Embed Size (px)
Citation preview

http://eeg.sagepub.com/Clinical EEG and Neuroscience
http://eeg.sagepub.com/content/43/2/161The online version of this article can be found at:
DOI: 10.1177/1550059411433612
2012 43: 161 originally published online 16 March 2012Clin EEG NeurosciJudith van Vliet, Wim Mulleners and Jan Meulstee
EEG Leading to the Diagnosis of Limbic Encephalitis
Published by:
http://www.sagepublications.com
On behalf of:
EEG and Clinical Neuroscience Society
can be found at:Clinical EEG and NeuroscienceAdditional services and information for
http://eeg.sagepub.com/cgi/alertsEmail Alerts:
http://eeg.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Mar 16, 2012OnlineFirst Version of Record
- Apr 16, 2012OnlineFirst Version of Record
- Jun 29, 2012Version of Record >>
at TEXAS SOUTHERN UNIVERSITY on November 27, 2014eeg.sagepub.comDownloaded from at TEXAS SOUTHERN UNIVERSITY on November 27, 2014eeg.sagepub.comDownloaded from

EEG Leading to the Diagnosis of LimbicEncephalitis
Judith van Vliet1, Wim Mulleners1, and Jan Meulstee1
AbstractLimbic encephalitis is characterized by subacute onset of short-term memory loss, seizures, sleep disturbances, as well as psychiatricand behavioral symptoms. A subgroup is associatedwith voltage-gated potassium channel antibodies (VGKC-Abs). Inmany cases, brainmagnetic resonance imaging (MRI) demonstrates hyperintense areas in the medial part of the temporal lobe. Also, pleiocytosis is fre-quently found. In this study, we describe a 69-year-old man with VGKC-Abs limbic encephalitis with generalized tonic–clonicseizures, increasing memory deficits, visual hallucinations, depression, and severe insomnia. Brain MRI and cerebrospinal fluid(CSF) were normal, while the electroencephalogram (EEG) showed bilateral frontal and temporal intermittent rhythmic delta activitywith disorganization and slowing of background activity, ultimately leading to the diagnosis of limbic encephalitis. The patient improvedmarkedly after starting immunosuppressive therapy, both clinically andelectrophysiologically. In addition to temporal lobe involvementon the brain MRI and CSF inflammation, we propose EEG abnormalities as an additional diagnostic criterion for limbic encephalitis.
Keywordselectroencephalography, limbic encephalitis, voltage-gated potassium channel, antibodies
Received March 1, 2011; accepted June 17, 2011.
Introduction
Limbic encephalitis is a rare disorder characterized by seizures,
short-term memory loss, as well as psychiatric and behavioral
symptoms such as depression, hallucinations, anxiety, and per-
sonality changes. Sleep disturbances have been reported as well,
both hypersomnia and insomnia. Onset is subacute in a few weeks
to months but may also evolve in a few days. Among others, lim-
bic encephalitis is linked to N-methyl-D-aspartate-receptor anti-
bodies (anti-NMDA-receptors)1 and to VGKC-Abs.2,3 The
latter are also associated with 2 other neurological syndromes,
acquired neuromyotonia, and Morvan syndrome.4 Morvan
syndrome is characterized by autonomic and central nervous
system involvement and neuromyotonia. Symptoms consist of
weight loss, hyperhidrosis, severe insomnia, and hallucinations.
Suggested diagnostic criteria for limbic encephalitis consist of
a typical clinical picture as described above, and at least one of the
following: (1) neuroimaging with evidence of temporal lobe
involvement, (2) CSF inflammation, and (3) detection of limbic
encephalitis–associated antibodies.5 In this study, we describe a
69-year-old man with VGKC-Abs limbic encephalitis, with a nor-
mal MRI and CSF examination, in which the EEG eventually led
to the diagnosis of limbic encephalitis.
Case Report
A 69-year-old man was known to have a renal cell carcinoma
on both sides, in 2002 and 2009, respectively, which resulted
in bilateral nephrectomy and peritoneal dialysis. In May
2010, the patient presented at the emergency room with 2
generalized tonic–clonic seizures. For a few weeks, he had
progressive insomnia, and on the last days he demonstrated
confused and aggressive behavior.
The patient showed severe postictal confusion, resulting in
temporary admission to the intensive care unit for sedation and
intubation. Neurological examination was otherwise normal.
White blood cell count, C-reactive protein, electrolytes, and
glucose were all normal. His creatinine was 958 mmol/L, blood
urea nitrogen (BUN) was 14.3 mmol/L, comparable to previous
values. Contrast-enhanced brain computed tomography (CT)
was uneventful. Analysis of CSF showed normal white blood
cell count (1 � 106) and normal protein level. An EEG,
performed during sedation with propofol to rule out a noncon-
vulsive status epilepticus, demonstrated diffuse slow-wave
activity without epileptic discharges. On the assumption of ure-
mic encephalopathy as the cause of his seizures, he was treated
with phenytoin.
1 Department of Neurology and Clinical Neurophysiology, Canisius Wilhel-
mina Hospital, Nijmegen, The Netherlands
Corresponding Author:
Judith van Vliet, Department of Neurology and Clinical Neurophysiology,
Canisius Wilhelmina Hospital, PO Box 9015, 6500 GS Nijmegen, The
Netherlands
Email: [email protected].
Clinical EEG and Neuroscience43(2) 161-164ª EEG and Clinical NeuroscienceSociety (ECNS) 2012Reprints and permission:sagepub.com/journalsPermissions.navDOI: 10.1177/1550059411433612http://eeg.sagepub.com
at TEXAS SOUTHERN UNIVERSITY on November 27, 2014eeg.sagepub.comDownloaded from

Six weeks later, he was admitted with pneumonia and a third
generalized tonic–clonic seizure. The brain MRI with gadoli-
nium was normal. Over the next few weeks, he visited the
emergency department several times, with symptoms of
depression and increasing memory deficits. He had visual
hallucinations and worsening insomnia and showed aggressive
behavior. All symptoms fluctuated during the day.
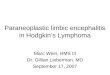
To rule out partial seizures as the cause of his fluctuating
confused behavior, a 24-hour ambulatory EEG was repeated
(Figure 1). No epileptic discharges were seen. However, the
EEG demonstrated marked worsening compared to the previous
recording, showing disorganization of the background, with
bilateral frontal and temporal intermittent rhythmic delta activity
(FIRDA and TIRDA). Remarkably, during 24 hours, sleep was
nearly absent, showing only a few periods of light drowsiness
without any vertex waves, sleep spindles or K complexes.
Taken together the clinical signs and the EEG pattern with
intermittent rhythmic frontotemporal delta activity, suggested
limbic encephalitis. The brain MRI and lumbar puncture were
repeated and again showed no abnormalities. Then, VGKC-
Abs testing was positive, and the diagnosis of limbic encephalitis
was confirmed.
The patient was treated with high doses of prednisolone
(60 mg/d). In a week, there was complete resolution of hal-
lucinations and confusion. Over the next few weeks, his insomnia
improved markedly. A repeated EEG (Figure 2) a few weeks after
starting treatment showed obvious improvement, with recurrence
of background organization. Diffuse slow-wave activity with
FIRDA was still present but far less pronounced compared to the
previous recording. Also, sleep had partially returned with recur-
rence of rapid eye movement (REM) sleep and non-REM light
sleep stages. Immunoglobulins were added as therapy, and the
patient showed further improvement.
Discussion
We report a male patient with a typical clinical picture of lim-
bic encephalitis. Of interest is the fact that EEG eventually led
to this diagnosis, while brain MRI and CSF examination were
normal.
Abnormalities on EEGs are frequently found in limbic
encephalitis, although recordings may be normal as well.6
The EEG may show nonspecific changes with generalized
slowing or uni- or bilateral temporal lobe epileptiform activ-
ity. Focal slow-wave activity in one or both temporal lobes
is another frequently noted feature.7,8 Dalmau et al1
described 92 patients with anti-NMDA-receptor encephali-
tis. All patients showed abnormalities on the EEGs, 23%had epileptic discharges and all other patients showed gen-
eralized or predominantly frontotemporal slow or disorga-
nized activity.
Diagnostic criteria have been formulated for limbic ence-
phalitis.5,9 These consist of typical clinical features (subacute
onset within 12 weeks of seizures, confusion, short-term
memory loss, and psychiatric symptoms), and at least one of
the following: (1) neuroimaging with evidence of temporal
lobe involvement, (2) CSF inflammation, and (3) detection of
limbic encephalitis–associated antibodies. Our patient does
meet these criteria, as VGKC-Abs was positive. However, the
normal findings of brain MRI and CSF examination caused a
delay in definite diagnosis. Therefore, we propose EEG
abnormalities as an additional diagnostic criterion to avoid a
Figure 1. Electroencephalogram (EEG) before treatment, 70 Hz, 0.1 Hz band-pass filter. EEG showing disorganization of the background withdiffuse slowing and intermittent rhythmic delta waves, most pronounced in both temporal areas.
162 Clinical EEG and Neuroscience 43(2)
at TEXAS SOUTHERN UNIVERSITY on November 27, 2014eeg.sagepub.comDownloaded from

delay in treatment. Generalized slowing, temporal lobe epilepti-
form activity, and uni- or bilateral predominantly frontotemporal
slow-wave activity may support the diagnosis. These findings
may be helpful not only in diagnosing limbic encephalitis but
also used to evaluate the effect of treatment during follow-up,
as demonstrated in this case.
A striking symptom in this case was insomnia, demonstrated
by ambulatory EEG recording, which showed hardly any sleep
apart from some short periods of drowsiness. During treatment,
the EEG showed partial improvement with recurrence of REM
sleep and non-REM light sleep stages. However, non-REM
deep sleep stages remained notably absent. Sleep disturbances
have been reported as symptom of limbic encephalitis. Mostly,
hypersomnia is reported,8,10 and severe insomnia is described
as well.11 Two other neurological syndromes are associated
with VGKC-Abs; acquired neuromyotonia, and Morvan
syndrome.4 Morvan syndrome is characterized by
neuromyotonia and involvement of autonomic and central
nervous system, with severe insomnia as an important symp-
tom. In Morvan syndrome, a lack of deep sleep is described,
as well as abnormal REM sleep with lack of atonia. There
seems to be some overlap between the features of limbic ence-
phalitis and Morvan syndrome.
In conclusion, abnormalities on EEG may help diagnose
limbic encephalitis in clinically suspected cases, notably in
patients with normal findings on neuroimaging and CSF anal-
ysis. Generalized slowing, temporal lobe epileptiform activity,
and uni- or bilateral predominantly frontotemporal slow-wave
activity support the diagnosis. Moreover, EEG may be used to
monitor clinical improvement after treatment. We believe that
the EEG as a diagnostic tool deserves greater attention in this
patient population.
It would be interesting to perform a large cohort study to
determine whether certain more specific EEG abnormalities
may point to the diagnosis limbic encephalitis.
Acknowledgment
We thank Ms S. Ruiter and Ms J. ten Cate, EEG technologists, for
recording the EEGs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to
the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship,
and/or publication of this article.
References
1. Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-
receptor encephalitis: case series and analysis of the effects of
antibodies. Lancet Neurol. 2008;7(12):1091–1098.
2. Buckley, Oger J, Clover L, et al. Potassium channel antibodies in
two patients with reversible limbic encephalitis. Ann Neurol.
2001;50(1):73–78.
3. Pozo-Rosich P, Clover L, Saiz A, Vincent A, Graus F. Voltage-gated
potassium channel antibodies in limbic encephalitis. Ann Neurol.
2003;54(4):530–533.
4. Liguori R, Vincent A, Clover L, et al. Morvan’s syndrome:
peripheral and central nervous system involvement with antibodies
Figure 2. Electroencephalogram (EEG) during treatment, 70 Hz, 0.1 Hz band-pass filter. EEG after several weeks of treatment with prednisolon,showing strikingly less delta wave activity compared to the previous one. Instead, background organization has returned, and it demonstrates ahigh index of theta activity.
van Vliet et al. 163
at TEXAS SOUTHERN UNIVERSITY on November 27, 2014eeg.sagepub.comDownloaded from

to voltage-gated potassium channels. Brain. 2001;124(pt 12):
2417–2426.
5. Graus F, Delattre JY, Antoine JC, et al Recommended diagnostic
criteria for paraneoplastic neurological syndromes. J Neurol Neu-
rosurg Psychiatry. 2004;75(8):1135–1140.
6. Vincent A, Buckley C, Schott JM, et al. Potassium channel antibody-
associated encephalopathy: a potentially immunotherapy-responsive
form of limbic encephalitis. Brain. 2004;127(pt 3):701–712.
7. Thieben MJ, Lennon VA, Boeve BF, Aksami AJ, Keegan M,
Vernino S. Potentially reversible autoimmune limbic encephalitis
with neuronal potassium channel antibody. Neurology. 2004;
62(7):1177–1182.
8. Gultekin SH, Rosenfeld MR, Voltz R, Eichen J, Posner JB,
Dalmau J. Paraneoplastic limbic encephalitis: neurological
symptoms, immunological findings and tumour association in
50 patients. Brain. 2000;123(pt 7):1481–1494.
9. Bataller L, Kleopa KA, Wu GF, Rossi JE, Rosenfeld MR, Dalmau
J. Autoimmune limbic encephalitis in 39 patients: immunopheno-
types and outcomes. J Neurol Neurosurg Psychiatry. 2007;78(4):
381–385.
10. Pellkofer HL, Kuempfel T, Jacobson L, Vincent A, Derfuss T.
Non-paraneoplastic limbic encephalitis associated with NMDAR
and VGKC antibodies. J Neurol Neurosurg Psychiatry. 2010;
81(12):1407–1408.
11. Montiel P, Sellal F, Clerc C, Richard P, Bataillard M. Limbic
encephalitis with severe sleep disorder associated with voltage-
gated potassium channels (VGKCs) antibodies. Rev Neurol.
2008;164(2):181–184.
164 Clinical EEG and Neuroscience 43(2)
at TEXAS SOUTHERN UNIVERSITY on November 27, 2014eeg.sagepub.comDownloaded from