Embed Size (px)
Citation preview

Enterococcus faecalisJose J. Ferrari D.D.S.
Graduate Endodontic DepartmentCase Western Reserve University

E. faecalis CharacteristicsEnterococcus faecalis formerly classified as Group
D Streptococcus.
Gram-positive cocci that occur singly, in pairs, or in short chains.
Facultative anaerobes.
They catabolize a variety of energy sources including carbohydrates, glycerol, lactate, malate, citrate, arginine, agmatine, and many α keto acids.
Displays gamma hemolysis on sheep’s blood agar

Cont. Characteristics• E. faecalis can cause life-threatening infections in humans,
especially in the nosocomial (hospital) environment.
• Major nosocomial pathogens causing bacteremia, endocarditis, bacterial meningitis, urinary tract, and various other infections
Live in vast quantities in the human intestinal lumen.
They are common in environments contaminated by human and animal faecal materials (e.g. urban sewage, recipient water, and soil receiving fertilizers of animal origin), as well as in food products derived from animals
Present in human female genital tract and oral cavity in lesser numbers.

Virulence Factors Aggregation Substance
− Biofilm formation helps resist Ca(OH)2
• Surface Adhesins– Adhesins that facilitate specific binding of enterococci to intestinal
epithelium, renal epithelial cells, human neutrophils, and macrophages
Superoxide formation– Tissue destruction– Neutrophil chemo-attractant
Gelatinase formation (GelE)
− Can hydrolyse gelatin, casein, haemoglobin, and other bioactive peptides.

Virulence factorsHyaluronidase
− Destroys CT
Cytolysin– Targets erythrocytes
AS-48– An antibiotic-like peptide found in some strains of
E. Faecalis– Competition with other bacteria

Virulence FactorsLTA (lipoteichoic acid) is involved in
inflammatory responses and sepsis syndrome biofilm formation and adhesion to teeth because of its absorptive activity to hydroxyapetite

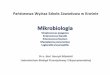
Scanning Electron Microscope

Primary Endodontic Infections Polymicrobial
Dominated by Gram-negative Anaerobic Rods
E. faecalis is found in 4to 40% of primary endodontic infections
− et al Rocas, Siqueira JOE 2004
Secondary Endodontic Infections• Compose of one or a few bacterial species
Predominantly Gram-positive microorganisms
9 times more likely to contain E. faecalis than primary endodontic infections

Primary Endodontic Infection

Secondary Endodontic Infection

Persistence of Periapical Lesion

Why in Endodontic Reinfection?

E. faecalis and Endodontic failures
E. faecalis is mostly associated with asymptomatic cases
Despite making up a small proportion of the flora in untreated canals, plays a major role in the etiology of persistent periradicular lesions after root canal treatment.
It is commonly found in a high percentage of root canal failures and it is able to survive in the root canal as a single organism or as a major component of the flora

E. faecalis: Endodontic RE-infections
Very seldom found in primary root canal infections– Sundqvist, JOE, 1992
VERY frequently found in endodontic RE-infections that have signs of chronic apical periodontitis– Engstrom, 1964, Moller, 1966
Can often occur as a monoculture in infected and treated root canals– Sundqvist, 1998

EcologyEnterococci have been described as extremely
hardy organisms capable of living in many mediums that would certainly kill other bacteria.
Capable of survival at 60 degrees Celsius for 30 minutes.
Enterocoocus faecalis is able to grow in 6.5% NaCl. Enterococci can also grow in 40% bile salts and over a broad range of pH.
Enterococci also have a large amount of natural antibiotic resistance.

E. faecalis Survival Within The Root Canal System
It exhibits widespread genetic polymorphisms
It possesses serine protease, gelatinase, collagen-binding proteins (ACE), help to bind to dentin
It can invade and live within dentinal tubules (250-400 microns)
It has the capacity to endure prolonged periods of starvation
Once nutritional supply become available starved cells are able to recover by utilizing serum

Penetrance of E. faecalis in the dentinal tubules
Penetrates 250 m in the tubules– Siren et al, 1997
Bovine model penetrates 300-400 m – Haapasalo, 1987
Penetrance of bacteria is retarded with keeping of the smear layer– Haapasalo, 1987– Case for keeping the smear layer?

E. faecalis Survival Within The Root Canal System
E. faecalis is able to form a biofilm that helps it resist destruction by enabling the bacteria to become 1000 times more resistant to phagocytosis, antibodies and antibacterials
In dentinal tubules it can resist intracanal dressings of calcium hydroxide for over 10 days
E. faecalis is less dependent upon virulence factors, it relies more upon its ability to survive and persist as a pathogen in the root canals of teeth.

Growth Phases of E. Faecalis
Longitudinal growth vs. starvation phase
When in the starvation phase, it can be 10,000 times more resistant to medicaments than when in its longitudinal growth phase– Portenier et al, 2005
More resistant to UV radiation, heat, NaOCl, H2O2, EtOH, and acid.– Giard et al, 1996
This viable but non-cultivable (VBNC) state may explain how it is a monoinfection in obturated canals
Return when the environment is more favorable for growth

Growth Phases cont...This starvation phase is poorly understood
Is not a spore forming bacteria
Synthesizes a myriad of genes in order to cope with its harsh environment and make energy– Giard et al, J Bacteriol, 2000

Quick review on Calcium Hydroxide
Is the most commonly used intracanal medicament
Calcium hydroxide releases hydroxyl ions in aqueous solutions, resulting in a high alkaline environment where most bacteria cannot survive
Is antimicrobial by raising the pH of the root canal environment
Dissolves tissue– Wadaki, Araski, Suda, Hasselgren

pH needed to kill E. Faecalis
At pH of 10.5 to 11.0, growth of E. faecalis was inhibited– McHugh et al, 2004
pH can only reach up to 10.3 because of the buffering effect of dentin.
pH gradient decreases deeper in the dentinal tubules
11.5 was necessary to eradicate

Adapts to the environmentE. faecalis has a functioning proton pump that
actually pumps hydrogen ions to acidify the cytoplasm in highly alkaline conditions– McHugh, Evans, 2002

Calcium Hydroxide and LTA
Calcium hydroxide inactivation of LTA appears to occur immediately (within 5 minutes) at a relatively low calcium hydroxide concentration (2.5 mg/mL).
Currently, the mechanism for inactivation of LTA by calcium hydroxide is unknown.
− deacylation of LTA
et al Baik, Kum JOE 2008 (November)

Therefore, E. faecalis is resistant to Ca(OH)2 intracanal/interappointment treatments

Current Strategies forEradication
Preparing the apical portion of the root canal to a larger size will help eliminate intracanal microorganisms
Full strength NaOCl is still effective against E. faecalis– Needs to be in contact– No substantivity
Need to be able to penetrate the tubules where they like to hide
Chlorhexidine is effective against E. faecalis– Smear layer prevents its contact– Has substantivity

Remove the Smear Layer!NaOCL to remove the ORGANIC component of
the smear layer
17% EDTA to remove the INORGANIC component of the smear layer
Final rinse with 2% CHX in the canal now that the tubules are opened up
Good technique for primary NSRCT’s
A MUST for NS RETX

Steps to Eliminate E. faecalis