Embed Size (px)
Citation preview

Circulation Journal Vol.78, April 2014
844 KINUGAWA K et al.Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
Tolvaptan (Otsuka Pharmaceutical Co, Ltd, Tokyo, Japan) is an oral arginine-vasopressin (AVP) type 2 receptor antagonist with an aquaretic effect.12–15 Tolvaptan increases urine volume without increasing electrolyte excretion into urine (ie, aquare-sis).14 Schrier et al have reported that tolvaptan increased serum sodium levels consistently in patients with hyponatremia.16 Tolvaptan is indicated for patients with hyponatremia and syn-drome of inappropriate antidiuretic hormone (SIADH) in the USA, and for SIADH in the EU.17 In Japan, tolvaptan has been approved for “volume overload in heart failure patients when adequate response was not obtained with other diuretics (eg, loop diuretics)” since 2010. The approval was based on the re-sults from the QUalification of Efficacy and Safety in the study of Tolvaptan in cardiac edema study (QUEST) study, in which Matsuzaki et al reported that tolvaptan showed efficacy in HF
onventional diuretics, including loop diuretics, are com-monly prescribed for heart failure (HF) patients with volume overload.1–6 Loop diuretics are clinically use-
ful to reduce volume overload, but patients sometimes have an insufficient response. In the Acute Decompensated Heart Failure Registry (ADHERE), diuretic resistance was observed in ap-proximately 30% of patients.7 A few therapeutic strategies, in-cluding salt restriction, intravenous administration of loop di-uretics, and combination therapy with loop and thiazide diuretics, have been developed to reduce resistance to loop diuretics, but often result in unsatisfactory resolution. Moreover, administra-tion of high-dose loop diuretics is recognized as inducing sev-eral adverse events, including renal impairment and hyponatre-mia, with higher mortality.5,8–11 Despite this unmet medical need, no new oral diuretics have been developed over the past decade.
C
Received February 3, 2014; revised manuscript received February 24, 2014; accepted February 27, 2014; released online March 21, 2014 Time for primary review: 11 days
Department of Therapeutic Strategy for Heart Failure, Graduate School of Medicine, University of Tokyo, Tokyo (K.K.); Internal Medicine and Cardiology, Nippon Medical School Musashi-Kosugi Hospital, Kawasaki (N.S.); Department of Cardiovascular Medicine, Kitasato University School of Medicine, Tokyo (T.I.); and Otsuka Pharmaceutical Co, Ltd, Tokyo (T.S., N.I., K.M.), Japan
This paper was presented at the 78th Annual Scientific Meeting of the Japanese Circulation Society, Late Breaking Cohort Studies 2-3 (March 22, 2014, Tokyo, Japan).
Mailing address: Koichiro Kinugawa, MD, Department of Therapeutic Strategy for Heart Failure, Graduate School of Medicine, University of Tokyo, 7-3-1 Hongo, Bunkyo-ku, Tokyo 113-8655, Japan. E-mail: [email protected]
ISSN-1346-9843 doi: 10.1253/circj.CJ-14-0126All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Efficacy and Safety of Tolvaptan in Heart Failure Patients With Volume Overload
– An Interim Result of Post-Marketing Surveillance in Japan –Koichiro Kinugawa, MD, PhD; Naoki Sato, MD, PhD; Takayuki Inomata, MD, PhD;
Toshiyuki Shimakawa, BSc; Noriaki Iwatake, MSc; Kazuki Mizuguchi, BSc
Background: Loop diuretics are commonly used in heart failure (HF) patients, but they are sometimes associated with insufficient response as well as adverse events. In such diuretics-resistant cases, tolvaptan, a vasopressin type 2 receptor antagonist, shows the improvement of volume overload without electrolyte imbalance. Tolvaptan was launched in Japan in 2010, and a post-marketing surveillance has been performed to evaluate the safety and effi-cacy of tolvaptan in real-world clinical settings.
Methods and Results: HF patients with insufficient response to loop diuretics were enrolled: 1,053 to evaluate for efficacy and 1,057 patients for the safety assessment. Decreases in body weight from baseline were 1.0±1.6 kg at day 2 and increases in urine volume were 631±1,179 ml at day 1 (both P<0.0001 vs. baseline). Congestive symptoms were significantly improved within 14 days. Adverse drug reactions (ADR) were observed in 18.7%, with thirst being the most frequent ADR (10%). Hypernatremia was a complication in 40 patients (3.8%). Predictive factors for the oc-currence of hypernatremia were the starting dosage of tolvaptan (15 mg/day), baseline serum sodium level (≥142 mEq/L) and serum potassium level (<3.8 mEq/L) at baseline.
Conclusions: In the real-world clinical setting, tolvaptan demonstrated aquaretic efficacy in HF patients with diuretic-resistant volume overload. We recommend a lower dose of tolvaptan in Japanese patients with normonatremia and hypokalemia to prevent hypernatremia. (Circ J 2014; 78: 844 – 852)
Key Words: Aquaretics; Congestive symptom; Loop diuretics; Vasopressin; Volume overload
LATE BREAKING COHORT STUDIES (JCS 2014)
Circulation Journal Vol.78, April 2014
845Post-Marketing Surveillance of Tolvaptan
MethodsStudy SettingThis surveillance was a prospective, multicenter, observation-al study, and was performed in compliance with Good Post-marketing Study Practice, an ordinance issued by the Ministry of Health, Labor and Welfare establishing the standards for im-plementation of post-marketing surveillance of all new drugs approved in Japan. Although the total study period is from 2011 to 2015, interim result from 2011 to 2013 have been al-ready reported to the Pharmaceuticals and Medical Devices Agency in Japan. The study is planning for final registration of 3,000 patients. In the present report, we describe the interim re-sults for the efficacy and safety features of tolvaptan.
Study ProtocolPatients Tolvaptan was given once daily in the morning to all enrolled patients (indication: HF with volume overload re-sistant to loop diuretics). Patients were excluded if they had an-uria, consciousness disturbance, difficulties with water intake,
patients with volume overload, and that its action was not as-sociated with electrolyte imbalance or renal impairment.18 The presence of worsening congestive symptoms is a leading cause of hospitalization, and reduction in the patient’s quality of life.19 In the QUEST study, improvement of congestive symptoms was also reported.18
However, the applicability of the results of the QUEST study is limited by the clinical trial’s strict inclusion and exclusion criteria for enrollment. Therefore, it is desirable to confirm whether the efficacy and safety features of tolvaptan in clinical trials can be extended to real-world clinical settings. Hence the aim of this study was to provide efficacy and safety data from post-marketing surveillance of tolvaptan in HF patients with volume overload. Hypernatremia is a major and unique concern with tolvaptan because of its aquaretic nature, and a risk anal-ysis was executed to predict the occurrence of hypernatremia after tolvaptan treatment.
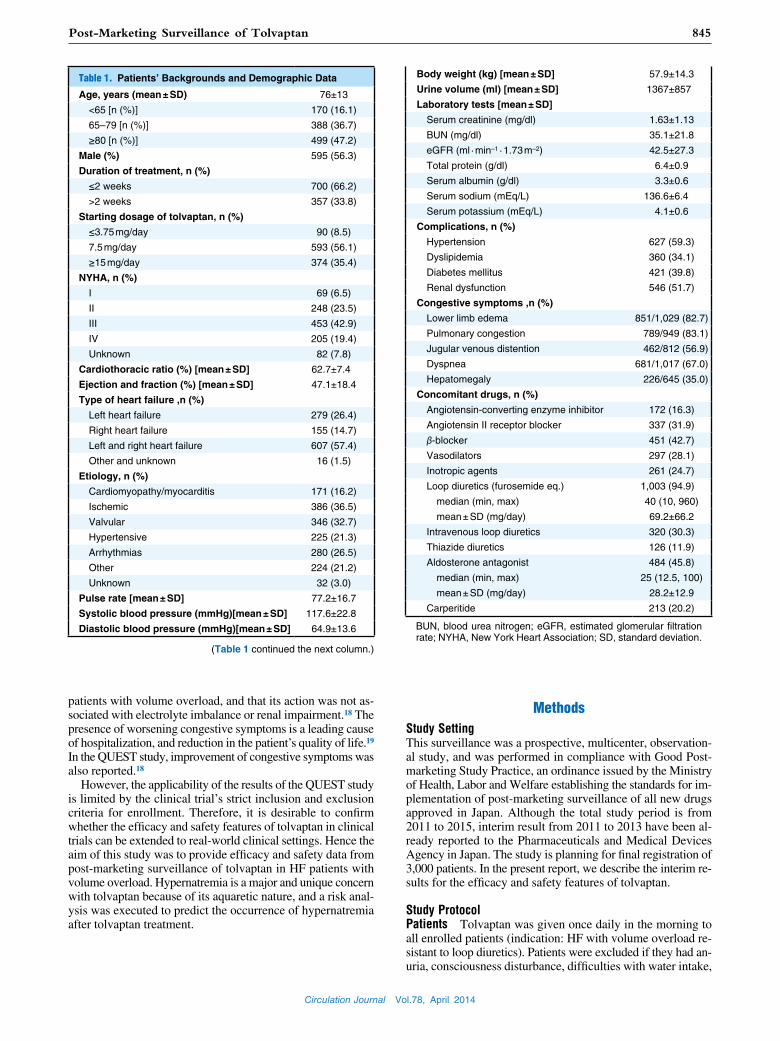
Table 1. Patients’ Backgrounds and Demographic Data
Age, years (mean ± SD) 76±13
<65 [n (%)] 170 (16.1)
65–79 [n (%)] 388 (36.7)
≥80 [n (%)] 499 (47.2)
Male (%) 595 (56.3)
Duration of treatment, n (%)
≤2 weeks 700 (66.2)
>2 weeks 357 (33.8)
Starting dosage of tolvaptan, n (%)
≤3.75 mg/day 90 (8.5)
7.5 mg/day 593 (56.1)
≥15 mg/day 374 (35.4)
NYHA, n (%)
I 69 (6.5)
II 248 (23.5)
III 453 (42.9)
IV 205 (19.4)
Unknown 82 (7.8)
Cardiothoracic ratio (%) [mean ± SD] 62.7±7.4 Ejection and fraction (%) [mean ± SD] 47.1±18.4
Type of heart failure ,n (%)
Left heart failure 279 (26.4)
Right heart failure 155 (14.7)
Left and right heart failure 607 (57.4)
Other and unknown 16 (1.5)
Etiology, n (%)
Cardiomyopathy/myocarditis 171 (16.2)
Ischemic 386 (36.5)
Valvular 346 (32.7)
Hypertensive 225 (21.3)
Arrhythmias 280 (26.5)
Other 224 (21.2)
Unknown 32 (3.0)
Pulse rate [mean ± SD] 77.2±16.7
Systolic blood pressure (mmHg)[mean ± SD] 117.6±22.8 Diastolic blood pressure (mmHg)[mean ± SD] 64.9±13.6
(Table 1 continued the next column.)
Body weight (kg) [mean ± SD] 57.9±14.3
Urine volume (ml) [mean ± SD] 1367±857 Laboratory tests [mean ± SD]
Serum creatinine (mg/dl) 1.63±1.13
BUN (mg/dl) 35.1±21.8
eGFR (ml · min–1 · 1.73 m–2) 42.5±27.3
Total protein (g/dl) 6.4±0.9
Serum albumin (g/dl) 3.3±0.6
Serum sodium (mEq/L) 136.6±6.4 Serum potassium (mEq/L) 4.1±0.6
Complications, n (%)
Hypertension 627 (59.3)
Dyslipidemia 360 (34.1)
Diabetes mellitus 421 (39.8)
Renal dysfunction 546 (51.7)
Congestive symptoms ,n (%)
Lower limb edema 851/1,029 (82.7)
Pulmonary congestion 789/949 (83.1)
Jugular venous distention 462/812 (56.9)
Dyspnea 681/1,017 (67.0)
Hepatomegaly 226/645 (35.0)
Concomitant drugs, n (%)
Angiotensin-converting enzyme inhibitor 172 (16.3)
Angiotensin II receptor blocker 337 (31.9)
β-blocker 451 (42.7)
Vasodilators 297 (28.1)
Inotropic agents 261 (24.7)
Loop diuretics (furosemide eq.) 1,003 (94.9) median (min, max) 40 (10, 960)
mean ± SD (mg/day) 69.2±66.2
Intravenous loop diuretics 320 (30.3)
Thiazide diuretics 126 (11.9)
Aldosterone antagonist 484 (45.8)
median (min, max) 25 (12.5, 100)
mean ± SD (mg/day) 28.2±12.9
Carperitide 213 (20.2)
BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate; NYHA, New York Heart Association; SD, standard deviation.
Circulation Journal Vol.78, April 2014
846 KINUGAWA K et al.
of tolvaptan, were recorded. Laboratory tests comprised the es-timated glomerular filtration rate (eGFR), and alanine amino-transferase (ALT), aspartate aminotransferase (AST), total bili-rubin (T-Bil), blood urea nitrogen (BUN), creatinine (Cr), serum sodium, and serum potassium concentrations. Adverse drug re-actions (ADRs) were summarized according to the physicians’ reports and listed by frequency. Serious adverse events were defined as those resulting in death, life-threatening events, ne-cessity or prolongation of hospitalization, persistent or signifi-cant disability, or intervention to prevent any of the above.
Statistical AnalysisChanges in body weight and urine volume from BL to each time point were analyzed by paired t-test. Data are expressed as mean ± standard deviation (SD). Congestive symptoms were analyzed by chi-square or Fisher’s exact test. The evaluation of lower limb edema and pulmonary congestion was by presence and absence, and compared by chi-square test or Fischer’s exact test.
The occurrence of hypernatremia was redefined for a risk analysis when at least 1 measurement of serum sodium level was ≥150 mEq/L throughout the tolvaptan treatment period. Pre-dictive factors that affect the occurrence of hypernatremia by tolvaptan were extracted from variables by performing appro-
hypernatremia, or were pregnant. The standard observation pe-riod was 2 weeks but treatment could be continued beyond that per physician’s judgment.
Evaluation of Clinical Effects Body weight was measured from baseline (BL) throughout the treatment periods, and chang-es in body weight at day 14 from BL were evaluated. Urine samples for determining cumulative 24-h urine volume were collected from BL through the consecutive treatment periods as were blood samples for clinical laboratory tests. For the eval-uation of body weight and clinical laboratory tests, BL was defined as the values immediately before initiation of treatment with tolvaptan. For the evaluation of urine volume, BL was defined as the cumulative 24-h urine volume on the day before starting tolvaptan.
Congestive Symptoms Congestive symptoms, including lower limb edema, dyspnea, pulmonary congestion, jugular ve-nous distention, and hepatomegaly, were recorded from BL through the consecutive treatment periods. Lower limb edema and pulmonary congestion were evaluated by symptomatic grad-ing (none, mild, moderate, and severe). Dyspnea, jugular venous distention, and hepatomegaly were evaluated by their presence or absence.
Safety Assessments Safety assessments, including clini-cal laboratory tests, vital signs, and ECG during administration
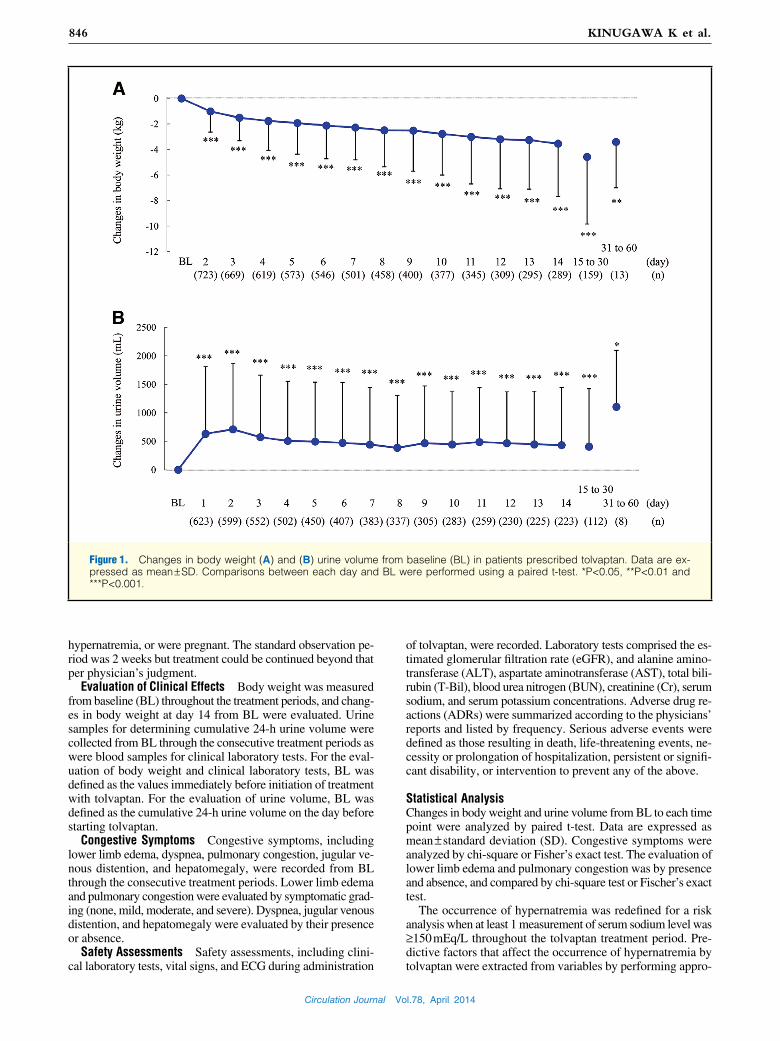
Figure 1. Changes in body weight (A) and (B) urine volume from baseline (BL) in patients prescribed tolvaptan. Data are ex-pressed as mean ± SD. Comparisons between each day and BL were performed using a paired t-test. *P<0.05, **P<0.01 and ***P<0.001.
Circulation Journal Vol.78, April 2014
847Post-Marketing Surveillance of Tolvaptan
classification was 62.3%.
Clinical EffectsDecrease in body weight by more than 1 kg at days 7 and 14 oc-curred in 65.6% and 76.6% of patients, respectively (Figure 1A). At days 2, 3, 7, and 14, body weight had decreased from BL by 1.0±1.6 kg, 1.5±1.8 kg, 2.3±2.5 kg, and 3.5±4.1 kg, respec-tively, with statistical significance (P<0.0001 for all time points). With each 3.75 mg/day, 7.5 mg/day and 15 mg/day of tolvap-tan, body weight was decreased by 1.3±2.1 kg, 2.1±2.4 kg, and 3.0±2.9 kg at day 7 (P<0.0001 for all time points); moreover, the decrease was 2.8±3.2 kg, 3.3±3.8 kg, 4.4±4.9 kg, respectively, at day 14 (P<0.0001 for all time points).
Further, the change in urine volume at days 1, 2, 3, 7, and 14 from BL was 631±1,179 ml, 710±1,159 ml, 572±1,090 ml, 442±1,001 ml, and 433±1,013 ml, respectively, with statistical significance (P<0.0001 for all time points) (Figure 1B). For each 3.75 mg/day, 7.5 mg/day and 15 mg/day of tolvaptan, urine volume increased 425±914 ml (P=0.0012), 657±1,127 ml (P<0.0001), and 863±1,264 ml, respectively, on day 1 (P<0.0001). The trends in body weight and urine volume were consistently observed throughout the 14 days of treatment.
priate statistics between 2 groups with and without hyperna-tremia. Variables that had P<0.05 in the univariate analysis were selected. Continuous variables were substituted for categorical data using the cut-off points calculated by receiver-operating characteristic (ROC) curve analysis. Multivariate analysis using these variables was executed to determine independent predic-tive factors.
Odds ratio (OR) and 95% confidence interval (CI) are shown. Statistical significance was defined as P<0.05 and all analyses were performed using SAS version 9.1.3 software SAS/STAT (SAS Institute, Japan).
ResultsBL CharacteristicsIn total, 1,840 patients with HF were registered, and 1,059 case report forms from 258 sites were collected; 4 were excluded from the efficacy analysis because of off-label use, so 1,053 were analyzed for efficacy. For the safety assessment, 2 were ex-cluded for violations of the enrollment criteria, so 1,057 were assessed. Patients’ backgrounds and demographic data are shown in Table 1. Mean age was 76 years, 56.3% were male, 33.8% had been prescribed tolvaptan for more than 2 weeks and the prevalence of classes III and IV HF according to the NYHA
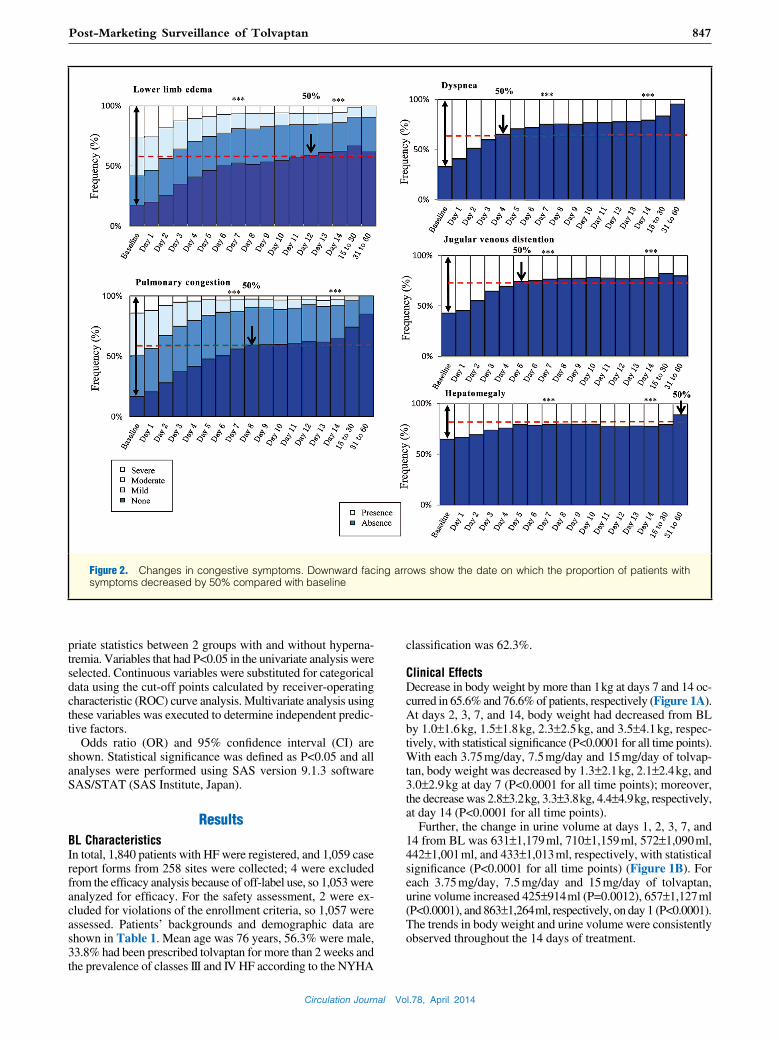
Figure 2. Changes in congestive symptoms. Downward facing arrows show the date on which the proportion of patients with symptoms decreased by 50% compared with baseline
Circulation Journal Vol.78, April 2014
848 KINUGAWA K et al.
35.0% at BL, 20.6% at day 7, and 22.6% at day 14. These con-gestive symptoms were significantly improved at days 7 and 14 (P<0.0001 for all symptoms). The half-time of each congestive symptom prevalence was: 4 days for dyspnea, 5 days for jugu-lar venous distention, 8 days for pulmonary congestion, and 12 days for lower limb edema.
Safety AssessmentAll ADRs are shown in Table S1, and occurred in 198 of the
Evaluation of Congestive SymptomsThe presence and grading of congestive symptoms in the HF patients is shown in Figure 2. Prevalence of any grade of lower limb edema was 82.7% at BL, 47.2% at day 7, and 37.5% at day 14. Prevalence of any grade of pulmonary congestion was 83.1% at BL, 43.8% at day 7, and 34.8% at day 14. Prevalence of dys-pnea was 67.0% at BL, 24.7% at day 7, and 20.5% at day 14. Prevalence of jugular venous distention was 56.9% at BL, 23.4% at day 7, and 21.4% at day 14. Prevalence of hepatomegaly was
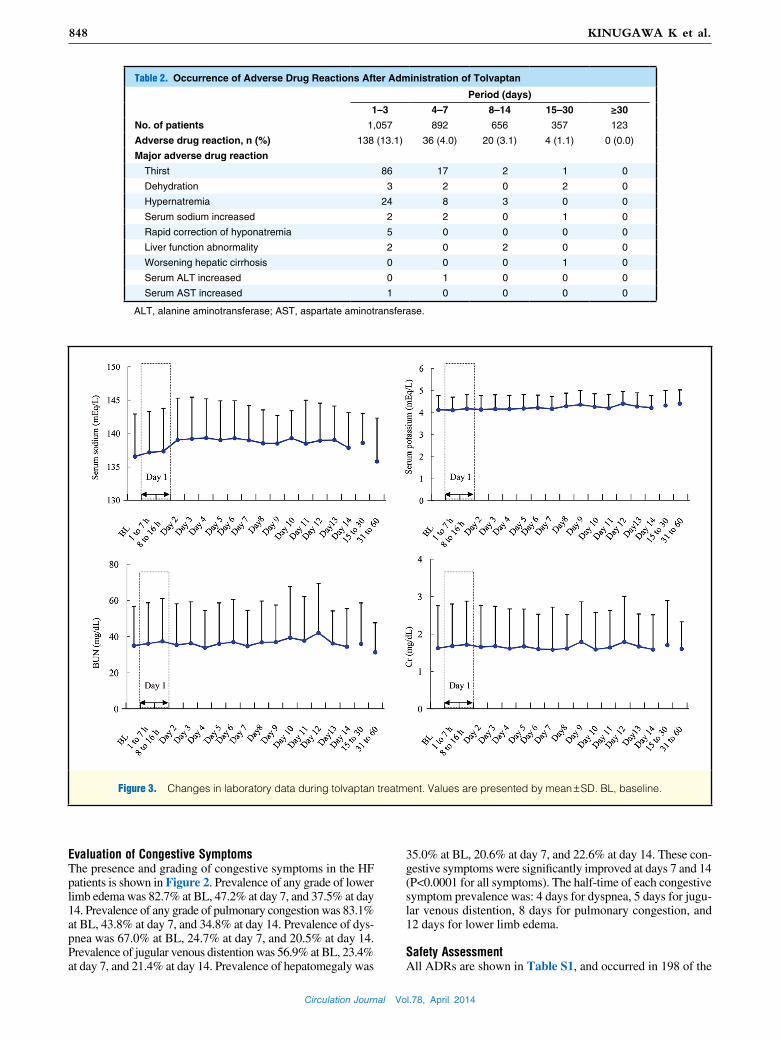
Table 2. Occurrence of Adverse Drug Reactions After Administration of Tolvaptan
Period (days)
1–3 4–7 8–14 15–30 ≥30
No. of patients 1,057 892 656 357 123
Adverse drug reaction, n (%) 138 (13.1) 36 (4.0) 20 (3.1) 4 (1.1) 0 (0.0)
Major adverse drug reaction
Thirst 86 17 2 1 0
Dehydration 3 2 0 2 0
Hypernatremia 24 8 3 0 0
Serum sodium increased 2 2 0 1 0
Rapid correction of hyponatremia 5 0 0 0 0
Liver function abnormality 2 0 2 0 0
Worsening hepatic cirrhosis 0 0 0 1 0
Serum ALT increased 0 1 0 0 0
Serum AST increased 1 0 0 0 0
ALT, alanine aminotransferase; AST, aspartate aminotransferase.
Figure 3. Changes in laboratory data during tolvaptan treatment. Values are presented by mean ± SD. BL, baseline.
Circulation Journal Vol.78, April 2014
849Post-Marketing Surveillance of Tolvaptan
correction of hyponatremia (5 patients, 0.47%). The time to ob-servation of the major ADRs is shown in Table 2. A large pro-portion of the major ADRs, including thirst and hypernatremia, occurred within 3 days of beginning administration of tolvaptan. Serum sodium, potassium, BUN and Cr concentration s were not significantly changed through the treatment period (Figure 3). Similarly, AST, ALT, T-Bil and eGFR did not significantly change during tolvaptan treatment (Figure S1). In total, there were 25 patients with serious ADRs. Of these, there were 8 cases of renal dysfunction, 6 of electrolyte imbalance including 2 of
1,057 patients (18.73%). Thirst was the most frequent ADR (n=106, 10.03%), but there was no significant different preva-lence of it among the dosages of tolvaptan. The relationship between dosage of tolvaptan and other ADR could not be eval-uated because of lower prevalence. Other frequent ADRs were hypernatremia (35 patients, 3.31%), renal impairment (15 pa-tients, 1.42%), increased BUN (9 patients, 0.85%), hyperkalemia (8 patents, 0.76%), dehydration (7 patients, 0.66%), hyperuri-cemia (6 patients, 0.57%), increased serum creatinine (5 patients, 0.47%), increased serum sodium (5 patients, 0.47%), and rapid
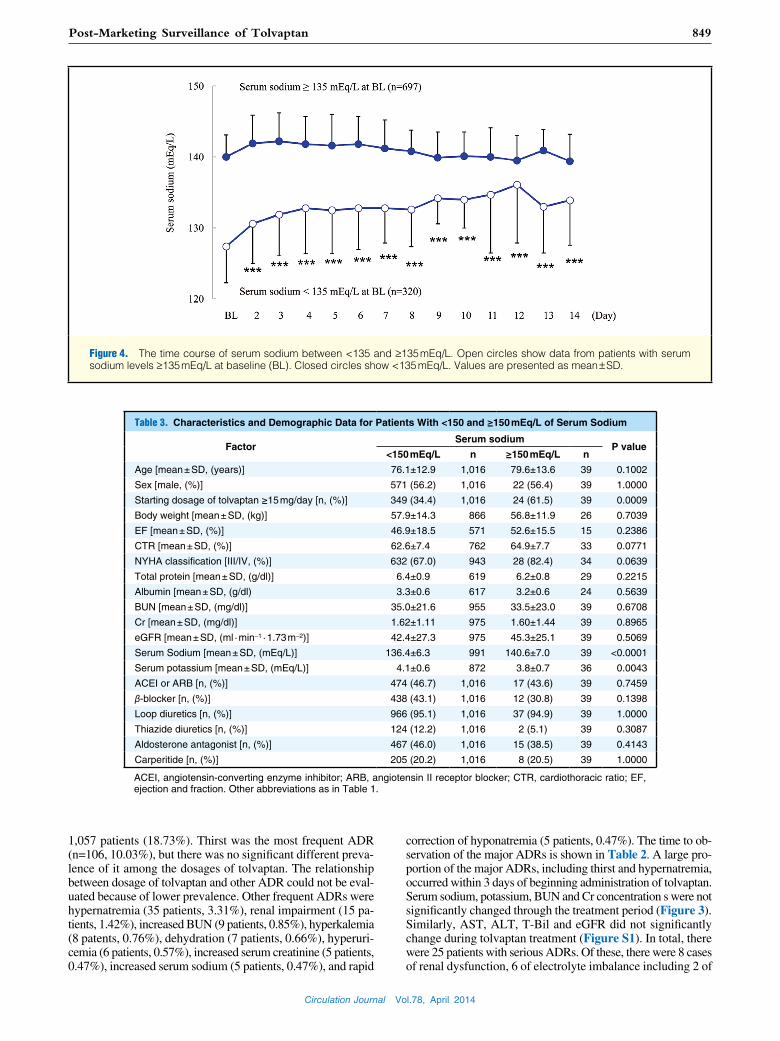
Figure 4. The time course of serum sodium between <135 and ≥135 mEq/L. Open circles show data from patients with serum sodium levels ≥135 mEq/L at baseline (BL). Closed circles show <135 mEq/L. Values are presented as mean ± SD.
Table 3. Characteristics and Demographic Data for Patients With <150 and ≥150 mEq/L of Serum Sodium
FactorSerum sodium
P value<150 mEq/L n ≥150 mEq/L n
Age [mean ± SD, (years)] 76.1±12.9 1,016 79.6±13.6 39 0.1002
Sex [male, (%)] 571 (56.2) 1,016 22 (56.4) 39 1.0000
Starting dosage of tolvaptan ≥15 mg/day [n, (%)] 349 (34.4) 1,016 24 (61.5) 39 0.0009
Body weight [mean ± SD, (kg)] 57.9±14.3 866 56.8±11.9 26 0.7039
EF [mean ± SD, (%)] 46.9±18.5 571 52.6±15.5 15 0.2386
CTR [mean ± SD, (%)] 62.6±7.4 762 64.9±7.7 33 0.0771
NYHA classification [III/IV, (%)] 632 (67.0) 943 28 (82.4) 34 0.0639
Total protein [mean ± SD, (g/dl)] 6.4±0.9 619 6.2±0.8 29 0.2215
Albumin [mean ± SD, (g/dl) 3.3±0.6 617 3.2±0.6 24 0.5639
BUN [mean ± SD, (mg/dl)] 35.0±21.6 955 33.5±23.0 39 0.6708
Cr [mean ± SD, (mg/dl)] 1.62±1.11 975 1.60±1.44 39 0.8965
eGFR [mean ± SD, (ml · min–1 · 1.73 m–2)] 42.4±27.3 975 45.3±25.1 39 0.5069
Serum Sodium [mean ± SD, (mEq/L)] 136.4±6.3 991 140.6±7.0 39 <0.0001
Serum potassium [mean ± SD, (mEq/L)] 4.1±0.6 872 3.8±0.7 36 0.0043
ACEI or ARB [n, (%)] 474 (46.7) 1,016 17 (43.6) 39 0.7459
β-blocker [n, (%)] 438 (43.1) 1,016 12 (30.8) 39 0.1398
Loop diuretics [n, (%)] 966 (95.1) 1,016 37 (94.9) 39 1.0000
Thiazide diuretics [n, (%)] 124 (12.2) 1,016 2 (5.1) 39 0.3087
Aldosterone antagonist [n, (%)] 467 (46.0) 1,016 15 (38.5) 39 0.4143
Carperitide [n, (%)] 205 (20.2) 1,016 8 (20.5) 39 1.0000
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CTR, cardiothoracic ratio; EF, ejection and fraction. Other abbreviations as in Table 1.
Circulation Journal Vol.78, April 2014
850 KINUGAWA K et al.
response to loop diuretics participated in real-world therapy, and the clinical efficacy (decreases in body weight and increas-es in urine volume) of tolvaptan was reconfirmed as observed in the QUEST study. In this study, these effects of tolvaptan were maintained beyond the 14-day study period (Figure 1). Furthermore, such clinical efficacy was associated with an im-provement of congestive symptoms that had been diuretic-re-sistant. In the QUEST study, tolvaptan significantly improved hepatomegaly and jugular venous distention after 7 days’ treat-ment, but the improvement of lower limb edema and pulmo-nary congestion was marginal. However, in the present study, significant efficacy for all congestive symptoms was observed within 7 days. In the real-world clinical setting, accumulated experience with this drug may facilitate faster resolution of patients’ symptoms; especially notable was that the proportion of patients with dyspnea decreased by 50% at day 4 compared with BL. The improvement in dyspnea was not evaluated in the QUEST study. The early improvement in dyspnea observed in this study is a clinically important result for physicians and pa-tients, because dyspnea is not only the most common cause for hospitalization21 but also the most intolerable symptom.
In the QUEST study, Matsuzaki et al demonstrated that tolvaptan at a dose of 15 mg could be administered without any major concerns for 7 days to HF patients with volume over-load.18 They reported 54.7% of patients had experienced ADRs in the tolvaptan group, but in the present study it was 18.7%, much less than observed in the QUEST study. In the real-world clinic, the dose of tolvaptan is adjusted according to the patient’s status, and so ADRs in the present study might be reduced com-pared with the QUEST study in which the dose of tolvaptan was fixed at 15 mg daily. The most common ADR remained thirst in this surveillance study, similar to the tolvaptan group of the QUEST study.
In the QUEST study and the EVEREST study,22 serious renal dysfunction occurred in few (~2%) patients treated with tolvap-tan. In this post-marketing surveillance, we also found that less than 1% of patients experienced serious renal dysfunction. These findings confirm that treatment with tolvaptan is less associated with renal dysfunction than conventional diuretic therapy.23,24 In this study, a lower frequency (<1%) of abnormal hepatic function was observed compared with the QUEST study. In the Tolvaptan Efficacy and Safety in Management of Autosomal Dominant Polycystic Kidney Disease and Its Outcomes (TEMPO) 3:4 trial, a greater proportion of tolvaptan use was accompanied by elevations of liver enzymes,25 which might have been caused by the higher dosage of tolvaptan at 60–120 mg daily in the TEMPO study.
Serum sodium levels did not significantly change through-out the tolvaptan treatment period. In our subanalysis, tolvap-tan increased serum sodium levels in patients with hyponatre-mia at BL, but did not change it in those with normonatremia (Figure 4). This finding further strengthens the previous result obtained from the QUEST study that tolvaptan was rarely ac-companied by electrolyte imbalance. This interesting regula-tory characteristic may ensure the safety of this drug under the
hypernatremia, 8 cardiovascular-related disorders and although 37 deaths were reported, there was only 1 case as an ADR. In the single case of death, the patient had disuse syndrome and severe debility, but no further detailed information was avail-able. Subgroup analysis was performed to evaluate the changes in serum sodium levels. In patients with serum sodium levels ≥135 mEq/L at BL, mean serum sodium levels did not change, whereas in patients with serum sodium levels <135 mEq/L at BL, the serum sodium levels were significantly increased (Figure 4).
Occurrence of HypernatremiaPredictive factors affecting the occurrence of hypernatremia by tolvaptan were analyzed. As shown in Table S1, hypernatremia was reported in 35 patients, but ADRs were based on the phy-sicians’ reports without standardized definitions. Therefore, we redefined hypernatremia for the risk analysis as having a serum sodium level ≥150 mEq/L during the tolvaptan treatment peri-od. As a result, 40 patients were extracted and 1 was excluded from this analysis because of a lack of data at BL. Characteristics and demographic data for patients with hypernatremia are shown in Table 3.
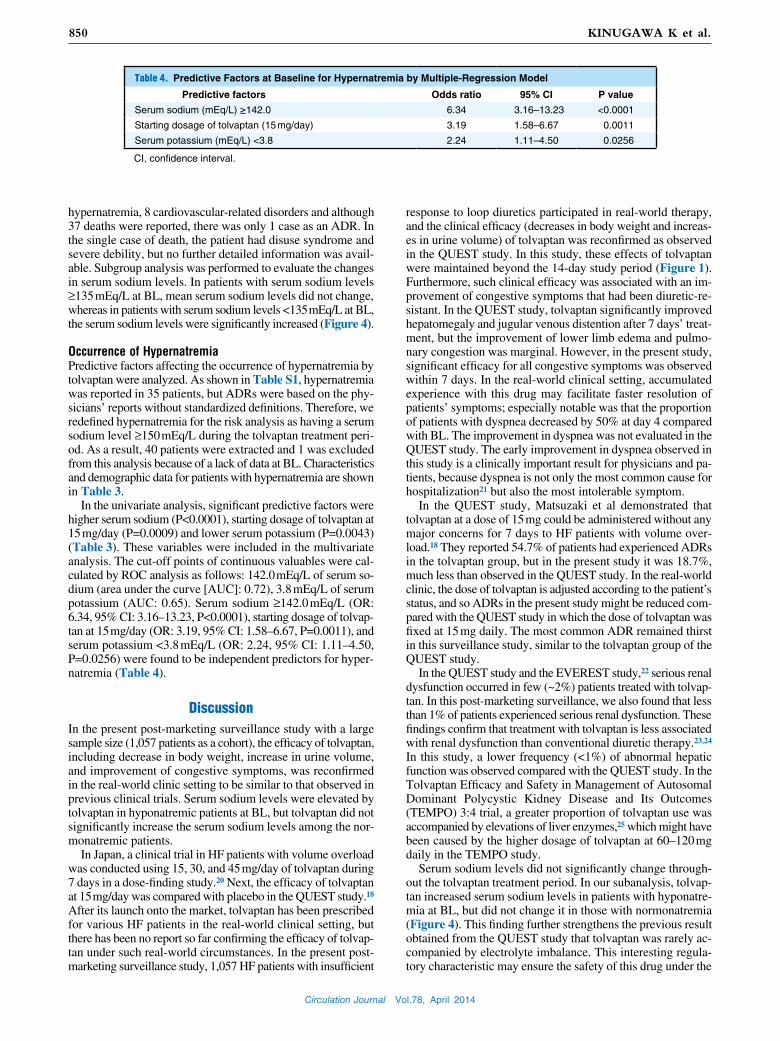
In the univariate analysis, significant predictive factors were higher serum sodium (P<0.0001), starting dosage of tolvaptan at 15 mg/day (P=0.0009) and lower serum potassium (P=0.0043) (Table 3). These variables were included in the multivariate analysis. The cut-off points of continuous valuables were cal-culated by ROC analysis as follows: 142.0 mEq/L of serum so-dium (area under the curve [AUC]: 0.72), 3.8 mEq/L of serum potassium (AUC: 0.65). Serum sodium ≥142.0 mEq/L (OR: 6.34, 95% CI: 3.16–13.23, P<0.0001), starting dosage of tolvap-tan at 15 mg/day (OR: 3.19, 95% CI: 1.58–6.67, P=0.0011), and serum potassium <3.8 mEq/L (OR: 2.24, 95% CI: 1.11–4.50, P=0.0256) were found to be independent predictors for hyper-natremia (Table 4).
DiscussionIn the present post-marketing surveillance study with a large sample size (1,057 patients as a cohort), the efficacy of tolvaptan, including decrease in body weight, increase in urine volume, and improvement of congestive symptoms, was reconfirmed in the real-world clinic setting to be similar to that observed in previous clinical trials. Serum sodium levels were elevated by tolvaptan in hyponatremic patients at BL, but tolvaptan did not significantly increase the serum sodium levels among the nor-monatremic patients.
In Japan, a clinical trial in HF patients with volume overload was conducted using 15, 30, and 45 mg/day of tolvaptan during 7 days in a dose-finding study.20 Next, the efficacy of tolvaptan at 15 mg/day was compared with placebo in the QUEST study.18 After its launch onto the market, tolvaptan has been prescribed for various HF patients in the real-world clinical setting, but there has been no report so far confirming the efficacy of tolvap-tan under such real-world circumstances. In the present post-marketing surveillance study, 1,057 HF patients with insufficient
Table 4. Predictive Factors at Baseline for Hypernatremia by Multiple-Regression Model
Predictive factors Odds ratio 95% CI P value
Serum sodium (mEq/L) ≥142.0 6.34 3.16–13.23 <0.0001
Starting dosage of tolvaptan (15 mg/day) 3.19 1.58–6.67 0.0011
Serum potassium (mEq/L) <3.8 2.24 1.11–4.50 0.0256
CI, confidence interval.

Circulation Journal Vol.78, April 2014
851Post-Marketing Surveillance of Tolvaptan
In conclusion, the results of the present interim post-market-ing surveillance confirmed the aquaretic efficacy and safety of tolvaptan in HF patients with volume overload and insufficient response to loop diuretics. On the other hand, the occurrence of hypernatremia, which attracted little attention in the QUEST study, was observed. Periodic careful observation of electrolytes is mandatory, especially during the initial phase of treatment. The predictive factors of hypernatremia were determined for the first time, which included higher levels of serum sodium, starting dosage of tolvaptan at 15 mg/day, and lower levels of serum potassium. We strongly recommend initiation of tolvap-tan at a lower dose in patients with normonatremia and hypo-kalemia.
AcknowledgmentsWe thank all investigators for their participation in the study. We also thank Ms Miyuki Nishio (CMIC PMS Co, Ltd.) for statistical analysis. We are grateful to Mr Koji Nakajima (Otsuka Pharmaceutical Co, Ltd.) for technical assistance. Name of grant: Otsuka Pharmaceutical Co, Ltd.
DisclosuresConflict of Interest: This trial was funded by Otsuka Pharmaceutical. Koichiro Kinugawa, Naoki Sato, and Takayuki Inomata were consultants for Otsuka Pharmaceutical. Koichiro Kinugawa, Naoki Sato, and Takayuki Inomata received honoraria from Otsuka Pharmaceutical for lectures. Koichiro Kinugawa made the final decision to submit for publication.
References 1. Brater DC, Chennavasin P, Seiwell R. Furosemide in patients with heart
failure: Shift in dose-response curves. Clin Pharmacol Ther 1980; 28: 182 – 186.
2. Gottlieb SS, Brater DC, Thomas I, Havranek E, Bourge R, Goldman S, et al. BG9719 (CVT-124), an A1 adenosine receptor antagonist, protects against the decline in renal function observed with diuretic therapy. Circulation 2002; 105: 1348 – 1353.
3. Vasko MR, Cartwright DB, Knochel JP, Nixon JV, Brater DC. Fu-rosemide absorption altered in decompensated congestive heart failure. Ann Intern Med 1985; 102: 314 – 318.
4. Felker GM. Loop diuretics in heart failure. Heart Fail Rev 2012; 17: 305 – 311.
5. Cowie MR, Komajda M, Murray-Thomas T, Underwood J, Ticho B, POSH Investigators. Prevalence and impact of worsening renal func-tion in patients hospitalized with decompensated heart failure: Results of the prospective outcomes study in heart failure (POSH). Eur Heart J 2006; 27: 1216 – 1222.
6. Hasselblad V, Stough WG, Shah MR, Lokhnygina Y, O’Connor CM, Califf RM, et al. Relation between dose of loop diuretics and outcomes in a heart failure population: Results of the ESCAPE Trial. Eur J Heart Fail 2007; 9: 1064 – 1069.
7. Peacock WF, Costanzo MR, De Marco T, Lopatin M, Wynne J, Mills RM, et al; ADHERE Scientific Advisory Committee and Inves-tigators. Impact of intravenous loop diuretics on outcomes of patients hospitalized with acute decompensated heart failure: Insights from the ADHERE registry. Cardiology 2009; 113: 12 – 19.
8. Gheorghiade M, Niazi I, Ouyang J, Czerwiec F, Kambayashi J, Zampino M, et al. Vasopressin V2-receptor blockade with tolvaptan in patients with chronic heart failure: Results from a double-blind, randomized trial. Circulation 2003; 107: 2690 – 2696.
9. Costello-Boerrigter LC, Smith WB, Boerrigter G, Ouyang J, Zimmer CA, Orlandi C, et al. Vasopressin-2-receptor antagonism augments water excretion without changes in renal hemodynamics or sodium and potassium excretion in human heart failure. Am J Physiol Ren Physiol 2006; 290: F273 – F278.
10. Butler J, Forman DE, Abraham WT, Gottlieb SS, Loh E, Massie BM, et al. Relationship between heart failure treatment and develop-ment of worsening renal function among hospitalized patients. Am Heart J 2004; 147: 331 – 338.
11. Howard PA, Dunn MI. Aggressive diuresis for severe heart failure in the elderly. Chest 2001; 119: 807 – 810.
12. Gassanov N, Semmo N, Semmo M, Nia AM, Fuhr U, Er F. Arginine vasopressin (AVP) and treatment with arginine vasopressin receptor antagonists (vaptans) in congestive heart failure, liver cirrhosis and syndrome of inappropriate antidiuretic hormone secretion (SIADH). Eur J Clin Pharmacol 2011; 67: 333 – 346.
unique Japanese indication, because we can use tolvaptan not only in hyponatremic patients but also in normonatremic ones.
However, the occurrence of hypernatremia in this study was relatively frequent compared with the QUEST study. Hyperna-tremia sometimes results in central nervous system disturbance, and therefore careful observation of serum sodium levels is essential. We observed that hypernatremia emerged within 3 days in most cases, and frequent measurement of electrolytes is recommended, especially during the initial phase of tolvap-tan treatment.
Although serum sodium levels must be monitored in all pa-tients treated with tolvaptan, there is a population that is prone to be complicated with hypernatremia. In this study, we reported 3 independent predictive factors for the occurrence of hyper-natremia for the first time: serum sodium ≥142.0 mEq/L, start-ing dosage of tolvaptan at 15 mg/day, and serum potassium <3.8 mEq/L. If a patient has a higher level of serum sodium at BL, hypernatremia may occur even with a small increase in the serum sodium concentration. However, as shown in Figure 4, most of the normonatremic patients were not complicated with hypernatremia, and there must be other factors causing the hypernatremia observed with tolvaptan.
Our analysis also suggests that hypokalemia is a risk factor for hypernatremia after tolvaptan treatment. We would like to propose that secondary aldosteronism with HF and loop diuretic therapy may be attributable to hypokalemia. Concomitant use of loop diuretics results in the inhibition of sodium reabsorp-tion at the thick ascending limb of Henle’s loop, and a large quantity of sodium reaches the distal tubule. Aldosterone block-ade might not be enough in some patients, even under antago-nist treatment, and in such patients aldosterone stimulates so-dium reabsorption and potassium excretion via Na+-K+ ATPase in the distal tubule. This is a common explanation of hypoka-lemia in HF patients treated with loop diuretics. Reabsorbed sodium does not immediately increase serum sodium levels because of the simultaneous reabsorption of water by elevated AVP, but the aquaresis by tolvaptan may result in hypernatremia in this setting. However, exact mechanisms need to be deter-mined in the future.
There have been no data reported about the dose-dependent effects of tolvaptan within the range of 3.75–15 mg daily, but anecdotal experience suggests that 15 mg of tolvaptan often causes marked aquaresis compared with lower doses. We also observed that 15 mg/day of tolvaptan was a risk factor for hy-pernatremia. Accordingly, we strongly recommend lower doses (ie, 3.75–7.5 mg daily) of tolvaptan in patients with normona-tremia and hypokalemia to avoid hypernatremia.
There was a trend, though statistically insignificant, showing that older people developed hypernatremia. It has been reported that older people easily become dehydrated probably because of physical and cognitive disabilities as well as blunted thirst,26 and the elderly should be carefully monitored if 15 mg/day tolvaptan is prescribed for them.
Some major limitations to this surveillance study are to be noted. (1) Existence of bias may be the fate of observational studies. Dosages and duration of tolvaptan treatment were de-pendent on physicians’ therapeutic strategies and patients’ con-ditions. (2) Approximately 30% of patients were treated for more than 2 weeks in this study, but the usefulness of long-term treat-ment should be explored in the future study. (3) Urine osmo-lality was reported to predict responses to tolvaptan,27 but those data were not available in this study. (4) B-type natriuretic peptide is an excellent marker of HF in terms of diagnosis, severity/staging, and prognosis, but those data were available for only 15% of this cohort.

Circulation Journal Vol.78, April 2014
852 KINUGAWA K et al.
nist, in patients hospitalized for heart failure: The EVEREST Clinical Status Trials. JAMA 2007; 297: 1332 – 1343.
23. Costello-Boerrigter LC, Smith WB, Boerrigter G, Ouyang J, Zimmer CA, Orlandi C, et al. Vasopressin-2-receptor antagonism augments water excretion without changes in renal hemodynamics or sodium and potassium excretion in human heart failure. Am J Physiol Renal Physiol 2006; 290: F273 – F278.
24. Matsue Y, Suzuki M, Seya M, Iwatsuka R, Mizukami A, Nagahori W, et al. Tolvaptan reduces the risk of worsening renal function in patients with acute decompensated heart failure in high-risk popula-tion. J Cardiol 2013; 61: 169 – 174.
25 Torres VE, Chapman AB, Devuyst O, Gansevoort RT, Grantham JJ, Higashihara E, et al. Tolvaptan in patients with autosomal dominant polycystic kidney disease. N Engl J Med 2012; 367: 2407 – 2418.
26. Hooper L, Bunn D, Jimoh FO, Fairweather-Tait SJ. Water-loss dehy-dration and aging. Mech Ageing Dev 2013 December 9, doi:10.1016/j.mad.2013.11.009 [E-pub ahead of print].
27. Imamura T, Kinugawa K, Shiga T, Kato N, Muraoka H, Minatsuki S, et al. Novel criteria of urine osmolality effectively predict response to tolvaptan in decompensated heart failure patients: Association be-tween non-responders and chronic kidney disease. Circ J 2013; 77: 397 – 404.
Supplementary FilesSupplementary File 1
Table S1. Incidence of adverse drug reactions with tolvaptan use
Figure S1. Changes in AST, ALT, T-Bil, and eGFR during tolvaptan treatment.
Please find supplementary file(s);http://dx.doi.org/10.1253/circj.CJ-14-0126
13. Decaux G, Soupart A, Vassart G. Non-peptide arginine-vasopressin antagonists: The vaptans. Lancet 2008; 371: 1624 – 1632.
14. Yamamura Y, Nakamura S, Itoh S, Hirano T, Onogawa T, Yamashita T, et al. OPC-41061, a highly potent human vasopressin V2-receptor antagonist: Pharmacological profile and aquaretic effect by single and multiple oral dosing in rats. J Pharmacol Exp Ther 1998; 287: 860 – 867.
15. Yi JH, Shin HJ, Kim HJ. V2 receptor antagonist; tolvaptan. Electro-lyte Blood Press 2011; 9: 50 – 54.
16. Schrier RW, Gross P, Gheorghiade M, Berl T, Verbalis JG, Czerwiec FS, et al. Tolvaptan, a selective oral vasopressin V2-receptor antago-nist, for hyponatremia. N Engl J Med 2006; 355: 2099 – 2112.
17. Zmily HD, Daifallah S, Ghali JK. Tolvaptan, hyponatremia, and heart failure. Int J Nephrol Renovasc Dis 2011; 4: 57 – 71.
18. Matsuzaki M, Hori M, Izumi T, Fukunami M for the Tolvaptan In-vestigators. Efficacy and safety of tolvaptan in heart failure patients with volume overload despite the standard treatment with conventional diuretics: A phase III, randomized, double-blind, placebo-controlled Study (QUEST Study). Cardiovasc Drugs Ther 2011; 25: S33 – S45.
19. JCS Joint Working Group. Guideline for management of vasculitis syndrome (JCS 2008) [Japanese Circulation Society]. Circ J 2011; 75: 474 – 503.
20. Abramow M, Cogan E. Clinical aspects and pathophysiology of di-uretic-induced hyponatremia. Adv Nephrol Necker Hosp 1984; 13: 1 – 28.
21. Sato N, Kajimoto K, Keida T, Mizuno M, Minami Y, Yumino D, et al.; TEND Investigators. Clinical features and outcome in hospitalized heart failure in Japan (from the ATTEND Registry). Circ J 2013; 77: 944 – 951.
22. Gheorghiade M, Konstam MA, Burnett Jr JC, Grinfeld L, Maggioni AP, Swedberg K, et al; Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Short-term clinical effects of tolvaptan, an oral vasopressin antago-





























