Embed Size (px)
Citation preview

Journal of Gastroenterology and Hepatology (2001) 16, 513–518
METHODS
Patients
The subjects in the present study were 57 endoscopi-cally confirmed duodenitis patients with or without H. pylori-associated gastritis. Twenty-seven patients (26males and one female; median age 44.4 years; range25–64 years) were H. pylori positive in their stomach(Hp-positive) and 30 patients (22 males and eightfemales; median age 43.1 years; range 19–71 years)were H. pylori negative (Hp-negative).
Patients who had: (i) evidence of a gastric or duode-nal ulcer or scar on endoscopy; (ii) Zollinger–Ellisonsyndrome or Crohn’s disease involving the duodenum;(iii) chronic liver disease or renal insufficiency; (iv)
INTRODUCTION
There have been many studies and several differentclassifications presented concerning the endoscopiccharacteristics of duodenitis since the advent of fiber-optic endoscopy.1–5 After publication of the SydneySystem,6 discussion of the occurrence of endoscopicgastritis and duodenitis based on the same classificationhas become possible.
In this study, we investigated the histological findingsof the stomach and duodenal bulb in patients withendoscopic duodenitis (bulbitis) with or without Heli-cobacter pylori-associated gastritis, with special attentionto the presence of gastric metaplasia (GM). We furtherstudied the extent and type of GM, and changes in GMafter eradication of the bacteria.
PEPTIC ULCER DISEASE: DIETARY FACTORS, ITS REPAIR ANDRELATIONSHIP WITH HELICOBACTER PYLORI INFECTION
Endoscopic duodenitis, gastric metaplasia and Helicobacter pylori
YOSHIHITO URAKAMI* AND TOSHIAKI SANO†
*Department of Gastroenterology, Urakami Gastro Clinic and †Department of Pathology,TokushimaUniversity, School of Medicine,Tokushima, Japan
AbstractBackground and Aims: The purpose of this study was to investigate the relationship between gastricmetaplasia and Helicobacter pylori in patients with endoscopic duodenitis.Methods: The subjects were 57 patients with endoscopic duodentitis with or without H. pylori-associated gastritis. Biopsy specimens were obtained from the stomach and duodenal bulb to assess thehistological findings and H. pylori infection. Gastric metaplasia was divided into three types: com-plete, intermediate and incomplete, according to the amount of mucus in the metaplastic cells. In 10H. pylori-positive patients, endoscopic and histological findings of duodenitis were compared before andafter eradication of the bacteria.Results: There was no significant difference in the extent of gastric metaplasia or the appearance andseverity of endoscopic duodenitis between H. pylori-positive and -negative groups. The complete typeof gastric metaplasia was frequently detected in the H. pylori-negative group, whereas the incompletetype was frequently observed in the H. pylori-positive group. After eradication of H. pylori, the incom-plete type changed to the complete type with a decrease of histological inflammation.Conclusions: The complete type of gastric metaplasia occurred frequently without H. pylori infection,whereas the incomplete type was frequently associated with H. pylori infection.© 2001 Blackwell Science Asia Pty Ltd
Key words: duodenitis, endoscopy, gastric metaplasia, Helicobacter pylori.
Correspondence: Dr Y Urakami, Urakami Gastro Clinic, 2–2-2 Kitaokinosu, Tokushima 770-0872, Japan.Accepted for publication 22 January 2001.

received non-steroidal anti-inflammatory drugs(NSAIDs) or who had acid-suppression treatment ortaken antibiotics in the previous month; or (v) previousgastric surgery were excluded.
Clinical procedures
Endoscopic findings on duodenal morphology weredefined according to the criteria of endoscopic duo-denitis described by the Sydney classification,6 includ-ing the subjective assessment of severity as mild,moderate or severe. The findings were then classifiedinto erythematous, erosive, nodular or hemorrhagicduodenitis. Endoscopy was performed by one endo-scopist with 30 years experience.
Three duodenal biopsies were performed from theendoscopically observed pathologic lesion showing aerythematous, erosive or nodular lesion in all patients.Three specimens obtained from the duodenum wereplaced in 10% buffered formalin and processed for histological examination.
Two paired biopsies were taken from the greater cur-vature of the gastric antrum and of the gastric corpusat the same time. Of the two paired biopsies, one wasused for a rapid urease test and the other was alsoplaced in 10% buffered formalin for histological exami-nation of gastritis and confirmation of H. pylori.
The H. pylori status was determined by using therapid urease test and histology. A patient was classifiedas being Hp-positive when both the urease test and his-tology were positive. When H. pylori was negative onboth the rapid urease test and histological examination,and the immunoglobulin (Ig)G antibody to H. pyloriwas negative in serum samples using an ELISA, apatient was classified as being Hp-negative.
Among the 27 endoscopic duodenitis patients whowere Hp-positive, 10 received triple therapy consistingof 30 mg/day lansoprazole, 1.5 g/day amoxicillin and500 mg/day metronidazole for 1 week for eradication ofH. pylori. The 10 patients underwent endoscopy again10 weeks after treatment. Three duodenal biopsies andtwo paired gastric biopsies were repeated, and weretaken from a topographic site similar to that in theinitial endoscopy. Endoscopic appearance and histologi-cal findings of duodenal inflammation were comparedbefore and after eradication of H. pylori.
Informed consent was obtained from all patients whoparticipated in the present study.
Histological methods
Duodenal and gastric sections were routinelyprocessed, cut at 3 mm, and stained with hematoxylinand eosin, Alcian blue periodic acid–Schiff, and Giemsastain. Duodenal sections stained with hematoxylin andeosin were used for the histological examination of duodenitis. Alcian blue periodic acid–Schiff was used to identify and assess the extent and degree of GM.Giemsa stain was used to identify the presence of H.pylori in the area of GM. Hematoxylin and eosin
514 Y Urakami and T Sano
staining of gastric biopsy specimens was used for histo-logical examination for gastritis, and Giemsa stain wasused for the detection of H. pylori.
The slides were evaluated by one experienced pathologist who was blinded to clinical, endoscopic andother tests for H. pylori. Gastric biopsy specimens were assessed by using the visual analog scales, as pro-posed by the updated Sydney System.7 Duodenal biopsyspecimens were also assessed by the same system.
In each biopsy specimen, a score from 0 to 3 (normal,mild, moderate or marked, respectively) was assigned toeach of the following morphologic variables: presenceof activity (i.e. the amount of neutrophil infiltration),presence of chronic inflammation (i.e. the amount ofmononuclear cell infiltration), and the presence ofatrophy (i.e. the loss of glandular tissue). The activityand inflammation scores of duodenal specimens werethe highest values in the three specimens obtained fromeach subject. Lymphoid follicles and H. pylori statusamong duodenal biopsy specimens were evaluated asbeing only positive or negative.
The extent of GM was classified according to ourpreviously reported method,8,9 which is as follows:grade 0, no GM observed; grade 1, GM involving a fewvilli; grade 2, GM involving several villi; and grade 3,GM involving almost all villi.
Gastric metaplasia was divided into three typesaccording to the amount of mucus in the metaplasticcells: complete, intermediate and incomplete.The com-plete type of GM was characterized by tall mucin-abundant cells (Fig. 1). In contrast, the incomplete type of GM was dark with cuboidal cells poor in mucin(Fig. 2). Frequently, H.pylori was seen colonizing in thistype of GM. The intermediate type was between thesetwo types.
Statistics
Neutrophil activity and chronic inflammation wereexpressed as mean ± SD. Differences were evaluated by
Figure 1 Complete-type gastric metaplasia. Tall columnarmetaplastic cells are abundant in mucin (hematoxylin andeosin, ¥ 75).

using the Mann–Whitney U-test, Fisher’s exact test,Wilcoxon signed rank test or Kruskal–Wallis test. Pvalues of < 0.05 were considered significant.
RESULTS
Endoscopic findings of duodenitis
In the 27 Hp-positive patients, the following mucosalchanges according to the Sydney classification of endoscopic duodentitis were found: erythematous duodenitis in 17 patients (63%), erosive duodenitis inseven patients (26%), and nodular duodenitis in threepatients (11%). The severity of endoscopic mucosalchanges in the duodenal bulb in this group was cate-gorized as mild in 13 patients (48%), moderate in ninepatients (33%), and severe in five patients (19%).
In the 30 Hp-negative patients, the following findingsof endoscopic duodenitis were observed: erythematousduodenitis in 23 patients (77%), erosive duodenitis insix patients (20%), and nodular duodenitis in onepatient (3%). The severity of endoscopic duodenitis inthis group was categorized as mild in 18 patients (60%),moderate in nine patients (30%) and severe in threepatients (10%).
Gastric metaplasia in endoscopic duodenitis 515
There was no significant difference in the severity ofendoscopic duodenitis between Hp-positive and -nega-tive groups (P = 0.310, Mann–Whitney U-test).
Histological findings of the gastric corpusand duodenal bulb
Table 1 compares the histological findings of the gastriccorpus and duodenal bulb in patients with endoscopicduodenitis between Hp-positive and -negative groups.With regard to gastric corpus, the Hp-positive grouphad significantly higher values for neutrophil activityand chronic inflammation than the Hp-negative group.No difference was found for corpus atrophy. Only twosubjects (Hp-positive patients) were affected by corpusatrophy, but it was only a very mild form.
With regard to the duodenal bulb, histological scoreswere higher in Hp-positive patients than in Hp-negativepatients in terms of neutrophil activity and chronicinflammation. Helicobacter pylori was detected in thearea of gastric metaplasia in 19 Hp-positive patients, butnot in the Hp-negative patients. Lymphoid follicles weredetected in eight Hp-positive patients, but seen in onlyone Hp-negative patient.
Extent of gastric metaplasia betweenHelicobacter pylori-positive and -negative groups
As shown in Table 2, GM was detected in both Hp-positive and -negative groups, but the difference was notsignificant.
Type of gastric metaplasia betweenHelicobacter pylori-positive and -negative groups
One of 27 Hp-positive patients and two of 30 Hp-negative patients were excluded from the present studybecause GM was not present in their biopsy specimens.Therefore, 26 Hp-positive patients and 28 Hp-negativepatients were evaluated to determine the type of GM(Table 3).
Figure 2 Incomplete-type gastric metaplasia. Helicobacterpylori-infected metaplastic cells are smaller and contain alower amount of mucin (hematoxylin and eosin, ¥ 75).
Table 1 Comparison of the histological findings between Helicobacter pylori-positive and -negative groups
Gastric corpus Duodenal bulb Lymphoid neutrophil Chronic Atrophy neutrophil Chronic H. pylori positivity follicles
activity inflammation n (%) activity inflammation n (%) n (%)
H. pylori +ve 1.4 ± 0.7 1.7 ± 0.5 2 (7) 1.7 ± 0.7 2.0 ± 0.3 19 (70) 8 (30)(n = 27) � * � * � * � * � * � † � ‡
H. pylori -ve 0.0 ± 0.0 0.5 ± 0.5 0 (0) 0.3 ± 0.5 1.3 ± 0.5 0 (0) 1 (3)(n = 30)
*P < 0.001 Mann–Whitney U-test. †P < 0.001 Fisher’s exact test. ‡P = 0.010 Fisher’s exact test.
The complete type of GM was seen in one of 26 (4%)Hp-positive patients, whereas it was detected in 20 of28 (71%) Hp-negative patients. In contrast, the incom-plete type of GM was observed in 20 of 26 (77%) Hp-positive patients and in four of 28 (14%) Hp-negativepatients, and the difference was significant (P < 0.001).
Endoscopic findings of duodenitis amongcomplete, intermediate and incomplete typeof gastric metaplasia
In the 21 patients with the complete type of GM, thefollowing mucosal changes of endoscopic duodenitiswere observed; erythematous duodenitis in 18 patients,erosive duodenitis in two patients and nodular duo-denitis in one patient. The severity of endoscopicmucosal changes in the duodenal bulb in this group wasmild in 11 patients, moderate in seven patients andsevere in three patients.
In the nine patients with the intermediate type ofGM, the following findings of endoscopic duodenitiswere noted: erythematous duodenitis in eight patientsand nodular duodenitis in one patient. The severity ofendoscopic duodenitis in this group was mild in fivepatients, moderate in three patients and severe in onepatient.
In the 24 patients with the incomplete type of GM,the following findings of endoscopic duodenitis wereobserved; erythematous duodenitis in 14 patients,erosive duodenitis in eight patients and nodular duo-denitis in two patients.The severity of endoscopic duo-denitis in this group was mild in 14 patients, moderatein seven patients and severe in three patients.
There was no significant difference in the endoscopicfindings of duodenitis (P = 0.390) or in the severity ofendoscopic duodenitis (P = 0.927) among the complete,intermediate and incomplete type of GM.
516 Y Urakami and T Sano
Histological findings of the gastric corpusand duodenal bulb among the complete,intermediate and incomplete types ofgastric metaplasia
Concerning the histological findings in the gastriccorpus, scores of neutrophilic activity were 0.1 ± 0.4,0.9 ± 1.1 and 1.1 ± 0.8 for complete, intermediate andincomplete type of GM, respectively (P < 0.001). Scoresof chronic inflammation were 0.5 ± 0.6, 1.3 ± 0.7 and1.5 ± 0.7 for complete, intermediate and incompletetype of GM, respectively (P < 0.001). There were sig-nificant differences in the histological findings of gastriccorpus among the complete, intermediate and incom-plete type of GM.
On the duodenal bulb, histological scores of neu-trophilic activity were 0.4 ± 0.6, 1.0 ± 1.0 and 1.5 ± 0.9with complete, intermediate and incomplete type ofGM, respectively (P < 0.001). The scores of chronicinflammation were 1.3 ± 0.5, 1.8 ± 0.4 and 1.8 ± 0.5 withcomplete, intermediate and incomplete type of GM,respectively (P = 0.001). There were significant differ-ences in the histological findings of duodenal bulb amongcomplete, intermediate and incomplete type of GM.
Extent of gastric metaplasia among the complete, intermediate and incomplete types
As shown in Table 4, in 21 patients with the complete-type GM, the extent of GM was grade 1 in one patient,grade 2 in 10 patients, and grade 3 in 10 patients. Innine patients with intermediate-type GM, grade 1 wasobserved in six patients, grade 2 in two patients, andgrade 3 in one patient. In 24 patients with the incom-plete-type GM, grade 1 was observed in 17 patients,grade 2 in five patients, and grade 3 in two patients.There were significant differences in the extent of GMamong the groups with complete-, intermediate-, andincomplete-type GM (P < 0.001).
Endoscopic and histological findings ofduodenitis before and after Helicobacterpylori eradication
In the Hp-positive group, 10 patients received success-ful eradication for H. pylori. In these 10 patients, endo-
Table 2 Extent of gastric metaplasia in Helicobacter pylori-positive and -negative groups
Grade 0 Grade 1 Grade 2 Grade 3
H. pylori +ve (n = 27) 1 15 7 4H. pylori -ve (n = 30) 2 9 10 9
P = 0.117 Mann–Whitney U-test.
Table 3 Type of gastric metaplasia in Helicobacter pylori-positive and -negative groups
Complete Intermediate Incomplete
H. pylori +ve (n = 26) 1 5 20H. pylori -ve (n = 28) 20 4 4
P < 0.001 Mann–Whitney U-test.
Table 4 Extent of gastric metaplasia among complete, inter-mediate and incomplete types
Grade 1 Grade 2 Grade 3
Complete (n = 21) 1 10 10Intermediate (n = 9) 6 2 1Incomplete (n = 24) 17 5 2
P < 0.001 Kruskal–Wallis.

scopic and histological findings of duodenitis beforeand 10 weeks after successful eradication were com-pared. The severity of endoscopic duodenitis was mildin two patients, moderate in six patients and severe intwo patients before eradication, but the duodenitis disappeared in one patient, became mild in seven pa-tients and moderate in two patients after eradication (P = 0.034).
Concerning the histological findings in the gastriccorpus, there was a significant decrease in neutrophilicactivity (1.7 ± 0.8 vs 0.0 ± 0.0, P = 0.004) and chronicinflammation (1.7 ± 0.5 vs 0.5 ± 0.5, P = 0.003) beforeand after H. pylori eradication. With respect to duode-nal histology, there was also a significant difference inneutrophilic activity (1.9 ± 0.7 vs 0.0 ± 0.0, P = 0.004)and chronic inflammation (2.0 ± 0.5 vs 1.0 ± 0.5, P =0.004) before and after H. pylori eradication.
The number of patients before eradication in GMgrades 0, 1, 2 and 3 was zero, four, four and two, re-spectively. Ten weeks after eradication therapy, therewere zero, zero, four and six patients with GM grades0, 1, 2 and 3, respectively (Table 5). However, there wasno significant difference in the extent of GM before and after H. pylori eradication (P = 0.057). Among 10patients before eradication therapy, one had complete-type GM, two had intermediate type and seven had the incomplete type. Ten weeks after successful eradi-cation therapy, all 10 patients showed the complete typeof GM (P = 0.005; Table 6). After eradication of H.pylori, GM changed from the incomplete to the com-plete type. Thus, the elimination of the gastric H. pyloriinfection resulted in an increase of the complete type of GM.
Gastric metaplasia in endoscopic duodenitis 517
DISCUSSION
In studies on endoscopic gastritis and duodenitis,the endoscopic findings had been classified by using criteria established by the investigators.1,3,4,5 However,because of the differences in the terminology for endo-scopic findings among studies, a mutual understandingwas difficult.5 After publication of the Sydney System,the description of endoscopic findings of gastritis andduodenitis by common terminology became possible,eliminating observer variation.
In the present study on endoscopic duodenitis, endo-scopic findings were evaluated according to the SydneySystem. Endoscopic findings of duodenitis such as ery-thema, erosions and nodularity were observed in bothHp-positive and -negative groups, but there was no sig-nificant difference in the severity of endoscopic duo-denitis between the groups. These results show thatneither the appearance of endoscopic findings of duo-denitis nor the severity of duodenitis is related to thepresence or absence of H. pylori-associated gastritis. Itis speculated that an acid-pepsin attack is the maincause of the appearance of endoscopic findings of duodenitis, irrespective of the presence or absence of H. pylori-associated gastritis. However, with regard tothe histological findings of duodenitis, the histologicalscores of neutrophil activity and chronic inflammation,H. pylori status and the presence of lymphoid follicleswere significantly higher in the Hp-positive group thanin the Hp-negative group. These findings stronglysuggest that the presence of H. pylori-associated gastri-tis is related to histological duodenitis, but not to theendoscopic appearance or the severity of duodenitis.
Our grading system to estimate the extent of GMclosely resembles the analog grading scales of intestinalmetaplasia in the updated Sydney System proposed by Dixon et al.7 We found GM frequently occurred inendoscopic duodenitis with or without H. pylori-associ-ated gastritis. There was no difference in the incidenceof GM between the two groups, and the extent of GMwas also not significantly associated with H. pylori infec-tion in the stomach.
There are two opposing views about the relationshipbetween the extent of GM and H. pylori. Wyatt et al.10
and Khulusi et al.11 reported that the extent of GM wasrelated to Helicobacter-associated gastritis. In contrast,Noach et al.12 reported that the presence and extent ofGM was not significantly associated with H.pylori infec-tion. Our study showed that the presence and extent ofGM in endoscopic duodenitis is not related to the presence of H. pylori-associated gastritis or duodenalinflammation.Whether H. pylori-associated gastritis waspresent or not, the appearance of metaplasia by itself ismost likely to be caused by duodenal injury13 or highacidity,14 and is considered to be a protective mecha-nism to excess acid.15
We classified GM into three types according to theamount of mucin in the metaplastic cells. When H.pylori is absent in the stomach, complete-type GMappeared in the duodenal bulb, and cellular infiltrationof the duodenal mucosa was mild. Incomplete-typeGM, in contrast with severe histological duodenitis, wasfrequently detected when H. pylori-associated gastritis
Table 5 Extent of gastric metaplasia before and after eradi-cation of Helicobacter pylori (10 cases)
Grade 0 Grade 1 Grade 2 Grade 3
Before eradication 0 4 4 2(n = 10)
After eradication 0 0 4 6(n = 10)
P = 0.057 Wilcoxon.
Table 6 Type of gastric metaplasia before and after eradica-tion of Helicobacter pylori (10 cases)
Complete Intermediate Incomplete
Before eradication 1 2 7(n = 10)
After eradication 10 0 0(n = 10)
P = 0.005 Wilcoxon.
was present. When eradication was achieved, incom-plete GM became well developed and mucin-abundant, reaching the complete-type GM withimproved histological duodenitis.
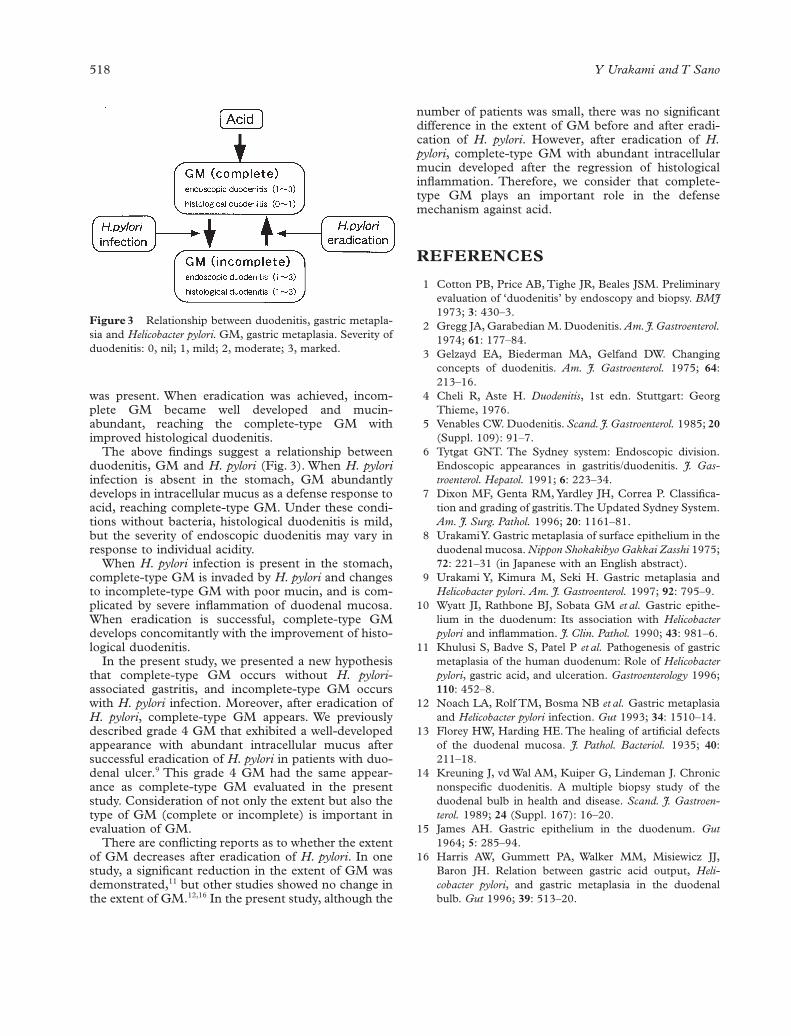
The above findings suggest a relationship betweenduodenitis, GM and H. pylori (Fig. 3). When H. pyloriinfection is absent in the stomach, GM abundantlydevelops in intracellular mucus as a defense response toacid, reaching complete-type GM. Under these condi-tions without bacteria, histological duodenitis is mild,but the severity of endoscopic duodenitis may vary inresponse to individual acidity.
When H. pylori infection is present in the stomach,complete-type GM is invaded by H. pylori and changesto incomplete-type GM with poor mucin, and is com-plicated by severe inflammation of duodenal mucosa.When eradication is successful, complete-type GMdevelops concomitantly with the improvement of histo-logical duodenitis.
In the present study, we presented a new hypothesisthat complete-type GM occurs without H. pylori-associated gastritis, and incomplete-type GM occurswith H. pylori infection. Moreover, after eradication ofH. pylori, complete-type GM appears. We previouslydescribed grade 4 GM that exhibited a well-developedappearance with abundant intracellular mucus aftersuccessful eradication of H. pylori in patients with duo-denal ulcer.9 This grade 4 GM had the same appear-ance as complete-type GM evaluated in the presentstudy. Consideration of not only the extent but also thetype of GM (complete or incomplete) is important inevaluation of GM.
There are conflicting reports as to whether the extentof GM decreases after eradication of H. pylori. In onestudy, a significant reduction in the extent of GM wasdemonstrated,11 but other studies showed no change inthe extent of GM.12,16 In the present study, although the
518 Y Urakami and T Sano
number of patients was small, there was no significantdifference in the extent of GM before and after eradi-cation of H. pylori. However, after eradication of H.pylori, complete-type GM with abundant intracellularmucin developed after the regression of histologicalinflammation. Therefore, we consider that complete-type GM plays an important role in the defense mechanism against acid.
REFERENCES
1 Cotton PB, Price AB, Tighe JR, Beales JSM. Preliminaryevaluation of ‘duodenitis’ by endoscopy and biopsy. BMJ1973; 3: 430–3.
2 Gregg JA, Garabedian M. Duodenitis. Am.J.Gastroenterol.1974; 61: 177–84.
3 Gelzayd EA, Biederman MA, Gelfand DW. Changingconcepts of duodenitis. Am. J. Gastroenterol. 1975; 64:213–16.
4 Cheli R, Aste H. Duodenitis, 1st edn. Stuttgart: GeorgThieme, 1976.
5 Venables CW. Duodenitis. Scand. J. Gastroenterol. 1985; 20(Suppl. 109): 91–7.
6 Tytgat GNT. The Sydney system: Endoscopic division.Endoscopic appearances in gastritis/duodenitis. J. Gas-troenterol. Hepatol. 1991; 6: 223–34.
7 Dixon MF, Genta RM, Yardley JH, Correa P. Classifica-tion and grading of gastritis.The Updated Sydney System.Am. J. Surg. Pathol. 1996; 20: 1161–81.
8 Urakami Y. Gastric metaplasia of surface epithelium in theduodenal mucosa. Nippon Shokakibyo Gakkai Zasshi 1975;72: 221–31 (in Japanese with an English abstract).
9 Urakami Y, Kimura M, Seki H. Gastric metaplasia andHelicobacter pylori. Am. J. Gastroenterol. 1997; 92: 795–9.
10 Wyatt JI, Rathbone BJ, Sobata GM et al. Gastric epithe-lium in the duodenum: Its association with Helicobacterpylori and inflammation. J. Clin. Pathol. 1990; 43: 981–6.
11 Khulusi S, Badve S, Patel P et al. Pathogenesis of gastricmetaplasia of the human duodenum: Role of Helicobacterpylori, gastric acid, and ulceration. Gastroenterology 1996;110: 452–8.
12 Noach LA, Rolf TM, Bosma NB et al. Gastric metaplasiaand Helicobacter pylori infection. Gut 1993; 34: 1510–14.
13 Florey HW, Harding HE. The healing of artificial defectsof the duodenal mucosa. J. Pathol. Bacteriol. 1935; 40:211–18.
14 Kreuning J, vd Wal AM, Kuiper G, Lindeman J. Chronicnonspecific duodenitis. A multiple biopsy study of theduodenal bulb in health and disease. Scand. J. Gastroen-terol. 1989; 24 (Suppl. 167): 16–20.
15 James AH. Gastric epithelium in the duodenum. Gut1964; 5: 285–94.
16 Harris AW, Gummett PA, Walker MM, Misiewicz JJ,Baron JH. Relation between gastric acid output, Heli-cobacter pylori, and gastric metaplasia in the duodenalbulb. Gut 1996; 39: 513–20.
Figure 3 Relationship between duodenitis, gastric metapla-sia and Helicobacter pylori. GM, gastric metaplasia. Severity ofduodenitis: 0, nil; 1, mild; 2, moderate; 3, marked.





























