 Unknown = .
Salmonella species
salmonella_species What species of Salmonella was identified?
Text
Second Salmonella species
salmonella_species2 What was the second Salmonella species identified, if applicable?
Text
Salmonella subtype
salmonella_subtype What subtype of Salmonella was identified?
Text
Campylobacter species
campylobacter_species What species of Campylobacter was identified?
Text
Shigella species shigella_species What species of Shigella was identified?
Text
Shigella subtype shigella_subtype What subtype of Shigella was identified?
Text
Shigella biotype shigella_biotype What biotype of Shigella was identified?
Text
Yersinia species yersinia_species What species of Yersinia was identified?
Text
Yersinia subtype yersinia_subtype What subtype of Yersinia was identified?
Text
Yersinia biotype yersinia_biotype What biotype of Yersinia was identified?
Text
* Unshaded fields were provided by QML, SNP and Pathology QLD. Shaded fields were provided by QHFSS. ID – identification; QML – Queensland Medical Laboratory; SNP – Sullivan Nicolaides Pathology; QLD – Queensland; QHFSS – Queensland Health Forensic and Scientific Services; PCR – polymerase chain reaction; CIDT – culture independent diagnostic testing; MLVA – multiple locus variable number tandem repeat analysis † not all laboratories provided this information

259
Chapter 5 Cluster of cases with Ralstonia species bacteraemia potentially associated with
propofol administration

260
Table of contents Prologue ................................................................................................................ 262
My role ............................................................................................................... 262
Lessons learned ................................................................................................ 263
Public health implications of this work ................................................................ 264
Acknowledgements ............................................................................................ 264
Master of Philosophy (Applied Epidemiology) core activity requirement ............. 265
Abstract ................................................................................................................. 265
Introduction ........................................................................................................... 266
Objectives ............................................................................................................. 268
Methods ................................................................................................................ 268
Epidemiological investigations ........................................................................... 268
Case definition ............................................................................................... 268
Case series .................................................................................................... 268
Microbiology ................................................................................................... 269
Simulated case-control and case-cohort studies............................................. 270
Bradford-Hill Framework ................................................................................. 270
Distribution chain of propofol .......................................................................... 271
Environmental investigation ............................................................................... 271
Testing of propofol ............................................................................................. 272
Delphi Method .................................................................................................... 273
Results .................................................................................................................. 273
Timeline of investigation..................................................................................... 273
Case series ........................................................................................................ 275
Environmental testing ........................................................................................ 284
Testing of propofol ............................................................................................. 284
Simulated epidemiological studies ..................................................................... 285
Distribution chain of propofol .............................................................................. 288
Assessment of causation using Bradford-Hill framework .................................... 289

261
Delphi Method ................................................................................................... 293
Discussion ............................................................................................................. 300
References ............................................................................................................ 304
Appendix 1: Targeted literature search and synthesis ........................................... 309
Appendix 2: Case report form ................................................................................ 312
Appendix 3: ProMED post requesting information about contamination of propofol317
Appendix 4: TGA testing ....................................................................................... 318

262
Prologue Study rationale On 1 May 2014, South Australia (SA) Health notified the Therapeutic Goods
Administration (TGA) of the isolation of Ralstonia species from blood cultures of
three bacteraemic patients in two different hospitals in Adelaide. Ralstonia is not a
common isolate in blood samples in pathology laboratories in SA, raising suspicion
of a possible outbreak of Ralstonia in South Australia. A preliminary investigation
by SA Health reported that the only exposure common to all three patients was
administration of a single brand of propofol, a widely used short acting anaesthetic
agent, regulated by TGA. The TGA quarantined the implicated batches of propofol
across Australia, and initiated an investigation into the source of infection. The
investigation was necessary to determine whether the quarantined propofol should
be recalled and disposed of, or released back into use.
My role Associate Professor Mahomed Patel provided supervision, and along with Anna-Lena
Arnold and I, we formed the “MAE Team” for investigation of this unusual cluster of
cases. We relocated to an office in the TGA for the initial part of the investigation,
assisting them directly with the epidemiological investigations. Later in the
investigation, we returned to our field placements, and assisted the Communicable
Diseases Network Australia working group (CDNA-WG) convened in response to this
cluster of cases. We also acted as facilitators of the Delphi process in the later stages
of the investigation.
As part of the MAE investigation team, I was involved in all discussions and planning of
the investigation, providing intellectual input at all stages of the investigation. I assisted
with collating case information into line lists and performing descriptive analyses. I also
conducted the simulations of analytical studies, and contributed to the assessment of
the Bradford-Hill framework along with the MAE team. My background in microbial
phylogenetics provided me with a comprehensive understanding of the genetic analysis
of the isolates, which allowed me to explain this aspect of the investigation to members
of the investigation team who had no previous experience with genetic analysis. I also,
along with Mahomed and Anna-Lena, drafted and critically reviewed documents
including multi-jurisdictional outbreak investigation reports, documents for the Delphi
rounds, literature reviews, as well as preparing the final reports to the CDNA and the
Australian Health Protection Principal Committee (AHPPC).

263
Lessons learned As this was my first ever outbreak investigation, I learned a lot of new things, even
though it didn’t end up being a “traditional” outbreak; this was more an investigation of
a cluster of cases of an uncommon disease that might have a common source. The
main thing I learned was the difficulty in engaging and encouraging cooperation when
many people with different agendas were involved. In hindsight, this investigation
should have been managed in a similar way to multijurisdictional outbreaks run by
OzFoodNet. OzFoodNet multijurisdictional outbreaks are run according to a standard
protocol, resulting in everyone knowing their role in the investigation. A similar
document for non-foodborne outbreaks would be useful for future outbreaks of this
type. Good communication and knowing roles is an important component of a
successful outbreak investigation.
The most valuable things I learned were all related to how to think like an
epidemiologist, rather than a microbiologist, although I think keeping the microbiology
in mind is also very important. Learning how to think like an epidemiologist from
Mahomed was an invaluable experience. We learned about the Bradford-Hill
framework in class, but applying the criteria in a practical situation was completely
different!
Interestingly, both this outbreak investigation, and the investigation of hepatitis A in the
next chapter reinforced to me the importance of not going into an outbreak
investigation with a preconceived idea of what the exposure was. In this investigation,
propofol was mentioned from the outset, and this may have led those involved in the
investigation to ignore evidence that might have implicated a different exposure. In
addition, the ignoring of non-bacteraemic cases of Ralstonia in Queensland (QLD),
despite these cases also being unexpected, caused the critical link between these
cases and some of the bacteraemic Ralstonia cases in QLD to be missed by the
CDNA-WG.
I really enjoyed learning how to simulate analytical studies in the absence of real data,
and getting to play with some basic commands in Stata and EpiInfo. But the most
interesting new method learned in this cluster investigation was the Delphi Method.
Using expert opinions rather than hard facts is very different to my experience during
life as a laboratory scientist. However, this technique is not without its pitfalls. If you
don’t ask a precise question, you won’t get a precise answer. On the other hand, no
matter how direct the question, there will always be someone who goes their own way

264
– in this case, we asked people to respond to scenarios with defined responses. One
person made up their own response, making it very difficult to combine responses. I
like a quote from the original paper discussing the Delphi Method,
“vague questions inviting general critical comment … produce literary
outpourings of little value for the analysis” (1).
Public health implications of this work This investigation showed the importance of looking for and sharing observations about
bacteraemia of uncommon causes, such as Ralstonia, in vulnerable populations such
as immunocompromised patients in hospitals. This investigation was unable to resolve
the source of the cases of Ralstonia in this cluster. However, during the course of the
investigation, we found that there was a perception among health care workers that the
outer surface of rubber stoppers of single use vials are sterile, protected from
contamination by the plastic lid. This investigation showed that the outer surface of
rubber stoppers are not sterile, and should always be swabbed with a suitable
disinfectant and allowed to dry before inserting the needle to withdraw the vial contents
for injection.
During the course of the investigation, a separate investigation of the cases in QLD
found an alternative source of infection. This investigation found that many of the cases
in QLD, including some additional non-bacteraemic cases, were associated with bottled
water used in a hospital. Although we were not directly involved in this investigation,
the QLD representatives on the CDNA-WG shared some aspects of the investigation
with the group. A memorandum was supplied to the Chief Executives of Health and
Hospital Services to remind clinicians that bottled water should not be considered
sterile, and as such is not suitable for severely immunocompromised patients.
Acknowledgements I would first like to acknowledge the invaluable help and supervision by Associate
Professor Mahomed Patel, and Anna-Lena Arnold, my MAE partner in crime during this
cluster investigation. I would also like to thank all those at the TGA who made us feel
very welcome during our time there, in particular Dr Bronwen Harvey, Karen Longstaff
and Dr Claire Behm. I also thank Dr Hanna Sidjabat and the team at the University of
Queensland Centre for Clinical Research (UQCCR) for DiversiLabTM analysis, and
Associate Professor Scott Beatson, Dr Nouri Ben Zakour and Mitchell Stanton-Cook at
University of Queensland School of Chemistry and Molecular Biology (UQ SCMB) for
whole genome sequencing (WGS) analysis.

265
Master of Philosophy (Applied Epidemiology) core activity requirement Investigate an acute public health problem or threat (typically a disease outbreak).
Literature review that demonstrates skills in conducting a targeted literature search and
synthesis (Appendix 1).
Abstract South Australia notified the TGA of an unusual cluster of three Ralstonia bacteraemia
cases potentially associated with propofol on 1 May 2014. Subsequently, QLD (four
cases) and Victoria (VIC, one case) also notified cases of Ralstonia bacteraemia and a
CDNA working group was convened to assist with the investigation.
Batches of the implicated propofol product were tested for microbial contamination of
both the vial contents and the outer surfaces of the vial closures (plastic flip off lid and
rubber stoppers) by the TGA, SA Pathology, the product manufacturer and two
independent laboratories. Isolates of Ralstonia from bacteraemia cases and an isolate
from a pooled sample of five vial lids and rubber stoppers from a single batch of
propofol were genotyped by DiversiLabTM rep-PCR and whole genome sequencing.
The epidemiological investigation included a case series, describing the cluster by
time, person, place and risk factors. The level of exposure to propofol required for a
significant measure of association was calculated through simulated case control and
case cohort studies. As it was deemed that an analytical study was unlikely to achieve
significance of association, causation was assessed using a combination of Bradford-
Hill criteria and consultation with an expert panel using the Delphi Method.
Eight cases of Ralstonia bacteraemia were identified nationally with onsets between 1
April 2014 and 4 May 2014. All cases were administered the same brand of propofol
prior to onset of bacteraemia suggesting that the measure of association would be
infinitely high. Application of the Bradford-Hill criteria and expert discussion via the
Delphi Method was unable confirm a single common source for all cases. Identification
of microbial contamination on the outer surface of the rubber stoppers of vials, in
combination with findings from the literature showed biological plausibility for
contamination of the outer surface of the rubber stoppers. The participants in the
Delphi panel agreed that, if the propofol was contaminated with Ralstonia, it was
contaminated on the outside of the vial rather than in the solution. Independent
investigations by QLD Health found cases of non-bacteraemic Ralstonia infection at the
same hospital in QLD, QLD3, where two cases of Ralstonia bacteraemia were

266
reported. An epidemiological investigation by QLD Health found an association
between all cases at this hospital and bottled drinking water, excluding these cases
from the propofol associated investigation.
At least two distinct sources of infection, bottled water and a second source that may
have been propofol, were identified during this investigation. However, it is unclear how
many cases were simply background cases. In the absence of a clear epidemiological
or microbiological link between illness and infection, using the Delphi method and a
group of experts can help to clarify some of the issues, but consensus may be difficult
to attain if the information provided to the group is not sufficiently comprehensive.
Introduction A staff member of South Australia (SA) Health identified three cases of bacteraemia
caused by Ralstonia species, within a single week in late April 2014, in patients at two
different hospitals in SA, and initiated further investigation. Initial investigations
reported that the only common exposure between all three cases was administration of
the same brand of the anaesthetic, propofol. SA Health notified the Therapeutic Goods
Administration (TGA) on 1 May 2014, prompting nationwide case finding and
investigation. These investigations aimed to determine if there were additional cases
elsewhere in Australia (as would be expected given the national distribution of the
propofol product), if the propofol product was the common source, and how it became
contaminated.
Outbreak investigations can make use of many different techniques in order to find an
answer and resolve the outbreak. In addition to classical analytical study methods, the
Delphi Method can be employed to assist with obtaining an answer to outbreak or
cluster investigations that can’t be resolved using traditional methods. The Delphi
Method was first designed and used to obtain expert opinion to inform strategies to
optimise the United States industrial target system and to estimate required numbers of
Atomic-bombs during the Cold War (1). The method makes use of a series of
questionnaires in an effort to achieve a consensus of opinion. During the question
rounds, additional information is supplied to participants as needed or requested,
allowing participants to change or enhance their responses. This method allows
participants to answer anonymously, removing the tendency for “group-think” and the
domination of opinions by stronger personalities inevitable in any group situation (1, 2).
Ralstonia pickettii is the type species of a genus of Gram negative bacteria first
proposed as a new species in 1995. Prior to this, species of Ralstonia were

267
taxonomically grouped in a number of genera, including Burkholderia, and
Pseudomonas (3). Three species, R. pickettii, R. mannitolilytica and R. insidiosa have
been implicated in human disease (4-30). R. mannitolilytica was first proposed as a
species distinct from R. pickettii in 2001 (31), and R. insidiosa was first identified in
2003 (25).
Ralstonia species are commonly found in the environment, especially associated with
water, including ultrapure water (32, 33) and in the water system of the Space Shuttle
Discovery (34). Ralstonia species are also able to survive in disinfectants (35-37). In
the clinical setting, Ralstonia species are not considered virulent but are commonly
found colonising cystic fibrosis patients and on occasion can cause pneumonia in these
patients (38-41). They have also been implicated in a large number of nosocomial
outbreaks worldwide due to contaminated medical devices (4, 10, 13, 26, 28), solutions
contaminated during manufacture (6, 9, 14, 18, 22) or through cross-contamination of
solutions in hospitals (7, 11, 15, 16, 19).
Propofol is a short acting anaesthetic agent, commonly used in hospitals and clinical
settings. It is a lipid and soybean based emulsion, and is a rich environment for the
growth of microorganisms (42-46). Since release in 1987, several outbreaks worldwide
have been attributed to contamination of propofol, although all have been as a result of
contamination through use, rather than contamination during manufacture (47-60).
There have been two outbreaks that the investigators considered may have been due
to a failure to disinfect the rubber stoppers (48, 53). None have been previously
reported in Australia.
The implicated brand of propofol is provided in a glass vial with a rubber stopper, metal
crimp and plastic flip off lid. The vial contents are sterilised after the vials are filled and
sealed. The flip off lid is not intended to protect the outer surface of the rubber stopper
from contamination. Experimental evidence shows that intentional contamination of the
outer surface of vials similar to propofol vials can result in contamination of the internal
surface of the plastic lid, and the upper surface of the rubber stopper (61, 62).
Contamination of the rubber stopper without disinfection before use can result in
contaminated needles or solutions (63, 64). Disinfection of the rubber stopper with an
alcohol swab or spray (considered standard infection control practice (65)) can reduce
onward transfer of contamination from the stopper to patients (62, 63).

268
Objectives The objective of this investigation was to determine if the cases of Ralstonia
bacteraemia reported in April and May 2014 were associated with a common exposure,
and if this common exposure was propofol. Case-finding for unidentified cases of
Ralstonia bacteraemia was also undertaken.
Methods
Epidemiological investigations Case definition A meeting of the Australian Health Protection Principal Committee (AHPPC) on 9 May
2014 selected the case definition for the study: “all cases of bacteraemia with blood
cultures positive for Ralstonia spp. and date of detection of infection since 1 January
2014”.
Case series Information about cases of Ralstonia bacteraemia from all jurisdictions were reported
via CDNA representatives to the TGA and CDNA-WG. The MAE team adapted a
questionnaire originally designed by QLD Health to collect additional information on
reported cases from hospital or public health staff, and included questions on
demographics, hospital and clinical details, laboratory testing details, medications
administered (including detailed information about propofol use) and clinical
procedures performed. The form used is included in Appendix 2. This information was
collated into a line list using Microsoft Excel.
As cases of Ralstonia are not notifiable to the National Notifiable Diseases Surveillance
System (NNDSS), background rates of isolation of Ralstonia species from laboratories
nation-wide were obtained through consultation with the Public Health Laboratory
Network (PHLN) of Australia. Members of the PHLN were asked to check records for
previous years and report how many Ralstonia isolates were made from blood cultures.
The laboratories that provided data to PHLN are shown in Table 1.

269
Table 1: Laboratories that provided information about isolates of Ralstonia
State Laboratory ACT The Canberra Hospital
Calvary Health Care National Capital Private Hospital
NSW South West Area Pathology Service Hunter Area Pathology Service Institute of Clinical Pathology and Medical Research South Eastern Area Laboratory Service SydPath Pacific Laboratory Medicine Services
NT Royal Darwin Hospital
QLD Queensland Health Forensic and Scientific Services
SA SA Pathology
TAS Royal Hobart Hospital
VIC Victorian Nosocomial Infectious Surveillance System
WA PathWest
In consultation with the TGA, we posted a message on ProMED (Appendix 3) asking if
other countries had an increase in propofol-associated Ralstonia bacteraemia.
Microbiology Bacterial cultures from confirmed cases were initially identified as Ralstonia species by
the pathology laboratories using either matrix assisted laser desorption/ionization-time
of flight (MALDI-TOF) or sequencing of the 16S rRNA gene. All isolates were
subsequently sent to the UQCCR to be compared using the DiversiLabTM platform
(bioMérieux) for rep-polymerase chain reaction (PCR) DNA fingerprinting (66). This
method utilises specially designed primers that produce different sized PCR products in
different species of highly similar bacteria. It can be used to differentiate bacteria to the
species level, and in some cases genotypes within a species (67). Additional Ralstonia
isolates held in the QLD culture collection were included in the DiversiLabTM analysis
for comparison with the isolates from cases in the cluster. In addition, Ralstonia
isolates from clinical samples (e.g. throat aspirates) from non-bacteraemic patients at
the same hospital as two of the bacteraemic cases were included. These non-
bacteraemic samples were not included in the cluster investigation as they did not meet
the case definition. DiversiLabTM results were shared with the Ralstonia CDNA-WG on
23 May 2014.

270
Isolates underwent Whole Genome Sequencing (WGS) at the Microbial Genomics
group in the SCMB at UQ. Sequencing was performed at the Australian Genome
Research Facility (AGRF) using the Illumina HiSeq2500. The Microbial Genomics
group in-house analysis pipeline was used for sequence assembly and phylogenetic
analysis. WGS results were made available to CDNA on 24 April 2015.
Simulated case-control and case-cohort studies To inform decisions about analytical epidemiological studies, we simulated hypothetical
case-control and case-cohort studies. We based our assumptions on what was already
known about the reported cases. For both the case-control and case-cohort
simulations, we calculated Odds Ratios (ORs) assuming a total of eight cases (the
number of cases that had been reported as of 29 May 2014) that had received propofol
prior to developing Ralstonia bacteraemia, and we tested four different scenarios of
cases who did not receive propofol before developing Ralstonia bacteraemia: zero (the
real situation at the time of the simulation), one, two and three. We assumed that each
case would be in a ward with ten other patients who did not have Ralstonia
bacteraemia, and for the case control, we simulated three controls per case. For each
scenario, the OR, 95% confidence intervals (CI) and p-values were calculated for four
different rates of propofol usage among controls: 90%, 50%, 25% and a value that
gave a significant 95% CI (lower bound just above 1) and p-value (<0.05). Due to
values of less than five in at least one cell in all simulations, Fisher’s exact test was
used to calculate 95% CI for scenarios with a value greater than zero in all cells and for
all p-values. For scenarios in which there were zero cases in one cell (i.e. zero cases
with no propofol exposure), Cornfield’s Approximation was used to calculate 95% CIs.
All calculations were conducted using StataSE 13.
Bradford-Hill Framework The Bradford-Hill framework for causation (68) was used to assess the causal
relationship between Ralstonia bacteraemia and propofol in this cluster of cases.
Causal association was assessed using the following criteria:
Strength of association between exposure and outcome
o This typically refers to measures of association obtained during analytical
studies. In this investigation we used a case series along with simulated
case-control and case-cohort measures of association.
o We also examined the association between illness and specific brands and
batches of propofol.
Consistency of findings across different populations

271
o Comparison of results from different study designs
o Review of past outbreaks published in the literature.
Specificity in the relationship between exposure and outcome
o Assessed by comparing specificity of
Genotypes of isolates of the bacteria from different locations
Batch numbers of propofol used
Type of disease (i.e. bacteraemia)
Temporality, i.e. the outcome occurred after (and not before) exposure
o Incubation time between administration of propofol and onset of
bacteraemia.
Biological gradient, i.e. dose-effect relationship between exposure and outcome
o Dose response related to bolus (single dose) versus infusions.
Biological plausibility of the association between exposure and disease
o How could the propofol or the outer surface of the vial rubber stopper have
become contaminated with bacteria?
o Is polyclonal contamination of propofol and/or the vial stopper plausible?
Coherence, i.e. cause-effect relationship does not conflict with what is known of the
natural history and biology of the disease
o Review of polyclonal outbreaks published in the literature.
Experimental evidence, i.e. removing exposure or laboratory-based experiments
o Effect of quarantining propofol
o Release of propofol from quarantine
Analogy
o Review of microbial contamination of medical products (drug solutions,
vials/rubber stoppers) published in the literature.
Distribution chain of propofol The distribution chain of propofol from manufacture in India through to use in a clinic or
hospital in Australia was determined through discussion with staff of the TGA.
Environmental investigation Details of any microbiological testing performed within the clinic or hospital were
requested as part of the questionnaire completed by hospital or public health staff, as is
shown in Appendix 2.

272
Testing of propofol Propofol vials were tested for the presence of Ralstonia species using the methods
described below. The TGA, SA Pathology, the manufacturer and two independent
laboratories tested a total of 2738 vials of propofol from 31 different batches (six
batches were not supplied to Australia), including the two batches originally implicated
by SA (A030906 and A030907). The vials were tested for contamination by four
different methods
1. Test for sterility (TGA, manufacturer, independent laboratories).
2. Test for bacterial endotoxins (TGA, manufacturer, independent laboratories).
3. Microbial contamination test of vial contents (TGA, SA Pathology and one
independent laboratory).
4. Microbial contamination test of flip-off lids and the external surface of the rubber
stopper (TGA, SA Pathology and one independent laboratory).
Both the test for sterility and the test for bacterial endotoxins are standard tests used
prior to release of injectable medicines. A “pass” result for the test for sterility means
that no bacterial or fungal contamination was detected in the portion of sample tested,
while a “pass” for the test for bacterial endotoxins means that no bacterial endotoxins
were detected in the portion of sample tested. If an injectable medicine gets a “pass”
for both tests, and if all other manufacturing and batch release criteria are met, then the
batch can be released (69).
The test for microbial contamination of vial contents is not a standard test for injectable
medicines but was included as an additional test in this investigation. Similarly, the test
for microbial contamination of flip off lids and rubber stoppers was adapted for the
purposes of this investigation. The method for the latter differed slightly between the
TGA and SA Pathology. Whereas the TGA laboratory is accredited for this type of
environmental test, and was able to ensure maintenance of aseptic technique
throughout the procedure, SA Pathology holds accreditation only for testing of human
diagnostic samples and medical devices, and they have limited accreditation for
environmental testing. The TGA was able to test the lid and stopper of one vial at a
time, whereas SA Pathology pooled the tests for groups of five vials (from a single
box), and placed the disinfected whole flip-off lid of each vial into the culture medium,
along with the swabs of the outer surfaces of the rubber stoppers. In addition, SA
Pathology did not use positive or negative controls during their procedure. Any isolates
obtained from environmental studies were sent to UQCCR for genotyping by
DiversiLabTM and to UQ SCMB for WGS.

273
Delphi Method Members for the expert panel volunteered to participate during the CDNA-WG
teleconference or were suggested by other members. The members included three
infectious disease physicians (two professors, one associate professor), a clinical
microbiologist and three medical epidemiologists. The Delphi coordination and
synthesis team consisted of Mahomed Patel, Anna-Lena Arnold and I. The Delphi
consisted of three rounds where responses were requested from participants and a
final concluding document.
In Round 1, we proposed a series of questions and asked for comment and
suggestions to revise and refine the questions. Suggestions for additional questions
were also sought. We used this input from the panel members to refine the questions
for Round 2. In Round 2, we asked the members to respond to the refined questions.
We collated and synthesised these responses and for Round 3, we de-identified the
responses and asked the members to comment on their own and other’s responses
and our synthesis. We also added additional questions to further explore the themes of
the responses in Round 2 and conducted a literature review to answer some questions
raised. Round 4 collated, synthesised and summarised the discussion of the previous
three rounds.
Results
Timeline of investigation Figure 1 shows a timeline of significant events during this investigation and the date of
detection of bacteraemia for all cases of Ralstonia reported during 2014.

274
Figure 1: Timeline of cases (by date of detection of Ralstonia) and events during the
investigation. Cases included in the investigation are shown in red, excluded cases are in brown

275
Case series Table 2 shows the number of isolations of Ralstonia by PHLN member laboratories
nationwide. Due to availability of data, different years were reported by different state
representatives. Based on the information provided, a mean of four cases of Ralstonia
bacteraemia were reported annually across Australia, compared with eight cases in the
5 week-period from 1 April to 4 May 2014.
Table 2: Frequency of isolation of Ralstonia species by state and year
State/ Territory
Number of Ralstonia isolates from blood cultures
Year Before April 2014 Between 1 April and 4 May 2014
QLD
2011 2012 2013
Jan-Mar 2014
1 2 3 0
4
SA 2013 Jan-Mar 2014
0 0 3
VIC 2004-2013 Jan-Mar 2014
5 0 1
NT 2013 Jan-Mar 2014
0 0 0
ACT 2012 2013
Jan-Mar 2014
1 0 0
0
TAS 2012 - 2013 0 0 WA 2012 – 2013 1 0
NSW
1998 2001 2003 2009
2010-Mar 2014
1 1 1 3 0
0
Australia 2011-2013 4 per year 8
The eight cases of Ralstonia bacteraemia were reported with a date of detection of
clinical infection (used as a proxy for onset of illness, as onset of bacteraemia is difficult
to determine in hospitalised patients) between 1 January 2014 and 4 May 2014 (the
date range included in the case definition). The epidemic curve is shown in Figure 2,
and the simplified line list is shown in Table 3. Three additional cases of Ralstonia
bacteraemia were reported during or after the investigation and Delphi Method were
completed. These three cases are not shown in the epidemic curve as they were not
included in the CDNA-WG investigation due to onset dates after completion of the
investigation. However, they have been included in the timeline in Figure 1. The three
cases include a child at SA3 and an adult at VIC2, both with a history of use of the
same brand of propofol after propofol had been released from quarantine and a case

276
from QLD3 that had no association with propofol. Although these cases were not
included in the CDNA-WG investigation, they will be included in the analysis and
discussion contained within this chapter. No other countries responded to our ProMED
post reporting Ralstonia bacteraemia associated with administration of propofol.
Cases were reported from six different hospitals and three different states. In QLD, one
case was reported from QLD hospital 1 in Brisbane (QLD1), one from QLD hospital 2
(QLD2, also in Brisbane) and two cases were reported from QLD hospital 3 (QLD3) at
the Gold Coast. In SA, two cases were reported by SA hospital 1 (SA1) and one from
an endoscopy unit at SA hospital 2 (SA2). Both hospitals are located in Adelaide. The
single case in VIC was reported by a rural hospital, also from a patient in an endoscopy
unit (VIC1).
All eight cases identified during the CDNA-WG investigation received propofol before
Ralstonia was isolated from their blood sample, although the exact batch numbers of
propofol used for each case were not certain as hospitals don’t routinely record batch
numbers when medications are used. The batch numbers shown in Table 4 were the
most likely batch numbers based on the hospital propofol inventory at the time of
reporting. Two of the cases received a single bolus dose of propofol (both before
endoscopy), while the remaining six cases received an infusion involving multiple vials
of propofol (shown as coloured bars in Figure 2). The time between the first injection of
propofol (the earliest possible time of infection if the propofol is contaminated) and
onset of bacteraemia ranged between 2 hours and 23 days.
All cases were adults (median 54 years, range 28-64), and 62.5% (n=5) were male
(Table 3). With the exception of the two cases who attended endoscopy clinics, all
other cases were in hospital for a period of time, and had multiple medical
interventions.

277
Figu
re 2
: Epi
dem
ic c
urve
sho
win
g th
e ei
ght c
ases
with
Ral
ston
ia b
acte
raem
ia s
ince
1 J
anua
ry 2
014
by d
ate
of d
etec
tion
of in
fect
ion
and
date
of p
ropo
fol
adm
inis
tratio
n. C
olou
r cod
ing
show
s ge
netic
sim
ilarit
y of
clin
ical
isol
ates
bas
ed o
n D
iver
siLa
b re
sults
. QLD
= Q
ueen
slan
d, S
A =
Sou
th A
ustra
lia, V
IC =
Vic
toria
,
END
O =
gas
tro-in
test
inal
end
osco
py u
nit,
OT
= op
erat
ing
thea
tre, I
CU
= in
tens
ive
care
uni
t, P
= da
te w
hen
prop
ofol
was
adm
inis
tere
d, P
I = d
ates
of p
ropo
fol
infu
sion
. For
“VIC
” and
“SA
2”, d
ate
of p
ropo
fol a
dmin
iste
red
was
sam
e as
det
ectio
n of
bac
tera
emia

278
Tabl
e 3:
Sim
plifi
ed li
ne li
st o
f cas
es o
f Ral
ston
ia b
acte
raem
ia d
urin
g 20
14
TGA
ID
Hos
pita
l Se
x Ag
e R
easo
n fo
r hos
pita
lisat
ion
Dat
e of
bac
tera
emia
sy
mpt
om o
nset
D
ate
prop
ofol
rece
ived
Sa
mpl
e (n
)
3401
80
QLD
1 M
64
Su
rgic
al
18/0
4/20
14
15/0
4/20
14
Bloo
d (4
), As
pira
te (3
)
3401
65
QLD
2 M
61
M
edic
al
4/05
/201
4 17
/04/
2014
, 25/
04/1
4 an
d 27
/04/
2014
Bl
ood
3397
61
QLD
3 F
54
Surg
ical
1/
05/2
014
8/04
/201
4 Bl
ood
(2)
3407
53
QLD
3 M
33
Su
rgic
al
1/05
/201
4 8/
04/2
014,
15/
04/2
014
and
2/05
/201
4 Bl
ood
3395
52
SA2
M
64
Surg
ical
– e
ndos
copy
17
/04/
2014
17
/04/
2014
Bl
ood
3395
47
SA1
M
28
Med
ical
– IC
U
18/0
4/20
14
Infu
sion
com
men
ced
13/0
4/20
14
Bloo
d (3
)
3395
49
SA1
F 52
M
edic
al –
ICU
23
/04/
2014
20
/4/2
014,
21/
4/20
14, i
nfus
ion
com
men
ced
23/4
/201
4 Bl
ood
3396
87
VIC
1 F
61
Surg
ical
– e
ndos
copy
1/
04/2
014
1/04
/201
4 Bl
ood
NA
QLD
3 M
59
M
edic
al
15/0
6/20
15
NA
Bloo
d
3469
78
VIC
2 M
64
M
edic
al –
ICU
28
/08/
2014
22
/08/
2014
Bl
ood
(2)
NA*
SA
3 M
1
Med
ical
– IC
U
Augu
st 2
014
Unk
now
n Bl
ood
* Thi
s ca
se w
as n
ot fo
rmal
ly re
porte
d to
the
TGA.
As
a re
sult,
spe
cific
info
rmat
ion
is n
ot a
vaila
ble.

279
Tabl
e 4:
Bat
ches
of p
ropo
fol t
hat m
ay h
ave
been
use
d pr
ior t
o ca
ses
deve
lopi
ng R
alst
onia
bac
tera
emia
Bra
nd
Bat
ch
Prod
uctio
n da
te
Rep
ortin
g H
ospi
tal*
Det
ails
of R
alst
onia
isol
ated
from
cas
es
Spec
ies
Div
ersi
LabTM
gen
otyp
e W
GS
geno
type
Prod
uct 1
A020
648
09/2
012
QLD
3 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
A020
647
09/2
012
QLD
3 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
A030
071
01/2
013
QLD
3 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
A030
085
01/2
013
QLD
3 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
A030
293
04/2
013
VIC
1 R
. man
nito
lilytic
a Si
ngle
ton
3 C
lade
3b
A030
288
04/2
013
VIC
1 R
. man
nito
lilytic
a Si
ngle
ton
3 C
lade
3b
A030
906†
09/2
013
SA1
R. m
anni
tolily
tica
Clu
ster
3
Cla
de 3
b SA
2 SA
1 R
. pic
ketti
i Si
ngle
ton
2 C
lade
2
VIC
1 R
. man
nito
lilytic
a Si
ngle
ton
3 C
lade
3b
A030
907†
09/2
013
SA1
R. m
anni
tolily
tica
Clu
ster
3
Cla
de 3
b SA
2 SA
1 R
. pic
ketti
i Si
ngle
ton
2 C
lade
2
VIC
1 R
. man
nito
lilytic
a Si
ngle
ton
3 C
lade
3b
A031
195
11/2
013
QLD
1 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
QLD
3
A031
202
11/2
013
QLD
1 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
QLD
3
A031
203
11/2
013
QLD
1 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
QLD
3
A031
210
11/2
013
QLD
1 R
. man
nito
lilytic
a C
lust
er 2
C
lade
3a
QLD
3 A0
3119
6 11
/201
3 Q
LD3
R. m
anni
tolily
tica
Clu
ster
2
Cla
de 3
a

280
Bra
nd
Bat
ch
Prod
uctio
n da
te
Rep
ortin
g H
ospi
tal*
Det
ails
of R
alst
onia
isol
ated
from
cas
es
Spec
ies
Div
ersi
LabTM
gen
otyp
e W
GS
geno
type
Prod
uct 2
A0
3050
4 06
/201
3 Q
LD2
R. i
nsid
iosa
Si
ngle
ton
6 C
lade
1
A031
110
11/2
013
QLD
2 R
. ins
idio
sa
Sing
leto
n 6
Cla
de 1
U
nkno
wn
Unk
now
n Q
LD1
R. m
anni
tolily
tica
Clu
ster
2
Cla
de 3
a * S
A =
Sout
h Au
stra
lia, Q
LD =
Que
ensl
and,
VIC
= V
icto
ria
† Mos
t lik
ely
impl
icat
ed b
atch
es b
ased
on
dist
ribut
ion
and
usag
e

281
A summary of the genotype analysis based on DiversilabTM is shown in Figure 3, and
follows the same colour coding as in Figure 2. The isolates from the eight cases of
Ralstonia bacteraemia fall into five different genotypes. No single genotype was found
in more than one state. The isolates from QLD1 and QLD3 were strains of R.
mannitolilytica (Cluster 2). The remaining isolate from QLD (QLD2), was a strain of R.
insidiosa (Singleton 6). Two of the isolates from SA, one from SA1 and one from the
SA2, were strains of R. mannitolilytica (Cluster 3), while the other isolate from SA1 is a
strain of R. pickettii (Singleton 2). The isolate from VIC1 is a strain of R. mannitolilytica,
Singleton 3. The figure includes samples from QLD that were not included in our
investigation. These samples are greyed out in Part A of the figure.
The phylogenetic relationship of the isolates in this cluster, based on WGS, is shown in
Figure 4. Part A of the figure shows the relationship of all isolates, clustering according
to the species previously identified. The resolution of this tree was too low to resolve
the relationships of the isolates of R. mannitolilytica, so part B shows a cladogram
(where branch lengths are not related to genetic distance) of the R. mannitolilytica
isolates. The QLD isolates form a clade of closely related isolates (Clade 3a) which is
distinct from the clade of clinical isolates that includes two SA isolates, the VIC1 isolate
as well as the isolate from the lid of the propofol vial (Clade 3b). These data were not
available during the Delphi process so assessments were made using only the
DiversiLabTM data. A comparison of the DiversiLabTM and WGS results is shown in
Table 5. Although the names given to genetically related groups identified by each
method are different, most groups contain the same isolates in each method, with the
exception of the VIC1 isolate, which shows a distinct genotype in the DiversiLabTM
analysis, but is genetically indistinguishable from the SA R. mannitolilytica isolates in
WGS.

282
Figure 3: Summary of DiversiLabTM analysis of Ralstonia isolates, adapted from figures
provided by Hanna Sidjabat, UQCCR. Dendrogram showing relatedness of isolates, as
determined by DiversiLabTM. Coloured boxes show multiple isolates from a single patient. All
other samples are one isolate per patient. QLD = Queensland, SA = South Australia, VIC =
Victoria, TA = tracheal aspirate, NA = not applicable (not samples from patients during 2014), *
= reference isolates. Samples shown in grey are not a part of the cluster of cases of
bacteraemia

283
A.
B.
Fi
gure
4: P
hylo
gene
tic re
late
dnes
s of
isol
ates
of R
alst
onia
. Iso
late
s in
gre
y ar
e no
t par
t of t
his
clus
ter i
nves
tigat
ion
and
are
incl
uded
for c
ompa
rison
onl
y. T
he
hosp
ital c
ode
is s
how
n in
bra
cket
s. B
oth
trees
wer
e ad
apte
d fro
m fi
gure
s pr
ovid
ed b
y th
e M
icro
bial
Gen
omic
s G
roup
at S
CM
B, U
Q. A
. Phy
loge
netic
tree
sho
win
g
the
rela
tions
hip
betw
een
isol
ates
in th
e di
ffere
nt s
peci
es. T
he le
ngth
of t
he b
ranc
h co
rresp
onds
to g
enet
ic d
ista
nce.
The
isol
ates
of R
. man
nito
lilyt
ica
(Cla
des
3a a
nd
3b) a
re h
ighl
y si
mila
r and
are
not
abl
e to
be
dist
ingu
ishe
d on
this
sca
le. B
. Cla
dogr
am o
f iso
late
s of
R. m
anni
tolily
tica.
The
bra
nch
leng
ths
are
not p
ropo
rtion
al to
the
gene
tic d
ista
nce.
The
isol
ates
of R
. man
nito
lilytic
a ca
n be
sep
arat
ed in
to tw
o di
stin
ct c
lade
s, C
lade
3a
and
Cla
de 3
b. T
he re
fere
nce
sequ
ence
use
d w
as a
dra
ft
vers
ion
of th
e se
quen
ce o
f iso
late
339
547.
Sam
ples
340
180-
1 to
340
180-
7 w
ere
inde
pend
ent i
sola
tes
from
a s
ingl
e pa
tient

284
Table 5: Comparison of DiversiLabTM and whole genome sequencing (WGS) results for clinical
isolates and the propofol lid isolate
TGA ID Hospital Species DiversiLabTM WGS 340165 QLD2 R. insidiosa Singleton 6 Clade 1 339549 SA1 R. pickettii Singleton 2 Clade 2 340180 QLD1 R. mannitolilytica Cluster 2 Clade 3a 340180 QLD1 R. mannitolilytica Cluster 2 Clade 3a 340753 QLD3 R. mannitolilytica Cluster 2 Clade 3a 339761 QLD3 R. mannitolilytica Cluster 2 Clade 3a 339547 SA1 R. mannitolilytica Cluster 3 Clade 3b 339552 SA2 R. mannitolilytica Cluster 3 Clade 3b 339687 VIC R. mannitolilytica Singleton 3 Clade 3b
NA Propofol R. mannitolilytica Cluster 3 Clade 3b
Environmental testing Limited environmental testing was done within the facilities reporting the cases. Only
SA1 reported the results of testing, stating that multiple swabs in the ICU were
negative. As a result, environmental testing focused on the suspected common
exposure of propofol vials.
Testing of propofol Vials of propofol from the two main implicated batches, in addition to vials from 23
other batches from the same manufacturer that were distributed in Australia were
tested for contamination of the propofol solution. Vials from 15 of these batches were
also tested for external contamination on the flip off lids and outer surface of the rubber
stoppers. A full list of batch numbers, tests, laboratories and results are shown in
Appendix 4. All tests for microbial or endotoxin contamination of the propofol solution
were negative.
In contrast, both the TGA and SA Pathology isolated a variety of species of bacteria
from the flip-off lids and/or outer surface of the rubber stoppers of the vials from the
implicated batches (A030906 and A030907) (Table 6). The TGA also isolated similar
species of bacteria from other batches tested (Appendix 4). All of the bacterial species
identified were common environmental or skin contaminants. SA Pathology also
isolated R. mannitolilytica from one pool of flip-off lids and swabs of rubber stopper
outer surfaces taken from five vials of batch A030907. Vials from the same box of
propofol were retested in an attempt to confirm the isolation of R. mannitolilytica but
this was not successful. The caveats provided by SA Pathology state that

285
“aseptic techniques were used; however, removal of vial lids was difficult
and adventitious contamination may have been introduced during the
sampling and testing processes….isolation of Bacillus species from some
pools might reflect lack of sporicidal activity of 70% alcohol used for
disinfection of external surfaces of vial lids”
In addition, SA Pathology had not been able to use appropriate positive and negative
controls. The single isolate was sent to UQCCR and SCMB for comparison with the
patient isolates, and is shown in Figure 3, labelled as “propofol”. This isolate was
similar to the two R. mannitolilytica isolates from SA in Cluster 3.
Table 6: Testing results for microbial contamination of flip-off lids and outer surfaces of rubber
stoppers of vials of propofol from the main implicated batches
Batch Lab Single
or pool
Number positive (number tested)
Percent positive
Bacterial species identified
A030906
TGA Single 12 (80 vials) 15% Bacillus, Gram positive cocci
SA Pathology Pool 10 (14 pools, 70
vials) 71% Bacillus (10 pools), coagulase-negative
staphylococci (3 pools)
A030907
TGA Single 7 (80 vials) 9% Bacillus, Gram positive cocci
SA Pathology Pool 15 (18 pools, 90
vials) 83%
Bacillus (10 pools), coagulase-negative
staphylococci (5 pools), Ralstonia mannitolilytica (1
pool)
Simulated epidemiological studies This cluster had only eight cases, all had received propofol produced at the same
manufacturing site from six different health care providers. Due to these factors,
discussions in meetings of the CDNA-WG were unable to decide if an analytical study
would be able to obtain a significant measure of association for administration of
propofol. In order to assess this, we calculated the ORs for simulations that mimic the
likely scenario of an analytical study. For both simulated scenarios (case control in
Table 7 and case cohort in Table 8), significance was attained between 30% propofol
use among controls (in a case control study where three cases of Ralstonia
bacteraemia did not receive propofol) and 65% propofol use among controls (in a case
cohort study where zero cases of Ralstonia bacteraemia did not receive propofol). This
level of propofol use is not realistic in a clinical setting, as propofol is a commonly used
anaesthetic. Therefore, a formal case control or case cohort study was not undertaken.

286
Tabl
e 7:
Sim
ulat
ion
of a
cas
e co
ntro
l stu
dy. T
he m
axim
um p
ropo
fol u
sage
that
resu
lts in
a s
tatis
tical
ly s
igni
fican
t ass
ocia
tion
is s
hade
d
Num
ber o
f cas
es w
ith
Ral
ston
ia b
acte
raem
ia
Num
ber i
n st
udy
base
with
out R
alst
onia
bac
tera
emia
O
dds
Rat
io
Rec
eive
d pr
opof
ol
Did
not
re
ceiv
e pr
opof
ol
Num
ber
elig
ible
as
cont
rols
Num
ber
sele
cted
as
cont
rols
(3
/cas
e)
% w
ho
rece
ived
pr
opof
ol
Num
ber i
n st
udy
base
w
ho re
ceiv
ed
prop
ofol
Num
ber o
f co
ntro
ls w
ho
rece
ived
pr
opof
ol
Poin
t es
timat
e 95
% C
I p-
valu
e
8
0 80
24
90
72
22
Und
efin
ed
0.2,
∞
0.6
64
51.2
15
U
ndef
ined
1.
1, ∞
0.
05
50
40
12
Und
efin
ed
1.8,
∞
0.01
25
20
6
Und
efin
ed
5.2,
∞
<0.0
01
1 90
27
90
81
24
1.0
0.1,
59.
0 0.
70
50
45
14
7.4
0.8,
354
.4
0.05
40
36
11
11
.6
1.2,
547
.7
0.01
25
23
7
22.9
2.
2, 1
062.
9 0.
002
2 10
0 30
90
90
27
0.4
0.04
, 6.3
0.
37
50
50
15
4.0
0.6,
43.
4 0.
09
35
35
11
6.9
1.1,
74.
4 0.
02
25
25
8 11
.0
1.6,
119
.1
0.00
5
3 11
0 33
90
99
30
0.3
0.03
, 2.5
0.
15
50
55
17
2.5
0.5,
16.
9 0.
19
30
33
10
6.1
1.1,
41.
6 0.
02
25
28
8 8.
3 1.
5, 5
7.4
0.01

287
Tabl
e 8:
Sim
ulat
ion
of a
cas
e co
hort
stud
y. T
he m
axim
um p
ropo
fol u
sage
that
resu
lts in
a s
tatis
tical
ly s
igni
fican
t ass
ocia
tion
is s
hade
d N
umbe
r of c
ases
with
Ral
ston
ia
bact
erae
mia
N
umbe
r in
coho
rt w
ithou
t Ral
ston
ia b
acte
raem
ia
OR
=RR
Rec
eive
d pr
opof
ol
Did
not
re
ceiv
e pr
opof
ol
Tota
l num
ber i
n co
hort
%
who
rece
ived
pr
opof
ol
Num
ber w
ho
rece
ived
pro
pofo
l Po
int e
stim
ate
95%
CI
p-va
lue
8
0 80
90
72
Und
efin
ed
0.2,
∞
0.45
65
52
U
ndef
ined
1.
1, ∞
0.
04
50
40
Und
efin
ed
2.0,
∞
0.00
6 25
20
U
ndef
ined
5.
9, ∞
<0
.001
1 90
90
81
0.89
0.
1, 4
3.8
0.63
50
45
8.
0 0.
99, 3
602.
6 0.
03
45
41
9.6
1.2,
432
.6
0.01
25
23
23
.3
2.8,
104
8.7
<0.0
01
2 10
0
90
90
0.44
0.
07, 4
.9
0.30
50
50
4.
0 0.
74, 4
0.0
0.07
40
40
6.
0 1.
1, 5
9.9
0.02
25
25
12
.0
2.1,
120
.0
<0.0
01
3 11
0
90
99
0.3
0.06
, 2.0
1 0.
12
50
55
2.7
0.6,
16.
3 0.
13
35
39
4.9
1.1,
29.
6 0.
02
25
28
7.8
1.7,
47.
9 0.
003

288
Distribution chain of propofol The propofol brands implicated in this cluster are produced in India. The distribution
chain is shown in Figure 5. Contamination of the product at the different points marked
in Figure 5, sections A, B and C, would be expected to result in different patterns of
contamination. If contamination occurred at any point in section A, the contamination
could be expected anywhere the product is sent to from the Sponsor’s (the company
that imports a product into Australia) warehouse (potentially the whole country).
Contamination in section B would be restricted to only the locations served by the
central pharmacy or wholesaler in which the contamination occurred, within a single
state. Contamination in section C would be localised to only the hospital in which the
contamination occurred.
Figure 5: Distribution of propofol in Australia. Different patterns of contamination are
represented by A, B and C. If contamination occurred during the part represented by “A”, it
would be spread across Australia, and the same genotype or genotypes could be expected to
be found across the country. If contamination occurred in part “B”, it would be restricted to the
state where it occurred. In part C, contamination would be localised to specific hospitals or
wards or patients

289
Assessment of causation using Bradford-Hill framework In the absence of an analytical study, and in order to make the most of the limited data
collected in this small cluster, we applied the Bradford-Hill framework to assess
causation and determine if there was a clear link between use of propofol and
Ralstonia bacteraemia. A full discussion of aspects of the cluster in relation to each
criterion is shown in Table 9.
Table 9: Assessment of Bradford-Hill framework for causation using evidence for and against
the implication of propofol as the source of Ralstonia infection. This table is modified and
updated from a table prepared as a collaborative effort by Mahomed Patel, Anna-Lena Arnold
and I for reporting to CDNA-WG
Standard of evidence suggested by Bradford Hill
Evidence for and against each standard (we have stated ‘Uncertain’ where data are lacking or we lack appropriate technical knowledge)
Strength of association between exposure and outcome
For
All cases with Ralstonia bacteraemia received propofol. This means
that there was zero risk if propofol was not administered and the
RR/OR for association of propofol with Ralstonia bacteraemia is very
high.
Six of the eight cases received a single brand of propofol, one received
the same brand in addition to a second brand, and one received only
the second product. The two implicated products are produced at the
same manufacturing plant.
Against
Any analytical study would have
o Low power (only eight cases)
o Multiple confounders (i.e. other opportunities to acquire the
infection)
o Multiple potential selection and measurement biases inherent
in a retrospective study, including undiagnosed Ralstonia
bacteraemia in people designated as non-cases and recall
bias about treatments
The strength of association with vials from specific propofol batch
numbers is unknown. The exact batches administered were confirmed
only for the patient at QLD2 (A031110 and A030504), while batch
details for the other cases were not certain. In total, at least three and
up to seven different batches may be implicated (as detailed in Table
4)

290
Standard of evidence suggested by Bradford Hill
Evidence for and against each standard (we have stated ‘Uncertain’ where data are lacking or we lack appropriate technical knowledge)
Propofol is frequently used in hospitals. An average of 4800 vials of
propofol produced by the implicated manufacturer is used every day
across Australia (personal communication, Vladimir Illievski, AFT
Pharmaceuticals).
Consistency of our findings across different populations
For
Multistate nosocomial outbreaks of Ralstonia have been reported from
contamination of medical products in multiple different studies and
publications. This shows consistency across studies using different
methodologies (10, 11, 15, 16, 19).
Multistate nosocomial outbreaks as a result of intrinsic contamination
of propofol have been reported in multiple different studies and
publications (13, 28, 70).
Multistate nosocomial outbreaks caused by polyclonal (≥2 isolates)
contamination of a medical product have been reported in the literature
(18, 22, 28).
Specificity in the relationship between exposure and outcome
For
An isolate of Ralstonia from the lid of a vial of propofol (A030907) is
genetically indistinguishable from clinical isolates from two patients
managed at the two hospitals in SA (based on DiversiLabTM results).
WGS results suggest that the VIC1 isolate is also genetically
indistinguishable from the isolate from the lid and the clinical isolates in
the two SA patients. Two of the propofol batch numbers that were
possibly used in VIC1 correspond to the possible batch numbers used
in SA.
Against
This isolation of Ralstonia from the lid of propofol vials could not be
replicated when the rubber stoppers from the same vials were retested
at a later date at the same laboratory (the flip-off lids were not able to
be retested).
The strains of Ralstonia isolated from eight cases belonged to three
different species of Ralstonia in four genetically distinct groups, i.e.
Clade 1 (R. insidiosa), Clade 2 (R. pickettii) and Clades 3a and 3b
(distinct groups of R. mannitolilytica) as shown in Figure 4.
o Two clades in SA – Clade 2 and Clade 3b (one isolate of R.
pickettii and 2 isolates of R. mannitolilytica respectively)

291
Standard of evidence suggested by Bradford Hill
Evidence for and against each standard (we have stated ‘Uncertain’ where data are lacking or we lack appropriate technical knowledge)
o Two clades in QLD – Clade 1 and Clade 3a (R. insidiosa and
R. mannitolilytica respectively)
o One clade in VIC – Clade 3b (R. mannitolilytica)
The specificity of association by propofol batch number is uncertain.
There are at least three and up to seven different batches implicated,
and it is not known which specific batches were used in six cases
(Table 4).
Specificity of type of disease is true if only cases identified according to
the case definition are considered.
o The cluster of cases with Clade 3a R. mannitolilytica in QLD
includes isolates from non-bacteramic patients and isolates
from patients who did not receive propofol.
o A later blood isolate from a case of Ralstonia bacteraemia who
did not receive propofol, also from QLD and also in the same
genetic cluster strengthens the case against specificity
o A separate investigation by QLD Health found convincing
evidence that the cases from QLD1 and QLD3 (including non-
bacteraemic cases) were associated with bottled water either
consumed or used for cleaning medical equipment.
Temporality, i.e. the outcome occurred after (and not before) exposure
For
All cases received propofol between two hours and 23 days before
developing clinical infection.
Uncertain
The expected incubation period for Ralstonia bacteraemia is unknown.
Members of the CDNA-WG (including clinicians) have expressed
uncertainty about the interval acceptable to be defined as the
incubation period. In two cases the incubation period was two and five
hours respectively (both of whom were given propofol immediately
before an endoscopy) and in two other cases, the incubation periods
were 23 days each.
Biological gradient, i.e. dose-effect relationship between
For
The very short incubation periods of two and five hours have been
interpreted as a dose-response relationship because patients being
prepared for an endoscopy are given large bolus dose/s of propofol.

292
Standard of evidence suggested by Bradford Hill
Evidence for and against each standard (we have stated ‘Uncertain’ where data are lacking or we lack appropriate technical knowledge)
exposure and outcome
Uncertain
Is a dose response relationship plausible if only the vial or the cap of
the vial was contaminated but not the propofol solution?
Biological plausibility of the association between exposure and disease
For
Injecting a solution when the needle is contaminated with Ralstonia is
known to cause bacteraemia.
The propofol solution and/or outer surface of the vial stopper could
have been contaminated if sterilisation procedures at the
manufacturing facility were inadequate.
The propofol packages and vials could have been contaminated during
transport, distribution and storage of supplies, and in the process of
drawing up and injecting the propofol solution.
The propofol packages and vials could have been contaminated with
multiple strains of Ralstonia.
Uncertain
The combination of polyclonal contamination of propofol with four
genetically different strains of Ralstonia, and cases in different states
having different unique genotypes requires explanation. One
explanation for this scenario is separate contamination events at state
level (see Figure 5 for an explanation).
Coherence i.e. cause-effect relationship does not conflict with what is known of the natural history and biology of the disease
For
Polyclonal Ralstonia contamination of medical solutions as well as of
medical devices has been reported (18, 22, 28)
Uncertain
There are no reports in the literature of contamination of a medical
product with four different strains of the same bacteria, and where
genotypes differ across localities.
Experimental evidence i.e. removing exposure or lab-based
For
No new propofol associated cases were reported during the period of
quarantine.
Two additional cases (one from SA and one from VIC) were reported

293
Standard of evidence suggested by Bradford Hill
Evidence for and against each standard (we have stated ‘Uncertain’ where data are lacking or we lack appropriate technical knowledge)
experiments in August 2014, after the propofol had been released from quarantine.
Against
No new cases were reported among those who received propofol
between 27 April 2014 and the date of quarantine on 2 May 2014 (5
days).
A new case with no reported association with propofol was reported on
26 June 2014 at QLD3.
Analogy For
Multiple strains (polyclonal) of other bacteria contaminating medical
solutions and devices have been reported.
Given the limited information available in this investigation, assessing this information
using the Bradford-Hill framework was unable to provide a definitive answer as to
whether the propofol was the source of the Ralstonia infections. A consensus opinion
via expert panel was sought using the Delphi Method.
Delphi Method The Delphi Method is a collaborative process used to build consensus about a topic by
using opinion and advice from an “Expert Panel”. After simulations showed the difficulty
of attaining statistical significance in analytical studies, assessment of causality with the
Bradford-Hill criteria resulted in more questions than answers, and discussions during
the teleconferences of the Ralstonia working group were unable to achieve any
conclusions, we decided to adapt the design of the Delphi Method to attempt to
achieve consensus about the major questions associated with this cluster. Specifically,
we wanted to discuss:
1. Were all the cases of Ralstonia bacteraemia reported during April and early May
2014 associated with the same exposure?
2. Was that exposure propofol?
3. Was the propofol liquid or the outer surface of the vial stopper contaminated with
Ralstonia?
4. How/where did the propofol vial become contaminated with Ralstonia?
Figure 6 shows the design of our Delphi and how many participants responded in each
round. The number of participants responding to the Delphi decreased over the course

294
of the process, from all seven Panel Members providing feedback in Round 1, six
Panel Members responding in Round 2, and five Panel Members responding in Round
3.
Figure 6: Summary of Delphi rounds used in this investigation
A synthesis of the Panel Member’s answers to the questions in Round 2 is provided in
Table 10, and a summary of the responses provided to scenarios posed in Round 3 is
provided in Table 11. Little consensus was achieved by Round 3, and discussion with
the participants suggested that further rounds would not help to resolve the
disagreements. This was a reflection of the uncertainty evident throughout this
investigation. Supported by the laboratory testing, the only question on which
consensus was achieved was whether contamination of propofol occurred in the
solution or the outside of the vial (specifically the outer surface of the rubber stopper or
plastic flip off lid). All members of the panel agreed that the propofol solution was
unlikely to be contaminated, but that the outer surface of the rubber stopper should not
be considered sterile, and that if the propofol was the source of some or all of the

295
cases, contamination of the outer surface of the rubber stopper may have been the
route of infection. Answers for the remaining questions varied widely, with some
participants considering some scenarios “almost certain”, while others considered the
same scenario “almost certainly not”.
Table 10: Synthesis of Panel Member’s answers to Round 2 Delphi questions as prepared by
Mahomed Patel, Anna-Lena Arnold and Fiona May
Question Facilitators’ synthesis and conclusion
Q 1: What incubation period could be considered consistent with a causal association between propofol administration and bacteraemia?
There were many potential confounders that
could impact on the duration of the incubation
period. To maintain a high index of suspicion
that the eight cases may all have been
associated with the administration of propofol,
we retained all cases for further consideration in
this analysis.
Q 2: If we assumed that propofol administration was causally associated with bacteraemia, can we conclude that pre-existing contamination of the propofol solution was unlikely and that the vial cap and/or rubber stoppers were more likely to have been the source of the Ralstonia?
The vial cap and/or rubber stoppers rather than
the propofol solution was the more likely source
of the Ralstonia, but other sources of the
bacteria cannot be excluded.
Q 3: How confidently can we exclude other possible sources of exposure (apart from propofol administration) to Ralstonia in some or all the cases?
Vial cap/rubber stopper was a likely source in
the SA cases (if supported by WGS), but other
sources of Ralstonia spp cannot be excluded for
the other cases.
Q 4: How likely is it that a patient with Ralstonia bacteraemia but without signs of a pulmonary infection may have transmitted Ralstonia to another patient as an explanation of why the same strain of Ralstonia was isolated from the sputum or tracheal aspirate of a patient who never received propofol?
Environmental contamination is the more likely
source.
Q 5a: How should we interpret the finding of the Ralstonia isolate from the vial cap, noting the caveat from SA Pathology?
Three members consider the isolation of
Ralstonia from the vial cap to be significant, and
one of them awaits confirmation with the results
of the WGS.

296
Question Facilitators’ synthesis and conclusion
Three members do not appear to be as
convinced of the clinical significance of the
finding in making a causal association.
Q 5b: How should we interpret the TGA result of contamination of the internal surface of flip-off seal and rubber stopper with other bacteria?
Vial cap/rubber stopper were contaminated with
environmental bacteria.
The plastic flip-off lid does not maintain sterility
of the outer surface of the rubber stopper (61,
62)
Q 5c: How do these interpretations influence your judgement of the hypothesis that propofol administration is causally associated with Ralstonia bacteraemia?
Similar to our summary in 5a: two members
support the hypothesis, and one of them awaits
confirmation with the results of the whole
genome sequence (WGS). Three members
appear not to be as convinced, and the sixth
member did not respond to this question.
Q 6: Can we confidently implicate or exclude propofol administration as the cause of Ralstonia bacteraemia in some or all the cases?
Two members suggest propofol administration is
a likely cause for the cases in SA, and one of
them awaits confirmation with the result of WGS.
One member suggests that contamination of the
vial at the manufacturing site could explain the
diverse genotypes - two genotypes in SA cases,
and one genotype each in the case from QLD2
and VIC1.
Q 7: Noting the genetic similarity between the R. mannitolilytica isolate from the propofol vial cap and the clinical isolates from the two cases in different SA hospitals, and the distinctive R. pickettii isolate from the second patient in the same neurosurgical unit of SA1, can we conclude that Ralstonia bacteraemia in all three cases was causally associated with the administration of propofol, and that the propofol/vial did not become contaminated in the respective clinical unit?
One member accepts propofol administration
was the source, three accept this explanation for
the two cases with R. mannitolilytica (one of
them accepts if this was confirmed with WGS).
Three members are uncertain about the source
for the case with R. pickettii. One member says
there is insufficient evidence to implicate
propofol, although this is possible.
Three members agree that it is unlikely that
contamination occurred in the clinical unit.
Q 8: How confident can we be that the The source of infection in the two bacteraemic

297
Question Facilitators’ synthesis and conclusion cases reported in QLD and/or VIC with diverse genetic strains were also causally associated with the administration of propofol because all of them had received propofol?
cases at QLD3, and possibly of the first case
reported from QLD1 in May was unlikely to be
propofol.
Source of the infection in the case from VIC1 is
uncertain.
Q 9: Based on the DiversiLab results and on the uncertainty of the batch number of propofol vials used in SA, VIC and QLD, what plausible hypotheses could we formulate on the likely site/s of contamination? More specifically, how likely is it that the propofol/vial may have been contaminated (a) at some stage before delivery to the clinical unit and (b) after arrival in the clinical unit?
One member considers contamination at the
factory as “the only plausible explanation” and
another member considers this acceptable if
clonality can be confirmed with WGS. One
member considers contamination occurred at
some point before propofol was distributed to SA
hospitals. Two other members are open-minded
about the locality where the vial may have been
contaminated.
Q 10: What is the likelihood the propofol/vial was contaminated at the site of manufacture?
One member considers this “highly likely” and
another “most likely”. Three members say there
is insufficient information to answer the question.
One member considers this possible “if we
assume the cases in different states are linked”.

298
Tabl
e 11
: Syn
thes
is o
f Pan
el M
embe
r’s re
spon
ses
to th
e pl
ausi
bilit
y of
six
hyp
othe
ses
Hyp
othe
sis
on s
ourc
e of
Ral
ston
ia
Plau
sibi
lity
of h
ypot
hese
s*
Com
men
t Tw
o SA
cas
es
with
R.
man
nito
lilyt
ica
SA1
case
w
ith
R.
pick
ettii
VIC
1 ca
se w
ith
R.
man
nito
lilyt
ica
QLD
2 ca
se
with
R.
insi
dios
a
QLD
1 ca
se w
ith
R.
man
nito
lilyt
ica
Two
QLD
3 ca
ses
with
R.
man
nito
lilyt
ica
1.
Prop
ofol
sol
utio
n co
ntam
inat
ed a
t th
e m
anuf
actu
ring
site
D
isag
ree
x5
Dis
agre
e x5
D
isag
ree
x5
Dis
agre
e x5
D
isag
ree
x5
Dis
agre
e x5
Al
l Pan
el M
embe
rs
agre
e th
is is
unl
ikel
y fo
r al
l cas
es
2.
Prop
ofol
sol
utio
n an
d vi
al c
ap/ru
bber
st
oppe
r co
ntam
inat
ed a
t th
e m
anuf
actu
ring
site
Dis
agre
e x5
D
isag
ree
x5
Dis
agre
e x5
D
isag
ree
x5
Dis
agre
e x5
D
isag
ree
x5
All P
anel
Mem
bers
ag
ree
this
is u
nlik
ely
for
all c
ases
3.
Onl
y vi
al
cap/
rubb
er s
topp
er
cont
amin
ated
at
the
man
ufac
turin
g si
te
Dis
agre
e x2
, Ag
ree
x2
Dis
agre
e x2
, Ag
ree
x2
Dis
agre
e x2
, Ag
ree
x2
Dis
agre
e x2
, Ag
ree
x1
Dis
agre
e x3
, Ag
ree
x1
Dis
agre
e x3
, Ag
ree
x1
Pane
l mem
bers
are
al
mos
t eve
nly
split
as
to
whe
ther
the
vial
ca
p/ru
bber
sto
pper
was
co
ntam
inat
ed a
t the
m
anuf
actu
ring
site
. Sl
ight
ly m
ore
mem
bers
th
ink
this
is u
nlik
ely,
pa
rticu
larly
for c
ases
fro
m s
tate
s ot
her t
han
SA.
4.
Vial
cap
/rubb
er
stop
per
cont
amin
ated
afte
r le
avin
g m
anuf
actu
ring
site
bu
t bef
ore
stoc
ked
in th
e cl
inic
al u
nit
Dis
agre
e x1
, Ag
ree
x3
Dis
agre
e x2
, Ag
ree
x2
Dis
agre
e x3
, Ag
ree
x1
Dis
agre
e x3
D
isag
ree
x3,
Agre
e x1
D
isag
ree
x3,
Agre
e x1
All m
embe
rs a
gree
this
is
unl
ikel
y fo
r the
cas
e fro
m Q
LD2.
Slig
htly
m
ore
mem
bers
thin
k th
is is
unl
ikel
y fo
r all
but
the
R. p
icke
ttii c
ase
from
SA1
. 5.
Vi
al c
ap/ru
bber
st
oppe
r D
isag
ree
x2,
Agre
e x2
D
isag
ree
x2,
Agre
e x2
D
isag
ree
x3,
Agre
e x1
D
isag
ree
x3
Dis
agre
e x3
, Ag
ree
x1
Dis
agre
e x3
, Ag
ree
x1
All m
embe
rs a
gree
this
is
unl
ikel
y fo
r the
cas
e

299
Hyp
othe
sis
on s
ourc
e of
Ral
ston
ia
Plau
sibi
lity
of h
ypot
hese
s*
Com
men
t Tw
o SA
cas
es
with
R.
man
nito
lilyt
ica
SA1
case
w
ith
R.
pick
ettii
VIC
1 ca
se w
ith
R.
man
nito
lilyt
ica
QLD
2 ca
se
with
R.
insi
dios
a
QLD
1 ca
se w
ith
R.
man
nito
lilyt
ica
Two
QLD
3 ca
ses
with
R.
man
nito
lilyt
ica
cont
amin
ated
in
clin
ical
uni
t due
to
poor
ase
ptic
te
chni
ques
from
QLD
2, M
embe
rs
are
even
ly s
plit
for t
he
SA c
ases
, but
mor
e m
embe
r con
side
r thi
s un
likel
y th
an li
kely
for
the
QLD
and
VIC
cas
es.
6.
Con
tam
inat
ion
was
no
t on
the
prop
ofol
vi
al c
ap/ru
bber
st
oppe
r, bu
t in
the
clin
ical
en
viro
nmen
t or
inje
ctin
g eq
uipm
ent i
n th
e cl
inic
al u
nit
Dis
agre
e x4
D
isag
ree
x2,
Agre
e x2
D
isag
ree
x2,
Agre
e x2
D
isag
ree
x2,
Agre
e x1
D
isag
ree
x4
Dis
agre
e x4
All m
embe
rs c
onsi
der
this
unl
ikel
y fo
r the
SA
R. m
anni
tolil
ytic
a ca
ses
and
all Q
LD c
ases
, but
ar
e cl
ose
to e
venl
y sp
lit
for o
ther
cas
es
* Pan
el M
embe
rs w
ere
aske
d to
sel
ect o
ne o
f the
follo
win
g re
spon
ses:
Alm
ost c
erta
in, h
ighl
y lik
ely,
like
ly/p
roba
ble,
unl
ikel
y or
alm
ost c
erta
inly
not
. Not
all
Pane
l M
embe
rs a
nsw
ered
all
ques
tions
, and
som
e Pa
nel M
embe
rs u
sed
othe
r res
pons
es. “
Alm
ost c
erta
in”,
“hig
hly
likel
y”, “
likel
y/pr
obab
le” a
nd “p
ossi
ble
still
!!” w
ere
defin
ed a
s “A
gree
”. “U
nlik
ely”
and
“Alm
ost C
erta
inly
Not
” wer
e de
fined
as
“Dis
agre
e”.

300
Discussion Despite using a number of different epidemiological techniques, including case series
analysis, simulation of analytical studies, assessment of causation and application of
the Delphi Method, we were unable to conclusively determine the source of this cluster
of cases of Ralstonia bacteraemia, or even if all cases were associated with a common
exposure. Although common in the environment (32-34), Ralstonia is not a commonly
reported cause of bacteraemia, so it was surprising that so many cases were reported
within a short time. However, it is not often tested for by laboratories as a routine, and
anecdotal reports suggest that if Ralstonia is isolated in pathology laboratories, and
there is no obvious reason to associate it with illness, it is often considered “a
contaminant” (personal communication, Dr Gary Lum).
The average number of cases reported by PHLN member labs in previous years was a
mean of four cases per year, suggesting that detection of eight cases in just over a
month was higher than expected and worthy of further investigation. There were a
further three reports of Ralstonia bacteraemia in July and August. However, due to
heightened national awareness, this may be an artefact of pathology laboratories
actively looking for Ralstonia, and genetic typing has not been provided for two of the
three. These latter three cases were identified during or after the conclusion of this
investigation, and were therefore not considered in the analysis as presented to the
CDNA-WG.
In response to the detection of Ralstonia in both bacteraemic and non-bacteraemic
patients at QLD3, QLD Health conducted an independent investigation, and identified
the source of these cases as a brand of bottled water provided to patients (personal
communication, Dr Heidi Carroll, QLD Health). An isolate of R. mannitolilytica of the
same genotype as that from the cases at QLD1 and QLD3 (Clade 3a) was obtained
from a sample of the water. QLD Health provided the Ralstonia CDNA-WG with
information about this investigation in June, and has not shared the final outcome of
the investigation. While this investigation was ongoing concurrently with our
investigation, a lack of information flow to the working group meant that these cases
were unnecessarily considered as having the same exposure as the remaining cases
throughout the entire epidemiological investigation and through the first three rounds of
the Delphi. On 11 July 2014, Dr Jeanette Young, the Chief Health Officer of QLD,
released a memorandum to chief executives at QLD Health and Hospital Services,
recommending against providing bottled water to immunocompromised patients. This
source of Ralstonia infection is consistent with a previous study that found Ralstonia
species in bottled water in France (71).

301
The percent similarity obtained with rep-PCR (repetitive sequence-based polymerase
chain reaction) techniques such as DiversiLabTM should be analogous to the true
genetic relationships between isolates since differences in rep-PCR patterns are due to
the underlying genetic sequence (i.e. isolates that are more similar to each other than
to other isolates by rep-PCR analysis are more genetically similar to each other (67)).
However, rep-PCR relationships are not directly related to genetic identity. Indeed, a
comparison of WGS with rep-PCR showed that they result in similar classifications for
different strains but rep-PCR doesn’t have the same sensitivity as WGS for highly
similar isolates (67). Similarly, in this study, the phylogenetic tree obtained by WGS
shares some of the same basic structure as the DiversiLabTM dendrogram but they
differ as the isolates become increasingly closely genetically related (genotypes of
species) and the clades identified by WGS are slightly different from those identified by
DiversiLabTM. DiversiLabTM analysis relies on kits designed for specific bacterial
genera. As there is no Ralstonia kit, the Pseudomonas kit was used for these samples
as this was the genus most closely related to Ralstonia. The effect this had on the
results of the analysis is unknown.
The most striking difference between the DiversiLabTM dendrogram and the WGS
phylogenetic analysis is the classification of the VIC1 isolate as being genetically
indistinguishable from the two SA clinical isolates and lid isolate in Clade 3b. This
evidence suggests a common source for the VIC1 isolate and the two SA isolates. The
isolate from the lid of a vial of propofol suggests propofol as this common source. This
classification was unknown during the Delphi process, and as such any conclusions
based on genetic relatedness did not take this into account. The WGS results only
became available after conclusion of the investigation. Rapid access to WGS data
would have provided evidence to link the propofol with cases from two states, and may
have negated the need for a Delphi. The singleton isolate from QLD2 is not closely
related to any other isolates and may be representative of sporadic Ralstonia infection.
If the propofol vial was contaminated with Ralstonia, it is impossible to confirm if it
became contaminated during manufacture, during storage and use in the clinical unit or
elsewhere along the distribution chain. It is unlikely that contamination occurred in the
clinical unit since the three genetically related cases in SA and VIC occurred in different
hospitals. Conversely, if the contamination occurred during manufacture, we would
expect a much higher incidence of Ralstonia bacteraemia across Australia than
reported, and we would expect the pattern of distribution of the genotypes to be more
uniform. If the cases in SA were associated with propofol, the most parsimonious
explanation is that contamination occurred after the propofol was distributed to SA.
However, this explanation does not account for the case in VIC. The hospital in which

302
the VIC1 case occurred is in the south west of VIC, and services patients from SA in
addition to south west VIC. Whether the propofol used in this hospital was sourced
from the same stocks as the SA hospitals is unknown.
More than 4800 vials of propofol of the implicated brand are used across Australia daily
(personal communication, Vladimir Illievski, AFT Pharmaceuticals), and even more
across the world. If contaminated at the manufacturer, one explanation for the low
number of reported cases is patchy external contamination of the vials in combination
with good clinical practice, including swabbing of rubber stoppers and immediate
administration of propofol after drawing into the syringe, and the low virulence of
Ralstonia. This theory is supported by evidence that disinfection of rubber stoppers on
similar styles of vials have shown that this can reduce the rate of contamination of
needles used to enter the vial (62, 63) and studies examining growth of bacteria in
contaminated propofol shows that the bacteria grow to detectable levels after a lag of
approximately 6 hours (43, 72, 73).
The Delphi method was used in this investigation. It was chosen as a more formal
method to achieve consensus than the informal discussions in the CDNA-WG
teleconferences. The anonymous nature of the responses in the Delphi method is a
useful way of getting the participant’s true opinions about a topic without feeling
pressured to conform to the prevailing opinion of the group. By conducting the rounds
by email, we were able to include participants from almost all jurisdictions. However,
although we were aiming only for consensus and not unanimity, we were not able to
achieve this after three rounds of questions. By the third round, only five participants
responded, and not all of the responding participants answered all questions. The
comment common to all respondents was that there was insufficient information to
make conclusions about many of the topics under consideration. Not all Delphi
processes result in consensus, and depending on subject matter, this is not always
expected or desirable (2, 74). Two major limitations of this study were not knowing that
QLD were conducting a separate investigation, and not having WGS results until many
months after the investigation was concluded. Both of these factors would have
provided valuable information that may have resulted in achieving consensus.
The expert panel achieved consensus on only one question. They agreed that the
propofol solution was unlikely to be contaminated, but that the outer surface of the
rubber stopper should not be considered sterile. Only two studies have assessed the
protection provided to the rubber stopper by the plastic flip off lid of glass vials. Buckley
et al. (2004) tested vials of sterile saline for contamination after removal from sterile
packaging (note that propofol is not shipped in secondary sterile packaging). They

303
found that even though the vials are shipped in sterile packaging, 1% of the vials (1 of
100 tested) were contaminated with Staphylococcus aureus when swabbed
immediately after the flip off lid was removed (62). Hilliard et al. (2013) intentionally
contaminated vials with the flip off lid in place (the lid was disinfected before removal to
prevent cross contamination from the lid itself). Two out of 12 control vials (not
immersed in E. coli solution) had contaminated rubber stoppers (specific contaminants
were not identified), while after immersion in the liquid culture of E. coli with the flip off
lid in place, contamination was detected on the rubber stoppers of seven out of 10
vials. None of the vials treated with aerosolised E. coli was contaminated (61). Most
infection control guidelines for clinicians and health care workers recommend swabbing
of the rubber stoppers of all vials before inserting the needle (for example (65)). The
Australian Guidelines for the Prevention and Control of Infection in Healthcare only
advise “adherence to practices that prevent contamination of injection equipment and
medication” (75). However, surveys of health care workers (76) suggest that this does
not always happen. Indeed, two previous outbreaks associated with propofol (48, 53)
identified failure to disinfect the rubber stopper as a potential source of infection.
This investigation was complicated by its multijurisdictional and multi-organisational
nature. Although regular teleconferences of the Ralstonia CDNA-WG were held,
sharing of information was not as open or as efficient as it could have been, and roles
were not well defined. Through OzFoodNet, Australia has a good system for
investigating multijurisdictional foodborne outbreaks, but this was the first non-
foodborne point source multijurisdictional outbreak/cluster investigated using some of
the principles used for OzFoodNet multijurisdictional outbreak investigation. We
adapted the OzFoodNet methods for this cluster investigation, but a formal guiding
document for all multijurisdictional outbreaks of all types would be useful.
Other limitations of this investigation included the restrictive case definition and the
assumption of an exposure from the beginning of the investigation. Restricting the case
definition to only bacteraemic cases ignored the non-bacteraemic cases that were at
the same hospital and of the same genotype as two of the bacteraemic cases. By
including these cases, we may have recognised the distinct nature of the cases in QLD
earlier, allowing us to focus the investigation only on the remaining cases. Similarly,
propofol was the focus of the investigation from very early on, despite there being little
evidence to implicate it. Indeed, the only “evidence” was an absence of other common
sources identified between the case at SA2 and the cases at SA1. Despite these
limitations and the lack of consensus about the resolution to the national outbreak, the
source of the cases in QLD was elucidated (bottled water) and no new cases of
Ralstonia bacteraemia have been reported in Australia between August 2014 and

304
August 2015, despite an agreement from CDNA members to continue reporting of
cases of Ralstonia bacteraemia. CDNA is now considering developing guidelines for
non-foodborne multijurisdictional investigations.
Finally, this cluster of cases of Ralstonia bacteraemia with at least two distinct sources
was unexpected. On the surface, it seems unlikely that there would be two separate
outbreaks or clusters with different sources of exposure of such a rarely isolated
species of bacteria. However, the true incidence of nosocomial Ralstonia bacteraemia
or colonisation is unknown in Australia and elsewhere, suggesting that at least some of
these cases may have been background, and gone unnoticed in a year without greater
awareness of Ralstonia.
References 1. Dalkey N, Helmer O. An experimental application of the Delphi Method to the use of experts. Management Science. 1963;9(3):458-67. 2. Hsu C-C, Sandford BA. The Delphi technique: making sense of consensus. Practical Assessment, Research and Evaluation. 2007;12(10). 3. Yabuuchi E, Kosako Y, Yano I, Hotta H, Nishiuchi Y. Transfer of two Burkholderia and an Alcaligenes species to Ralstonia gen. Nov.: Proposal of Ralstonia pickettii (Ralston, Palleroni and Doudoroff 1973) comb. Nov., Ralstonia solanacearum (Smith 1896) comb. Nov. and Ralstonia eutropha (Davis 1969) comb. Nov. Microbiology and Immunology. 1995;39(11):897-904. 4. Adiloglu AK, Ayata A, Sirin C, Yondem C, Okutan H. [Case report: nosocomial Ralstonia pickettii infection in neonatal intensive care unit]. Mikrobiyoloji Bulteni. 2004;38(3):257-60. 5. Candoni A, Trevisan R, Patriarca F, Silvestri F, Fanin R. Pseudomonas pickettii (Biovar VA-II): a rare cause of bacteremias in haematologic patients. European Journal of Haematology. 2001;66(5):355-6. 6. Chetoui H, Delhalle E, Osterrieth P, Rousseaux D. Ribotyping for use in studying molecular epidemiology of Serratia marcescens: comparison with biotyping. Journal of Clinical Microbiology. 1995;33(10):2637-42. 7. Forgie S, Kirkland T, Rennie R, Chui L, Taylor G. Ralstonia pickettii bacteremia associated with pediatric extracorporeal membrane oxygenation therapy in a Canadian hospital. Infection Control and Hospital Epidemiology. 2007;28(8):1016-8. 8. Fujita S, Yoshida T, Matsubara F. Pseudomonas pickettii bacteremia. Journal of Clinical Microbiology. 1981;13(4):781-2. 9. Gardner S, Shulman ST. A nosocomial common source outbreak caused by Pseudomonas pickettii. Pediatric Infectious Disease. 1984;3(5):420-2. 10. Kendirli T, Ciftci E, Ince E, Incesoy S, Guriz H, Aysev AD, et al. Ralstonia pickettii outbreak associated with contaminated distilled water used for respiratory care in a paediatric intensive care unit. The Journal of Hospital Infection. 2004;56(1):77-8. 11. Kimura AC, Calvet H, Higa JI, Pitt H, Frank C, Padilla G, et al. Outbreak of Ralstonia pickettii bacteremia in a neonatal intensive care unit. The Pediatric Infectious Disease Journal. 2005;24(12):1099-103.

305
12. Kismet E, Atay AA, Demirkaya E, Aydin HI, Aydogan H, Koseoglu V, et al. Two cases of Ralstonia pickettii bacteremias in a pediatric oncology unit requiring removal of the Port-A-Caths. Journal of Pediatric Hematology/Oncology. 2005;27(1):37-8. 13. Labarca JA, Trick WE, Peterson CL, Carson LA, Holt SC, Arduino MJ, et al. A multistate nosocomial outbreak of Ralstonia pickettii colonization associated with an intrinsically contaminated respiratory care solution. Clinical Infectious Diseases. 1999;29(5):1281-6. 14. Lacey S, Want SV. Pseudomonas pickettii infections in a paediatric oncology unit. The Journal of Hospital Infection. 1991;17(1):45-51. 15. Maroye P, Doermann HP, Rogues AM, Gachie JP, Megraud F. Investigation of an outbreak of Ralstonia pickettii in a paediatric hospital by RAPD. The Journal of Hospital Infection. 2000;44(4):267-72. 16. Marroni M, Pasticci MB, Pantosti A, Colozza MA, Stagni G, Tonato M. Outbreak of infusion-related septicemia by Ralstonia pickettii in the Oncology Department. Tumori. 2003;89(5):575-6. 17. Mikulska M, Durando P, Pia Molinari M, Alberti M, Del Bono V, Dominietto A, et al. Outbreak of Ralstonia pickettii bacteraemia in patients with haematological malignancies and haematopoietic stem cell transplant recipients. The Journal of Hospital Infection. 2009;72(2):187-8. 18. Moreira BM, Leobons MB, Pellegrino FL, Santos M, Teixeira LM, de Andrade Marques E, et al. Ralstonia pickettii and Burkholderia cepacia complex bloodstream infections related to infusion of contaminated water for injection. The Journal of Hospital Infection. 2005;60(1):51-5. 19. Pasticci MB, Baldelli F, Camilli R, Cardinali G, Colozza A, Marroni M, et al. Pulsed field gel electrophoresis and random amplified polymorphic DNA molecular characterization of Ralstonia pickettii isolates from patients with nosocomial central venous catheter related bacteremia. The New Microbiologica. 2005;28(2):145-9. 20. Pellegrino FL, Schirmer M, Velasco E, de Faria LM, Santos KR, Moreira BM. Ralstonia pickettii bloodstream infections at a Brazilian cancer institution. Current Microbiology. 2008;56(3):219-23. 21. Raveh D, Simhon A, Gimmon Z, Sacks T, Shapiro M. Infections caused by Pseudomonas pickettii in association with permanent indwelling intravenous devices: four cases and a review. Clinical Infectious Diseases. 1993;17(5):877-80. 22. Roberts LA, Collignon PJ, Cramp VB, Alexander S, McFarlane AE, Graham E, et al. An Australia-wide epidemic of Pseudomonas pickettii bacteraemia due to contaminated "sterile" water for injection. The Medical Journal of Australia. 1990;152(12):652-5. 23. Sudo H, Hisada Y, Ito M, Kotaki H, Minami A. Burkholderia pickettii spondylitis. Spinal Cord. 2005;43(8):499-502. 24. Yuen KH, Ng FH, Mok KY, Ng WF. Monomicrobial nonneutrocytic bacterascites due to Burkholderia pickettii. The American Journal of Gastroenterology. 1998;93(11):2308-9. 25. Coenye T, Goris J, De Vos P, Vandamme P, LiPuma JJ. Classification of Ralstonia pickettii-like isolates from the environment and clinical samples as Ralstonia insidiosa sp. nov. International Journal of Systematic and Evolutionary Microbiology. 2003;53(Pt 4):1075-80. 26. Block C, Ergaz-Shaltiel Z, Valinsky L, Temper V, Hidalgo-Grass C, Minster N, et al. Deja vu: Ralstonia mannitolilytica infection associated with a humidifying respiratory therapy device, Israel, June to July 2011. Eurosurveillance. 2013;18(18):20471.

306
27. Daxboeck F, Stadler M, Assadian O, Marko E, Hirschl AM, Koller W. Characterization of clinically isolated Ralstonia mannitolilytica strains using random amplification of polymorphic DNA (RAPD) typing and antimicrobial sensitivity, and comparison of the classification efficacy of phenotypic and genotypic assays. Journal of Medical Microbiology. 2005;54(Pt 1):55-61. 28. Jhung MA, Sunenshine RH, Noble-Wang J, Coffin SE, St John K, Lewis FM, et al. A national outbreak of Ralstonia mannitolilytica associated with use of a contaminated oxygen-delivery device among pediatric patients. Pediatrics. 2007;119(6):1061-8. 29. Mukhopadhyay C, Bhargava A, Ayyagari A. Ralstonia mannitolilytica infection in renal transplant recipient: first report. Indian Journal of Medical Microbiology. 2003;21(4):284-6. 30. Phillips I, Eykyn S, Laker M. Outbreak of hospital infection caused by contaminated autoclaved fluids. Lancet. 1972;1(7763):1258-60. 31. De Baere T, Steyaert S, Wauters G, Des Vos P, Goris J, Coenye T, et al. Classification of Ralstonia pickettii biovar 3/'thomasii' strains (Pickett 1994) and of new isolates related to nosocomial recurrent meningitis as Ralstonia mannitolytica sp. nov. International Journal of Systematic and Evolutionary Microbiology. 2001;51(Pt 2):547-58. 32. Kulakov LA, McAlister MB, Ogden KL, Larkin MJ, O'Hanlon JF. Analysis of bacteria contaminating ultrapure water in industrial systems. Applied and Environmental Microbiology. 2002;68(4):1548-55. 33. Adley CC, Ryan MP, Pembroke JT, Saieb FM. Ralstonia pickettii: biofilm formation in high-purity water. Cardiff: Biofilm Club; 2005. 34. Koenig DW, Pierson DL. Microbiology of the Space Shuttle water system. Water Science and Technology. 1997;35(11-12):59-64. 35. Anderson RL, Holland BW, Carr JK, Bond WW, Favero MS. Effect of disinfectants on pseudomonads colonized on the interior surface of PVC pipes. American Journal of Public Health. 1990;80(1):17-21. 36. Barbut F, Kosmann MJ, Lalande V, Neyme D, Coppo P, Gorin NC. Outbreak of Ralstonia pickettii pseudobacteremia among patients with hematological malignancies. Infection control and Hospital Epidemiology. 2006;27(6):642-4. 37. Oie S, Kamiya A. Bacterial contamination of commercially available ethacridine lactate (acrinol) products. The Journal of Hospital Infection. 1996;34(1):51-8 38. Coenye T, Vandamme P, LiPuma JJ. Infection by Ralstonia species in cystic fibrosis patients: identification of R. pickettii and R. mannitolilytica by polymerase chain reaction. Emerging Infectious Diseases. 2002;8(7):692-6. 39. Coenye T, Goris J, Spilker T, Vandamme P, LiPuma JJ. Characterization of unusual bacteria isolated from respiratory secretions of cystic fibrosis patients and description of Inquilinus limosus gen. nov., sp. nov. Journal of Clinical Microbiology. 2002;40(6):2062-9. 40. Coenye T, Spilker T, Reik R, Vandamme P, Lipuma JJ. Use of PCR analyses to define the distribution of Ralstonia species recovered from patients with cystic fibrosis. Journal of Clinical Microbiology. 2005;43(7):3463-6. 41. Stelzmueller I, Biebl M, Wiesmayr S, Eller M, Hoeller E, Fille M, et al. Ralstonia pickettii-innocent bystander or a potential threat? Clinical Microbiology and Infection. 2006;12(2):99-101. 42. Arduino MJ, Bland LA, McAllister SK, Aguero SM, Villarino ME, McNeil MM, et al. Microbial growth and endotoxin production in the intravenous anesthetic propofol. Infection Control and Hospital Epidemiology. 1991;12(9):535-9.

307
43. Erden IA, Gulmez D, Pamuk AG, Akincia SB, Hascelik G, Aypar U. The growth of bacteria in infusion drugs: propofol 2% supports growth when remifentanil and pantoprazole do not. Brazilian Journal of Anesthesiology. 2013;63(6):466-72. 44. McHugh GJ, Roper GM. Propofol emulsion and bacterial contamination. Canadian Journal of Anaesthesia. 1995;42(9):801-4. 45. Obayashi A, Oie S, Kamiya A. Microbial viability in preparations packaged for single use. Biological & Pharmaceutical Bulletin. 2003;26(5):667-70. 46. Sklar GE. Propofol and postoperative infections. The Annals of Pharmacotherapy. 1997;31(12):1521-3. 47. Abdelmalak BB, Bashour CA, Yared JP. Skin infection and necrosis after subcutaneous infiltration of propofol in the intensive care unit. Canadian Journal of Anaesthesia. 2008;55(7):471-3. 48. Bennett SN, McNeil MM, Bland LA, Arduino MJ, Villarino ME, Perrotta DM, et al. Postoperative infections traced to contamination of an intravenous anesthetic, propofol. The New England Journal of Medicine. 1995;333(3):147-54. 49. Centers for Disease Control. Postsurgical infections associated with an extrinsically contaminated intravenous anesthetic agent--California, Illinois, Maine, and Michigan, 1990. MMWR Morbidity and Mortality Weekly Report. 1990;39(25):426-7, 33. 50. Chen SH, Kung CC, Fung ST. Endotoxemia due to propofol contamination in four consecutive patients. Journal of the Formosan Medical Association. 2014;113(5):328-9. 51. Fischer GE, Schaefer MK, Labus BJ, Sands L, Rowley P, Azzam IA, et al. Hepatitis C virus infections from unsafe injection practices at an endoscopy clinic in Las Vegas, Nevada, 2007-2008. Clinical Infectious Diseases. 2010;51(3):267-73. 52. Gutelius B, Perz JF, Parker MM, Hallack R, Stricof R, Clement EJ, et al. Multiple clusters of hepatitis virus infections associated with anesthesia for outpatient endoscopy procedures. Gastroenterology. 2010;139(1):163-70. 53. Henry B, Plante-Jenkins C, Ostrowska K. An outbreak of Serratia marcescens associated with the anesthetic agent propofol. American Journal of Infection Control. 2001;29(5):312-5. 54. Klein J, Huisman I, Menon AG, Leenders CM, van Eeghem KH, Vos MG, et al. [Postoperative infection due to contaminated propofol]. Nederlands tijdschrift voor geneeskunde. 2010;154:A767. 55. Muller AE, Huisman I, Roos PJ, Rietveld AP, Klein J, Harbers JB, et al. Outbreak of severe sepsis due to contaminated propofol: lessons to learn. The Journal of Hospital Infection. 2010;76(3):225-30. 56. Kuehnert MJ, Webb RM, Jochimsen EM, Hancock GA, Arduino MJ, Hand S, et al. Staphylococcus aureus bloodstream infections among patients undergoing electroconvulsive therapy traced to breaks in infection control and possible extrinsic contamination by propofol. Anesthesia and Analgesia. 1997;85(2):420-5. 57. Mathis S. Closing in on health care-associated infections in the ambulatory surgical center. The Journal of Legal Medicine. 2012;33(4):493-528. 58. Massari M, Petrosillo N, Ippolito G, Solforosi L, Bonazzi L, Clementi M, et al. Transmission of hepatitis C virus in a gynecological surgery setting. Journal of Clinical Microbiology. 2001;39(8):2860-3. 59. McNeil MM, Lasker BA, Lott TJ, Jarvis WR. Postsurgical Candida albicans infections associated with an extrinsically contaminated intravenous anesthetic agent. Journal of Clinical Microbiology. 1999;37(5):1398-403.

308
60. Veber B, Gachot B, Bedos JP, Wolff M. Severe sepsis after intravenous injection of contaminated propofol. Anesthesiology. 1994;80(3):712-3. 61. Hilliard JG, Cambronne ED, Kirsch JR, Aziz MF. Barrier protection capacity of flip-top pharmaceutical vials. Journal of Clinical Anesthesia. 2013;25(3):177-80. 62. Buckley T, Dudley SM, Donowitz LG. Defining unnecessary disinfection procedures for single-dose and multiple-dose vials. American Journal of Critical Care. 1994;3(6):448-51. 63. Simon PA, Chen RT, Elliott JA, Schwartz B. Outbreak of pyogenic abscesses after diphtheria and tetanus toxoids and pertussis vaccination. The Pediatric Infectious Disease Journal. 1993;12(5):368-71. 64. Sheth NK, Post GT, Wisniewski TR, Uttech BV. Multidose vials versus single-dose vials: a study in sterility and cost-effectiveness. Journal of Clinical Microbiology. 1983;17(2):377-9. 65. Dolan SA, Felizardo G, Barnes S, Cox TR, Patrick M, Ward KS, et al. APIC position paper: safe injection, infusion, and medication vial practices in health care. American Journal of Infection Control. 2010;38(3):167-72. 66. Healy M, Huong J, Bittner T, Lising M, Frye S, Raza S, et al. Microbial DNA typing by automated repetitive-sequence-based PCR. Journal of Clinical Microbiology. 2005;43(1):199-207. 67. Dominguez SR, Anderson LJ, Kotter CV, Littlehorn CA, Arms LE, Dowell E, et al. Comparison of Whole-Genome Sequencing and Molecular-Epidemiological Techniques for Clostridium difficile Strain Typing. Journal of the Pediatric Infectious Diseases Society. 2015. 68. Hill AB. The Environment and Disease: Association or Causation? Proceedings of the Royal Society of Medicine. 1965;58:295-300.. 69. Therapeutic Goods Administration. TGA guidelines for sterility testing of therapeutic goods. 2006. 70. Centers for Disease Control and Prevention. Nosocomial Ralstonia pickettii colonization associated with intrinsically contaminated saline solution--Los Angeles, California, 1998. MMWR Morbidity and Mortality Weekly Report. 1998;47(14):285-6. 71. Falcone-Dias MF, Vaz-Moreira I, Manaia CM. Bottled mineral water as a potential source of antibiotic resistant bacteria. Water Research. 2012;46(11):3612-22. 72. Sosis MB, Braverman B. Growth of Staphylococcus aureus in four intravenous anesthetics. Anesthesia and Analgesia. 1993;77(4):766-8. 73. Strachan FA, Mansel JC, Clutton RE. A comparison of microbial growth in alfaxalone, propofol and thiopental. The Journal of Small Animal Practice. 2008;49(4):186-90. 74. Mullen PM. Delphi: myths and reality. Journal of Health Organization and Management. 2003;17(1):37-52. 75. NHMRC. Australian guidelines for the prevention and control of infection in healthcare. Commonwealth of Australia; 2010. 76. Woodbury A, Knight K, Fry L, Margolias G, Lynde GC. A survey of anesthesiologist and anesthetist attitudes toward single-use vials in an academic medical center. Journal of Clinical Anesthesia. 2014;26(2):125-30.

309
Appendix 1: Targeted literature search and synthesis How commonly is contamination on the stoppers of glass medicine vials
reported in the literature?
How frequently and how easily are the rubber stoppers of glass vials contaminated with the flip off lid in place?
After a comprehensive search of the literature, only two papers have been identified
that assessed the frequency of contamination of rubber stoppers of any glass medicine
vials immediately after the plastic flip-off lid has been removed (1, 2). One of these
studies also assessed how well the lid protects the rubber stopper from intentional
contamination with a bacterial solution. No studies have examined where this
contamination is likely to have occurred along the chain of distribution. However, this is
likely to be difficult given that environmental contamination is possible at any point from
exiting the steriliser at the manufacturer to opening the vial in the clinical unit.
Although the style of packaging of saline vials is different to that of propofol (sterile
vials are provided in a pack of five in a plastic bag), and indeed the vials are less likely
to have become contaminated during distribution, Buckley et al (1994) found that 1% (1
of 100 tested) of rubber stoppers of saline vials were contaminated (with
Staphylococcus epidermidis) when swabbed immediately after the flip off lid was
removed (1).
A study by Hilliard et al (2013) intentionally contaminated the rubber stoppers with
cultures of E. coli before removing the flip off lid (the lid was disinfected before removal
to prevent cross contamination from the lid itself). Two out of 12 control vials (not
immersed in E. coli solution) had contaminated rubber stoppers (specific contaminants
were not identified), while after immersion in the liquid culture of E. coli with the flip off
lid in place, contamination was detected on the rubber stoppers of seven out of 10 vials
Interestingly, none of the vials treated with aerosolised E. coli were contaminated (2).
Although we could not identify other studies that specifically assessed the frequency of
contaminated rubber stoppers or the internal surface of the vial cap at the time the flip-
off cap is removed in the clinical setting, the plastic flip off lid should not be expected to
maintain sterility of the rubber stopper.

310
Does contamination of the rubber stopper result in contamination of the solution or transfer to the needle?
Only two studies were identified that assessed what would happen on the syringe
needle if the rubber stopper was contaminated. Simon’s study (1993) was triggered
when rubber stoppers on multi-dose vaccine vials became contaminated after they
were stored on benches on which blood cultures were performed. The rubber stoppers
of a vial of DTP vaccine were intentionally contaminated with a solution of
Streptococcus. The contents of the vials remained sterile, even after puncturing them
five times with a needle. However, the needles they used to puncture these rubber
stoppers did become contaminated (3) suggesting a mechanism for the contamination
and potential transmission of the infection to patients.
Another study assessed contamination of a variety of solutions with differing bacterial
growth potential (including sterile water, heparin and insulin) (4). The sterility of the
rubber stoppers of these vials were tested by entering the vial without swabbing the
rubber stopper or intentionally contaminating the rubber stopper with a mix of bacteria
before the stopper was punctured with a needle. They found low levels of
contamination of the solution in each of these scenarios (4). They did not test whether
the needles became contaminated. These studies suggest that if the rubber stopper is
contaminated, it is possible for this contamination to be transferred to the patient
through injection of the product either via contamination of the solution or the needle.
Does disinfection of the stoppers prior to use prevent transfer of contamination to the solution or needle?
Although disinfection of the rubber stopper is considered standard infection control
practice (as outlined in the Delphi Round 2 document and reported in in reference (5)
below, few studies have assessed how well alcohol disinfection of rubber stoppers
remove contamination. Two studies that examined the results of swabbing
contaminated rubber stoppers with 70% isopropyl alcohol found that this removed the
contamination from the stopper and resulted in no needles becoming contaminated
after piercing the stopper (1, 3).
In contrast, a study comparing routine handling of propofol with strict adherence to the
manufacturer’s recommendations reported no difference in levels of contamination.
However, this study only examined use of an infusion pump rather than bolus doses
(6).
These studies appear to suggest that standard infection control technique, including
disinfection of rubber stoppers before piercing with a needle, can protect against

311
environmental contamination of the stopper, and therefore protect against transmission
of the microbe to the patient.
Search terms use for this review:
Vial, stopper, diaphragm, septum, contaminat*, bacteria*, disinfect*, alcohol, isopropyl
References
1. Buckley T, Dudley SM, Donowitz LG. Defining unnecessary disinfection
procedures for single-dose and multiple-dose vials. American journal of critical care :
an official publication, American Association of Critical-Care Nurses. 1994;3(6):448-51.
Epub 1994/11/01.
2. Hilliard JG, Cambronne ED, Kirsch JR, Aziz MF. Barrier protection capacity of
flip-top pharmaceutical vials. Journal of Clinical Anesthesia. 2013;25(3):177-80. Epub
2013/04/09.
3. Simon PA, Chen RT, Elliott JA, Schwartz B. Outbreak of pyogenic abscesses
after diphtheria and tetanus toxoids and pertussis vaccination. The Pediatric Infectious
Disease Journal. 1993;12(5):368-71. Epub 1993/05/01.
4. Sheth NK, Post GT, Wisniewski TR, Uttech BV. Multidose vials versus single-
dose vials: a study in sterility and cost-effectiveness. Journal of Clinical Microbiology.
1983;17(2):377-9. Epub 1983/02/01.
5. Dolan SA, Felizardo G, Barnes S, Cox TR, Patrick M, Ward KS, et al. APIC
position paper: safe injection, infusion, and medication vial practices in health care.
American Journal of Infection Control. 2010;38(3):167-72. Epub 2010/03/30.
6. Lorenz IH, Kolbitsch C, Lass-Florl C, Gritznig I, Vollert B, Lingnau W, et al.
Routine handling of propofol prevents contamination as effectively as does strict
adherence to the manufacturer's recommendations. Canadian Journal of Anaesthesia.
2002;49(4):347-52. Epub 2002/04/03.

312
Appendix 2: Case report form

313

314

315

316

317
Appendix 3: ProMED post requesting information about contamination of propofol
Published Date: 2014-05-22 02:52:11 Subject: PRO/EDR> Ralstonia pickettii, sepsis - Australia: contaminated propofol, alert Archive Number: 20140522.2489978 RALSTONIA PICKETTII, SEPSIS - AUSTRALIA: CONTAMINATED PROPOFOL, ALERT ********************************************************************* A ProMED-mail post http://www.promedmail.org ProMED-mail is a program of the International Society for Infectious Diseases http://www.isid.org [1] Date: Tue 20 May 2014 From: Claire Behm <[email protected]> [edited] Increase in cases of ralstonia bacteremia associated with propofol in Australia ---------------------------------------------------------------------- The Therapeutic Goods Administration of Australia (TGA) is gathering information about cases with ralstonia bacteremia that are potentially related to administration of propofol. A multijurisdictional investigation has identified 8 cases of ralstonia bacteremia with a common link to administration of propofol. The most recent Australian case was reported on 4 May 2014. Investigations are ongoing. We look forward to hearing if colleagues in other countries have noticed any unusual increase in clinical isolations of ralstonia associated with propofol or other medical products or devices. -- Dr Claire Behm Signal Investigation - Medicines Office of Product Review Therapeutic Goods Administration Australia <[email protected]> [ProMED-mail thanks Dr Behm for bringing this outbreak to our attention. - Mod.ML]

318
Appendix 4: TGA testing Complete testing summary as provided by TGA, available at http://www.tga.gov.au/safety/alerts-medicine-provive-mct-lct-
140707.htm#.VBUJPGPiuSo
Testing results update
The TGA and three external laboratories have tested samples from 25 batches of
propofol 1% emulsion for injection supplied to Australia and New Zealand for sterility
and bacterial endotoxins. Samples from more than 1680 vials from these batches were
tested for compliance with sterility requirements and a further 97 vials were tested for
the presence of bacterial endotoxins. All samples passed the criteria for the tests for
sterility and bacterial endotoxins.
The external surfaces of injection vials, including the outer surface of the rubber
stopper and the inner surface of the vial lid, are not required to be sterile and so might
not be free from microbial contamination. Nevertheless, one laboratory undertook
testing of the outer surface of rubber stoppers and the inner surface of vial lids and
reported a positive test result for Ralstonia mannitolilytica from a single test pool of five
lids and rubber stoppers. As indicated in the Table, the laboratory has placed several
caveats on this test result.
To further investigate this finding the TGA and an external laboratory also tested the
outer surface of rubber stoppers and the inner surface of vial lids for microbial
contamination. In total, stoppers and lids from 524 vials across 15 batches of propofol
1% emulsion for injection have been tested. While this additional testing has revealed
microbial contamination on a low number of lids and rubber stoppers, this
contamination did not include Ralstonia mannitolilytica.

319
Table A1: Propofol 1 % emulsion for injection - results of microbiological testing
Batch number Laboratory1
Test for Sterility2
(vials tested)
Test for Bacterial
Endotoxins3 (vials tested)
Microbial Contamination
Test4 - vial contents
(vials tested)
Microbial Contamination Test - flip-off lid and
rubber stopper external surfaces5
No. positive for bacterial growth/no.
tested
Bacteria isolated
A030906 A Pass (20) Pass (1) Pass (3) 12/80 Bacillus species, Gram-positive cocci
B Pass (80) Pass (4) - - - C - - Pass (12) 10/14
pools 6, 7 (total 70 tested)
Bacillus species x 10 Coagulase-negative staphylococci x 3
A030907 A Pass (20) Pass (1) Pass (3) 7/80 Bacillus species, Gram-positive cocci
B Pass (80) Pass (4) - - - C - - Pass (10) 15/18 pools6,
7 (total 90 tested)
Bacillus species x 10 Coagulase-negative staphylococci x 5 Ralstonia mannitolilytica(1 pool)7
A031266 A - Pass (1) - - - B Pass (61) Pass (4) - - - D Pass (20) Pass (1) Pass (20) 0/20 -
A031267 A - Pass (1) - - - B Pass (61) Pass (4) - - - D Pass (20) Pass (1) Pass (20) 0/20 -
A040081 A - Pass (1) - - - B Pass (61) Pass (4) - - - D Pass (20) Pass (1) Pass (20) 0/20 -
A031282 B Pass (60) Pass (3) - - - E Pass (20) Pass (2) - - -
A031283 B Pass (60) Pass (3) - - - E Pass (20) Pass (2) - - -
A030021 A - Pass (1) - - - B Pass (60) Pass (3) - - -
A030146 A - Pass (1) - - - B Pass (60) Pass (3) - - -
A030293 A - Pass (1) Pass (3) - - B Pass (60) Pass (3) - - -
A0308728 B Pass (60) Pass (4) - - - A0308398 B Pass (40) Pass (4) - - - A0308408 B Pass (40) Pass (4) - - - A0309328 B Pass (60) Pass (4) - - - A0309368 B Pass (60) Pass (4) - - -

320
Batch number Laboratory1
Test for Sterility2
(vials tested)
Test for Bacterial
Endotoxins3 (vials tested)
Microbial Contamination
Test4 - vial contents
(vials tested)
Microbial Contamination Test - flip-off lid and
rubber stopper external surfaces5
No. positive for bacterial growth/no.
tested
Bacteria isolated
A0309378 B Pass (60) Pass (4) - - - A031027 B Pass (60) Pass (4) - - - A031069 B Pass (60) Pass (4) - - - A030504 B Pass (60) Pass (3) - - - A031202 B Pass (60) Pass (3) - - - A030288 B Pass (60) Pass (3) - - - A031203 A - - - 0/5 -
B Pass (60) Pass (3) - - - A031210 A - - - 1/5 Gram-
positive cocci
B Pass (60) Pass (3) - - - A030085 A - - - 2/20 Bacillus
species, Gram-positive cocci
B Pass (60) Pass (3) - - - A031195 A - - - 1/20 Bacillus
species, Gram-positive cocci
B Pass (60) Pass (3) - - - A031196 A - - - 2/20 Bacillus
species, Gram-positive cocci
B Pass (60) Pass (3) - - - A031256 A - - - 5/18 Bacillus
species, Gram-positive cocci
B Pass (60) Pass (3) - - - A031110 A - - - 4/20 Bacillus
species, Gram-positive cocci
B Pass (60) Pass (3) - - - A020647 A - - - 0/2 -
B Pass (60) Pass (3) - - - A020648 A - - - 1/19 Bacillus
species B Pass (60) Pass (3) - - -
A030071 A - - - 1/15 Gram-positive cocci
B Pass (60) Pass (3) - - - Notes
1. Laboratories A. TGA B. Manufacturer C. External laboratory7

321
D. External laboratory E. External laboratory
2. The Test for Sterility is a standard pharmacopoeial batch release test for an injectable medicine. A 'Pass' result means that no microbial contamination was detected in the portion of the samples that were tested. Each test uses 20 vials.
3. The Test for Bacterial Endotoxins is a standard pharmacopoeial batch release test for an injectable medicine. A 'Pass' result means that bacterial endotoxins were not detected in the portion of the samples that were tested.
4. The Microbial Contamination Test is not applicable to a sterile medicine. It was performed only as an adjunct test to estimate the level of microbial contamination should vial contents be contaminated. A 'Pass' result means that no microbial contamination was detected in the portion of the samples that were tested.
5. Flip-off lid and rubber stopper external surface swab tests were performed to assess bacterial contamination on these surfaces.
6. Testing was performed on pooled samples. Each pool contained the flip-off lids and swabs from the external surface of rubber stoppers from 5 vials.
7. Laboratory C has placed the following caveats on their test results: o The laboratory holds accreditation for testing of human diagnostic samples and
for testing of clinical, non-human specimens for investigation of nosocomial infections in outbreaks and/or individuals, e.g. gastrointestinal endoscopes, vascular catheter tips and transfusion bags. The laboratory has limited accreditation for environmental testing
o Testing of the flip-off lids and external surface of the rubber stoppers included testing of the entire flip-off lid after disinfection of the outer surface of the lid with 70% alcohol. Aseptic techniques were used; however, removal of vial lids was difficult and adventitious contamination might have been introduced during the sampling and testing processes, e.g. the detection of coagulase-negative staphylococci in some pools. Isolation of Bacillus species from some pools might reflect lack of sporicidal activity of 70% alcohol used for disinfection of external surfaces of vial lids.
o Test methods were adapted in-house. Test methods have not been fully validated and results should be interpreted accordingly.
o Ralstonia mannitolilytica was isolated from 1 of 32 pools. Ralstonia species are rarely recognised as contaminants in this laboratory.
These batches were not supplied to Australia or New Zealand Where a laboratory did not perform a test as part of the investigation the cell has a hyphen and is shaded.

322

323
Chapter 6 A case control study to determine the source of an outbreak of hepatitis A in
Queensland, 2015

324
Table of contents Prologue ................................................................................................................ 325
Study rationale ................................................................................................... 325
My role ............................................................................................................... 325
Lessons learned ................................................................................................ 325
Public health implications of this work ................................................................ 326
Acknowledgements ............................................................................................ 327
Master of Philosophy (Applied Epidemiology) core activity requirement ............. 327
Abstract ................................................................................................................. 327
Introduction ........................................................................................................... 328
Methods ................................................................................................................ 329
Study design ...................................................................................................... 329
Case definition and exclusion criteria ............................................................. 329
Control selection and exclusion criteria .......................................................... 329
Case control study and data analysis ............................................................. 330
Results .................................................................................................................. 331
Descriptive epidemiology ................................................................................... 331
Case control study ............................................................................................. 332
Discussion ............................................................................................................. 336
References ............................................................................................................ 338
Appendix 1: Lay summary for OzFoodNet website ................................................ 340
Appendix 2: Case questionnaire ............................................................................ 343
Appendix 3: Control questionnaire ......................................................................... 355

325
Prologue
Study rationale On 12 February 2015, OzFoodNet Victoria (VIC) informed the OzFoodNet national
network that three cases of locally acquired hepatitis A had been notified between
3 January 2015 and 6 February 2015, all with a single common exposure to a
popular brand of frozen mixed berries. On 13 February 2015, OzFoodNet New
South Wales (NSW) reported an additional locally acquired case of hepatitis A with
onset of illness 30 January 2015. The NSW case also reported consumption of the
implicated frozen mixed berries. On 14 February 2015, the distributor of the
implicated frozen mixed berries announced a voluntary consumer level recall of the
product. On 16 February, the Communicable Diseases Network Australia (CDNA)
recommended that OzFoodNet initiate a multi-jurisdictional outbreak investigation
(MJOI) into the cluster of cases of hepatitis A, and on 17 February 2015, the
National Incident Room (NIR) was activated. OzFoodNet conducted a case control
study to identify risk factors associated with illness in this outbreak of hepatitis A.
My role I attended the Australian Government Department of Health Rapid Assessment
Team (RAT) meeting on 16 February 2015, the result of which was the activation
of the NIR on 17 February 2015. As a result of the activation, I relocated to the NIR
to assist Ben Polkinghorne (OzFoodNet co-ordinating epidemiologist) as part of the
“epi team” for the MJOI. My role included scientific literature reviews and
situational awareness activities, minute taking at the regular teleconferences and
the Structured Audit, contributing to question time briefs, Situation Reports and
other advice, and developing and managing the NetEpi database tools used for
recording of case information and the results of the case control study.
I also assisted OzFoodNet Queensland (QLD) by conducting telephone interviews
of controls for the case control study, and analysing the QLD case control data to
compare with the national data. This chapter will focus on the QLD case control
sub-study.
Lessons learned Having a planned and organised MJOI response with guidelines to follow made
this outbreak a completely different experience compared with the Ralstonia
outbreak. In addition, having a formal debrief (structured audit) at the OzFoodNet
face-to-face in Adelaide on 24 June 2015 was very informative, and hopefully the
learnings from the structured audit will be applied to future MJOIs.

326
Most of the comments from the structured audit could be summarised under
themes of effective communication and knowing roles. Effective communication is
incredibly important in investigations where multiple people and multiple agencies
are involved. Similarly, knowing roles makes getting things done much easier as
people know what is required of them, and tasks don’t get missed or replicated.
Even though the berries were the suspected source from the beginning of the
investigation, I learned about the dangers of ill-considered case definitions,
especially those that include the suspected exposure. In reporting to ministers and
the media, it was decided early on to report the number of cases that had eaten
the implicated frozen mixed berries. However, this became problematic as
secondary and apparently outbreak-related non-berry cases were identified. It got
very complicated as there were three different case definitions for different
contexts.
In general, this outbreak was a real eye-opener about the conflict between what
information is required for epidemiology and what is required for pol itical
communications. And then there is what the media reports, which is often
completely unrelated to the facts!
As this was the first time I had participated in a case control study, I learned a lot
from listening to all the discussions about control selection and inclusion and
exclusion criteria. There are so many options for control selection, and it was great
to listen to all the experienced OzFoodNet epidemiologists discuss the pros and
cons of each. I also discovered, somewhat to my surprise, that I really enjoy
interviewing people. Most people are lovely and happy to help out. During the
analysis of the case control data, I also learned how to deal with zero cells to be
able to calculate an approximate Odds Ratio.
Public health implications of this work Learnings from this MJOI will be added to the MJOI Guidelines document currently
being drafted. Future MJOIs will benefit from these learnings.
An unforseen outcome of this outbreak was a greater awareness in the public
about the origins of foods. Although these berries were labelled as a product of
China, many people seemed to not be aware that these frozen berries were not a
product of Australia. Indeed, an indirect outcome of this outbreak will be changes
to country of origin labelling of food.

327
Acknowledgements Thanks to all the OzFoodNet members involved in this outbreak, especially Ben,
for his guidance in the NIR, and Russell Stafford (OzFoodNet QLD) for enabling
me to assist with the QLD interviews and then analyse the Queensland data.
Thanks also to Anna-Lena Arnold and Lisa McHugh (MAE scholars) for their
assistance with interviewing.
Master of Philosophy (Applied Epidemiology) core activity requirement Investigate an acute public health problem or threat.
A relevant report on the project (no more than 2 pages) to a non-scientific
audience such as the community or other stakeholder, as a press release or in the
form of a ministerial brief Appendix 1.
Abstract As part of a national investigation into a 2015 multi-jurisdictional hepatitis A outbreak, a
case control study was conducted by all jurisdictions that reported cases to identify risk
factors for illness. Since QLD had more cases than any other jurisdiction, OzFoodNet
QLD conducted an independent analysis of the data from QLD only.
Hepatitis A cases included in the case-control study were unambiguously locally
acquired (i.e. they had not travelled outside Australia during their exposure period), had
an onset of illness on or after 21 January 2015 and were notified in QLD. Cases were
excluded if the genotype was not IA or if the sequence was different from the outbreak
sequence (if known). Controls were cases of Salmonella notified in QLD and were
matched with cases based on age group and local government area at a ratio of two
controls to a case. Cases and controls were interviewed by telephone using a
questionnaire with defined questions. Analysis of data was performed using StataSE
13.
Twelve cases meeting the case definition were notified in QLD. The adjusted OR
calculated by exact logistic regression for consumption of frozen mixed berries was
41.9 (95% CI 5.5 – ∞, p-value <0.001) providing strong evidence that the implicated
frozen mixed berries were the source of the outbreak. No other food was associated
with illness.
The positive association between consumption of frozen mixed berries and hepatitis A
infection in QLD cases supports the evidence from national microbiological and
traceback studies.

328
Introduction Most cases of hepatitis A notified in Australia are in returned travellers who acquired
the illness in an endemic country overseas. In 2012, only 18% of hepatitis A
notifications in Australia were locally acquired and the majority of these were
secondary cases who had close contact with primary cases who contracted their
infection overseas (1). Hepatitis A is transmitted via the faecal-oral route, and in
developed countries transmission is often via food contaminated by either infectious
food handlers or in the case of fresh produce, via infectious workers or contamination
of the water used in production (2). Hepatitis A virus is resistant to many forms of
decontamination used in food production, such as chlorination, and can survive in
frozen produce for years (3). The incubation period can vary from 15 to 50 days, but is
usually 28 to 30 days. Symptoms of hepatitis A include fever, malaise, anorexia,
nausea, abdominal discomfort, pale faeces and jaundice (2). Severity can vary from a
mild illness lasting 1 to 2 weeks, to severe disease requiring a liver transplant in rare
cases. Hospitalisation is common (4).
In Australia, previous outbreaks of hepatitis A have been associated with poor
sanitation or food handling and have included imported semi-dried tomatoes (5) and
locally grown oysters (6), mussels (7) and prawns (8). In recent years, fresh and frozen
berries have been implicated in outbreaks of hepatitis A worldwide (9-19).
From 16 February to 27 May 2015, a multi-jurisdictional outbreak investigation
(MJOI) was conducted to investigate cases of locally acquired hepatitis A. From the
beginning of the MJOI, a single brand of frozen mixed berries was implicated as the
likely source of infection due to four cases of locally acquired hepatitis A (three in
Victoria and one in New South Wales) reporting eating this food product and having no
other common exposures. By the completion of the voluntary recalls on Monday 16
February 2015, QLD had notified four cases of hepatitis A that had also reported eating
the implicated berries. Sequencing of isolates from these four QLD cases returned
genotype 1A with an identical sequence, providing further evidence to support the
hypothesis that imported frozen mixed berries were the source of infection for this
outbreak. This sequence was later shown to be identical to that of other cases from the
national investigation. OzFoodNet decided to conduct a national case control study to
provide additional analytical evidence to support implication of the mixed berry product
and document the magnitude of the association. As QLD reported more outbreak
associated cases of hepatitis A than any other state, OzFoodNet QLD performed a
sub-analysis on QLD data only.

329
The aim of this study was to assess the association between hepatitis A and a variety
of food exposures among cases notified in QLD, and compare associations with the
results of the national case control study.
Methods
Study design The case control study was frequency matched on both age group (0-4 years, 5-17
years, 18-49 years and 50 years and older) and local government area (LGA) or health
region. Two controls were interviewed per case.
Case definition and exclusion criteria For the purposes of the case control study, a confirmed case was defined as a case of
hepatitis A (meeting the national case definition (20)) notified in QLD, with a Genotype
1A virus isolate of an identical genome sequence to the outbreak strain, with onset of
illness on or after 21 January 2015 and before 14 May 2015, who had not travelled
outside of Australia during their exposure period.
Cases of hepatitis A were excluded from the study if they had travelled overseas during
their exposure period (2 to 7 weeks before onset of symptoms), did not speak English
or were unable to give coherent answers to questions, were unable to provide a date of
onset of illness, or had close contact with a person known or suspected to have had
hepatitis A during the case’s exposure period (possible secondary transmission).
Permission for cases under 18 years of age was required from a parent or guardian.
For cases under 15 years of age, the parent or guardian was interviewed; for cases 15
to 17 years of age, the parent or guardian decided if they or the case were to be
interviewed. All interviews were conducted via telephone.
Control selection and exclusion criteria Two controls were selected for each case. Controls were sourced from notified cases
of Salmonella infection in QLD with a notification date in the two weeks prior to onset of
the hepatitis A case to which the control was matched. Controls were selected to
frequency match with cases based on age group (0-4 years, 5-17 years, 18-49 years
and 50 years and older) and local government area (LGA) or health region.
Controls were excluded from the study if they had travelled overseas during the two
months prior to infection, did not speak English or were unable to give coherent
answers to questions, had close contact with a person known or suspected to have had
hepatitis A during the control’s exposure period, had past infection or symptoms
consistent with hepatitis A, had received vaccination for hepatitis A, had received
normal human immunoglobulin (NHIG) during the two months prior to illness, lived in a

330
country or region with high or very high hepatitis A endemicity for a year or more during
the first five years of their life, or were not contactable by telephone. Controls who were
part of a Salmonella outbreak investigation were excluded.
A list of possible controls was randomised and contact via telephone was attempted.
All controls were called four times on at least two different days. At least two calls were
made before 9am or after 5pm on weekdays, or on a weekend. No message was left if
an answering machine picked up the call. If no contact was made after four calls, the
next person in the list was contacted. Permission for contacts under 18 years of age
was required from a parent or guardian. For those under 15 years of age, the parent or
guardian was interviewed; for those 15 to 17 years of age, the parent or guardian
decided if they or the control were to be interviewed.
Case control study and data analysis The questionnaire used for cases and controls is shown in Appendix 2 (case) and
Appendix 3 (control). Cases were interviewed as soon as possible after notification and
interviews with controls were conducted in March and April 2015. Case interviews
included the national hepatitis A questionnaire in addition to the case control
questionnaire. After completing the interview for the hepatitis A case control study,
controls were asked if they would like to answer additional questions specific for their
Salmonella illness. Responses to questions were entered onto hard copy
questionnaires and were later entered into the NetEpi hepatitis A case control
questionnaire. NetEpi is a password protected online outbreak management database
managed by the Australian Government Department of Health. All QLD data was
downloaded to a comma separated values (.csv) file from NetEpi for analysis.
All data cleaning, recoding and analyses were performed using the statistical package
StataSE 13. The free text descriptive variables entered after an answer of “other” were
visually examined for common responses. New variables to accommodate those
responses were created with responses of yes, no or unknown. These new variables
included a symptom category of “headache”, a food category of “fish” and a package
size and brand of “implicated frozen mixed berries 1kg”.
For ease of interviewing, sub-questions after a response of “no” for having eaten a
particular food type (for example any seafood or any berries) were skipped during the
interview, resulting in missing responses to the specific foods in the category (such as
fish after any seafood, or strawberries after any berries). If a recorded response was no
to the overall category, the responses for the specific foods within the category were
changed from missing to no, allowing a more accurate analysis of the individual
exposures. All other missing data was excluded from the analysis.

331
A new composite variable was created to show those who ate any berry product. This
variable had yes/no/unknown categories. A yes for this exposure category included any
person who reported eating any fresh berry, frozen berry or berry containing food
(dessert or drink).
To assess potential recall bias due to awareness of the national voluntary recall of the
implicated frozen mixed berries, a series of questions were asked to both cases and
controls, including whether they were aware of the food recall, and if they remembered
the brands and types of berries recalled. These questions were included at the end of
the questionnaire to avoid further bias of the exposure data.
The statistical significance of differences in the demographic variables (p-values) was
calculated using Fisher’s Exact method. Odds ratios (ORs) and associated 95%
confidence intervals (CIs) and p-values were calculated for all exposures. ORs were
calculated both with and without controlling for matching variables (age group and
LGA) where possible to adjust for the matched analysis. Fisher’s Exact method was
used to calculate p-values where at least one value was below 5. Chi-square was used
to calculate all other p-values. Associations were considered significant when the CI
did not include 1 and the p-value was less than 0.05. To obtain an estimated OR for
categories where one or more values were zero, a value of one was added to each cell
of the two by two table. In addition, the “exlogistic” command in StataSE13 was used to
conduct an exact logistic regression, providing an OR even when one or more values
are zero.
Results
Descriptive epidemiology A total of 12 cases of hepatitis A that were notified in QLD met the case definition.
Onset of illness ranged from 22 January 2015 to 31 March 2015 (Figure 1). Case ages
ranged from 13 years to 54 years, with a median of 31 years, and ten cases (83%)
were male. Cases were reported from Brisbane (seven cases, 58%), Gold Coast (three
cases, 25%), North QLD (one case, 8%) and Central QLD (one case, 8%).

332
Figure 1: Epidemiological curve of outbreak cases of hepatitis A in QLD by week of symptom
onset, 2015
Case control study Although the study design included matching on age group and LGA, sufficient controls
were unable to be matched to two cases; one child from the Gold Coast and one adult
from North QLD. As matching on sex was not done, and the demographics of this
hepatitis A outbreak skewed towards males, the ratio of males to females in the
controls was different to cases. However, this difference was not significant (Table 1).
Table 1: Comparison of the demographics of cases of hepatitis A in QLD notified between 21
January 2015 and 14 May 2015 with frequency matched controls*
Case (n=12) Control (n=22) p-value
Gender Male 10 (83%) 10 (45%)
0.07 Female 2 (17%) 12 (55%)
Age group* 5-17 years 3 (25%) 5 (23%)
1.0 18-49 years 7 (58%) 13 (59%) 50+ years 2 (17%) 4 (18%)
LGA*
Brisbane 7 (58%) 14 (64%)
1.0 Cairns 1 (8%) 1 (5%) Central QLD 1 (8%) 2 (9%) Gold Coast 3 (25%) 5 (23%)
* Controls were frequency matched (2:1) to cases based on age group and LGA
In the univariable analysis, the only foods that showed a significant association with
illness were those involving frozen berries (Table 2 and Table 3). All cases consumed

333
frozen mixed berries and although the OR and upper bound of the 95% CI were unable
to be calculated, the lower bound for the association was 10.5 with a p-value of less
than 0.001 in unmatched analysis. The estimated OR for frozen mixed berries was 46.8
(95% CI 4.4 – 2094.2, p-value <0.001). The OR calculated by exact logistic regression
was 53.6 (95% CI 7.1 – ∞, p-value <0.001). When adjusted for the gender and age
group, the OR for consumption of frozen mixed berries was 41.9 (95% CI 5.5 – ∞, p-
value <0.001). The adjusted exact OR for Brand 1 (the implicated brand) of frozen
mixed berries was 48.1 (95% CI 6.8 – ∞, p-value <0.001). A similar estimation for
Brand 2 frozen mixed berries resulted in an OR of 6.7 (95% CI 0.7 – ∞, p-value 0.01).
Multivariable analyses on multiple food exposures were not performed because all
exposures with statistically significant increased ORs were subcategories of the same
food and were therefore collinear.
All cases and controls were aware of the recall, and only one case (8%) and eight
controls (or their guardians; 36%) were unable to remember the specific brand.

334
Tabl
e 2:
Uni
varia
ble
anal
ysis
of f
ood
expo
sure
s of
cas
es a
nd c
ontro
ls in
QLD
dur
ing
the
five-
wee
k ex
posu
re p
erio
d. S
igni
fican
t ass
ocia
tions
are
sha
ded
Expo
sure
C
ases
C
ontr
ols
Odd
s R
atio
95
% C
I† p
No.
exp
osed
To
tal
%
No.
exp
osed
To
tal
%
Any
seaf
ood
5 12
42
12
21
57
0.
5 0.
1 - 2
.2
0.41
M
usse
ls*
1 12
8
0 22
0
unsp
ecifi
ed
0.0
- uns
peci
fied
0.35
C
rab
1 12
8
7 22
32
0.
2 0.
0 –
2.0
0.13
Pr
awns
pur
chas
ed c
ooke
d 3
12
25
8 22
36
0.
6 0.
1 - 3
.0
0.53
Pr
awns
pur
chas
ed ra
w*
0 11
0
6 21
29
0.
0 0.
0 –
1.0
0.07
O
yste
rs
1 12
8
3 22
14
0.
6 0.
1 –
6.5
0.67
Fi
sh
1 12
8
7 21
33
0.
2 0.
0 - 1
.7
0.10
Su
shi
3 12
25
14
22
64
0.
2 0.
0 –
0.9
0.03
An
y sm
oked
fish
2
11
18
6 21
29
0.
6 0.
1 –
3.5
0.57
Sa
lmon
2
11
18
6 21
29
0.
6 0.
1 –
3.5
0.57
An
y fr
esh
berr
y 6
12
50
12
22
55
0.8
0.2
– 3.
6 0.
82
Stra
wbe
rrie
s 6
12
50
10
22
46
1.2
0.3
– 5.
5 0.
78
Blu
eber
ries
1 12
8
9 22
41
0.
1 0.
0 - 1
.2
0.06
B
lack
berr
ies
1 12
8
1 21
5
2.0
0.1
– 37
.8
0.65
R
aspb
errie
s 1
12
8 8
22
36
0.1
0.0
- 1.4
0.
08
Froz
en b
errie
s (a
ny)*
12
12
10
0 6
21
29
unsp
ecifi
ed
6.6
- uns
peci
fied
<0.0
01
Froz
en m
ixed
ber
ries*
12
12
10
0 4
21
19
unsp
ecifi
ed
10.5
- un
spec
ified
<0
.001
Fr
ozen
str
awbe
rrie
s 1
11
9 1
21
5 1.
8 0.
1 –
33.4
0.
71
Froz
en b
lueb
errie
s 1
12
8 1
21
5 1.
6 0.
1 –
28.5
0.
75
Froz
en b
lack
berr
ies*
1
11
9 0
21
0 un
spec
ified
0.
0 - u
nspe
cifie
d 0.
34
Ber
ry d
rinks
3
12
25
6 21
27
0.
8 0.
1 –
4.2
0.79
B
erry
des
sert
* 0
12
0 4
20
20
0.0
0.0
- 1.5
0.
27
Fres
h to
mat
oes
9 12
75
16
22
73
1.
2 0.
2 –
6.0
0.85

335
Expo
sure
C
ases
C
ontr
ols
Odd
s R
atio
95
% C
I† p
No.
exp
osed
To
tal
%
No.
exp
osed
To
tal
%
Drie
d to
mat
oes*
0
12
0 3
22
14
0.0
0.0
- 2.3
0.
54
Lettu
ce
11
12
92
20
21
95
0.7
0.0
– 9.
7 0.
75
Sprin
g on
ion
3 9
33
9 20
45
0.
6 0.
1 –
3.3
0.57
* U
nmat
ched
ana
lysi
s is
pre
sent
ed d
ue to
insu
ffici
ent c
ases
and
/or c
ontro
ls to
yie
ld a
val
ue fo
r Odd
s R
atio
and
CI a
fter s
tratif
icat
ion
by m
atch
ed v
aria
bles
† C
I – C
onfid
ence
Inte
rval
Tabl
e 3:
Uni
varia
ble
anal
ysis
of e
xpos
ures
spe
cific
to fr
ozen
mix
ed b
errie
s fo
r cas
es a
nd c
ontro
ls in
QLD
dur
ing
the
five-
wee
k ex
posu
re p
erio
d. S
igni
fican
t
asso
ciat
ions
are
sha
ded
Expo
sure
C
ases
C
ontr
ols
Odd
s R
atio
95
% C
I† p
No.
exp
osed
To
tal
%
No.
exp
osed
To
tal
%
Bra
nd 1
froz
en m
ixed
ber
ries*
12
12
10
0 1
21
5 un
spec
ified
31
.4 -
unsp
ecifi
ed
<0.0
01
Bra
nd 1
1kg
froz
en m
ixed
ber
ries*
10
10
10
0 0
3 0
unsp
ecifi
ed
8.5
- uns
peci
fied
0.00
3 B
rand
2 fr
ozen
mix
ed b
errie
s*
4 12
33
0
21
0 un
spec
ified
2.
4 - u
nspe
cifie
d 0.
01
Bra
nd 3
froz
en m
ixed
ber
ries*
0
12
0 1
21
5 0
0.0
- uns
peci
fied
1 B
rand
4 fr
ozen
mix
ed b
errie
s 1
12
8 2
21
10
0.8
0.0
– 9.
4 0.
88
Bra
nd 5
froz
en m
ixed
ber
ries*
0
12
0 0
21
0 un
spec
ified
un
spec
ified
un
spec
ified
O
ther
bra
nd o
f fro
zen
mix
ed b
errie
s 1
12
8 1
21
5 2.
0 0.
1 –
37.8
0.
6 * U
nmat
ched
ana
lysi
s is
pre
sent
ed d
ue to
insu
ffici
ent c
ases
and
/or c
ontro
ls to
yie
ld a
val
ue fo
r OR
and
CI a
fter s
tratif
icat
ion
by m
atch
ed v
aria
bles
† C
I – C
onfid
ence
Inte
rval

336
Discussion All cases of hepatitis A in QLD that met the case definition for inclusion in the case
control study and 29% of controls consumed frozen mixed berries during their potential
exposure period. The association between illness and consumption of frozen mixed
berries was significant with an OR of 41.9, meaning that the odds of developing a
hepatitis A infection was 41.9 times higher in people who had consumed frozen mixed
berries (of any brand) than those who had not. A similar calculation for the specific
exposure of Brand 1 frozen mixed berries resulted in an estimated OR of 48.1. These
values are comparable to the ORs calculated in the national analysis, 48.7 (95% CI 6.2
– 2073, p-value <0.001) and 440 (95% CI 31.7 – 18531, p-value <0.001) respectively
(M. Easton, unpublished data). These results support the microbiological and case
series evidence (all cases ate the implicated brand of frozen mixed berries) implicating
Brand 1 frozen mixed berries as the source of this outbreak in Queensland. Berries are
a biologically plausible exposure for hepatitis A, as a number of berry-related hepatitis
A outbreaks have been reported worldwide (9-19) and freezing has no impact on
virulence of hepatitis A virus (3).
The questionnaire used in this study included a range of food products that have been
associated with hepatitis A outbreaks in the past, including seafood (6, 8), berries (9-
19) and semi-dried tomatoes (5). However, the potential for experimenter bias was
unavoidable as many questions were focused on berries and berry products, making it
obvious to interviewees that berries were of interest. Given the wide press coverage of
this outbreak from the time the Australian distributor recalled the implicated frozen
mixed berries on 14 February 2015, exposure suspicion bias (21) affecting the memory
recall of consumption of berries was unavoidable for both cases and controls. Indeed,
all cases and controls (or their guardians) in the QLD study were aware of the food
recall. Given this, cases would be more likely to recall eating berries, while controls
would be less likely to recall eating berries, biasing the association away from the null.
The extent of this measurement bias is unknown.
Controls for this study were selected from among those who had been diagnosed with
Salmonella in the two weeks prior to notification of the hepatitis A case to which they
were matched. This source for selection was chosen after long discussions among the
members of OzFoodNet. Although Salmonella controls are convenient, and already
have a valid phone number available through the pathology report (in most cases),
people who have been sick with Salmonella may not be representative of the true
population at risk of developing hepatitis A in this outbreak due to eating patterns
associated with subsequent Salmonella infection which is most commonly egg
associated in Australia (22) as opposed to hepatitis A which is associated with

337
international travel, seafood and berries. This bias was mitigated by only including non-
outbreak cases so infection was more likely attributable to a habitually eaten food
rather than a one-off restaurant meal. Additionally, controls who have recently been
diagnosed with gastroenteritis meet the requirement for control selection from the same
study base as the cases in that they would have been diagnosed and notified to the
national notifiable diseases surveillance system as cases if they had hepatitis A, as
they have a similar health seeking behaviour as cases. This method of control selection
should mitigate selection bias (23).
In order for the period of food exposure for controls to approximately match that of the
case, controls were selected from those within the same age group and LGA who were
notified in a two-week period before the matching case. This time period was used so
that the period of food consumption among the controls was similar to the period of
food consumption for the case, therefore matching the same period of risk. The period
of food consumption surveyed was five weeks. Since interviews were conducted during
late March and early April, and some cases and controls were asked for food histories
from early December 2014, four months earlier, recall bias was considered to be an
issue. However, as both cases and controls were sick after the period of exposure,
both groups will have greater recall of the foods eaten prior to their illness than people
who have not recently been ill, particularly for foods they think were responsible for
their illness so the bias should be non-differential.
An advantage of selecting controls from among people who have been ill with a
different disease is that they were more willing to participate than people who have not
been ill, and were particularly eager to talk about their illness. The information collected
about their Salmonella illness provides some insight into sporadic Salmonella and has
been recorded in NetEpi. Similarly, the advantage of a high profile outbreak such as
this is that participants are more likely to understand why the study is being done.
A possible source of measurement bias in this study was interviewer bias. Cases were
interviewed by staff from their local public health unit, and controls were interviewed by
three MAE students. However, the questionnaire was designed with defined wording of
questions so interviewers were less likely to ask leading questions.
A limitation of this study was the difficulty conducting matched analysis due to low
numbers of participants in the study combined with universal exposure of all cases to
the implicated frozen mixed berries. Analysing data without adjusting for matching in a
frequency matched case control study will bias the OR towards the null (24). However,
the unmatched association between the implicated frozen mixed berries and illness is
large; suggesting that even with confounders unaccounted for the berries would still be
associated with illness.

338
In conclusion, this case control study was able to identify a significant association
between illness and consumption of the implicated frozen mixed berries as the likely
source of hepatitis A infection for the Queensland sub-analysis for the multi-
jurisdictional outbreak in the first half of 2015.
References 1. NNDSS Annual Report Writing Group. Australia's notifiable disease status, 2012: Annual report of the National Notifiable Diseases Surveillance System. Communicable Diseases Intelligence Quarterly Report. 2015 Mar;39(1):E46-E136. 2. Fiore AE. Hepatitis A transmitted by food. Clinical Infectious Diseases. 2004 Mar 1;38(5):705-15. 3. Butot S, Putallaz T, Sanchez G. Effects of sanitation, freezing and frozen storage on enteric viruses in berries and herbs. International Journal of Food Microbiology. 2008 Aug 15;126(1-2):30-5. 4. Heymann DL. Control of Communicable Diseases Manual. 19 ed.; 2008. 5. Donnan EJ, Fielding JE, Gregory JE, Lalor K, Rowe S, Goldsmith P, et al. A multistate outbreak of hepatitis A associated with semidried tomatoes in Australia, 2009. Clinical Infectious Diseases. 2012 Mar;54(6):775-81. 6. Conaty S, Bird P, Bell G, Kraa E, Grohmann G, McAnulty JM. Hepatitis A in New South Wales, Australia from consumption of oysters: the first reported outbreak. Epidemiology and Infection. 2000 Feb;124(1):121-30. 7. Dienstag JL, Gust ID, Lucas CR, Wong DC, Purcell RH. Mussel-associated viral hepatitis, type A: serological confirmation. Lancet. 1976 Mar 13;1(7959):561-3. 8. Lee D, Ashwell M, Ferson M, Beer I, McAnulty J. Hepatitis A outbreak associated with a Mothers' Day 'Yum Cha' meal, Sydney, 1997. New South Wales Public Health Bulletin. 2004 Jan-Feb;15(1-2):6-9. 9. Calder L, Simmons G, Thornley C, Taylor P, Pritchard K, Greening G, et al. An outbreak of hepatitis A associated with consumption of raw blueberries. Epidemiology and Infection. 2003 Aug;131(1):745-51. 10. Chiapponi C, Pavoni E, Bertasi B, Baioni L, Scaltriti E, Chiesa E, et al. Isolation and genomic sequence of hepatitis A virus from mixed frozen berries in Italy. Food and Environmental Virology. 2014 Sep;6(3):202-6. 11. Fitzgerald M, Thornton L, O'Gorman J, O'Connor L, Garvey P, Boland M, et al. Outbreak of hepatitis A infection associated with the consumption of frozen berries, Ireland, 2013--linked to an international outbreak. Eurosurveillance. 2014;19(43). 12. Gillesberg Lassen S, Soborg B, Midgley SE, Steens A, Vold L, Stene-Johansen K, et al. Ongoing multi-strain food-borne hepatitis A outbreak with frozen berries as suspected vehicle: four Nordic countries affected, October 2012 to April 2013. Eurosurveillance. 2013;18(17):20467. 13. Hutin YJ, Pool V, Cramer EH, Nainan OV, Weth J, Williams IT, et al. A multistate, foodborne outbreak of hepatitis A. National Hepatitis A Investigation Team. The New England Journal of Medicine. 1999 Feb 25;340(8):595-602. 14. Niu MT, Polish LB, Robertson BH, Khanna BK, Woodruff BA, Shapiro CN, et al. Multistate outbreak of hepatitis A associated with frozen strawberries. The Journal of Infectious Diseases. 1992 Sep;166(3):518-24. 15. Ramsay CN, Upton PA. Hepatitis A and frozen raspberries. Lancet. 1989 Jan 7;1(8628):43-4.

339
16. Reid TM, Robinson HG. Frozen raspberries and hepatitis A. Epidemiology and Infection. 1987 Feb;98(1):109-12. 17. Rizzo C, Alfonsi V, Bruni R, Busani L, Ciccaglione A, De Medici D, et al. Ongoing outbreak of hepatitis A in Italy: preliminary report as of 31 May 2013. Eurosurveillance. 2013;18(27). 18. Collier MG, Khudyakov YE, Selvage D, Adams-Cameron M, Epson E, Cronquist A, et al. Outbreak of hepatitis A in the USA associated with frozen pomegranate arils imported from Turkey: an epidemiological case study. The Lancet Infectious Diseases. 2014 Oct;14(10):976-81. 19. Swinkels HM, Kuo M, Embree G, Fraser Health Environmental Health Investigation T, Andonov A, Henry B, et al. Hepatitis A outbreak in British Columbia, Canada: the roles of established surveillance, consumer loyalty cards and collaboration, February to May 2012. Eurosurveillance. 2014;19(18). 20. Department of Health. Hepatitis A National Guidelines for Public Health Units. 2009 [updated 2009; cited 15 November 2015]; Available from: http://www.health.gov.au/internet/main/publishing.nsf/Content/FB28A405CBF6E64ECA257BF0001DAB33/$File/hepa-song.pdf. 21. Delgado-Rodriguez M, Llorca J. Bias. Journal of Epidemiology and Community Health. 2004 Aug;58(8):635-41. 22. OzFoodNet Working Group. Monitoring the incidence and causes of diseases potentially transmitted by food in Australia: Annual report of the OzFoodNet network, 2011. Communicable Diseases Intelligence Quarterly Report. 2015;39(2):E236-64. 23. Grimes DA, Schulz KF. Compared to what? Finding controls for case-control studies. Lancet. 2005 Apr 16-22;365(9468):1429-33. 24. Aschengrau A, Seage GR. Essentials of Epidemiology in Public Health. 2 ed.: Jones and Bartlett; 2008.

340
Appendix 1: Lay summary for OzFoodNet website Outbreak of hepatitis A associated with imported mixed berries,
Australia 2015
OzFoodNet is a national network of people who investigate foodborne disease
outbreaks (epidemiologists). On 12 February 2015, OzFoodNet in Victoria reported
that three people sick with locally acquired hepatitis A had all eaten the same brand of
imported frozen mixed berries in the months before they became ill. These people also
reported no other common exposure that could explain the source of their infection.
Hepatitis A is a gastrointestinal illness caused by exposure to food or drink
contaminated with the hepatitis A virus, but it takes 15 to 50 days after consumption of
the contaminated food before people become sick. Transmission from person to
person can also occur. Common symptoms of hepatitis A include fever, nausea,
abdominal discomfort and jaundice (yellowing of the eyes and skin). The national
guidelines that health departments follow to investigate and to respond to people with
hepatitis A infections can be found here:
http://www.health.gov.au/internet/main/publishing.nsf/Content/cdna-song-hepa.htm
Since the successful introduction of the hepatitis A vaccine in the late 1990s, it is very
rare to become infected with hepatitis A in Australia. For further information on
vaccination for hepatitis A see:
http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/Handboo
k10-home~handbook10part4~handbook10-4-4
Most Australian residents with hepatitis A were infected during recent overseas travel.
Previous foodborne hepatitis A outbreaks in Australia have been linked to
contaminated foods, including seafood and semi-dried tomatoes. All people reported to
health departments in Australia with hepatitis A are interviewed about risk factors
including overseas travel and about specific foods they may have eaten that were
identified as the cause of previous outbreaks. Consumption of berries was recently
added to the list of foods asked about at these interviews as they have been identified
as a cause of several hepatitis A outbreaks overseas. It is very unusual for three
people with hepatitis A who hadn’t been overseas to report eating the same brand of
frozen mixed berries before they became sick. This made investigators suspect that
berries were the cause of their infection.
On 13 February 2015, OzFoodNet epidemiologists in New South Wales reported that a
person with hepatitis A had also eaten the implicated frozen mixed berries.
The Victorian Department of Health and Human Services then recommended that a
consumer level recall of the berries should take place, and on 14 February 2015 the

341
parent company began a nationwide voluntary recall of the frozen mixed berries and
several related products that were packed in the same factories.
As cases had now been identified in two different states, OzFoodNet commenced a
nationwide epidemiological investigation, known as a multi-jurisdictional outbreak
investigation or MJOI. Over the next few months, several different types of
investigations were undertaken to identify the cause of the increase in people
diagnosed with hepatitis A, including:
Testing faeces (poo) specimens in a pathology laboratory is the way most
gastrointestinal diseases including hepatitis A are diagnosed. Faeces
specimens were provided by the people with hepatitis A, and hepatitis A virus
was detected in the specimens. Public health reference laboratories tested the
genetic material of the hepatitis virus that was found and it became quickly
apparent that these hepatitis A virus specimens were indistinguishable. This
means that it is highly likely that the cause of illness in all of the people
diagnosed with hepatitis A came from the same source.
If they hadn’t already, OzFoodNet investigators in all states and territories re-
interviewed people diagnosed with hepatitis A that had been reported in the
months before the recall to find out if they had eaten berries, even if they had
been overseas. These people had been previously interviewed about other
foods consumed and overseas travel during the period two to seven weeks
before their illness.
An open package of the implicated frozen mixed berries that was in the freezer
of one of the outbreak cases was obtained, and hepatitis A virus was detected
in the berries. The genetic material of this virus was indistinguishable to that
found in the faeces of someone sick in the outbreak. This means that it is likely
that the illness in the people was from the contaminated product.
Hepatitis A virus was also detected in an unopened bag of the implicated frozen
mixed berries that had been recalled. Unfortunately, there was not enough virus
to determine if this virus was the same as the viruses from the people with
hepatitis A. As this was an unopened package of berries, the virus was present
in the berries before the package was sealed and was more evidence that
contaminated berries were the cause of the outbreak. Food products should
have no hepatitis A in them.
OzFoodNet performed a case control study which measures the risk associated
with eating specific foods and getting infected with hepatitis A virus. In this case
control study, the same series of questions about foods eaten were asked to
both cases (people diagnosed with hepatitis A) and controls (people without

342
hepatitis A). The responses were compared to identify foods that were more
commonly eaten by people with hepatitis A. This study showed that the odds of
contracting a hepatitis A infection was more than 400 times higher in people
who ate the implicated frozen mixed berries than for people who did not eat
them. No associations were identified between illness and any other foods.
When the MJOI ended on 27 May 2015, a total of 33 people across six states
and territories had the outbreak strain of hepatitis A. Of those, 28 people had
eaten the implicated frozen mixed berries in the 15-50 days before they became
ill. Of the seven people who couldn’t remember eating the frozen mixed berries,
three people probably got their infection from a person who ate the frozen
mixed berries. The source of illness for the remaining four people was unable to
be determined.
The combination of these investigations provides compelling evidence that the
implicated frozen mixed berries were the source of this outbreak of hepatitis A. The
contamination occurred during growing, harvesting or packaging of the berries most
likely due to a breakdown in procedure. It is likely that the rapid recall of this product
prevented more people becoming infected.

343
Appendix 2: Case questionnaire Hepatitis A Case Control Study
Case questionnaire – to be completed for cases who are still eligible for the case control study after completing sections 1-6 of the standard Hep A questionnaire.
Jurisdictional Case number: ______________________ Date of case interview: ___ / ___ /____
Age ____ Sex: M / F
Local Government Area/PHU: ____________ Post Code: _______
Name and telephone details………………………………………………………………………
Exclusion Criteria Summary– Please tick if Excluded
Unable to speak English or answer questions appropriately
Travelled overseas in the exposure period
Spent > 1 year in the first 5 years of life in a country on Appendix 1
Close contact with a person known or suspected to have Hepatitis A
Unable to provide date of onset of illness or jaundice
Case: Eligible Ineligible
Eligibility questions – Please note even if the case is ineligible for the CC study, please complete this questionnaire as the food questions have been removed from the standard questionnaire

344
1. What was the date first symptom? (Transcribe from previous questionnaire if already interviewed) ___ / ___ / ______
Exposure period: ___ / ___ / ______ to ___ / ___ / _______
(Calculate 15 – 50 days prior to answer to question 1)
2. Have you travelled overseas during the exposure period (as above)?
Yes Travelled from : ___ / ___ / ______ to ___ / ___ / ______
Country/ies visited: ______________________________
No
Unknown
3. Have you had household/close contact with any persons known or suspected to have Hepatitis A during your exposure period (as above)?
Yes name of person and relationship to case………………………………………….
No
Unknown
4. Did you live in another country other than Australia for more than 1 year in the first 5 years of your life?
No Yes, country: ______________________________
SECTION 2: FOOD EXPOSURES
I would like to ask you some questions relating to the foods you ate during the period of time before you became unwell. This time period is:
From ____/_____/___ to ____/_____/____ As this is a long period of time you may like to get a calendar or diary to help you remember what foods you may have been eating at this time.
1. During this time did you eat any type of fresh seafood?
Yes
No proceed to Q8

345
Unknown
2. Did you consume mussels?
Yes Were the mussels raw? Yes No Unknown
No
Unknown
3. Did you consume crab?
Yes No Unknown
4. Did you consume prawns (purchased cooked)?
Yes No Unknown
5. Did you consume prawns (purchased raw)?
Yes No Unknown
6. Did you consume oysters?
Yes Were the oysters raw? Yes No Unknown
No
Unknown
7. Did you consume any other seafood?
Yes Please specify the type ……………………………………………..
No
Unknown
8. Did you consume sushi/sashimi?
Yes
No
Unknown
9. Did you consume smoked fish/seafood of any type?
Yes
No proceed to Q12
Unknown
10. Did you consume smoked salmon?
Yes No Unknown
11. Did you consume other smoked fish/seafood?

346
Yes Please specify the type ………………………………..
No
Unknown
12. During this period did you consume fresh berries of any type (eaten at home and/or in a restaurant or cafe)?
Yes
No proceed to Q18
Unknown
13. Did you consume fresh strawberries?
Yes No Unknown
14. Did you consume fresh blue berries?
Yes No Unknown
15. Did you consume fresh blackberries?
Yes No Unknown
16. Did you consume fresh raspberries?
Yes No Unknown
17. Did you consume any other fresh berries?
Yes Please specify the type ………………………………………..
No
Unknown
18. Did you consume at home, any commercially packaged frozen berries of any type (this includes frozen berries which you may have added to a drink such as a smoothie or milkshake)?
Yes
No proceed to Q39
Unknown
19. Did you consume frozen mixed berries?
Yes
No proceed to Q 23
Unknown
20. Was the brand of these frozen mixed berries:

347
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size…………………………………………………………………
21. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen mixed berries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
22. Did you consume these frozen mixed berries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown 23. Did you consume frozen strawberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 27
Unknown
24. Was the brand of these frozen strawberries:
Coles ? Yes No Unknown
Woolworths ? Yes No Unknown
Nannas ? Yes No Unknown
Creative Gourmet ? Yes No Unknown
Sara Lea ? Yes No Unknown
Other ? Yes No Unknown Please specify brand……..

348
Please specify packet size………………………………………………………………………………
25. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen strawberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
26. Did you consume these frozen strawberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
27. Did you consume frozen blueberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 31
Unknown
28. Was the brand of these frozen blueberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size………………………………………………………………
29. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen blueberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown

349
Daily? Yes No Unknown
30. Did you consume these frozen blueberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
31. Did you consume frozen blackberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 35
Unknown
32. Was the brand of these frozen blackberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size…………………………………………………………………
33. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen blackberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily ? Yes No Unknown
34. Did you consume these frozen blackberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
35. Did you consume frozen raspberries? (not as an ingredient of mixed berries)
Yes

350
No proceed to Q 39
Unknown
36. Was the brand of these frozen raspberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size…………………………………………………………………
37. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen raspberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily ? Yes No Unknown
38. Did you consume these frozen raspberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
39. Is there a child/children 5 years of age living in the household?
Yes (if more than one child 5 years, please note here ………………………….)
No proceed to Q43
Unknown
40. Did this child/any of these children consume any frozen berries at any time in the three months prior to your symptoms?
Yes
No proceed to Q44
Unknown

351
41. What type of frozen berry would they have consumed?
Mixed berries? Yes No Unknown
Strawberries? Yes No Unknown
Blueberries? Yes No Unknown
Blackberries? Yes No Unknown
Raspberries? Yes No Unknown
42. Would this child/these children have consumed the frozen berries raw (eg without cooking them in a sauce, dessert or muffin etc)?
Yes No Unknown
43. Was the brand of these frozen berries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size…………………………………………………………………
44. Did you consume any drinks such as smoothies or milk shakes or yoghurt prepared outside the home (such as in a juice bar or a café) where any type of berry was an ingredient?
Yes provide details of the drink consumed …………………………………………
No
Unknown
45. Did you consume any uncooked desserts such as mousse or desserts with an uncooked topping
(such as pavlova) prepared outside the home (eg in a café or restaurant) where any type of berry was an ingredient?
Yes provide details of the dessert consumed ……………………………………………
No
Interviewer note: If case answered yes please specify the name and address of premises.

352
Unknown
46. During this time did you eat any type of fresh tomatoes?
Yes
No proceed to Q48
Unknown
47. Were these tomatoes:
Cherry tomatoes? Yes No Unknown
Roma tomatoes? Yes No Unknown
Regular round? Yes No Unknown
Other? Yes No Unknown - Please specify the type …………………
48. During this time did you eat any type of dried or semi dried tomatoes?
Yes
No proceed to Q50
Unknown
49. Were these dried tomatoes:
Sun dried ? Yes No Unknown
Semi dried ? Yes No Unknown
Other ? Yes No Unknown
50. During this time did you eat any type of lettuce?
Yes
No
Unknown
51. During this time did you eat any spring onions?
Yes
No
Interviewer note: If case answered yes please specify the name and address of premises.

353
Unknown
The last part of this section is to ask you a few questions about the current national recall of frozen berries:
Are you aware of the recent national recall of frozen berries?
Yes
No
Unsure
Do you remember the brands of frozen berries that were included in the recall?
Yes Please specify...
No
Unsure
Do you remember what type of berries were included in the recall?
1. Blackberries
2. Blueberries
3. Strawberries
4. Raspberries
5. Mixed berries
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Where did you first learn about the recall of berries?
1. Newspaper
2. Website
3. Facebook
4. Twitter
5. Television
6. Radio
7. Company web
8. Friends
9. Other
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure Please Specify………….
Interviewer note: If case answered yes to consuming any frozen berries please ask whether they have any frozen berries left at home that could be collected for testing. Details here

354
Continue with sections 7b -10 of the standard Hep A questionnaire if not previously interviewed or thank the case for their time if questionnaire already complete.

355
Appendix 3: Control questionnaire Hepatitis A Case Control Study
Control questionnaire
Corresponding Jurisdictional Case number: _____________ Date of case interview: ___ / ___ /____
Control ID ___________________________ Date control notified ___ / ___ /____
Control Age ____ Control sex: M / F
Local Government Area/PHU: ____________ Post Code: _______
Date of control interview: ___ / ___ /______
Name and telephone contact for control………………………………………………………………………
Exclusion Criteria Summary– Please tick if Excluded
Previous diagnosis of Hepatitis A
Has received two vaccinations against Hepatitis A
Unable to speak English or answer questions appropriately
Travelled overseas in the 2 months prior to notification
Spent > 1 year in the first 5 years of life in a country which is on the exclusion list
Close contact with a person known or suspected to have Hepatitis A
Control: Eligible Ineligible

356
Preamble
The health department has been notified (by doctor/laboratory) that you have had a recent Salmonella infection and visited Dr .................. around ....../....../.......(specimen date). At the present time, your type of Salmonella is not part of any recognised outbreak that the health department is investigating. We would like to speak to you about your Salmonella infection but firstly we would like you to assist us with another outbreak due to hepatitis A. We are asking people who have not had hepatitis A to participate in this study so that we can compare them with people who have had hepatitis A. This study is being conducted under the “jurisdictional” health act.
We would like to ask you questions about some foods you have may have eaten in the 5 weeks before the onset of your Salmonella illness. The questions should take about 15 minutes and you can stop at any time if you want to. Your participation is voluntary and all responses are totally confidential. There will be no identifying information kept on you for this study.
Do you agree to participate?
Do you have the time right now to answer these questions?
If NO, arrange an alternative time to phone back to conduct the interview: Date / / Time_______
If YES, continue:
Eligibility questions:
1. Did you live in another country other than Australia for more than 1 year in the first 5 years of your life?
No Yes , Country: ______________________________
Interviewer note: If control lived in a country on appendix 1 of the protocol list do
not complete remainder of this questionnaire – cease interview here.
2. Have you travelled overseas during the 2 months prior to __/__/__(control’s notification date)?
Yes No Unknown
Interviewer note: If control answers yes do not complete remainder of this
questionnaire – cease interview here
3. Have you previously been diagnosed by a doctor as having Hepatitis A or do you recall having symptoms of jaundice (yellow skin/eyes)?
Yes No Unknown
Verbal consent given for interview Yes No

357
Interviewer note: If control answers yes do not complete the remainder of this
questionnaire – cease interview here
4. Have you received two vaccinations for Hepatitis A in the past? Vaccinations for Hepatitis A are called Havrix or Twinrix and are not part of the normal vaccination program.
Yes No Unknown
Interviewer note: If control answers yes do not complete the remainder of this
questionnaire – cease interview here
5. Have you received NHIG in the 2 months prior to the onset of your Salmonella illness.
Yes No Unknown
Interviewer note: If control answers yes do not complete the remainder of this
questionnaire – cease interview here
6. Have you had household/close contact with any persons known or suspected to have Hepatitis A during the period __/__/__ to __/__/__
Yes No Unknown
Interviewer note: If control answers yes do not complete the remainder of this
questionnaire - cease interview here
FOOD EXPOSURES
I would like to ask you some questions relating to the foods you ate during the 5 week period before your Salmonella illness. So, before I commence the questionnaire, I need to ask the onset date of your Salmonella illness so we can calculate this 5 week period.
What was the onset date of your diarrhoea? ___/___/___
So, the 5 week time period I will be asking you about is from ___/___/___ to ___/___/___ (onset date of diarrhoea). As this is a long period of time you may like to get a calendar or diary to help you remember what foods you may have been eating at this time.
52. During this time did you eat any type of fresh seafood ?
Yes
No proceed to Q8
Unknown
53. Did you consume mussels?

358
Yes Were the mussels raw? Yes No Unknown
No
Unknown
54. Did you consume crab?
Yes No Unknown
55. Did you consume prawns (purchased cooked)?
Yes No Unknown
56. Did you consume prawns (purchased raw)?
Yes No Unknown
57. Did you consume oysters?
Yes Were the oysters raw? Yes No Unknown
No
Unknown
58. Did you consume any other seafood?
Yes Please specify the type ……………………………………………..
No
Unknown
59. Did you consume sushi/sashimi?
Yes
No
Unknown
60. Did you consume smoked fish/seafood of any type?
Yes
No proceed to Q12
Unknown
61. Did you consume smoked salmon?
Yes No Unknown
62. Did you consume other smoked fish/seafood?
Yes Please specify the type …………………………………………..

359
No
Unknown
63. During this period did you consume fresh berries of any type (eaten at home and/or in a restaurant or cafe)?
Yes
No proceed to Q18
Unknown
64. Did you consume fresh strawberries?
Yes No Unknown
65. Did you consume fresh blue berries?
Yes No Unknown
66. Did you consume fresh blackberries?
Yes No Unknown
67. Did you consume fresh raspberries?
Yes No Unknown
68. Did you consume any other fresh berries?
Yes Please specify the type ……………………………………………..
No
Unknown
69. Did you consume at home, any commercially packaged frozen berries of any type (this includes frozen berries which you may have added to a drink such as a smoothie or milkshake)?
Yes
No proceed to Q39
Unknown
70. Did you consume frozen mixed berries?
Yes
No proceed to Q23

360
Unknown
71. Was the brand of these frozen mixed berries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other ? Yes No Unknown Please specify brand……..
Please specify packet size………………………………………………………………………
72. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen mixed berries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
73. Did you consume these frozen mixed berries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
74. Did you consume frozen strawberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 27
Unknown
75. Was the brand of these frozen strawberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..

361
Please specify packet size………………………………………………………………………
76. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen strawberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
77. Did you consume these frozen strawberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
78. Did you consume frozen blueberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 31
Unknown
79. Was the brand of these frozen blueberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size………………………………………………………………
80. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen blueberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown

362
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
81. Did you consume these frozen blueberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
82. Did you consume frozen blackberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 35
Unknown
83. Was the brand of these frozen blackberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size……………………………………………………………………
84. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen blackberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
85. Did you consume these frozen blackberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown

363
86. Did you consume frozen raspberries? (not as an ingredient of mixed berries)
Yes
No proceed to Q 39
Unknown
87. Was the brand of these frozen raspberries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size……………………………………………………………………
88. During the time period we are interested in (from ____/_____/___ to ____/_____/____) which of the following categories best describes your consumption pattern for these frozen raspberries:
Less than once a month? Yes No Unknown
Once or twice a month? Yes No Unknown
Once or twice per week? Yes No Unknown
Three to five times a week? Yes No Unknown
Daily? Yes No Unknown
89. Did you consume these frozen raspberries raw (eg without cooking them in a
sauce, dessert or muffin etc)?
Yes No Unknown
90. Is there a child/children 5 years of age living in the household?
Yes (if more than one child 5 years, please note here ……………………………..)
No proceed to Q44
Unknown
91. Did this child/any of these children consume any frozen berries at any time in the three months prior to your symptoms?

364
Yes
No proceed to Q44
Unknown
92. What type of frozen berry would they have consumed?
Mixed berries? Yes No Unknown
Strawberries? Yes No Unknown
Blueberries? Yes No Unknown
Blackberries? Yes No Unknown
Raspberries? Yes No Unknown
93. Would this child/these children have consumed the frozen berries raw (eg without cooking them in a sauce, dessert or muffin etc)?
Yes No Unknown
94. Was the brand of these frozen berries:
Coles? Yes No Unknown
Woolworths? Yes No Unknown
Nanna’s? Yes No Unknown
Creative Gourmet? Yes No Unknown
Sara Lee? Yes No Unknown
Other? Yes No Unknown Please specify brand……..
Please specify packet size…………………………………………………………………
95. Did you consume any drinks such as smoothies or milk shakes or yoghurt prepared outside the home (such as in a juice bar or a café) where any type of berry was an ingredient?
Yes provide details of the drink consumed ……………………………………
No
Unknown
96. Did you consume any uncooked desserts such as mousse or desserts with an uncooked topping (such as pavlova) prepared outside the home (eg in a café or restaurant) where any type of berry was an ingredient?
Yes provide details of the dessert consumed …………………………………
No
Unknown

365
97. During this time did you eat any type of fresh tomatoes?
Yes
No proceed to Q48
Unknown
98. Were these tomatoes:
Cherry tomatoes? Yes No Unknown
Roma tomatoes? Yes No Unknown
Regular round? Yes No Unknown
Other? Yes No Unknown - Please specify the type………………
99. During this time did you eat any type of dried or semi dried tomatoes?
Yes
No proceed to Q50
Unknown
100. Were these dried tomatoes:
Sun dried? Yes No Unknown
Semi dried? Yes No Unknown
Other? Yes No Unknown
101. During this time did you eat any type of lettuce?
Yes
No
Unknown
102. During this time did you eat any spring onions?
Yes
No
Unknown

366
The last part of this section is to ask you a few questions about the current national recall of frozen berries:
Are you aware of the recent national recall of frozen berries?
Yes
No
Unsure
Do you remember the brands of frozen berries that were included in the recall?
Yes Please specify ..
No
Unsure
Do you remember what type of berries were included in the recall?
6. Blackberries
7. Blueberries
8. Strawberries
9. Raspberries
10. Mixed berries
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Where did you first learn about the recall of berries?
10. Newspaper
11. Website
12. Facebook
13. Twitter
14. Television
15. Radio
16. Company web
17. Friends
18. Other
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure
Yes No Unsure Please specify………
Please proceed with the usual jurisdictional investigation of the person’s Salmonella infection, if they are agreeable.

367
Chapter 7 Teaching experience

368
Introduction This chapter outlines my teaching experiences during my Master of Philosophy in
Applied Epidemiology (MAE). The first section is a record of my ‘Lessons from the
Field’, with suggested answers shown in orange text. As most people in my cohort
have little laboratory experience, I chose new technologies that are currently being
introduced into public health pathology laboratories nationwide, including culture
independent diagnostic testing and whole genome sequencing, as my topic. These
new techniques will have a large impact on epidemiology through changes in the
sensitivity of detection of pathogens, and through potential loss of subtyping
information, as discussed in Chapter 4. Through developing the instructions for my
lessons from the field, I learned the importance of focusing questions and giving clear
and easy to follow instructions. It can be hard to make something that you are very
familiar with simple enough for inexperienced people to follow.
The second section of this chapter shows the activity and slides used for teaching the
first year MAE cohort about measures of test performance conducted in March 2015.
As this teaching session was prepared and conducted in a group of three people, I
learned about cooperation and sharing of responsibilities. The three of us have
different strengths and we were able to plan our session to take advantage of those
strengths. The feedback from all the students involved was positive, which showed the
benefit of having an interesting and engaging presentation and then an activity at the
end of the session. Our session was last, and started late, but the students were happy
to continue the activity into their lunch break demonstrating their interest. Making the
activity fun also helped cement the concepts they learned during the session.

369
Lessons from the Field Lesson from the field 8 – Laboratory testing into the future
Learning Objectives After completing this exercise, you should be able to:
Explain the new laboratory methods (culture independent diagnostic testing -
CIDT) that have been recently introduced into diagnostic pathology laboratories
and the new methods of the future (whole genome sequencing (WGS) and
metagenomics).
Describe why CIDT is desired by laboratories, and why epidemiologists may be
concerned.
Describe how WGS will enhance epidemiological investigations.
Use GenBank to find information and sequences for communicable diseases.
Part 1 – the CIDT “dark ages”:
Laboratory testing for infectious diseases in Australia and worldwide is currently
undergoing a series of changes in response to the availability of changing
technologies. As Zoe showed in her LFF, typing of organisms (for example MLVA)
allows for greater discrimination between similar isolates than is possible with
traditional phage typing or serotyping methods. Typing assists investigators to assess
which cases in an outbreak are related to a common source, i.e. which cases are
outbreak cases and which are unrelated sporadic cases.
However, technology has advanced again, onwards from MLVA, as it is wont to do.
Many laboratories across Australia have introduced culture independent methods
(CIDT) for testing of common pathogens. In Australia, this predominantly means PCR
testing directly from clinical samples. As the name implies, these techniques don’t
require growth of a pure culture of the pathogen. For now, laboratories are still
The LFF teleconference will be conducted on Wednesday 16 September 2015 between 10:00 – 11:00 AEST. To join the teleconference, dial 1800 047396 and then enter the conference PIN code
24779149#. If you have any trouble please call me on 0415 975 120 or email me on
Please save your responses to the questions in a word file and send back to
[email protected] by COB Friday 11 September 2015.

370
performing cultures, either concurrently with CIDT testing, or reflexively, meaning for
PCR positive samples only.
Read the article “Effect of culture-independent diagnostic tests on future emerging
infections program surveillance” by Langley et al. and answer the following questions
shown in bold – dot point and short responses are fine:
Q1. Why might laboratories and clinicians prefer to use CIDT methods like PCR?
a. Faster b. More sensitive, especially when antimicrobial treatment has begun c. Less technical experience required d. Can detect polymicrobial infections e. Safer than culturing dangerous organisms f. Some organisms are difficult or unable to be cultured g. Can quantitate pathogen load h. Cheaper after initial cost
Q2. Why would epidemiologists prefer culture (and subsequent culture-requiring typing methods like MLVA) to be continued?
a. Outbreak detection may require subtyping information, for example, MLVA for Salmonella can distinguish between baseline cases and an outbreak
b. Can detect emergence of new strains’ c. Antimicrobial resistance pattern tests currently require culture d. PCR can’t detect the difference between dead and alive organisms e. Minor molecular mutations may result in decreased sensitivity of
CIDT Q3. What might it mean if the results between methods are discordant – i.e.
PCR positive, culture negative (other than false positives)? a. PCR is detecting dead organisms b. Some organisms don’t culture easily or at all, but CIDT will detect
them c. Polymicrobial infection or normal flora may outcompete the
pathogen in culture d. Antimicrobial therapy has made the pathogen unculturable
Q4. Look at Table 1 showing Ralstonia isolates as identified by PCR and describe what you think might be going on in terms of outbreaks (i.e. which cases might be linked, which might not – ignore any thoughts of contamination with multiple different species):

371
a. Case numbers 3 to 9 are probably associated with propofol – a multijurisdictional outbreak with cases in QLD, SA and VIC
Table 1: Species of Ralstonia identified by PCR, isolated from cases of bacteraemia
and a sample of the drug Propofol
Case number Propofol exposure Hospital Species
1 Yes QLD2 R. insidiosa
2 Yes SA1 R. pickettii
3 Yes QLD1 R. mannitolilytica
4 Yes QLD1 R. mannitolilytica
5 Yes QLD3 R. mannitolilytica
6 Yes QLD3 R. mannitolilytica
7 Yes SA1 R. mannitolilytica
8 Yes SA2 R. mannitolilytica
9 Yes VIC R. mannitolilytica
Propofol isolate NA NA R. mannitolilytica
Part 2 – the WGS “age of enlightenment”
The next step forward in laboratory testing is currently being planned and is beginning
to be implemented around the world. Whole genome sequencing (WGS) is, as the
name implies, sequencing of the whole genome of an organism. While sequencing
technologies have been around for a long time, recent advances have made it cheaper
and quicker to sequence large amounts of DNA or RNA in a single analysis, allowing
multiple entire bacterial genomes to be sequenced in only hours. Of course, as with
everything in life, sequencing is not going to solve all our problems without adding new
ones. WGS currently requires laboratories to obtain a culture, thus losing the gains in
sensitivity associated with CIDT.
Read the article “Stopping outbreaks with real-time genomic epidemiology” by Tang et
al. and answer the following questions. Again, dot point answers are fine:
Q5. What are some advantages of WGS, particularly in relation to CIDT? a. Is able to be used to determine some subtypes and antimicrobial
sensitivities. b. Able to discriminate between related strains and not related strains
for outbreak detection

372
c. Can track origin and transmission dynamics of outbreaks by following the evolution of the pathogen
d. The sequence of an organism is absolute – techniques for analysis may change (e.g. which gene to compare, how to define closely related isolates) but the sequence will always be the same allowing re-analysis of old sequences and comparison with new isolates as techniques change
Q6. Can you think of any disadvantages? a. Currently still requires a culture – so not as sensitive as CIDT b. Slow and expensive – for now c. Technically challenging d. Lots of data to store – need changes in data storage practices
Now you are going to have a look at some sequencing data that is shared publicly
online. There are three main databases that are widely used for sequence data
storage; The European Molecular Biology Laboratory (EMBL), DNA Data Bank of
Japan (DDBJ) and GenBank. They were developed separately back before the internet
was common, but are now all are linked so that if a sequence is submitted to one, it
shows up in all. GenBank is associated with National Center for Biotechnology
Information (NCBI) and PubMed, which I know you are all familiar with, so we will play
with it.
1. Go to PubMed (http://www.ncbi.nlm.nih.gov/pubmed) and click on the drop
down next to the search box.
2. Select “nucleotide” in the top left hand categorical drop down menu (as shown
in the screenshot below). This will allow you to search all nucleotide sequences
in the database.

373
3. Searching GenBank uses the same rules as searching on PubMed. Search for
Ebola virus sequences, from Sierra Leone in 2014 (Ebola AND “Sierra Leone”
AND 2014).
4. Click on the link Zaire ebolavirus isolate Ebola virus/H.sapiens-
wt/SLE/2014/Makona-NM042.3, complete genome, accession KM233118.1 (it
should be at or near the top, depending how many new sequences have been
added since I wrote this! If you are having problems finding this entry, you can
search using the unique accession number) and have a look at the entry. This
is a beautifully annotated sequence, so there is a lot to scroll through, most of
which you won’t need as epis, but it is good to be familiar with GenBank.
a. Near the top there is a link to the PubMed entry for the paper this virus
isolate was sequenced for.
Q7. What is the name of the paper? a. Genomic surveillance elucidates Ebola virus origin and
transmission during the 2014 outbreak
b. Scroll down some more, and you’ll see a section under “Features” called
“source”. This section contains information about the isolate, including
country of isolation, date and host.
Q8. What date was the sample collected? a. 12 June 2014
c. The next section shows the predicted sequences of the proteins – you
are probably not going to be interested in those. Right at the bottom is
the nucleotide sequence. This sequence can be downloaded and used
to search for similar sequences and make phylogenetic trees (a
phylogenetic tree is a graphical representation of how different
sequences are related. It is similar to a family tree. You can see an
example of one on the next page), but we are not going to cover that
here.
5. Try searching for other organisms you are interested in. Have a look at some
entries, and you’ll note how some are not as well annotated as the one we just
looked at.

374
Q9. From our perspective as epidemiologists, what do you think should be the minimum information entered into this publicly accessible database?
a. There are many discussions currently ongoing on around the world on this topic. The bare minimum would be:
i. Collection date ii. Source (i.e. human, food)
iii. Country iv. Someone to contact for more information
But how useful is WGS? Do we really need the increased resolution provided by WGS?
Let’s have a look at some of the additional information provided by WGS. Look at the
Ralstonia table again, this time with WGS data added (Table 2).
Table 2: Whole genome sequencing analysis of Ralstonia isolates.
Case number Propofol exposure Hospital Species WGS
1 Yes QLD2 R. insidiosa Clade 1
2 Yes SA1 R. pickettii Clade 2
3 Yes QLD1 R. mannitolilytica Clade 3a
4 Yes QLD1 R. mannitolilytica Clade 3a
5 Yes QLD3 R. mannitolilytica Clade 3a
6 Yes QLD3 R. mannitolilytica Clade 3a
7 Yes SA1 R. mannitolilytica Clade 3b
8 Yes SA2 R. mannitolilytica Clade 3b
9 Yes VIC R. mannitolilytica Clade 3b
Propofol isolate NA NA R. mannitolilytica Clade 3b
The data from Table 2 is represented as a phylogenetic tree in Figure 1. The length of
the branches corresponds to genetic difference i.e. longer branches correspond to a
greater genetic difference. You can see that the different groups are quite obvious.

375
Figure 1: Phylogenetic analysis of Ralstonia isolates
Q10. What do you think about the possible outbreaks now? a. The QLD isolates no longer look like they are associated with the
propofol. Only SA and VIC isolates look like they could be part of a propofol associated outbreak.
Part 3: The future
Two new technologies that will change epidemiology are currently being developed for
clinical use. One is a new sequencing technology developed by Oxford Nanopore.
Current sequencers can only sequence short bits of DNA (~300 bp – the bacterial
genome is chopped up prior to sequencing). In order to get a whole genome sequence
of an organism, overlapping short bits of DNA need to be put together like a jigsaw.
This is complicated, and takes time. It can also be confused by repeat sequences.
However, the new technologies being developed by Nanopore can sequence really
long pieces of DNA. And even more excitingly, they’ve developed a sequencer that is
the size of a USB drive (called MinION), and can be used in the field (see picture below
– isn’t it cute!). If you are interested in some further reading, the paper “Rapid draft

376
sequencing and real-time nanopore sequencing in a hospital outbreak of Salmonella”
by Quick et al. discusses an investigation of an outbreak that used both WGS and
Nanopore MinION during an outbreak. The methods section is a little technical, but you
can skip over it without losing the gist of the article.
Metagenomics sounds complicated, but is just whole genome sequencing directly on
clinical samples rather than sequencing of pure cultures. Using these methods, every
single thing in the sample that has DNA can be sequenced (or RNA if you are looking
for RNA viruses etc – although this requires an extra RNA to DNA step). This includes
human DNA and the DNA from the normal human microbiome (the microorganisms
that inhabit our bodies as normal flora), so as you can imagine, finding out which
sequence corresponds to the organism causing the illness requires a lot more work
(and computational power). But research groups are successfully using this technology
in a wide variety of samples, so it is only a matter of time before it is usable in the
clinical setting. The paper “A culture-independent sequence-based metagenomics
approach to the investigation of an outbreak of Shiga-toxigenic Escherichia coli
O104:H4” by Loman et al. provides further reading for those interested, and shows the
use of metagenomics on outbreak samples. The study was done retrospectively, but
provides some insight on the power of metagenomics, especially for pathogen
discovery. Again, the methods section gets very technical, so feel free to skip it.
Conclusion:
We are at a critical stage for the introduction of WGS into public health. With proper
planning, we could have a great, consistent, nationwide system that will see us into the
future. As brand new epidemiologists with an appreciation of nationally consistent
systems, we are perfectly placed to drive this introduction.
References
Langley G., Besser J., Iwamoto M., Lessa F.C., Cronquist A., Skoff T.H., Chaves S.,
Boxrud D., Pinner R.W. and Harrison L.H. 2015. Effect of culture-independent

377
diagnostic tests on future emerging infections program surveillance. EID. 21(9):1582-
1588
Tang P. and Gardy J.L. 2014. Stopping outbreaks with real-time genomic
epidemiology. Genome Medicine. 6:104
Further reading
Quick J., Ashton P., Calus S., Chatt C., Gossain S., Hawker J., Nair S., Neal K., Nye
K., Peters T., De Pinna E., Robinson E., Struthers K., Webber M., Catto A., Dallman
T.J., Hawkey P. and Loman N.J. 2015. Rapid draft sequencing and real-time nanopore
sequencing in a hospital outbreak of Salmonella. Genome Biology. 16:114
Loman N.J., Constantinidou C., Christner M., Rohde H., Chan J.Z.M., Quick J., Weir
J.C., Quince C., Smith G.P., Betley J.R., Aepfelbacher M. and Pallen M.J. 2013. A
culture-independent sequence-based metagenomics approach to the investigation of
an outbreak of Shiga-toxigenic Escherichia coli O104:H4. JAMA 309(14):1502-1510

378
Lesson for first year MAE students – Measures of test performance Activity outline and role
During the 2015 course block, Chatu Yapa, Zoe Cutcher and I taught the first year
students how and why to calculate measures of test performance including sensitivity,
specificity, positive predictive value and negative predictive value. Zoe began the
lesson with an introduction to the measures of test performance, including how to
calculate them. Chatu followed this up by discussing her experiences as a doctor in an
Ebola treatment centre in Liberia, and how the measures of test performance were
important in diagnosing and classifying patients. I finished by taking the students
through an activity designed to calculate the measures of association in fictional
settings with different prevalence of disease. To make the activity more fun and
memorable, students were provided with hats to represent laboratory confirmation of
infection (the gold standard comparison test) with measles and red stickers to
represent symptoms consistent with measles infection. The activity used a clinical case
definition of symptoms consistent with measles only, with no laboratory evidence
considered. By combining the props in different ways we were able to represent true
positives (true measles infection with symptoms – hat and stickers), true negatives (no
hat or stickers), false positives (symptoms consistent with measles but no measles
infection - stickers with no hat) and false negatives (true measles infection with no
symptoms – hat but no stickers). The students were able to count the number of people
in each category and calculate the measures of test performance. The activity sheet
and slides for the activity are included below.
Left: Darren (MAE cohort 2015) showing off his “true positive measles infection”; Right:
students hard at work calculating measures of test performance.

379
Activity Session
Resources required:
1. Activity sheet for each student 2. Answer sheets for teaching team 3. Stickers – to represent measles case definition 4. Party hat – to represent true measles
Activity 1.
You are working in a public health unit (PHU) in Canberra. There has been a report
of a case of measles who attended your MAE graduation at ANU. Your PHU has
been tasked with finding all new cases of measles in an effort to stop transmission.
Your supervisor hasn’t done the MAE, and insists that the case definition should
only include rash as confirmation of a measles case. You decide to see how
accurately this case definition identifies cases of measles by doing a mini study of
your fellow MAE attendees.
Case definition positive = Anyone in this room with rash today (red spots)
Truth positive = Anyone who actually has measles as determined by super
accurate lab testing (party hats)
1. Count the number of lab confirmed measles cases in the group and the number
of cases determined positive by the case definition to complete the two by two
table below.
Truth (super accurate
lab test) Total
Positive Negative
Case definition Positive 3 2 5
Negative 1 8 9
Total 4 10 14
a) What is the prevalence of measles in this group? 28.6%
b) What is the:
a. Sensitivity of the case definition? 75%
b. Specificity of the case definition? 80%

380
c. Predictive value positive of the case definition? 60%
d. Predictive value negative of the case definition? 88.9%
Activity 2.
Since measles has been eliminated in Australia and cases are rare, you want to
compare our case definition with how it would work in a country where measles is
endemic and therefore has a higher prevalence. You are thrilled to learn there is an
ongoing outbreak of measles in the Philippines. You are assigned to a GOARN
group to go over and help out with diagnosis. You decide to test out how the
Australian case definition would work applied in this situation.
Truth (super accurate
lab test) Total
Positive Negative
Case definition Positive 6 1 7
Negative 2 4 6
Total 8 5 13
a) What is the prevalence of measles in this group? 61.5%
b) What is the:
a. Sensitivity of the case definition? 75%
b. Specificity of the case definition? 80%
c. Predictive value positive of the case definition? 85.7%
d. Predictive value negative of the case definition? 66.7%
c) How does performance of the case definition differ in this different setting?
In what ways is it the same? Explain why it differs?

381

382