Embed Size (px)
Citation preview
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 1
January 6th 2012A cardiologist received a phone call from Dr. S. Re: 40-year-old woman from El Salvador who has what looks like eosinophilic myocarditis with a large mass in her left ventricle. Her eosinophil count is 18 percent. He wants to send the patient urgently for evaluation.
January 16th 201240-year-old woman who immigrated from El Salvador age 18. She has been healthy without any prior medical or cardiovascular problems. However, in October of last year, she began to develop increasing symptoms of diarrhea, abdominal pain, and finally nausea and vomiting. She has been very ill and has lost 12 pounds over the past few months.
One week ago, she developed intermittent chest pain and was hospitalized. At that time, she was found to have a mass in her left ventricle as well as hypereosinophilia. Dr. S has treated her with aspirin, warfarin, and Lopressor and is sending her here for further evaluation. All of her history is through an interpreter. However, Ms. A states that she is severely ill, very weak, unable to walk up more than three steps before having to stop because of symptoms of shortness of breath and fatigue. She has not had any neurologic events.
Patient complains of pain. Location: Abdominal Pain.On a scale of 0 to 10, patient rates pain a 6.
Medications:
Aspirin Low Dose 81 mg tablet enteric coated 1 TABLET by mouth one time daily.
Celexa 20 mg tablet 1 TABLET by mouth one time daily.
Coumadin 2 mg tablet 1 TABLET by mouth one time daily.
ergocalciferol (Vit D2) 50,000 unit capsule 1 capsule by mouth every week.
gabapentin tablet 1 TABLET by mouth every morning.
Lopressor tablet 1 TABLET by mouth two times a day.
omeprazole 20 mg capsule enteric coated 1 capsule by mouth one time daily.
Vitamin B-2 100 mg tablet 1 TABLET by mouth one time daily.
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 2
Vitals:
Height: 167.0 cm. Weight: 59.00 kg. BSA(G): 1.66 M2. BMI: 21.155 KG/M2. (16-Jan-2012 07:40)
Blood Pressure: 96/54 mmHg, average of several readings, right arm sitting. Pulse Rate: 76/minute. (16-Jan-2012 07:40)Blood Pressure: 105/70 mmHg. Pulse Rate: 90/minute, regular. (16-Jan-2012 07:41)
Exam:
General: She appears weak, tired, and ill but in no acute distress. She is oriented times three with a normal mental status and speaks through an interpreter.Skin: Integument is normal.Head: Examination is normal.ENT: Examination is normal. She does have peripheral cyanosis.Vessels: Her jugular venous pressure is not elevated.Heart: There is a 1+ right ventricular lift. There is a palpable P2. First heart sound is normal. Second heart sound is widely split with inspiration with an increased pulmonic component intensity 3+/4+. There is a soft 1/6 diastolic decrescendo murmur, high-pitched quality, at the left sternal border.Lungs: Clear.Abdomen: Soft and nontender without masses.Extremities: The pulses are full. There is no edema.

EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 3
IRP:
Ms. A presents with some type of systemic illness associated with increased eosinophil count as well as a mass in her left ventricle. Although we do need to confirm the hematologic and cardiac findings by our own laboratory tests (we have no outside records at this time), this most likely represents a hypereosinophilic syndrome with cardiac involvement. Her echocardiogram is classic for the intermediate stage characterized by a large apical thrombus. She is at very high risk of embolic events, and I have recommended that we hospitalize her for urgent testing as well as a diagnosis. We will get our own blood work; specifically, our eosinophil count. She should be seen by our hematologist. She will need intravenous heparin if her INR is not therapeutic as well as hydration. Once the diagnosis is confirmed, then urgent treatment should be begun, most likely high-dose steroid as well as the possibility of tyrosine kinase inhibition. Also get serology to rule out Chagas disease, but the echocardiogram that I reviewed from outside certainly looks like hypereosinophilic disease.
We do need to watch her for the development of significant left ventriculardysfunction during aggressive treatment. At some time, a CT angiogram or an MR angiogram should be performed to rule out embolic events to her coronary artery as a cause of her chest pain. I have attempted to discuss these recommendations with the patient through the interpreter, but we will hospitalize her urgently today following her laboratory testing and get back to Dr. S with the results of this evaluation.
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 4
Hospital Note:
Outside echocardiogram was reviewed. This showed a large 4.5 x 3.5 mass at the apical site of the left ventricle involving two-thirds of the left ventricular cavity. There was restrictive filling due to this. LV size was normal with an EF of about 45%. There was mild mitral regurgitation with a large left atrium.
Other tests such as ECG, chest x-ray, echo to be done here at Mayo as well as an MRI to be done here at Mayo are still pending. Outside records are pending.
IMPRESSION#1 Eosinophilic myocarditis#2 Left ventricular thrombus, most likely due to No. 1#3 Angina at rest #4 Abdominal pain, nausea, vomiting, and diarrhea
PLANMs. A presents with what seems to be eosinophilic heart disease. She is unfortunately feeling very unwell and lethargic and is dehydrated and is also having episodes of chest pain. I would suggest that we admit her to the hospital so that we can investigate her further as well as treat her further. We will need to do our own blood work including a full blood count, eosinophilic count, and blood smear. We also need to do our own echocardiogram as well as an MRI with MRA of the coronary arteries to exclude coronary embolism or coronary arteritis as causes of her chest pain. We will need to involve Hematology for the treatment of her hypereosinophilia. We will need to involve Allergy for possible cause of her hypereosinophilia. We will need to test her stools for parasites as a cause of her infectious disease, and we will also rule out Chagas disease.
Dr. G on the Cards Service has been informed that the patient will be admitted to his service for further investigation and treatment.
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 5
ECHOCARDIOGRAM:
1. Findings consistent with hypereosinophilic syndrome.
2. Large laminated thrombus occupies the apical two-thirds of the left ventricular cavity. A
small right ventricular apical thrombus is also present. 3. Mild left ventricular enlargement.
4. Calculated left ventricular ejection fraction; 49 %. 5. Mild generalized left ventricular hypokinesis. 6. Grade 3/4 left ventricular diastolic dysfunction, consistent with severely elevated left ventricular filling pressure. 7. Mildly thickened mitral valve without subvalvular thrombotic obliteration or leaflet tethering. Mild central mitral regurgitation. 8. Normal right ventricular size and systolic function. 9. Mildly thickened tricuspid valve. No subvalvular thrombotic obliteration or leaflet tethering. Mild central tricuspid regurgitation 10. Estimated right ventricular systolic pressure; 69 mmHg. 11. Tiny pericardial effusion.
She travelled to her home country of El Salvador (originally emigrated at 18 years old) around May 2011. She exposed to chickens, ducks, turkeys, and dogs. She underwent a colonoscopy with showed erythema of the left colon and biopsy which showed tubular adenoma. There was no mention about presence or absence of eosinophils. Two weeks ago she developed chest pain, dyspnea on exertion and shortness of breath.
She states that she has had migraines for 3 years. Her family thinks that she has had difficulty remembering things for the last year or so. She also complains of numbness in her hands during the night for the last year. She denies a past history of allergic rhinitis but has had some nasal congestion recently. She denies joint swelling, oral ulcers, and hemoptysis.
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 6
Catherine R. Weiler, MD, PhD, 4-6116, 16-Jan-2012 19:47In brief, Ms. A is a 40-year-old lady referred to Saint Marys Hospital for management of eosinophilic myocarditis. Ms. A is from South America and had recently visited Guatemala. A few months ago, she started having problems with diarrhea and subsequently-worsening systemic symptoms. She was recently found to have peripheral blood eosinophilia with an eosinophil count around 2,000 eosinophils per microliter. She was found to have a thrombus in the left and right ventricle along with changes consistent with endocarditis and eosinophilic myocarditis.
Outside- negative QuantiFERON, IgG toxoplasma positive/IgM negative, negative stool O/P, negative trypanosoma Ab, E Histolytica Ab negativeHere- positive MPO Ab
#1 Elevated eosinophils#2 LV thrombus, RV thrombus with EF 48%, delayed enhancement subendocardial LV #3 Intermittent forgetfulness#4 History of nausea/vomit/diarrhea
Ms. A's symptoms and laboratory tests are concerning for cardiac involvement of eosinophilia of uncertain etiology. The differential diagnosis for the etiology of the hypereosinophilia includes but is not limited to parasitic infection, underlying bone marrow disorder, allergic phenomena, medication related, Churg Strauss. As she has evidence of thrombosis and organ dysfunction, steroid therapy is highly recommended but her travel history makes her at high risk for worsening parasitic infection if this is instituted. Therefore, we would recommend comprehensive parasitic work up to be sent as below with concurrent administration of steroid therapy with acknowledgement of the risk of worsening parasitic infection, especially strongyloides (recommend IgG and stool culture). Serology and cultures for parasitic infection can take 1-2 weeks for results.
1. Start Prednisone 100 mg daily tomorrow AM after AM cortisol is drawn - AM cortisol 1/172. Daily CBC with automated differential drawn at the same time each AM as eosinophils may vary depending on the time of day and intrinsic cortisol levels3. Parasitic work up
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 7
-Trichinella Ab -Echinococcus -Stool o and p X 3-Strongyloides stool culture 88699-Serologies:
a. Toxocariasis/Visceral Larval Migrans Test # 40945 b. Strongyloides IgG Antibody by Elisa,
3. Work up for primary bone marrow disorder for hypereosinophilic syndrome
-CHIC-2 deletion-BCR-ABL -Leukemia/lymphoma phenotype -T cell receptor gene rearrangement - Defer to Hematology for consideration of bone marrow biopsy
4. Other labs-Tryptase-Troponin -Aldolase-SPEP-IgE-IL5
5. Positive MPO Ab- CXR- UA
6. Thrombophilia work up per primary team and Hematology7. If possible obtain outside colonoscopy slides to be evaluated for eosinophilic infiltration
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 8
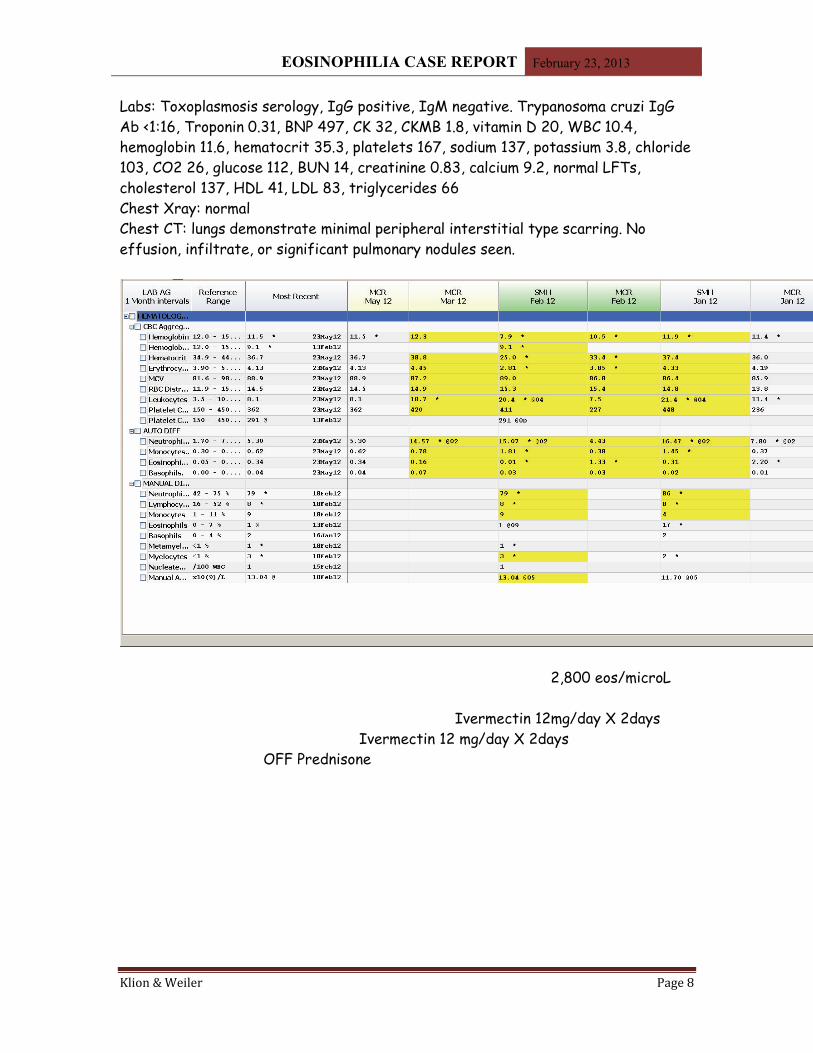
Labs: Toxoplasmosis serology, IgG positive, IgM negative. Trypanosoma cruzi IgG Ab <1:16, Troponin 0.31, BNP 497, CK 32, CKMB 1.8, vitamin D 20, WBC 10.4, hemoglobin 11.6, hematocrit 35.3, platelets 167, sodium 137, potassium 3.8, chloride 103, CO2 26, glucose 112, BUN 14, creatinine 0.83, calcium 9.2, normal LFTs, cholesterol 137, HDL 41, LDL 83, triglycerides 66Chest Xray: normalChest CT: lungs demonstrate minimal peripheral interstitial type scarring. No effusion, infiltrate, or significant pulmonary nodules seen.
2,800 eos/microL
Ivermectin 12mg/day X 2daysIvermectin 12 mg/day X 2days
OFF Prednisone
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 9
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 10
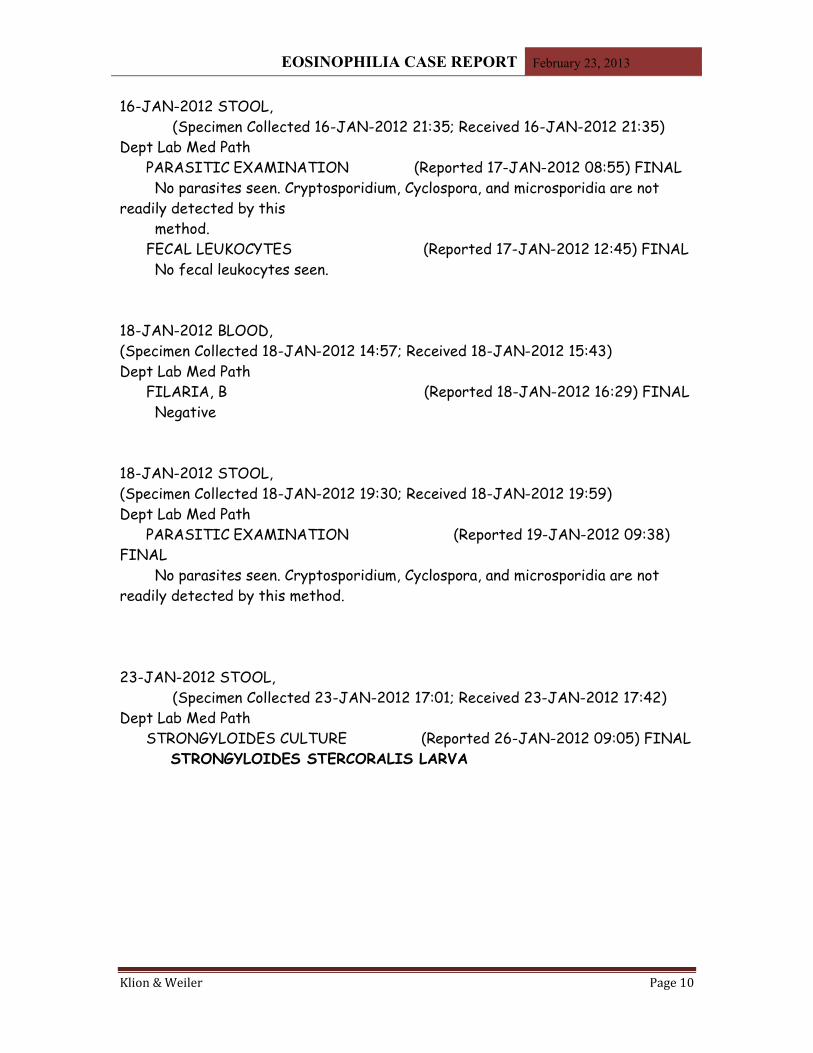
16-JAN-2012 STOOL, (Specimen Collected 16-JAN-2012 21:35; Received 16-JAN-2012 21:35) Dept Lab Med Path PARASITIC EXAMINATION (Reported 17-JAN-2012 08:55) FINAL No parasites seen. Cryptosporidium, Cyclospora, and microsporidia are not readily detected by this method. FECAL LEUKOCYTES (Reported 17-JAN-2012 12:45) FINAL No fecal leukocytes seen.
18-JAN-2012 BLOOD, (Specimen Collected 18-JAN-2012 14:57; Received 18-JAN-2012 15:43) Dept Lab Med Path FILARIA, B (Reported 18-JAN-2012 16:29) FINAL Negative
18-JAN-2012 STOOL, (Specimen Collected 18-JAN-2012 19:30; Received 18-JAN-2012 19:59) Dept Lab Med Path PARASITIC EXAMINATION (Reported 19-JAN-2012 09:38) FINAL No parasites seen. Cryptosporidium, Cyclospora, and microsporidia are not readily detected by this method.
23-JAN-2012 STOOL, (Specimen Collected 23-JAN-2012 17:01; Received 23-JAN-2012 17:42) Dept Lab Med Path STRONGYLOIDES CULTURE (Reported 26-JAN-2012 09:05) FINAL STRONGYLOIDES STERCORALIS LARVA
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 11
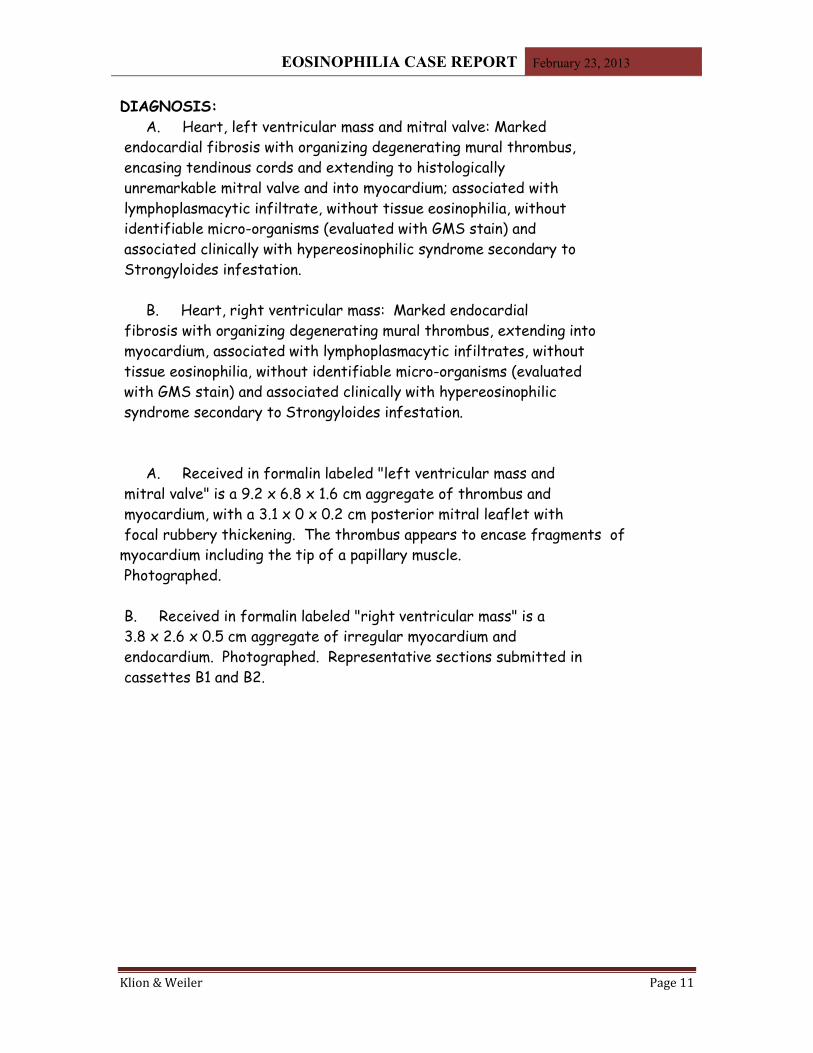
DIAGNOSIS: A. Heart, left ventricular mass and mitral valve: Marked endocardial fibrosis with organizing degenerating mural thrombus, encasing tendinous cords and extending to histologically unremarkable mitral valve and into myocardium; associated with lymphoplasmacytic infiltrate, without tissue eosinophilia, without identifiable micro-organisms (evaluated with GMS stain) and associated clinically with hypereosinophilic syndrome secondary to Strongyloides infestation.
B. Heart, right ventricular mass: Marked endocardial fibrosis with organizing degenerating mural thrombus, extending into myocardium, associated with lymphoplasmacytic infiltrates, without tissue eosinophilia, without identifiable micro-organisms (evaluated with GMS stain) and associated clinically with hypereosinophilic syndrome secondary to Strongyloides infestation.
A. Received in formalin labeled "left ventricular mass and mitral valve" is a 9.2 x 6.8 x 1.6 cm aggregate of thrombus and myocardium, with a 3.1 x 0 x 0.2 cm posterior mitral leaflet with focal rubbery thickening. The thrombus appears to encase fragments of
myocardium including the tip of a papillary muscle. Photographed.
B. Received in formalin labeled "right ventricular mass" is a 3.8 x 2.6 x 0.5 cm aggregate of irregular myocardium and endocardium. Photographed. Representative sections submitted in cassettes B1 and B2.
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 12
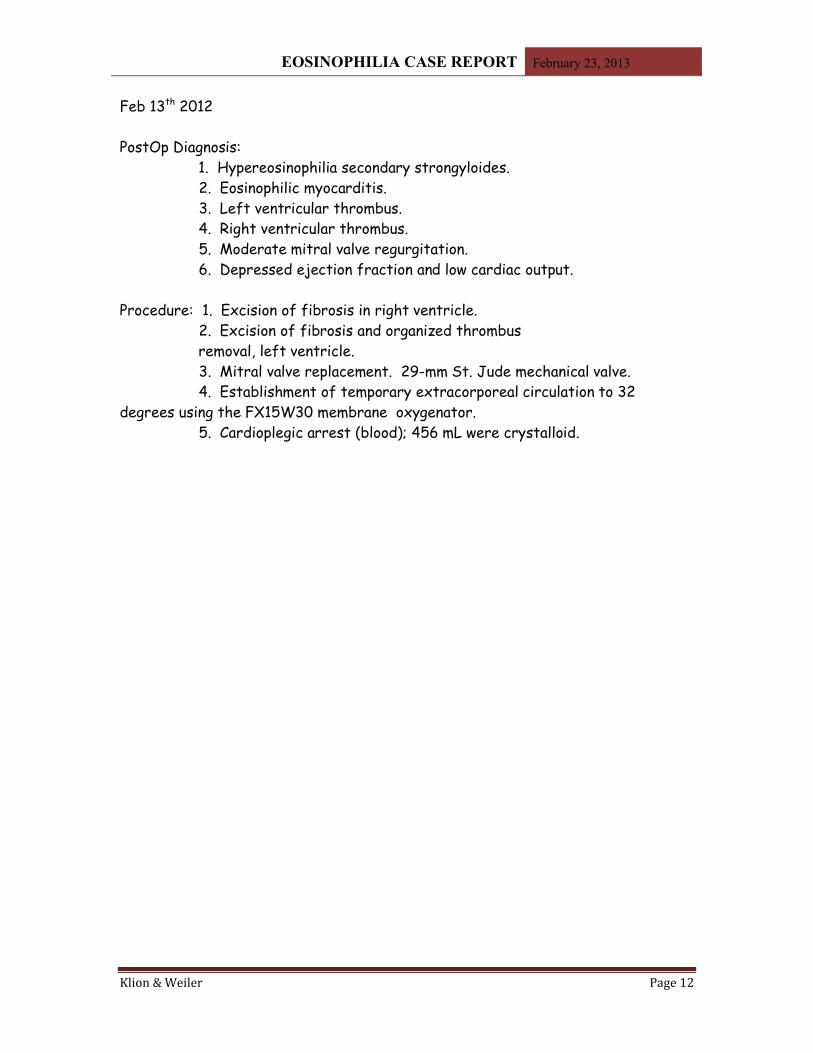
Feb 13th 2012
PostOp Diagnosis: 1. Hypereosinophilia secondary strongyloides.
2. Eosinophilic myocarditis. 3. Left ventricular thrombus. 4. Right ventricular thrombus. 5. Moderate mitral valve regurgitation. 6. Depressed ejection fraction and low cardiac output. Procedure: 1. Excision of fibrosis in right ventricle. 2. Excision of fibrosis and organized thrombus removal, left ventricle. 3. Mitral valve replacement. 29-mm St. Jude mechanical valve. 4. Establishment of temporary extracorporeal circulation to 32 degrees using the FX15W30 membrane oxygenator. 5. Cardioplegic arrest (blood); 456 mL were crystalloid.
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 13
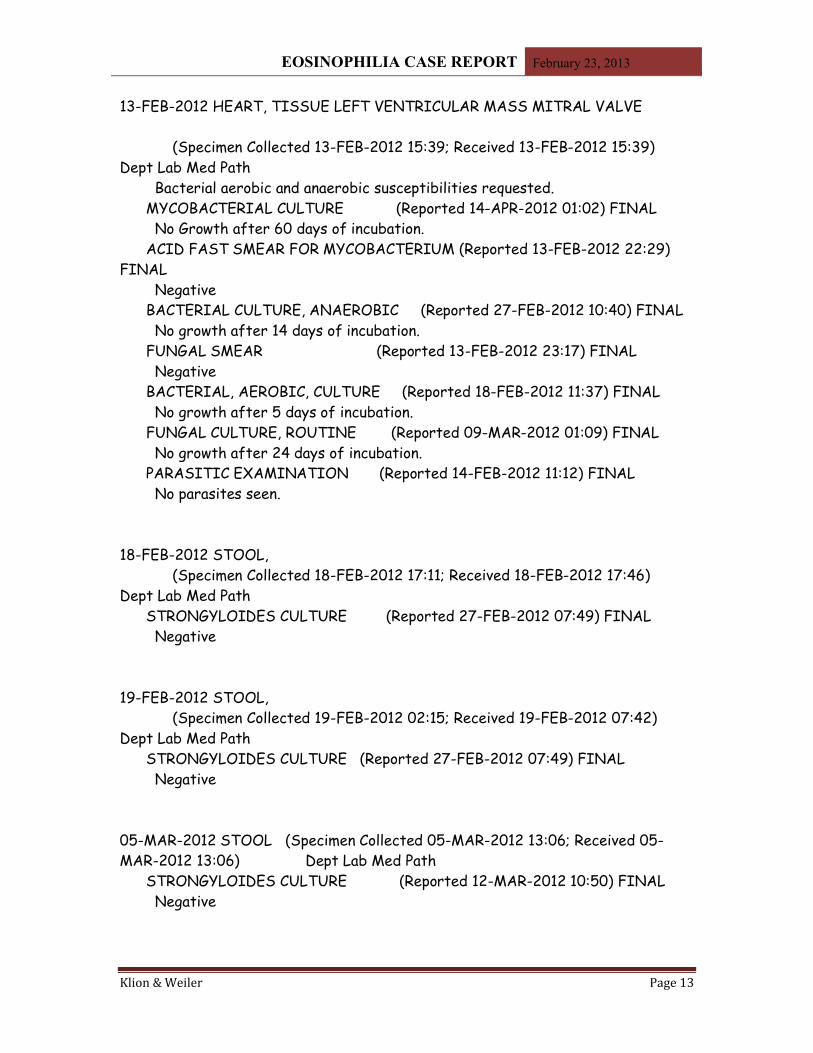
13-FEB-2012 HEART, TISSUE LEFT VENTRICULAR MASS MITRAL VALVE
(Specimen Collected 13-FEB-2012 15:39; Received 13-FEB-2012 15:39) Dept Lab Med Path Bacterial aerobic and anaerobic susceptibilities requested. MYCOBACTERIAL CULTURE (Reported 14-APR-2012 01:02) FINAL No Growth after 60 days of incubation. ACID FAST SMEAR FOR MYCOBACTERIUM (Reported 13-FEB-2012 22:29) FINAL Negative BACTERIAL CULTURE, ANAEROBIC (Reported 27-FEB-2012 10:40) FINAL No growth after 14 days of incubation. FUNGAL SMEAR (Reported 13-FEB-2012 23:17) FINAL Negative BACTERIAL, AEROBIC, CULTURE (Reported 18-FEB-2012 11:37) FINAL No growth after 5 days of incubation. FUNGAL CULTURE, ROUTINE (Reported 09-MAR-2012 01:09) FINAL No growth after 24 days of incubation. PARASITIC EXAMINATION (Reported 14-FEB-2012 11:12) FINAL No parasites seen.
18-FEB-2012 STOOL, (Specimen Collected 18-FEB-2012 17:11; Received 18-FEB-2012 17:46) Dept Lab Med Path STRONGYLOIDES CULTURE (Reported 27-FEB-2012 07:49) FINAL Negative
19-FEB-2012 STOOL, (Specimen Collected 19-FEB-2012 02:15; Received 19-FEB-2012 07:42) Dept Lab Med Path STRONGYLOIDES CULTURE (Reported 27-FEB-2012 07:49) FINAL Negative
05-MAR-2012 STOOL (Specimen Collected 05-MAR-2012 13:06; Received 05-MAR-2012 13:06) Dept Lab Med Path STRONGYLOIDES CULTURE (Reported 12-MAR-2012 10:50) FINAL Negative
EOSINOPHILIA CASE REPORT February 23, 2013
Klion & Weiler Page 14
23-MAY-2012 STOOL, (Specimen Collected 23-MAY-2012 08:40; Received 23-MAY-2012 08:40) Dept Lab Med Path STRONGYLOIDES CULTURE (Reported 30-MAY-2012 08:01) FINAL Negative





























