Embed Size (px)
Citation preview
Echocardiographically Guided Electrophysiologic Testing in Pregnancy
MichaelS. Lee, MD, Steven J. L. Evans, MD, Steven Blumberg, MD, Monty M. Bodenheimer, MD, and Scott L. Roth, MD, New Hyde Park, New York
Electrophysiologic testing is usually performed with fluoroscopy to guide catheter positioning. This method of visualizing catheter placement may not be ideal for patients who are pregnant. We report four cases of echocardiographically guided placement of catheters for electrophysiologic testing because of the consideration of pregnancy. Adequate visualization of catheters was possible, allowing for proper catheter positioning and complete electrophysiologic testing, including the recording of atrial, His-bundle, and ventricular potentials, as well as cardiac stimulation and induction of tachycardia. This method holds promise for patients in whom fluoroscopy may be relatively contraindicated, such as pregnant patients, as well as patients in whom it is desirable to avoid x-ray exposure such as women of childbearing age and young children. (JAM Soc EcHOCARDIOGR 1994;7:182-6.)
Although catheter positioning during electrophysiologic testing is generally performed with x-ray fluoroscopy to guide catheter position, two-dimensional echocardiography is an alternative method of guiding catheter placement. Echocardiographically guided catheter placement obviates the need for irradiation and may be of utility for patients in whom radiation exposure is undesirable, such as women of childbearing age and especially women who are pregnant.
METHODS
A standard two-dimensional echocardiogram was obtained before electrophysiologic testing and evaluated for adequacy of visualization of the heart chambers on the right side. The inferior vena cava, right atrium, high right atrium, tricuspid valve, tricuspid annulus, and right ventricle (RV) (including apex) were well visualized in all patients. After informed consent was obtained, the patients were brought to the electrophysiology laboratory in the fasting state. In the first patient a right antecubital cutdown was
From the Division· of Adult Cardiology, the Harris Chasanoff Heart Institute, Long Island Jewish Medical Center.
Reprint requests: Steven J. Evans, MD, Division of Adult Cardiology, the Harris ChasanoffHeart Institute, Long Island Jewish Medical Center, New Hyde Park, NY 11042.
Copyright© 1994 by the American Society ofEchocardiography. 0894-7317/94$3.00 + 0 27/1/51212
182
Table 1 Echocardiographic views obtained
Echocardiographic view
Subcostal
Parasternal short-axis Parasternal R V inflow Modified parasternal R V
inflow Apical four-chamber
Structures visualized
IVC, IVC-RA juncture, SVC-RA juncture
High RA, TV, RV outflow tract TA, TV and annulus, RV RVapex
RA, TV, RV apex
IVC, Inferior vena cava; R V, right atrium; SVC, superior vena cava; TV, tricuspid valve.
performed. In the following three patients the right groin was prepared and anesthetized with 2% lidocaine, and two venous sheaths were inserted. After obtaining venous access, two steerable 6F, four-polar electrophysiologic catheters were advanced under echocardiographic guidance through the inferior vena cava (three patients) or the superior vena cava (one patient). If the catheter met with resistance during advancement, it was withdrawn slightly, re-angled under echocardiographic guidance, and re-advanced.
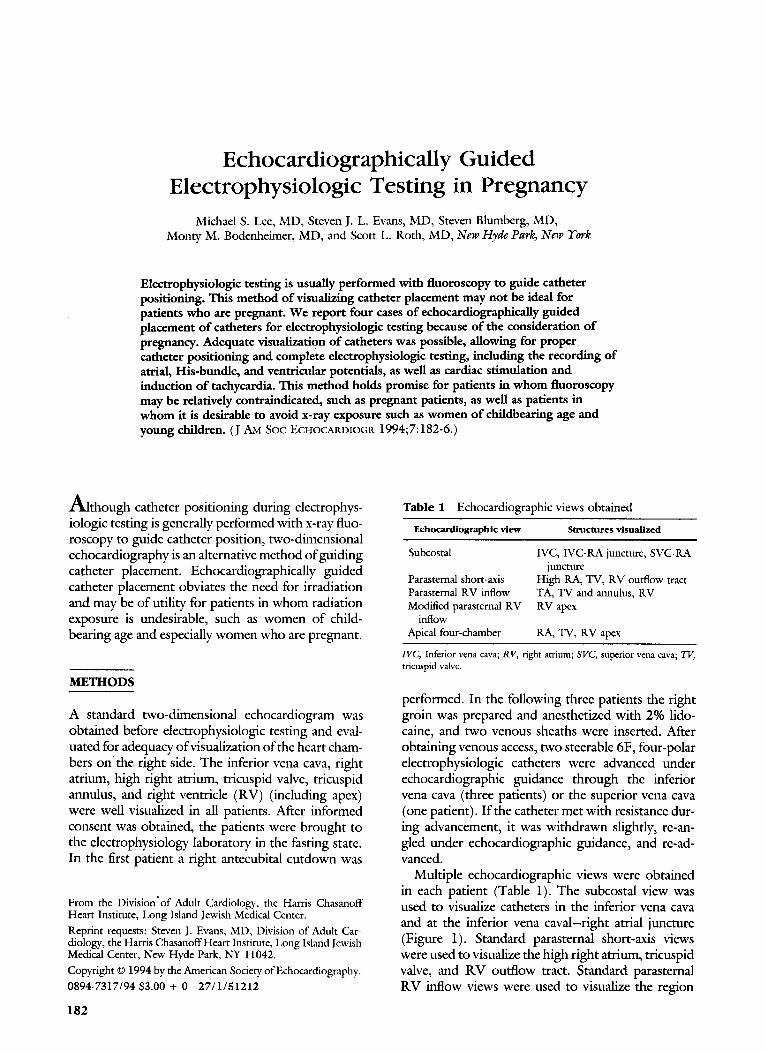
Multiple echocardiographic views were obtained in each patient (Table 1). The subcostal view was used to visualize catheters in the inferior vena cava and at the inferior vena caval-right atrial juncture (Figure 1). Standard parasternal short-axis views were used to visualize the high right atrium, tricuspid valve, and R V outflow tract. Standard parasternal R V inflow views were used to visualize the region
Journal of the American Society of Echocardiography Volume 7 Number 2 Lee et al. 183
Figure 1 Standard subcostal view. Catheter (arrows) was advanced from inferior vena cava (IV C) into right atrium (RA).
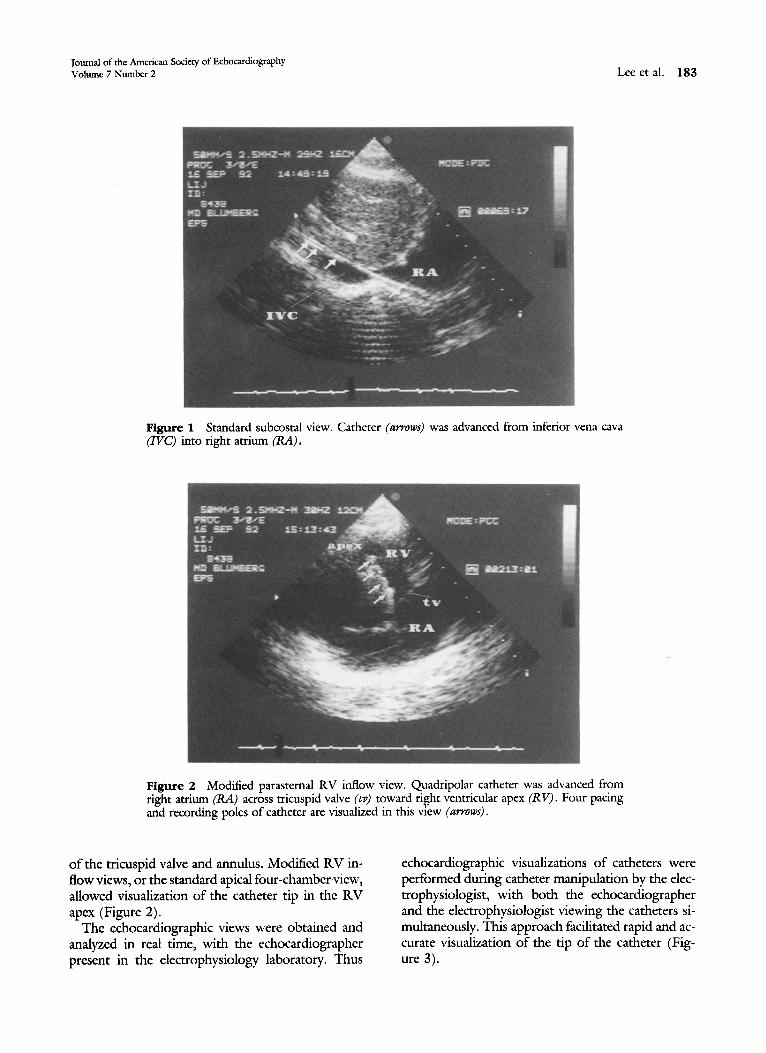
Figure 2 Modified parasternal R V inflow view. Quadripolar catheter was advanced from right atrium (RA) across tricuspid valve (tv) toward right ventricular apex (R V). Four pacing and recording poles of catheter are visualized in this view (arrows) .
of the tricuspid valve and annulus. Modified R V inflow views, or the standard apical four-chamberview, allowed visualization of the catheter tip in the R V apex (Figure 2).
The echocardiographic views were obtained and analyzed in real time, with the echocardiographer present in the electrophysiology laboratory. Thus
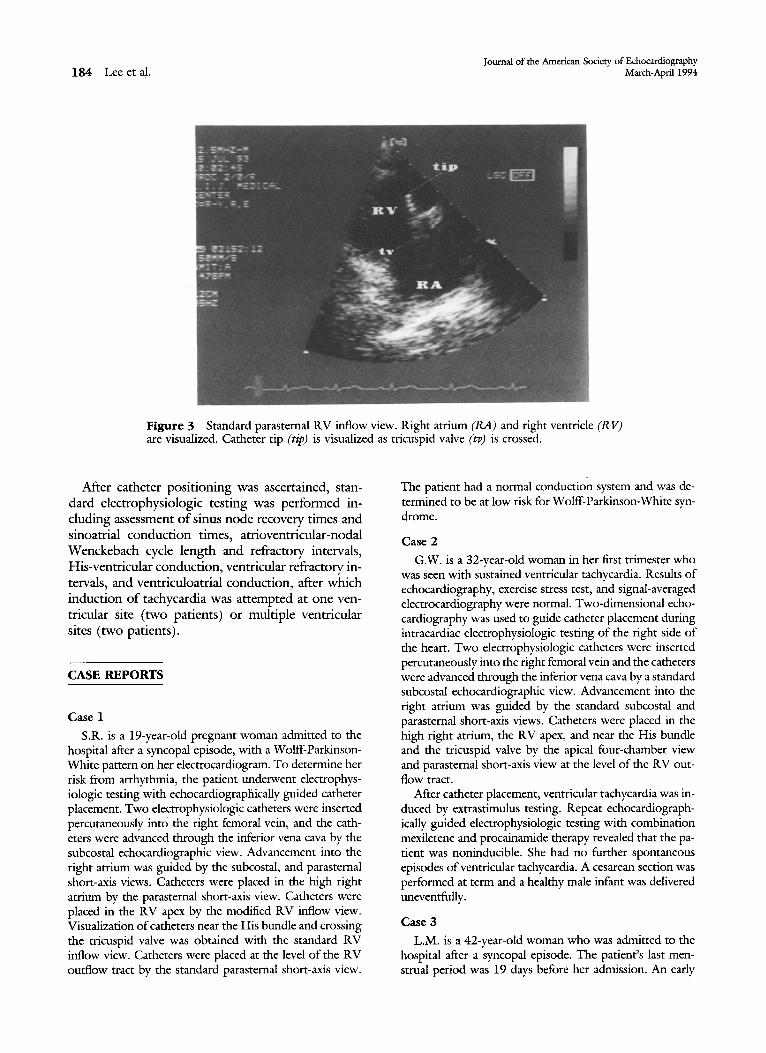
echocardiographic visualizations of catheters were performed during catheter manipulation by the electrophysiologist, with both the echocardiographer and the electrophysiologist viewing the catheters simultaneously. This approach facilitated rapid and accurate visualization of the tip of the catheter (Figure 3).
184 Lee eta!. Journal of the American Society of Echocardiography
March-Aprill994
Figure 3 Standard parasternal RV inflow view. Right atrium (RA) and right ventricle (R V) are visualized. Catheter tip (tip) is visualized as tricuspid valve (tv) is crossed.
Mter catheter positioning was ascertained, standard electrophysiologic testing was performed including assessment of sinus node recovery times and sinoatrial conduction times, atrioventricular-nodal W enckebach cycle length and refractory intervals, His-ventricular conduction, ventricular refractory intervals, and ventriculoatrial conduction, after which induction of tachycardia was attempted at one ventricular site (two patients) or multiple ventricular sites (two patients).
CASE REPORTS
Case l
S.R. is a 19-year-old pregnant woman admitted to the hospital after a syncopal episode, with a Wolff-ParkinsonWhite pattern on her electrocardiogram. To determine her risk from arrhythmia, the patient underwent electrophysiologic testing with echocardiographically guided catheter placement. Two electrophysiologic catheters were inserted percutaneously into the right femoral vein, and the catheters were advanced through the inferior vena cava by the subcostal echocardiographic view. Advancement into the right atrium was guided by the subcostal, and parasternal short-axis views. Catheters were placed in the high right atrium by the parasternal short-axis view. Catheters were placed in the RV apex by the modified RV inflow view. Visualization of catheters near the His bundle and crossing the tricuspid valve was obtained with the standard R V inflow view. Catheters were placed at the level of the R V outflow tract by the standard parasternal short-axis view.
The patient had a normal conduction system and was determined to be at low risk for Wolff-Parkinson-White syndrome.
Case 2
G.W. is a 32-year-old woman in her first trimester who was seen with sustained ventricular tachycardia. Results of echocardiography, exercise stress test, and signal-averaged electrocardiography were normal. Two-dimensional echocardiography was used to guide catheter placement during intracardiac electrophysiologic testing of the right side of the heart. Two electrophysiologic catheters were inserted percutaneously into the right femoral vein and the catheters were advanced through the inferior vena cava by a standard subcostal echocardiographic view. Advancement into the right atrium was guided by the standard subcostal and parasternal short-axis views. Catheters were placed in the high right atrium, the R V apex, and near the His bundle and the tricuspid valve by the apical four-chamber view and parasternal short-axis view at the level of the R V outflow tract.
After catheter placement, ventricular tachycardia was induced by extrastimulus testing. Repeat echocardiographically guided electrophysiologic testing with combination mexiletene and procainamide therapy revealed that the patient was noninducible. She had no further spontaneous episodes of ventricular tachycardia. A cesarean section was performed at term and a healthy male infant was delivered uneventfully.
Case 3
L.M. is a 42-year-old woman who was admitted to the hospital after a syncopal episode. The patient's last menstrual period was 19 days before her admission. An early

Journal of the American Society of Echocardiography Volume 7 Number 2
pregnancy could not be ruled out because of the window period in which the standard pregnancy test may be falsely negative. 1 The patient underwent electrophysiologic testing by echocardiographically guided catheter placement, through an antecubital vein cutdown. The parasternal and apical views afforded adequate visualization of the catheters. The patient had a normal conduction system study and no inducible arrhythmias. The patient was discharged from the hospital with a cardiac event recorder, which revealed transient, spontaneous complete heart block requiring permanent pacemaker implantation. The pacemaker was implanted with standard fluoroscopic imaging because it had been determined at that time that the patient was not pregnant.
Case4
T.M. is a 21-year-old woman admitted to the hospital after a presyncopal episode in the first trimester of pregnancy. She had previously had several syncopal episodes. Echocardiography, signal-averaged electrocardiography, and stress testing were normal, and blood test results for Lyme disease and sarcoidosis were negative. The patient underwent electrophysiologic testing by echocardiographically guided catheter placement. Subcostal views afforded visualization of the catheters in the inferior vena cava and right atrium. Modified parasternal views assisted catheter placement across the tricuspid valve into the R V apex and outflow tract. The patient was found to have a normal conduction system study and no arrhythmias were inducible.
DISCUSSION
Although two-dimensional echocardiography has been used previously to guide electrophysiologic testing, there are no reports of echocardiographically guided electrophysiologic testing used specifically for consideration of pregnancy. 2 Permanent pacemaker implantation in a pregnant woman has been reported with the guidance of the electrocardiogram and twodimensional echocardiography. 3 Transesophageal echocardiography has also been used to guide catheter placement during radiofrequency catheter ablation and to guide insertion of a physiologic pacemaker in early pregnancy. 4•
5 These studies revealed the utility of echocardiography in visualizing catheters.
There are several advantages of using echocardiography to guide catheter placement. Echocardiography enables visualization of the position of the catheters in relation to the heart structures on the right side. Other benefits of echocardiographically guided electrophysiologic study include the ability to assess complications associated with catheter placement such as pericardia! effusion caused by perfo-
Lee et al. 185
ration of the R V free wall and perforation of the ventricular septum. Echocardiography was judged to be better than fluoroscopy in guiding catheters in one study because of its ability to detect complications as they arose. 2
At our institution, echocardiographically guided electrophysiologic ~esting has been performed successfully in all pregnant patients in whom the procedure was attempted (four attempts and four successes, to date). One potential problem that may be encountered is advancement of the catheter from the iliac vein or antecubital vein into the vena cavae. Although echocardiography was used to guide the catheters once they entered the great veins, the advancement from the site of insertion to the inferior vena cava (three patients) and superior vena cava (one patient) was performed blindly. It is likely that catheter advancement was facilitated by three factors. First, the patients were young, healthy women and likely had less venous tortuosity in the smaller veins. Second, the plasma volume of pregnant women is expanded, again decreasing the likelihood of becoming obstructed by venous tortuosity. Third, the use of a flexible, deflectable-tip catheter allows for easy passage even in the setting of venous tortuosity, because the tip of the catheter loops over and usually follows the largest open pathway up 'toward the vena cavae. With this technique, the catheters were advanced easily in all patients, without the need for a luminal catheter with a guide wire.
Previous authors have suggested that echocardiography is of limited utility for guiding catheter placement because of inability to visualize the catheter tip. With our approach, the catheter tip is visualized easily during electrophysiologic testing. Two factors may make this possible. First, the echocardiographic views are analyzed in real time. Thus the echocardiographer is communicating information about catheter location to the electrophysiologist as catheter manipulation is being performed. Second, the presence of four metal poles at the end of the catheter makes the tip more echogenic than the body of the catheter. Thus although in the past there has been uncertainty as to whether echocardiography actually demonstrates the tip of the catheter, in these four patients, when the echocardiographic image revealed tip contact with the tissue, excellent electrograms and pacing thresholds were obtained. This suggests that, at least with a 2 mm metal tip electrode, echocardiography may be used to identify the tip and judge tip-tissue contact.
Use of real-time echocardiographic image analysis and emphasis on the echogenic segment of the catheter allow rapid and accurate determination of cath-

186 Lee et al.
eter tip position. Thus once advanced into the right side of the heart, catheters are easily positioned at all of the standard electrophysiologic positions.
In view of the ease and safety of echocardiographically guided catheter placement, it is preferable to
fluoroscopy during electrophysiologic testing in ptegnant women. The use of echocardiography for catheter placement should also be <:onsidered in children and women of childbearing age, because adequate protection from radiation mlly not always be achieved during fluoroscopy.
REFERENCES
l. Flood JT, Hodgen GD. The physrology of fertilization, implantation, and early human development. In: Scott JR, DiSaia PJ, Hammond CB, Spellacy WN, eds. Danforth's obstetrics
J oumal of the American Society of Echocardiography March-April 1994
and gynecology. 6th ed. Philadelphia: JB Lippincott, 1990: 86-7.
2. Drinkovic N. Subcostal echocardiography to determine right ventricular pacing catheter position and control advancement of electrode catheters in intracardiac electrophysiologic studies. Am J Cardiol1981;47:1260-5.
3. Gudal M, Kervancioglu C, Oral D, et al. Permanent pacemaker implantation in a pregnant woman with the guidance of ECG and tWo-dimensional echocardiography. Pacing Clin Electrophysioll987;10:543-5.
4. Goldman AP, Irwin JM, Glbver MU, Mick W. Transesophageal echocardiography to improve positioning of radiofrequency ablation catheters in left-sided Wolff-Parkinson-White syndrome. PACE Pacing Clin Electrophysiol 1991;14:1245-50.
5. Jordaens LJ, Vandenbogaerde JF, Van deBruaene P, De Buyzere M. Transesophageal echocardiography for insertion of a physiological pacemaker in early pregnancy. Pacing Clin Electrophysiol 1990;13:955-7.





























