Embed Size (px)
Citation preview

Practical Therapeutics
Drugs 15: 72-79 (1978)© ADIS Press 1978
Drug Interactions with Antihypertensive Drugs
J.E. Crook and A.S. Nies*
Division of Clinical Pharmacology, Department of Pharmacology, Vanderbilt UniversitySchool of Medicine, Nashville, Tennessee
Summary Drug interactions with antihypertensive drugs can be either beneficial or hazardous. Thehazardous interactions are relatively inf requent but must be shown so they can be avoided.Those of most importance involve interaction with guanethidine-type agents and tricyclic antidepressants. amphetamine-type anorexiants or phenolpropanolamine-type common coldremedies; combined use of potassium retaining diuretics with potassium supplements; and incautious use of diuretics with cardiac glycosides. The beneficial interactions are the basis formodern antihypertensive therapy and can be of major help (f logically applied 10 therapeuticproblems.
A large body of information concerning drug interactions has been generated during the presentdecade. The majority of the interactions reported haveemphasised the adverse nature of the phenomenon.However, this does not apply to all cases. Indeed,some drug interactions can be a major help to theclinician. Proper utilisation of the interaction assumesthat the individual pharmacological characteristics ofthe involved drugs are known and that a therapeuticgoal is clearly outlined prior to therapy. This reviewwill point out the potentially useful interactionsamong different groups of antihypertensive agents, inaddition to those interactions that increase the risk ofside-effects and detract from the desired therapeuticendpoint. The two major types of drug interactionsare: (1) those that alter the amount of drug at the siteof action by affecting the drug's absorption, distribution or elimination (pharmacokinetic interactions),
and (2) those that alter the effectof any given amountof drug (pharmacodynamic interactions).
J. General Considerations
Needless to say, the first step towards' correctionof an existing adverse interaction is its recognition.The first clue to the possibility that an interaction istaking place may simply be that the desiredtherapeutic goal has not been reached or that bloodpressure control previously obtained is now lost.Once it has been determined that the patient is complying with the outlined regimen (either by pill count,plasma drug levels, 24 hour urine sodium levels, etc)
• Dr . Nies is a Burroughs Wellcome Scholar in Clinical Pharmacology. Supported in part by GM 15431. GM 00 113.

Drug Interactions with Antihypertensives
Table I. Recognit ion and ut ilisation of drug interactions occurring with antihypertensive drugs
A. Recogn ition of undesirable interactionsa) First clue may be loss of well established blood pres
sure control or failure to achieve normalisation of ploodpressure.
b) Patients or other clinicians may unknowing ly add drugsthat interact adversely so an in-depth review of allmedications self-prescribed or received is necessary.
c) Acceleration of associated diseases or newly emergentillnesses may cause confusion and should prompt athorough re-evaluation of the patient.
B. Drug interactions that are undesirablea) Potassium retaining diuretics with potassium supple
ments (avoid).b) Guanethidine and related drugs comb ined w ith tr i
cyclics , amphetamines, ephedrine, etc . (avoid, exceptfenfluramine or moderate dosage of doxepin).
c) Clonidine combined with desipram ine (avoid).d) Propranolol and other ~-blockers with hypoglycaemic
agents (use with caution).e) Monoamine oxidase inhibitors with foods rich in
tyramine or dopamine , proprietary medicines that contain ephedrine, phenylpropanolamine , etc. (avoid).
f) Incaut ious use of digitalis and diuret ics (avoidpotassium depletion).
C. Drug interactions that are desirablea) Diuretics remain a cornerstone of antihypertens ive
therapy. Their ability to control blood pressure orrestrict adverse effects may be enhanced"by interaction with:1) Sodium restricted diets.2) Potassium sparing diuretics .3) Cautious use of cardiac glycosides.4) Sympathetic inhibiting drugs frequently require
concomitant diuretic therapy for maximumefficacy.
b) Vasodilators may be used in a desirable interaction
with:1) Sympathetic inhibit ing drugs to offset the undesir
able reflexively induced cardiovascular effects.2) Diuret ics to minim ise flu id retention.
then further investigation is needed. An updatedmedication history from the patient is essential as thismay have been modified by the patient or by otherclinicians due to the presence of another disease state.
73
Even geographical relocation may playoJ a role,especiallyif there is a change in the mineral content ofthe drinking water. Many proprietary or 'over-thecounter' medications have a high sodium content or,as with 'cough and cold' preparations, contain ingredients that may interact with antihypertensive drugs.
Before considering the variety of intra- and intergroup interactions that may occur among the antihypertensive drugs, it should be re-emphasised thatthere are both 'desirable' and 'undesirable' types (tableI), The 'desirable' interactions are characterised by anincreased therapeutic usefulness with a decreasedlevel of side-effects. The 'undesirable: interactionshave characteristics that defeat the purpose of therapyand increase the risk of side-effects associated withany plan of therapy.
2. PharmacokineticInteractions
Since antihypertensive drugs are usually administered orally on a continuous basis, the gastrointestinal organ system and its contents are the first tocome into contact with the medication. Although thepresence of food or altered gut motility plays a role inthe absorption of other medications (Hartshorn,1977; Nimmo, 1976), these factors have not beenshown to affect the absorption of the blood pressurelowering agents. However, the contents of certainfoods. most notably the tyramine-rich cheeses, canadd a dangerous element to the therapeutic regimenwith monoamine oxidase inhibitor type antihypertensive agents (see section 4.4).
The distribution of an antihypertensive drug to itssite of action can be altered by other drugs. This typeof interaction has been well studied (Mitchell et al.,1970) and is best typified by the interaction ofguanethidine, bethanidine or debrisoquine and the tricyclic antidepressants (see section 4.1).
Alteration of the elimination of antihypertensivedrugs does not seem to be a clinically importantmechanism of interaction. However, recent work hasshown that propranolol can decrease hepatic bloodflow and thereby reduce the clearance of some other

Drug Interactions with Antihypertensives
Table II. Classification of diuretics by site of action
74
Class
1. Potassium losing nstriureticsa) Thiazide and thiazide-like
Bendrofluazide (bendroflumethiazidelBenzthiazideChlorothiazideChlorthalidoneClopamideCyclopenthiazideCyclothiazideHydrochlorothiazideHydroflumethiazideMefrusideMethyclothiazideMetolazonePolythiazideQuinethazoneTrichlormethiazide
b] 'Loop' diureticsEthacrynic acidFrusemide (furosemide)Bumetanide
2. Potassium retaining natriureticsSpironolactoneTriamtereneAmiloride
Site of action
Distal convulute<jtubule
Ascending (thick)limb of Henle's loop
Distal tubule andcollecting duct
Mechanism of action
Interference withsodium reabsorption
Interference withactive sodium andchloride reabsorption
Interference insodium/ potassiumexchange
drugs, such as lignocaine (lidocaine), that are avidlyextracted by the liver (Nies et al., 1974).
Although most reviews of drug interaction focuson the pharmacokinetic aspects mentioned above, themajority of the beneficial interactions and some of theadverse interactions among antihypertensive drugsare of the pharmacodynamic type and do not resultfrom alterations of drug absorption, distribution orelimination.
3. Interactions with Diuretics
Diuretics constitute the largest class of antihypertensive agents. Table II lists some of the more common diuretics, subdivided according to their sites of
action. Although other factors may contribute to theireffectiveness, the major factor is an ability to induce anegative sodium and water balance.
Limiting sodium intake may often be the firsttherapy used when the diagnosis of hypertension isestablished. Dustan et al. (t 973) have shown thatsodium deprivation can mimic the effect of diureticsin lowering blood pressure. Viewed in this context,the addition of a diuretic to sodium restriction constitutes a desirable form of drug interaction in thatless diuretic will be required for a given degree ofsodium and water depletion and blood pressurereduction. On the other hand, excessive sodium intake can nullify the effects of diuretics on blood pressure. These considerations become even more important when patients are also being treated with a

Drug Interactions w ith Antihypertensives
'blocker' of the sympathetic nervous system. All ofthe drugs that inhibit adrenergic function result insodium retention and this effect tends to raise theblood pressure and counteract the antihypertensiveaction of the drugs producing a 'pseudotolerance',Adrenergic blockade can still be present but the antihypertensive effect is masked by the sodium retention, and diuretics will restore the antihypertensiveefficacy of the adrenergic blocker (Dustan et aI.,1972) .
The possibility for interaction among the variousdiuretics within a group is virtually negligibleas thereshould be no reason to co-administer more than Idiuretic from a group. If the maximum effect of anyof the thiazide-like diuretics is insufficient then oneshould substitute a 'loop' diuretic rather than addanother thiazide. In general, thiazides are the diureticsof first choice unless renal failure exists in which case'loop' diuretics are more effective. A desirable intergroup pharmacodynamic interaction is exemplifiedby the combination of a thiazide or 'loop' diureticwith one of the potassium-retaining natriuretics inorder to avoid potassium wasting and hypokalaemia.Combined therapy in this case, is helpful in off-setting a potential for interaction that arises not from thedrugs per se, but from an adverse effect common tothe thiazides and 'loop' diuretics (i.e. hypokalaemia),Should cardiac glycosides and diuretics be usedsimultaneously, the risk of potentially fatal digitalisinduced arrhythmias is increased because potassiumdepletion sensitises the myocardium to the toxicef!"ects of digitalis. However, prior to using apotassium retaining natriuretic , the clinician must beaware of the danger of producing hyperkalaernia ifpotassium supplementation (medication orpotassium-rich foods) is continued or if renal failureis present. Although not an antihypertensive drug,potassium supplementation is so often an integralpart of cardiovascular therapy that it may be continued without regard for the potentially serious interactions with potassium retaining diuretics.
Hyperglycaemia, hyperuricaemia and hypercalcaemia are best classified as adverse reactions thatmay occur during treatment with diuretics. They are
75
not the result of interactions but represent a potentialsource of interaction, especially if they are not recognised for what they are. The chance for undesirablereactions escalates if tratment of the adverse effects isdeemed necessary and another drug is added to theregimen.
In a similar manner, the adverse effects may betroublesome by manifesting themselves in a patientwho previously had well controlled diabetes or gout.Under such circumstances, modification of either thedose or drug employed may be beneficial in re-establishing control. Although diuretics are usually considered the drugs of first choice for hypertension, acogent argument can be made for using a ~
adrenoceptor blocking drug (~-blocker) for initialtherapy of a patient with adult onset diabetes orsymptomatic gout. Newer diuretics that areuricosuric may also be helpful in this situation.
4. Interactions With Adrenergic InhibitingDrugs
For many patients, diuretic therapy alone is notable to adequately control the hypertension. In suchpatients, a drug affecting the sympathetic nervoussystem is added to the diuretic in order to take advantage of the desirable interactions between these classesof drugs. The diuretics avoid the fluid retention that iscommonly produced by drugs inhibiting sympatheticfunction and thereby increase the antihypertensiveefficacy of these drugs. Many of the sympathetic inhibiting drugs also interfere with renal renin release.Since all diuretics are potent stimulators of reninrelease, the combination of a diuretic plus a sympathetic inhibiting drug frequently results in a plasmarenin activity that is less than with the diuretic alone.Whether these effects on renin are important to thecontrol of blood pressure with this combination isstill a matter for further study. The sympathetic inhibiting drugs that are most potent in preventingrenin release are the ~-blockers and clonidine,followed by methyldopa and reserpine. Guanethidineis not very effective in decreasing plasma renin ac-

Drug Interactions with Antihypertensives 76
Days
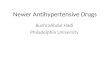
17~ I I Z ~ IDesipramine mg!day
Fig. 1. Effect of a tricyclic antidepressant on guanethidinecontrolled blood pressure. 1 to 2 days were required for interaction to become fully apparent (after Mitchell et . al., 1970).
1 2
than with the tricyclic antidepressants, and the interaction is therefore less profound (Stafford andFann, 1977). Additionally, the phenothiazines arefairly potent o-adrenoceptor blocking drugs at thesedoses and this effect tends to reduce blood pressureand mask the interaction with guanethidine. Otherdrugs which can interact with guanethidine and related compounds, presumably by inhibiting thenoradrenaline pump mechanism, include the tricyclicdrugs pizotifen, which is used as a migraineprophylactic (Bailey, 1976), and mazindol an anorexiant (Boakes, 1977).
A second undesirable interaction may occur at thesame site. Indirectly acting sympathomimetic aminessuch as amphetamine, ephedrine. pseudoephedrine,phenolpropanolamine. or phenylephrine compete sue-
tivity, and in fact in some circumstances,guanethidine increases plasma renin activity as itdecreases arter ial pressure (Ferguson et al., 1976).Bethanidine and debrisoquine are similar toguanethidine in this regard.
4.1 Interactions with Guanethidine and RelatedDrugs
Hazardous interactions with this group of drugscan be clinically important. The most thoroughlystudied have been with guanethidine and relatedguanidinium drugs bethanidine and debrisoquine(Stafford and Fann, 1977). These drugs must betransported into the adrenergic neuron to exert theireffect. The active transport mechanism that pumpsnoradrenaline (norepinephrine) mto the sympatheticnerve ending is also used to transport the basicguanidinium compounds such as guanethidine acrossthe cell membrane. Once in the neuron, guanethidineparalyses the neuron and also depletes the vesicles ofnoradrenaline. If the 'noradrenaline pump' is inhibited, guanethidine and related compounds cannotenter the neuron and therefore cannot exert an antihypertensive effect. The tricyclic antidepressants arepotent inhibitors of this pump and therefore interactwith guanethidine.
Expression of the loss of blood pressure control istime and drug-related. With guanethidine, severaldays are required before the effect is noticeable.However, with bethanidine the effect of the interaction is seen in a few hours . Re-establishment of control after the tricyclics are discontinued is prolongedto as much as 5 days (Mitchell et al., 1970; Mitchelland Oates, 1970). As shown in figure I, the interaction is significant and undesirable. Doxepin has a lessmarked effect on the noradrenaline pump mechanismand interaction with guanethidine only becomes significant with doses of doxepin of 200mg or moredaily (Pinder et al. 1977). Chlorpromazine can alsoinhibit the neuron pump at doses of greater than150mg/day. However, the degree of inhibition is less

Drug Interactions w ith Antihypertensives
cessfully with guanethidine for the uptake and storageprocess. Thus , concurrent use of these drugs also produces a therapeutic failure. Since indirect acting sympathomimetics are frequent ingredients of over thecounter preparations for cough, cold and hay fever,this type of interaction may easily occur unless patients are specifically warned of this possibility.Amphetamine-type anorexiants (except fenfluramine)should be avoided in weight reduction programmes inobese hypertensive subjects treated with guanethidineor related drugs .
4.2 Interactions with Clonidine
The only possible significant adverse interactionreported with clonidine is that with tricyclic antidepressants , specifically desipramine. The introduction of desipramine to a patient controlled withclonidine can result in a rise in pressure after I to 7days (Briant et al., 1973). The mechanisin of this interaction is unknown. Combination of clonidine withamitriptyline or imipramine did not prove a problem(Raftos et al., 1973).
4.3 Interactions with Propranolol and Other~-Adrenoceptor Blocking Drugs
Hazardous interactions occuring with propranololare, in reality, interactions of the drug with a disordered physiological environment. Because of the ~
adrenoceptor blockade produced by propranolol , ~
adrenoceptor agonists cannot have their effect at normal doses. Therefore, ifbronchodilation is essential inan asthmatic patient on propranolol, much moreisoprenaline (isoproterenol) or salbutamol, terbutalineetc than usual would be necessary. This adverse interaction is entirely predictable from pharmacologicalconsiderations and should be less of a problem with~-blockers that are relatively more selective for thecardiac ~I-receptor (e.g. metoprolol, atenolol ,acebutolol) than the ~2-receptors in lung and vascularsmooth muscle.
77
In a similar manner, blockade of ~-adrenoceptors
will alter the physiological response to hypoglycaemiasothat there is less patient awareness of the problem(Lloyd-Mostyn and Oram , 1975). The tachycardia,palpitations, tremor and feeling of anxiety that are theusual harbingers of hypoglycaemia are abolished bypropranolol, although the sweating remains. Thereare a few case reports of propranolol enhancing theeffects of hypoglycaemic agents, perhaps by reducingadrenergically-stimulated glycogenolysis (Kotler etal., 1966; MacKintosh, 1967). however , this effect ismuch less important than the fact that the adrenergicsymptoms of hypoglycaemia are blocked.
If the circulating levels of catecholamines are elevated, propranolol can produce hypertension thatresults from a-adrenergic vasoconstriction unopposedby any ~-adrenergic vasodilatation . This phenomenonhas been reported during drug-induced hypoglycaemia and during clonidine withdrawal, aswell as with pheochromocytoma (Bailey and Neale1976; Lloyd-Mostyn and Oram , 1975).
4.4 Interactions With Monoamine OxidaseInhibitors
Monoamine oxidase inhibitors such as pargylinewere introduced into the therapy of hypertensionwith the expectation that one of their more notableside-effects, hypotension, would prove useful. In present day therapeutics, they offer minimal usefulnessin an antihypertensive treatment plan. However,treatment of other disorders such as depressive illnessmay utilise them, and the physician should be awareof some of the major interactions that can occur.Moreover, the guanidinium adrenergic neuroneblocking compound debrisoquine possesses somemonoamine oxidase inhibitor activity and a 'cheese'interaction has been reported (Amery and Deloof,1970).
The hypertensive crisis that can follow ingestionof tyramine-rich foods (cheddars and gruyere cheesescontain relatively large amounts) and beverages(mainly chianti-type wines) is almost legendary and

Drug Interactions with Antihypertensives
results from release of large amounts ofcatecholamine into the circulation.
Another well publicised undesirable interactionwith a similar mechanism is that occurring withproprietary cough and cold remedies (Cuthbert et al.,1969) and with sympathomimetic-amine anorexiantsexcept fenfluramine (Simpson, 1973). Many of thecough and cold preparations contain phenylpropanolamine, phenylephrine, pseudoephedrine orephedrine and pose a real possibility of elevatingblood pressure precipitously.
Perhaps less well known but equally important adverse interactions have been reported with thesulphonylureas (Adnitt, 1968; Cooper and Ashcroft,1966) arid pethidine/meperidine (Vigran, 1964).Levodopa is a relatively recent addition to the alreadylengthy list of drugs that produce undesirable interactions with monoamine oxidase inhibitors (Hunter etal., 1970; Sourkes, 1971). In this instance, the postulated mechanism is an interference with the storageand release of dopamine and noradrenaline.
5. Interactions With Vasodilators
The vasodilators hydrallazine and prazosin, ofwhich hydrallazine is the prototype, have only recently begun to assume real importance in antihypertensive therapy because of a beneficial pharmacodynamic interaction.
When hydrallazine, a direct acting vasodilator,was first used, it was not felt to be very effectiveandit produced a high incidence of undesirable effectssuch as tachycardia, palpitations and precipitation ofangina. Only recently has it become evident that thephenomena of poor tolerance and lack of efficacywere both related to an increased sympathetic tonethat was reflexly stimulated by the vasodilatation.This sympathetic outflow worked against the antihypertensive effects of hydrallazine by increasing thecardiac output and stimulating renin release. The undesirable symptoms of palpitations and angina pectoris also were mediated by the sympathetic nervous
78
system. When hydrallazine is combined with a sympathetic inhibiting drug, usually propranolol, its antihypertensive efficacy is markedly enhanced and theside-effectsrelated to the sympathetic nervous systemdecreased. Prazosin exerts its vasodilator activity byblockade of post-synaptic o-adrenoceptors andbecause of this different mode of action to hydrallazine does not increase sympathetic tone. Its antihypertensive activity is also enhanced by combineduse with propranolol or other ~-blockers (Brogden etal., 1977). Addition of a diuretic to diminish thesodium retention associated with vasodilators completes the triad of a successful therapeutic interaction.
6. Conclusion
There are other interactions among the antihypertensive drugs that have not been discussed. In general,they are undesirable and include interactions of the'loop' diuretics with aminoglycoside antibiotics, longterm corticosteroid therapy with its attendant hypokalaemia potentiated by thiazide and 'loop'diuretics and many more described in various reviewsand books (e.g. Grahame-Smith , 1977; Koch-Weser,1975; Morrelli, 1976; Nies, 1975). However, wewished to emphasise that all drug interactions in antihypertensive therapy are not undesirable. The frequent use of multiple antihypertensive agents oftenresults in beneficial interactions that are predictablebased on an understanding of the pharmacology ofthe antihypertensive drugs. Therefore, of thenumerous permutations and combinations of interactions that are possible, we have presented those felt tobe most beneficial as well as those most clinically important adverse interactions. Rather than become enmeshed in a quagmire of infrequent and poorly understood interactions, an effort has been made to describe the best understood interactions. In this reviewit has been our intention to assist in the treatment ofhypertensive disease rather than frighten therapistsaway from the considerable benefit to be gained byusing multiple drug regimens.

Drug Interac tions with Antihypertensives
References
Adnitt, P.I.: Hypoglycemic action of monoamine oxidase inhibitor.;(MAOrs). Diabetes 17: 628-633 (\ 968).
Adverse Interactions. The Medical Letter 19: 5-12 (\ 977).Amery. A. and Deloof, W .: Cheese reaction during debrisoquine
treatment. Lancet 2: 613 ( I970).Bailey. R.R.: Antagonism of debrisoquine sulphate by pizotifen
(Sandomigran), New Zealand Medical Journal 83: 449 (I 976).Bailey. R.R. and Neale. TJ.: Rapid clonidine withdrawal with
blood pressure overshoot exaggerated by beta blockade. BritishMedical Journal I : 942-943 (\ 976).
Boakes, AJ .: Antagonism of bethanidine by mazindol. BritishJournal of Clinical Pharmacology 4: 486 (1977).
Briant. R.H.: Reid. J .L. and Dollery, C.T.: Interaction betweenclonidine and desipramine . British Medical Journal I: 522-523(\ 973).
Brogden. R.N.: Heel. R.C.: Speight. T.M. and Avery. G.S.:Prazosin. A review of its pharmacological properties andtherapeutic efficacy. Drugs 14: 163 (\ 977).
Cooper . A.S. and Ashcroft. G.: Potentiation of insulin hypoglycemia by M.A.O.1. antidepressant drugs. Lancet I:407-409 (1966).
Cuthbert. M.F.: Greenberg. M.P. and Morley. S.W .: Cough andcold remedies: a potential danger to patients on monoamineoxidase inhibitors. British Medical Journal I: 404-406 (1969).
Dustan, H.P.: Bravo. E.L. and Tarazi, R.C.: Volume dependentessential and steroid hypertension. American Journal of Cardiology 31: 606-614 (\ 973).
Dustan, H.P.: Tarazi , R.C. and Bravo. E.L.: Dependence of arterial pressure on intravascular volume in treated hypertens ivepatients. New England Journal of Medicine 286: 86 1-866((972).
Ferguson. R.K.: Rothenberg . RJ. and Nies, A.S.: Patient acceptance of guanethidine as therapy for mild to moderate hypertension. A comparison with reserpine. Circulation 54: 32-37(\ 976).
Grahame-Srnith, D.G.: Drug Interactions. (University Park Press.Baltimore 1977).
Hartshorn. E.A.: Food and drug interactions. Journal of theAmerican Dietetic Association 70: 15-19 (\ 977).
Hunter. K.R.: Boakes, EJ.: Laurence. D.R. and Stern. G.M.:Monoamine oxidase inhibitors and L-dopa. British MedicalJournal 3: 388 (197m.
Koch-Weser, J .: Drug interactions in cardiovascular therapy .American Heart Journal 90: 93-116 (\ 975).
79
Kotler. M.N.: Berman. L. and Rubenstein. A.H.: Hypoglycemiapotentiated by propranolol. Lancet 2: 1389-1390 (1966).
Lloyd-Mostyn. R.H. and Oram, S.: Modification by propranololof cardiovascular effects of induced hypoglycemia. Lancet I:1213-1215 (1975).
MacKintosh. T.F.: propranolol and hypoglycemia. Lancet I : 104(1967).
Mitchell. J .R.: Cavanaugh . J .H.: Arias. L. and Oates. J .A.:Guanethidine and related agents. III. Antagonism by drugswhich inhibit the norepinephrine pump in man. Journal ofClinical Investigation 49: 1596-1604 (197m .
Mitchell. J.R. and Oates. J.A.: Guanethidine and related agents. I.Mechanism of the selective blockade of adrenergic neuronsand its antagonism by drugs. Journal of Pharmacology andExperimental Therapeutics 172: 100-107 (\ 970).
Morrelli, H.F.: Drug interactions in hypertension: Advantageousand adverse. Hospital Formulary 213-216 (1976).
Nies, A.S.: Adverse reactions and interactions limiting the use ofantihypertensive drugs. American Journal of Medicine 58:495-503 (1975).
Nies, A.S.: Shand . D.G. and Branch. R.A.: Hemodynamic druginteractions: in Card iovascular Clinics 6: 43-53 (\ 974).
Nimmo. W .D.D.: Drugs. diseases and altered gastric emptying.Clinical Pharmacokineti cs I : 189 (\ 976).
Pinder . R.M.: Brogden. R.N.: Speight. T.M. and Avery. G.S.:Doxepin up-to-date: A review of its pharmacological properties and therapeutic efficacy with part icular reference todepression. Drugs 13: 161 (1977).
Raftos, J .: Bauer. G.E .: Lewis. R.G.: Stokes. G .S.: Mitchell. A.S.:Young. A.A. and Maclachlan. I.: Clonidine in severe hypertension. Medical Journal of Australia I: 786 ( I973).
Simpson . F.O.: Antihypertensive drug therapy. Drugs 6: 333(\ 973).
Sourkes, T.L.: Actions of levodopa and dopamine in the centralnervous system. Journ al of the American Medical Association218: 1909-1911 {\ 971l.
Stafford. J .R. and Fann , W .E.: Drug interactions withguanidinium antihypertensives. Drugs 13: 57-64 (\ 977).
Vigran, I.M.: Dangerous potentiation of meperidine hydrochlor ideby pargyline hydrochloride . Journ al of the American MedicalAssociation 187: 953-954 (\ 964).
Author's address: Dr James E. Crook. Division of ClinicalPharmacology. Department of Pharmacology. Vanderbilt University School of Medicine. Nashville. Tennessee 3 7232 (USA).