Embed Size (px)
Citation preview
JOURNAL OF VASCULAR SURGERYVolume 58, Number 5 Abstracts 1439
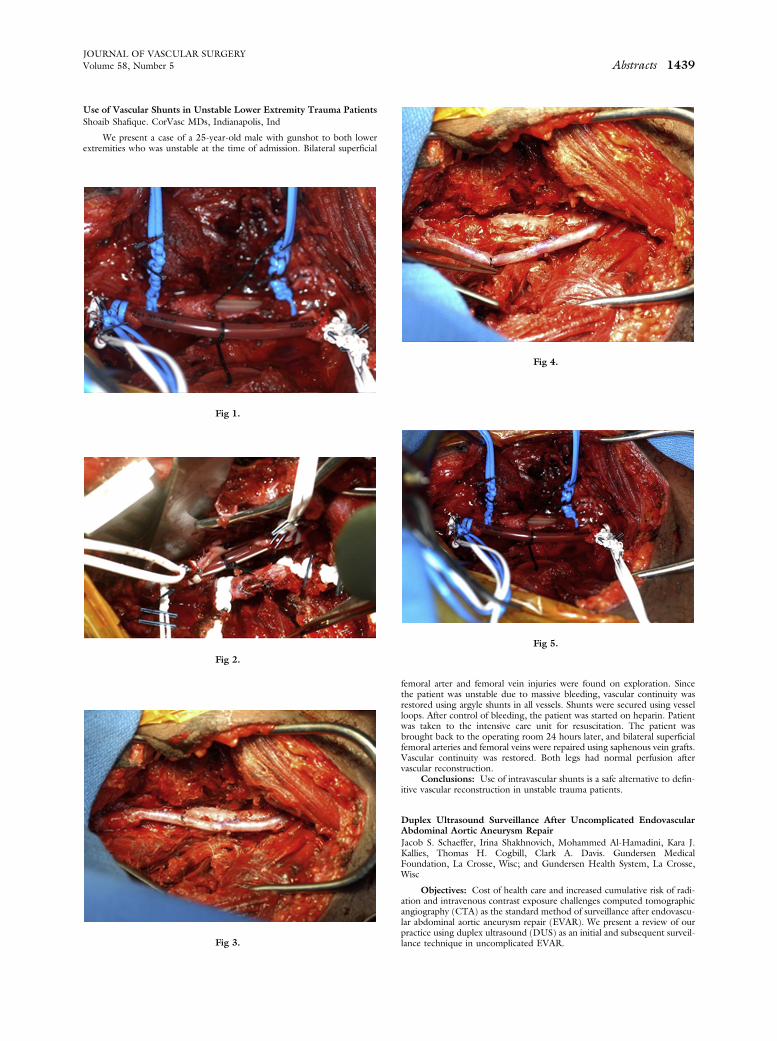
Use of Vascular Shunts in Unstable Lower Extremity Trauma PatientsShoaib Shafique. CorVasc MDs, Indianapolis, Ind
We present a case of a 25-year-old male with gunshot to both lowerextremities who was unstable at the time of admission. Bilateral superficial
Fig 1.
Fig 2.
Fig 3.
Fig 4.
Fig 5.
femoral arter and femoral vein injuries were found on exploration. Sincethe patient was unstable due to massive bleeding, vascular continuity wasrestored using argyle shunts in all vessels. Shunts were secured using vesselloops. After control of bleeding, the patient was started on heparin. Patientwas taken to the intensive care unit for resuscitation. The patient wasbrought back to the operating room 24 hours later, and bilateral superficialfemoral arteries and femoral veins were repaired using saphenous vein grafts.Vascular continuity was restored. Both legs had normal perfusion aftervascular reconstruction.
Conclusions: Use of intravascular shunts is a safe alternative to defin-itive vascular reconstruction in unstable trauma patients.
Duplex Ultrasound Surveillance After Uncomplicated EndovascularAbdominal Aortic Aneurysm RepairJacob S. Schaeffer, Irina Shakhnovich, Mohammed Al-Hamadini, Kara J.Kallies, Thomas H. Cogbill, Clark A. Davis. Gundersen MedicalFoundation, La Crosse, Wisc; and Gundersen Health System, La Crosse,Wisc
Objectives: Cost of health care and increased cumulative risk of radi-ation and intravenous contrast exposure challenges computed tomographicangiography (CTA) as the standard method of surveillance after endovascu-lar abdominal aortic aneurysm repair (EVAR). We present a review of ourpractice using duplex ultrasound (DUS) as an initial and subsequent surveil-lance technique in uncomplicated EVAR.

Fig 3. Carotid mycotic aneurysm specimen and histology
JOURNAL OF VASCULAR SURGERY1440 Abstracts November 2013
Methods: A retrospective review of imaging surveillance was conduct-ed for patients who underwent EVAR from 2004 to 2012 and had$1 post-operative imaging study. DUS was the primary imaging modality afteruncomplicated EVAR, with CTA reserved for patients with suspicious find-ings such as new endoleak or increase in sac size. Correlation between DUSresults and CTA were assessed for sac size and presence and type ofendoleak.
Results: Mean follow-up was 2.2 years for 114 patients. Twenty-three endoleaks (5 type I, 17 type II, and 1 type IV) were detected in22 patients. Ten (43%) endoleaks were identified on DUS alone andbecause the aneurysm sac was stable or smaller, CTA was not obtained.None of these patients suffered subsequent undetected endoleak orrupture. Eight (35%) endoleaks were identified initially on DUS andconfirmed by CTA, and three of these patients had secondary interven-tions. One (4%) endoleak was identified on CT only. There was one falsepositive and three false negative endoleaks on DUS. One patient witha false negative result had an endoleak identified on subsequent CTAand underwent coil embolization. The other two patients’ follow-upcourse deviated from our protocol due to severe comorbidities includingrenal disease, and therefore, follow-up CTA was not obtained. One ofthese patients presented with rupture and death. Among 26 patientswith both DUS and CTA, positive predictive value and negative predictivevalue were 0.86 and 0.88, respectively. Sac size on DUS was stronglycorrelated to CT (r ¼ 0.8; P < .001).
Conclusions: In our experience, DUS was safe and effective for initialand follow-up surveillance after uncomplicated EVAR.
Ruptured Carotid Mycotic Tuberculoid Aneurysm from IntravesicalBacillus Calmette-GuerinAnahita Dua, SreyRam Kuy, Henryk Baraniewski, Cheong J. Lee.Department of Vascular Surgery, Medical College of Wisconsin,Milwaukee, Wisc; the Center for Translational Injury Research, Universityof Texas-Houston, Houston, Tex; and the University of Illinois atChicago, Chicago, Ill
Fig 1. Computed tomography scan of the head and neck
Fig 2. Ruptured carotid mycotic aneurysm resection and reconstruction
Objectives: Mycotic aneurysms as a result of intravesical BacillusCalmette-Guerin (BCG) treatment are rare. Ruptured carotid mycoticaneurysms are particularly exceptional and present challenging vascularsurgical problems.
Case Study: A 73-year-old man with a history of lung cancer andurothelial carcinoma who was undergoing chemotherapy presented tohis primary care physician with a progressivelyenlarging right neckmass over a 5-month period (Fig 1). He was referred to an otolaryngol-ogist for a biopsy under local anesthesia. During the attempted biopsy,the patient developed facial asymmetry and had a near syncopalepisode. Vascular surgery was consulted emergently. A computedtomography scan was performed, revealing a carotid pseudoaneurysmwithin a mass enveloping the carotid bifurcation. The patient under-went immediate operative exploration. A hard, fibrotic tumor wasencountered just deep to the sternocleidomastoid muscle, emanatingfrom the carotid sheath (Fig 2). Given the patient’s cancer history,this was suspected to be a metastatic implant, presenting as a rupturedaneurysm (Fig 3). We proceeded with radical resection and carotidreplacement using PTFE (Fig 2). His postoperative course wasuneventful, and his facial asymmetry resolved. His final pathologicalspecimen showed necrotizing granulomas and few multinucleated giantcells concerning for a tuberculoma (Fig 3). Postoperatively, we learnedthat the patient’s urothelial carcinoma had been treated with intraves-ical (BCG). The patient did well postoperatively with anti-tuberculosistreatment.
Conclusions: Intravesicular BCG immunotherapy is an acceptedtreatment for patients with urothelial carcinoma. Rare complicationsof arterial mycotic aneurysms have been reported, with the majoritybeing infrarenal aortic mycotic aneurysms. We describe a rare case ofa carotid mycotic aneurysm following intravesical BCG treatment anddescribe its successful management. Symptoms of cervical lymphade-nopathy in the seeing of BCG treatment should prompt the clinicianto evaluate for systemic tuberculoid dissemination and the possibilityof life-threating mycotic aneurysms. A prosthetic vascular graft can bea durable repair for a ruptured carotid mycotic aneurysm in the emer-gent setting.
Subclavian Vein Stent Fracture Caused by Venous MotionAlexandros Mallios, Kevin Taubman, Paul Claiborne, John Blebea.Department of Vascular Surgery, University of Oklahoma, Tulsa, Okla
Objectives: Primary subclavian vein stents are not recommended dueto risk of fracture as they are compressed between the clavicle and first rib.After thoracic outlet decompression, stent insertion is indicated for venousre-stenosis. We present a case suggesting that repetitive vein movementduring respiration may induce sufficient strain to cause stent fracture evenafter first rib removal.
Case Report: A 56-year-old male with a prior venous thoracic outletsyndrome (TOS) presented with recurrent arm swelling. Six years earlier,he had undergone a right first rib resection for decompression (Fig 1), fol-lowed a year later with percutaneous transluminal angioplasty (PTA) andplacement of a self- expanding Nitinol stent for right subclavian veinstenosis (Fig 2). The patient did well for 5 years but then presented tous with recurrent arm swelling. A venogram revealed a stent fracture andre-stenosis of the right subclavian vein with minimal contrast flow (Fig3). Interestingly, we observed that the medial half of the stent was movingin concert with the movements of the medial part of the subclavian vein.The fracture of the stent was localized at the junction of the mobile and