Embed Size (px)
Citation preview

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.October 1, 2015 • Volume 5 • Number 7 cases-anesthesia-analgesia.org 107
Copyright © 2015 International Anesthesia Research SocietyDOI: 10.1213/XAA.0000000000000188
Pain is common after major abdominal surgeries. Uncontrolled postoperative pain increases the inci-dence of postoperative complications.1,2 Multimodal
analgesia can improve pain control in the postoperative period and reduces complications that may arise from using a single mode of analgesia. For example, reliance on opioid analgesia increases the incidence of adverse effects of opi-oids including pruritus, nausea, and vomiting, as well as respiratory depression.3
The true incidence of respiratory depression varies in different studies. Non-obstetric studies report an incidence of respiratory depression with neuraxial opioids in 0.01% to 7% of patients.4 The incidence of respiratory depression after systemic opioid administered by IV patient-controlled analgesia (PCA) was reported to be 1.2%, 1.26%, and 1.97% in 3 different studies.5–7
Effective regional anesthesia techniques for abdominal surgery include epidural analgesia, paravertebral block, and transversus abdominis plane (TAP) block.8 Multiple approaches have been used for TAP blocks including the commonly used ultrasound-guided midaxillary approach. TAP block provides analgesia mainly in T10-L2 dermatomes.9 TAP blocks are sometimes patchy with variable wound cov-erage.10 The use of an ultrasound-guided approach at the level of the quadratus lumborum muscle is new and may provide wider spread of local anesthetic (T5-L1) than TAP blocks, and hence better analgesia.11 The patient gave verbal permission for the authors to publish the report.
CASE DESCRIPTIONA 50-year-old man, weighing 95 kg, with a medical his-tory of anxiety, prostate cancer, prostatectomy, and rectal
cancer was admitted to the hospital for anterior procto-sigmoidectomy and low colorectal anastomosis through a midline longitudinal incision. Epidural analgesia was sug-gested; however, the surgical team preferred to use IV PCA for postoperative pain to avoid possible hemodynamic side effects of the epidural. After uneventful surgery, the patient received IV hydromorphone in the postanesthesia care unit for pain management. Hydromorphone PCA was initiated and set at 0 mg basal, 0.3 mg bolus with a 6-minute lockout interval, total 3 mg/h. After achieving an accept-able level of pain control, the patient was transferred to the floor. Per institutional protocol, the patient received 2 L/min nasal oxygen. Nurse monitoring included respi-ratory rate and sedation score every 1 hour for the first 2 hours after initiation of hydromorphone PCA, then every 4 hours. In addition, he was monitored with continuous pulse oximetry.
On the first postoperative day, the patient complained of increased abdominal pain and required supplemen-tal hydromorphone (total additional 1.2 mg in 3 divided doses). Although still receiving nasal oxygen, the patient developed respiratory failure requiring intervention by the Acute Medical Emergency team. He was unrespon-sive, apneic, with oxygen saturation in the 50s. He had strong palpable pulses and adequate arterial blood pres-sure. His airway was secured by nasal airway insertion and bag-mask ventilation, which promptly increased his oxygen saturation to the 90s. A 12-lead electrocardiogram did not show any acute ST/T wave changes. Naloxone IV was given in 2 doses of 0.4 mg each. The patient awoke and followed commands. He was able to maintain adequate respiratory effort and 99% oxygen saturation with a 100% nonrebreathing mask.
With reversal of opioid analgesia, the patient com-plained of excruciating abdominal pain, which was managed by IV acetaminophen and IV ketorolac. The IV hydromorphone PCA was discontinued. The pain man-agement team was consulted. The surgical team still pre-ferred to avoid a thoracic epidural if possible. Therefore, we considered bilateral continuous quadratus lumborum blocks.
We present a case of acute postoperative abdominal pain after proctosigmoidectomy and colorectal anastomosis that was treated by bilateral continuous quadratus lumborum block. The block was performed in the lateral position under ultrasound guidance with a 15-mL bolus of 0.5% bupivacaine injected anterior to the quadratus lumborum muscle followed by bilateral cath-eter placement. Each catheter received a continuous infusion of 0.1% bupivacaine at 8 mL/h and an on-demand bolus 5 mL every 30 minutes. Sensory level was confirmed by insensitivity to cold from T7 through T12. The block was devoid of hemodynamic side effects or motor weak-ness. This case demonstrates that bilateral continuous quadratus lumborum catheters can provide extended postoperative pain control. (A&A Case Reports. 2015;5:107–11.)
From the Departments of *General Anesthesia, †Pain Management, and ‡Outcomes Research, Cleveland Clinic, Cleveland, Ohio.
Accepted for publication March 10, 2015.
Funding: None.
The authors declare no conflicts of interest.
Address correspondence to Mohamed Shaaban, MD, Departments of General Anesthesia and Pain Management, Cleveland Clinic, 9500 Euclid Ave., E-31, Cleveland, OH 44195. Address e-mail to [email protected].
Bilateral Continuous Quadratus Lumborum Block for Acute Postoperative Abdominal Pain as a Rescue After Opioid-Induced Respiratory DepressionMohamed Shaaban, MD,*† Wael Ali Sakr Esa, MD, PhD,*† Kamal Maheshwari, MD,*†‡ Hesham Elsharkawy, MD, MSc,*† and Loran Mounir Soliman, MD*†
CLINICAL CAREE
Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.108 cases-anesthesia-analgesia.org A & A CAsE REpORts
After obtaining informed consent, the patient was transferred to the induction room. He was connected to a pulse oximeter and electrocardiograph. Noninvasive arte-rial blood pressure was measured every 3 minutes. The patient was placed in a lateral position (Fig. 1). Using rou-tine aseptic technique, a high-frequency (6–12 MHz) linear ultrasound transducer probe in a sterile cover (Venue 40, GE Healthcare, Waukesha, WI) was placed horizontally between the coastal margin and the iliac crest. The 3 mus-cle layers of the abdominal wall were identified: external oblique, internal oblique, and transversus abdominis mus-cles (Fig. 2). The fascia surrounding the transversus abdom-inis muscle was tracked posteriorly to its origin, where the transversus abdominis muscle merges with the thoracolum-bar fascia surrounding the quadratus lumborum muscle (Fig. 3). A 17G 3-inch-long nonstimulating echogenic needle (Plexus FlexBlock, ARROW, Reading, PA) was inserted in-plane with the ultrasound probe and targeted toward the fascia transversalis. Normal saline 3 mL was used to iden-tify the splitting of the fascia. We injected 10 mL bupivacaine 0.5% in the same plane after negative aspiration. This was seen spreading around the quadratus lumborum muscle (Figs. 4 and 5). A 19G (1.1-mm diameter × 60 cm) echo-genic styletted peripheral nerve catheter (Plexus FlexBlock, ARROW) was advanced 5 cm beyond the tip of the needle with minimal resistance, and another 5 mL bupivacaine 0.5% was injected to confirm the appropriate location of the catheter tip within the quadratus lumborum fascial plane.
The procedure was repeated on the other side after plac-ing the patient in the opposite lateral position. We injected a total of 15 mL bupivacaine 0.5% on each side. Within 15 minutes, the patient reported pain as mild to none, with a
pain score ranging between 2 and 3 (on a numeric rating scale 0–10). After the initial bolus, the patient was unable to feel cold in the upper, middle, and lower abdomen bilaterally. Both catheters were connected to the patient-controlled infu-sion pumps with 0.1% ropivacaine at a basal rate of 8 mL/h each and an on-demand bolus of 5 mL every 30 minutes.
Daily patient examination revealed sensory level T7-L1 bilaterally, while the infusion was running. The catheters remained in place for 7 days. For the first 4 days, the patient reported no pain. There were no significant changes in his hemodynamics nor was there any weakness or difficulty with ambulation. On postoperative day 5, the patient started
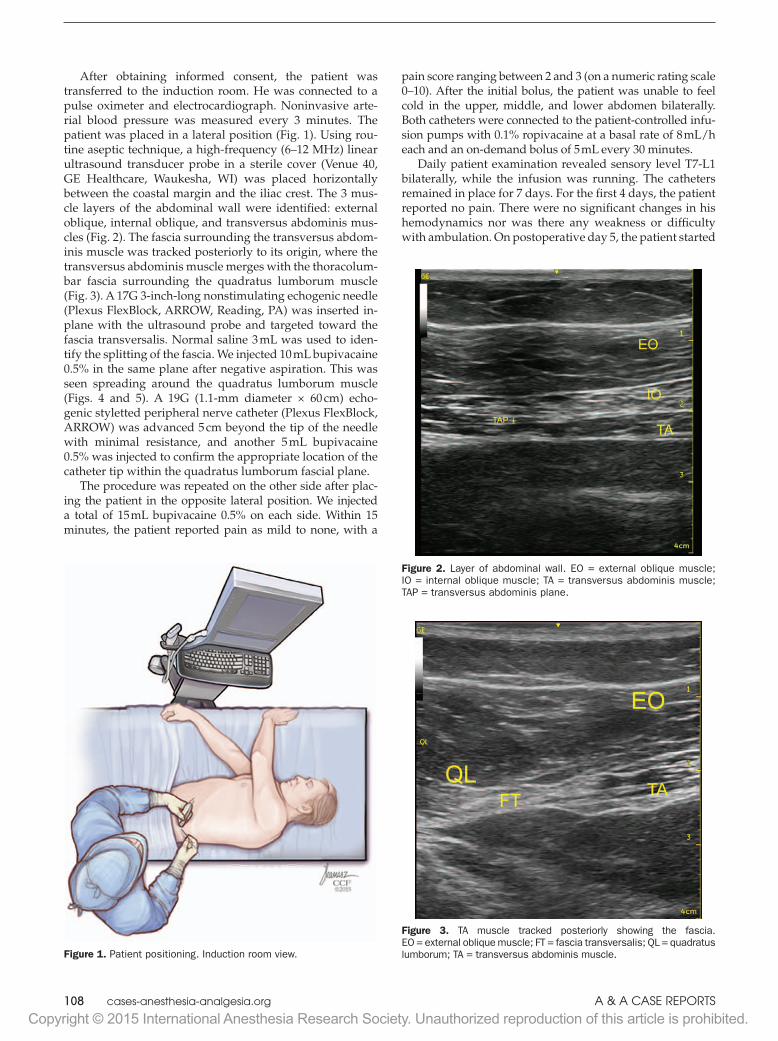
Figure 1. Patient positioning. Induction room view.
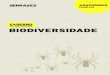
Figure 2. Layer of abdominal wall. EO = external oblique muscle; IO = internal oblique muscle; TA = transversus abdominis muscle; TAP = transversus abdominis plane.
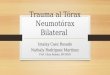
Figure 3. TA muscle tracked posteriorly showing the fascia. EO = external oblique muscle; FT = fascia transversalis; QL = quadratus lumborum; TA = transversus abdominis muscle.
Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.October 1, 2015 • Volume 5 • Number 7 cases-anesthesia-analgesia.org 109
an oral diet and began to take oral oxycodone tablets and slowly transitioned to an oral regimen. The catheters were removed on postoperative day 7, and he was discharged to home. The length of stay was dictated by the surgical plans, unrelated to pain management.
DISCUSSIONUntreated pain can lead to increased patient stress and dis-satisfaction, in addition to other cardiopulmonary compli-cations and slower recovery.1,2 There are many approaches to pain control after abdominal and colorectal surgeries. Epidural analgesia is associated with a shorter duration of postoperative ileus, attenuation of stress response, fewer pulmonary complications, and improved postoperative pain control and recovery.12
Thoracic paravertebral block has been used as an alter-native to an epidural providing analgesia for different indi-cations. Blind and ultrasound-guided techniques have been described with various success and complication rates. It is still considered a neuraxial block with comparable side effects to an epidural.13
TAP block is a simple alternative after abdominal sur-gery, with the advantage of lacking the sympathetic effects of neuraxial anesthesia. In one study, TAP blocks were shown to provide better analgesia and reduce opioid requirements when compared with a control group receiv-ing morphine PCA, nonsteroidal antiinflammatory drugs, and acetaminophen.14
The extent of analgesia provided by the TAP block depends on the site of injection and pattern of spread within the plane. Currently, there are a number of ultrasound-guided approaches in use, including an anterior oblique subcostal approach, a midaxillary approach, and a more recently proposed posterior approach.9–11 Studies have not yet definitely identified the appropriate local anesthetic
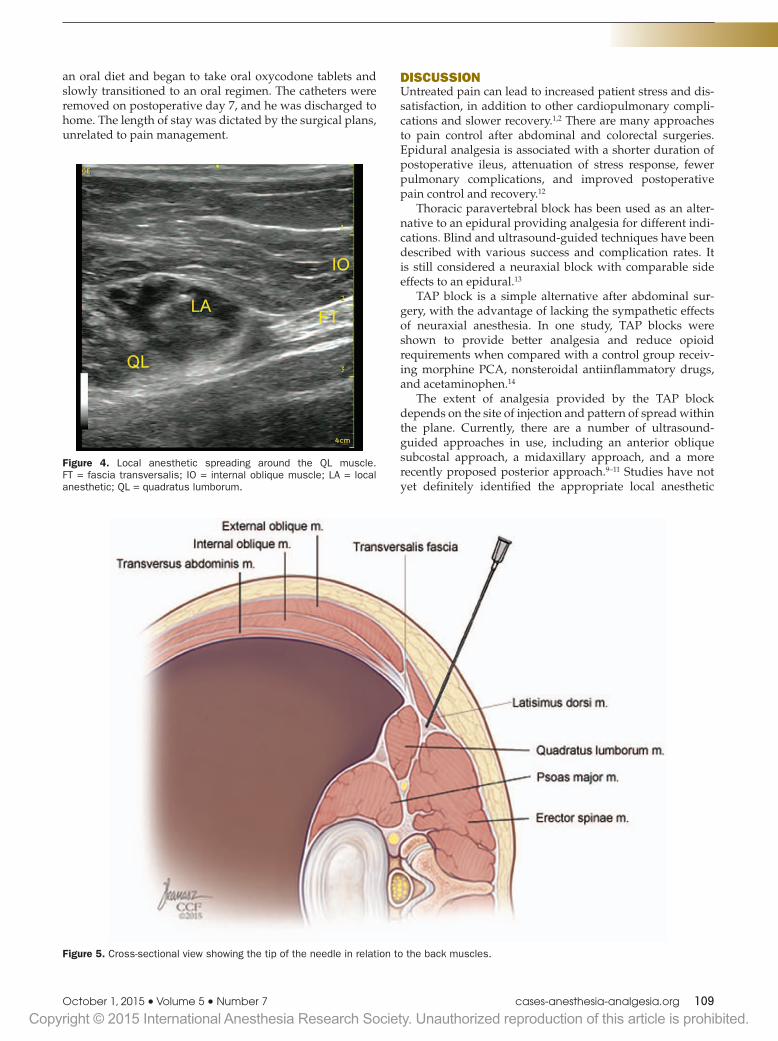
Figure 4. Local anesthetic spreading around the QL muscle. FT = fascia transversalis; IO = internal oblique muscle; LA = local anesthetic; QL = quadratus lumborum.
Figure 5. Cross-sectional view showing the tip of the needle in relation to the back muscles.
Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.110 cases-anesthesia-analgesia.org A & A CAsE REpORts
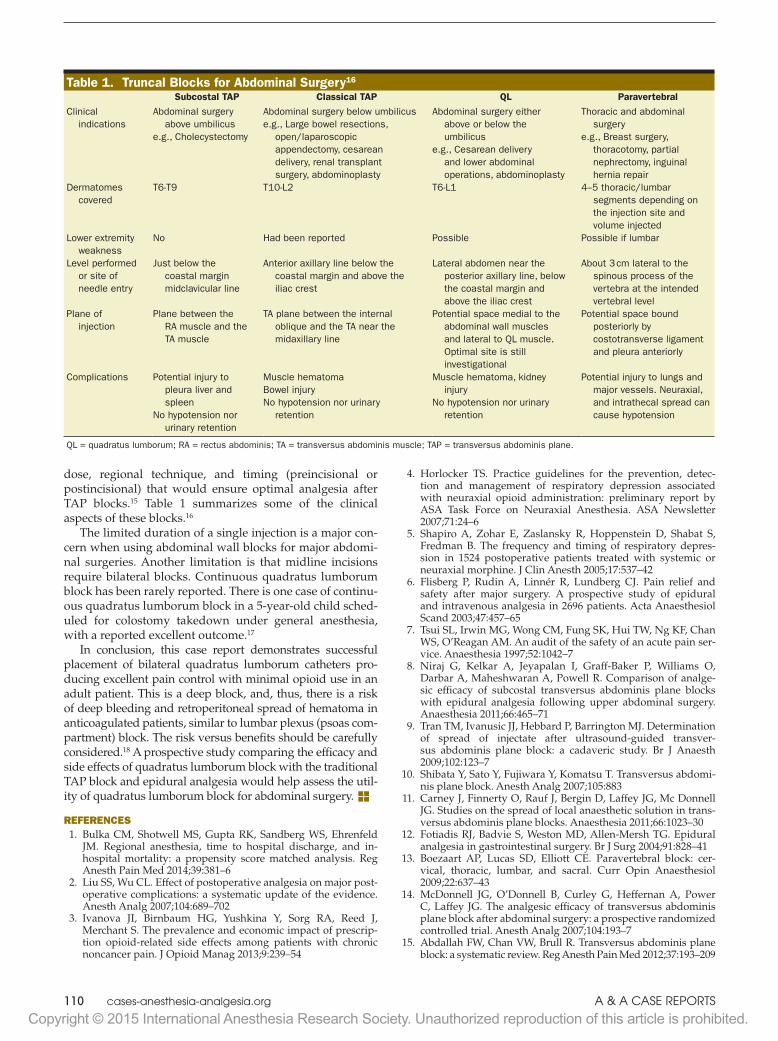
dose, regional technique, and timing (preincisional or postincisional) that would ensure optimal analgesia after TAP blocks.15 Table 1 summarizes some of the clinical aspects of these blocks.16
The limited duration of a single injection is a major con-cern when using abdominal wall blocks for major abdomi-nal surgeries. Another limitation is that midline incisions require bilateral blocks. Continuous quadratus lumborum block has been rarely reported. There is one case of continu-ous quadratus lumborum block in a 5-year-old child sched-uled for colostomy takedown under general anesthesia, with a reported excellent outcome.17
In conclusion, this case report demonstrates successful placement of bilateral quadratus lumborum catheters pro-ducing excellent pain control with minimal opioid use in an adult patient. This is a deep block, and, thus, there is a risk of deep bleeding and retroperitoneal spread of hematoma in anticoagulated patients, similar to lumbar plexus (psoas com-partment) block. The risk versus benefits should be carefully considered.18 A prospective study comparing the efficacy and side effects of quadratus lumborum block with the traditional TAP block and epidural analgesia would help assess the util-ity of quadratus lumborum block for abdominal surgery. EREFERENCES 1. Bulka CM, Shotwell MS, Gupta RK, Sandberg WS, Ehrenfeld
JM. Regional anesthesia, time to hospital discharge, and in-hospital mortality: a propensity score matched analysis. Reg Anesth Pain Med 2014;39:381–6
2. Liu SS, Wu CL. Effect of postoperative analgesia on major post-operative complications: a systematic update of the evidence. Anesth Analg 2007;104:689–702
3. Ivanova JI, Birnbaum HG, Yushkina Y, Sorg RA, Reed J, Merchant S. The prevalence and economic impact of prescrip-tion opioid-related side effects among patients with chronic noncancer pain. J Opioid Manag 2013;9:239–54
4. Horlocker TS. Practice guidelines for the prevention, detec-tion and management of respiratory depression associated with neuraxial opioid administration: preliminary report by ASA Task Force on Neuraxial Anesthesia. ASA Newsletter 2007;71:24–6
5. Shapiro A, Zohar E, Zaslansky R, Hoppenstein D, Shabat S, Fredman B. The frequency and timing of respiratory depres-sion in 1524 postoperative patients treated with systemic or neuraxial morphine. J Clin Anesth 2005;17:537–42
6. Flisberg P, Rudin A, Linnér R, Lundberg CJ. Pain relief and safety after major surgery. A prospective study of epidural and intravenous analgesia in 2696 patients. Acta Anaesthesiol Scand 2003;47:457–65
7. Tsui SL, Irwin MG, Wong CM, Fung SK, Hui TW, Ng KF, Chan WS, O’Reagan AM. An audit of the safety of an acute pain ser-vice. Anaesthesia 1997;52:1042–7
8. Niraj G, Kelkar A, Jeyapalan I, Graff-Baker P, Williams O, Darbar A, Maheshwaran A, Powell R. Comparison of analge-sic efficacy of subcostal transversus abdominis plane blocks with epidural analgesia following upper abdominal surgery. Anaesthesia 2011;66:465–71
9. Tran TM, Ivanusic JJ, Hebbard P, Barrington MJ. Determination of spread of injectate after ultrasound-guided transver-sus abdominis plane block: a cadaveric study. Br J Anaesth 2009;102:123–7
10. Shibata Y, Sato Y, Fujiwara Y, Komatsu T. Transversus abdomi-nis plane block. Anesth Analg 2007;105:883
11. Carney J, Finnerty O, Rauf J, Bergin D, Laffey JG, Mc Donnell JG. Studies on the spread of local anaesthetic solution in trans-versus abdominis plane blocks. Anaesthesia 2011;66:1023–30
12. Fotiadis RJ, Badvie S, Weston MD, Allen-Mersh TG. Epidural analgesia in gastrointestinal surgery. Br J Surg 2004;91:828–41
13. Boezaart AP, Lucas SD, Elliott CE. Paravertebral block: cer-vical, thoracic, lumbar, and sacral. Curr Opin Anaesthesiol 2009;22:637–43
14. McDonnell JG, O’Donnell B, Curley G, Heffernan A, Power C, Laffey JG. The analgesic efficacy of transversus abdominis plane block after abdominal surgery: a prospective randomized controlled trial. Anesth Analg 2007;104:193–7
15. Abdallah FW, Chan VW, Brull R. Transversus abdominis plane block: a systematic review. Reg Anesth Pain Med 2012;37:193–209
Table 1. Truncal Blocks for Abdominal Surgery16
Subcostal TAP Classical TAP QL ParavertebralClinical
indicationsAbdominal surgery
above umbilicuse.g., Cholecystectomy
Abdominal surgery below umbilicuse.g., Large bowel resections,
open/laparoscopic appendectomy, cesarean delivery, renal transplant surgery, abdominoplasty
Abdominal surgery either above or below the umbilicus
e.g., Cesarean delivery and lower abdominal operations, abdominoplasty
Thoracic and abdominal surgery
e.g., Breast surgery, thoracotomy, partial nephrectomy, inguinal hernia repair
Dermatomes covered
T6-T9 T10-L2 T6-L1 4–5 thoracic/lumbar segments depending on the injection site and volume injected
Lower extremity weakness
No Had been reported Possible Possible if lumbar
Level performed or site of needle entry
Just below the coastal margin midclavicular line
Anterior axillary line below the coastal margin and above the iliac crest
Lateral abdomen near the posterior axillary line, below the coastal margin and above the iliac crest
About 3 cm lateral to the spinous process of the vertebra at the intended vertebral level
Plane of injection
Plane between the RA muscle and the TA muscle
TA plane between the internal oblique and the TA near the midaxillary line
Potential space medial to the abdominal wall muscles and lateral to QL muscle. Optimal site is still investigational
Potential space bound posteriorly by costotransverse ligament and pleura anteriorly
Complications Potential injury to pleura liver and spleen
No hypotension nor urinary retention
Muscle hematomaBowel injuryNo hypotension nor urinary
retention
Muscle hematoma, kidney injury
No hypotension nor urinary retention
Potential injury to lungs and major vessels. Neuraxial, and intrathecal spread can cause hypotension
QL = quadratus lumborum; RA = rectus abdominis; TA = transversus abdominis muscle; TAP = transversus abdominis plane.

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.October 1, 2015 • Volume 5 • Number 7 cases-anesthesia-analgesia.org 111
16. Børglum J, Jensen K. Abdominal surgery: advances in the use of ultrasound-guided truncal blocks for perioperative pain management. In: Derbel F, ed. Abdominal Surgery. InTech, 2012:69–94
17. Visoiu M, Yakovleva N. Continuous postoperative analgesia via quadratus lumborum block—an alternative to transversus abdominis plane block. Paediatr Anaesth 2013;23:959–61
18. Horlocker TT, Wedel DJ, Rowlingson JC, Enneking FK, Kopp SL, Benzon HT, Brown DL, Heit JA, Mulroy MF, Rosenquist RW, Tryba M, Yuan CS. Regional anesthesia in the patient receiving antithrombotic or thrombolytic therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Third Edition). Reg Anesth Pain Med 2010;35:64–101