Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Epidemiology of breast cancer – selected highlights
Jack Cuzick
Cancer Research UK Department of Epidemiology, Mathematics and Statistics, Wolfson Institute of PreventiveMedicine, London, UK
SUMMARY. The main risk factors for breast cancer can be usefully grouped into four major categories—family
history/genetic, reproductive/hormonal, proliferative benign breast pathology, and mammographic density. Thesefactors are briefly reviewed and quantitative estimaters of risk are given. A computer programme for combiningthem to produce individualized risk profiles is described. The ongoing IBIS-II trial of chemoprevention forhigh risk postmenopausal women is presented as one approach to managing high risk women.r 2003 Elsevier Ltd.All rights reserved.
Keywords: Breast cancer; Risk factors; Epidemiology; Risk profile; Chemoprevention; IBIS
INTRODUCTION
The main risk factors for breast cancer can be usefullygrouped into four major categories:
1. Family history/genetic.2. Reproductive/hormonal.3. Proliferative benign breast pathology.4. Mammographic density.
These four factors have now been thoroughly studiedand accurate quantitative estimates for the risk are nowavailable for many of them. The most useful summarycomes from the Oxford collaboration, which has nowproduced a series of papers estimating risk for individualfactors. This brief review will draw heavily on thatsource. Less is known about the possible interactionbetween these factors and virtually nothing is knownabout how different factors influence the risk ofdifferent types of breast cancer e.g. oestrogen receptorpositive vs negative tumours. Risk factors appear to belargely independent and this facilitates building a modelto predict risk for individuals. We describe one such
model below, but emphasise the need for carefulcalibration of such models on a range of data sets fromdifferent countries, and for women with different sets ofrisk factors.
FAMILY HISTORY/GENETICS
Many people identify genetic susceptibility of breastcancer solely with the known high-penetrance muta-tions of the BRCA1 and BRCA2 genes. In the generalpopulation these genes are rare, with a frequencyof less than 0.5% and account for fewer than 5% ofbreast cancers. However, they can be important inspecific circumstances such as multiple case families,where the penetrance can be as high as 80%. Heregene testing can separate carriers from non-carriersat a young age and offer reassurance to those whoare negative or some form of prophylactic interven-tion to those who are positive. Testing may also beuseful in certain founder populations such as AshkenaziJews, where the gene frequency is in excess of 2% andrisk is high.However most of the familial aggregation of breast
cancer is associated with a large number of as yetunknown genes with a lower individual penetrance.1
This makes genetic testing impossible, and risk must beassessed on phenotypic markers of the cancers which
ARTICLE IN PRESS
The Breast (2003) 12, 405–411
0960-9776/$ - see front matter r 2003 Elsevier Ltd. All rights reserved.
doi:10.1016/S0960-9776(03)00144-9
Address correspondence to: Dr Jack Cuzick, Cancer Research UK
Department of Epidemiology, Mathematics and Statistics, Wolfson
Institute of Preventive Medicine, Charterhouse Square, London
EC1M 6BQ, UK. Tel.: +44-207882 6196; Fax: +44-207882 6252;
E-mail: [email protected]
405

occur within the family. The most important of theseare:
i. number of relatives affected;ii. bilaterality;iii. relatedness of the affected case; andiv. age of onset of breast cancer.
The overall data on these factors are summarised inCGHFBG2 and shown briefly in Tables 1 and 2. InTable 1, it can be seen that the risk almost doubles if afirst degree relative (mother, sister, daughter) has hadbreast cancer and almost triples for two such relatives.Bilaterality can be treated effectively as two independentcancers, so that the risk is roughly similar for onerelative with bilateral cancer or for two separaterelatives with unilateral breast cancer. Second degreeblood relatives confer approximately half of the excessrisk of first degree relatives. Extensive pedigrees withbreast and/or ovarian cancer lead to a generally higherrisk, but in some circumstances this may be moredifficult to recognise when all the cancers appear on the
paternal side. In this case, the key information providedby the mother is unavailable and if no sister exists, allaffected female relatives will be second degree or moredistant. Careful linkage analysis is needed in thiscircumstance to estimate risk. Table 2 indicates thatthe relative risks are higher when the relative’s canceroccurred at a young age and when the woman herself isyoung. This is a particularly useful indicator when thefamily history is sparse, but needs modification forextensive family histories, where the risk for BRCA1 orBRCA2 carriers is known to remain high even at olderages.
REPRODUCTIVE/HORMONAL FACTORS
Several lines of evidence point to oestrogen levels as aprime factor for the development of breast cancer. Theseinclude laboratory studies, direct measurements in post-menopausal woman3 and risk reductions in womentaking anti-oestrogens.4 Details of the mechanisms arestill unclear, however, and a precise understanding ofthe detailed aspects of oestrogen induced carcinogenesisstill eludes us. However accurate quantitative estimatesof risk are now available for its epidemiologic correlates,and these are summarised in Table 3. There arerefinements to these estimates – e.g. the risk of breastcancer increases in the initial years following childbirth(which is generally at a young enough age that theabsolute risk is small), but then decreases for the rest ofthe woman’s life, possibly reflecting the effects ofoestrogen in pregnancy in causing extensive differentia-tion of terminal ducts and in their subsequent involu-tion. Weight operates only for post-menopausal women,where oestrogen levels are determined by the conver-sion of fat in adipose tissue to oestrogen via aromatisa-tion. The basis for the risk increase with alcoholconsumption is unclear, but could well reflect theinfluence of the liver on hormone profiles. Alcoholconsumption is known to increase the enzyme sex
ARTICLE IN PRESS
Table 1 Number of relatives with breast cancer
Number of first-degreerelatives with breast cancer
Cases(n=58209)
Controls(n=101 986)
Riskratio
None 50 713 94 548 1.00 (ref)1 6810 6998 1.802 603 404 2.933 or more 83 36 3.90
From CGHFBG.2
Table 2 Relative risk of breast cancer associated with different ages atdiagnosis and different current ages
Woman’s age Relative’s age at diagnosis of breast cancer(years)
o40 years 40–49 years 50–59 years 460 years
o40 5.7 2.9 2.8 2.040–49 3.0 2.0 2.3 1.750–59 2.0 2.2 1.6 1.6460 1.4 1.4 1.5 1.4
From CGHFBG.2
Table 3 Reproductive and hormonal risk factors for breast cancer
Factor Change in relative risk Comment
First childbirth Increase of 3% for each year of delay Nulliparous equivalent to first childbirth at age 30Age at menarche Decrease of 4%/yearAge at menopause Increase of 3%/yearBreast feeding Decrease of 4.3%/yearParity Decrease of 7%/birthOral contraceptive in use 24% increase for current or recent users onlyHRT use 2.3%/year in current or recent users onlyWeight Increase of 1%/kg Post-menopausal onlyHeight Increase of 1%/cmAlcohol Increase 7%/drink/day 1 drinkE10 g alcohol
From CGHFBG,16–19 Robbins et al.20 and van de Brandt et al.21
406 The Breast
hormone binding globulin (SHBG), which is producedin the liver. This in turn leads to higher total serumlevels of oestrogen.The effect of height is likely to be mediated by other
hormones such as epidermal growth factor or insulin-like growth factor, and more work is needed to elucidatethe mechanism involved. Oral contraceptives are arelatively minor risk factor, since they only exert aneffect on current or very recent users, and mostly areused when the woman is young so that the absolute riskis low. The risk associated with replacement therapy ismore serious, as exposure occurs during the prime riskperiod for breast cancer. This exposure is especiallyrelevant for preparations containing a progestagen.However risks are only appreciable for use exceeding 5
years, and the case for long-term use of HRT is nowtenuous, as there are better drugs for controllingosteoporosis (bisphosphonates) and the supposed bene-fits of cardiovascular disease now appear to have beenillusory. It would seem appropriate to restrict HRT useto its original indication of controlling menopausalsymptoms, and this rarely requires treatment for morethan 2 years.
BENIGN BREAST DISEASE
Risks of cancer following benign breast disease havelong been of interest, with large epidemiology studiesdating back to the 1940s.5 See Ernster6 for an early
ARTICLE IN PRESS
Table 4 Benign breast disease—summary
Type of benign disease Relative risk
Lobular carcinoma-in-situ 8–10Atypical hyperplasia 4–5Proliferative lesion without atypia 2Non-proliferative lesion No excess risk
See Dupont and Page7 and Page and Dupont.22
Table 5 Mammographic density and breast cancer risk
Percent of breast film covered by ‘densities’
None o10% 10–25 25–50 50–75 475
Rel. risk 1.0 1.2 2.2 2.4 3.4 5.3% of controls 4.9 12.7 19.5 27.0 22.2 13.7
Population attributable risk (PAR): 450% density PAR=33%;
475% density PAR=15%. From Boyd et al.9
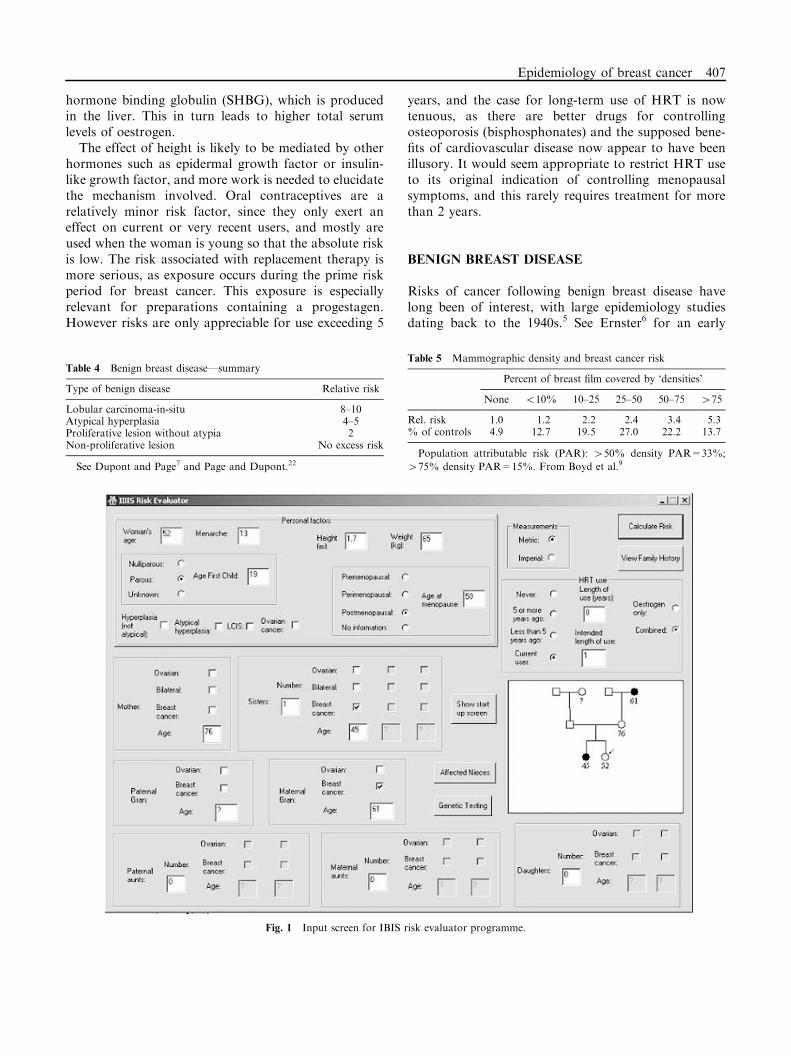
Fig. 1 Input screen for IBIS risk evaluator programme.
Epidemiology of breast cancer 407
review. It is now clear that benign disease in the absenceof proliferation does not carry any excess risk, simplehyperplasia roughly doubles the risk and atypicalhyperplasia increases the risk about 4-fold (Table 4).7
These lesions appear to reflect a field-effect and cancerstypically do not arise at or near the site of the benignlesion. This is in contrast to ductal carcinoma in situ(DCIS) when the risks are very high if left untreated andcancer develops directly from the lesion. Woman withDCIS are also at about a 4-fold increased risk ofdeveloping new contralateral tumours. Lobular carci-nomas in-situ is on the border between benign andinvasive disease. The lesions show markers of aninvasive phenotype but subsequent cancers are equallylikely to show up in either breast. In any case the risk ofcancer is high and these woman need careful surveillanceand in some cases preventive interventions.
MAMMOGRAPHIC DENSITY
Based on original observations of Wolfe et al.,8 Boydet al.,9 and others have clearly demonstrated that the
extent of radiographically opaque areas on the mam-mogram are an important measure of the risk ofdeveloping breast cancer. In fact having more than50% of the breast covered by densities constitutes thesingle factor with the largest population attributable riskof any known risk factor for breast cancer. Althoughdensity decreases after the menopause, risk is apparentfor both pre- and post-menopausal women9 (Table 5).Factors such as parity and weight influence breastdensity, but available evidence suggests that the impactof breast density is approximately independent of otherrisk factors.10
ASSESSING RISK IN INDIVIDUALS
When assessing risk for an individual it is necessary tocombine the risks associated with different possible riskfactors. This is not so important for women at very highrisk (e.g. BRCA1 carriers with a family history), where asingle factor is dominant, but it is vital for assessing ifwoman are at a moderately increased risk (e.g. 2–4 foldrelative risks). On a population basis, most of the excess
ARTICLE IN PRESS
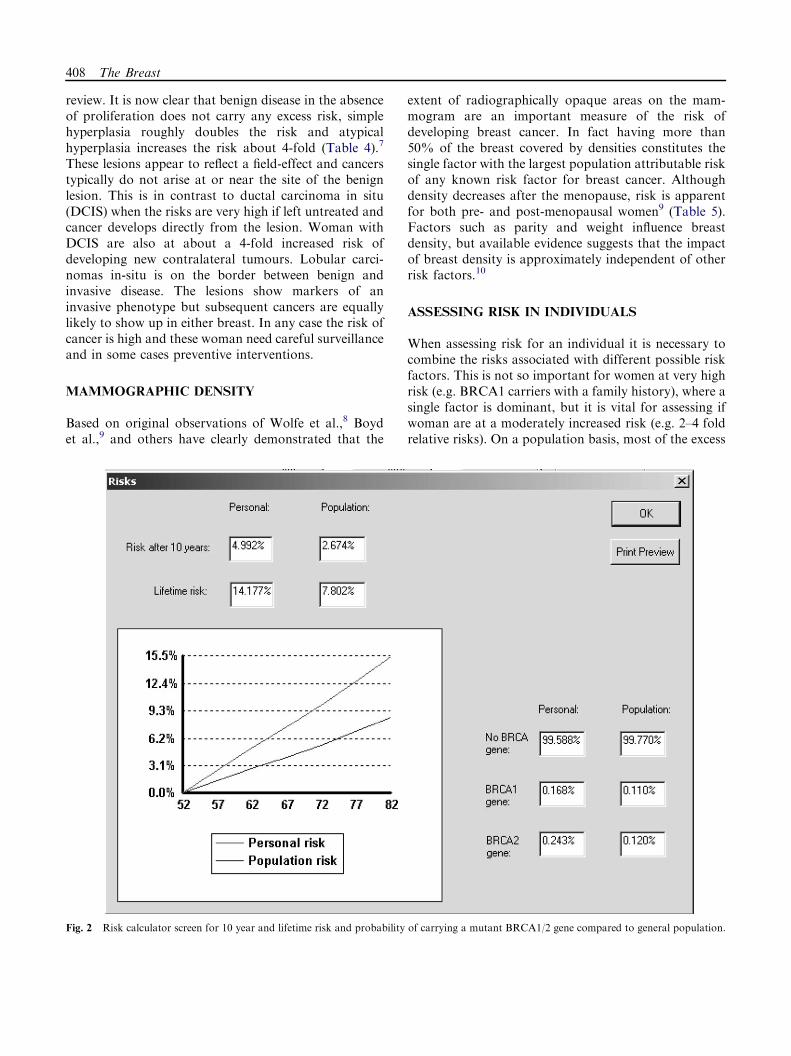
Fig. 2 Risk calculator screen for 10 year and lifetime risk and probability of carrying a mutant BRCA1/2 gene compared to general population.
408 The Breast

risk is found in this group, and accurate risk assessmentis required for these women if well focused preventionstrategies are to be employed. Two models have beenused in the past. The Gail model,11 which focuses onacquired risk factors and does not investigate familyhistory in detail, and the Claus model,12 which onlyconsiders family history. Recently we have combinedand refined these features to produce a comprehensivemodel,13 which provides an estimate of 10-year risk andlifetime risk using a wide range of factors. The modeluses frailty methods to estimate the probability ofhaving a very high risk gene mutation (e.g. BRCA1/2), amoderately high risk gene, or a normal gene andcombines this with acquired risk factors to produce asimple but comprehensive output. Consider the follow-ing example which is illustrated in Figs 1–3.
A 52-year-old woman has had one sister with breastcancer at age 45, a mother who died without breastcancer at age 76 and a maternal grandmother whodevelop breast cancer at age 61. The woman had amenarche of age 13, a child at age 19 and became post-menopausal at age 50. She weighs 65 kg and is 1.7m tall.She has used HRT for the last year only. Fig. 1 showsthe data entry screen and her pedigree, which is built inreal time as information is added. Fig. 2 graphs her riskas a function of time indicating and a 10-year risk of5.0% and a lifetime risk of 14.2% compared topopulation average risks of 2.7% and 7.8% respectively.Her chances of having a BRCA1 mutation is estimatedat 0.17% and a BRCA2 mutation at 0.24%, which are1.5 and 2.0 times the population values respectively. Thefull data are then summarised for printing (Fig. 3).
ARTICLE IN PRESS
Fig. 3 Printed output from IBIS Risk calculator programme.
Epidemiology of breast cancer 409
By changing the different input parameters it ispossible to determine the contribution of differentfactors to her risk. Access to the programme is availableto investigators in the IBIS-II prevention trial and to themedical professionals who obtain access to the protectedpart of the IBIS website (www.ibis-trials.org).
PREVENTION OF BREAST CANCER IN
HIGH-RISK WOMEN
Being able to determine risk is of little value unlesssomething can be done about it. Interventions need tobe tailored to the individual, taking account of personalpreferences and risk levels. At the very high end, e.g. forknown BRCA1 carriers with a family history, the risk ofbreast cancer is approximately 80% and surgicalinterventions such as bilateral mastectomy or oophor-ectomy are viable options. At the other extreme forwomen with a weak or no family history or other strongrisk factors, regular attendance for screening, weightcontrol and possibly increased exercise are probablyadequate. However about 10% of woman are atmoderately increased risk (2–4 fold) and a more activeintervention short of surgery is worth consideration.Prophylactic tamoxifen has been shown to decrease theincidence of ER-positive breast cancer by about 50%,leading to about a one-third reduction in all breastcancer.4 However this intervention increases venousthromboembolic events about 2-fold and endometrial
cancer to about 212 times the population rates.4 For post-
menopausal women, aromatase inhibitors show evenmore promise and anastrozole has now shown greaterreduction in recurrence than for tamoxifen and a muchgreater reduction in new contralateral tumours (ATAC
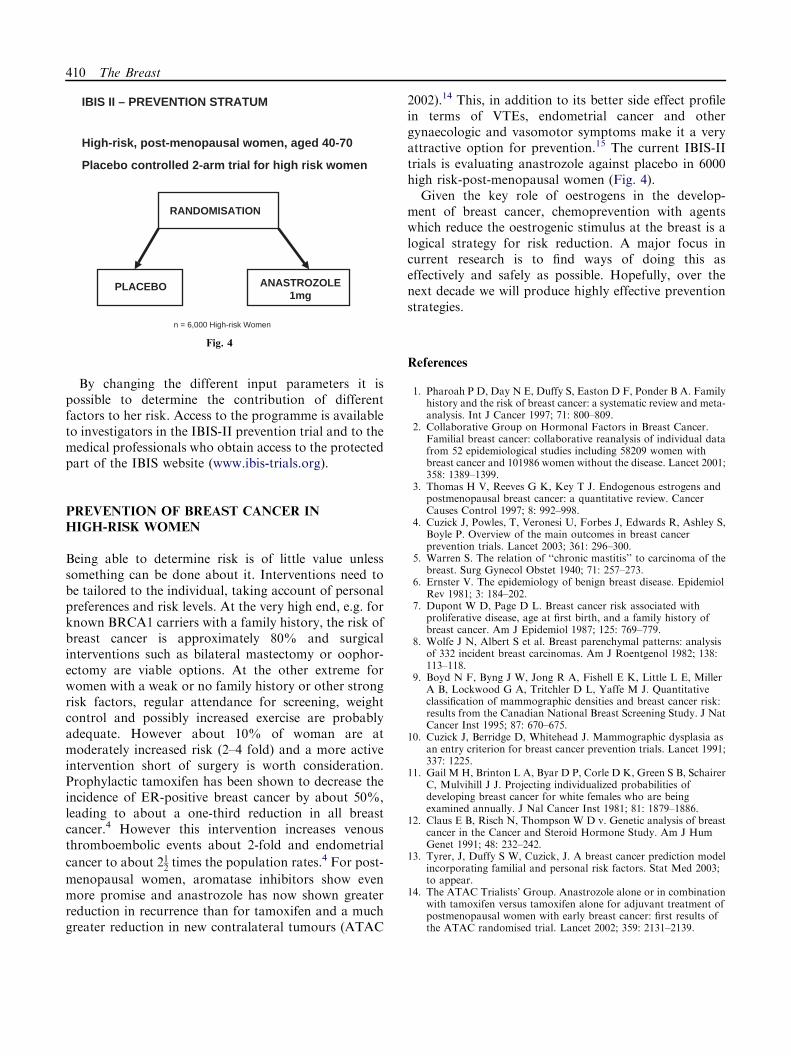
2002).14 This, in addition to its better side effect profilein terms of VTEs, endometrial cancer and othergynaecologic and vasomotor symptoms make it a veryattractive option for prevention.15 The current IBIS-IItrials is evaluating anastrozole against placebo in 6000high risk-post-menopausal women (Fig. 4).Given the key role of oestrogens in the develop-
ment of breast cancer, chemoprevention with agentswhich reduce the oestrogenic stimulus at the breast is alogical strategy for risk reduction. A major focus incurrent research is to find ways of doing this aseffectively and safely as possible. Hopefully, over thenext decade we will produce highly effective preventionstrategies.
References
1. Pharoah P D, Day N E, Duffy S, Easton D F, Ponder B A. Familyhistory and the risk of breast cancer: a systematic review and meta-analysis. Int J Cancer 1997; 71: 800–809.
2. Collaborative Group on Hormonal Factors in Breast Cancer.Familial breast cancer: collaborative reanalysis of individual datafrom 52 epidemiological studies including 58209 women withbreast cancer and 101986 women without the disease. Lancet 2001;358: 1389–1399.
3. Thomas H V, Reeves G K, Key T J. Endogenous estrogens andpostmenopausal breast cancer: a quantitative review. CancerCauses Control 1997; 8: 992–998.
4. Cuzick J, Powles, T, Veronesi U, Forbes J, Edwards R, Ashley S,Boyle P. Overview of the main outcomes in breast cancerprevention trials. Lancet 2003; 361: 296–300.
5. Warren S. The relation of ‘‘chronic mastitis’’ to carcinoma of thebreast. Surg Gynecol Obstet 1940; 71: 257–273.
6. Ernster V. The epidemiology of benign breast disease. EpidemiolRev 1981; 3: 184–202.
7. Dupont W D, Page D L. Breast cancer risk associated withproliferative disease, age at first birth, and a family history ofbreast cancer. Am J Epidemiol 1987; 125: 769–779.
8. Wolfe J N, Albert S et al. Breast parenchymal patterns: analysisof 332 incident breast carcinomas. Am J Roentgenol 1982; 138:113–118.
9. Boyd N F, Byng J W, Jong R A, Fishell E K, Little L E, MillerA B, Lockwood G A, Tritchler D L, Yaffe M J. Quantitativeclassification of mammographic densities and breast cancer risk:results from the Canadian National Breast Screening Study. J NatCancer Inst 1995; 87: 670–675.
10. Cuzick J, Berridge D, Whitehead J. Mammographic dysplasia asan entry criterion for breast cancer prevention trials. Lancet 1991;337: 1225.
11. Gail M H, Brinton L A, Byar D P, Corle D K, Green S B, SchairerC, Mulvihill J J. Projecting individualized probabilities ofdeveloping breast cancer for white females who are beingexamined annually. J Nal Cancer Inst 1981; 81: 1879–1886.
12. Claus E B, Risch N, Thompson W D v. Genetic analysis of breastcancer in the Cancer and Steroid Hormone Study. Am J HumGenet 1991; 48: 232–242.
13. Tyrer, J, Duffy S W, Cuzick, J. A breast cancer prediction modelincorporating familial and personal risk factors. Stat Med 2003;to appear.
14. The ATAC Trialists’ Group. Anastrozole alone or in combinationwith tamoxifen versus tamoxifen alone for adjuvant treatment ofpostmenopausal women with early breast cancer: first results ofthe ATAC randomised trial. Lancet 2002; 359: 2131–2139.
ARTICLE IN PRESS
RANDOMISATION
ANASTROZOLE1mg
n = 6,000 High-risk Women
PLACEBO
IBIS II – PREVENTION STRATUM
High-risk, post-menopausal women, aged 40-70
Placebo controlled 2-arm trial for high risk women
Fig. 4
410 The Breast

15. Cuzick J. A brief review of the International Breast CancerIntervention Study (IBIS), the other current breast cancerprevention trials, and proposals for future trials. In: Anthony M,Dunn B K, Sherman S, eds. Selective Estrogen ReceptorModulators [SERMs]; Ann N Y Acad Sci 2002; 949:123–133.
16. Collaborative Group on Hormonal Factors in Breast Cancer.Breast cancer, hormonal contraceptives: collaborative reanalysisof individual data on 53 297 women with breast cancer and 100 239women without breast cancer from 54 epidemiological studies.Lancet 1996; 347: 1713–1727.
17. Collaborative Group on Hormonal Factors in Breast Cancer.Breast cancer, hormone replacement therapy: collaborativereanalysis of data from 51 epidemiology studies of 52 705 womenwith breast cancer and 108 411 women without breast cancer.Lancet 1997; 350: 1047–1059.
18. Collaborative Group on Hormonal Factors in Breast Cancer.Breast cancer, breastfeeding: collaborative reanalysis of individualdata from 47 epidemiological studies in 30 countries, including
50 302 women with breast cancer and 96973 women without thedisease. Lancet 2002; 360: 187–195.
19. Collaborative Group on Hormonal Factors in Breast Cancer.Alcohol, tobacco and breast cancer – collaborative reanalysis ofindividual data from 53 epidemiology studies, including 58 515women with breast cancer and 95 067 women without the disease.Br J Cancer 2002; 87: 1234–1245.
20. Robbins A S, Brescianini S, Kelsey J L. Regional differences inknown risk factors and the higher incidence of breast cancer in SanFrancisco. J Natl Cancer Inst 1997; 89: 960–965.
21. van den Brandt P A, Spiegelman D, Yaun S S, Adami H O,Beeson L, Folsom A R, Fraser G, Goldbohm R A, Graham S,Kushi L, Marshall J R, Miller A B, Rohan T, Smith-Warner S A,Speizer Fe, Willett W C, Wolk A, Hunter D J. Pooled analysis ofprospective cohort studies on height, weight, and breast cancerrisk. Am J Epidemiol 2000; 152: 514–527.
22. Page D L, Dupont W D. Anatomic markers of humanpremalignancy and risk of breast cancer. Cancer 1990; 66:1326–1335.
ARTICLE IN PRESS
Epidemiology of breast cancer 411