Embed Size (px)
Citation preview
Enucleation after Plaque Radiotherapy for Posterior Uveal Melanoma
Histopathologic Findings
CAROL L. SHIELDS, MD, l JERRY A. SHIELDS, MD, l ULF KARLSSON, MD,2 HYMAN MENDUKE, PhD,3 LUTHER W. BRADY, MD2
Abstract: A review of 1019 patients with posterior uveal melanomas, who were treated with episcleral plaque radiotherapy between April 1976 and December 1987, showed that 59 (6%) of these patients have thus far required enucleation of the affected eye. The most common clinical reasons for enucleation were tumor regrowth (51 %) and neovascular glaucoma (31 %). These irradiated melanomas were of mixed cell type in 40 cases (68%), spindle in 10 cases (17%), totally necrotic in 7 cases (12%), and epithelioid in 2 cases (3%). Some degree of tumor necrosis was seen in all cases. Overall, the median number of mitoses per 40 high-power fields in these irradiated tumors was O. Most (64%) of the tumors had no identifiable mitosis in 40 high-power fields. A three-way simultaneous comparison of the following groups was made: irradiated eyes enucleated for tumor regrowth, irradiated eyes enucleated for neovascular glaucoma, and a matched group of nonirradiated posterior uveal melanomas. This comparison showed that the largest tumor dimension was significantly greater in the irradiated eyes enucleated for tumor regrowth than in the other two groups. Mitotic activity was significantly higher in the irradiated tumor regrowth and nonirradiated groups than in the irradiated neovascular group. There was no significant difference among the three groups in an analysis of height. The results suggested that mitotic activity may exist after plaque radiotherapy, especially when there is clinical evidence of tumor regrowth. Ophthalmology 1990; 97:1665-1670
Originally received: January 23, 1989 Revision accepted: June 22, 1990
1 Oncology Service, Wills Eye Hospital, Jefferson Medical College, Thomas Jefferson University, Philadelphia.
2 Department of Radiation Oncology and Nuclear Medicine, Hahnemann Medical College, Hahnemann University, Philadelphia.
3 Department of Pharmacology, Jefferson Medical College, Thomas Jef-ferson University, Philadelphia.
Supported in part by the Heed Foundation, Chicago, IL, the Macula Foundation Research Fund, New York, NY, and the Eye Tumor Research Fund Incorporated, Gladwyne, PA.
Episcleral plaque radiotherapy has proven to be an effective method of controlling the growth of melanomas of the ciliary body and choroid. 1-10 In the most cases, the tumor responds to this treatment by gradually decreasing in size over a period of months to years.8
,10 In most cases the tumor shows excellent regression and the affected eye is retained, often with good vision. Such eyes are not enucleated, and consequently little histopathologic material is available. Unfortunately, in some cases regrowth of the tumor or severe complications of the radiotherapy may necessitate enucleation of the affected eye. II
-16
Reprint requests to Carol L. Shields, MD, Oncology Service, Wills Eye Hospital, 9th & Walnut Sts, Philadelphia, PA 19107.
There is little information in the literature on the histopathologic findings of plaque-irradiated uveal mela-
1665

OPHTHALMOLOGY • DECEMBER 1990 • VOLUME 97 • NUMBER 12
Table 1. Histopathologic Findings in 59 Enucleated Eyes after Plaque Irradiation
Tumor Size Cell Type Median
Reason for No. of Eyes Mean (mm) Mitoses Enucleation (%) LTD x Height E M S N 40 HPF
Tumor growth 30 (51) 13 X 5 0 21 5 4 2.5 Neovascular glaucoma 18 (31) 10 X 5 1 12 3 2 0 Patient/preference 5 (8) 10 X 5 1 3 1 0 0 Scleral necrosis 4 (7) 7X4 0 3 0 1 0 Bullous keratopathy 1 (2) 11 X 2 0 1 0 0 0 Hemolytic glaucoma 1 (2) 9X2 0 0 1 0 0
Total 59 (100) 11 X 5 2 40 10 7 0
LTD = largest tumor dimension; E = epithelioid; M = mixed; S = spindle; N = necrotic; HPF = high-power fields.
nomas.9.13,17 In 1977, MacFaul and Morgan17 reported the histopathologic changes of irradiated choroidal melanoma in 23 eyes that came to enucleation after cobalt-60 plaque radiotherapy. More recently, Lommatzsch9
briefly commented on the histopathologic findings in 64 eyes that had ruthenium-106-irradiated uveal melanoma and noted that there was tumor cell activity in 52 of those 64 enucleated eyes.
Other forms of irradiation such as helium ion and proton beam are used to treat uveal melanomas. The microscopic effects of helium ion irradiation on uveal melanomas were reported in 1987 by Crawford and Char,18 who found that mitotic figures were "extremely rare" in helium ion-treated tumors. Others19,2o have evaluated the histopathologic features of proton beam irradiation in a few cases of uveal melanoma and noted the significant role of tumor ischemia in melanoma regression,
We studied in detail the histopathologic findings in 59 enucleated eyes that had been treated with various types of radioactive plaques. To our knowledge, this is the largest number of cases contained in a detailed histopathologic report of eyes enucleated after radiation. The clinical features of the patients and tumors in this select group have been reported in a separate communication.21 In this study, we assessed the histopathologic findings in this group of enucleated eyes.
MATERIALS AND METHODS
All patients with the diagnosis of posterior uveal melanoma who were treated with episcleral plaque radiotherapy on the Oncology Service at Wills Eye Hospital between April 1976 and December 1987 were identified. Those patients who subsequently underwent enucleation of the treated eye were selected for further study. In these cases, the tumor size (indirect ophthalmoscopic estimation of largest tumor diameter [LTD] and ultrasonographic height in millimeters) as clinically estimated immediately before plaque irradiation was recorded.
The microscopic glass slides prepared from these formalin-fixed, paraffin-embedded enucleated globes were
1666
reviewed. Using calipers, the LTD and tumor height were measured in millimeters. With standard light microscopic techniques, two representative hematoxylin-eosin-stained glass slides from the pupil-optic nerve segment were studied. In heavily pigmented tumors, standard bleached preparations were used to identify cytoplasmic and nuclear detail better. In every case, gross sections had been made through the largest portion of the tumor. The individual tumors were evaluated for predominant cell type (using the modified Callender classification22
) and number of mitoses per 40 high-power fields (40 X objective, 10 X ocular). Only unequivocal mitotic figures were counted. Each tumor was assessed for the stage of extraocular extension (graded as none, intrascleral, vortex vein, small extrascleral [<5 mm in diameter], or large extrascleral [>5 mm in diameter]).
As a comparison group, we identified 59 eyes with posterior uveal melanoma that were treated with enucleation as primary treatment without irradiation therapy before enucleation. These eyes were matched on a one-to-one basis to the eyes in the plaque-irradiated group with regard to pretreatment clinical tumor size and location of the melanoma as recorded on the chart. The location was graded as primarily involving the choroid posterior to the equator, the choroid between the equator and the ora serrata, or the ciliary body. The size of the nonirradiated posterior uveal melanoma was matched to within 2 mm of indirect ophthalmoscopic estimation of LTD and ultrasonographic height and was limited to a maximum LTD of 13 mm and height of 8 mm. These were dimensions that would potentially be amenable to plaque radiotherapy had this method of treatment been chosen. The comparison group was then evaluated in an identical fashion for the glass slide LTD and height as measured by calipers and the number of mitoses per 40 high-power fields.
RESULTS
Of 2400 patients with posterior uveal melanoma who were evaluated on the Ocular Oncology Service at Wills
SHIELDS et al • ENUCLEATION AFTER PLAQUE RADIOTHERAPY
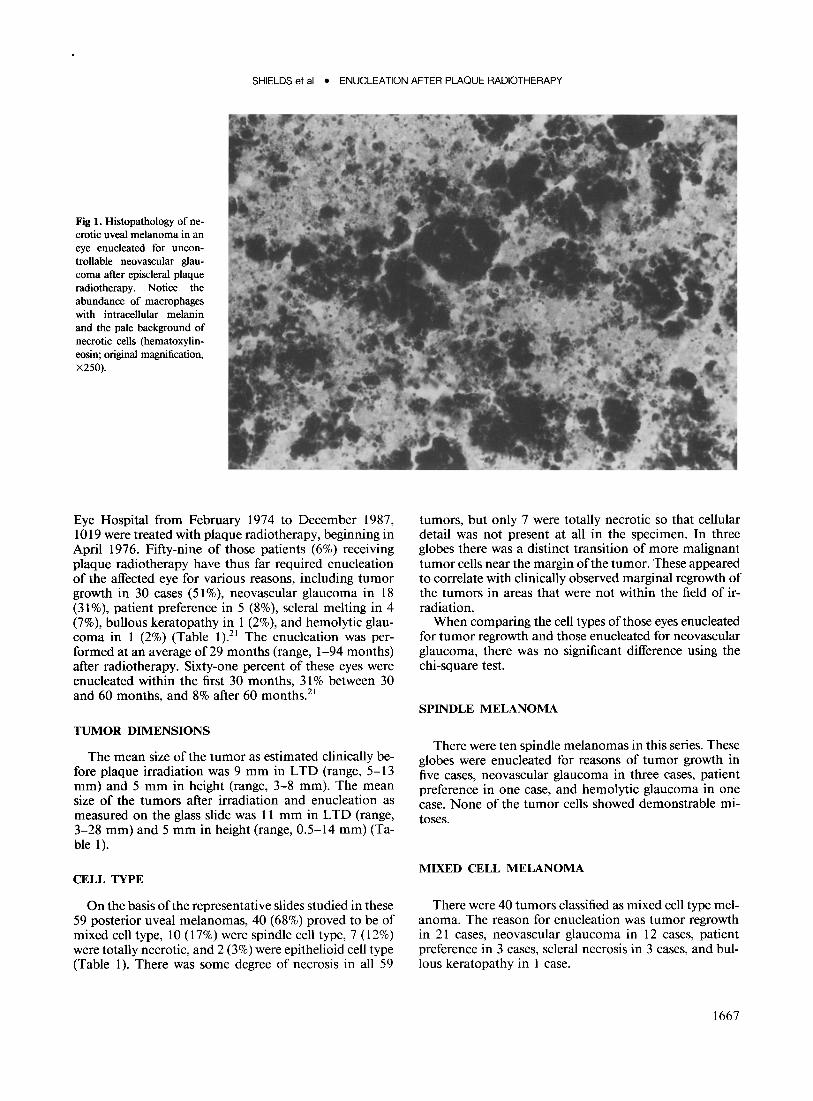
Fig 1. Histopathology of necrotic uveal melanoma in an eye enucleated for uncontrollable neovascular glaucoma after episcleral plaque radiotherapy. Notice the abundance of macrophages with intracellular melanin and the pale background of necrotic cells (hematoxylineosin; original magnification, X250).
Eye Hospital from February 1974 to December 1987, 1019 were treated with plaque radiotherapy, beginning in April 1976. Fifty-nine of those patients (6%) receiving plaque radiotherapy have thus far required enucleation of the affected eye for various reasons, including tumor growth in 30 cases (5 1 %), neovascular glaucoma in 18 (31 %), patient preference in 5 (8%), scleral melting in 4 (7%), bullous keratopathy in 1 (2%), and hemolytic glaucoma in 1 (2%) (Table 1).21 The enucleation was performed at an average of29 months (range, 1-94 months) after radiotherapy. Sixty-one percent of these eyes were enucleated within the first 30 months, 31 % between 30 and 60 months, and 8% after 60 months.21
TUMOR DIMENSIONS
The mean size of the tumor as estimated clinically before plaque irradiation was 9 mm in LTD (range, 5-13 mm) and 5 mm in height (range, 3-8 mm). The mean size of the tumors after irradiation and enucleation as measured on the glass slide was 11 mm in LTD (range, 3-28 mm) and 5 mm in height (range, 0.5-14 mm) (Table 1).
CELL TYPE
On the basis ofthe representative slides studied in these 59 posterior uveal melanomas, 40 (68%) proved to be of mixed cell type, 10 (17%) were spindle cell type, 7 (12%) were totally necrotic, and 2 (3%) were epithelioid cell type (Table 1). There was some degree of necrosis in all 59
tumors, but only 7 were totally necrotic so that cellular detail was not present at all in the specimen. In three globes there was a distinct transition of more malignant tumor cells near the margin of the tumor. These appeared to correlate with clinically observed marginal regrowth of the tumors in areas that were not within the field of irradiation.
When comparing the cell types of those eyes enucleated for tumor regrowth and those enucleated for neovascular glaucoma, there was no significant difference using the chi-square test.
SPINDLE MELANOMA
There were ten spindle melanomas in this series. These globes were enucleated for reasons of tumor growth in five cases, neovascular glaucoma in three cases, patient preference in one case, and hemolytic glaucoma in one case. None of the tumor cells showed demonstrable mitoses.
MIXED CELL MELANOMA
There were 40 tumors classified as mixed cell type melanoma. The reason for enucleation was tumor regrowth in 21 cases, neovascular glaucoma in 12 cases, patient preference in 3 cases, scleral necrosis in 3 cases, and bullous keratopathy in 1 case.
1667

OPHTHALMOLOGY • DECEMBER 1990 • VOLUME 97 • NUMBER 12
Table 2. Extraocular Extension in Enucleated Eyes with Plaque-irradiated Posterior Uveal Melanomas
Tumor Size (mm)*
Reason for Degree of Cell Mitosest Enucleation EOE LTD x Height Type 40 HPF
SN Intrascleral 8x8 N 0 NVG Intrascleral 9x6 M 0 NVG Intrascleral 3 x 1 M 0 TG Intrascleral 12 x 2 M 17 TG Vortex vein 14 x 10 S 0 TG Vortex vein 12 x 5 M 9 SN <5 mm EOE 8x2 M 0 NVG <5 mm EOE 12 x 4 N 0 SN >5 mm EOE 6x3 M 0 TG >5 mm EOE 15 x 2 M 5
EOE = extraocular extension; LTD = largest tumor diameter; HPF = high-power fields; SN = scleral necrosis; N = necrotic; NVG = neovascular glaucoma; M = mixed; TG = tumor growth; S = spindle.
* Mean, 10 x 4 mm. t Median, O.
EPITHELIOID CELL MELANOMA
There were only two epithelioid cell melanomas in this study. The tumors averaged 14 mm in LTD and 8 mm in mean height. The reasons for enucleation were patient preference in one case and neovascular glaucoma in the other.
NECROTIC MELANOMA
There were seven totally necrotic melanomas in which no viable tumor cells were identified (Fig 1). The reasons for enucleation were clinically suspected tumor growth in four cases, neovascular glaucoma in two cases, and scleral necrosis in one case. There was no mitotic activity noted in these tumors.
MITOTIC ACfIVITY
Overall, the median number of unequivocal mitoses per 40 high-power fields was 0 (Table 1). Thirty-eight tumors (64%) had no demonstrable mitoses in 40 highpower fields. The 30 globes with melanoma that were enucleated for tumor regrowth had a median of 2.5 mitoses per 40 high-power fields, and mitotic activity was observed in 17 of these globes (57%). The globes that were enucleated for neovascular glaucoma had a median of 0 mitosis per 40 high-power fields and mitoses were observed in only 3 (17%) of 18 cases.
EXTRAOCULAR EXTENSION
There were ten globes with extension of the posterior uveal melanoma beyond the confines of the inner sclera (Table 2). The degree of extraocular extension was intrascleral in four cases, vortex vein in two cases, small episcleral nodule «5 mm in diameter) in two cases, and
1668
large episcleral nodule (>5 mm in diameter) in two cases. The reasons for enucleation were tumor growth in four cases, neovascular glaucoma in three cases, and scleral melting in three cases. The extraocular extension was not clinically apparent before surgery in eight of the ten cases. It was clinically visible in two cases of scleral melting.
The cell types of the tumors with extraocular extension ranged from spindle melanoma with 0 mitosis to mixed cell melanoma with 17 mitoses per 40 high-power fields. The mean size of the posterior uveal melanoma in these cases was 10 mm in LTD and 4 mm in height. Five of these ten intraocular melanomas were 3 mm or less in height.
FINDINGS IN MATCHED NONIRRADIATED POSTERIOR UVEAL MELANOMAS
There were 59 eyes with posterior uveal melanoma in our comparison group that had not received prior radiation therapy of any type. These 59 comparison eyes were selected out of a total pool of 897 eyes enucleated for posterior uveal melanoma over the time of this study. The clinical tumor size ranged in size from 5 to 13 mm in LTD and 2 to 8 mm in height (mean size, 10 mm in LTD and 6 mm in height). The histologic glass slide tumor size ranged from 4 to 13 mm in LTD and 1 to 8 mm in height (mean size, 10 mm in LTD and 6 mm in height). In these matched eyes, the median number of mitoses per 40 high-power fields was 4 (range, 0-60). There were 3~tumors (66%) with greater than 0 mitoses per 40 highpower fields.
The three largest groups in this study were compared simultaneously with regard to glass slide LTD and height and mitotic activity. These groups included irradiated eyes enucleated for tumor regrowth, irradiated eyes enucleated for neovascular glaucoma, and the nonirradiated matched group. Using the Newman-Keuls test, the irradiated tumor regrowth group had a significantly larger LTD (mean, 12.7 mm) than the irradiated neovascular group (mean, 9.6 mm; P < 0.01) or nonirradiated group (mean, 10.4 mm; P < 0.05). The LTD of the irradiated neovascular group and nonirradiated group did not differ significantly. An analysis of variance showed no significant difference in tumor height among the three groups.
Using the chi-square test comparing all three groups simultaneously, the presence of mitoses within the tumor (mitotic activity> 0) was found to be highly statistically significant (P < 0.001). Using the Bonferroni adjustment to account for the three comparisons made, we found that mitotic activity greater than 0 was significantly more common in the irradiated tumor regrowth group (17 [57%] of 30 cases with> 0 mitoses) than the irradiated neovascular group (3 [17%] of 18 cases with> 0 mitoses; P < 0.05 in both cases). The presence of mitotic activity did not significantly differ between the irradiated tumor regrowth group and the nonirradiated group (P> 0.05). However, the presence of mitotic activity was significantly greater in the non irradiated group (39 [66%] of 59 cases> 0) than in the irradiated neovascular group (3 [17%] of 18 cases > 0; P < 0.001 in both cases).

SHIELDS et al • ENUCLEATION AFTER PLAQUE RADIOTHERAPY
DISCUSSION
In 1977, MacFaul and Morgan 17 reported on a series of 100 patients with choroidal melanomas who were treated with cobalt-60 plaque radiotherapy and stated that 23 of these patients eventually underwent enucleation for reasons of tumor growth, blindness, glaucoma, and scleral necrosis. The histopathologic findings of the studied globes showed that 22 of the cases were spindle cell type, 1 was mixed cell type, and there was no occurrence of epithelioid cell type. Necrosis was present to some degree in six cases (26%), tumor hemorrhage in six cases (26%), tumor inflammatory cells in three cases (13%), and vitreous hemorrhage in five cases (21%). Mitotic activity was not evaluated. Since this initial report, there have been no published cases of a large series evaluating the histopathologic effects of radioactive plaque therapy on posterior uveal melanomas.
In our series of 59 eyes enucleated after plaque radiotherapy for posterior uveal melanoma, we found several important histopathologic features. The LTD as measured on the glass slides in those irradiated eyes with clinical evidence of tumor regrowth was significantly greater than for those irradiated eyes enucleated for neovascular glaucoma and those enucleated without prior plaque radiotherapy. The tumor height did not significantly differ in those irradiated eyes with tumor regrowth as compared with irradiated eyes removed for neovascular glaucoma or those without prior plaque radiotherapy. This suggests that the eyes with tumor regrowth developed the growth not so much in thickness but in horizontal lateral dimensions.
The overall mitotic activity in the irradiated eyes was a median of 0 mitoses per 40 high-power fields; mitotic cells were found in 21 (36%) of the 59 tumors. In the irradiated eyes enucleated for tumor regrowth, the mitotic activity was a median of2.5 per 40 high-power fields, and the presence of mitotic activity in these eyes was significantly greater than in those irradiated eyes enucleated for neovascular glaucoma (median mitotic activity, 0). This confirmed our clinical impression that regrowing irradiated posterior uveal melanomas are indeed mitotically active.
Crawford and Char18 reported that 28 of255 eyes with uveal melanoma treated with charged-particle radiation were eventually enucleated. Results of histopathologic examination of those eyes showed that mitotic figures within the tumors were "rare" and only five tumors had a single mitosis in 80 high-power fields. Their findings may reflect the finding that only four (15%) of the eyes in their series were enucleated for reasons of tumor regrowth, whereas the remaining eyes were enucleated for reasons of neovascular glaucoma, painful keratitis, vitreous hemorrhage, and autopsy. Autopsy cases were not included in our current study.
The cell types of the uveal melanomas in our study included spindle (17%), mixed (68%), epithelioid (3%), and necrotic (12%). MacFaul and Morgan 17 reported
spindle cell type in 96% and mixed cell type in 4% of the cases in their series. Crawford and Char18 observed spindle melanoma in 41 %, mixed cell type in 52%, and necrotic cell type in 7%. The differences in cell types seen within the three studies are probably due to several factors, including the reasons for enucleation, time from radiotherapy to enucleation, and microscopic interpretation by the pathologist.
Extraocular extension was present in ten of our cases (Table 2). The tumor was less than or equal to 3 mm in height in 50% of the cases, and the extraocular extension was clinically suspected in only two cases (2 cases of obvious scleral necrosis). These relatively flat, diffuse melanomas have a tendency to extend extrasclerally, and this has been noted in prior reports.23 Three of the four cases of scleral necrosis in our series had evidence of extraocular extension of the tumor through the weakened sclera. MacFaul and Morgan 17 reported two cases of scleral necrosis in their series, neither of which had microscopic evidence of extraocular extension.
In summary, 6% of eyes with plaque-irradiated posterior uveal melanoma eventually required enucleation of the irradiated eye. These patients have had follow-up intervals of varying lengths, and this percentage may not be truly representative of this population. The reasons for enucleation are tumor regrowth, neovascular glaucoma, patient preference, scleral necrosis, among others. Overall, the median mitotic activity of these irradiated eyes was 0, but those eyes enucleated because of tumor regrowth tended to show significant histopathologic evidence of mitotic activity (median mitotic activity, 2.5 per 40 high-power fields).
REFERENCES
1. Stallard HB. Radiotherapy for malignant melanoma of the choroid. Br J OphthalmoI1966; 50:147-55.
2. Long RS, Galin MA, Rotman M. Conservative treatment of intraocular melanomas. Trans Am Acad Ophthalmol Otolaryngol 1971; 75:84-
93. 3. Bedford MA. The use and abuse of cobalt plaques in the treatment
of choroidal malignant melanomata. Trans Ophthalmol Soc UK 1973;
93:139-43. 4. Rotman M, Long RS, Packer S, et al. Radiation therapy of choroidal
melanoma. Trans Ophthalmol Soc UK 1977; 97:431-5. 5. MacFaul PA. Local radiotherapy in the treatment of malignant mela
noma of the choroid. Trans Ophthalmol Soc UK 1977; 97:421-7. 6. Ellsworth RM. Cobalt plaques for melanoma of the choroid. In: Jakobiec
FA, ed. Ocular and Adnexal Tumors. Birmingham, AL: Aesculapius Publishing Co, 1978:76-9.
7. Packer S, Rotman M. Radiotherapy of choroidal melanoma with iodine-125. Ophthalmology 1980; 87:582-90.
8. Shields JA, Augsburger JJ, Brady LW, Day JL. Cobalt plaque therapy of posterior uveal melanomas. Ophthalmology 1982; 89:1201-7.
9. Lommatzsch PK. Results after J3-irradiation (,06Ru/'06Rh) 01 choroidal melanomas: 20 years ' experience. Br J Ophthalmol 1986; 70:844-
51. 10. Cruess AF, Augsburger JJ, Shields JA, et al . Regression of posterior
uveal melanomas following Cobalt-50 plaque radiotherapy. Ophthal
mology 1984; 91:1716-9.
1669

OPHTHALMOLOGY • DECEMBER 1990 • VOLUME 97 • NUMBER 12
11. Hayreh SS, Post-radiation retinopathy. A fluorescence fundus angiographic study. Br J Ophthalmol 1970; 54:705-14.
12. MacFaul PA, Bedford MA. Ocular complications after therapeutic irradiation. Br J Ophthalmol1970; 54:237-47.
13. Char DH, Lonn LI, Margolis LW. Complications of cobalt plaque therapy of choroidal melanomas. Am J OphthalmoI1977; 84:536-41.
14. Brown GC, Shields JA, Sanborn G, et al. Radiation retinopathy. Ophthalmology 1982; 89: 1494-1501.
15. Brown GC, Shields JA, Sanborn G, et al. Radiation optic neuropathy. Ophthalmology 1982; 89:1489-93.
16. Cruess AF, Augsburger JJ, Shields JA, et al. Visual results following cobalt plaque radiotherapy for posterior uveal melanomas. Ophthalmology 1984; 91:131-6.
17. MacFaul PA, Morgan G. Histopathological changes in malignant rnelanomas of the choroid after cobalt plaque therapy. Br J Ophthalmol 1977; 61:221-8.
1670
18. Crawford JB, Char DH. Histopathology of uveal melanomas treated with charged particle radiation. Ophthalmology 1987; 94:639-43.
19. Seddon JM, Gragoudas ES, Albert OM. Ciliary body and choroidal melanomas treated by proton beam irradiation: histopathologic study of eyes. Arch Ophthalmol1983; 101:1402-8.
20. Ferry AP, Blair CJ, Gragoudas ES, Volk SC. Pathologic examination of ciliary body rnelanoma treated with proton beam irradiation. Arch Ophthalmol1985; 103:1849-53.
21. Shields CL, Shields JA, Karlsson U, et al. Reasons for enucleation after plaque radiotherapy for posterior uveal melanoma: clinical findings. Ophthalmology 1989; 96:919-24.
22. McLean IW, Zimrnerman LE, Evans RM. Reappraissal of Callender's spindle A type of malignant melanorna of the choroid and ciliary body. Am J Ophthalmol 1978; 88:557-65.
23. Font RL, Spaulding AG, Zimmerman LE. Diffuse malignant melanoma of the uveal tract: a clinicopathologic report of 54 cases. Trans Am Acad Ophthalmol Otolaryngol1968; 72:877-95.


![The Technique of Tonsil Enucleation - Semantic Scholar...Dec., 1936] TECHNIQUE OF TONSIL ENUCLEATION: WILLIAMSON 727 Special Article THE TECHNIQUE OF TONSIL ENUCLEATION By H. WILLIAMSON,](https://img.dokumen.tips/doc/110x75/5e9dc57b42f70b199c246bec/the-technique-of-tonsil-enucleation-semantic-scholar-dec-1936-technique.jpg)