Embed Size (px)
Citation preview

British Journal of Surgery 1996, 83,516-519
Endovascular repair of abdominal aortic aneurysm: an initial experience A . N A S I M , M . M . T H O M P S O N , R . D . S A Y E R S , A . B O L I A and P . R . F . B E L L
Department of Surgery, Clinical Sciences Building, Leicester Royal Infirmary NHS Trust, Leicester LE2 7LX, UK Correspondence to: Mr A. Nasim
Endovascular repair of abdominal aortic aneurysm (AAA) was attempted in ten patients over a 12-month period. Median age was 72 (range 61-82) years and median AAA diameter was 5.5 (range 5.2-6.0) cm. An aortoaortic (tube) graft was used in seven patients and a tapered aortoiliac reconstruction in three. There were two failures requiring conversion to open repair. Additional procedures included iliac artery angioplasty (two), coil embolization of an associated common iliac aneurysm (one) and femorodistal bypass (one). Median operating time was 162 (range
95-270) min and median blood loss was 1200 (range 800-2000) ml. Median hospital stay was 9 (range 5-21) days. Complications included death (one), reversible acute tubular necrosis (one) and prolonged ventilation (one). Postoperative evaluation with duplex ultrasonography and computed tomography demonstrated three perigraft leaks (two proximal and one distal). It is concluded that endovascular repair of AAA is feasible but is associated with significant complications and requires careful evaluation before widespread use.
Conventional elective abdominal aortic aneurysm (AAA) repair is associated with a mortality ra te of approximately 5 pe r cent in many centres'-'. The risks of conventional repair increase in elderly patients and in those with coexisting cardiorespiratory disease". A n alternative approach to AAA repair involves insertion of a graft- stent combination via a peripheral artery, which is anchored t o ao r t a of normal diameter above a n d below the aneurysm by its expandable metallic stents7. This avoids both laparotomy a n d aortic clamping and may b e a safer alternative in high-risk patientsx. T h e feasibility of this technique was first demonstrated in animal experi- ments"-" and recently several reports of initial clinical experience have emerged'"7. The authors ' early experience with this technique using bo th tube a n d aortoiliac grafts is described.
Patients and methods Patients were assessed before operation by means of computed tomography (CT), magnetic resonance imaging and intra-arterial digital subtraction angiography (with a calibrated catheter). Local ethical committee approval was obtained for this study and all patients gave written consent.
Endovascular grafts The Endovascular Grafting System (Endovascular Technologies, Menlo Park, California, USA) was used in patients who had a sufficient proximal (more than 1.5 cm) and distal (more than 1 cm) aortic cuff to allow a tube graft repair. The catheter delivery system of this device comprises a coaxial unit that consists of a capsule containing the compressed graft, a retractable capsule jacket that permits graft delivery and a movable balloon catheter which is used to fix the stent hooks at the proximal and distal ends of the graft into the aortic wall (Fig. I ) . This catheter-based delivery system is introduced via a 28-Fr sheath placed in the common femoral or iliac artery over a guidewire".
Patients with an insufficient distal aortic cuff or with aortoiliac aneurysm underwent endoluminal placement of a tapered aortoiliac graft combined with a femorofemoral bypass and embolization of the contralateral common iliac artery (Fig. 2). This device consisted of a 4.2-mm diameter, 4-cm long Palmaz stent (Johnson and Johnson, Warren, New Jersey, USA)
Paper accepted 7 July 1995
attached to a tapered polytetrafluoroethylene graft (Impra, Droitwich, UK). The graft-stent combination was mounted on a 3-cm diameter balloon dilatation catheter (Optiplast, Vas-cath, Ontario, Canada). This assembly was loaded into a 21-Fr sheath (Cook, Letchworth, UK) and introduced via a 24-Fr sheath in a manner similar to that of May et al. 14.
Implantation technique The operation was performed under general anaesthesia in a fully equipped vascular operating theatre. All patients received heparin (5000 units) subcutaneously twice daily on the day before the procedure and this was continued until discharge. A further 5000 units heparin were administered intravenously at the start of the procedure. Through a groin incision a longitudinal common femoral arterdotomy was used to introduce the graft-stent combination. A 10-mm diameter Dacron (Meadox, Caddington, UK) graft was sutured end-to-side to the common iliac artery via a retroperitoneal approach in patients with a tortuous or narrowed common femoral artery and used as a temporary conduit as described by Parodi'. Accurate positioning of the endoluminal graft was performed under digital fluoroscopic control (Phillips BVM 29; Phillips Medical Systems, Best, The Netherlands) and stent deployment was aided by balloon inflation for 1 min at 2 atm (approximately 202 kPa) intraluminal pressure. During inflation of the balloon the mean arterial blood pressure was maintained at 80 mmHg. Angiography was performed on completion of the procedure to confirm successful exclusion of the aneurysm sac from the circulation. In patients with tapered aortoiliac grafts, the contralateral common iliac artery was occluded by stainless steel emholization coils (Cook). Retrograde angiography was performed to confirm successful occlusion. The contralateral leg was revascularized with a 10-mm diameter Dacron femoro- femoral crossover graft.
After operation all patients were monitored for 24 h in the intensive care unit. A colour duplex scan and contrast-enhanced CT were performed before discharge from hospital to exclude perianastomotic reflux into the aneurysm sac. All patients were reviewed at 6 weeks and underwent physical examination, plain abdominal radiography, colour duplex scanning and contrast- enhanced CT. This sequence was repeated at 6months and 1 year. Any abnormalities revealed by these investigations were further evaluated with angiography.
Results Over a 12-month per iod f rom March 1994 t o February 1995, 66 patients were assessed fo r endovascular repair;
516 0 1996 Blackwell Science Ltd

ENDOVASCULAR REPAIR O F ABDOMINAL AORTIC ANEURYSM 517
Fig. 1 Radiographic image of a the catheter delivery system containing a compressed graft. Note the radio-opaque markers positioned at the level of proximal and distal aortic cuffs. b Deployment catheter being withdrawn after deployment of the tube graft
seven (11 per cent) were suitable for a straight graft repair. A further 23 (35 per cent) were suitable for a bifurcated graft repair. Endovascular repair was attempted in ten patients (nine men and one woman). Median age was 72 (range 61-82) years and median AAA diameter was 5 5 (range 5.2-6.0) cm. Preoperative risk factors included peripheral vascular disease in five patients, ischaemic heart disease in three, hypertension in two, diabetes mellitus in two and stroke in one. Three of these patients were considered poor candidates for conventional repair.
A tube graft repair was attempted in seven patients and a tapered aortoiliac reconstruction in three. Two patients in the latter group required conversion to an open procedure, one because of an iliac artery perforation produced during sheath insertion and the other because of graft migration from poor proximal fixation to the aortic wall. Both patients were considered ‘fit’ for open surgery which was carried out successfully. A temporary iliac conduit using a Dacron graft was constructed in seven patients to overcome narrow or tortuous common femoral arteries. In two a common iliac artery stenosis was encountered which required angioplasty to facilitate sheath insertion. One of the patients treated with a tube graft also had an isolated right common iliac aneurysm
Fig. 2 Completion angiogram showing a a tapered aortoiliac graft and b coil embolization of the left common iliac artery
which was treated by coil embolization and a left-to-right femorofemoral crossover graft. Median operating time in those undergoing successful endoluminal repair was 162 (range 95-270) min. The patient with the procedure time of 270 min also required a right femorodistal vein bypass graft for rest pain and repair of bilateral, femoral aneurysms. Median blood loss was 1200 (range 800-2000) ml and six of the eight patients undergoing successful endovascular repair required blood transfusion.
Median hospital stay was 9 (range 5-21) days. Complications included death due to bronchopneumonia after microembolization and renal failure (one), reversible acute tubular necrosis (one) and prolonged ventilation (one). The patient who died had a history of myocardial infarction, congestive cardiac failure and stroke. The procedure was uneventful but 12 h after operation he developed an acutely ischaemic right leg requiring embolectomy and fasciotomy. The postoperative course was further complicated by renal failure and death from bronchopneumonia occurred 12 days after the procedure.
Postoperative evaluation with colour duplex ultra- sonography and contrast-enhanced CT demonstrated a proximal leak (Fig. 3 ) in two patients and a distal leak in one. All leaks were encountered after a tube graft repair. One of the proximal leaks had resolved at 6 weeks’ follow- up; the other persisted at 6 weeks. The distal leak was still
0 1996 Blackwell Science Ltd, British Journal of Surgery 1996,83, 516-519

518 A. N A S I M , M. M. T H O M P S O N , R . D . S A Y E R S , A . B O L I A and P . R . F . B E L L
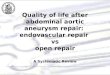
Fig. 3 Intravascular ultrasonographic image of an endoluminal graft showing incomplete seal at the proximal stent site
present at 6 months’ follow-up, but there was no increase in the size of the aneurysm sac.
Discussion Endovascular repair of AAA has been proposed as a less invasive alternative to conventional repair, particularly in patients with coexisting cardiopulmonary disease’. Although reports of initial experience from several centres suggest that this technique is feasible’”’’, various problems have been encountered that need further evaluation before its widespread application.
One of the most serious complications is microemb~lization~~’~. This may cause multiorgan failure in the early postoperative period and is usually fatal. The exact mechanism of microembolization is not known, although it is thought that it may occur during guidewire or endoluminal graft manipulation within the aneurysm sac. This complication was encountered in one patient who died 12 days after the procedure. Balloon inflation at the level of the renal arteries during proximal stent deployment may also be a contributing factor. If the balloon encroaches over renal artery ostia, it may cause atheromatous debris to embolize into the kidney. Another important factor is the amount of contrast medium administered during these procedures. This may account for the transient renal failure in a patient in the present series, who was known to have left renal artery stenosis. The postoperative CT scan in this patient showed the stent to be well clear of the renal arteries.
Incomplete seal at the proximal or distal stent sites was present in three patients and was also encountered by Parodi7, Moore and Vescera15 and Chuter et a1.IH. This results in incomplete exclusion of the aneurysm from the circulation with potential continued aneurysm expansion. The authors’ policy has been to observe these with regular colour duplex and contrast-enhanced CT scanning. Some of these may seal once the stent has been incorporated into the aortic wall. However, if the leak increases in magnitude or if there is an increase in the size of the aneurysm sac, further endovascular intervention or conversion to open repair is indicated. Although animal studies have shown incorporation of the stent into the aortic wall, there is no evidence that this also occurs in the atheromatous human aorta. Failure of stent incorporation may predispose to graft migration in the long term.
Another important problem is that of blood loss during the procedure. A sheath with a haemostatic valve was used for endoluminal tube graft insertion in the present series; despite this, there were considerable blood losses. Blood loss appears to occur mainly during guidewire or catheter exchanges. Blood replacement may increase the incidence of complications, and improvements in both devices and technique are necessary to minimize losses.
Parodi” attempted endovascular aneurysm repair in 6.5 patients between September 1900 and October 1994 with aortoaortic and aortoiliac grafts. He reported initial success in 84 per cent of aortoaortic implantations and in 7.5 per cent of aortoiliac procedures. Complications included microembolization in three patients, with incomplete seal in five (one proximal and four distal) and rupture as a result of a persistent leak in two. Similarly, in a series of 53 endovascular aneurysm repairs, May2” had primary success in 43 patients; ten were converted to open repair due to a combination of stent migration, access problems, balloon malfunction and difficulty with deployment of bifurcated systems. Some SO per cent of patients had vascular complications (femoral artery damage, proximal or distal perigraft leaks); 2.5 per cent had other systemic complications (renal failure, cardiac failure and stroke).
The aforementioned series and the authors’ own early experience show that, although endovascular AAA repair is feasible, it is not without problems. The procedure may be long, complicated and associated with major blood loss. The conversion rate at present is about 1.5-20 per cent and so the technique may not be suitable for unfit patients.
References 1 Fielding JWL, Black J, Ashton F, Slaney G, Campbell DJ.
Diagnosis and management of 528 abdominal aortic aneurysms. BMJ 1981; 283: 355-9.
2 Greenhalgh RM. Prognosis of abdominal aortic aneurysm. BMJ 1996 301: 136. -.
3 Naylor AR, Webb J, Fowkes FGR, Ruckley CV. Trends in abdominal aortic aneurvsm surgerv in Scotland (1972-1984). Eur J Vasc Surg 1988; 2‘217-21: ’
4 Johnston KW. Ruptured abdominal aortic aneurysm: six-year follow-up results of a multicenter prospective study. Canadian Society for Vascular Surgery Aneurysm Study Group. J Vusc Surg 1994; 19: 888-900.
5 Akkersdijk GJM, van der Graaf Y, van Bockel JH, de Vries AC, Eikelboom BC. Mortality rates associated with operative treatment of infrarenal abdominal aortic aneurysm in the Netherlands. Br J Surg 1994; 81: 706-9.
6 Katz DJ, Stanley JC, Zelenock GB. Operative mortality rates for intact and ruptured abdominal aortic aneurysms in Michigan: an eleven-year statewide experience. J Vasc Surg
7 Parodi JC. Endovascular repair of abdominal aortic aneurysms. In: Advances in Vuscular Surgery, Vol. 1. St Louis, Missouri: Mosby Year Book, 1993: 85-106.
8 Sayers RD, Thompson MM, Bell PRF. Endovascular stenting of abdominal aortic aneurysms. Eur J Vasc Surg 1993; 7:
9 Dotter CT. Transluminally-placed coilspring endarterial tube grafts. Long-term patency in canine popliteal artery. Invest Radio1 1969; 4: 329-32.
10 Balko A, Piasecki GJ, Shah DM, Carney WI, Hopkins RW, Jackson BT. Transfemoral placement of intraluminal polyurethane prosthesis for abdominal aortic aneurysm. J Surg Res 1986; 40: 305-9.
11 Lawrence DD Jr, Charnsangavej C, Wright KC, Gianturco C,
1994; 19: 804-15.
225-7.
0 1996 Blackwell Science Ltd, British Journal of Surgery 1996,83, 516-519

E N D O V A S C U L A R R E P A I R O F A B D O M I N A L A O R T I C A N E U R Y S M 519
Wallace S. Percutaneous endovascular graft: experimental evaluation. Radiology 1987; 163: 357-60.
12 Laborde JC, Parodi JC, Clem MF et nl. Intraluminal bypass of abdominal aortic aneurysm: feasibility study. Radiology
13 Parodi JC, Palmaz JC, Barone HD. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann Vasc Surg 1991; 5: 491-9.
14 May J, White G, Waugh R, Yu W, Harris J. Treatment of complex abdominal aortic aneurysms by a combination of endoluminal and extraluminal aortofemoral grafts. J Vasc
15 Moore WS, Vesceta CL. Repair of abdominal aortic aneurysm by transfemoral endovascular graft replacement.
16 Yusuf SW, Baker DM, Chuter TAM, Whitaker SC, Wenham
1992; 184: 185-90.
SUT 1994; 19: 924-33,
Ann Surg 1994; 220: 331-41.
PW, Hopkinson BR. Transfemoral endoluminal repair of abdominal aortic aneurysm with bifurcated graft. Lancet
17 Veith FJ. Transluminally placed endovascular stented grafts and their impact on vascular surgery. J Vasc Surg 1994; 20:
18 Chuter TAM, Wendt G, Hopkinson BR et al. Early clinical experience with bifurcated endovascular grafts for abdominal aortic aneurysm repair. J Endovusc Sum 1995: 2: 126
1994; 344: 650-1.
855-60.
Y
(Abstract). 19 Parodi JC. Limitations of the Parodi device for abdominal
aortic aneurysm exclusion based on four years' experience. JEndovasc Surg 1995; 2: 121-2 (Abstract).
20 May J. Comparison of the Sydney and EVT prosthesis for treatment of aneurysmal disease. J Endovasc Surg 1995; 2: 122 (Abstract).
0 1996 Blackwell Science Ltd, British Journal of Surgery 1996, 83,516-519