Embed Size (px)
Citation preview

Injury, Int. J. Care Injured xxx (2014) xxx–xxx
G Model
JINJ-5775; No. of Pages 6
Effects of unconsciousness during spinal immobilizationon tissue-interface pressures: A randomized controlledtrial comparing a standard rigid spineboard with a newlydeveloped soft-layered long spineboard§
Baukje Hemmes a,*, Peter R.G. Brink a,b, Martijn Poeze a,b,c
a Network Acute Care Limburg, Maastricht University Medical Center, Maastricht, The Netherlandsb Department of Traumatology, Maastricht University Medical Center, Maastricht, The Netherlandsc NUTRIM School for Nutrition, Toxicology and Metabolism, Maastricht University, Maastricht, The Netherlands
A R T I C L E I N F O
Article history:
Accepted 9 June 2014
Keywords:
Spineboard
Tissue-interface pressure
Anaesthetized patients
Trauma
A B S T R A C T
Background: Immobilization of the spine of patients with trauma at risk of spinal damage is usually
performed using a rigid long spineboard or vacuum mattress, both during prehospital and in-hospital
care. However, disadvantages of these immobilization devices in terms of discomfort and tissue-
interface pressures have guided the development of soft-layered long spineboards. We compared tissue-
interface pressures between awake and anaesthetized (unconscious) patients during immobilization on
a rigid spineboard and a soft-layered long spineboard.
Methods: In this comparative study, 30 anaesthetized patients were randomized to immobilization on
either the rigid spineboard or the soft-layered spineboard for the duration of their elective surgery.
Tissue-interface pressures measured using an Xsensor pressure-mapping device were compared with
those of 30 healthy volunteers who were immobilized sequentially on the rigid spineboard and the soft-
layered spineboard. Redness of the sacrum was also recorded for the anaesthetized patients immediately
after the surgery.
Results: For both anaesthetized patients and awake volunteers, tissue-interface pressures were
significantly lower on the soft-layered spineboard than on the rigid spineboard, both at start and
after 15 min. On the soft-layered spineboard, tissue interface pressure and peak pressure index (PPI) for
the sacrum were significantly lower for anaesthetized patients than for awake volunteers. Peak
pressures and PPI on the rigid spineboard were equal for both groups. Tissue-interface pressures did not
change significantly over time. Redness of the sacrum was significantly more pronounced on the rigid
spineboard than on the soft-layered spineboard.
Conclusions: This prospective randomized controlled trial shows that using a soft-layered spineboard
compared to a rigid spineboard for spinal immobilization resulted in lower tissue-interface pressures in
both awake volunteers and anaesthetized patients. Moreover, tissue-interface pressures on the soft-
layered spineboard were lower in anaesthetized patients than in awake volunteers. These findings show
the importance of using a soft-layered spineboard to reduce tissue-interface pressure, especially for
patients who cannot relieve pressure themselves by changing position.
� 2014 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
Injury
jo ur n al ho m epag e: ww w.els evier . c om / lo cat e/ in ju r y
§ Results of this study were presented at the 2nd Focus meeting of the EPUAP on
skin health and the microclimate, Southampton, UK, April 9, 2014.
* Corresponding author at: Network Acute Care Limburg, Maastricht University
Medical Center, PO Box 5800, 6202 AZ, Maastricht, The Netherlands.
Tel.: +31 43 3871435.
E-mail addresses: [email protected] (B. Hemmes),
[email protected] (Peter R.G. Brink), [email protected] (M. Poeze).
Please cite this article in press as: Hemmes B, et al. Effects of uncpressures: A randomized controlled trial comparing a standard rigid sInjury (2014), http://dx.doi.org/10.1016/j.injury.2014.06.006
http://dx.doi.org/10.1016/j.injury.2014.06.006
0020–1383/� 2014 Elsevier Ltd. All rights reserved.
Background
Spinal immobilization with long spineboards and cervicalcollars for extrication and transfer of trauma patients is a standardprecaution in both prehospital and in-hospital protocols [1].Especially for unconscious trauma patients, who are unable tomaintain spinal alignment by muscular tone, these methods areconsidered essential to protect the spine from further injury.
Although there is a general consensus that the patient shouldbe removed from the spineboard as soon as reasonably possible,
onsciousness during spinal immobilization on tissue-interfacepineboard with a newly developed soft-layered long spineboard.

B. Hemmes et al. / Injury, Int. J. Care Injured xxx (2014) xxx–xxx2
G Model
JINJ-5775; No. of Pages 6
the average time patients are reported to spend on a spineboardhas been estimated to be around 1 h [2,3]. There is extensiveevidence, however, that prolonged immobilization causes signifi-cant discomfort and pain, and on occasion may cause pressureulceration over bony prominences, leading to prolonged hospitalstay and increased cost of care [4–12].
Pressure ulceration occurs as a result of reduced perfusiondue to prolonged pressure and/or shear injury to the tissues.Increased pressure can lead to compression of the dermalcapillaries. When the pressure is relieved, reactive hyperaemia,clinically seen as a bright flush or reddened area that blanchesunder light pressure, can occur. At this stage of so-calledblanchable erythema, damage to the underlying tissues has notyet occurred [13]. Shear injury occurs as the result of sliding,when the soft tissues are stretched relative to each other. Theprocess of shear injury can occur quickly and the first signs ofcell damage can be seen within minutes. In a recent study wedemonstrated that when using a rigid spineboard, the maximumstrains on the tissues can exceed the threshold for deformationdamage [14]. Healthy conscious subjects may adopt pressurerelieving strategies, involving position changes, to minimize therisk of exceeding this threshold at specific body regions.However, unconscious patients are thought not to adopt thesestrategies and may therefore be at higher risk of developingpressure induced tissue damage.
Therefore, this study investigated the hypothesis that whenlying on a rigid spineboard, unconsciousness results in highertissue-interface pressure compared to the awake status. Inaddition, a recent comparative study reported significantly lowerinterface pressures on a prototype spine board with soft, coveredinlay [10]. Since the soft inlay may compensate for the lack ofmovement during unconsciousness, our second hypothesis wasthat there would be no difference in tissue-interface pressurebetween anaesthetized and awake status when lying on the soft-layered long spineboard.
Methods
Study design
We conducted a prospective, randomized, single-blinded,comparative study on tissue-interface pressures and redness ofthe skin using a standard rigid long spineboard and a soft-layeredlong spineboard in patients undergoing surgery under generalanaesthesia. Tissue interface pressures were compared with thoseof a group of awake healthy volunteers. The study has beenassigned ISRCTN96064657.
Table 1Subject characteristics.
Anaesthetized
Device Rigid spineboard
Number 15
Gender (M/F) 11/4
Age (years) 51.5 (16.2)
BMI (kg/m2) 24.5 (2.9)
Type of surgery
Hernia inguinalis 10/15
Hernia epigastrica 3/15
Hernia umbilicalis 2/15
Hernia inguinoscrotalis –
Time on immobilization device (min) 63 (18)
n.a.: not applicable.* P: a = difference between anaesthetized rigid spineboard and awake rigid spineboard
soft-layered spineboard P < 0.05; n.s.: not significant (P > 0.05).
Please cite this article in press as: Hemmes B, et al. Effects of unpressures: A randomized controlled trial comparing a standard rigid sInjury (2014), http://dx.doi.org/10.1016/j.injury.2014.06.006
Recruitment of participants
A sample of 30 patients (25 men and 5 women) was recruited atthe outpatient department of the Maastricht University MedicalCenter. Patients included were scheduled for open abdominal wallhernia repair under general anaesthesia, with an expected durationof less than 2 h. Patients with pressure ulceration either at time ofinclusion or in the medical history, or with pain other than that dueto the operation indication were excluded. Approval was obtainedfrom the Medical Research Ethics Committee of the MaastrichtUniversity Medical Center. Written informed consent wasobtained from all participants before they were enrolled in thestudy.
A power analysis was performed using the peak pressuresfound previously [10] on the standard rigid spine board and thesoft-layered long spineboard in awake and healthy volunteers. Thepower analysis showed that if we included 12 patients in each ofthe conditions, we should be able to detect a 25% increase in peakpressure index (PPI, see below) between awake and unconsciouspatients on the soft-layered spine board (mean PPI 171 (SD 33))with an alpha error of 0.05 and a beta error of 0.2.
Interventions
Two different support devices designed for prehospital traumacare were tested: a standard long spineboard (Ferno-Washington,Wilmington, OH), and a prototype soft-layered long spineboard.After induction of anaesthesia, patients were randomly assigned toone of the two devices. The pressure-mapping mat was placed onthe device and the patient was then placed on the device. Pressurewas recorded during the entire surgery. The control groupconsisted of awake healthy volunteers who were randomly puton each device for 15 min, with an interval between the devices of5 min, while tissue-interface pressures were recorded continu-ously.
Measurements
Tissue-interface pressures were continuously measured usingan Xsensor X2-6912 pressure-mapping device (Xsensor Technolo-gy, Calgary, Canada). This system consists of a thin, easily foldablefull-body pressure-mapping pad, equipped with 6912 capacitivesensors. This pad was placed between the subject and the supportsurface, without folds. Pressure on the sensors generates a voltagedifference, which increases linearly with the pressure. Weconnected the pad to a laptop computer with special Xsensorsoftware (version 4.2), for real-time pressure recording.
Anaesthetized Awake P*
Soft-layered
spineboard
Rigid spineboard,
soft-layered spineboard
15 30 –
14/1 19/11 b
49.6 (18.9) 39.0 (11.1) a,b
24.2 (3.2) 24.7 (3.4) n.s.
n.s.
11/15 n.a.
– n.a.
2/15 n.a.
2/15 n.a.
65 (12) n.a. n.s.
P < 0.05; b = difference between anaesthetized soft-layered spineboard and awake
consciousness during spinal immobilization on tissue-interfacepineboard with a newly developed soft-layered long spineboard.
B. Hemmes et al. / Injury, Int. J. Care Injured xxx (2014) xxx–xxx 3
G Model
JINJ-5775; No. of Pages 6
Directly after the surgery, visual inspection and semi-quantita-tive grading of the skin redness of the patient’s back wasperformed. Any redness was tested for being blanchable using aclear plastic disc, so as to distinguish between blanchable and non-blanchable erythema [15].
Outcome measures
Pressures were recorded continuously from the start ofthe anaesthesia until the end of the surgical procedure andreported as described previously [10]. Briefly, peak pressures (inmmHg) measured at the scapulae, the sacrum, and the heels wererecorded continuously. The Peak Pressure Index (PPI) wascalculated as a measure of pressure on a larger surface area
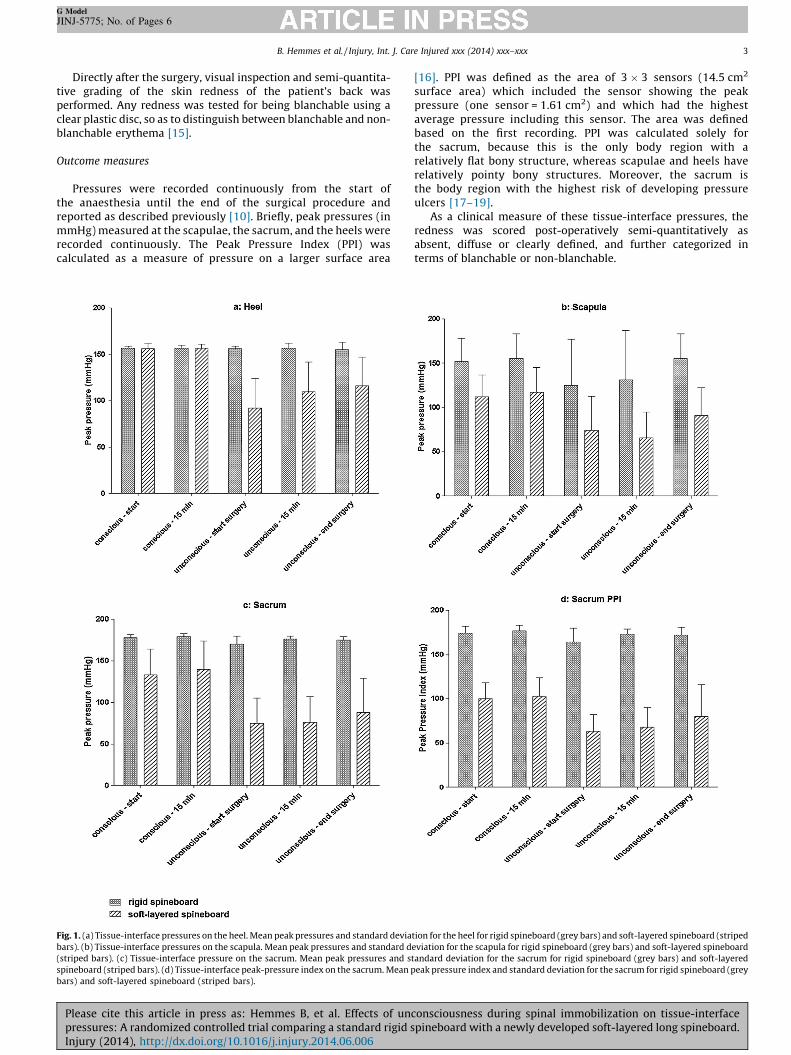
Fig. 1. (a) Tissue-interface pressures on the heel. Mean peak pressures and standard devia
bars). (b) Tissue-interface pressures on the scapula. Mean peak pressures and standard d
(striped bars). (c) Tissue-interface pressure on the sacrum. Mean peak pressures and s
spineboard (striped bars). (d) Tissue-interface peak-pressure index on the sacrum. Mean p
bars) and soft-layered spineboard (striped bars).
Please cite this article in press as: Hemmes B, et al. Effects of uncpressures: A randomized controlled trial comparing a standard rigid sInjury (2014), http://dx.doi.org/10.1016/j.injury.2014.06.006
[16]. PPI was defined as the area of 3 � 3 sensors (14.5 cm2
surface area) which included the sensor showing the peakpressure (one sensor = 1.61 cm2) and which had the highestaverage pressure including this sensor. The area was definedbased on the first recording. PPI was calculated solely forthe sacrum, because this is the only body region with arelatively flat bony structure, whereas scapulae and heels haverelatively pointy bony structures. Moreover, the sacrum isthe body region with the highest risk of developing pressureulcers [17–19].
As a clinical measure of these tissue-interface pressures, theredness was scored post-operatively semi-quantitatively asabsent, diffuse or clearly defined, and further categorized interms of blanchable or non-blanchable.
tion for the heel for rigid spineboard (grey bars) and soft-layered spineboard (striped
eviation for the scapula for rigid spineboard (grey bars) and soft-layered spineboard
tandard deviation for the sacrum for rigid spineboard (grey bars) and soft-layered
eak pressure index and standard deviation for the sacrum for rigid spineboard (grey
onsciousness during spinal immobilization on tissue-interfacepineboard with a newly developed soft-layered long spineboard.

Fig. 2. Example of diffuse redness on the sacrum after lying on the soft-layered
spineboard during surgery.
Table 2Redness at the sacrum, anaesthetized patients.
Redness at the sacrum Rigid
spineboard
Soft-layered
spineboard
Total
No redness 1 9 10
Diffuse redness 5 6 11
Clearly defined redness 9 0 9
Total 15 15 30
Chi2 = 15.49, P < 0.01.
B. Hemmes et al. / Injury, Int. J. Care Injured xxx (2014) xxx–xxx4
G Model
JINJ-5775; No. of Pages 6
Data collection and processing
Statistical analysis was performed using the Statistical Packagefor Social Sciences (SPSS, IBM), version 20.0.0.1. Pressures arepresented as mean � SD. Analysis of tissue-interface pressuresinvolved repeated-measures analysis of variance with correction ofthe degrees of freedom using the Greenhouse–Geisser estimates ofsphericity when Mauchly’s test indicated that the assumptionof sphericity had been violated, using time as the within-groupfactor and treatment as the between-group factor. Post hoc groupcomparisons at the different time points were only performed whenthe overall repeated-measures tests were statistically significant. Allscores were tested for normality using the Kolmogorov–Smirnov test.Parametric variables were compared using Student’s t-test, whilenon-parametric variables were compared using the Mann–Whitney U
statistic. Nominal variables were compared across independentgroups using the chi-squared test or Fisher’s exact test. Homogeneityof variance was assessed using Levene’s test. Level of significance wasset at P < 0.05.
Results
Patients
Characteristics of anaesthetized subjects and awake controlsare described in Table 1. No differences in demographics orbaseline characteristics were found between the patientsrandomized for rigid spineboard or soft-layered spineboard.Participants in the patient group were on average older and moreoften male than in the awake volunteers group. No relationshipwas found between pressure values and age or gender.
Fig. 3. Example of clearly defined redness on the sacrum after lying on the rigid
spineboard during surgery.
Please cite this article in press as: Hemmes B, et al. Effects of unpressures: A randomized controlled trial comparing a standard rigid sInjury (2014), http://dx.doi.org/10.1016/j.injury.2014.06.006
Tissue-interface pressures
In both awake volunteers and anaesthetized patients, peakpressures for scapula and sacrum and peak pressure index (PPI) atthe sacrum were significantly lower on the soft-layered spineboardthan on the rigid spineboard (Fig. 1a–d). Peak pressures at the heelwere similar for both devices for awake volunteers, and weresignificantly lower for patients under anaesthesia on the soft-layered spineboard than for the healthy volunteers. Peak pressuresand sacrum PPI on the soft-layered spineboard were significantlylower for anaesthetized patients compared to awake volunteers(P < 0.01). Peak pressures on rigid spineboard did not differbetween anaesthetized patients and awake volunteers (P > 0.05).No significant changes in pressure were seen during the course ofthe pressure measurements (P > 0.05).
Redness
Redness was assessed for anaesthetized patients only (Figs. 2and 3). There was a clear difference in redness on the sacrumafter surgery, with significantly more patients without anyredness at all on the soft-layered spineboard and significantlymore volunteers with clearly defined redness on the rigidspineboard (Table 2). In all cases the redness was blanchable andhad disappeared at the 2 h postoperative follow up assessment.
Discussion
This study showed that unconscious subjects placed on a soft-layered spine board had lower tissue-interface pressures thanconscious subjects, while no differences between these two groupswere found when using a rigid spine board. Patients underanaesthesia and awake controls both had significantly lowertissue-interface pressures on the soft-layered spineboard than onthe rigid spineboard.
Despite a growing body of evidence that immobilizing patientson a rigid spineboard can cause a number of adverse effects such asaspiration, respiratory problems, pain, and pressure ulceration[6,10,20–25], the use of spineboards is expected to continue inpractice. In addition to efforts to increase awareness in order tolimit the use of spineboards, more tissue-protective devices forspinal immobilization have been developed to minimize the risksof pain and pressure ulcer development. However, evidenceshowing how these products compare with traditionally used rigidspineboards is scarce. In an earlier study [10] we compared thetissue-interface pressures between the rigid spineboard and thesoft-layered spineboard in healthy, awake volunteers. It wasunknown, however, whether these results for conscious healthysubjects could be translated to the target group of patientsincapable of moving to relieve pressure, such as unconsciouspatients or patients with spinal cord injury. In this study wetherefore looked at anaesthetized patients as a proxy for thesepatient categories. The average duration of the surgical procedurewas about one hour, which is in practice equal to the average time atrauma patient is immobilized on a spineboard [2,3].
consciousness during spinal immobilization on tissue-interfacepineboard with a newly developed soft-layered long spineboard.

B. Hemmes et al. / Injury, Int. J. Care Injured xxx (2014) xxx–xxx 5
G Model
JINJ-5775; No. of Pages 6
Earlier studies showed that the use of a rigid spineboard leads todiscomfort and high tissue-interface pressures [6,9,10,16,21]. Wehave also previously demonstrated that using a rigid spineboardled to a considerably higher maximum tissue strain than thethreshold at which deformation damage can occur [14]. These hightissue-interface pressures are therefore a significant risk factor forthe development of pressure ulcers [26], which are bothdebilitating for the patient [27–29] and costly for the hospital[4,8,30]. We found equally high tissue-interface pressures for bothawake volunteers and anaesthetized patients using the rigidspineboard, with values comparable to those from earlier studies[6,10,16]. The tissue-interface pressures experienced by theunconscious patients on the rigid spineboard remained compara-ble to those for the awake subjects. In addition, tissue-interfacepressures on the soft-layered spineboard were significantly lowerfor the unconscious patients than for the awake volunteers. Boththese observations are remarkable, as they did not confirm ourinitial hypothesis that both spineboards would lead to an increasein pressures. The data from our study suggest that each board has aceiling effect. The rigid spineboard reaches this ceiling almostimmediately, while the tendency of the pressure to increase on thesoft-layered spineboard suggests that its ceiling effect is reachedlater. Although the former may be speculative, the bottom lineremains that the risk of tissue damage by pressure-induced tissuedeformation is reduced by using the soft-layered spineboardcompared to the rigid spineboard.
After removal from the spineboard, reactive hyperaemiaoccurred, indicating that there had been a period of relativehypoperfusion. This was especially noticeable with the rigidspineboard, with 9 out of 15 patients showing clearly definedredness, compared to 0 out of 15 patients on the soft-layeredspineboard. There is a trade-off between pressure and timeregarding pressure-induced tissue damage with higher pressurescausing tissue damage sooner than lower pressures [31,32]. In ourstudy the pressures did not lead to permanent damage to the softtissue; the redness had disappeared in all patients at the follow upassessment of the skin two hours after the end of the surgery. Thepatients remained haemodynamically stable during the procedureand had only low-risk comorbidities. Tissue hypoperfusion leadingto tissue ischaemia and cell necrosis occurs more rapidly inhypotensive patients because of compromised microcirculationcaused by poor perfusion [25]. Especially patients with shock orspinal cord damage combined with altered conscious levels are atincreased risk of hypotension, so immobility, time or pressure-related risk factors should be reduced.
A number of comments need to be made on the interpretationof our observations. First, although weight and body mass index ofthe participants were representative of those in the general Dutchpopulation, age and gender were not completely comparablebetween healthy volunteers and the patients undergoing surgeryand anaesthesia. Second, our study was single-blinded, as theresearcher who performed the pressure measurements andredness evaluations knew which device the volunteer was lyingon. However, pressure measurements were objectified by usingthe Xsensor pressure mapping device. Redness was objectified bytesting blanchableness using a clear plastic disc. Photos were takento enable classification of the redness afterwards. The redness ofthe skin was also judged by an independent, blinded observer withno knowledge of the allocation of the patients. Kappa was 0.811and differences of opinion were resolved through discussion.Furthermore, visual inspection of the skin was undertaken as anindicator of tissue damage. Although hyperaemia was noted in asignificant number of patients, we do not know how this relates totissue ischaemia and cell necrosis. Further studies should thereforefocus on the relation between local tissue-interface pressures andindicators of tissue damage.
Please cite this article in press as: Hemmes B, et al. Effects of uncpressures: A randomized controlled trial comparing a standard rigid sInjury (2014), http://dx.doi.org/10.1016/j.injury.2014.06.006
In conclusion, this randomized study found tissue-interfacepressures to be significantly lower for the soft-layered spineboardthan for the rigid spineboard, for both awake volunteers andanaesthetized patients. Furthermore, tissue-interface pressuresusing the soft-layered spineboard were lower for the anaesthetizedpatients than for the awake volunteers. Redness of the skin of thesacrum was significantly less on the soft-layered spineboard thanon the rigid spineboard. These findings show the importance ofusing a soft-layered spineboard for tissue-interface pressurereduction, and may be of importance for trauma patients with areduced level of consciousness.
Conflict of interest
The authors state there are no conflicts of interest. No externalfunding was received for this study.
References
[1] American College of Surgeons Committee on Trauma. Advanced Trauma LifeSupport for doctors, Chicago, IL; 2008.
[2] Cooney DR, Wallus H, Asaly M, Wojcik S. Backboard time for patients receivingspinal immobilization by emergency medical services. Int J Emerg Med2013;6:17–9.
[3] Lerner EB, Moscati R. Duration of patient immobilization in the ED. Am J EmergMed 2000;18:28–30.
[4] Allman RM, Goode PS, Burst N, Bartolucci AA, Thomas D. Pressure ulcers,hospital complications, and disease severity: impact on hospital costs andlength of stay. Adv Skin Wound Care 1999;12:22–30.
[5] Baldwin KM, Ziegler SM. Pressure ulcer risk following critical traumatic injury.Adv Skin Wound Care 1998;11:168–75.
[6] Cordell WH, Hollingsworth JC, Olinger ML, Stroman SJ, Nelson DR. Pain andtissue-interface pressure during spine-board immobilization. Ann Emerg Med1995;26:31–6.
[7] Dealey C, Posnett J, Walker A. The cost of pressure ulcers in the UnitedKingdom. J Wound Care 2012;21:261–6.
[8] Graves N, Birrell FA, Whitby M. Modeling the economic losses from pressureulcers among hospitalized patients in Australia. Wound Repair Regen2005;13:462–7.
[9] Hauswald M, Hsu M, Stockoff C. Maximizing comfort and minimizing ische-mia: a comparison of four methods of spinal immobilization. Prehosp EmergCare 2000;4:250–2.
[10] Hemmes B, Poeze M, Brink PRG. Reduced tissue-interface pressure and in-creased comfort on a newly developed soft-layered long spineboard. J Trauma2010;68:593–8.
[11] Watts D, Abrahams E, MacMillan C, Sanat J, Silver R, VanGorder S, et al. Insultafter injury: pressure ulcers in trauma patients. Orthop Nurs 1998;17:84–91.
[12] Zlupko GR, Megargel RE, O’Connor RE. Patient discomfort due to indiscrimi-nant use of spinal immobilization. Prehosp Emerg Care 2004;8:101.
[13] Dealey C, Lindholm C. Pressure ulcer classification. In: Romanelli M, Clarck M,Cherry G, Colin D, Defloor T, editors. Science and practice of pressure ulcermanagement. London, UK: Springer London; 2006.
[14] Oomens CWJ, Zenhorst W, Broek M, Hemmes B, Poeze M, Brink PRG, et al. Anumerical study to analyse the risk for pressure ulcer development on a spineboard. Clin Biomech 2013;28:736–42.
[15] Vanderwee K, Grypdonck MHF, de Bacquer D, Defloor T. The reliability of twoobservation methods of nonblanchable erythema, grade1 pressure ulcer. ApplNurs Res 2006;19:156–62.
[16] Keller BPJA, van Overbeeke J, van der Werken Chr. Interface pressure mea-surement during surgery: a comparison of four operating table surfaces. JWound Care 2005;15:5–9.
[17] Amlung SR, Miller WL, Bosley LM. The 1999 National Pressure Ulcer Preva-lende Study: a benchmarking approach. Adv Skin Wound Care 2001;14:297–301.
[18] Vanderwee KM, Clark M, Dealey C, Gunningberg L, DeFloor T. Pressure ulcerprevalence in Europe: a pilot study. J Eval Clin Pract 2007;13:227–35.
[19] Vangilder C, Macfarlane GD, Meyer S. Results of nine international pressureulcer prevalence surveys: 1989 to 2005. Ostomy Wound Manage 2008;54:40–54.
[20] Brownlee AE. Managing spinal immobilisation devices in the emergencydepartment. Australas Emerg Nurse J 2005;8:79–83.
[21] Chan D, Goldberg RM, Mason J, Chan L. Backboard versus mattress splintimmobilization: a comparison of symptoms generated. J Emerg Med1996;14:293–8.
[22] Kwan I, Bunn F. Effects of prehospital spinal immobilization: a systematicreview of randomized trials on healthy subject. Prehospital Disaster Med2005;20:47–53.
[23] Vickery D. The use of the spinal board after the pre-hospital phase of traumamanagement. Emerg Med J 2001;18:51–4.
onsciousness during spinal immobilization on tissue-interfacepineboard with a newly developed soft-layered long spineboard.

B. Hemmes et al. / Injury, Int. J. Care Injured xxx (2014) xxx–xxx6
G Model
JINJ-5775; No. of Pages 6
[24] Bauer D, Kowalski R. Effect of spinal immobilization devices on pulmonaryfunction in the healthy, nonsmoking man. Ann Emerg Med 1988;17:915–8.
[25] Berg G, Nyberg S, Harrison P, Baumchen J, Gurss E, Hennes E. Near-infraredspectroscopy measurement of sacral tissue oxygen saturation in healthy volun-teers immobilized on rigid spine boards. Prehosp Emerg Care 2010;14:419–24.
[26] DeFloor T. The risk of pressure sores: a conceptual scheme. J Clin Nurs1999;8:206–16.
[27] Hopkins A, Dealey C, Bale S, DeFloor T, Worboys F. Patient stories of living witha pressure ulcer. J Adv Nurs 2006;56:345–53.
[28] Gorecki C, Brown JM, Nelson EA, Briggs M, Schoonhoven L, Dealey C, et al.Impact of pressure ulcers on quality of life in older patients: a systematicreview. J Am Geriatr Soc 2009;57:1175–83.
Please cite this article in press as: Hemmes B, et al. Effects of unpressures: A randomized controlled trial comparing a standard rigid sInjury (2014), http://dx.doi.org/10.1016/j.injury.2014.06.006
[29] Spilsbury K, Nelson A, Cullum N, Iglesias C, Nixon J, Mason S. Pressure ulcersand their treatment and effects on quality of life: hospital inpatient perspec-tives. J Adv Nurs 2007;57:494–504.
[30] Bennett GG, Dealey C, Posnett J. The cost of pressure ulcers in the UK. AgeAgeing 2004;33:230–5.
[31] Reswick J, Rogers J. Experience at the Rancho Los Amigos Hospitalwith devices and techniques to prevent pressure sores. In: Reswick J,Rogers J, editors. Bed sore mechanics. London: MacMillan Press; 1976 . p.301–10.
[32] Linder-Ganz E, Engelberg S, Scheinowitz M, Gefen A. Pressure-time cell deaththreshold for albino rat skeletal muscles as related to pressure sore biome-chanics. J Biomech 2006;39:2725–32.
consciousness during spinal immobilization on tissue-interfacepineboard with a newly developed soft-layered long spineboard.





























