Embed Size (px)
Citation preview

Effects of High-dose and Low-dose Preoperative Irradiation on Low Anterior Anastomoses in Dogs*
MELVIN P. BUBRICK, M.D., t ERIC S. ROLFSMEYER, M.D.,+ ROBERT M. SCnAUER, M.D.,f DANIEL A. FEENEY, D.V.M.,+ GARY R. JOHNSTON, D.V.M.,$ ROBERT L. STROM, M.D.,} CLAUDE R. HITCHCOCK, M.D., PH.D.'~
Bubrick MP, Rolfsmeyer ES, Schauer RM, Feeney DA, Johnston GR, Strom RL, Hitchcock CR. Effects of high-dose and low-dose preoperative irradiation on low anterior anastomoses in dogs. Dis Colon Rectum 1982;25:406-415.
Twenty mongrel dogs underwent preoperative irradiation to the colon and rectum, receiving 4000 rads according to the Nominal Standard Dose Equation. Each dog then underwent anterior re- section of the rectosigmoid, and reconstructive technique was randomized into two groups consisting of either handsewn or EEA-stapled anastomoses. Anastomoses were examined digital ly and radiographically at the time of surgery and on the seventh postoperative day. There were four radiographic leaks among the handsewn anastomoses, but only one was cl inical ly significant and associated with peritonitis. There were no leaks among the ten EEA-stapled anastomoses. The data suggest that low anterior resection and anastomosis can be done safely after 4000 rad ir- radiation and that the EEA-stapled anastomosis may be prefer- able. [Key words: Anastomosis; Carcinoma, Colon; Radiation therapy; Rectum; Stapling device]
THE MANAGEMENT OF carc inoma o f the colon and rec tum has included the adjunctive use of radia t ion the rapy u n d e r a wide n u m b e r of protocols over m a n y years. 1-1~ Al though controversy exists over the op- t i m u m methods of utilizing radiat ion therapy, it ap- pears clear that there are some clearcut benef i t s f rom its use in colorectal cancer.
T h e cu r ren t t rend in the surgical m a n a g e m e n t of carc inoma o f the r ec tum and rec tos igmoid involves the use of opera t ions des igned to spare the rectal sphincter and preserve continence. 12 T h e in t roduc- tion of the EEA stapling device in par t icular has ex- t e n d e d the range of the low an te r io r resect ion to allow for preserva t ion of the r ec tum in the presence of low-lying tumors that were previously t rea ted by abdominope r inea l resection a lone? 8
* Presented as part of symposium at the meeting of the Ameri- can Society of Colon and Rectal Surgeons, Colorado Springs, Col- orado, June 7 to 11, 1981.
Address reprint requests to Dr. Bubrick: Hennepin County Med- ical Center, 701 Park Avenue, Minneapolis, Minnesota 55415.
From the Departments of +Surgery and w Hennepin Coun O' Medical Center;
the Minneapolis Medical Research Foundation; and the $Department of Small Animal Clinical Sciences,
Universih' (~ Minnesota College of Veterina U Medicine,
Minneapolis Minnesota
T h e combinat ion of surgery and p reopera t ive ir- radiat ion the rapy for low-lying lesions of the r ec tum previously has had limited usage largely because o f fear on the par t o f the su rgeon that p reopera t ive radiat ion the rapy might commi t the pat ient to have an abdominope r inea l resection in situations where low an te r io r resection might have technically been possible. This reflects the long-held view that the risks o f p e r f o r m i n g a low anastomosis in an i r radia ted field are unacceptably high. Recent r epo r t s f r o m the litera- ture , however , suggest that bowel anas tomoses , in fact , can be p e r f o r m e d sa fe ly a f t e r i r r a d i a t i o n therapy utilizing e i ther handsewn or stapling tech- niques.Z, lo, 11, la. 1~, 16
A prev ious an imal s tudy f r o m o u r l a b o r a t o r y TM
showed that such anas tomoses were safe af ter 2000 rads of i r radiat ion. This fol low-up study was des igned to assess this ma t t e r f u r t he r by p re t r ea t ing the colon and rec tum with the equivalent o f 4000 rads and then evaluat ing the safety o f p e r f o r m i n g an anastomosis using the handsewn and stapling techniques.
M e t h o d s a n d M a t e r i a l s
Twen ty mongre l dogs weighing 39 to 52 pounds unde rwen t the equivalent o f 4000-rad p reopera t ive radiat ion the rapy to the r ec tum by the following pro- tocol (Fig. 1): 250 kVp, 15 m A or thovol tage x-ray unit was used, and surface source distance (SSD) was 50 cm. T h e half-value layer o f the x-ray b e a m was 2.6
0012-3706/82/0700/0406/$01.30 �9 American Society of Colon and Rectal Surgeons
4 0 6
Volume 25 Number 5 HIGH- AND LOW-DOSE IRRADIATION 407
q ~ ; "r
Site of transverse 1 ~ j
section ~d,{6~z m~"16 c .~ "fi B" t" ; ' ' ' '~ "Q- s ~c./A I 4~k- - J ' -
SZ
114 total 0 ~ exposure / /
PORTAL eact / / given from / . - f PORTAL C
\ portJ I / /4cn ~/ / cm surface covered / / by portals A & B
R-meter within -~ 7cm ~- plastic shield
Thimble chamber portion of R-meter (measured exposure 1502.6 Roentgens total)
,,,,o,,, / , / \ exposure / _ e ~ / P O R T A L PORTAL \ ~ \\given from/ ~ / ' B
\ - ~ \ aech / _ ~ /
Plastic tubing Thimble shield for chamber portion R-meter of R-meter
(measured exposure 1502.6 Roentgens total)
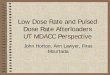
FIG. l. Protocol for administration of 4000 rads by NSD equation.
mm of coppe r (mm Cu). T h e radiat ion dose was measu red utilizing a " th imble" radiat ion c h a m b e r (Victoreen R meter, Model 500 and thimble chamber Model 550-6A, Vic to reen Inc., Cleve land , Ohio) placed in the rec tum with the sensitive volume in the center of the x-ray beam. Plastic tubing was placed in the rec tum to protec t the R meter f rom damage due to peristalsis or feces. While radiation was adminis- tered the accumulated dose was moni to red for each portal to allow accurate dosimetry.
Ventral dorsal, r ight-to-left obfique (VDRLO), and left-to-right oblique (VDLRO) portals were used to adminis ter 716 rads to a 4-cm length o f the rec tum in o ne dose . A n t e r o p o s t e r o v e n t r a l do r sa l o b l i q u e (APVDO) and pos te roan te roven t ra l dorsal obl ique (PAVDO) portals were used to adminis ter 716 rads to the same 4-cm length o f the rec tum in one dose. T h e area o f the colon receiving i rradiat ion was cen te red along a line pe rpend icu la r to the long axis o f the body, 7 cm f rom the anus. T h e VDRLO and VDLRO portals exposed an area 4 x 6 cm on the surface o f each dog's skin on the side o f the x-ray tube. T h e APVDO and PAVDO exposed an area o f 6 cm o f skin surface located an ter ior ly and posteriorly, respec- tively, to the VDRLO and VDLRO portals, with no surface overlap. Each o f the four portals del ivered
358 rads to the colon. T h e angle (off vertical) for each portal was de te rmined specifically for each animal, depend ing on body weight and shape.
Calculations were p lanned to simulate a 4000-rad, 26-day, 20-fraction, high-dose protocol for preopera-
segment
Group I I Group II Randomized
Hand sutured
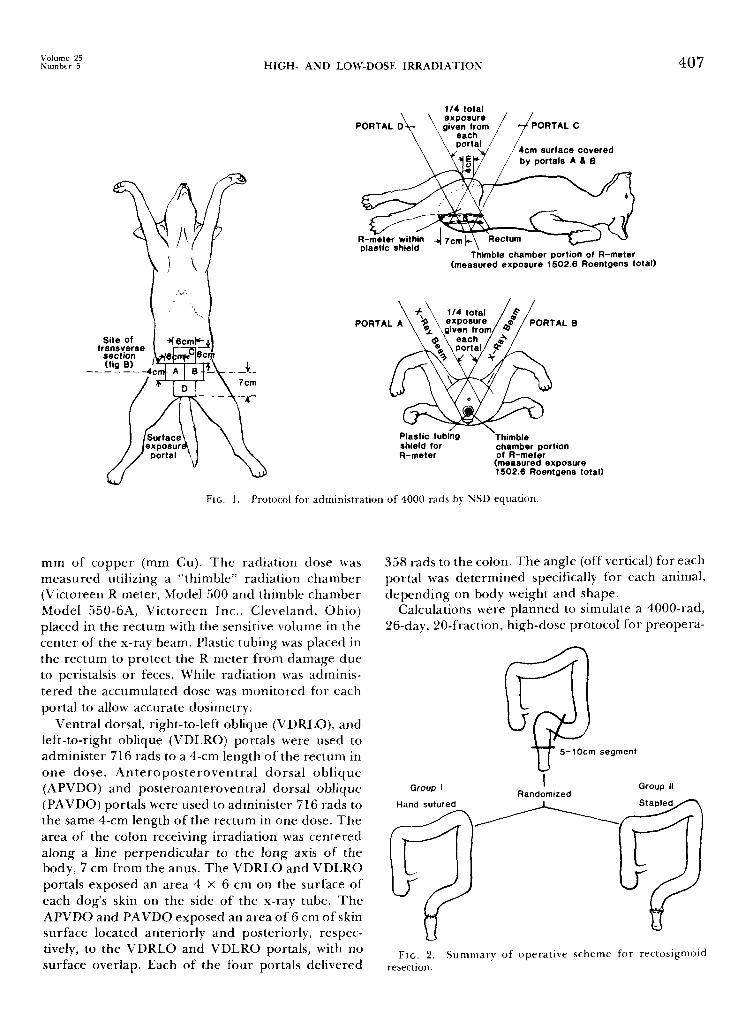
FIc. 2. Summary of operat ive scheme for rectosigmoid resection.
Dis. Col. & Rect. 408 B U B R 1 C K , E T AL. July-August 1982
tive irradiat ion therapy using the Nominal S tandard Dose Equat ion (NSD) as follows2~ NSD = dose (total) • (days on treatment) -'H • (number o f frac- tions) -'24. According to the NSD equation, a total dose o f 1362 rads was to be del ivered by four portals (340.5 rads per portal). A 5 per cent increase in dep th dose was adminis tered to compensate for absorpt ion o f the plastic tubing on the dorsal side o f the R meter .
After a three-week rest period, the dogs were ran- domly selected to undergo low anter ior resection and anastomosis using e i ther a two-layer invert ing hand- sewn t e c h n i q u e ( G r o u p I) o r an E E A - s t a p l e d technique (Group II).
T h e preopera t ive prepara t ion , surgical technique, and postoperat ive radiographic study method were identical to those descr ibed previously for similar studies f rom this laboratory, x9'2~ Preoperat ive prep- aration consisted of mechanical bowel cleansing with three per ioperat ive int ravenous doses o f carbenicillin (Geopen| Surgery was done t h rough a midline inci- sion using aseptic technique and in t ravenous sodium thiopental anesthesia. At operat ion, the rec tum was fully mobilized, bo th lateral rectal stalks were divided, and a 5-to-10-cm segment o f rectosigmoid was re-
sected. An end- to -end anastomosis was then made be- tween the proximal sigmoid and the ext raper i toneal rectum using ei ther of the two operat ive techniques (Fig. 2).
Anas tomoses were eva lua ted by b a r i u m - e n e m a examinat ion on the day o f surgery and on the seventh postoperat ive day and then every seven days if a leak was identified. T h e level o f anastomosis was evaluated by digital examinat ion on the day of surgery and on the seventh postoperat ive day. T h e abdominal wound was also inspected at this time. All dogs were killed at one to two m o n t h s pos topera t ive ly and carefu l ly examined for evidence of anastomotic dehiscence, per ianastomotic abscess, and in t raper i toneal abscess.
Resul t s
Ef fec t s o f Irradiat ion: T h e irradiation was toler- ated well by the animals. T h e r e was some evidence of skin damage and alopecia in all animals, slightly more marked than that seen in animals subjected to lower- dose irradiat ion. Grossly, at surgery, the rectosig- moid, p rox imal colon, and small bowel a p p e a r e d normal. Histologically, all resected specimens were
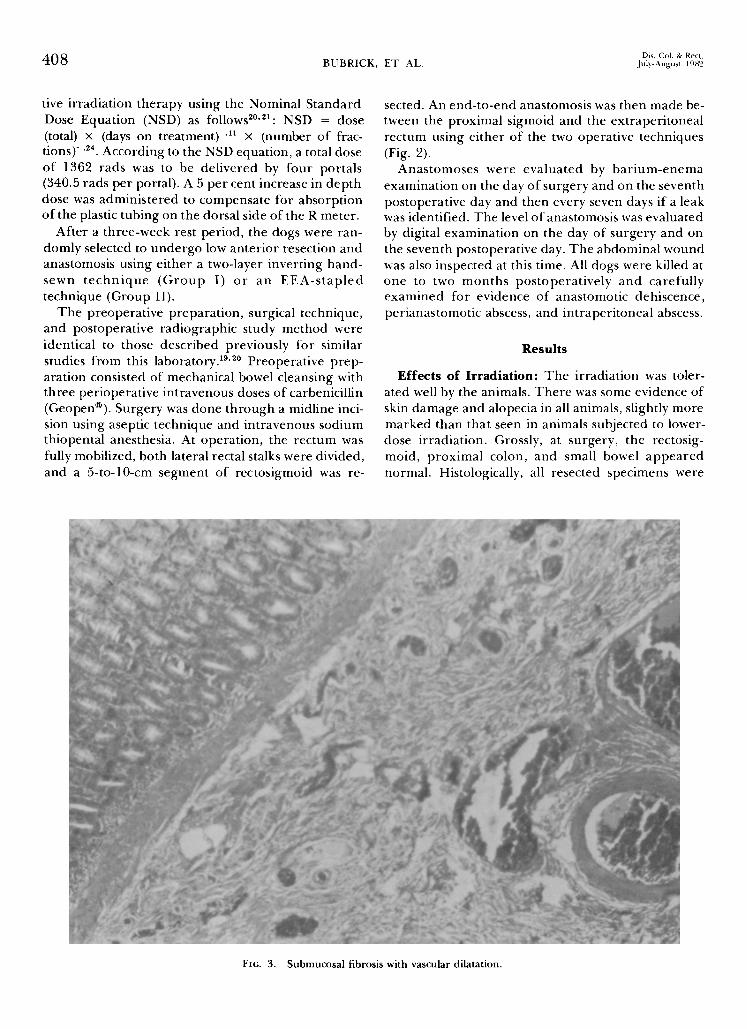
FIG. 3. Submucosal fibrosis with vascular dilatation.

Volume 25 Number 5 H I G H - A N D L O W - D O S E I R R A D I A T I O N 409
FIG. 4. N e o v a s c u l a r i z a t i o n .
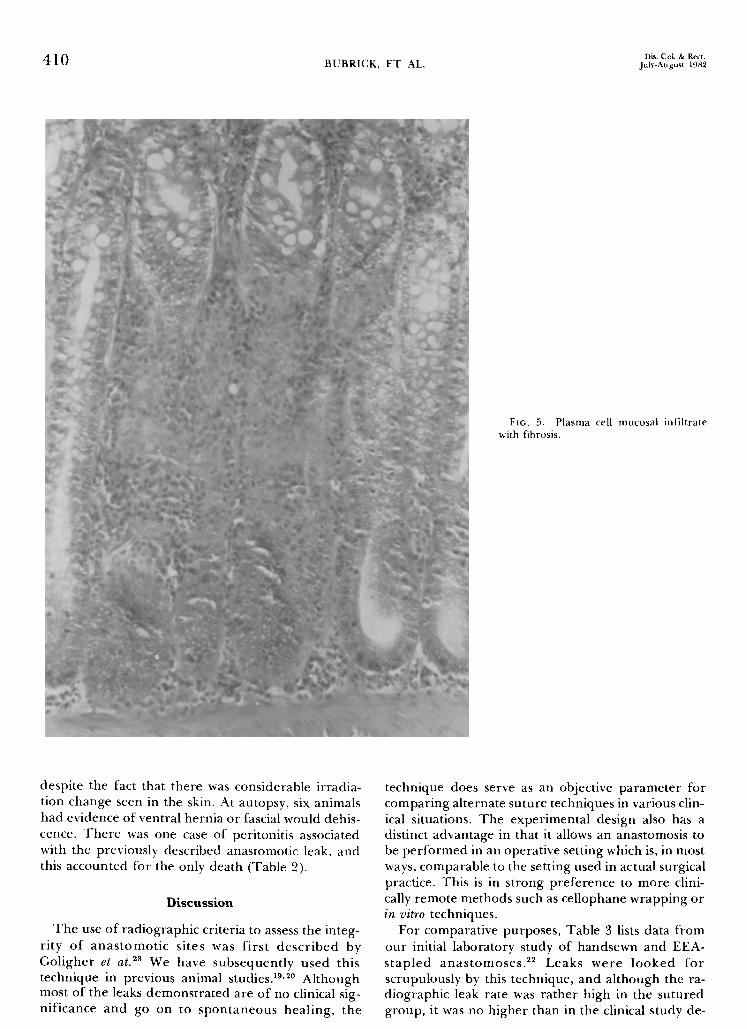
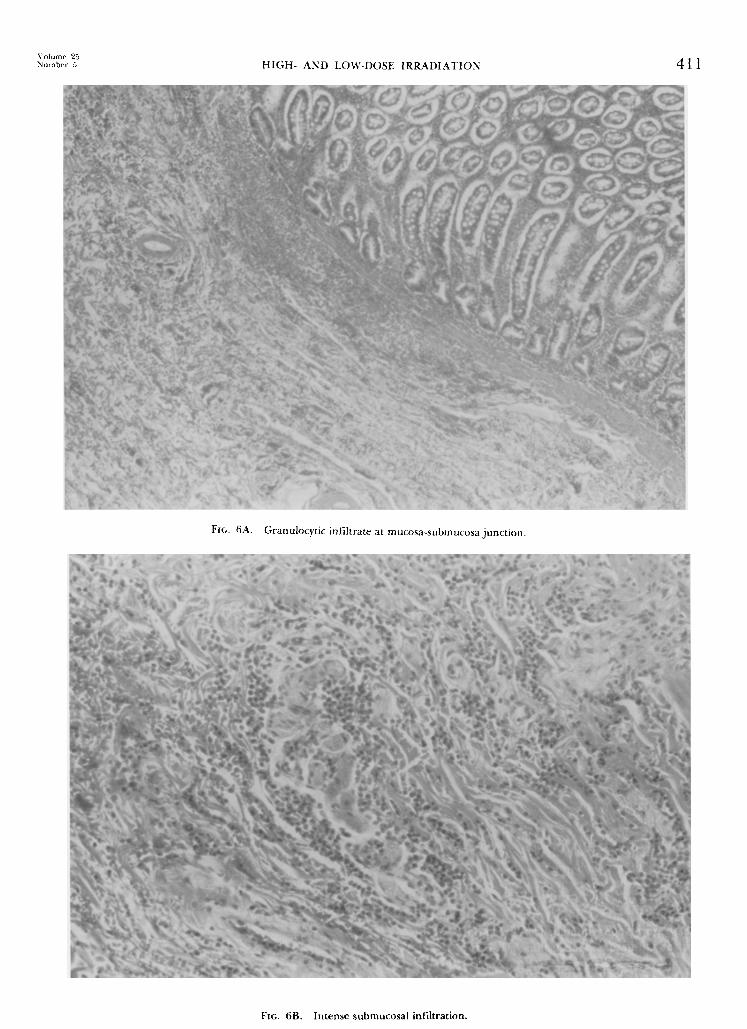
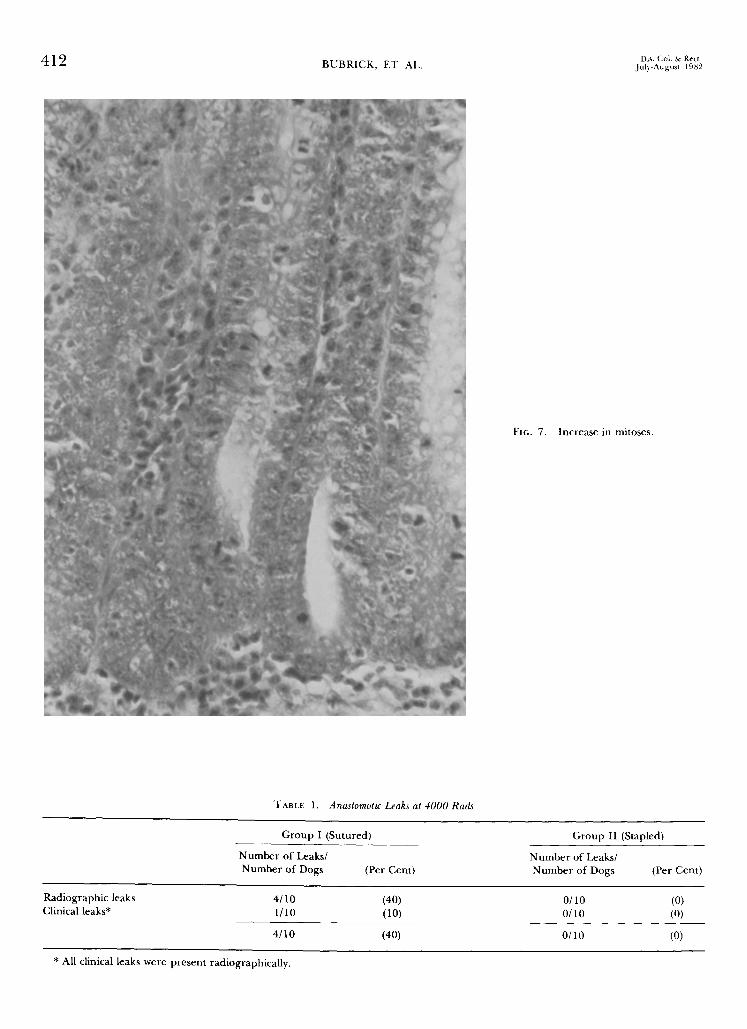
found to have evidence o f irradiation effect. These changes appeared as extension of the changes previ- ously noted at 2000 rads. The key findings included (1) submucosal fibrosis with vascular dilatation (Fig. 3), (2) neovascularization of the mucosa (Fig. 4), (3) plasma cell mucosal infiltrate with fibrosis (Fig. 5), (4) granulocytic infiltration at the junct ion of the mucosa and submucosa (Fig. 6A), with extension of this infil- trate into the submucosa (Fig. 6B, and (5) some evi- dence of increased mitoses (Fig. 7).
Level of Anastomosis: All anastomoses measured within 6 cm of the dentate line.
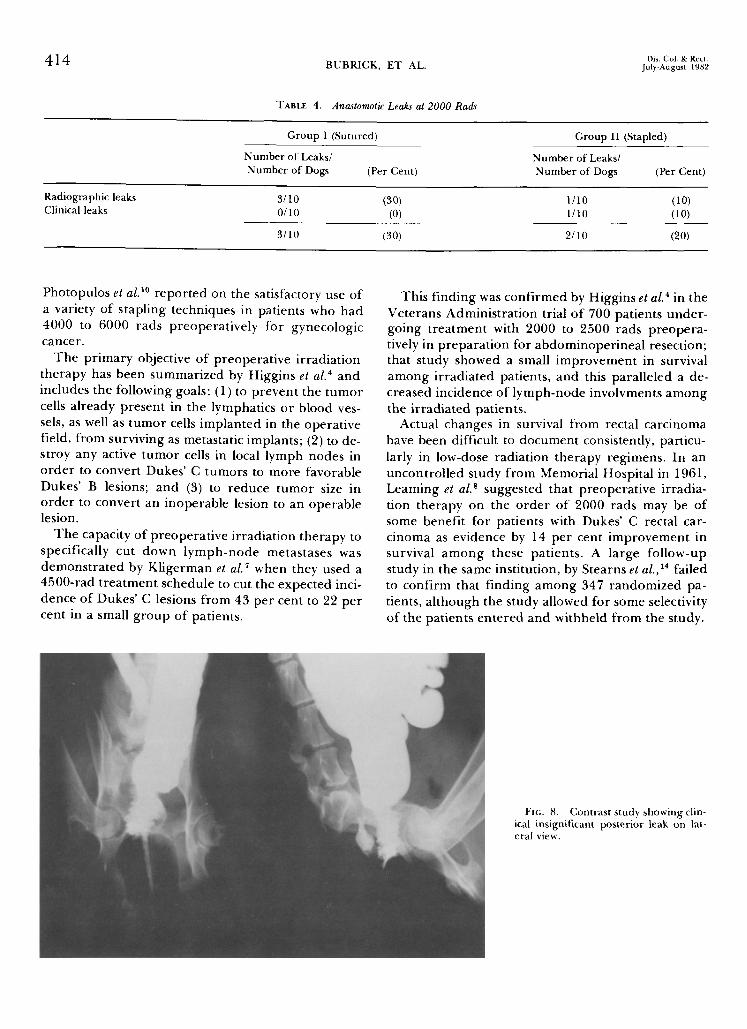
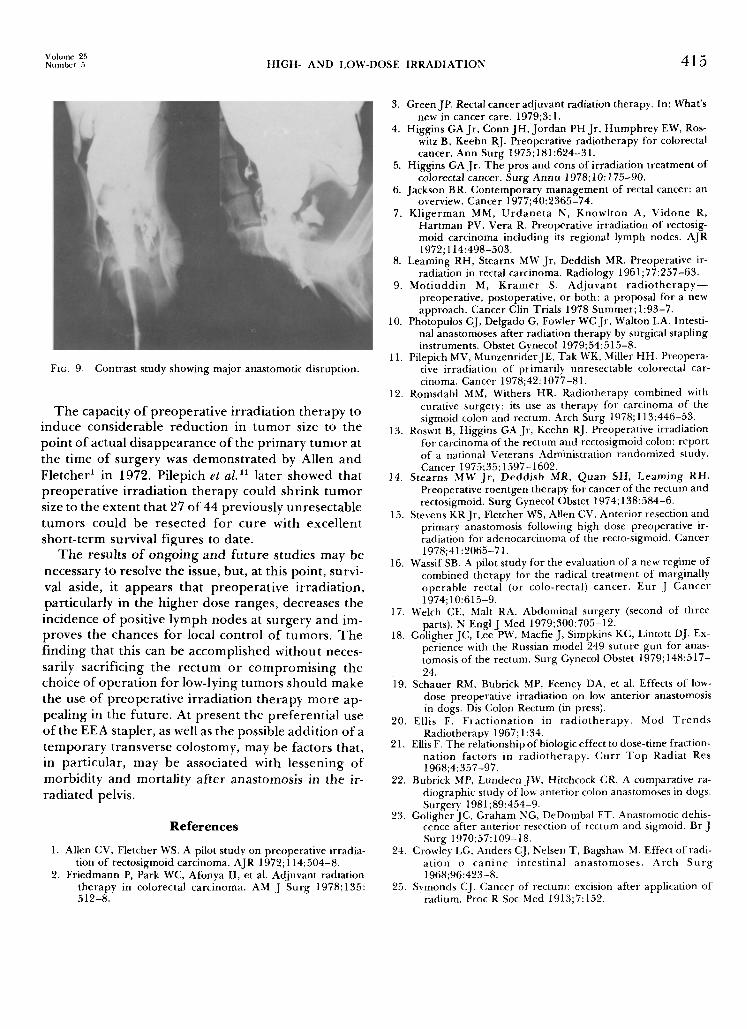
Anastomot ic Leaks: T h e r e were f o u r radio- graphically identified leaks in the ten Group I dogs (40 per cent) and no leaks among the 10 Group II dogs (Table 1). These data are marginally significant (P < 0.08). None of the leaks were demonstrable in the immediate postoperative period. Three o f the leaks were harmless and closed spontaneously within 14 days of the time of discovery (Fig. 8). One of the leaks was clinically significant and the dog went on to develop peritonitis and died as a result of it (Fig. 9).
Complications: There were no wound infections as evidenced by clinical cellulitis or pu ru len t exudate,
Dis. Col. & Rect. 410 B U B R I C K , E T AL, July-August 1982
FIG. 5. P lasma cell mucosa l infi l t rate with fibrosis.
despite the fact that there was considerable irradia- tion change seen in the skin. At autopsy, six animals had evidence of ventral hernia or fascial would dehis- cence. T h e r e was one case of peritonitis associated with the previously described anastomotic leak, and this accounted for the only death (Table 2).
D i s c u s s i o n
T h e use o f radiographic criteria to assess the integ- r i ty o f a n a s t o m o t i c si tes was f i rs t d e s c r i b e d by Gol igher et at. 23 We have subsequent ly used this technique in previous animal studies. 19,2~ Al though most of the leaks demons t ra t ed are o f no clinical sig- n i f icance and go on to s p o n t a n e o u s heal ing, the
technique does serve as an objective pa ramete r for compar ing al ternate suture techniques in various clin- ical situations. T h e exper imenta l design also has a distinct advantage in that it allows an anastomosis to be p e r f o r m e d in an operat ive setting which is, in most ways, comparable to the setting used in actual surgical practice. This is in s trong p re fe rence to more clini- cally remote methods such as cel lophane wrapping or in vi tro techniques.
For comparat ive purposes, Table 3 lists data f rom our initial laboratory study of handsewn and EEA- s t a p l e d a n a s t o m o s e s . ~2 Leaks we re l o o k e d fo r scrupulously by this technique, and a l though the ra- diographic leak rate was ra ther high in the su tured group, it was no h igher than in the clinical s tudy de-
Volume 25 Number 5 H I G H - AND LOW-DOSE I R R A D I A T I O N 411
FIG. 6B. In tense submucosa l infi l t rat ion.
Dis. Col. & Rect. 412 BUBRICK, ET AL, Jul)-August 1982
FIG. 7. Increase in mitoses.
TABLE I. Anastomotic Leaks at 4000 Rads
Group I (Sutured)
Number of Leaks/ Number of Dogs (Per Cent)
Group II (Stapled)
Number of Leaks/ Number of Dogs (Per Cent)
Radiographic leaks Clinical leaks*
4/10 (40) 1/10 (10)
4/10 (40)
O/10 (0) O/i 0 (0)
O/10 (0)
* All clinical leaks were present radiographically.

V o l u m e 25 .X'umber 5 H I G H - AND LOW-DOSE I R R A D I A T I O N 413
TABLE 2. Complications
Number of Complications/ Number of Dogs (Per Cent)
Wound infections 0/20 (0) Ventral hernia or 6/20 (30)
wound dehiscence
Peritonitis 1/20 (5)
Total complications 7/20 (35)
Deaths 1/20 (5)
scribed by Goligher et al. z3 Table 4 lists the results o f two comparable groups o f dogs t reated with lower dose p r e o p e r a t i v e i r r ad ia t ion cons is t ing o f 2000 rads. TM No statistically significant d i f fe rence could be detected between the two techniques. In the cu r ren t study, the 40 per cent leak rate among su tured dogs compared with the 0 per cent leak rate among stapled dogs is o f m a r g i n a l statist ical s ign i f icance . It is noteworthy, however, that the definite t rend in all three studies is toward a strong p re fe rence in favor o f the EEA-stapled anastomosis regardless o f the ex- per imenta l situation.
Perhaps o f g rea te r concern in this s tudy is the demons t ra t ion that an anastomosis can be done safely regardless o f technique af ter ra ther high dosages o f p r e o p e r a t i v e i r r ad ia t ion the rapy . T h e s tudy was made feasible by utilization o f the nominal s tandard dose equation. Limitations of the nominal s tandard dose equat ion have been discussed previously by us? 9 Despite its drawbacks, we found working with the NSD concept far super ior to a t tempt ing any fraction- ated irradiat ion schedules on exper imenta l animals. Logistic and technical cons idera t ions would have made the use o f f rac t ionated schedules especially undesirable.
T h e choice o f the three-week resting per iod af te r radiat ion therapy until the time o f surgery was found
tO be satisfactory in o u r previous work, and this choice is consistent with the time selected f rom the exper imenta l work o f others. 24
Only minimal data are available in the l i terature on the safety of pe r fo rming a low anter ior anastomosis af ter high-dose radiation therapy. Actually, the first case of combined radiation therapy and t u m o r exci- sion for rectal carcinoma was r epor t ed in 1914 by Symonds, 2~ who t reated a rectal t u m o r with rad ium and subsequently r emoved the t u m o r and reun i ted the bowel.
Crowley et al . d e m o n s t r a t e d that can ine anas- tomoses could be done safely af ter 1500 rads of treat- ment. O u r recent s tudy utilizing 2000 rads gave simi- lar resu l t s with 95 p e r cen t o f all a n a s t o m o s e s ultimately healing. TM Roswit et al. 13 noted, in the Veterans Administrat ion Surgical Adjuvant Study Group, that wound healing was satisfactory among patients who received low-dose irradiat ion and who subsequently did have anastomoses. In 1978, Stevens et al. 15 re- po r t ed on 13 patients u n d e r g o i n g t r ea tmen t with 5000 rads preoperat ively, followed by low an te r ior resection. Th o se au thors no ted an increased inci- dence of pelvic and anastomotic complications and r e c o m m e n d e d t em p o ra ry colostomy before having patients undergo such anastomoses in the future .
F r i edmann et aL z recently r epor ted on six patients undergo ing pelvic anastomoses af ter receiving 4500 to 5000 rads preoperat ively. All anastomoses were protected with a proximal colostomy; two minor anas- tomotic leaks did develop, but ultimately the leaks healed and all colostomies could be taken down. Was- sir a6 described four patients receiving modera te -dose irradiation therapy at 3450 rads with subsequent safe anastomoses. Pilepich et al. H t reated 44 patients, hav- ing otherwise unresectable colorectal carcinoma, with a combinat ion o f 4500- to 6000-rad radiat ion the rapy followed by surgery. Seven o f the patients u n d e r w e n t an ter ior resection protected u n d e r cover o f a trans- verse colostomy. T h e anastomoses healed wi thout complications in all seven patients. More recently,
TABLE 3. Anastomotic Leaks in Nonirradiated Dogs
Group I (Sutured)
Number of Leaks/ Number of Dogs (Per Cent)
Group II (Stapled)
Number of Leaks/ Number of Dogs (Per Cent)
Radiographic leaks Clinical leaks*
13/20 (65) 4/20 (20)
13/20 (65)f
4/20 2
(2O) (10)
4/20 (20)
* All clinical leaks were present radiographically. t P < 0.003.
Dis. Col. & Rect. 414 BUBRICK, ET AL. July-August 1982
TABLE 4. Anastomotic Leaks at 2000 Rads
Group I (Sutured)
Number of Leaks/ Number of Dogs (Per Cent)
Group II (Stapled)
Number of Leaks/ Number of Dogs (Per Cent)
Radiographic leaks 3/10 (30) Clinical leaks 0/10 (0)
3/10 (30)
1/lo 0o) 1/lo 00)
2/10 (20)
Photopulos et al. 1~ reported on the satisfactory use of a variety of stapling techniques in patients who had 4000 to 6000 rads preoperatively for gynecologic cancer.
The primary objective of preoperative irradiation therapy has been summarized by Higgins et al. 4 and includes the following goals: (1) to prevent the tumor cells already present in the lymphatics or blood ves- sels, as well as tumor cells implanted in the operative field, from surviving as metastatic implants; (2) to de- stroy any active tumor cells in local lymph nodes in order to convert Dukes' C tumors to more favorable Dukes' B lesions; and (3) to reduce tumor size in order to convert an inoperable lesion to an operable lesion.
The capacity of preoperative irradiation therapy to specifically cut down lymph-node metastases was demonstrated by Kligerman et al .7 when they used a 4500-rad treatment schedule to cut the expected inci- dence of Dukes' C lesions from 43 per cent to 22 per cent in a small group of patients.
This finding was confirmed by Higgins et al. 4 in the Veterans Administration trial of 700 patients under- going treatment with 2000 to 2500 rads preopera- tively in preparation for abdominoperineal resection; that study showed a small improvement in survival among irradiated patients, and this paralleled a de- creased incidence of lymph-node involvments among the irradiated patients.
Actual changes in survival from rectal carcinoma have been difficult to document consistently, particu- larly in low-dose radiation therapy regimens. In an uncontrolled study from Memorial Hospital in 1961, Learning et al. 8 suggested that preoperative irradia- tion therapy on the order of 2000 rads may be of some benefit for patients with Dukes' C rectal car- cinoma as evidence by 14 per cent improvement in survival among these patients. A large follow-up study in the same institution, by Stearns et al . , 14 failed to confirm that finding among 347 randomized pa- tients, although the study allowed for some selectivity of the patients entered and withheld from the study.
FlG. 8. Contrast study showing clin- ical insignificant posterior leak on lat- eral view.
Volume 25 Number 5 HIGH- AND LOW-DOSE IRRADIATION 4 1 5
FIG. 9. Contrast study showing major anastomotic disruption.
T h e capaci ty o f p r e o p e r a t i v e i r r a d i a t i o n t h e r a p y to i n d u c e c o n s i d e r a b l e r e d u c t i o n in t u m o r size to the p o i n t o f ac tua l d i s a p p e a r a n c e o f the p r i m a r y t u m o r at
the t ime o f s u r g e r y was d e m o n s t r a t e d by Al len a n d
F le tche r 1 in 1972. P i lepich et al .n l a te r showed tha t p r e o p e r a t i v e i r r a d i a t i o n t h e r a p y cou ld s h r i n k t u m o r size to the e x t e n t tha t 27 o f 44 prev ious ly u n r e s e c t a b l e
t u m o r s c o u l d be r e s e c t e d for c u r e wi th e x c e l l e n t s h o r t - t e r m survival f igures to date.
T h e resul ts o f o n g o i n g a n d f u t u r e s tudies may be
necessary to resolve the issue, bu t , at this po in t , survi-
val aside, it a p p e a r s tha t p r e o p e r a t i v e i r r a d i a t i o n , pa r t i cu la r ly in the h i g h e r dose r anges , decreases the
i nc idence o f posi t ive l y m p h n o d e s at su rge ry a n d im- p roves the chances for local con t ro l o f t umor s . T h e f i n d i n g tha t this can be a c c o m p l i s h e d w i t h o u t neces-
sari ly sacr i f ic ing the r e c t u m o r c o m p r o m i s i n g the choice of o p e r a t i o n for low- ly ing t u m o r s s h o u l d m a k e the use o f p r e o p e r a t i v e i r r a d i a t i o n t h e r a p y m o r e ap-
pea l i ng in the fu tu r e . At p r e s e n t the p r e f e r e n t i a l use o f the EEA stapler , as well as the possible a d d i t i o n o f a t e m p o r a r y t r ansve r se colos tomy, may be factors that , in pa r t i cu l a r , may be assoc ia ted wi th l e s s e n i n g of
m o r b i d i t y a n d mor ta l i t y a f t e r anas tomos i s in the ir- r a d i a t e d pelvis.
References
1. Allen CV, Fletcher WS. A pilot study on preoperative irradia- tion of rectosigmoid carcinoma. AJR 1972; 114:504-8.
2. Friedmann P, Park WC, Afonya II, et al. Adjuvant radiation therapy in colorectal carcinoma. AM J Surg 1978;135: 512-8.
3. GreenJP. Rectal cancer adjuvant radiation therapy. In: What's new in cancer care. 1979;3:1.
4. Higgins GA Jr, Conn JH, Jordan PH Jr, Humphrey EW, Ros- witz B, Keehn RJ. Preoperative radiotherapy for colorectal cancer. Ann Surg 1975; 181:624-31.
5. Higgins GA Jr. The pros and cons of irradiation treatment of colorectal cancer. Surg Annu 1978; 10:175-90.
6. Jackson BR. Contemporary management of rectal cancer: an overview. Cancer 1977;40:2365-74.
7. Kligerman MM, Urdaneta N, Knowlton A, Vidone R, Hartman PV, Vera R. Preoperative irradiation of rectosig- moid carcinoma including its regional lymph nodes. AJR 1972; 114:498-503.
8. Learning RH, Stearns MW Jr, Deddish MR. Preoperative ir- radiation in rectal carcinoma. Radiology 1961;77:257-63.
9. Motiuddin M, Kramer S. Adjuvant radiotherapy-- preoperative, postoperative, or both: a proposal for a new approach. Cancer Clin Trials 1978 Summer; 1:93-7.
10. Photopulos GJ, Delgado G, Fowler WC Jr, Walton LA. Intesti- nal anastomoses after radiation therapy by surgical stapling instruments. Obstet Gynecol 1979;54:515-8.
11. Pilepich MV, MunzenriderJE, Tak WK, Miller HH. Preopera- tive irradiation of primarily unresectable colorectal car- cinoma. Cancer 1978;42:1077-81.
12. Romsdahl MM, Withers HR. Radiotherapy combined with curative surgery: its use as therapy for carcinoma of the sigmoid colon and rectum. Arch Surg 1978; 113:446-53.
13. Roswit B, Higgins GA Jr, Keehn RJ. Preoperative irradiation for carcinoma of the rectum and rectosigmoid colon: report of a national Veterans Administration randomized study. Cancer 1975:35:1597-1602,
14. Stearns MW Jr, Deddish MR, Quan SH, Learning RH. Preoperative roentgen therapy for cancer of the rectum and rectosigmoid. Surg Gynecol Obstet 1974; 138:584-6.
15. Stevens KRJr, Fletcher WS, Allen CV. Anterior resection and primary anastomosis following high dose preoperative ir- radiation for adenocarcinoma of the recto-sigmoid. Cancer 1978;41:2065-71.
16. Wassif SB. A pilot study for the evaluation of a new regime of combined therapy for the radical treatment of marginally operable rectal (or colo-rectal) cancer. Eur J Cancer 1974;10:615-9.
17. Welch CE, Malt RA. Abdominal surgery (second of three parts). N Engl J ivied 1979;300:705-12.
18. Goligher JC, Lee P~, Macfie J, Simpkins KC, Lintott DJ. Ex- perience with the Russian model 249 suture gun for anas- tomosis of the rectum. Surg Gynecol Obstet 1979; 148:517- 24.
19. Schauer RM, Bubrick MP, Feeney DA, et al. Effects of low- dose preoperative irradiation on low anterior anastomosis in dogs. Dis Colon Rectum (in press).
20. Ellis F. Fractionation in radiotherapy. Mod Trends Radiotherapy 1967; 1:34.
21. Ellis F. The relationship of biologic effect to dose-time fraction- nation factors in radiotherapy. Curr Top Radiat Res 1968;4:357-97.
22. Bubrick MP, Lundeen JW, Hitchcock CR. A comparative ra- diographic study of low anterior colon anastomoses in dogs. Surgery 1981;89:454-9.
23. Goligher JC, Graham NG, DeDombal FT. Anastomotic dehis- cence after anterior resection of rectum and sigmoid. Br J Surg 1970;57:109-18.
24. Crowley LG, Anders C J, Nelsen T, Bagshaw M. Effect of radi- ation o canine intestinal anastomoses. Arch Surg 1968;96:423-8.
25. Symonds CJ. Cancer of rectum: excision after application of radium. Proc R Soc Med 1913;7:152.