-
Elizabeth LuleManager, ACTafricaThe Unfinished HIV/AIDS Agenda
for Africa
Africa Region Consultation Kigali, Rwanda
June 13,2007
-
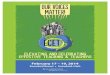
Global HIV epidemic, 19902005*HIV epidemic in sub-Saharan
Africa, 19852005*Number of people living with HIV% HIV prevalence,
adult (1549)Number of peopleliving with HIV
(millions)0102030405019901995200020050.01.02.03.04.05.0198519901995200020050510152025300.02.55.07.512.515.0%
HIV prevalence, adult (1549)Number of peopleliving with HIV
(millions)Status of the AIDS EpidemicThis bar indicates the range
around the estimate10.0Source: UNAIDS, 2006
-
OutlineWhy a new Africa HIV/AIDS Agenda for Action?
What is the new HIV/AIDS Agenda for Action?
What are the Banks comparative advantage and value-added?
What guidance do we need from the decision meeting?
-
Why A New Agenda for Action?Epidemic has changedMore financial
resources, but great need to ensure resources are used effectively
and efficientlyUnfinished multisectoral agenda Country needs have
changedBank must continue to learn how to address epidemics
-
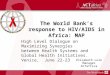
15-35%3-7%1-5%0-0.1%Middle-income countries are hardest hit
Source: UNAIDS 2004 estimates used unless recent national
population-based HIV survey available
-
Gender inequalities in HIV/AIDS
HIV Prevalence in Francistown, BotswanaSource: BAIS, 2005
-
Africas children are paying the price Source: UNAIDS, 2006
-
Global Resources Available Compared to Estimated Need$11.6
billion$14.9 billion$22.1 billionSource: The Henry J. Kaiser Family
Foundation (www.kff.org) Original source UNAIDS Most available
resources are:
Volatile Short term Off-budgetNot strategicPoorly coordinated
External prioritiesTechnology focused
-
Our AIDS portfolio has declinedSource: Business Warehouse, March
2007. Data includes total commitments for MAP projects and coded
amounts for projects with HIV/AIDS components.IDA 13IDA 14
-
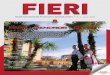
How MAP Funds were spentLocal ResponseUS $502m committedUS $306m
spent38%32%17%13%Institutional Strengthening$423m committed$258m
spentHealth Sector Response$223m committed$137m spentPublic Sector
Response (beyond health)US $172m committedUS $104m spent
Chart2
38
32
17
13
Sheet1
Local response38
Institutional strengthening32
Health response17
Public sector (non-health)13
Sheet1
0
0
0
0
Sheet2
Sheet3
Sheet4
Sheet5
Sheet6
-
The Unfinished Multisectoral Agenda
-
What Our Partners Want From UsMacro and micro-economic analysis
(impact of HIV/AIDS) Financing gaps: prevention, especially
interventions for populations at riskCapacity buildingPredictable,
sustainable and flexible fundingMajor/only funding for some
countriesFocus on fiduciary aspects, governance and
accountabilityReaching communitiesMulti-sectoral approach
-
Bottom lineHIV/AIDS undermines the Banks Poverty Reduction
mission and achievement of the MDGs
We need to build on results achieved thus far Epidemic
resurgence in Uganda reflects declining prevention
effortsMainstreaming HIV/AIDS in key sectors is an unfinished
agendaUniquely positioned to put HIV/AIDS on the development
agendaRespond to the changing global AID architecture
-
Agenda for Action: Conceptual Framework
-
Strategic PillarsFoundation of the four strategic pillars is to
Renew the Banks commitment
Pillar 1: Focus the response through evidence based and
prioritized national HIV/AIDS strategies
Pillar 2: Scale-up targeted multi-sectoral and civil society
response
Pillar 3: Deliver effective results through increased country
M&E capacity
Pillar 4: Harmonize donor collaboration
-
Selected Anticipated Results
Objective
Anticipated Results
Countries access to predictable, flexible and sustainable
financing for HIV/AIDS provided.
Funds committed to HIV/AIDS (at least $250 million annually)
including IDA, IBRD, PRSCs, ACGF, and IDF increased.
Support to sub-regional and cross-border initiatives
provided.
Improved HIV/AIDS awareness and prevention efforts through
sub-regional and cross-border initiatives
Appropriate HIV/AIDS efforts into countries and Banks
development agenda embedded (policy procedures).
Review 10 CASs and ISNs and 6 PRSPs to ensure HIV/AIDS is
appropriately incorporated.
HIV/AIDS integrated into at least 75% of PRSPs, CASs and ISNs
prepared each year.
Bank support in capacity building to develop prioritized, and
costed national strategies and action plans provided.
Capacity building and technical assistance to develop
prioritized, costed national strategies and annual action plans in
20 countries over five years.
HIV/AIDS components in transport, infrastructure, urban and
private sectors to address gender inequalities and social
protection for vulnerable groups increased.
At least 10 analytical efforts addressing HIV and key sectors,
gender inequality, OVCs, and regional aspects.
Harmonized M&E frameworks at the country level
strengthened.
Bank to continue to play leading role (GAMET) in supporting
countries.
All countries have a harmonized, functional M&E system
reporting and using data.
Collaboration with key partners to harmonize and strengthen
national M&E systems, HR capacity, procurement and supply
chains strengthened.
GAMET to continue to support countries to strengthen M&E in
close collaboration with other partners.
Joint planning and analytical work with UNAIDS and other
partners increased.
All countries would have moved towards joint annual national
program reviews and planning.
Knowledge generation and sharing to improve prioritization,
decision-making and program design supported.
Design and impact of HIV/AIDS investments based on knowledge
sharing.
Countries and partners fully engaged in knowledge generation and
sharing.
-
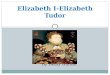
A girl at a daycare center in Kibera, in Nairobi, Kenya. The
center provides basic education and meals for orphaned children.A
boy and his grandmother in Maseru, Lesotho. He is one of three
grandchildren she cares forfollowing the death of their parents
from AIDS.The 19-year-old girl on the left cares for herself, her
two siblings, andher older sister's three children in Harare,
Zimbabwe. Her parents andolder sister died of AIDS.Source: UNAIDS,
UNICEF and USAID, Children on the Brink 2004.The Cost of
Inaction
Even though the HIV prevalence rates have stabilized in
sub-Saharan Africa, the actual number of people infected continues
to grow Because of population growth. Applying the same prevalence
rate to a growing population will result in increasing numbers of
people living with HIV
Diverse epidemics across the ContinentSome countries with
concentrated epidemics and very low prevalence (under1%)Others with
generalized epidemics and prevalence rates approaching
40%Overwhelmingly heterosexual transmission, along with
Mother-to-Child TransmissionWomen especially young women more
vulnerable (59% of people living with AIDS)12 million orphans a
generation lost
Bank support only 5 percent of totalThis graph shows the
percentage and amount of funding given to each of the sectors that
were funded by the MAP. The 32% of funding given for institutional
strengthening, shows the commitment of the Bank to creating
conducive institutional structures to manage, coordinate, monitor
and evaluate the HIV response at the national and local levels.
This graph also shows that the MAP achieved its principle of
using multiple implementation agencies.
PERCENTAGES OF ACTIVE COMMITMENTS BY SECTOR FOR HIV/AIDSAs of
March 2007. none of the PRSCs have included HIV/AIDS as a theme
While the majority of HIV/AIDS projects are managed by Human
Development (Health, Nutrition and Population, Education and Social
Protection), continued efforts are being made to mainstream
HIV/AIDS into non-health sectors. Sectors in the Africa Region that
have integrated HIV/AIDS into their sectoral response include
Education, Urban Development, Transport, Social Protection, Social
Development, Rural Sector, and the Private Sector.
Projects with HIV/AIDS components of less than $5 million are
also managed by Water Supply and Sanitation, Environment, and
Public Sector Governance.
WB funding fills key gaps and needsMost predictable, long-term
& flexible fundingMajor/only funding for some countriesMacro
and micro-economic analysis (impact of HIV/AIDS), policy
dialogueFocus on fiduciary aspects, governance and
transparencyFinancing gaps: prevention, especially interventions
for populations at riskReaching communitiesMulti-sectoral
approachHealth system strengtheningCapacity building
Banks comparative advantage/value-added in:
Strategy
Implementation
Monitoring and Evaluation
Agenda for Action:
Renew the commitment to sustain the response
Focus the response by supporting evidence based prioritized
strategies and implementation
Target the multi-sectoral response
Deliver results through enhanced efficiency, effectiveness and
transparency
Make the money work
COST OF INACTION:


![[PPT]Pharmaceutical Procurement Demystified - Global … · Web viewPharmaceutical Procurement Demystified Managing supply chains through the Public Sector Sangeeta Raja ACTafrica](https://img.dokumen.tips/doc/110x75/5ac1d34f7f8b9ac6688dd1cf/pptpharmaceutical-procurement-demystified-global-viewpharmaceutical-procurement.jpg)