Embed Size (px)
Citation preview

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 1/8
ENDOCRINOLOGY – DR. ESGUERRA
THYROID GLAND
THYROID DEVELOPMENT
The fetal thyroi ari!e! fro" a# o$t%o$&hi#' of the fore'$t at the (a!e of the to#'$e )fora"e#&e&$"*. It "i'rate! to it! #or"al lo&atio# o+er the thyroi &artila'e (y ,- / 01 of 'e!tatio#. Thethyroi (ilo(e !ha%e i! re&o'#i2e (y 3 01 of 'e!tatio#4 a# &hara&teri!ti& thyroi folli&le &ella# &olloi for"atio# i! !ee# (y / 01.
Thyro'lo($li# !y#the!i! o&&$r! fro" 5 014 io i#e tra%%i#' o&&$r! (y ,- / 014 a# thyro6i#e )T5*a# 4 to a le!!er e6te#t4 triio othyro#i#e )T7* !y#the!i! a# !e&retio# o&&$r fro" 8 01 of 'e!tatio#.
There i! e+i e#&e that !e+eral tra#!&ri%tio# fa&tor!9TT:- ;N<=-8. 4 TT:-8 )al!o ter"e :O=E *4 N<=8.>4a# PA=,9are i"%orta#t i# thyroi 'la# "or%ho'e#e!i! a# i?ere#tiatio#4 a# %o!!i(ly al!o i# it!&a$ al "i'ratio# to it! @#al lo&atio#. The!e fa&tor! al!o (i# to the %ro"oter! of thyro'lo($li# a# thyroi%ero6i a!e 'e#e! a# !o i# $e#&e thyroi hor"o#e %ro $&tio#.
Hy%othala"i& #e$ro#! !y#the!i2e thyrotro%i#-relea!i#' hor"o#e )TRH* (y B-, 014 the %it$itary %ortal+e!!el !y!te" (e'i#! e+elo%"e#t (y ,- / 014 a# thyroi -!ti"$lati#' hor"o#e )TSH* !e&retio# i! e+i e#t(y 8 01 of 'e!tatio#
Maturation of the hypothalamic pituitary-thyroid axis occurs over the second half of gestation, but normalfeedback relationships are not mature until approximately 3 mo of postnatal life. Other transcriptionfactors, including PROP-and Pit- , are important for di!erentiation and gro"th of thyrotrophs, along "ith somatotrophs andlactotrophs
THYROID PHYSIOLOGY )Not i!&$!!e *:$#&tio# of thyroi 'la# i! to !y#the!i2e T5 a# T7
#he only kno"n physiologic role of iodine $or iodide %&'( in its ioni)ed form* is in the synthesis of thesehormonesRDA of io i#e )io i2e *I#fa#t! - 7/ ;1';85hrChil re# – /- 8/ ;1';85hrA ole!&e#t! F a $lt! – >/ ;1';85hr
A%%ro6i"ately o#e-thir of "ater#al T5 &ro!!e! the %la&e#ta a# fet$!
Mater#al T5 %lay! a role i# fetal e+elo%"e#t e!%e&ially that of the (rai#4 (efore the !y#the!i! of fetal thyroi hor"o#e (e'i#!.
At (irth4 there i! a# a&$te relea!e of TSH %ea1 !er$" &o#&e#tratio#! rea&h B/ "U;L 7/ "i#$te!follo0i#' eli+ery i# f$ll-ter" i#fa#t!.
HYPOTHYROIDISM
Most cases of congenital hypothyroidism are not hereditary and result from thyroid dysgenesis+ome cases are familial these are usually caused by one of the inborn errors of thyroid hormonesynthesis (dyshormonogenesis ) and may be associated "ith a goiter
A##
8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 2/8
ENDOCRINOLOGY – DR. ESGUERRA
Thyroi y!'e#e!i! – M cause of permanent congenital hypothyroidism accounting for /- 01 of cases.
A%la!ia4 Hy%o%la!ia4 or a# E&to%i& 'la# Detected by Newborn Screening - 2lood obtained by heel-prick bet"een and 0 days of life is
placed on a 4lter paper card and sent to a central screening laboratory Most infants "ith congenital hypothyroidism are detected by ne"born screening programs in the st
fe" "k after birth, before obvious clinical symptoms and signs develop . &n approximately 33% of cases of dysgenesis, even sensitive radionuclide scans can 4nd no
remnants of thyroid tissue $ aplasia *. &n the other 66% of infants, rudiments of thyroid tissueare found in an ectopic location , any"here from the base of the tongue $ lingual thyroid * to thenormal position in the neck $ hypoplasia* .
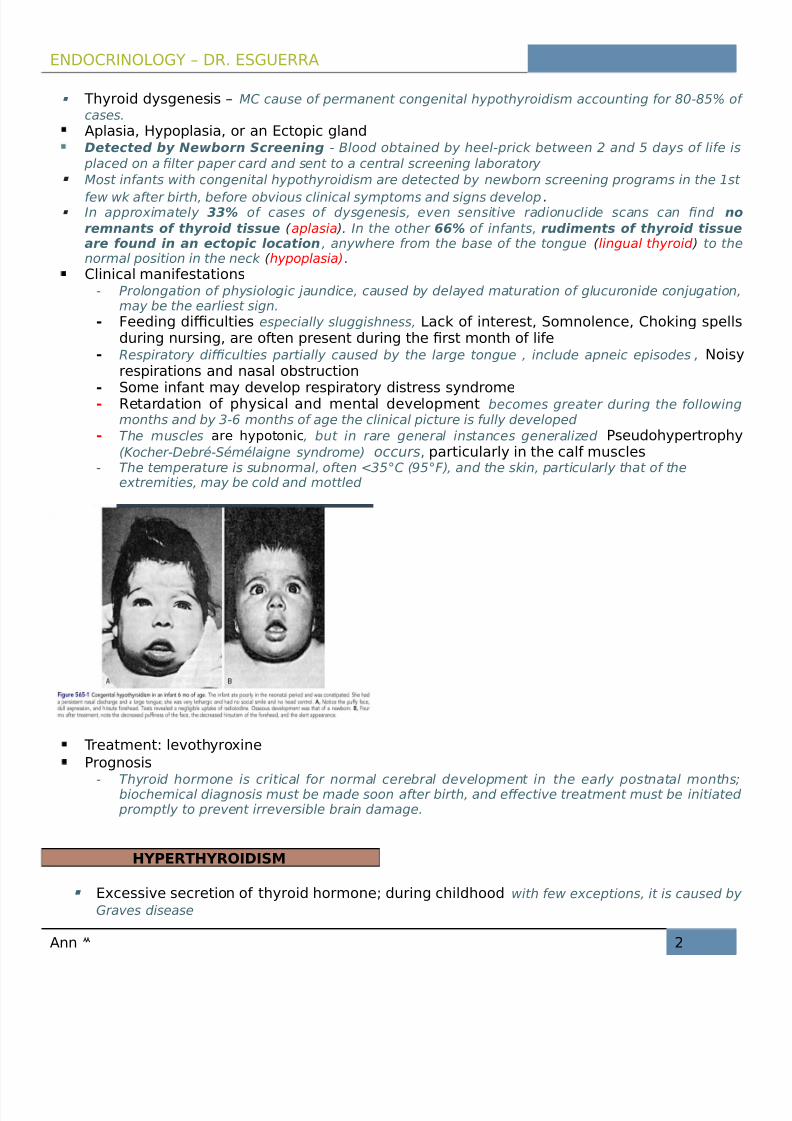
Cli#i&al "a#ife!tatio#!- Prolongation of physiologic 5aundice, caused by delayed maturation of glucuronide con5ugation,
may be the earliest sign.- :ee i#' i &$ltie! especially sluggishness, La&1 of i#tere!t4 So"#ole#&e4 Cho1i#' !%ell!
$ri#' #$r!i#'4 are ofte# %re!e#t $ri#' the @r!t "o#th of life- Respiratory di6culties partially caused by the large tongue , include apneic episodes , Noi!y
re!%iratio#! a# #a!al o(!tr$&tio#
- So"e i#fa#t "ay e+elo% re!%iratory i!tre!! !y# ro"e- Retar atio# of %hy!i&al a# "e#tal e+elo%"e#t becomes greater during the follo"ingmonths and by 3-7 months of age the clinical picture is fully developed
- #he muscles are hy%oto#i& , but in rare general instances generali)ed P!e$ ohy%ertro%hy$8ocher-9ebr:-+:m:laigne syndrome* occurs 4 %arti&$larly i# the &alf "$!&le!
- #he temperature is subnormal, often ;30< $=0<>*, and the skin, particularly that of theextremities, may be cold and mottled
Treat"e#t le+othyro6i#e Pro'#o!i!
- #hyroid hormone is critical for normal cerebral development in the early postnatal monthsbiochemical diagnosis must be made soon after birth, and e!ective treatment must be initiated promptly to prevent irreversible brain damage.
HYPERTHYROIDISM
E6&e!!i+e !e&retio# of thyroi hor"o#e $ri#' &hil hoo "ith fe" exceptions, it is caused by ?raves disease
A## 8

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 3/8
ENDOCRINOLOGY – DR. ESGUERRA
Gra+e ! i!ea!e – ly"%ho&yti& i#@ltratio# of thyroi 'la# is an autoimmune disorder production of thyroid-stimulating immunoglobulin that binds to and activates the ?-protein@coupledthyroid-stimulating hormone (TS ) receptor results in di!use toxic goiter >J of all %atie#t ! 0ith hy%erthyroi i!" are yo$#'er tha# > year! of a'e
Pea1 i#&i e#&e o&&$r! $ri#' a ole!&e#&e #he incidence is approximately 0 times higher ingirls than in boys.
Sy"%to"!- #he earliest signs in children may be emotional disturbances accompanied by motor
Hy%era&ti+ity- Irrita(ility- Altere "oo- I#!o"#ia – restless sleepersA they tend to kick their covers o! - A#6iety- Poor &o#&e#tratio#- Heat i#tolera#&e- I#&rea!e !0eati#'- Pal%itatio#!4 fati'$e- Kea1#e!!4 y!%#ea- Kei'ht lo!! 0ith i#&rea!e a%%etite )0ei'ht 'ai# i# /J of %atie#t!*- Pr$rit$!- I#&rea!e !tool fre $e#&y- Thir!t a# %oly$ria- Oli'o"e#orrhea or a"e#orrhea
A## 7

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 4/8
ENDOCRINOLOGY – DR. ESGUERRA
A## 5

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 5/8
ENDOCRINOLOGY – DR. ESGUERRA
CONGENITAL GOITER
A## >

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 6/8
ENDOCRINOLOGY – DR. ESGUERRA
?oiter is the enlargement of thyroid gland. Persons "ith enlarged thyroids can have normalfunction of the gland (euthyroidism)! thyroid de4ciency (hypothyroidism)! oroverproduction of the hormones (hyperthyroidism)U!$ally !%ora i&"ongenital goiter Re!$lt fro" a fetal T5 !y#theti& efe&t fro" a "i#i!tratio# of
a#ti-thyroi r$'! or io i e! $ri#' %re'#a#&y for treat"e#t of "ater#al thyroto6i&o!i!.?oitrogenic drugs that cross the placenta at high doses can interfere "ith synthesis of thyroidhormone, resulting in goiter and hypothyroidism in the fetusGoiter i! al"o!t al0ay! %re!e#t i# the i#fa#t 0ith #eo#atal Gra+e ! i!ea!e. #hyroidenlargement results from transplacental passage of maternal thyroid-stimulatingimmunoglobulin. #hese goiters usually are not large the infant manifests clinical symptoms of hyperthyroidism. #he mother often has a history of ?raveBs disease, or the diagnosis of maternal ?raves may be revealed through the evaluation of neonatal hyperthyroidism. #+Creceptor@activating mutations are also a recogni)ed cause of congenital goiter andhyperthyroidism
Pendred syndromeD &odine de4ciency
HYPOPARATHYROIDISM
Cypocalcemia is common in neonates bet"een and E hr of life, especially in premature infants,
in infants "ith asphyxia, and in infants of diabetic mothers $early neonatal hypocalcemia* Ffter thend to 3rd day and during the st "k of life, the type of feeding also is a determinant of the level of aserum calcium $late neonatal hypocalcemia*. #he role played by the parathyroid glands in thesehypocalcemic infants remains to be clari4ed, although functional immaturity of the parathyroidglands is invoked as pathogenetic factor. &n a group of infants "ith transient idiopathichypocalcemia $ - "k of age*, serum levels of parathyroid hormone $P#C* are signi4cantly lo"er than those in normal infants. &t is possible that the functional immaturity is a manifestation of adelay in development of the en)ymes that convert glandular P#C to secreted P#C other mechanisms are possible.A%la!ia or hy%o%la!ia of the %arathyroi 'la# ! i! ofte# a!!o&iate 0ith the DiGeor'e!y# ro"e;+elo&ar iofa&ial !y# ro"eHy%o&al&e"ia +ita"i# D4 "a'#e!i$"Ma#ife!tatio#
- Ch+o!te1 !i'# GlicitationH #apping on the face at a point 5ust anterior to the ear and 5ust belo" the
)ygomatic bone Positive responseH #"itching of the ipsilateral facial muscles, suggestive of neuromuscular
excitability caused by hypocalcemia
A## B

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 7/8
ENDOCRINOLOGY – DR. ESGUERRA
- Tro$!!ea$ !i'#- GlicitationH &nIating a sphygmomanometer cu! above systolic blood pressure for several
minutes- Positive responseH Muscular contraction including Iexion of the "rist and
metacarpophalangeal 5oints, hyperextension of the 4ngers, and Iexion of the thumb on the palm, suggestive of neuromuscular excitability caused by hypocalcemia
- Lary#'eal or Car%o%e al !%a!"- Co#+$l!io#! 0ith or 0itho$t lo!! of &o#!&io$!#e!!. #hese episodes can begin "ith abdominal
pain, follo"ed by tonic rigidity, retraction of the head, and cyanosis. Hy%o%arathyroi i!" i!"i!ta1e# for e%ile%!y
- Hea a&he4 +o"iti#'4 i#&rea!e ICP4 a# %a%ille e"a "ay (e a!!o&iate 0ith &o#+$l!io#!a# "i'ht !$''e!t a (rai# t$"or.
- Cal&i$" le+el i! lo0 )>-3 "'; L*- Ele+ate Pho!%hor$! le+el )3- 8 "'; L*
Treat"e#t- E"er'e#&y treat"e#t of #eo#atal teta#y &o#!i!t of >- / "l or -7 "';1' of a /J
!ol$tio# of Cal&i$" Gl$&o#ate )ele"e#tal &al&i$" .7 "'; L * at the rate of /.0- ./mJKmin "hile the heart rate is monitored and a total dose not to exceed / mg of elementalcalciumKkg. Fdditionally, , 0 dihydroxycholecalciferol $calcitriol* should be given.
- Fn adeLuate intake of calcium should be ensured. +upplemental calcium can be given in theform of calcium gluconate or calcium glubionate to provide // mg of elemental calciumdaily, but it is rarely essential. >oods "ith high phosphorus content such as milk, eggs, andcheese should be reduced in the diet.
- linical evaluation of the patient and freLuent determinations of the serum calcium levelsare indicated in the early stages of treatment to determine the reLuirement for calcitriol or vitamin 9 . &f Cypercalcemia occurs, therapy should be discontinued and resumed at alo"er dose after the serum calcium level has returned to normal
A## 3

8/16/2019 Endocrinology Pedia
http://slidepdf.com/reader/full/endocrinology-pedia 8/8
ENDOCRINOLOGY – DR. ESGUERRA
Refere#&e!Dr. Mari+i& E!'$erra ! le&t$re
elson #extbook of Pediatrics /G
A## ,