Embed Size (px)
DESCRIPTION
Guideline up date for Dyslipidemia 2014
Citation preview
Disease of Lipoprotein Metabolism and Lipidemia, Obesity
By… Krairat Komdee, MD.
Department of Internal Medicine, Phayao Hospital
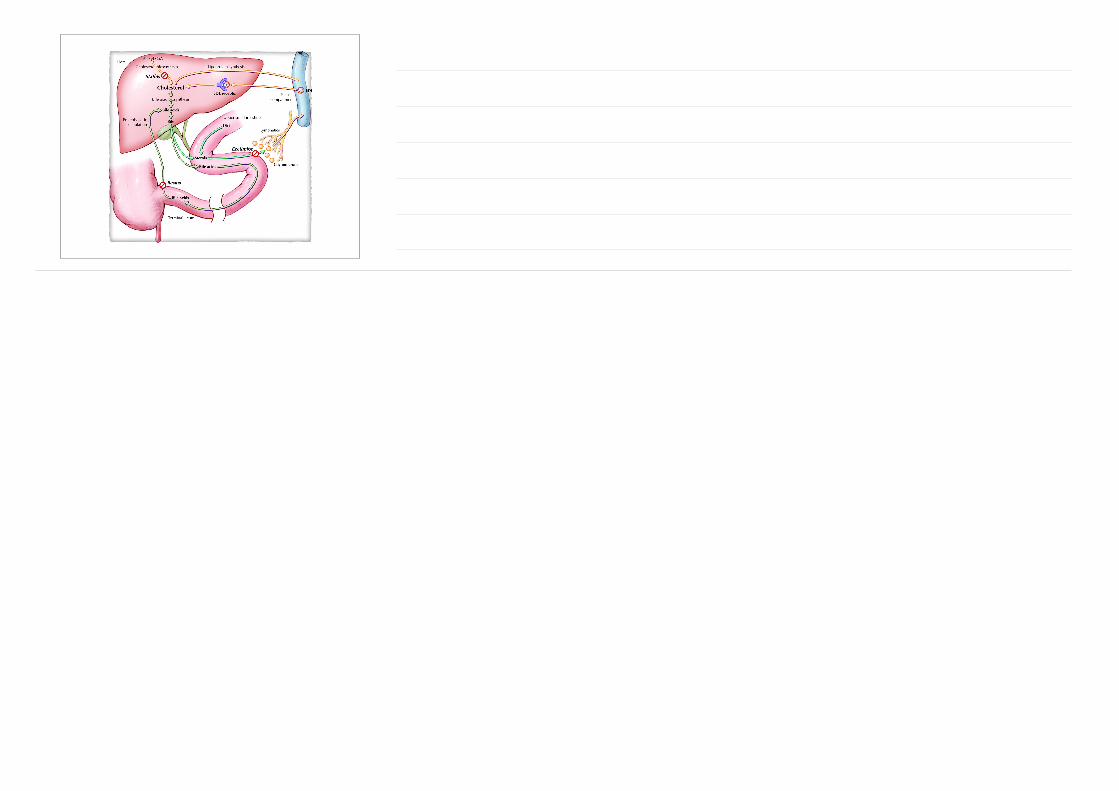
Dietary cholesterol ~ 300-700mg/day
Biliary cholesterol ~ 1000mg/day
Adapted from Champe PC, Harvey RA. Biochemistry. 2nd ed. Philadelphia: Lippincott Raven, 1994; Glew RH. In Textbook of Biochemistry with Clinical Correlations. 5th ed. New York: Wiley-Liss, 2002:728-777; Ginsberg HN, Goldberg IJ. In Harrison’s Principles of Internal Medicine. 14th ed. New York: McGraw-Hill, 1998:2138-2149; Shepherd J Eur Heart J Suppl 2001;3(suppl E):E2-E5; Hopfer U. In Textbook of Biochemistry with Clinical Correlations. 5th ed. New York: Wiley-Liss, 2002:1082-1150.
Physiologic role of cholesterolNormal biologic function
Component of cell membranes
Precursor of other steroids
Cortisol, progesterone, estrogen, testosterone, bile acids
Excess cholesterol
CHD
XanthomasAdapted from Saladin KS. Anatomy and Physiology. 2nd ed. Boston: McGraw-Hill, 2001; Jones PH et al. In Hurst’ s The Heart. Arteries and Veins. 9th ed. New York: McGraw-Hill, 1998:1553-1581; Ginsberg HN, Goldberg IJ. In Harrison’s Principles of Internal Medicine. 14th ed. New York: McGraw-Hill, 1998:2138-2149.
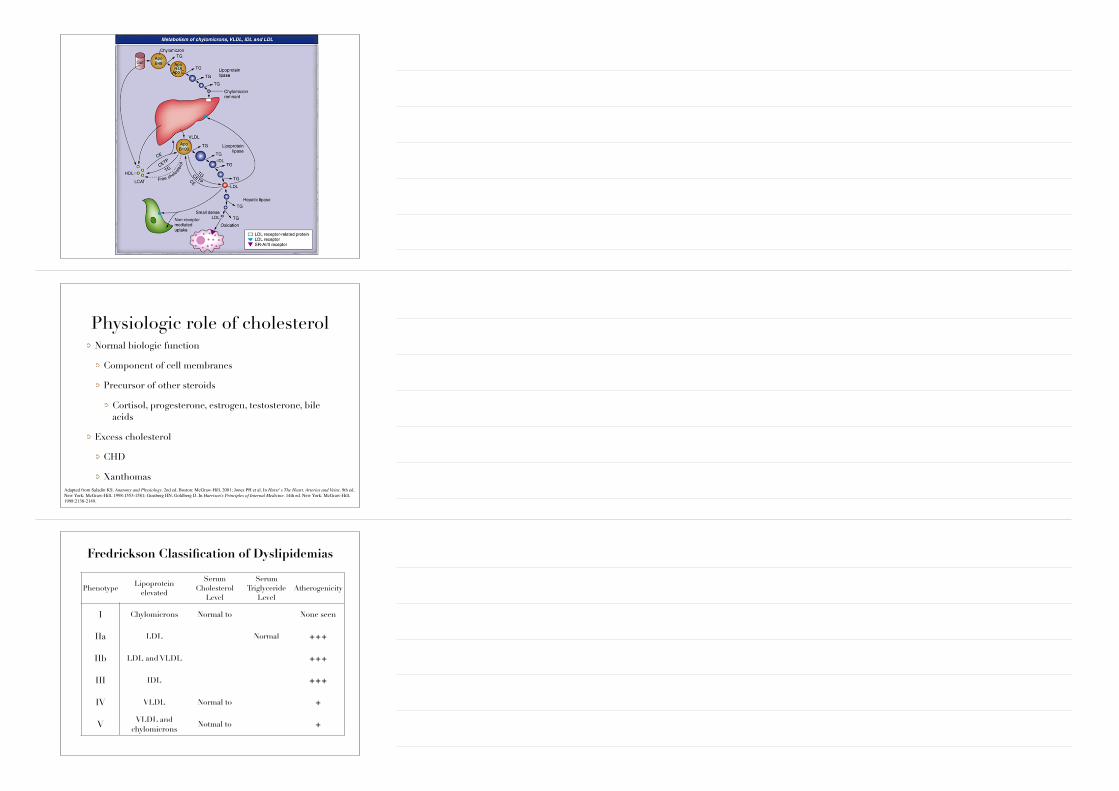
Fredrickson Classification of Dyslipidemias
PhenotypeLipoprotein
elevated
SerumCholesterol
Level
SerumTriglyceride
LevelAtherogenicity
I Chylomicrons Normal to None seen
IIa LDL Normal +++
IIb LDL and VLDL +++
III IDL +++
IV VLDL Normal to +
V VLDL and chylomicrons
Notmal to +
Types of Dyslipidemia1. Hypertriglyceridemia
2. Hypercholesterolemia
3. Hyperalphalipoproteinemia
4. Hypoalphalipoproteinemia
5. Hypobetalipoproteinemia
Common genetic dyslipidemiaFamilial hypercholesterolemia
Polygenic hypercholesterolemia
Familial defective apolipoprotein B100
Familial hypertriglyceridemia
Familial combined hyperlipidemia
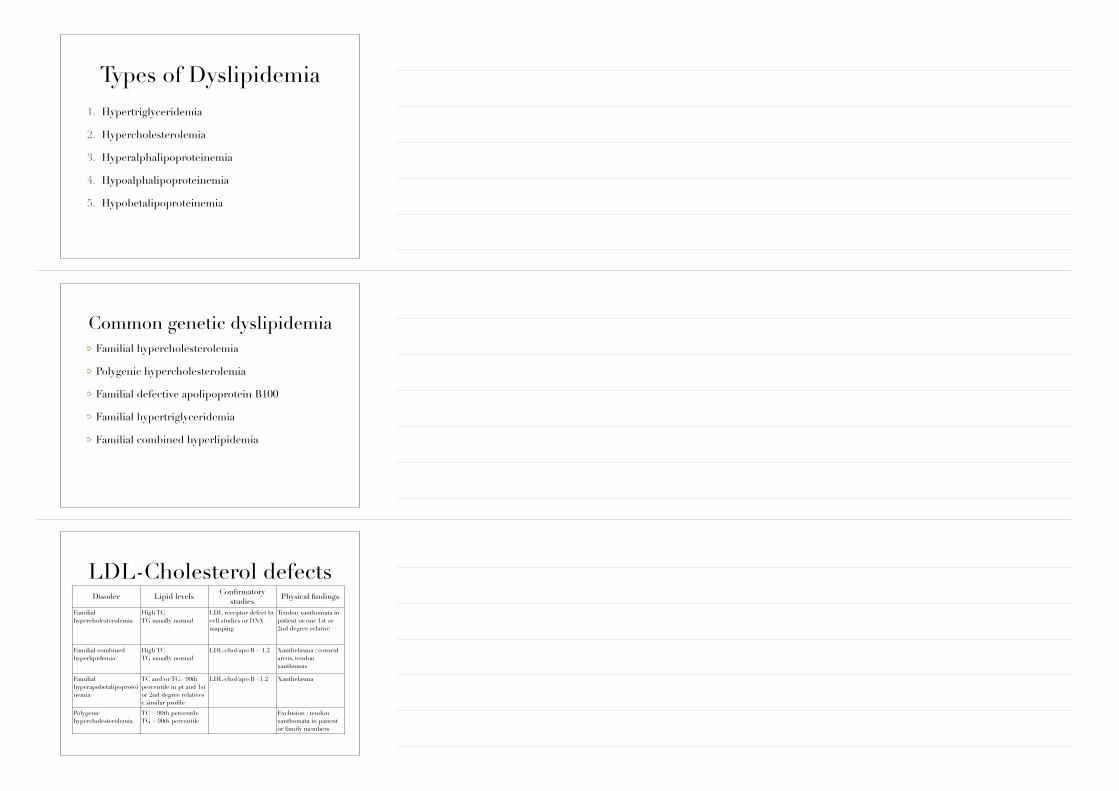
LDL-Cholesterol defectsDisoder Lipid levels Confirmatory
studiesPhysical findings
Familial hypercholesterolemia
High TC TG usually normal
LDL receptor defect by cell studies or DNA mapping
Tendon xanthomata in patient or one 1st or 2nd degree relative
Familial combined hyperlipidemia
High TC TG usually normal
LDL-chol/apo B < 1.2 Xanthelasma ; corneal arcus, tendon xanthomas
Familial hyperapobetalipoproteinemia
TC and/or TG> 90th percentile in pt and 1st or 2nd degree relatives c similar profile
LDL-chol/apo B <1.2 Xanthelasma
Polygenic hypercholesterolemia
TC > 90th percentile TG < 90th percentile
Exclusion : tendon xanthomata in patient or family members
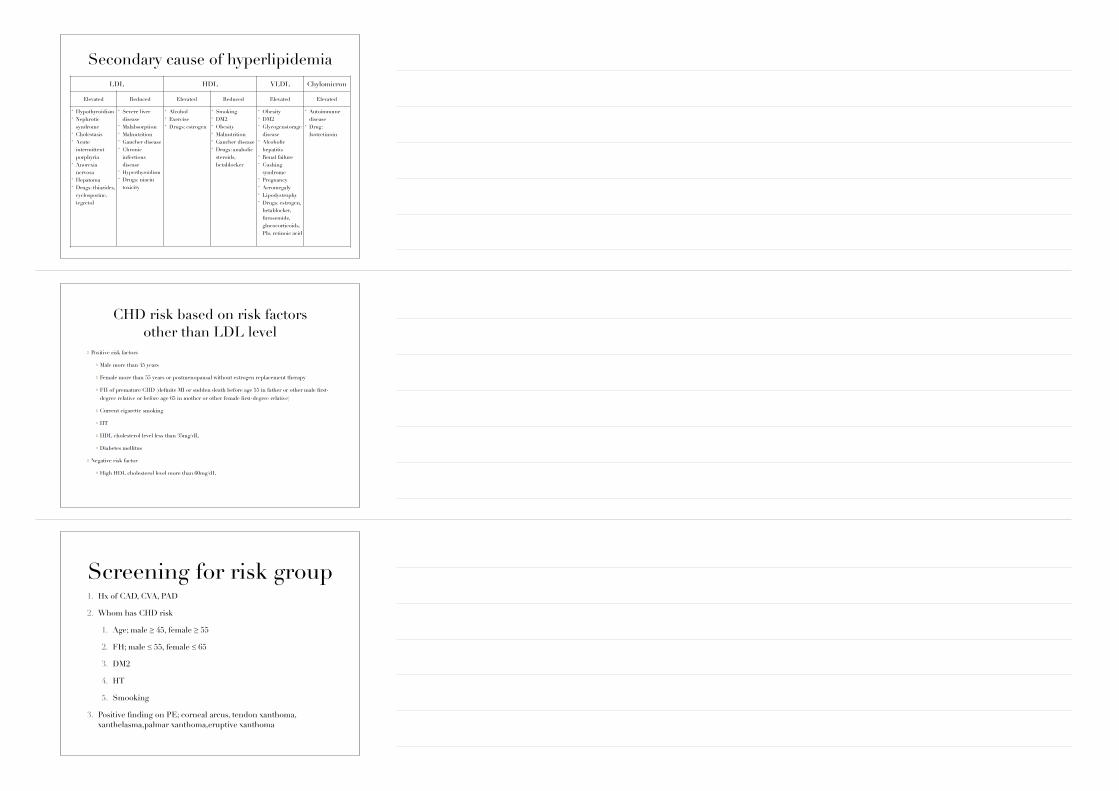
Secondary cause of hyperlipidemiaLDL HDL VLDL Chylomicron
Elevated Reduced Elevated Reduced Elevated Elevated
• Hypothyroidism • Nephrotic
syndrome • Cholestasis • Acute
intermittent porphyria
• Anorexia nervosa
• Hepatoma • Drugs: thiazides,
cyclosporine, tegretol
• Severe liver disease
• Malabsorption • Malnutrition • Gaucher disease • Chronic
infectious disease
• Hyperthyroidism • Drugs: niacin
toxicity
• Alcohol • Exercise • Drugs: estrogen
• Smoking • DM2 • Obesity • Malnutrition • Gaucher disease • Drugs: anabolic
steroids, betablocker
• Obesity • DM2 • Glycogenstorage
disease • Alcoholic
hepatitis • Renal failure • Cushing
syndrome • Pregnancy • Acromegaly • Lipodystrophy • Drugs: estrogen,
betablocker, furosemide, glucocorticoids, PIs, retinoic acid
• Autoimmune disease
• Drug: Isotretinoin
CHD risk based on risk factors other than LDL level
Positive risk factors
Male more than 45 years
Female more than 55 years or postmenopausal without estrogen replacement therapy
FH of premature CHD (definite MI or sudden death before age 55 in father or other male first-degree relative or before age 65 in mother or other female first-degree relative)
Current cigarette smoking
HT
HDL cholesterol level less than 35mg/dL
Diabetes mellitus
Negative risk factor
High HDL cholesterol level more than 60mg/dL
Screening for risk group1. Hx of CAD, CVA, PAD
2. Whom has CHD risk
1. Age; male ≥ 45, female ≥ 55
2. FH; male ≤ 55, female ≤ 65
3. DM2
4. HT
5. Smooking
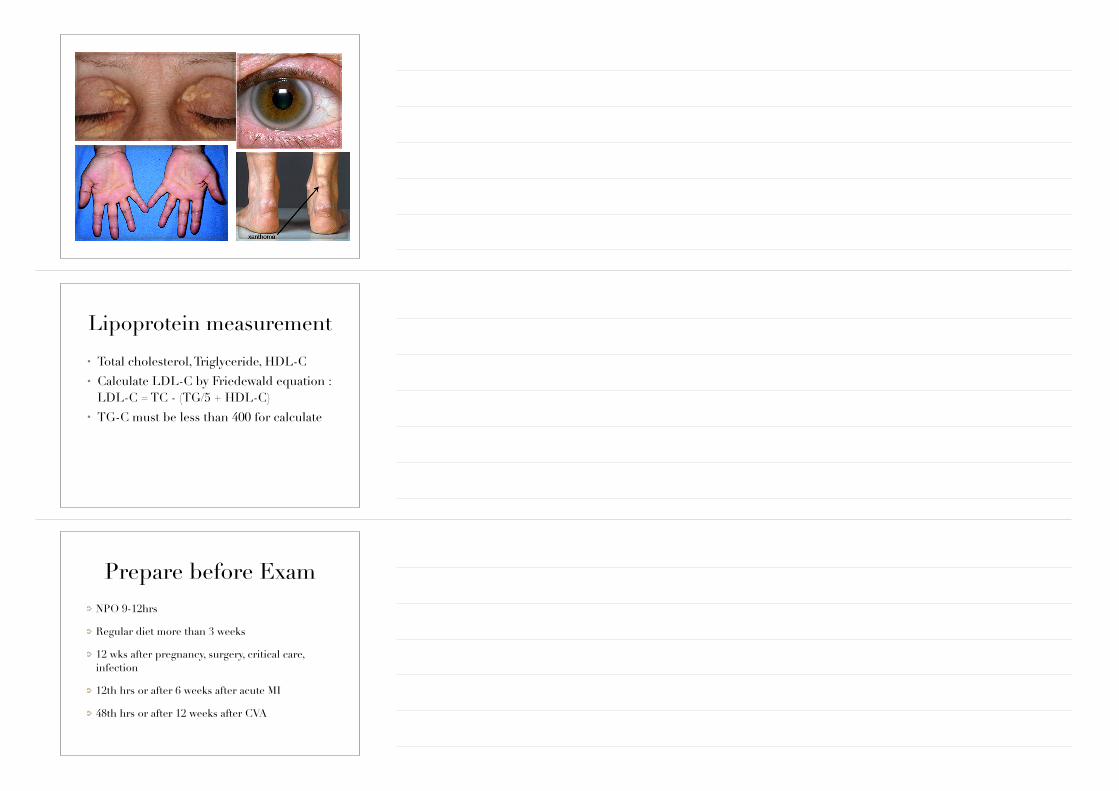
3. Positive finding on PE; corneal arcus, tendon xanthoma, xanthelasma,palmar xanthoma,eruptive xanthoma
Lipoprotein measurement
• Total cholesterol, Triglyceride, HDL-C • Calculate LDL-C by Friedewald equation :
LDL-C = TC - (TG/5 + HDL-C) • TG-C must be less than 400 for calculate
Prepare before ExamNPO 9-12hrs
Regular diet more than 3 weeks
12 wks after pregnancy, surgery, critical care, infection
12th hrs or after 6 weeks after acute MI
48th hrs or after 12 weeks after CVA
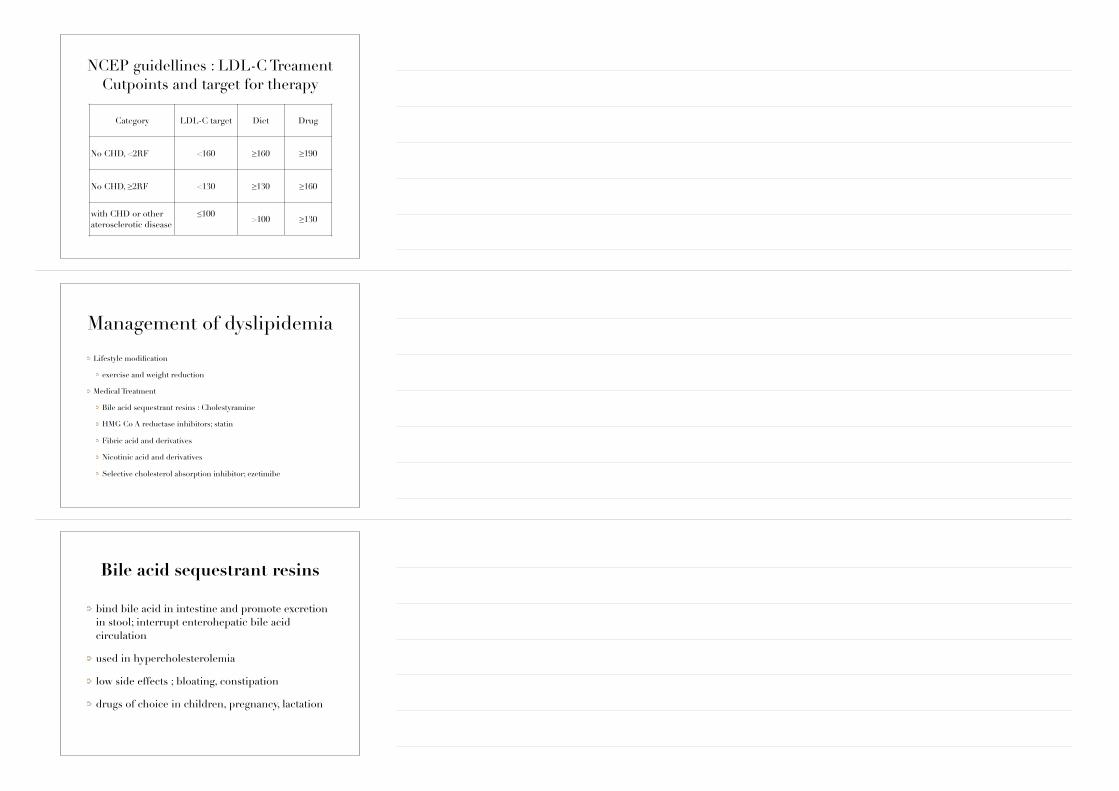
NCEP guidellines : LDL-C Treament Cutpoints and target for therapy
Category LDL-C target Diet Drug
No CHD, <2RF <160 ≥160 ≥190
No CHD, ≥2RF <130 ≥130 ≥160
with CHD or other aterosclerotic disease
≤100 >100 ≥130
Management of dyslipidemia
Lifestyle modification
exercise and weight reduction
Medical Treatment
Bile acid sequestrant resins : Cholestyramine
HMG Co A reductase inhibitors; statin
Fibric acid and derivatives
Nicotinic acid and derivatives
Selective cholesterol absorption inhibitor; ezetimibe
!
Bile acid sequestrant resins
bind bile acid in intestine and promote excretion in stool; interrupt enterohepatic bile acid circulation
used in hypercholesterolemia
low side effects ; bloating, constipation
drugs of choice in children, pregnancy, lactation
HMG CoA reductase inhibitorsInhibits HMG-CoA reductase
Interpatient variability in response to statin
most common side effect; myopathy, hepatotoxicity
Nicotinic acid and derivatives
inhibits lipoprotein secretion
used in hypercholesterolemia
side effects; flushing, itching, hepatitis, oesophageal reflux
increase HDL-C at high dose
Selective cholesterol absorption inhibitor
improve LDL-C, TC, HDL, TG
cholesterol absorption inhibitors
target cholesterol absorption in intestine
mechanism of action complementary of statin
achieves lipid reductions greater than statin alone
may be use as mono therapy for patients intolerant to statin