Embed Size (px)
Citation preview

REVIEW ARTICLE
Echocardiography and Heart Failure: A Glimpse of theRight Heart
AdamPleister,M.D.,* Rami Kahwash,M.D.,* Garrie Haas,M.D.,* StefanoGhio,M.D.,†Antonio Cittadini,M.D.,‡and Ragavendra R. Baliga,M.D.,M.B.A.*
*Division of Cardiovascular Medicine, The Ohio State University Wexner Medical Center, Columbus, Ohio;†Thoracic and Vascular Department, Fondazione IRCCS Policlinico San Matteo, Pavia, Italy; and‡Department of Translational Medical Sciences, University�a Federico II, Napoli, Italy
The catastrophic consequences for patients in the settings of certain clinical conditions such as acuteright ventricular infarction or massive pulmonary embolism with right heart failure illustrate the essentialrole that the right ventricle plays in sustaining life. With the development of more sophisticated diag-nostic imaging technologies at the end of the last century and the dawn of this century, the importanceof the right ventricle has been clearly demonstrated. The continued and evolving nature of our under-standing of the right ventricle was emphasized in 2006, when the National Heart, Blood, and LungInstitute formed a working group focused on developing a better understanding of the right ventricle inboth healthy and disease states. The objective of this review paper is to examine the right ventriclestructure and function and describe the role of echocardiography in the evaluation of the right ventricleand right heart failure. Special focus will be on echocardiographic images and major society guidelines.(Echocardiography 2014;00:1–13)
Key words: heart failure, echocardiography, right ventricular function, right ventricle
The catastrophic consequences for patients inthe settings of certain clinical conditions such asacute right ventricular (RV) infarction or massivepulmonary embolism with right heart failure illus-trate the essential role that the RV plays in sus-taining life. Historically, however, the RV hasbeen dismissed as a less than useful componentof the circulatory system and evolution appearsto have given the right heart a second-place sta-tus, at least initially: the right heart only appearsin mammals and birds, while the evolution ofmost reptiles, amphibians, fish, and invertebratesdid not require a RV.1 During fetal growth, theRV derives from the neural crest cells that travelto the developing heart, rather than originatingfrom the fundamental mesodermal heart tubethat the left ventricle and atria arise from. Withthe development of more sophisticated diagnos-tic imaging technologies at the end of the lastcentury and the dawn of this century, the impor-tance of the RV has been clearly demonstrated.The continued and evolving nature of our
understanding of the RV was emphasized in2006, when the National Heart, Blood, and LungInstitute formed a working group focused ondeveloping a better understanding of the RV inboth healthy and disease states.2 In addition, themedical literature has developed a significantinterest in this area.1,2 The objective of thisreview paper is to examine the RV structure andfunction and describe the role of echocardiogra-phy in the evaluation of the RV.
RV Structure and Function:Background:The RV functions as a low-pressure, high-volumepump, as opposed to the left ventricle, whichmay be defined as a high-pressure and high-vol-ume pump.3 Experiments in the 1940s and1950s suggested that the RV was an organ ofminor physiologic consequence.4,5 As diagnostictechnologies advanced, an improved under-standing developed in regards to RV function indisease states: determining RV systolic and dia-stolic function is important in the managementof many cardiac conditions, including acute de-compensated heart failure, chronic heart failurein the setting ventricular dyssynchrony requiringbiventricular pacing, chronic heart failure requir-ing ventricular assist devices (VAD), pulmonary
Address for correspondence and reprint requests: Adam Pleis-ter M.D., Division of Cardiovascular Medicine - Department ofInternal Medicine, The Ohio State University Wexner MedicalCenter, 473 West 12th Avenue, Suite 200 DHLRI, Columbus,Ohio, 43210-1267. Fax: (614) 293-5614;E-mail: [email protected]
1
© 2014, Wiley Periodicals, Inc.DOI: 10.1111/echo.12678 Echocardiography

hypertension, dysrhythmias requiring permanentpacemakers, cardiac transplantation, and con-genital heart disease (especially in the growingadult population with surgical correction in child-hood).
Anatomy of the RV:The anatomy of the RV is distinctly different fromthat of the left ventricle, although they are func-tionally interdependent.3 While the shape of theleft ventricle may be described as ellipsoid andconcentric, the RV may be described as bow- orcrescent-shaped. In addition, the overall musclemass of the RV is only about one-sixth of the leftventricle. However, during the course of one car-diac cycle, the RV usually contains a somewhatgreater volume of blood compared to the leftventricle. Also, the RV appears to have anincreased distensibility compared to the left ven-tricle. Nonetheless, these two anatomically differ-ent chambers are connected by a complexnetwork of muscle fibers resulting in functionalinterdependence.
In general, there are two regions of the RVused anatomic description and imaging report-ing (in addition to the interventricular septum):the body of the RV (or sinus) and the RV outflowtract (also described as the conus or infundibu-lum). During the embryonic development of thevertebrae heart, the RV outflow tract arises fromthe bulbus cordis (a chamber distal to and sepa-rate from the common ventricle).6 While itappears that the RV body and outflow tract havethe same wall thickness, the outflow tract has afunctional superiority given its lack of arching orcurvature in comparison to the body.
Function of the RV:The RV functions and pumps in synchrony withthe left ventricle, with the RV attached to thehigh-compliance pulmonary vasculature and theleft ventricle connected to the less compliant sys-temic circulation. The entire heart is envelopedwithin the pericardium, which itself does not sig-nificantly change in size due to acute changes involume or pressure in any of the four cardiacchambers. This is due to the structural matrix ofthe pericardium, comprised of collagen and elas-tin fibers. Therefore, in this relatively “closed” sys-tem, acute clinical alterations in volume orpressure in either ventricle can affect the otherventricle. This concept was initially proposed byBernheim in 1910,7 who suggested that hyper-trophy and dilation of the left ventricle couldcompress the RV and result in RV dysfunction.Further studies in the 1900s on a feline model ofheart failure provided evidence for Bernheim’shypothesis.8 Furthermore, observation of humanpatients with heart failure demonstrated that
initial RV dysfunction (such as volume and pres-sure overload in the setting of atrial septaldefects) led to a subsequent left ventriculardysfunction, due to the ventricular septum beingforced leftward.9 Even in the absence of the peri-cardium, it appears that the functional co-depen-dence of the two ventricles persists. Inexperiments with an isolated beating heart in theabsence of a pericardium, two groups demon-strated that load of one ventricle shifted the dia-stolic pressure-volume relation of the otherventricle, and that a shift of the interventricularseptum to the left via RV loading decreased leftventricular chamber dimensions.10,11 Clearly,however, the presence of an intact pericardiumwill affect the co-dependent function of the ven-tricles, which has been demonstrated in isolatedheart preparations in the presence and, by wayof comparison, absence of a pericardium.12
Right Heart Dysfunction and VentricularInterdependence:In the clinical setting, certain disease states haveclearly demonstrated the functional interdepen-dence of the two ventricles. In particular, this hasbeen documented in RV myocardial infarction,cardiac transplantation and subsequent acute RVfailure, left ventricle mechanical assist deviceimplantation, and acute pulmonary embolus.3 Allof these severe deteriorations of cardiac functionresult in low cardiac output and require criticalcare unit management. The etiology in eacharises from distention of the RV in the setting of astiff pericardium and resulting decreased left ven-tricle preload.
In the setting of pulmonary embolism, pul-monary artery and RV volumes are increased,with subsequent decreases in systemic bloodpressure and cardiac output. With a large, acutepulmonary embolism, this hemodynamic com-promise can lead to death.13 Experimental mod-els of produced pulmonary embolus in caninesyielded significant decreases in dimensions ofthe left ventricle (from the interventricular sep-tum to the left ventricular free wall).14 Thus, withincreased RV pressure in the setting of pulmo-nary embolus, functional ventricular interdepen-dence results in underfilling of the left ventricle.In the setting of acute RV myocardial infarction,elevated right-sided heart pressures result. Onestudy showed that opening the pericardiumhelped to increase cardiac output by approxi-mately one-third as well as to increase the leftventricle size.15 This again demonstrates howthe pericardium resists acute changes in ventric-ular hemodynamics; in particular, increased RVafterload can result in a shift of the interventricu-lar septum to the left with resultant decreasedcardiac output.
2
Pleister, et al.

Some question exists as to which anatomicstructure and its functional consequences playthe more dominant role in the functional interde-pendence of the ventricles: the interventricularseptum or the restraining effect of the pericar-dium.3 A human study showed that an increasein the systemic peripheral resistance results inincreased afterload of both the right and leftventricles and increased RV volumes, which sug-gested that pericardial restraint, rather interven-tricular septum shift, may play a more dominantrole in ventricular interdependence.16
Cellular and Biochemical Implications:The right and left ventricles also differ in theirbiochemistry and cellular biology properties. Inthe porcine heart, the mitochondrial density ofthe RV is decreased compared to that of the leftventricle.17 In addition, the mitochondrial tomyofibril ratio of the left ventricle and the inter-ventricular septum are similar to each other andboth much greater than in the RV. This ratio is amarker for myocardial oxygen consumption andworkload, indicating comparatively decreasedvalues in the RV. The decreased oxygen demandof RV myocardial tissue results in a protectiveeffect from ischemia and resultant necrosis dueto right coronary artery occlusion. This protectiveeffect can be explained by increased oxygenextraction during stress and a greater systolic todiastolic coronary blood flow ratio as comparedto the left ventricle, resulting in increased oxygendelivery during ischemic events.3 A porcinemodel of right coronary artery occlusion revealeddecreased RV necrosis in the absence of previousleft-to-right collateral vessel development.18 Inthe same animal model, previous RV damageand hypertrophy caused by pulmonary arterybanding did not spare the RV from necrosis; inthis model both normal and hypertrophic RV hada similar degrees of left-to-right collateral coro-nary vessels.
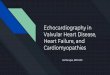
Right Ventricular Ejection Fraction:The RV’s inherent protection from ischemia likelyplays a role in its importance in predicting mor-tality and morbidity in heart failure. In thosepatients with advanced systolic heart failure, aright ventricular ejection fraction (RVEF) less than40% suggests a greater likelihood of hospitaliza-tion and death, while a value below 20% qualifiesas an independent predictor of increased risk ofhospitalization and death.19
A normal, healthy RVEF (greater than 40%)requires a synchronized physiologic interactionbetween the two defined anatomic regions of theRV, the body and outflow tract, and also the in-terventricular septum. The outflow tract contracts
about 30–50 msec after the body of the RV.20
Studies have shown that increased sympathetictone can eliminate this contraction delay, whileincreased vagal tone can lengthen the delay.21
Experimental models in canines suggest that nor-mal RV ejection relies on active shortening of thefree wall surface area in the early phase and septalto free wall distance in the late phase.3 Duringthe late phase, the blood located in the outflowtract flows into the pulmonary artery due toblood momentum.22 Furthermore, the interven-tricular septum likely plays a significant role in thelate phase of RV contraction, as demonstrated incanine studies which showed that RV free wallshortening stops before the free wall to septaldimension reaches maximal excursion.3,23
Impact of the Left Ventricle:A significant contributor to RV ejection is the leftventricle. This was demonstrated in experimentsin canines which demonstrated that significantdamages to the RV free wall resulted a minimaldecrease in RV function.4 Implied from this find-ing is that left ventricular contraction directlyimpacts RV systolic function.4,24 Additional stud-ies in humans with ventricular dyssynchrony fromleft or right bundle branch block demonstratedventricular interdependence via transmission ofleft ventricle developed pressure to the RV.25 Inaddition, a laprine animal model demonstratedthat increased left ventricular volume resulted inincreased RV pressure.11 Further studies in thelaprine model showed that coronary artery liga-tion with resultant left ventricle free wall ischemiayielded a rapid decrease in RV pressures.11 Asnoted previously, these animal models were notconsidered physiologic due to the absence of anintact pericardium and loss of diastolic function.3
In the clinical setting, the importance of left ven-tricle contractile function to RV systolic functionhas been observed for several decades, and wasdemonstrated in a small series of patients withpostcardiac surgery heart failure requiring vaso-pressor and intra-aortic balloon pump and thensubsequent mechanical VAD placement.26 Preop-erative assessment of ventricular function did notpredict which patients would require VAD place-ment; however, those patients with perioperativemyocardial infarction predicted those patientswho would eventually require VAD placement.Eighty-seven percent of the patients developedbiventricular failure, and of these patients, thosethat received a biventricular VAD had a betterchance of being weaned from intensive care unitsupport and eventually surviving than thosepatients who received a left-side only VAD. Ofnote, those patients with left-sided only ventricu-lar failure did well with left-side only VAD.
3
Echocardiography in RV Heart Failure

Echocardiographic Imaging of the RightHeart:Background:The widespread use of echocardiography in diag-nostic medicine continues to develop with tech-nological improvements and the advancement ofclinical knowledge. An echocardiogram is oftenthe first test of choice in patients who presentwith dyspnea. The analysis of the RV has posed adefinite challenge, although the aforementionedincreased appreciation of RV dysfunction on mor-bidity and mortality has created an increasedneed for improved diagnostic methods for evalu-ating the RV. The development of two-dimen-sional echocardiography (2DE) allowed forimproved evaluation of RV size and function.Standardized approaches to RV evaluation havemade it easier for routine evaluation and compar-ison of RV function over time.27 Given its avail-ability, portability, relatively low cost (comparedto other imaging modalities), and lack of risk orradiation exposure, transthoracic echocardio-gram remains the test of choice for initial evalua-tion of suspected right heart dysfunction.
Other Imaging Modalities:A brief review of other imaging modalities will aidto understand the advantages (and disadvan-tages) of echocardiography in the evaluation ofthe right heart. Chest x-ray is often used as aninitial step for patients with suspected right heartdisease as it is widely available and relatively inex-pensive. The RV is best viewed in the lateral view,with RV enlargement noted when the cardiac sil-houette involves more than 40% of the lower ret-rosternal space. Enlargement of the RV can causethe heart to rotate in a posterior direction andalso can push the RV outflow tract in a lateraldirection. Of course, a routine chest x-ray canalso visualize other disease processes, includingacute infection processes, pulmonary edema,intrinsic pulmonary disease, enlargement of theright atria, and left ventricular enlargement. Ifany cardiac abnormality is noted on a routinechest x-ray, the next diagnostic step is most oftenthe echocardiogram.
Nuclear imaging plays a role in the evaluationof RV function, particularly in the assessment ofRV volumes and function and also myocardialcharacterization. First-pass radionuclide ventricu-lography, with bolus injection of technetium-99mwith RV counts of at least 40%, allows for oneimaging plane and is the test of choice for nuclearevaluation of RV evaluation. Also, gated equilib-rium blood pool imaging can be used. Due to theadvantages of other imaging modalities relativeto these techniques, nuclear scans are not rou-tinely used for the evaluation of RV function and
volume. Positron emission tomography has beenapplied to characterize RV myocardial metabolismwith fluorodeoxyglucose-18F (FDG) in patientswith known left heart dysfunction.28 A negativecorrelation exists between RVEF and the RV-to-leftventricle FDG ratio.28,29 This imaging is bestobtained in the setting of RV hypertrophy and inparticular with pulmonary hypertension, and canallow for evaluation of RV ischemia.30
Cardiac catheterization with cine angiogramsof the RV can obtain several views of the RV,although no more than two are usually per-formed and recorded due to a desire to limitiodinated contrast dye. With these projections,RV volume and function can be quantitated usingSimpson’s rule31 or other approaches.28 Theadvantage of invasive diagnostic right heart cath-eterization is that other valuable testing can bedone at that time, including recording of a vari-ety of right heart and pulmonary hemodynamicmeasurements and also pulmonary angiography,if indicated. Given other imaging techniquesavailable and the risk of an invasive procedurewith significant dye load, RV angiography is notoften used in routine evaluation of the RV sizeand function.
Computed tomography (CT scans) are widelyused for the evaluation of pulmonary embolus,and nongated CT scans have been used in thesetting of acute pulmonary embolus to examinethe RV as a predictor of thirty-day mortality.32
Other quantified measures, including three-dimensional (3D) imaging and interventricularseptal displacement, have been developed asmortality predictors in this clinical setting.28 Heli-cal scans of the heart with electrocardiographicgating has been shown to provide accurate RVfunction and volume quantification.33 However,the need for radiation and contrast (compared toother modalities which require neither) has lim-ited the use of CT scanning in this setting; mostoften CT is used in patients with suspected rightheart dysfunction or congenital heart diseasewith a permanent device (such as mechanicalVAD or permanent pacemaker).28
Cardiac magnetic resonance imaging (CMR)has recently developed as a valuable tool in theevaluation of the RV. CMR is currently consideredthe “gold standard” in the assessment of RV vol-umes and ejection fraction.34 The ability toobtain unlimited, highly reproducible images inhigh resolution without radiation exposure, with-out contrast administration requirement (in thesetting of function assessment only), and withoutthe acoustic limitations of ultrasound has made itone of the diagnostic tests of choice in the evalu-ation of patients with suspected right heart dys-function.28 CMR is more expensive, less broadly
4
Pleister, et al.

available, and more time-consuming comparedto echocardiography, however, and patients withmedical devices (see CT section above) areunable to undergo scanning due to the magneticfield. CMR is often applied to the evaluation ofpatients with pulmonary hypertension due to theability to quantify RV hypertrophy, enlargement,and systolic function.28 In adult patients withcomplex congenital heart disease with involve-ment of the RV (such as tetralogy of Fallot ortransposition of the great arteries), CMR is thetest of choice as other imaging modalities aremore limited in this setting.35 CMR is also wellsuited for the evaluation of suspected arrhythmo-genic cardiomyopathy, given its ability to evalu-ate RV dysfunction and enlargement and todetect (with use of a contrast agent) fatty depos-its and/or fibrosis in the myocardium.36
Echocardiographic Methods in RV Evalution:Despite the various advantages of the otherimaging modalities detailed above, ultrasound ofthe heart is still the most common diagnosticmodality used in the evaluation of patients withsuspected or known right heart dysfunction, witha significant amount of information availablefrom standard echocardiographic techniques, asdetailed in Table I.28 Current clinical guidelinesendorse the use of echocardiography in this set-ting.37 Advantages of echocardiography includelow comparative cost, widespread availability,portability (currently handheld echocardiogramsare being developed for widespread application),
and safety (no radiation exposure and newercontrast agents, although not required for anexam, appear nontoxic and well tolerated). Asechocardiography has been used for decades, asignificant amount of clinical trial data and evi-dence-based medicine in the management ofheart failure and heart disease in general arefounded on echocardiography data. Also, the useof Doppler allows for the evaluation of certainhemodynamic parameters. Limitations existspecifically in the setting of echocardiographicevaluation of the RV: the complex shape of thechamber does not allow for the use of geometricmodels for volume and function quantification,the retrosternal position of the RV creates a bar-rier for ultrasound waves, and the high-volume,low-pressure system of the RV with its thinnerwalls and prominent trabeculations (in compari-son to the left ventricle) confound dataanalysis.28
TABLE I
Echocardiographic Techniques to Assess the Right Ventricle(RV)
M-modeRV wall thicknessRV outflow tract shorteningTricuspid annular plane systolic excursion (TAPSE)
(Fig. 1)2D echo (Fig. 2)Linear dimensionsVisual assessment of RV volumes/ejection fractionVentricular eccentricity indexFractional area change
Conventional DopplerRV systolic pressures (Fig. 3)Myocardial performance indexDoppler tissue imagingMyocardial performance indexIsovolumic acceleration (IVA)Strain and strain rate
Speckle trackingStrain and strain rate
3D echo (Figs. 4 and 5)RV volumesRV ejection fraction
A
B
Figure 1. A. Normal TAPSE: M-mode and apical four-cham-ber view measurement of systolic tricuspid annular planeexcursion which represents the systolic right ventricular (RV)function (normal >1.6 cm). B. Abnormal TAPSE: M-mode andapical four-chamber view measurement of systolic tricuspidannular plane excursion which represents the systolic RV func-tion (abnormal <1.6 cm).
5
Echocardiography in RV Heart Failure

RV Volume and Morphology:RV size and morphology are assessed via echocar-diography via 2D imaging.38 RV pressure over-load can be evaluated with standardized imageacquisition and may reveal RV hypertrophy, dila-
tation, and abnormal interventricular septummotion.28 Hypertrophy is characterized by anend-diastolic free wall thickness of greater than5 mm and correlates with increased afterload.39
With chronic elevated pressure, the RV will dilate
A C
B
E
F
D
Figure 2. A. Normal right ventricular dimensions. B. Abnormal right ventricular dimensions. C. Right ventricular (RV) dimensionsin a patient with pulmonary embolism. D. RV pressure overload causing flattening of septum or “D-sign.” E. RV pressure overloadcausing flattening of septum or “D-sign” in left panel (right panel normal and middle panel suggest slightly increased pressure). F.“D-sign” with enlarged RV cavity seen.
6
Pleister, et al.

and function will become impaired. Given thecurved shape and complicated structure of theRV, volumes are difficult to evaluate in an objec-tive manner, and the 2D approaches used rou-tinely and accurately in left ventricle that employSimpson’s formula are often imprecise. Measure-ments of transverse and longitudinal lengths areused instead, along with subjective comparisonof relative size of the RV versus the left ventricle[Table II].28 Common practice dictates that a RVdiastolic area that visually appears to be equal toor greater than that of the left ventricle (in a stan-dard four-chamber image) indicates RV enlarge-ment (Fig. 2).40
An important marker of RV pressure overloadis flattening of the interventricular septum(Fig. 2D,E) with motion of the septum towardthe left ventricle during end-systole. In addition,volume overload of the RV can also cause flatten-ing of the septum (Fig. 2F) and movementtoward the left ventricle, in this case during end-diastole.28 As noted previously, this septal motioncauses under filling of the left ventricle anddecreased stroke volume, and can cause criticalillness in certain settings. The ratio of the left ven-tricle anteroposterior to septal-lateral short-axiscavity dimension at end-systole or end-diastole istermed the left ventricle eccentricity index, andvalues above one indicate RV overload.28,40 Fur-thermore, the relation of septal curvature to leftventricle free wall curvature as well as the degreeof septal curvature can be employed to estimateRV systolic pressures and trans-septal pressuregradients.28,41
RV Function:Several techniques are used to measure RV sys-tolic function with several emerging techniquesin continued development, as detailed inTable I.41 Routine practice involves the use ofvisual estimation of function from multiple imag-
ing planes. Other more objective techniques willbe discussed below.
RV fractional area change is the percentchange in ventricle chamber area in the apicalfour-chamber view throughout the course of thecardiac cycle; it correlates well with CMR dataFigure 3. Enlarged right atrium on 3D echocardiography.
A
B
C
Figure 4. A. Doppler of tricuspid regurgitant jet estimatingpeak right ventricular systolic pressure as high as ~51 mmHg.B. Doppler of tricuspid regurgitant jet estimating peak rightventricular systolic pressure at ~39 mmHg. C. Doppler of tri-cuspid regurgitant jet estimating peak right ventricular systolicpressure at ~31 mmHg
7
Echocardiography in RV Heart Failure

and can predict death, heart failure, and strokeafter myocardial infarction.41–43
RV index of myocardial performance (RIMP) isa calculation used to evaluate RV systolic and dia-stolic function; it is defined as a ratio of total RVisovolumic time divided by RV ejection time.44
The RIMP value can be correlated with RVEFusing nuclear ventriculography and appears tobe less affected by heart rate and loading condi-tions.28,44,45 RIMP values greater than 0.55 bytissue Doppler and 0.40 by pulsed-wave Dopplersignify ventricular dysfunction.40
Tricuspid annular plane systolic excursion(TAPSE) uses M-mode apical four-chamber viewsto evaluate longitudinal RV function, with avalue less than 1.6 cm suggestive of RV dysfunc-tion. It is predictive of mortality in advancedsystolic heart failure46 and pulmonary hyperten-sion.28,40,47 Correlation with other standardizedimaging modalities is under continued investiga-tion, although initial studies suggested closecorrelation with radionuclide angiography.42,48
Drawbacks of TAPSE are that only one-dimen-sional (1D) images representing the basal RV areused,28 however, it is currently recommendedfor routine use in the evaluation of RVfunction.40
Pulsed Doppler tissue imaging (DTI) objec-tively measures peak velocities with a tricuspidlateral annular systolic velocity value below9.7 cm/sec indicating abnormal contractility andpossible early RV dysfunction,28,34,49 with this
A
B
Figure 5. A. Speckle tracking of RV. B. Speckle tracking ofRV. RV = Right ventricle.
TABLE II
Normal Adult Right Ventricular (RV) Echocardiographic Dimensions (See Fig. 2)
DimensionRV Length
(Base-to-Apex) Basal RV Mid RV RV Outflow Tract Pulmonary Artery
Normal range, cm 7.1–7.9 2.0–2.8 2.7–3.3 2.5–2.9 1.5–2.1
TABLE III
Measures of Right Ventricular (RV) Function
Method RVEF on 2D
FractionalArea Change
(FAC)TAPSE(Fig. 1) RIMP
IsovolumicAcceleration
(IVA)S0 (Pulsed)(Fig. 6)
RVEF on 3D(Fig. 4)
Abnormal <44% <35% <1.6 cm Pulsed>0.44Tissue>0.55
Not defined <10 cm/sec <44%
Limitations Unreliable Endocardialborderneeds to beaccuratelytraced
Load andangledependent
Not reliable inelevated RApressures orirregular heartrates likeatrial fib
Load and angledependent;varies with ageand heart rate
Angle dependent,assumes allsegments havesimilar function;limited datain elderly
Not readilyavailable
RVEF, right ventricular ejection fraction.
8
Pleister, et al.
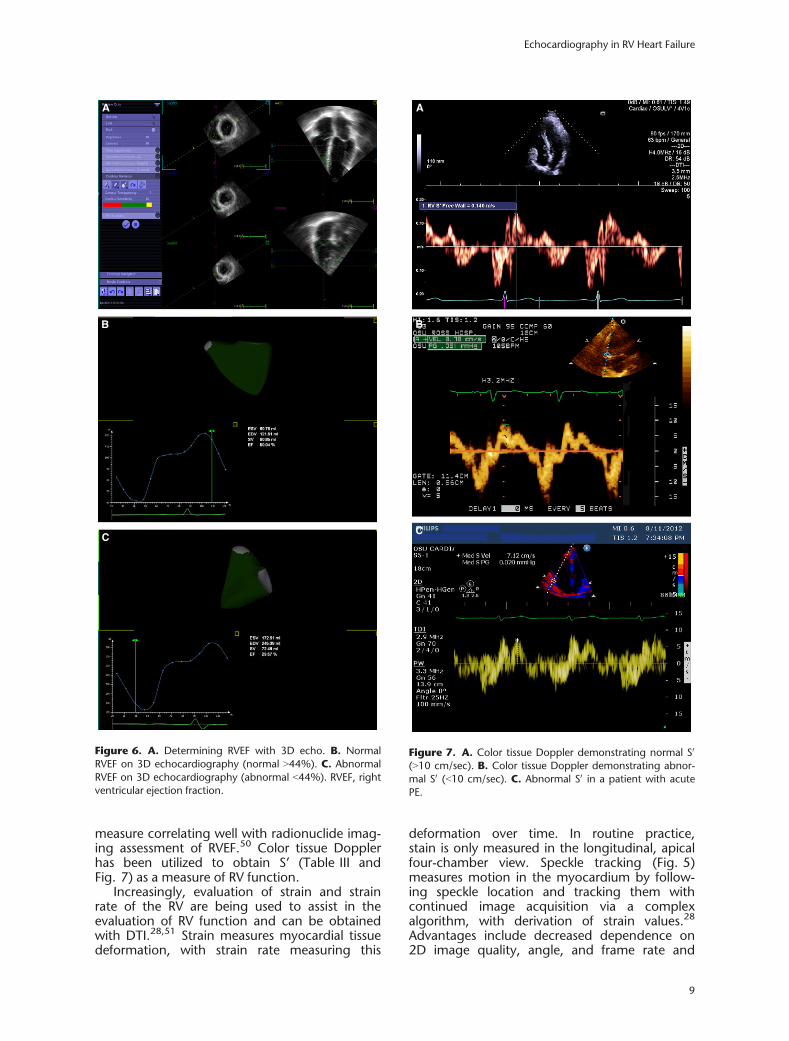
measure correlating well with radionuclide imag-ing assessment of RVEF.50 Color tissue Dopplerhas been utilized to obtain S’ (Table III andFig. 7) as a measure of RV function.
Increasingly, evaluation of strain and strainrate of the RV are being used to assist in theevaluation of RV function and can be obtainedwith DTI.28,51 Strain measures myocardial tissuedeformation, with strain rate measuring this
deformation over time. In routine practice,stain is only measured in the longitudinal, apicalfour-chamber view. Speckle tracking (Fig. 5)measures motion in the myocardium by follow-ing speckle location and tracking them withcontinued image acquisition via a complexalgorithm, with derivation of strain values.28
Advantages include decreased dependence on2D image quality, angle, and frame rate and
A
B
C
Figure 6. A. Determining RVEF with 3D echo. B. NormalRVEF on 3D echocardiography (normal >44%). C. AbnormalRVEF on 3D echocardiography (abnormal <44%). RVEF, rightventricular ejection fraction.
A
B
C
Figure 7. A. Color tissue Doppler demonstrating normal S0
(>10 cm/sec). B. Color tissue Doppler demonstrating abnor-mal S0 (<10 cm/sec). C. Abnormal S0 in a patient with acutePE.
9
Echocardiography in RV Heart Failure

measurement of RV strain in both the short andlong axis. Clinical studies confirm correlationwith both global and regional RV function.28,52
The measurement of RV diastolic dysfunctionis under continued development. Pulsed waveDoppler measurement of tricuspid inflow andmyocardial DTI provides one method of diastolicanalysis and yields objective data for E/A,E/E0, and E0/A0 ratios. Also, measurement of theisovolumic relaxation time can provide informa-tion regarding RV diastolic dysfunction.28,43,53
Advanced Echocardiographic Analysis of theRV:Evaluation of RV hemodynamics can be obtainedvia several methods, including objective analysisof RV systolic pressures via application of themodified Bernoulli equation to the tricuspid re-gurgitant jet. Other modalities include Dopplerimaging of the RV outflow tract and estimationof right atrial pressure via measurement of infe-rior vena cava diameter and inferior vena cavachange with respiratory variation (Table IV andFig. 8).28,40,54
The development of 3D echocardiographyhas occurred as a result of improved technologyin the setting of advanced transducers, improvedimage analysis, and high-level software develop-ment. Using full-volume image acquisition, theentire RV may be visualized (Fig. 6) and does notrequire geometric assumptions to measure car-diac chambers, which is often a problem with tra-ditional methods and the complex structure ofthe RV.28 Real time 3D techniques have beenshown to accurately provide objective measure-ment of RV volumes.55
Practical Assessment of the RV:Heart Failure:The first step is to evaluate pulmonary arterypressure (PAP): several studies have establishedthe prognostic value of pulmonary hypertensionin cohorts of ambulatory patients with heart fail-ure.56 The cutoffs used were quite different andsomewhat arbitrary as there is no definition ofpulmonary hypertension based on the systolicpulmonary pressure estimated at echocardiogra-phy. Guidelines in fact recommend that pulmo-nary hypertension is diagnosed on the basis ofmean PAP at right heart catheterization. Pulmo-nary regurgitation velocity can be used to assesspulmonary artery diastolic pressure; however,caution is required as it is usually difficult to cor-rectly align the ultrasound beam with the pulmo-nary regurgitant jet to obtain accurate values.Mathematical formulae have been publishedwhich allow for the calculation of pulmonary vas-cular resistance; however, this measurement isnecessary only when patients have to bescreened for heart transplant and in this situationa precise hemodynamic determination must beobtained.
TABLE IV
Inferior Vena Cava Diameter to Assess Volume Status
Inferior vena cava (IVC) normally collapses more than 50%with inspiration or sniffing: Collapse <50% suggests volumeoverload
Correlation between RA pressure (CVP) and IVC appearance:1 CVP 0–5 cm: IVC totally collapses on inspiration and is
<1.5 cm in diameter
2 CVP 5–10 cm: IVC collapses >50% on inspiration and is1.5–2.5 cm in diameter
3 CVP 11–15 cm: IVC collapses <50% on inspiration andis 1.5–2.5 cm in diameter
4 CVP 16–20 cm: IVC collapses <50% on inspiration andis >2.5 cm in diameter
5 CVP >20 cm: No change in IVC on inspiration and is>2.5 cm in diameter
A
B
Figure 8. A. Normal inferior vena cava diameter. B. Dilatedinferior vena cava.
10
Pleister, et al.

The simplest echocardiographic indicator ofRV function, i.e. the TAPSE has proved to be arobust prognostic indicator in heart failure; aTAPSE ≤14 mm is associated with a high risk ofdeath or hospitalization or urgent heart trans-plantation during follow-up.46 Importantly, riskstratification in heart failure may be greatlyenhanced if TAPSE and systolic PAP are consid-ered together.57
To summarize, pulmonary artery systolic pres-sure and TAPSE represent the minimum datasetin heart failure patients.
Pulmonary Hypertension:In patients with pulmonary hypertension, survivaland progression of the disease are stronglydependent on the ability of the RV to adapt tothe chronically elevated PAP. Although severalechocardiographic variables have been associ-ated with outcome, in recent years the simpleTAPSE has drawn the attention of research-ers.47,58,59 Importantly, TAPSE is only the firststep of a pathophysiological approach to the RVfunction with echocardiography. Patients withnormal or relatively preserved TAPSE can be fur-ther stratified according to the degree of tricus-pid regurgitation, since TAPSE might beoverestimated in the presence of significant tri-cuspid regurgitation. Patients having a reducedTAPSE can be further stratified according to theleft ventricular eccentricity index in diastole, sincethis is a good indicator of RV diastolic pres-sures.47
Finally, the visual inspection of the shapeof the Doppler flow velocity envelope of theRV outflow tract may provide useful insightinto the hemodynamic basis of pulmonaryhypertension: the presence of mid-systolicnotching is associated with the most severepulmonary vascular disease and right heartdysfunction.60
In summary, TAPSE, the degree of tricuspidregurgitation, the end-systolic left ventriculareccentricity index, and the envelope of the RVoutflow tract at pulsed Doppler represent theminimum dataset in pulmonary hypertensionpatients.
Guidelines from Major Societies:The American College of Cardiology and Ameri-can Heart Association 2013 Guideline for theManagement of Heart Failure recommends 2Dechocardiogram with Doppler for the initial eval-uation of heart failure.61 In addition, they recom-mend repeat measurements of ejection fractionin patients with heart failure who have had a sig-nificant change in clinical status or received treat-ment that might affect cardiac function or for
consideration of device therapy. Both of these areI Class of Recommendations with C Level of Evi-dence. Specifically, they state that RV size andfunction should be measured and that all valves,including the tricuspid and pulmonic valves,should be evaluated for anatomic and flowabnormalities. In addition, secondary changes (inparticular the severity of tricuspid valve insuffi-ciency) should be determined. The tricuspid valveregurgitant gradient, measurement of inferiorvena cava diameter, and the inferior vena cavadiameter response during respiration providesestimates of PAP and central venous pressure,and therefore give insight to right heart functionduring heart failure.
The Heart Failure Association of the Euro-pean Society of Cardiology 2012 guidelines forthe diagnosis and treatment of acute andchronic heart failure recommend transthoracicechocardiogram, along with electrocardiogram,as the two most useful tests in patients withsuspected heart failure.62 The data obtainedfrom the echocardiogram provide measure-ments of chamber volumes, wall thickness,valve function, and systolic and diastolic func-tion, which are crucial in deciding appropriatetherapies. Specifically, the echocardiogram canprovide data in regards to RV function and PAP,in addition to left ventricular function. IsolatedRV failure may occur in the setting of acute cor-onary syndrome or after massive pulmonaryembolism and treatment approaches contrastthose of treatment for left ventricular dysfunc-tion. Specifically, vasodilators and diureticsshould be avoided or used cautiously, as theymay cause reduction in RV filling, in the settingof isolated right heart failure. Furthermore, pro-gressive isolated RV failure may occur in patientswith pulmonary hypertension, and specificagents are indicated in pulmonary hypertensionthat are not part of the standard therapy for leftventricular dysfunction. Medications which helpto decrease pulmonary arterial resistanceinclude type V phosphodiesterase inhibitors,endothelin antagonists, and prostacyclin ana-logues.
Conclusions:Accurate determination of RV function is impor-tant in the management and prognosticationof heart failure. Echocardiography has emerged asimportant modality in assessment of RV functionand the suspicion that RV function is impairedshould be considered when there is reduced(TAPSE <16 mm), increased tricuspid regurgita-tion peak velocity (when>3.4 m/sec), increasedsystolic PAP (increased when >50 mmHg), ordilated inferior vena cava (>2.5 cm).
11
Echocardiography in RV Heart Failure

References1. Crawford MH: The right ventricle. Foreword. Cardiol Clin.
2012;30:ix.2. Goldstein JA, Rich JD: Faces of right ventricular failure.
Cardiol Clin. 2012;30:xi.3. Dell’Italia LJ: Anatomy and physiology of the right ventri-
cle. Cardiol Clin. 2012;30:167–187.4. Donald DE, Essex HE: Pressure studies after inactivation of
the major portion of the canine right ventricle. Am J Phys-iol 1954;176:155–161.
5. Starr IJW, Meade R: The absence of conspicuous incre-ments of venous pressure after severe damage to theright ventricle of the dog, with a discussion of the rela-tion between clinical congestive failure and heart disease.Am Heart J 1943;26:291–301.
6. Keith A: Fate of the bulbus cordis in the human heart.Lancet 1924;204:1267–1273.
7. Bernheim D: De l’asystolie veineuse dans l’hyper trophiedu coeur gauche par stenose concomitante du ventriculedroit. Rev Med 1910;39:785.
8. Henderson Y, Prince A: The relative systolic discharges ofthe right and left ventricles and their bearing on pulmo-nary congestion and depletion. Heart 1914;5:217–226.
9. Dexter L: Atrial septal defect. Br Heart J 1956;18:209–225.
10. Bemis CE, Serur JR, Borkenhagen D, et al: Influence ofright ventricular filling pressure on left ventricular pres-sure and dimension. Circ Res 1974;34:498–504.
11. Santamore WP, Lynch PR, Heckman JL, et al: Left ventric-ular effects on right ventricular developed pressure. J ApplPhysiol 1976;41:925–930.
12. Maruyama Y, Ashikawa K, Isoyama S, et al: Mechanicalinteractions between four heart chambers with andwithout the pericardium in canine hearts. Circ Res1982;50:86–100.
13. Jardin F, Gurdjian F, Desfonds P, et al: Hemodynamicfactors influencing arterial hypoxemia in massive pulmo-nary embolism with circulatory failure. Circulation1979;59:909–912.
14. Belenkie I, Dani R, Smith ER, et al: Ventricular interactionduring experimental acute pulmonary embolism. Circula-tion 1988;78:761–768.
15. Belenkie I, Sas R, Mitchell J, et al: Opening the pericar-dium during pulmonary artery constriction improves car-diac function. J Appl Physiol 2004;96:917–922.
16. Dell’Italia LJ, Walsh RA: Right ventricular diastolic pres-sure-volume relations and regional dimensions duringacute alterations in loading conditions. Circulation1988;77:1276–1282.
17. Singh S, White FC, Bloor CM: Myocardial morphometriccharacteristics in swine. Circ Res 1981;49:434–441.
18. Peter RH, Ramo BW, Ratliff N, et al: Collateral vesseldevelopment after right ventricular infarction in the pig.Am J Cardiol 1972;29:56–60.
19. Meyer P, Filippatos GS, Ahmed MI, et al: Effects of rightventricular ejection fraction on outcomes in chronic sys-tolic heart failure. Circulation 2010;121:252–258.
20. Meier GD, Bove AA, Santamore WP, et al: Contractilefunction in canine right ventricle. Am J Physiol 1980;239:H794–H804.
21. Pace JB, Keefe WF, Armour JA, et al: Influence of sympa-thetic nerve stimulation on right ventricular outflow-tractpressures in anesthetized dogs. Circ Res 1969;24:397–407.
22. Spencer MP, Greiss FC: Dynamics of ventricular ejection.Circ Res 1962;10:274–279.
23. Raizada V, Sahn DJ, Covell JW: Factors influencing lateright ventricular ejection. Cardiovasc Res 1988;22:244–248.
24. Santamore WP, Dell’Italia LJ: Ventricular interdepen-dence: Significant left ventricular contributions to right
ventricular systolic function. Prog Cardiovasc Dis1998;40:289–308.
25. Feneley MP, Gavaghan TP, Baron DW, et al: Contributionof left ventricular contraction to the generation of rightventricular systolic pressure in the human heart. Circula-tion 1985;71:473–480.
26. Pennington DG, Merjavy JP, Swartz MT, et al: The impor-tance of biventricular failure in patients with postopera-tive cardiogenic shock. Ann Thorac Surg 1985;39:16–26.
27. Ling LF, Marwick TH: Echocardiographic assessment ofright ventricular function: How to account for tricuspidregurgitation and pulmonary hypertension. JACC Cardio-vas Imaging 2012;5:747–753.
28. Sanz J, Conroy J, Narula J: Imaging of the right ventricle.Cardiol Clin 2012;30:189–203.
29. Mielniczuk LM, Birnie D, Ziadi MC, et al: Relationbetween right ventricular function and increased rightventricular [18f]fluorodeoxyglucose accumulation inpatients with heart failure. Cir Cardiovas Imaging2011;4:59–66.
30. Gomez A, Bialostozky D, Zajarias A, et al: Right ventricu-lar ischemia in patients with primary pulmonary hyper-tension. J Am Coll Cardiol 2001;38:1137–1142.
31. Gentzler RD II, Briselli MF, Gault JH: Angiographic estima-tion of right ventricular volume in man. Circulation1974;50:324–330.
32. Schoepf UJ, Kucher N, Kipfmueller F, et al: Right ventricu-lar enlargement on chest computed tomography: A pre-dictor of early death in acute pulmonary embolism.Circulation 2004;110:3276–3280.
33. Plumhans C, Muhlenbruch G, Rapaee A, et al: Assess-ment of global right ventricular function on 64-mdctcompared with mri. AJR Am J Roentgenol 2008;190:1358–1361.
34. Champion HC, Michelakis ED, Hassoun PM: Comprehen-sive invasive and noninvasive approach to the rightventricle-pulmonary circulation unit: State of the art andclinical and research implications. Circulation2009;120:992–1007.
35. Frank L, Dillman JR, Parish V, et al: Cardiovascular MRimaging of conotruncal anomalies. Radiographics2010;30:1069–1094.
36. Jain A, Tandri H, Calkins H, et al: Role of cardiovascularmagnetic resonance imaging in arrhythmogenic rightventricular dysplasia. J Cardiovasc Magn Reson2008;10:32.
37. Douglas PS, Khandheria B, Stainback RF, et al: ACCF/ASE/ACEP/ASNC/SCAI/SCCT/SCMR 2007 appropriate-ness criteria for transthoracic and transesophageal echo-cardiography: A report of the american college ofcardiology foundation quality strategic directions com-mittee appropriateness criteria working group, americansociety of echocardiography, american college of emer-gency physicians, american society of nuclear cardiology,society for cardiovascular angiography and interventions,society of cardiovascular computed tomography, andthe society for cardiovascular magnetic resonanceendorsed by the american college of chest physiciansand the society of critical care medicine. J Am Coll Cardiol2007;50:187–204.
38. Lang RM, Bierig M, Devereux RB, et al: Recommenda-tions for chamber quantification: A report from the amer-ican society of echocardiography’s guidelines andstandards committee and the chamber quantificationwriting group, developed in conjunction with the euro-pean association of echocardiography, a branch of theeuropean society of cardiology. J Am Soc Echocardiogr2005;18:1440–1463.
39. Matsukubo H, Matsuura T, Endo N, et al: Echocardio-graphic measurement of right ventricular wall thickness.A new application of subxiphoid echocardiography. Cir-culation 1977;56:278–284.
12
Pleister, et al.

40. Rudski LG, Lai WW, Afilalo J, et al: Guidelines for theechocardiographic assessment of the right heart inadults: A report from the american society of echocardi-ography endorsed by the european association of echo-cardiography, a registered branch of the europeansociety of cardiology, and the canadian society ofechocardiography. J Am Soc Echocardiogr 2010;23:685–713; quiz 786–688.
41. King ME, Braun H, Goldblatt A, et al: Interventricular sep-tal configuration as a predictor of right ventricularsystolic hypertension in children: A cross-sectional echo-cardiographic study. Circulation 1983;68:68–75.
42. Anavekar NS, Gerson D, Skali H, et al: Two-dimensionalassessment of right ventricular function: An echocardio-graphic-mri correlative study. Echocardiography2007;24:452–456.
43. Anavekar NS, Skali H, Bourgoun M, et al: Usefulness ofright ventricular fractional area change to predict death,heart failure, and stroke following myocardial infarction(from the valiant echo study). Am J Cardiol2008;101:607–612.
44. Tei C, Dujardin KS, Hodge DO, et al: Doppler echocar-diographic index for assessment of global right ventricu-lar function. J Am Soc Echocardiogr 1996;9:838–847.
45. Karnati PK, El-Hajjar M, Torosoff M, et al: Myocardial per-formance index correlates with right ventricular ejectionfraction measured by nuclear ventriculography. Echocar-diography 2008;25:381–385.
46. Ghio S, Recusani F, Klersy C, et al: Prognostic usefulnessof the tricuspid annular plane systolic excursion inpatients with congestive heart failure secondary to idio-pathic or ischemic dilated cardiomyopathy. Am J Cardiol2000;85:837–842.
47. Ghio S, Klersy C, Magrini G, et al: Prognostic relevance ofthe echocardiographic assessment of right ventricularfunction in patients with idiopathic pulmonary arterialhypertension. Int J Cardiol 2010;140:272–278.
48. Ueti OM, Camargo EE, Ueti Ade A, et al: Assessment ofright ventricular function with doppler echocardio-graphic indices derived from tricuspid annular motion:Comparison with radionuclide angiography. Heart2002;88:244–248.
49. Lindqvist P, Waldenstrom A, Henein M, et al: Regionaland global right ventricular function in healthy individu-als aged 20-90 years: A pulsed doppler tissue imagingstudy: Umea general population heart study. Echocardiog-raphy 2005;22:305–314.
50. Meluzin J, Spinarova L, Bakala J, et al: Pulsed dopplertissue imaging of the velocity of tricuspid annular systolicmotion; a new, rapid, and non-invasive method of
evaluating right ventricular systolic function. Eur Heart J2001;22:340–348.
51. La Gerche A, Jurcut R, Voigt JU: Right ventricular functionby strain echocardiography. Curr Opin Cardiol2010;25:430–436.
52. Teske AJ, De Boeck BW, Olimulder M, et al: Echocardio-graphic assessment of regional right ventricular function:A head-to-head comparison between 2-dimensional andtissue doppler-derived strain analysis. J Am Soc Echocardi-ogr 2008;21:275–283.
53. Mertens LL, Friedberg MK: Imaging the right ventricle–current state of the art. Nat Rev Cardiol 2010;7:551–563.
54. Pellicori P, Carubelli V, Zhang J, et al: Ivc diameter inpatients with chronic heart failure: Relationships andprognostic significance. JACC Cardiovas Imaging2013;6:16–28.
55. Lu X, Nadvoretskiy V, Bu L, et al: Accuracy and reproduc-ibility of real-time three-dimensional echocardiographyfor assessment of right ventricular volumes and ejectionfraction in children. J Am Soc Echocardiogr 2008;21:84–89.
56. Damy T, Goode KM, Kallvikbacka-Bennett A, et al: Deter-minants and prognostic value of pulmonary arterial pres-sure in patients with chronic heart failure. Eur Heart J2010;31:2280–2290.
57. Ghio S, Temporelli PL, Klersy C, et al: Prognostic rele-vance of a non-invasive evaluation of right ventricularfunction and pulmonary artery pressure in patientswith chronic heart failure. Eur J Heart Fail 2013;15:408–414.
58. Forfia PR, Fisher MR, Mathai SC, et al: Tricuspid annulardisplacement predicts survival in pulmonary hyperten-sion. Am J Respir Crit Care Med 2006;174:1034–1041.
59. Mathai SC, Sibley CT, Forfia PR, et al: Tricuspid annularplane systolic excursion is a robust outcome measure insystemic sclerosis-associated pulmonary arterial hyper-tension. J Rheumatol 2011;38:2410–2418.
60. Arkles JS, Opotowsky AR, Ojeda J, et al: Shape of the rightventricular doppler envelope predicts hemodynamicsand right heart function in pulmonary hypertension. Am JRespir Crit Care Med 2011;183:268–276.
61. Yancy CW, Jessup M, Bozkurt B, et al: 2013 ACCF/AHAguideline for the management of heart failure: a report ofthe American College of Cardiology Foundation/Ameri-can Heart Association Task Force on Practice Guidelines.J Am Coll Cardiol 2013;62:e147–e239.
62. McMurray JJV, Adamopoulos S, Anker SD, et al: ESCguidelines for the diagnosis and treatment of acute andchronic heart failure 2012. Eur Heart J 2012;33:1781–1847.
13
Echocardiography in RV Heart Failure