Embed Size (px)
Citation preview

Computers in Human Behavior 31 (2014) 446–452
Contents lists available at SciVerse ScienceDirect
Computers in Human Behavior
journal homepage: www.elsevier .com/locate /comphumbeh
Enhancing neuroanatomy education using computer-based instructionalmaterial
0747-5632/$ - see front matter � 2013 Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.chb.2013.03.005
⇑ Corresponding author. Address: Department of Basic Psychology, Psychobiologyand Methodology of Behavioral Science, Faculty of Psychology, University ofSalamanca, Avda. De la Merced, s/n, ES-37008 Salamanca, Spain. Tel.: +34669197002.
E-mail addresses: [email protected] (P. Ruisoto Palomera), [email protected] (J.A.Juanes Méndez), [email protected] (A. Prats Galino).
Pablo Ruisoto Palomera a,⇑, Juan A. Juanes Méndez b, Alberto Prats Galino c
a Department of Basic Psychology, Psychobiology and Methodology of Behavoiral Science, University of Salamanca, Spainb Department of Human Anatomy, University of Salamanca, Spainc Laboratory of Surgical Anatomy, University of Barcelona, Spain
a r t i c l e i n f o
Article history:Available online 10 April 2013
Keywords:Medical informaticsTrainingEvaluationNeuroanatomy
a b s t r a c t
The understanding of spatial relationships between brain structures taken from conventional sectionalimages is a major problem in learning anatomy. However, scientific literature has suggested that highervisuospatial abilities and computer-based instructional 3D visualizations may facilitate learning anat-omy. This paper aims (1) to develop a computer-based tool to explore neuroanatomy based on three-dimensional images and (2) to compare whether the educational value assigned by students variesaccording to their visuospatial ability. An anatomical and functional viewer was developed with PositronEmission Tomography images to visualize three-dimensional models of real brain structures. Studentsassigned a high educational value to this tool, regardless of their visuospatial skills. The discussion sectionanalyzes the implications of this technique in neuroanatomy training.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
A good understanding of neuroanatomy is difficult to achieve, inparticular, spatial relationship comprehension together with accu-rate interpretation of functional images (Giles, 2010; Older, 2004;Ruisoto, Juanes, Contador, Mayoral, & Prats-Galino, 2012; Zinchuk,Flanagan, Tubridy, Miller, & McCullough, 2010). Instructionalmaterial involved in learning neuroanatomy and student’s visuo-spatial ability can help explain this phenomenon.
On the one hand, traditional learning methods have consisted onvisual exploration of printed material (Rohen, Lütien-Drecoll, &Yocochi, 2009; Schünke, Schulte, & Schumacher, 2008), cross sec-tional images such as those in the Visible Human Project (Dev & Sen-ger, 2005; Juanes, Prats, Lagándara, & Riesco, 2003) and MagneticResonance Imaging (MRI) (Miles, 2005; Robb & Hanson, 2006), thatprovide limited two-dimensional representations of three-dimen-sional brain structures. As a consequence, students must performcomplex mental reconstructions which require a great cognitiveload that impair neuroanatomy learning (Duncan & Ayache, 2000).Meanwhile, most computer based-instructional material has fo-cused on the development of three-dimensional representations ofanatomical structures (Dev et al., 2002; Drake, McBride, Lachman,
& Pawlina, 2009; Estévez, Lindgren, & Bergethon, 2010; Petersson,Sinkvist, Wang, & Smedby, 2009; Temkin, Acosta, Hatfield, Onal, &Tong, 2002; Temkin, Acosta, Malvankar, & Vaidyanath, 2006). More-over, the usefulness and cost-effectiveness of three-dimensionalrepresentations has been well documented in anatomy learning(Chariker, Naaz, & Pani, 2011; Hilbelink, 2009; McNulty, Sonntag,& Sinacore, 2009; Rizzolo et al., 2006), and students have also shownpreference for the use of three-dimensional representations (Gould,Terrell, & Fleming, 2008; McNulty et al., 2009).
On the other hand, student’s individual visuospatial ability toestablish and handle general spatial relationships cannot be sepa-rated from their ability to comprehend irregular brain structureswith the corresponding spatial arrangements (Fernández, Dror, &Smith, 2011; Guillot, Champely, Batier, Thiriet, & Collet, 2007;Hoyek et al., 2009; Huk, 2006). However, whether visuospatialability is a better predictor than instructional material is still con-troversial (Garg, Norman, & Sperotable, 2001; Ruisoto et al., 2012).Students with poor visuospatial ability may find three-dimensionalrepresentations more attractive since they reduce the cognitiveload of mental reconstruction. Nevertheless, literature is scarceand whether student’s visuospatial ability may influence theirpreference for this three-dimensional instructional material stillneeds to be researched.
Recent progress in information technology and medical imagingcalls for the development of new instructional material that maybe applied to understanding brain activation areas in functionalimages, specially Positron Emission Tomography (PET) images, gi-ven the increasing number of studies using this technique to iden-

P. Ruisoto Palomera et al. / Computers in Human Behavior 31 (2014) 446–452 447
tify brain function and its relevance in the study of neurologicaland psychiatric patients (Abou-Saleh, 2006; Eldaief & Dougherty,2008; MacQueen, 2010; Phillips, 2007; Silén, Wirell, Kvist, Nyland-er, & Smedby, 2008). However, the lack of well-defined spatial ref-erences in functional imaging hinders its interpretation.
To address these problems, the aim of this study was twofold:(a) to develop a computer-based tool for educational use in neuro-anatomy, improving functional image interpretation; and (b) toexamine spatial ability in neuroanatomy students and comparewhether preference for neuroanatomy computer-based resourcesvaried according to their visuospatial ability.
2. Materials and methods
2.1. Participants
The sample consisted of 65 volunteers recruited from the Uni-versity of Salamanca in Spain (35 females and 30 males). Ages ran-ged from 23 to 29 at the beginning of the study (M = 24.8 + 1.21).Eligibility criteria required them to be enrolled in a medical under-graduate anatomy course. All participants gave their informed con-sent to take part in the study and did not receive any compensationfor their participation.
2.2. Procedure and outcome measures
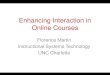
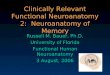
MRI and PET scans were acquired from a 41 year-old healthyright handed normal male volunteer with no history of brain orvascular disease. Morphological T1 weighted neuro-MRI scanswere carried out on a (1.5 T) Phillips Medical System scanner(Fig. 1), and functional PET scans on a Phillips Medical Systemscanner using the two most common tracers in research and med-
Fig. 1. Brain images used in the study. From top to bottom: morphological MRI, functionthree orthogonal planes: axial, coronal and sagittal.
ical care: fluorine-18 (18F) fluorodeoxyglucose (FDG), called18F-FDG-PET images, and 18-fluoro-L-DOPA, called 18F-DOPA-PETimages (Fig. 1). All sectional images were obtained in DigitalImaging and Communications in Medicine (DICOM) format. Priorto commencing, ethical clearance was sought from local ethicscommittee following the principles established in the Declarationof Helsinki.
2.2.1. Development of three-dimensional brain structurerepresentations
High quality three-dimensional models of superficial and sub-cortical brain structures were developed using the Amira™ soft-ware program, version 5.3 (Mercury Computer Systems/TGS, SanDiego, CA). The process started with the bilateral segmentation ofregions of interest (ROI) for every structure from MRI sections. ROIswere defined for each brain structure according to their visibleedges, shape, size, and location under the supervision of an expertneuroanatomist. A unique label field like ‘‘lateral ventricle’’ or‘‘putamen’’ was added to each ROI creating a list of brain struc-tures. Then, an intermediate polygon surface mesh was createdfor each brain structure using the marching cubes algorithm(Pommert, Tiede, & Höhne, 2002). Finally, three-dimensional mod-els were exported to Direct X format (3D Exploration software,Right Hemisphere Inc., Auckland, New Zealand).
2.2.2. Co-registration of three-dimensional models and functionalimages
Co-registration consisted in unifying information in data setsfrom the two image modalities used in the study, MRI and PET,which were obtained using craniometric landmarks as parametersguaranteeing the same angle of acquisition. Mutual informationwas also maximized by aligning and adjusting position and orien-
al 18F-FDG-PET and 18F-DOPA-PET. From left to right: examples of sections in the

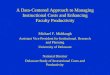
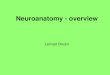
Fig. 2. Example of stimulus item used in Yela’s visuospatial test (reproduced with permission from Yela Desarrollo de Superficies/L.L. Thurstone, Adaptación M. Yela, 1st ed.,1969, 12 p., ™Técnicos Especialistas Asociados).
448 P. Ruisoto Palomera et al. / Computers in Human Behavior 31 (2014) 446–452
tation of MRI, 18FDG-PET and 18F-DOPA-PET images. As a result,three-dimensional models created from morphological MRI imagescan be embedded in functional PET images, where more activatedareas show up in brighter colors, but no clear edges required forsegmentation are visible.
2.2.3. Anatomical and functional viewerFinally, an anatomical and functional viewer was created using
Visual C and ActiveX controls for Windows™ platforms. Thisapplication supported two types of graphic elements: (1) three-dimensional models of brain structures and (2) simultaneous dis-play of sectional functional images in the three-orthogonal spaceplanes (sagittal, axial and coronal).
2.2.4. Evaluation of student’s perception of the anatomical andfunctional viewer’s educational value
Participants were asked to anonymously complete an onlinerating-scale to measure the educational value that they assignedto the viewer after exploring it for 10 min individually. This surveyconsisted of four items: Item #1 stated: ‘‘Interactive visualizationof brain structure three-dimensional models facilitates a betterunderstanding of spatial relationships within the brain than con-ventional printed material, including cross-sectional brainimages’’. Item #2: ‘‘Interactive visualization of three-dimensionalmodels embedded in functional images facilitates a better identifi-cation of activation areas in the brain than exploration of sectionalimages alone’’. Item #3: ‘‘This viewer offers a high-value educa-tional tool for learning neuroanatomy’’. Item #4: ‘‘This viewer of-fers a high-value educational tool for accurately interpretingbrain activation areas in functional images’’. Participants answeredaccording to the following seven point Likert-type scale (range:1–7): 1 – ‘‘totally disagree’’, 2 – ‘‘strongly disagree’’, 3 – ‘‘partiallyor somewhat agree’’, 4 – ‘‘neither agree nor disagree’’, 5 – ‘‘partiallyor somewhat disagree’’, 6 – ‘‘strongly agree, and 7 – ‘‘totally agree’’.
2.2.5. Evaluation of student’s visuospatial aptitudeFinally, participants completed a computerized version of the
Surface Development Test (Yela, 1969), originally developed byThurstone (1938), to measure their visuospatial ability. The taskconsisted of an association between letters on a concrete surfacein a three-dimensional figure and between numbers in a two-dimensional geometric image corresponding with the develop-ment of its surface. This test contained 12 items and the maximumcompletion time was 14 min. An example item is shown in Fig. 2.
2.3. Statistical analysis
Data management and analysis was performed using SPSS sta-tistical package, version 18.0 for Windows (SPSS Inc., Chicago, IL).Participants were divided into two groups based on their perfor-mance on the computerized version of Yela’s test (Yela, 1969):High visuospatial ability group, if scores were higher than the50th percentile; and low visuospatial ability group, if scores werelower than the 50th percentile. The participant with a score equalto the 50th percentile was excluded from the study. Comparisonsin educational value perceptions between the students with highand low visuospatial ability were made using independent Studentt-tests. Significance level (P) was set at 0.01 using the Student t-test.
3. Theory/calculation
The Cognitive Load Theory (CLT) refers to the application oflearning principles in the area of instructional design, especiallyfor complex disciplines or technically challenging learning mate-rial, such as neuroanatomy. According to this theory, studentsmust perform complex mental reconstructions of three-dimensional brain structures when using two-dimensionalsectional images as learning material (Sweller, 1988). To makemental reconstructions, students need to retain and manipulatelarge amounts of information at once, which entails a cognitiveoverload and impairs student’s learning process and motivation(Clark & Mayer, 2007; Clark, Nguyen, & Sweller, 2006). This theoryaims to facilitate complex functional image interpretation fromnew instructional material for learning and teaching neuroanat-omy, and should reduce the cognitive load associated with mentalrepresentations using three-dimensional images of the brain struc-tures involved (Paas, Renkl, & Sweller, 2004), which will optimizestudent’s engagement in the learning process (Paas, Tuovinen,Van Merriënboer, & Darabi, 2005).
4. Results
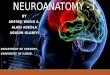
A computer-based viewer was developed for educational pur-poses in neuroanatomy. This viewer enabled the interactive brainstructure study of spatial relationships and of activation areas infunctional images. Particularly, it provides a tool for dynamic scenecomposition and real-time interaction with three-dimensionalbrain structure models and sectional functional images of theiractivity (Fig. 3).
Three-dimensional models provide a complete representationof complex brain structures and show how they are assembled inthe space within the brain (Fig. 3). The viewer included interactive

Fig. 3. Graphical user interface of the computer-based viewer. Right side of the screen shows intuitive graphic controls to interact with three-dimensional models andorthogonal plane cuts corresponding to functional images. [Note: translation of the text (original in Spanish) from top to bottom and left to right: models; show all; hide all;subthalamic nucleus; sustantia nigra; pontine-nuclei; globus pallidus; thalamus; corpus striatum; cerebrum; plane cuts; sagittal; axial; coronal; and activate transparency].
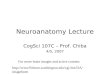
Fig. 4. Presentation of three-dimensional deep brain structure models viewed from different rotation angles showing various activation levels. From left to right: lateral,postero-lateral and posterior view.
Fig. 5. Examples of three-dimensional models for superficial and deep brain structures embedded in DOPA-PET sections (row above) and FDG-PET sections (row below).
P. Ruisoto Palomera et al. / Computers in Human Behavior 31 (2014) 446–452 449
features to (1) select three-dimensional models from a hierarchicallist, allowing individual or group visualization of brain structures
within the scene (Figs. 3–5), (2) rotate the models displayed inthe scene to allow exploration of anatomical details from different

Table 1Statistical analysis of rating-scale scores for participants with high and low visuospatial ability.
Low-visuospatial ability (n = 32) High-visuospatial ability (n = 32) Student’s t-test P value
Item #1 (M + SD) 6.38 (+0.66) 6.16 (+0.68) 1.313 >0.05Item #2 (M + SD) 6.47 (+0.51) 6.34 (+0.60) 0.933 >0.05Item #3 (M + SD) 6.41 (+0.61) 6.13 (+0.79) 1.586 >0.05Item #4 (M + SD) 6.50 (+0.72) 6.19 (+0.82) 1.607 >0.05
450 P. Ruisoto Palomera et al. / Computers in Human Behavior 31 (2014) 446–452
perspectives and angles with and without functional displayedplane cuts, which is done by pressing the left mouse button andmoving the cursor over the scene, and (3) apply transparency to se-lected models to enable the exploration of hidden deep structures(Figs. 4 and 5).
Sectional functional images can be displayed in any of thethree-orthogonal planes of acquisition, and plane position can beshifted using the scrollbar and moving the cursor horizontally.Three-dimensional models embedded in sectional functionalimages provide accurate visual clues for interpreting activationareas within the brain from complex functional images (Fig. 5).Three-dimensional models show the original activation color visi-ble from conventional FDG-PET and DOPA-PET images, but addingextra spatial clues and morphological details.
Finally, rating scale results are displayed in Table 1, which showa profound and positive impact on how students feel about thistool in neuroanatomy learning. Furthermore, students with highvisuospatial ability (M = 23.42 ± 2.29) and low visuospatial ability(M = 19.23 ± 3.76) showed no significant differences in the higheducational value assigned to this tool for learning spatial relation-ships (items 1 and 3) and facilitating functional image interpreta-tion (items 2 and 4).
5. Discussion
This study provides a computer-based tool aimed to increaseavailable resources for neuroanatomy education. It offers a morecomprehensive representation of morphological details, spatialrelationships and brain activation areas than conventional sec-tional images.
This tool is consistent with recent developments in anatomyeducation (Drake et al., 2009; Gómez, Sobreviela, Olivilla, & Juanes,2010; Hansen, 2008; Sugand, Abrahams, & Khurana, 2010; Turney,2007), which have focused on making computer-based three-dimensional representations an effective approach to achieve agood understanding of complex neuroanatomical concepts, giventhe decline in hours devoted to this end in recent years, and thelack of opportunities to directly interact with real anatomical ob-jects (McLachlan, Bligh, Bradley, & Searle, 2004; Parker, 2002).
Three-dimensional reconstructions have already been devel-oped for the study of numerous anatomical structures: cranialnerves (Yeung, Fung, & Wilson, 2011), the inner and middle ear(Nicholson, Chalk, Funnell, & Daniel, 2006), the pelvic girdle(Espuña et al., 2006), and temporal bone (Kockro & Hwang, 2009;Venali, Deveze, Lallemant, Guevara, & Mondain, 2010; Wiet et al.,2002). In fact, this approach has been found to be more effectiveand efficient than conventional learning material. For example,medical students that had access to computer-based learning re-sources scored significantly higher in anatomy exams than thosewho did not (McNulty et al., 2009), and those who accompaniedtheir lectures with a three-dimensional anatomy tutorial scoredsignificantly higher in the final exam, especially in the most com-plex tasks (Venali et al., 2010).
However, some studies have either (1) used few pre-calculatedthree-dimensional views or QuickTime movies simulating
three-dimensional effects (Carmichael & Pawlin, 2000; Elizondo-Omaña et al., 2004; Nieder, Scott, & Anderson, 2000) or (2) usedthree-dimensional representations correlated with morphologicalimages (i.e. MRI or Visible Human Project), which fail to includecomplete three-dimensional clues (Crossingham et al., 2009;Espuña et al., 2006; Nowinski et al., 2009). In contrast, our tooltakes a step further and provides real-time interaction withthree-dimensional models and the possibility to embed them inreal functional images. Results have demonstrated that studentscan easily create any scene composition by rotating, removing orretrieving individual brain structures and/or functional plane cuts,offering powerful graphic clues for the understanding of complexspatial relationships and brain activation areas within the func-tional images.
Basically, two reasons support this approach for enhancing neu-roanatomy education. First, three-dimensional models, like theones provided with this tool, will reduce the cognitive demandsassociated with mental reconstructions from sectional images(Paas et al., 2004; Sweller, 1988). Second, it offers students theopportunity of personal self-directed brain anatomy exploration,which will increase the likelihood of students to actively engagein the learning process (Kirschner, Kester, & Corbalan, 2011; Paaset al., 2005; Venali et al., 2010), and it offers a better understandingof complex neuroanatomical concepts such as spatial relationshipswithin the brain (Chariker et al., 2011; McNulty et al., 2009).
Furthermore, this tool offers an additional advantage, which isto correlate these interactive and high-quality three-dimensionalmodels of real brain structures with complex functional images.By visualizing three-dimensional models embedded in functionalimages, this tool provides additional spatial references that facili-tate the identification of activation areas within the brain (Ruisotoet al., 2012). Hence, this tool may be extremely useful whensearching tumor metastasis since its functional images, PET imagesparticularly, are used for diagnosis, staging, and monitoring treat-ment of cancer (Yasuda et al., 2000).
This paper also enhances the current knowledge regarding stu-dent’s views on computer-based instructional material. Resultshave shown that students assigned a high educational value tothe viewer. This is consistent with previous studies, which pointedout student’s preference for instructional material which includesthe possibility of rotating three-dimensional models (Silén et al.,2008) and multimedia contents in the study of neuroanatomy(Gould et al., 2008). Surprisingly, medical students with higher vis-uospatial ability did not differ significantly from those with lowervisuospatial ability in the educational value assigned to this tool. Itwas expected that students with greater difficulties in handlingspatial relationships, which is necessary to comprehend three-dimensional neuroanatomy images, would consider it more attrac-tive and assign a higher educational value to this tool than thosewho were already skilled in handling spatial relationships. Never-theless, both groups assigned a very high educational value.
Finally, three main limitations of the study must be outlined.First, environmental factors, such as vocational activities involvingspatial skills, were not controlled; second, although the partici-pant’s ages were noted, this factor was not taken into accountwhen analyzing results and may also potentially influence spatial

P. Ruisoto Palomera et al. / Computers in Human Behavior 31 (2014) 446–452 451
ability (Salthouse, Babcock, Skovronek, Mitchell, & Palmon, 1990);and third, participants for this study were all from the University ofSalamanca, and had received the same anatomy teaching, thereforeit might be that this university may teach anatomy differentlywhen compared with other universities, and so, these studentsmay have a higher or lower average score on visuospatial abilityor show a different perception of educational value with this tool.
In the near future, we plan to broaden this tool for online accessand for OS, iOS and android operative systems. Also, studies needto be done in order to evaluate if this computer-based tools reducethe learning curve required by students when acquiring neuroana-tomical concepts.
6. Conclusions
This study provides a computer-based tool which responds tothe increasing need of student centered instructional materialand improves neuroanatomy education. This tool is presented asan interactive anatomical and functional viewer, where studentscan actively manipulate meaningful and understandable represen-tations of brain structures and their spatial relationships, and as away to explore and analyze complex functional images in the samescene, comparable to a simulated cadaver brain dissection experi-ence. Finally, students considered this viewer a tool of great educa-tional value, regardless of their visuospatial ability, and therefore,initial difficulties previously described for managing spatialrelationships.
Acknowledgement
The authors would like to thank the Center of Image and Tech-nology for Biomedical Knowledge (CITEC-B; Madrid) for their tech-nical support.
References
Abou-Saleh, M. T. (2006). Neuroimaging in psychiatry: An update. Journal ofPsychosomatic Research, 61, 289–293.
Carmichael, S. W., & Pawlin, W. (2000). Animated power point as a tool to teachanatomy. The Anatomical Record, 261, 83–88.
Chariker, J. H., Naaz, F., & Pani, J. R. (2011). Computer-based learning ofneuroanatomy: A longitudinal study of learning, transfer, and retention.Journal of Educational Psychology, 103, 19–31.
Clark, R., & Mayer, R. (2007). E-learning and the science of instruction. San Francisco:Pfeiffer.
Clark, R., Nguyen, F., & Sweller, J. (2006). Efficiency in learning: Evidence-basedguidelines to manage cognitive load. San Francisco: Pfeiffer.
Crossingham, J. L., Jenkinson, J., Woolridge, N., Gallinger, S., Tait, G. A., & Multon, C.A. E. (2009). Interpreting three-dimensional structures from two-dimensionalimages: A web-based interactive 3D teaching model of surgical liver anatomy.International Hemato Pancreato Biliary Journal, 11, 523–528.
Dev, P., Montgomery, K., Senger, S., Heinrichs, W. L., Srivastava, A., & Waldron, K.(2002). Simulated medical learning environments on the internet. Journal of theAmerican Medical Informatics Association, 9, 437–447.
Dev, P., & Senger, S. (2005). The visible human and digital anatomy learninginitiative. Studies in Health Technology and Informatics, 111, 108–114.
Drake, R. L., McBride, J. M., Lachman, N., & Pawlina, W. (2009). Medical education inthe anatomical sciences: The winds of change continue to blow. AnatomicalScience of Education, 2, 253–259.
Duncan, J. S., & Ayache, N. (2000). Medical image analysis: Progress over twodecades and the challenges ahead. IEEE Transactions on Pattern Analysis andMachine Intelligence, 22, 85–105.
Eldaief, M., & Dougherty, D. (2008). Advances in neuroimaging: Impact inpsychiatric practice. Psychiatric Times, 25, 1–9.
Elizondo-Omaña, R. E., Morales, J. A., Lopez, S., Leon, I., Patiño, R., & Cavazos, F.(2004). Traditional teaching supported by computer assisted learning formacroscopic anatomy. Anatomical Record (New Anatomist), 278, 18–22.
Espuña, M., Juanes, J. A., Prats, A., Batlle, T., Gómez, J. J., & Iglesias, G. (2006).Modelización virtual de la pelvis femenina a partir de imágenes de resonanciamagnética. Suelo Pélvico, 2, 85–90.
Estévez, M. E., Lindgren, K. A., & Bergethon, P. R. (2010). A novel three-dimensionaltool for teaching human neuroanatomy. Anatomical Sciences of Education, 3,309–317.
Fernández, R., Dror, I. E., & Smith, C. (2011). Spatial abilities of expert clinicalanatomists: Comparison of abilities between novices, intermediates, andexperts in anatomy. Anatomical Science of Education, 4, 1–8.
Garg, A. X., Norman, G., & Sperotable, L. (2001). How medical students learn spatialanatomy. Lancet, 357, 363–364.
Giles, J. (2010). Clinical neuroscience attachments: A student’s view of ‘neuro-phobia’. The Clinical Teacher, 7, 9–13.
Gómez, J. J., Sobreviela, E., Olivilla, F., & Juanes, J. A. (2010). New advances insystems for the visualization and presentation of teaching materials. Tesi, 11,7–27.
Gould, D. J., Terrell, M. A., & Fleming, J. (2008). A usability study of users’ perceptionstowards a multimedia computer-assisted learning tool for neuroanatomy.Anatomical Sciences of Education, 1, 175–183.
Guillot, A., Champely, S., Batier, C., Thiriet, P., & Collet, C. (2007). Relationshipbetween spatial abilities, mental rotation and functional anatomy learning.Advances in Health Sciences Education. Theory and Practice, 12, 491–507.
Hansen, M. M. (2008). Versatile, immersive, creative and dynamic virtual 3-Dhealthcare learning environments: A review of the literature. Medical InternetJournal, 10, 26.
Hilbelink, A. J. (2009). A measure of the effectiveness of incorporating 3D humananatomy into an online undergraduate laboratory. British Journal of EducationTechnology, 40, 664–672.
Hoyek, N., Collet, C., Rastello, O., Fargier, P., Thiriet, P., & Guillot, A. (2009).Enhancement of Mental Rotation Abilities and its Effect on Anatomy Learning.Teaching and Learning in Medicine, 21, 201–206.
Huk, T. (2006). Who benefits from learning with 3D models? The case of spatialability. Journal of Computer Assisted Learning, 22, 392–404.
Juanes, J. A., Prats, A., Lagándara, M. L., & Riesco, J. M. (2003). Application of the‘‘Visible Human Project’’ in the field of anatomy: A review. European Journal ofAnatomy, 7, 147–159.
Kirschner, F., Kester, L., & Corbalan, G. (2011). Cognitive load theory and multimedialearning, task characteristics, and learner engagement: The current state of theart. Computers in Human Behavior, 27, 1–4.
Kockro, R. A., & Hwang, P. Y. (2009). Virtual temporal bone: An interactive 3-dimensional learning aid for cranial base surgery. Neurosurgery, 64, 216–229.
MacQueen, G. M. (2010). Will there be a role for neuroimaging in clinicalpsychiatry? Journal of Psychiatry and Neuroscience, 35, 291–293.
McLachlan, J. C., Bligh, J., Bradley, P., & Searle, J. (2004). Teaching anatomy withoutcadavers. Medical Education, 38, 418–424.
McNulty, J. A., Sonntag, B., & Sinacore, J. M. (2009). Evaluation of computer-aidedinstruction in a gross anatomy course: A six-year study. Anatomical ScienceEducation, 2, 2–8.
Miles, K. A. (2005). Diagnostic imaging in undergraduate medical education: Anexpanding role. Clinical Radiology, 60, 742–745.
Nicholson, D. T., Chalk, C., Funnell, W. R. J., & Daniel, S. J. (2006). A randomizedcontrolled study of a computer-generated three-dimensional model forteaching ear anatomy. Medical Education, 40, 1081–1087.
Nieder, G. L., Scott, J. N., & Anderson, M. D. (2000). Using quicktime virtual realityobjects in computer-assisted instruction of gross anatomy: Yorick-the VR skull.Clinical Anatomy, 13, 287–293.
Nowinski, W. L., Thirunavuukarasuu, A., Volkau, I., Marchenko, Y., Aminah, B., Gelas,A., et al. (2009). A new presentation and exploration of human cerebralvasculature correlated with surface and sectional neuroanatomy. AnatomicalSciences of Education, 2, 24–33.
Older, J. (2004). Anatomy: A must for teaching the next generation. Surgeon, 2(2),79–90.
Paas, F., Renkl, A., & Sweller, J. (2004). Cognitive load theory: Instructionalimplications of the interaction between information structures and cognitivearchitecture. Instructional Science, 32, 1–8.
Paas, F., Tuovinen, J., Van Merriënboer, J. J. G., & Darabi, A. (2005). A motivationalperspective on the relation between mental effort and performance: Optimizinglearners’ involvement in instructional conditions. Educational Technology,Research and Development, 53, 25–33.
Parker, L. M. (2002). Anatomical dissection: Why are we cutting it out? Dissection inundergraduate teaching. Australian & New Zealand Journal of Surgery, 72,910–912.
Petersson, H., Sinkvist, D., Wang, C., & Smedby, Ö. (2009). Web-based interactive 3Dvisualization as a tool for improved anatomy learning. Anatomical Science ofEducation, 2, 61–68.
Phillips, M. L. (2007). The emerging role of neuroimaging in psychiatry:Characterizing treatment-relevant endophenotypes. American Journal ofPsychiatry, 164, 697–699.
Pommert, A., Tiede, H., & Höhne, K. H. (2002). Volume visualization. Brain mapping:The methods. Hamburg: Elsevier.
Rizzolo, L. J., Stewart, W. B., O’Brien, M., Haims, A., Rando, W., Abrahams, J., et al.(2006). Design principles for developing an efficient clinical anatomy course.Medical Teacher, 28, 142–151.
Robb, R. A., & Hanson, D. P. (2006). Biomedical image visualization research usingthe visible human datasets. Clinical Anatomy, 19, 240–253.
Rohen, J. W., Lütien-Drecoll, E., & Yocochi, C. (2009). Atlas de anatomía humana.Barcelona: Elsevier.
Ruisoto, P., Juanes, J. A., Contador, I., Mayoral, P., & Prats-Galino, A. (2012).Experimental evidence for improved neuroimaging interpretation using three-dimensional graphic models. Anatomical Sciences Education, 5, 132–137.
Salthouse, T. A., Babcock, R. L., Skovronek, E., Mitchell, D. R., & Palmon, R. (1990).Ages and experience effects in spatial visualization. Developmental Psychology,26, 128–136.
Schünke, M., Schulte, E., Schumacher, U. (2008). Prometheus, Texto y Atlas deAnatomía. Madrid, Panamericana.

452 P. Ruisoto Palomera et al. / Computers in Human Behavior 31 (2014) 446–452
Silén, C., Wirell, S., Kvist, J., Nylander, E., & Smedby, O. (2008). Advanced 3Dvisualization in student-centred medical education. Medical Teacher, 30,e115–e124.
Sugand, K., Abrahams, P., & Khurana, A. (2010). The anatomy of anatomy: A reviewfor its modernization. Anatomical Sciences Education, 3, 83–93.
Sweller, J. (1988). Cognitive load during problem solving: Effects on learning.Cognitive Science, 12, 257–285.
Temkin, B., Acosta, E., Hatfield, P., Onal, E., & Tong, A. (2002). Web-based three-dimensional virtual body structures: W3D-VBS. Journal of the American MedicalInformatics Association, 9, 425–436.
Temkin, B., Acosta, E., Malvankar, A., & Vaidyanath, S. (2006). An interactive three-dimensional virtual body structures system for anatomical training over theinternet. Clinical Anatomy, 19, 267–274.
Thurstone, L. L. (1938). Primary mental abilities: Psychometric monographs, no. 1 (1sted.). Chicago, IL: University of Chicago Press. 121 p.
Turney, W. (2007). Anatomy in a modern medical curriculum. Annals of the RoyalCollege of Surgeons of England, 89, 104–107.
Venali, F., Deveze, A., Lallemant, B., Guevara, N., & Mondain, M. (2010).Enhancement of temporal bone anatomy learning with computer 3Drendered imaging softwares. Medical Teacher, 32, 282–288.
Wiet, G. J., Stredney, D., Sessanna, D., Bryan, J. A., Wellling, D. B., & Schmalbrock, P.(2002). Virtual temporal bone dissection: An interactive surgical simulator.Otolaryngology: Head Neck Surgery, 127, 79–83.
Yasuda, S., Ide, M., Fujii, H., Nakahara, T., Mochizuki, Y., Takahashi, W., et al. (2000).Application of positron emission tomography imaging for cancer screening.British Journal of Cancer, 83, 1607–1611.
Yela, M. (1969). Manual del test. Desarrollo de superficies (2a ed.). TEA Ediciones,Madrid.
Yeung, J. C., Fung, K., & Wilson, T. D. (2011). Development of a computer-assistedcranial nerve simulation from the visible human dataset. Anatomical Science ofEducation, 4, 92–97.
Zinchuk, A. V., Flanagan, E. P., Tubridy, N. J., Miller, W. A., & McCullough, L. D. (2010).Attitudes of US medical trainees towards neurology education: ‘‘Neuro-phobia’’—A global issue. BMC Medical Education, 10, 49–56.