Embed Size (px)
DESCRIPTION
n
Citation preview
Functional Endoscopic Sinus Surgery
•
Name:Ali Salman AlHassanName:Ali Salman AlHassan
Academic no.:2061100033Academic no.:2061100033
Introduction
• Functional endoscopic sinus surgeryFunctional endoscopic sinus surgery (FESS) is a surgical modality for some (FESS) is a surgical modality for some diseases of the nose and paranasal sinuses. diseases of the nose and paranasal sinuses. It is the mainstay in the surgical treatment It is the mainstay in the surgical treatment of sinusitis and nasal polyposis, including of sinusitis and nasal polyposis, including fungal sinusitis.fungal sinusitis.
Indications
• Chronic sinusitis refractory to medical Chronic sinusitis refractory to medical treatment treatment
• Recurrent sinusitis Recurrent sinusitis
• Nasal polyposis Nasal polyposis
• Antrochoanal polyps Antrochoanal polyps
• Sinus mucoceles Sinus mucoceles
• Excision of selected tumors Excision of selected tumors
• Cerebrospinal fluid (CSF) leak closure Cerebrospinal fluid (CSF) leak closure
• Orbital decompression (eg, Graves Orbital decompression (eg, Graves ophthalmopathy) ophthalmopathy)
• Optic nerve decompression Optic nerve decompression • Dacryocystorhinostomy (DCR) Dacryocystorhinostomy (DCR) (Operation to relieve blockage of (Operation to relieve blockage of
nasolacrimal duct) nasolacrimal duct)
• Choanal atresia repair Choanal atresia repair
• Foreign body removal Foreign body removal
• Epistaxis controlEpistaxis control
Relevant Anatomy
• ImmediatelyImmediately upon entering the nasal cavity, upon entering the nasal cavity, the first structures encountered are the the first structures encountered are the nasal nasal septum and the inferior turbinate. septum and the inferior turbinate.
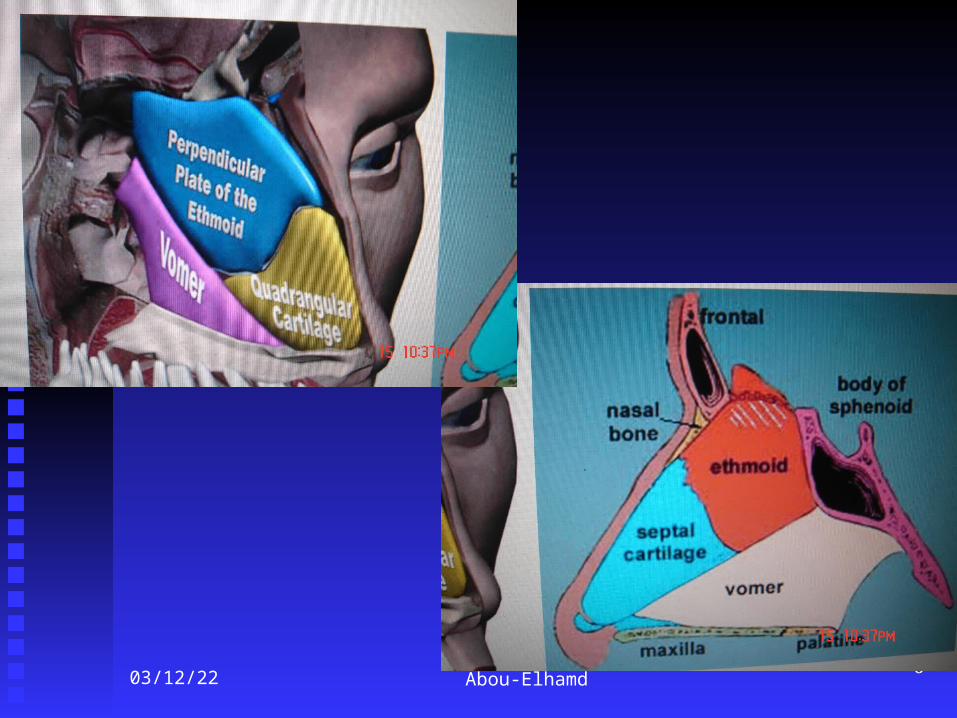
• The nasal septum consists of the quadrangular cartilage The nasal septum consists of the quadrangular cartilage anteriorly, extending to the perpendicular plate of the anteriorly, extending to the perpendicular plate of the ethmoid bone posterosuperiorly and the vomer ethmoid bone posterosuperiorly and the vomer posteroinferiorly. Recognizing deflections of the nasal posteroinferiorly. Recognizing deflections of the nasal septum preoperatively is important because they may septum preoperatively is important because they may significantly contribute to nasal obstruction and limit significantly contribute to nasal obstruction and limit endoscopic visualization during surgery. endoscopic visualization during surgery.
04/18/23 Abou-Elhamd 6
04/18/23 Abou-Elhamd 7
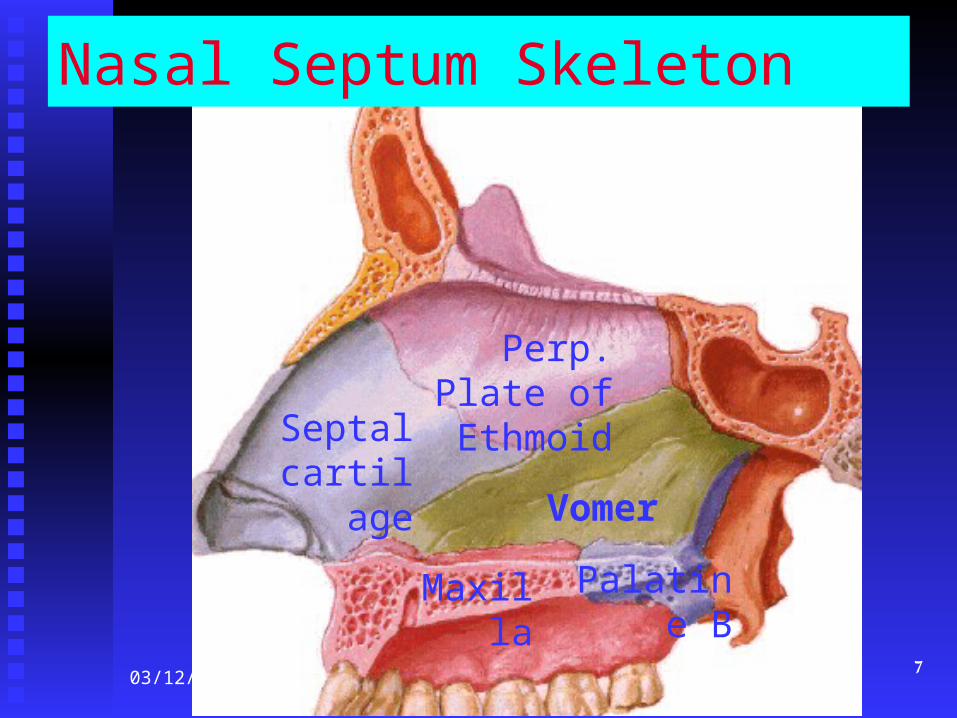
Nasal Septum Skeleton
Perp. Plate of Ethmoid
Septal cartilage
Vomer
Maxilla Palatine B
• The inferior meatusThe inferior meatus, where the nasolacrimal , where the nasolacrimal duct opens, is located approximately duct opens, is located approximately 1 cm 1 cm beyond the most beyond the most anterior edge of the inferior anterior edge of the inferior turbinate.turbinate.
• As the endoscope is further advanced into As the endoscope is further advanced into the nose, the nose, the next structure the next structure encountered is encountered is the middle turbinatethe middle turbinate. The middle turbinate . The middle turbinate is is a key landmarka key landmark in endoscopic sinus surgery. in endoscopic sinus surgery.
04/18/23 Abou-Elhamd 9
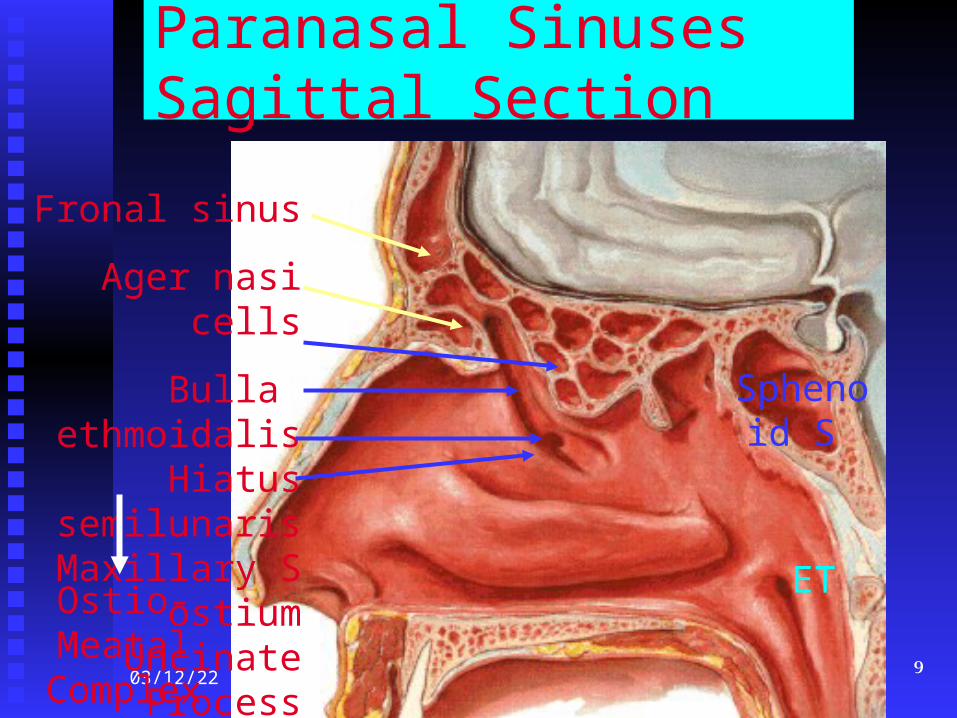
Paranasal Sinuses Sagittal Section
Fronal sinus
Ager nasi cells
Bulla ethmoidalis Hiatus semilunaris
Maxillary S ostium Uncinate Process
Ostio-Meatal Complex
Sphenoid S
ET
• Superiorly,Superiorly, the middle turbinate attaches to the middle turbinate attaches to the skull base at the cribriform plate. the skull base at the cribriform plate. As such, As such, care care should always be taken when should always be taken when manipulating the middle turbinate. The manipulating the middle turbinate. The horizontal component of the middle turbinate horizontal component of the middle turbinate is referred to as the basal (or grand) lamella, is referred to as the basal (or grand) lamella, and it represents the dividing point between and it represents the dividing point between anterior and posterior ethmoid air cells. anterior and posterior ethmoid air cells.
• Posteriorly and inferiorlyPosteriorly and inferiorly, the middle , the middle turbinate attaches to the lateral nasal wall at turbinate attaches to the lateral nasal wall at the crista ethmoidalis, just anterior to the the crista ethmoidalis, just anterior to the sphenopalatine foramen.sphenopalatine foramen.
maxillary sinus
• The uncinate process is the next key The uncinate process is the next key structure to be identified in endoscopic sinus structure to be identified in endoscopic sinus surgery. This L-shaped bone of the lateral surgery. This L-shaped bone of the lateral nasal wall forms the anterior border of the nasal wall forms the anterior border of the hiatus semilunaris, or the infundibulum. The hiatus semilunaris, or the infundibulum. The infundibulum is the location of the infundibulum is the location of the ostiomeatal complexostiomeatal complex, where the natural , where the natural ostium of the maxillary sinus opens.ostium of the maxillary sinus opens.
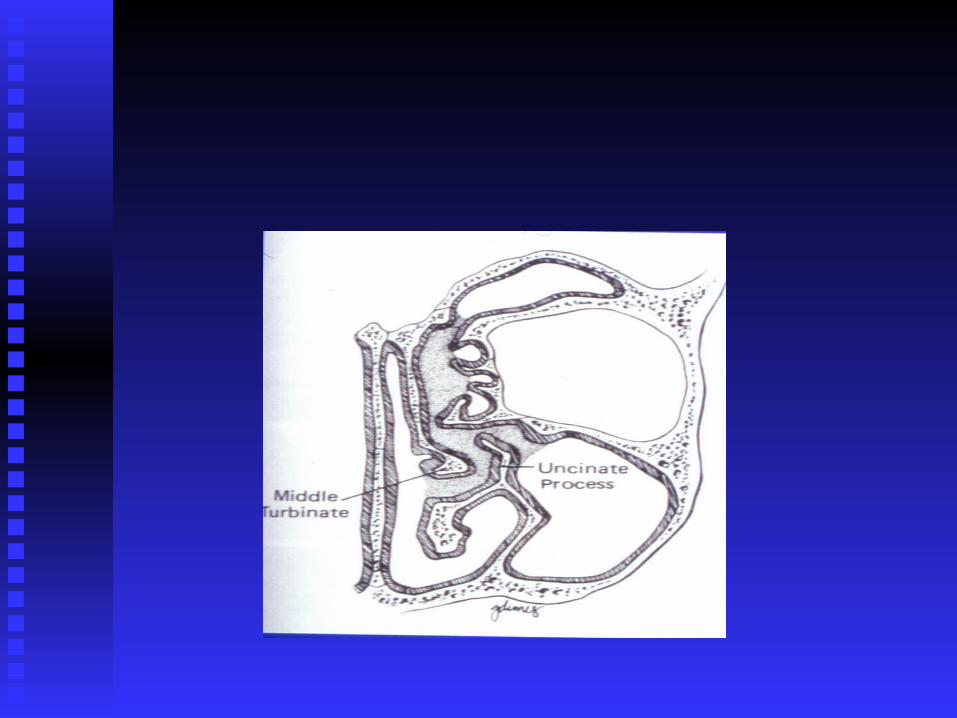
• For patients with sinus disease, a patent ostiomeatal For patients with sinus disease, a patent ostiomeatal complex is critical for an improvement of complex is critical for an improvement of symptoms. symptoms. AnteriorlyAnteriorly, the uncinate process attaches , the uncinate process attaches to the to the lacrimal bonelacrimal bone, and, , and, inferiorlyinferiorly, the uncinate , the uncinate process attaches to the process attaches to the ethmoidal process of the ethmoidal process of the inferior turbinateinferior turbinate. Once the uncinate process is . Once the uncinate process is removed, the natural maxillary ostium can be seen. removed, the natural maxillary ostium can be seen. It lies at It lies at level of the inferior border of the middle level of the inferior border of the middle turbinate, superior to the inferior turbinate.turbinate, superior to the inferior turbinate.
• The natural maxillary ostium is the destination The natural maxillary ostium is the destination for the mucociliary flow within the maxillary for the mucociliary flow within the maxillary sinus. sinus. Therefore,Therefore, for optimal results, the for optimal results, the surgically enlarged surgically enlarged maxillary antrostomy must maxillary antrostomy must include the natural ostium. include the natural ostium.
• failure to include the maxillary ostium failure to include the maxillary ostium in in endoscopic surgical antrostomy is one of the endoscopic surgical antrostomy is one of the key patterns of key patterns of failure in functional endoscopic failure in functional endoscopic sinus surgery. sinus surgery.
• The maxillary sinusThe maxillary sinus, approximately 14-15 , approximately 14-15 mL in mL in volumevolume, is bordered , is bordered superiorlysuperiorly by the by the inferior orbital wall, inferior orbital wall, mediallymedially by the lateral by the lateral nasal wall, and nasal wall, and inferiorlyinferiorly by the alveolar by the alveolar portion of the maxillary bone.portion of the maxillary bone.
• The The nextnext structure to be encountered is the structure to be encountered is the ethmoid bullaethmoid bulla, which is one of the most , which is one of the most constant anterior ethmoidal air cells. It is constant anterior ethmoidal air cells. It is just beyond the natural ostium of the just beyond the natural ostium of the maxillary sinus and forms the posterior maxillary sinus and forms the posterior border of the hiatus semilunaris.border of the hiatus semilunaris.
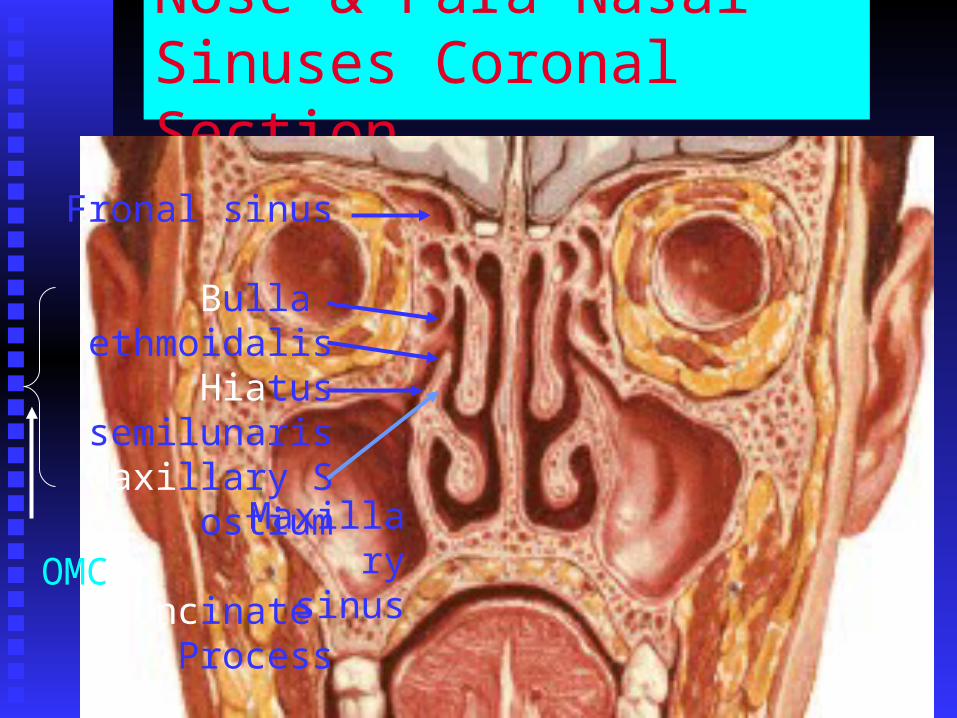
Nose & Para Nasal Sinuses Coronal Section
Fronal sinus
Bulla ethmoidalis Hiatus semilunaris
Maxillary S ostium
Uncinate Process Maxillary
sinusOMC
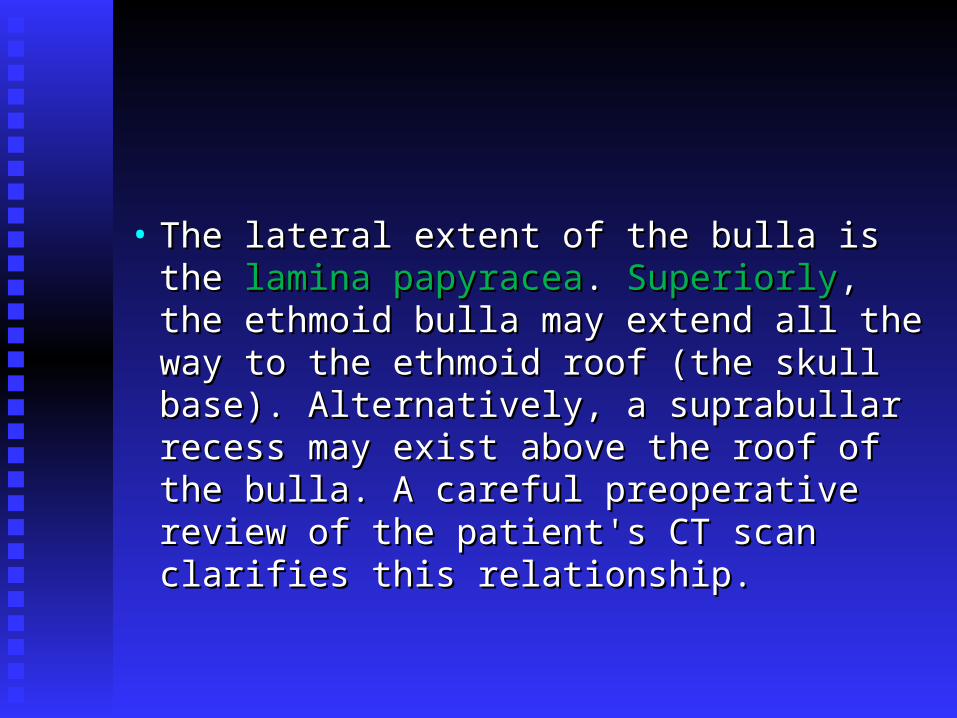
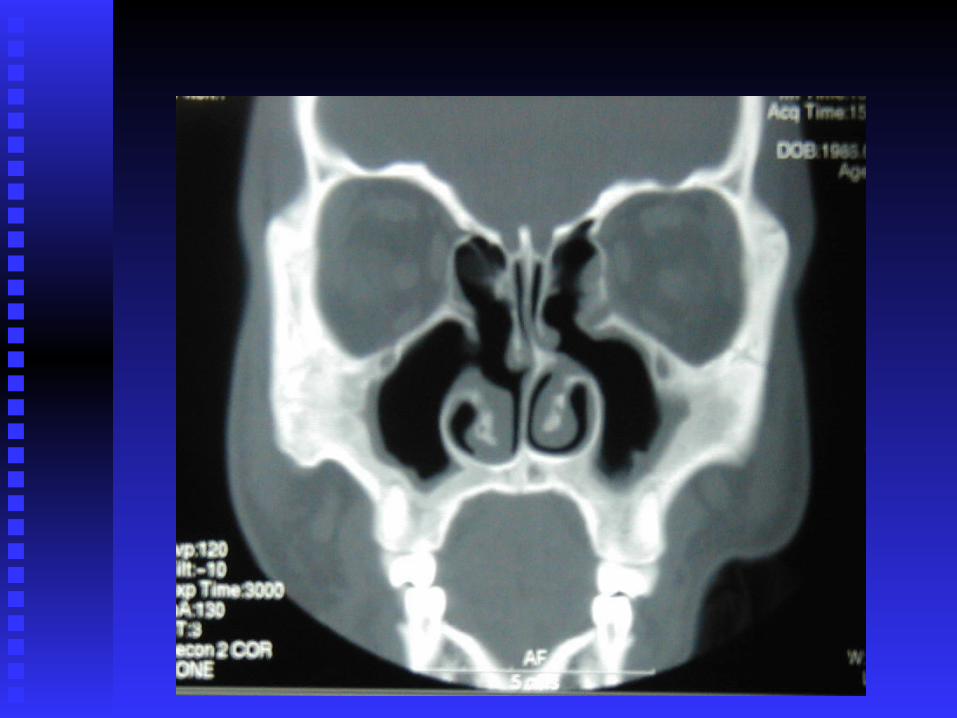
• The lateral extent of the bulla is the The lateral extent of the bulla is the laminalamina papyraceapapyracea. . SuperiorlySuperiorly, the ethmoid bulla , the ethmoid bulla may extend all the way to the ethmoid roof may extend all the way to the ethmoid roof (the skull base). Alternatively, a suprabullar (the skull base). Alternatively, a suprabullar recess may exist above the roof of the bulla. recess may exist above the roof of the bulla. A careful preoperative review of the A careful preoperative review of the patient's CT scan clarifies this relationship.patient's CT scan clarifies this relationship.
The ethmoid sinus
• consists of a variable number (typically 7-consists of a variable number (typically 7-15) of air cells. The most 15) of air cells. The most laterallateral border of border of these air cells is the these air cells is the lamina papyracealamina papyracea, and , and the most the most superiorsuperior border of these cells is the border of these cells is the skull base. Supraorbital ethmoid cells may skull base. Supraorbital ethmoid cells may be present. A review of the patient's CT be present. A review of the patient's CT scan alerts the surgeon to these variations.scan alerts the surgeon to these variations.
• The basal lamella of the middle turbinate The basal lamella of the middle turbinate separates the anterior ethmoid cells from separates the anterior ethmoid cells from the posterior ethmoid cells. the posterior ethmoid cells. Anterior Anterior ethmoid ethmoid cells drain to the cells drain to the middle meatusmiddle meatus, , and the and the posterior cells posterior cells drain into the drain into the superior meatus.superior meatus.
• ExenterationExenteration of the posterior ethmoid cells of the posterior ethmoid cells leads to the face of the leads to the face of the sphenoidsphenoid. The . The sphenoid sinus is the most posterior of the sphenoid sinus is the most posterior of the paranasal sinuses, sitting just superior to the paranasal sinuses, sitting just superior to the nasopharynx and just anterior and inferior nasopharynx and just anterior and inferior to the to the sella turcicasella turcica..
sphenoid sinus.
• The The internal carotid internal carotid artery is typically the artery is typically the most most posterior and medial impression posterior and medial impression seen seen within the sphenoid sinus. In approximately within the sphenoid sinus. In approximately 7% of cases, the bone is dehiscent. The 7% of cases, the bone is dehiscent. The opticoptic nervenerve and its bony encasement and its bony encasement produce an produce an anterosuperioranterosuperior indentation indentation within the roof of the sphenoid sinus.within the roof of the sphenoid sinus.
• The The locationlocation of the of the natural ostium natural ostium of the of the sphenoid sinus is sphenoid sinus is variablevariable; approximately ; approximately 60%60% are located are located medial to the superior medial to the superior turbinateturbinate, and , and 40% are 40% are located located lateral to the lateral to the superior turbinate.superior turbinate.
frontal sinus
• The frontal recess, or the frontal outflow The frontal recess, or the frontal outflow tract, is the tract that leads from the frontal tract, is the tract that leads from the frontal sinus into the nasal cavitysinus into the nasal cavity
• Often, the Often, the ethmoid bullaethmoid bulla is the is the posteriorposterior borderborder of the frontal sinus outflow tract. of the frontal sinus outflow tract. AnteriorlyAnteriorly, the frontal sinus outflow tract is , the frontal sinus outflow tract is bordered by the bordered by the uncinateuncinate process or the agger process or the agger nasi cells (frontal anterior ethmoid air cells).nasi cells (frontal anterior ethmoid air cells).
• If any of these cells are enlarged or if If any of these cells are enlarged or if scarring is present from a previous surgery, scarring is present from a previous surgery, resultant outflow tract obstruction, leading resultant outflow tract obstruction, leading to frontal sinusitis, may occur. Typically, to frontal sinusitis, may occur. Typically, the the medialmedial wallwall of the of the frontalfrontal recessrecess is is formed by the formed by the laminalamina papyraceapapyracea..
Contraindications
• Certain conditions may require an external Certain conditions may require an external approach for complete treatment of disease; approach for complete treatment of disease; these include:these include:
• intraorbitalintraorbital complicationscomplications ofof acuteacute sinusitissinusitis, , such as orbital abscess or frontal osteomyelitis such as orbital abscess or frontal osteomyelitis with Potts puffy tumor. An open approach in with Potts puffy tumor. An open approach in these instances, with or without additional these instances, with or without additional endoscopic assistance, may be preferable. endoscopic assistance, may be preferable.
• After 2 failures After 2 failures to to endoscopically manage endoscopically manage CSF leaks associated with CSF rhinorrheaCSF leaks associated with CSF rhinorrhea, , patients should be referred to a patients should be referred to a neurosurgeon for closure using a neurosurgeon for closure using a neurosurgical approach.neurosurgical approach.
Complications
• Bleeding Bleeding • Synechiae formation Synechiae formation • Orbital injury Orbital injury • Diplopia Diplopia • Orbital hematoma Orbital hematoma • Blindness Blindness • CSF leak CSF leak • Direct brain injury Direct brain injury • Nasolacrimal duct injury/epiphora Nasolacrimal duct injury/epiphora (watering of the eye)(watering of the eye)
Outcome and Prognosis
• Outstanding short- and long-term results Outstanding short- and long-term results have been reported. have been reported. In one study, symptoms In one study, symptoms improved in 66 of 72 patientsimproved in 66 of 72 patients following following endoscopic sinus surgery, with a endoscopic sinus surgery, with a mean mean follow-up time of 7.8 years.follow-up time of 7.8 years. In In anotheranother report, quality of life report, quality of life improvedimproved for for 85%85% of of the patient population, with a the patient population, with a meanmean follow-follow-upup timetime of 31.7 months.of 31.7 months.
Thank you








![Visual Computing for ENT Surgery Planningsphenoidalis,Blue: Sinus frontalis,Green: Sinus ethmoidalis (From:[Krüger et al.,2008]). 20.2 PLANNING AND TRAINING ENDOSCOPIC SINUS SURGERY](https://img.dokumen.tips/doc/110x75/607b2ddb357dfe4b8125856c/visual-computing-for-ent-surgery-planning-sphenoidalisblue-sinus-frontalisgreen.jpg)




















