Embed Size (px)
Citation preview

Meeting Highlights
2004 © Ashley Publications Ltd ISSN 1472-8222 151
Ashley Publicationswww.ashley-pub.com
1. Introduction
2. Osteoarthritis
3. Identifying novel targets to
tackle inflammatory diseases
4. Assessing the development of
new therapies to target
cytokines and chemokines
5. Chemokines
6. Conclusion and expert opinion
Drug Discovery and Development for Inflammatory Diseases6 – 7 October 2003, Copenhagen, Denmark
Carl K Edwards IIIResearch Business Area Dermatology, USA; Schering AG/Berlex Biosciences, 2600 Hilltop Drive,
Richmond, CA 94804-0099, USA; The University of Colorado Health Sciences Center, School of
Medicine, Division of Infectious Diseases, 4200 Colorado Blvd, Denver, CO 80208, USA
Numerous recent investigations have pointed to a key role of the pro-inflam-matory, pleotropic cytokines TNF-α and IL-1 in host defence and inflamma-tory disease processes. TNF and IL-1 overexpression has been found in diseasetarget tissue and in the circulation of patients with acute and chronic inflam-matory diseases, and it was suggested early on in this field of basic medicalresearch that TNF-α and IL-1 were crucial in these diseases. Over the last10 years, several approaches to inhibit TNF-α and, in one case, IL-1 activity,have been developed by the biotechnology and pharmaceutical industries.These include neutralising antibodies to TNF-α as well as soluble TNF-α recep-tors with characteristic properties designed to bind the 17 kDa solubletrimeric TNF-α and the 26 kDa membrane-bound form of TNF-α. Clinical trialshave demonstrated significant effects with these agents and it is likely thatblocking TNF-α will become an important standard therapeutic option for cli-nicians. The data available from these trials contribute to the further under-standing of inflammation by demonstrating the major role of thesecytokines. This research and clinical background have provided the basis for avariety of lectures on novel drug discovery targets, the current status of previ-ously identified targets and technologies to develop new therapeutics ininflammation. At this meeting, emphasis was placed upon drug targets andtheir validation in animal models and early stage clinical trials.
Keywords: IL-1, inflammation, osteoarthritis (OA), pro-inflammatory cytokines, psoriasis,rheumatoid arthritis (RA), TNF-α
Expert Opin. Ther. Targets (2004) 8(2):151-163
1. Introduction
This symposium focused on Drug Discovery and Development for InflammatoryDiseases, held on October 6 – 7 2003 in Copenhagen, Denmark, and included avariety of lectures on novel targets, the current status of previously identified targetsand technologies to develop new therapeutics in inflammation. Major emphasis wasplaced upon drug targets and their validation. The meeting was chaired by D Heine-gard (University of Lund, Sweden) and M Karow (Regeneron Pharmaceuticals, Inc.,USA) and was attended by approximately 40 delegates. Most of the delegates werefrom the biotechnology and/or pharmaceutical industry. The event proved useful forthose requiring information on the frontiers, challenges, latest results and new hopesin the development of anti-inflammatory agents for a number of acute and chronicdiseases, including rheumatoid arthritis (RA), osteoarthritis (OA), psoriasis andmultiple sclerosis (MS).
For reprint orders, please contact:[email protected]

Drug Discovery and Development for Inflammatory Diseases
152 Expert Opin. Ther. Targets (2004) 8(2)
2. Osteoarthritis
Heinegard and D Walsh (University of Nottingham, UK)reviewed OA from a clinical–mechanistic angle. After a shortintroduction by Heinegard, Walsh followed with a very inter-esting overview discussion, ‘Should osteoarthritis be classified asan inflammatory disease’. OA is a cartilage disease with inflam-mation and a high incidence of angiogenesis. It has a high prev-alence in the general population (nearly 20 million peopleworldwide and growing) and, consequently, a significant medi-cal need, with only pain-killing drugs as partial remedies forsymptom control, high spending per capita on complementarymedicines and often the need for total joint replacement. Cur-rent therapies alleviate symptoms but are unable to cure or evenmodify the progression of the disease. Traditional views of OAare as a mechanical problem or ‘wear and tear’ arthritis. Thisalone cannot explain the high degree of heritability, and bio-chemical and cellular abnormalities associated with the disease.It is increasingly recognised that inflammation is a commonfeature of this disease, associated with the severity and rapidprogression of joint damage. Different inflammatory mecha-nisms distinguish OA and RA, whereas other components ofchronic inflammation including angiogenesis may be commonto both diseases. Anti-inflammatory therapies are more effectivethan simple analgesics for symptom control in OA. The efficacyof anti-inflammatory strategies in disease modification is onlyrecently receiving attention. The first pharmaceutical agent tosubstantially modify disease progression in OA will revolution-ise the treatment of musculoskeletal disease. Targets presentedfor the disease included C-reactive protein to decrease the ele-vated acute phase response in OA, as well as antiangiogenesisfactors to prevent ossification. Collagen fibrillogenesis was iden-tified as a deficient process, with cartilage oligomeric matrixprotein (COMP) as a stimulatory target. Data were presentedshowing that a matrix metalloproteinase, MMP-13, preventsexcessive cleavage of the collagen lattice. Inhibitors of MMPwere proposed as drugs with potential for disease-modifyingproperties; no structures were revealed. A workable assayrequires explant culture. Progress in monitoring disease progres-sion includes a combination of classical imaging with X-raysand clinical grading with markers such as COMP. This combi-nation technology may facilitate assessment of the clinical effectof future disease-modifying drugs earlier than the current targetof 2 years.
3. Identifying novel targets to tackle inflammatory diseases
3.1 PimecrolimusA Stuetz (Novartis Institute for Biomedical Research, Aus-tria), provided an excellent overview of immunosuppressivecompounds currently being developed and marketed byNovartis. In the seminar entitled ‘Increasing the therapeuticwindow within calcineurin inhibitors: therapeutic options fortreatment of skin diseases and other chronic inflammatory
conditions’, Stuetz provided a detailed discussion on themechanism of action of pimecrolimus. Pimecrolimus is asemisynthetic derivative of the macrocyclic natural productascomycin. Its discovery was the result of an extensive inter-disciplinary research effort to identify a compound that selec-tively targeted inflammation with minimal impairment oflocal and systemic immunosurveillance [1]. More than400 novel ascomycin derivatives have been synthesised, char-acterised, and structure–activity relationships determined,and pimecrolimus was selected for development based on itsfavourable pharmacology and safety profile. Pimecrolimusbinds to macrophilin-12 and inhibits calcineurin and thetranscription and synthesis of T-helper (TH)1- and 2-typecytokines in T cells. In contrast to corticosteroids, pime-crolimus has a cell-selective mode of action, exerting (e.g., noeffect) on Langerhans/dendritic cells, which have a centralfunction in the (skin-associated) immune system. Topicaltreatment with pimecrolimus does not induce skin atrophy incontrast to corticosteroids. Pimecrolimus does not permeateskin to the same extent as corticosteroids and tacrolimus,indicating a lower potential for systemic side effects after top-ical application. Based on their shared mode of action, thepharmacological profiles of the calcineurin inhibitors pime-crolimus, tacrolimus and cyclosporin A are expected to besimilar. Comparative pharmacology studies, however,revealed major differences. In allergic contact dermatitis(ACD) in mice, pimecrolimus only inhibited the elicitationbut not the sensitisation phase, in contrast to cyclosporin Aand tacrolimus. Oral pimecrolimus demonstrated superiorefficacy in rat models of ACD but much less activity in ratmodels of systemic immunosuppression (Figure 1). Further-more, oral pimecrolimus protected severe combined immun-odeficient (SCID) mice from developing T cell-inducedinflammatory bowel disease (IBD) without systemic immu-nosuppression, indicating therapeutic potential in otherchronic inflammatory conditions also. Multi-centre studieshave since proved that pimecrolimus cream 1% (Elidel®,Novartis) is highly effective and safe in atopic dermatitis(AD) patients, suitable for the short-term treatment andlong-term management of AD in adults, children and babiesas young as 3 months [2]. Phase II studies in psoriasis patientsfor up to 3 months’ treatment revealed oral pimecrolimus tobe highly effective and safe. Pharmacogenomic analysis ofblood samples showed downregulation of gene expressionassociated with leukocyte activation/proliferation, lym-phocyte chemotaxis and trafficking as well as inflammationbut no changes in gene expression that might be linked withdrug-related side effects.
3.2 Synthetic phosphorothioate-stabilised oligodeoxynucleotides (CpG ODNs)J Vollmer (Coley Pharmaceutical Group, Germany) thengave a seminar entitled ‘Activating Toll-Like Receptor 9 withCpG DNA’. Upon microbial infection, the host has tomount a multiplicity of immune responses that target the

Edwards III
Expert Opin. Ther. Targets (2004) 8(2) 153
invading pathogen. This is achieved in part by the use of par-ticular receptors expressed differentially on mammalianinnate immune cells, the Toll-like receptors (TLRs). Thepathogen structures that are selectively recognised by TLR9in bacterial or viral DNA are deoxycytidyl–deoxyguanosin(CpG) dinucleotides in specific sequence contexts(CpG motifs). The stimulatory activity of pathogen DNAcan be mimicked by short synthetic proprietary phospho-rothioate-stabilised oligodeoxynucleotides (CpG ODNs)containing such motifs that are being developed byColey Pharmaceutical Group. The TLR9-mediated stimula-tion of the vertebrate innate immune system, and subse-quently of the adaptive immune system (Figure 2), allows theuse of TLR9 agonists as highly effective vaccine adjuvants forinfectious diseases or as stand-alone therapy and in combina-tion with other therapies in cancer or asthma and allergy.Three CpG ODN classes have been described so far: the A-,B- and C-classes with distinct immune stimulatory activities.Clinical vaccine trials in normal human volunteers and inimmunocompromised HIV-infected patients showed thatCpG ODNs could strongly enhance vaccination strategies.The addition of a B-class CpG ODN (VaxImmune™) to acommercial hepatitis B vaccine (Engerix-B®, GlaxoSmith-Kline) markedly increased rates of seroconversion andinduced significantly higher antigen-specific antibody titres.Encouraging results for the treatment of human tumourscome from small Phase I tumour vaccine trials that suggest
activity of the B-Class CpG ODN ProMuneTM. ProMuneTM
is also being evaluated in human Phase I and II clinical trialsas a monotherapy or in combination with chemotherapy forthe treatment of patients with different cancers. So far,CpG ODNs have generally been well-tolerated and the stud-ies suggest that ProMuneTM has antitumour activity in cancerpatients. CpG ODNs, therefore, may represent targetedimmune modulator drugs with broad potential applicationsin cancer, infectious diseases, and asthma and allergy.
3.3 Protein kinase inhibitorsA Lewis (Celgene Corp., USA) discussed the therapeuticpotential for inhibitors of this (stress-induced) mitogen-acti-vated protein kinase family class of compounds. In his semi-nar, ‘The JNK Pathway and its Role in InflammatoryDiseases’, Lewis showed selectivity of Celgene compoundscompared with a series of screening compounds and reviewedthe role of the Jun N-terminal kinase (JNK) pathway andthese agents in inflammatory diseases [3]. JNK plays an impor-tant role in the transcription of several inflammatorycytokines and degradative enzymes in apoptosis, mRNA sta-bility (IL-2, -3 and TNF-α) as well as in receptor signalling(recently, it has been demonstrated to phosphorylate insulinreceptor subtype [IRS]). The first selective JNK inhibitor,SP-60012, has more recently been shown to possess inhibi-tory activity against other kinases. However, additional panJNK inhibitors are now available that are effective in a variety
Figure 1. Pimecrolimus is as effective as or superior to tacrolimus in skin inflammation, but less immunosuppressive.ACD: Allergic contact dermatitis.
0.0
0.5
1.0
1.5
2.0
2.5
Graft vs host
(s.c.)
Kidney transplant
(oral)
Antibody formation
(s.c.)
ACD rat
(oral)
ACD mouse
(s.c., oral)
Pim
ecro
limus
:tacr
olim
us
1/66 1/15
Immunosuppression models/rat
Relative potency, pimecrolimus:tacrolimus
Tacrolimus
Skin inflammation models
1/48
2
1

Drug Discovery and Development for Inflammatory Diseases
154 Expert Opin. Ther. Targets (2004) 8(2)
of animal models of disease including rat adjuvant-inducedarthritis, mouse collagen arthritis and acute and chronic aller-gic asthma models in mice and rats. In the latter, JNK inhibi-tion reduces cellular influx into the airways and lungs, inhibitscytokine production (IL-1, -4, -13, TNF-α, RANTES [regu-lated upon activation, normal T cell-expressed and secreted])as well as reducing smooth muscle cell proliferation and air-way hyper-reactivity. CC-401 has entered clinical trials andhas shown activity in rat warm liver ischaemia–reperfusioninjury as well as liver transplant. It appears to work most effi-ciently when administered to both a donor and as part of theorgan preservative solution. CC-401 is well-tolerated withminor adverse effects in a single dose study in volunteers.Additional efforts are being made to develop JNK isoform-selective compounds. It was suggested that JNK1-selectivedrugs might be useful to treat OA and diabetes. JNK inhibi-tors effectively control diabetes (plasma glucose, insulin
responsiveness and body weight) in the db/db mouse as wellas preserve β cell islet cells. Inhibition of the JNK pathwayappears to have great potential in a variety of diseases and livesup to its reputation as the ‘universal target’.
3.4 Redistribution technology: cell-based p38–MAPK and MAPKAP-kinase 2 translocation modulatorsAnother technology-driven presentation was given byL Pagliaro (VP Discovery Projects, BioImage A/S, Denmark),who showed applicability of redistribution technology foridentification of nucleus translocation inhibitors forMAPKAP-kinase 2 (MK2) in the TNF-α signalling cascade.The seminar entitled ‘Cell-Based p38–MAPK PathwayScreening for anti-TNF-α Drugs: Identification of KinaseInhibitors and MAPKAP-kinase 2 Translocation Modulators’,emphasised that MK2 is an important intracellular regulatorof the production of cytokines, such as TNF-α , IL-6 and
TLR9
T cellIFN-α
TNF-α
IL-12
IFN-γ
IP-10
Other cytokines/chemokines Increased
MHC
+
+
+
+
+
pDC
NK cell,
monocytesTLR9
agonist
CTL
CpG ODN
Adaptive immunityInnate immunity
B cell
Increased Ab secretion
Increased sensitivity to antigen
IL-6
IL-10+
+
TLR9
CpG ODN
Figure 2. Scheme of TLR9-mediated immune stimulatory effects. Among all different TLR stimuli, the most specific pathway toinduce a TH1 innate immune response appears to be via TLR9. Only human B cells and pDCs directly recognise CpG ODN; other immunecells lacking TLR9 are indirectly activated. Within minutes upon exposure to CpG ODN, specific signalling pathways are stimulated,leading to a multiplicity of secondary effects that link the innate to an adaptive immune response.CpG ODN: Oligodeoxynucleotide; CTL: Cytotoxic T lymphocyte; IP: Inducible protein; MHC: Major histocompatibility complex; NK: Natural killer; pDC: Plasmacytoiddendritic cell; TLR: Toll-like receptor.

Edwards III
Expert Opin. Ther. Targets (2004) 8(2) 155
IFN-γ, that are involved in many acute and chronic inflam-matory diseases, for example, RA and IBD. MK2 is activatedthrough the p38–MAPK pathway and its stimulatory effecton cytokine production depends on translocation of MK2from the nucleus to the cytoplasm (Figure 3). BioImage Redis-tribution® assays use the translocation of a green fluorescentprotein (GFP)-tagged target, such as MK2, as the primaryread-out for high-throughput screens. BioImage has devel-oped a high-throughput MK2 Redistribution® assay and hasused it to screen a diverse small-molecule library of approxi-mately 250,000 compounds. The hit compounds were coun-ter-screened in a panel of redistribution, functional andbiochemical assays to determine potencies, selectivities andmodes of action. Both MK2 nuclear export and p38–MAPKpathway inhibitors were identified. Selected classes are cur-rently being further investigated and are progressing to chem-ical optimisation. The programme identified a selectivetranslocation modulator for the kinase, designatedSCR-0265096, which displayed EC50 (effective concentrationfor half-maximum response) values of 1.6 µM in a redistribu-tion assay and 0.3 µM for p38 phosphorylation, with a 5- to25-fold lower potency in assays for other kinases (Figure 4).This lead will be further characterised and optimised.
3.5 Transcription factors: NF-κBC Korstanje (Biological Development Department,Yamanouchi Europe, The Netherlands) gave a seminar enti-tled ‘Is NF-κB Too pleotropic to Target with Drugs?’. Kor-stanje focused on the role of NF-κB in the activation cascade
of inflammatory cells and mediators and its role in cellularhousekeeping versus constitutive activation in pathologicalprocesses [4]. The crucial position of NF-κB in the TNF-αsignalling cascade (e.g., in polymorphonuclear cells [PMNCs]and monocytes), where inhibitors of the NF-κB complex areexpected to augment the apoptosis-promoting effect ofTNF-α (via caspases) by inhibiting the antiapoptotic pathwaythrough cellular inhibitors of apoptosis (cIAPs), was reportedas an important concept for diseases that depend heavily onoveractivation of the inflammatory and hyperproliferativearms of TNF-α. NF-κB activation is elementary to immuneand inflammatory reactions, anti- and pro-apoptotic proc-esses and cell cycle regulation. NF-κB is a family of transcrip-tion factors that is activated by a broad range of extracellularsignals that use various pathways for signal transduction.NF-κB is primarily found in the cytoplasm as an inactiveform. Activation requires phosphorylation, leading to uncou-pling of the complex and translocation of NF-κB to thenucleus, where transcription can be initiated. The role ofNF-κB in the activation cascade of inflammatory cells andmediators and on its role in cellular housekeeping versus con-stitutive activation in pathological processes was the focus ofthis lecture. In this line of thinking, the proof-of-concept(POC) in OA and RA for various principles to inhibit theactivation of the NF-κB–IκB complex was discussed. In vivoPOC has been published for inhibitor of κB kinase (IKK)βinhibitors such as SPC-839 (Celgene, Inc., USA),BMS-345541 (Bristol-Myers Squibb, USA) and the acan-thoic acid derivative NPI-1302a-3 (Nereus Pharmaceuticals,
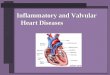
Figure 3. MK2 activation and nuclear export stimulate TNF-α biosynthesis. Activated p38 phosphorylates MK2 in the nucleus ofthe cell. Activated MK2 then translocates to the cytoplasm via a Crm1 transport protein-dependent mechanism. In the cytoplasm, MK2phosphorylates a group of proteins called ARE-BP that are bound to cytokine mRNA molecules and inhibit their translation.Phosphorylation inactivates the repressors, and synthesis of TNF-α can commence.ARE-BP: AU-rich element-binding protein; Crm1: Crem 1; LPS: Lipopolysaccharide; MK2: MAPKAP-kinase 2; MKK: MAPK kinase.
Cytoplasm
Nucleus
Stress signals, e.g., pro-inflammatorycytokines and LPS
MKK3/6
p38
p38-p
MK2
MK2-p
TNF-α
Crm1
Crm1
TNF-αmRNA
ARE-BP
-p
-p

Drug Discovery and Development for Inflammatory Diseases
156 Expert Opin. Ther. Targets (2004) 8(2)
USA), as well as for IκBδN, a deletion mutant of IκB (MountSinai School of Medicine, USA) and an oligo NF-κBsequence decoy (University of Naples, Italy). In addition,overactivation of T cells via the CD28 T cell costimulationpathway is considered a valid target for NF-κB inhibitors,whilst POC is given in the literature for IKKβ inhibitors inin vivo myeloma and lymphoma models.
3.6 Cellular brailleM Sjöberg (Karo Bio AB, Sweden) gave an excellent seminaron the use of new drug discovery technology to elucidatemore potent glucocorticoid agents that would have less severeside effects. This seminar was entitled ‘A Novel Approach toan Old Concept: Identification of Dissociated Glucocorti-coids for Inflammatory Diseases’. Glucocorticoid receptor(GR) ligands are the most potent anti-inflammatory agentsknown but have a number of side effects that limit their use.With new insights into the mechanism of GR action, it is pos-sible to develop potent anti-inflammatory glucocorticoidsdevoid of the most serious side effects. Karo Bio’s technologybase, including receptor–ligand three-dimensional determina-tion, chemistry synthesis and design and Cellular Braille™technology, is well suited to addressing these issues. Throughthe use of BioKey® peptide probes that can sense
ligand-induced surface changes, it is possible to map surfacesof the receptor that are involved in different mechanisms oftarget gene regulation (Figure 5). Karo Bio is involved in thedesign and synthesis of novel compounds that may potentiallybecome important anti-inflammatory agents with animproved therapeutic index. Peptides have been identifiedthat differentially bind to GR in the presence of different lig-ands. Use of these peptides in mammalian two-hybrid assays(Cellular Braille) has allowed compounds (steroidal and non-steroidal) with known characteristics to be separated into fourmajor classes: agonists, antagonists, dissociated ligands and‘borderline’ compounds. The major classes were further sub-divided into multiple subclasses. Sjöberg and her group arenow in the process of selecting compounds from subclasses ofdissociated GR agonists for further characterisation andin vivo efficacy studies. With this information, the GR Cellu-lar Braille assay will help to predict in vitro as well as in vivobiological responses and will therefore facilitate identificationand optimisation of lead and back-up compounds withdesired characteristics. It is possible to rapidly screen largenumbers of compounds using Cellular Braille profiling toidentify novel GR agonists, antagonists and selectiveGR modulators or to determine the GR-related characteristicsof subclasses of compounds. Finally, given a novel compound
Figure 4. Profile of a nuclear export inhibitor. This compound class was identified in the MK2 redistribution screen (black diamonds)and was shown to inhibit the LPS-induced TNF-α release from peripheral blood mononuclear cells (open circles) by affecting theCrm1-dependent nuclear export of MK2. The compound does not affect the activation (open diamonds) or the activity (black asterisks) ofthe upstream kinase p38.Crm1: Crem 1; LPS: Lipopolysaccharide; MK2: MAPKAP-kinase 2.
SCR-0261375
-7 -6 -5 -4-25
0
25
50
75
100
125
150
p-p38
TNF-αMK2
p38a kinase
Log (concentration) (M)
Inhi
bitio
n (%
)

Edwards III
Expert Opin. Ther. Targets (2004) 8(2) 157
with desirable in vivo properties, Karo Bio can identify newBioKey probes that recognise the induced conformation ofGRs for use in screening for comparable compounds.
4. Assessing the development of new therapies to target cytokines and chemokines
After a brief introduction on the status of new biological dis-ease modifiers being brought through late-stage clinicaldevelopment (M Karow, Regeneron Pharmaceuticals, USA),M Braddock (Associate Director, Respiratory and Inflamma-tion Research Area, AstraZeneca, UK) gave an in-depthreview of the relevance of animal models to drug discoveryand drug development, entitled ‘Linking Animal Modelswith Translational Science in Inflammatory Disease’. Effec-tive drug discovery is critically dependent on the design ofsafe clinical trials completed to agreeable end points for theclinicians. The understanding of inflammatory disease of thejoint and lung has been helped by the development of acuteand chronic animal models that serve to assist in the deci-sion-making process. In big Pharma, ‘picking the winner’ outof large screening series requires a sophisticated iterative proc-ess of going through screening tools, disease characteristicsand animal models with translational value. Carefullyselected human tissue samples and adequate histopathology
support play an important role in this process [5]. The use ofwell-defined animal models and in vitro explant systems,whilst knowing limitations, helps in selecting and developingpotential drug candidates.
K Asadullah (Schering AG, Germany) gave an eloquentoverview on the role of cytokines in inflammatory cutaneousdiseases entitled, ‘Cytokine application and neutralisation:novel therapeutic approaches for inflammatory cutaneousdiseases’. Cytokines play a pivotal role in the initiation, prop-agation and regulation of immunological responses. They areof utmost importance in the pathogenesis of several diseases.Using cytokines or cytokine antagonists as immunomodula-tors exhibiting either immunosuppressive or immunostimu-latory effects is a rapidly emerging field and is already addingor is about to add significantly to the therapeutic arsenal formalignant and inflammatory disease. Several cytokines arecurrently in clinical development for inflammatory derma-toses. IFN-γ and IL-10 have been used in AD and IL-4, -10and -11 have been used in psoriasis. Moreover, neutralisingIL-8, -12/-23, -18 and TNF is currently being tested in pso-riasis. All in all, the clinical effects are heterogeneous and afew approaches may finally lead to novel approved therapeu-tic options. All observations in these clinical trials, however,are promoting our knowledge of the pathophysiology of theskin diseases targeted. Of the new therapeutics for psoriasis,
Figure 5. Cellular Braille™ Technology in the drug discovery process.GR: Glucocorticoid receptor.
Cellular BrailleCellular Braille™™ technology technology
Ligand-induced surface conformations
Criteria for moving forward:Dissociated BrailleTM Fingerprint
LigandLigand binding binding
Criteria for moving forward:GR affinity and GR specificity
Target indication-related screensTarget indication-related screens
Select compounds for furthercharacterisation and
in vivo efficacy studies

Drug Discovery and Development for Inflammatory Diseases
158 Expert Opin. Ther. Targets (2004) 8(2)
an anti-TNF-α antibody (infliximab) is somewhat moreeffective than the soluble TNF receptor drug etanercept insevere psoriasis, with PASI (Psoriasis Area-and-SeverityIndex) score improvements of ∼ 80 and 75%, respectively.Recently, efficacy was shown for IL-4 in psoriasis. Examplesof failures were additionally provided, such as the use ofIL-8 antagonists in psoriasis and IL-10 in AD and psoriasis.However, a more recent long-term evaluation of IL-10 inpsoriasis indicates that population differences may exist forthe efficacy of the drug (Figure 6) [6,7]. The current status ofcytokine and anticytokine therapy for psoriasis and AD wasdiscussed in great detail.
Karow then gave an exciting overview of a new technol-ogy that appears efficacious in early clinical trials, ‘CytokineTraps: High Affinity Inhibitors of Cytokine Activity’.Cytokines can be blocked by the use of soluble receptors;however, the use of this approach for cytokines such as IL-1,-4, -6 and -13 that use multi-component receptor systems islimited because monomeric soluble receptors generallyexhibit low affinity of function as agonists [8,9]. Karowdescribed a generally applicable method to create very highaffinity blockers called ‘cytokine traps’ that consist of humanheteromeric receptor elements linked to Fc to create potentsoluble inhibitors of cytokine function. Traps potently blockcytokines in vitro and in vivo and represent substantialadvances in creating novel therapeutic candidates forcytokine-driven diseases.
In a general overview of the status of anti-TNF-α therapeu-tics in the biopharmaceutical industry, ‘Assessing the Progressof Small Molecule Inhibitors to Modulate Cytokines’,C Edwards (Schering AG/Berlex Biosciences, USA) providednumerous examples of the diverse approaches that facilitatethe identification of the drugs of today and tomorrow(Figure 7). TNF antibody drugs, TNF-α receptor-releasingenzyme (TRRE) and p38 kinase inhibition were briefly dis-cussed. Various methods that affected distinct parts of theNF-κB transcription pathway had a differential impact on thesynthesis of TNF-α, IL-1β, IFN-γ and IL-8 following activa-tion in vitro or in animal models with LPS. The PEGylatedform of soluble TNF receptor 1 (TNF-RI) (Pegsunercept,Amgen, Inc.) is in a Phase II trial for RA (doses of 400 and800 µg/kg). Week 12 results showed up to 50% improvementin subjective ratings for joint tenderness and swelling, as wellas pain reduction [10]. In another Phase II trial, the drug hadsimilar efficacy to etanercept administered twice-weekly. POCstudies for OA and RA for various principles to inhibit activa-tion of the NF-κB–IκB complex were discussed. Edwardsreviewed POC for targets upstream of NF-κB, such asNF-κB-inducing kinase (NIK), IKK and approaches toinhibit NF-κB–IκB dissociation. NIK inhibition was dis-cussed as a therapeutic candidate for RA and systemic lupuserythematosus (SLE), as well as B cell lymphoma. In addition,a histone deacetylase inhibitor lead compound, suberoylani-lide hydroxamic acid (SAHA, Aton Pharma, Inc.), induced
Figure 6. Immunological dysbalance in psoriasis.APC: Antigen-presenting cell; TH: T-helper.
IL-12IL-18
TNF-α, IL-1, IL-6, IL-8
TH2IL-4, IL-5, IL-10
IL-10
APC
TH cell
TH1IFN-γ, IL-2

Edwards III
Expert Opin. Ther. Targets (2004) 8(2) 159
significant reduction of IL-1, -6 and IFN-γ upon LPS activa-tion in mice and an antiproliferative effect in vitro. Therefore,there is ample evidence supporting the use of NF-κB as a drugtarget for inflammatory disease.
The topic of clinical efficacy of newer therapeutics andstrategies for dermatological use was further addressed in apresentation by G Grütz (Institute of Medical Immunology,Humboldt-Charite University of Berlin) entitled, ‘ExpressionProfiling of IL-10 Regulated Genes: A way for Identificationof New Immunosuppressive Agents?’. In the case of IFN-γ,too low a response resulted in justifying the inconvenience ofsubcutaneous injections and high costs. IL-10 is a majorimmunosuppressive cytokine that has been used in clinical tri-als to treat inflammatory diseases. Among those, psoriasispatients showed the best improvement. However, the molecu-lar mechanism of IL-10 action is poorly understood. To gaininsight into the molecular effects of IL-10, Grütz and his teamat the Charite in Berlin performed a gene expression profilingapproach comparing in vitro IL-10-treated monocytes versusnon-treated monocytes. In addition, this group analysed geneexpression changes during IL-10 therapy in psoriatic patients.The data indicated that a high number of IL-10-inducedgenes are related to a clearance of pathogens and that thechemokine profile shifts towards one that favours TH2 devel-opment [13]. This group then tested IL-10-regulated candidategenes that have been described by others to be responsible forthe IL-10 inhibition on LPS-induced TNF-α release. The
haem oxygenase (HO)-1 induction in human monocytes ismoderate and rather late. Irreversible inhibition by zinc pro-toporphyrin (ZnPP) does not abrogate the IL-10 inhibitoryeffect. The adenoviral overexpression of suppressor ofcytokine signalling (SOCS)-3 in primary human monocytesdid not affect LPS-induced TNF-α production – a result thathas now been confirmed by others with gene targetingapproaches. Adenoviral overexpression of the stronglyIL-10-induced AP-1 inhibitor, B-ATF, did not mediate aninhibitory effect on TNF-α and IL-6 release. Since this groupcould not demonstrate a strong inhibitory effect onLPS-induced signalling or TNF mRNA induction, they arenow focusing on identifying genes that influence post-tran-scriptional regulation of TNF-α production.
5. Chemokines
R Horuk (Department of Immunology, Berlex Biosciences,USA) gave an excellent updated chemokine presentation enti-tled ‘Chemokine Receptor Antagonists: Promising New Tar-gets’. Discovered in the 1980s, the chemokine superfamilycurrently has 43 human members, making it the target subsetof cytokines. Members are defined by conserved sequencesand a common three-dimensional fold and can be dividedinto two major functional groups – homeostatic and inflam-matory – depending on whether they are produced constitu-tively and thereby control basal lymphocyte trafficking or
p75 receptor
p55 TNFR
p55 TNFRPegsunercept
Onercept
Etanercept
Hinge
B. TNF receptors
Infliximab
AdalimumabD2E7(humanised)
CDP571(human)
Made by phagedisplay fromhuman components
Hypervariable regionsgrafted
Mouse Fv
Human Fc
A. Anti-TNF monoclonal antibodies
Figure 7. Structure of TNF inhibitors currently being tested in the clinic.

Drug Discovery and Development for Inflammatory Diseases
160 Expert Opin. Ther. Targets (2004) 8(2)
whether they must be induced, for example, by pathogens orinjury and thereby control deployment of effector leukocytesin emergencies. These classical functions, described in detailin the 1990s, have been repeatedly validated in vivo usinggenetically and immunologically manipulated animals and arestill thought to be the main activities of chemokines. Horukthen described an antagonist approach for the humanCCR1 chemokine receptor with a novel set of antagonists, the4-hydroxypiperidines, which were discovered by high-throughput screening of human CCR1 and then subsequentlyoptimised. These and other analogues of the lead template,BX-510, which have major differences in potency for humanand mouse CCR1, were reviewed as well as animal model dataefficacy in various models used for MS (Figure 8) [14].
Biomarkers that support outcome predictors are currentlythe focus of clinical drug development research, and the FDAclosely monitors progress in this field. This topic, ‘From Soupto Nuts: A Comprehensive Strategy for Biomarkers in DrugDevelopment’, was discussed by B Edmonds (Enabling Tech-nologies, Lilly Research Laboratories, USA), who additionallypresented at the adjacent IBC symposium on Biomarkers.Edmunds advocated the use of biomarkers early on in drugdevelopment and surrogate end points for mechanism ofaction support and guidance into new indications. For this, amultiplexer’s toolbox is required with microscale technologyto facilitate the performance of multiple assays in small
volume samples of blood and urine. Powerful bioinformaticsare required for data mining and pattern recognition. A majorchallenge is the validation of new technologies. Several exam-ples of new drug development with the use of multiplebiomarkers in a Phase III setting were provided.
In the last seminar of the conference, S Gilman (Millen-nium Pharmaceuticals, USA) provided an excellent review ofthe chemokine therapeutics programme at Millennium andthoughtfully described the real pragmatic challenges in dis-covering small-molecule antagonists to these G-protein-cou-pled receptor (GPCR) proteins. His talk was entitled,‘Discovery and Development of Novel Chemokine Antago-nists: Opportunities and Challenges’. Many Pharmaceuticalcompanies have invested much time and effort in this areaand, to date, the payoff for this investment has not been real-ised. However, Millennium is continuing this research and themost recent data suggest that second-generation antagonistsfor some human chemokine receptors have real promise.
6. Conclusion and expert opinion
With the use of anti-TNF-based therapies for the treatment ofinflammatory diseases, there is little question that TNF-αplays an important role in their pathogenesis. However, pro-inflammatory cytokines such as IL-1 and TNF-α did notevolve to harm the host but rather evolved as beneficial to the
Figure 8. The CCR1 antagonist is efficacious in a rat EAE model of MS.CCR: CC Chemokine receptor; EAE: Experimental autoimmune encephalomyelitis; MS: Multiple sclerosis.
-0.5
0
0.5
1
1.5
2
2.5
3
3.5
0 5 10 15 20 25
Vehicle
5 mg/kg
20 mg/kg
50 mg/kg
Ave
rage
clin
ical
sco
re
Time (days)

Edwards III
Expert Opin. Ther. Targets (2004) 8(2) 161
host. Other cytokines such as IL-18 and -15, which also play arole in autoimmune diseases, similarly evolved as beneficial tothe host, particularly in terms of host defence to infection.The use of anticytokine therapies has, in fact, revealed theimportance of some cytokines to host defence in humans. Thelevel of risk to the host, however, remains controversialbecause of the absence of required data:
• What is the risk of infection in patients with psoriasistreated with immunosuppressive agents such as methotrex-ate (MTX) without anti-TNF-α-based therapies?
• How many patient years of therapy are used to calculatethe denominator?
• What is the true number of the numerator when reportinginfection is voluntary?
In the case of infliximab, a single injection of the antibody iscarried forward and added to the database for a number ofpatient years of treatment, whereas this is not the methodused to calculate the database for the IL-1 receptor antagonist(Anakinra) or etanercept.
In general, a host challenged with an infection musters theassistance of these cytokines in order to prevent the microbefrom spreading and to eliminate the infection by microbio-cidal mechanisms. For non-intracellular bacteria, the effectorcell is the phagocyte, most notably the neutrophil. These cellshave the machinery to engulf the organism and kill it in thephagolysosome. Gram-positive bacteria such as Streptococciand Staphylococci are examples of neutrophil and cell adhesionmolecule-dependent host defence. In the case of macrophageintracellular microorganisms, the killing mechanism of theinfected macrophage involves IFN-γ and nitric oxide (NO)production. However, obligate intracellular organisms such asMycobacterium tuberculosis, Listeria, Histoplasma and Salmo-nella can survive and replicate inside the macrophage byusurping killing. Most notably, cytokines such as TNF-α andIFN-γ increase the killing mechanisms and a balance isachieved whereby a microorganism such as M. tuberculosis cansurvive inside a macrophage, but further spread and overt dis-ease are kept to a minimum by a competent immune system.Reducing TNF-α activity impairs the host’s mechanisms ofkilling intracellular organisms by reducing the synergism ofTNF-α plus IFN-γ, which regulate NO production.
Cytokines act at several levels to combat Gram-positiveinfection: inducing the expression of endothelial and cellularadhesion molecules to facilitate the adherence of phagocytesto surfaces is an important first step. Next, increasing the pro-duction of local chemokines results in emigration of thephagocyte into the infected tissue. By stimulating NO pro-duction, cytokines provide the chemical agents for killing themicrobe. Cytokines such as IL-1 and TNF-α are expressedduring this time of burgeoning infection; however, produc-tion of cytokines is tightly regulated such that when the infec-tion is cleared, production of these pro-inflammatorycytokines ceases. Thus, the rapid ‘on’ and rapid ‘off ’ produc-tion limits any negative effect of cytokine-mediated
inflammation. In the case of a chronic disease, the activatorarm of the cytokine cascade stays in the ‘on’ mode. As a result,there are increasingly greater amounts of the cytokines pro-duced day after day and year after year. It appears that in dis-eases such as psoriasis, the production of these cytokines isdysregulated by the disease processes.
For the patient, the aim of therapy is to block the inflam-matory proliferation effects of these cytokines. For a diseasesuch as psoriasis, the therapeutic effect is a reduction in cellu-lar migration into the skin. Although decreased cell adhesion,cellular infiltration and a reduction in the inflammatorymediators such as NO reduce host defence, the net effect ofanticytokine therapy appears to benefit the host. This may bedue to the fact that simple pharmacokinetics limit the dura-tion of depressed host function and allow the host’s mecha-nisms for fighting infection to be transiently suppressed withsomewhat the same result as once a day or every other daycorticosteroids accomplish. One benefit of shorter-actingagents such as soluble TNF receptors is that host defencefunctions related to TNF return to the normal range morefrequently compared to long-acting antibodies to TNF-α.
Since the introduction of therapies using TNF blockers,increased infections have not been unexpected. Of these, riskof serious infections with Gram-positive organisms isincreased compared to Gram-negative infections. Voluntaryreports of bacterial infections, however, do not reflect the trueincidence because diagnosis and treatment are fairly routine.In contrast, because of their uncommon occurrence, infec-tions with intracellular organisms are increasingly reportedand analysed. Other complications such as the developmentof lupus-like disease, demyelinating disease and worsening ofheart failure were unexpected and, in fact, contrary to theconcept of reducing TNF activity [15]. On March 4 2003, theUS FDA convened the Arthritis Advisery Board in order toreview complications of TNF blockers [101]. Examination ofthe briefing documents from this meeting reveals that patientyears of etanercept use is associated with fewer reports ofopportunistic infections, including tuberculosis, than patientyears of infliximab or adalimumab. Moreover, in calculatingyears of patient use of infliximab, a single administration ofthis antibody is carried forward indefinitely to the total yearsof use, thus enlarging the denominator and reducing thenumber of cases per patient years of exposure. Host defencesagainst intracellular organisms such as Listeria [16], Histo-plasma [17], Pneumocystis or Salmonella [18] dominate the use ofinfliximab. In the case of infections with M. tuberculosis,50% are extrapulmonary or disseminated [19].
The two anti-TNF-α monoclonal antibodies used to treatRA are of the IgG1 class and have revealed an increase in thenumber of opportunistic infections. The incidence of infectionsin RA is increased compared to the population without the dis-ease and is thought to be due to the immunosuppressive compo-nent of the disease in the absence of treatment with agents suchas prednisone, MTX or cyclosporin. In RA patients treated withthese agents, infections are further increased. Studies on

Drug Discovery and Development for Inflammatory Diseases
162 Expert Opin. Ther. Targets (2004) 8(2)
infections in patients with plaque psoriasis are less comprehen-sive but one can assume that the use of MTX or cyclosporin inthis disease also increases the risk of infection. However, thereare few reports of opportunistic infections in patients withplaque psoriasis even with treatment with MTX or cyclosporin.
As discussed at length at the IBC conference, the ‘off ’ rateof TNF-α binding to the Type II cell-bound receptor is rapidwhen compared to the binding to the Type I receptor [20]. Inmany ways, the same type of rapid ‘off ’ rate is observed whenone considers membrane TNF-α and the binding of theType II soluble receptor. The soluble TNF receptor Type II asthe Fc bivalent construct (etanercept) binds to membraneTNF-α but this interaction is reversible in that the inhibitionof biological activity is less than that of infliximab and thebinding is of a lower affinity [21]. In contrast, infliximab formsmore stable complexes with membrane TNF-α relative to thecomplexes formed with etanercept. Moreover, a greaternumber of infliximab molecules bound to membrane TNF-αwith higher avidity compared to etanercept. This was sup-ported by the observation that infliximab exhibited a greaterreduction in the biological activity of membrane TNF-α-bear-ing cells on endothelial target cells compared to etanercept [20].These studies are consistent with the concept that the actionof etanercept on membrane as well as soluble TNF-α is‘reversible’, whereas the binding of monoclonal anti-TNF-αantibodies is more effective for either soluble TNF-α in theextracellular space as well as membrane TNF-α.
In contrast, etanercept does not lyse cells or activate cas-pase-3 in cells expressing membrane TNF-α [22]. Althoughetanercept is constructed with the complement receptordomains of human IgG1, the hinge region of the fusion ofthe Fc chain to the p75 extracellular domain of theTNF receptor is missing one of the CH2 groups and hencethe structure is predicted to be more rigid than the Fc ofnatural antibodies. Whether this is the explanation or not,etanercept does not activate complement and does not lysecells expressing membrane-bound TNF-α . It is also the case
of other soluble receptors of TNF receptors (lenercept,onercept and pegsunercept). Thus, one must consider anyclinical event indicative of decreased host defence againstinfection associated with therapy using any method ofTNF-α neutralisation (infliximab, adalimumab,anti-TNF-α monoclonal antibodies of the IgG4 class,etanercept, lenercept, onercept and pegsunercept) withinfection associated with monoclonal antibodies that fixcomplement and also result in loss of membrane-boundTNF-α (infliximab and adalimumab).
In summary, the drug discovery and development advancesof the biopharmaceutical industry worldwide have now beenrealised from earlier cytokine and chemokine basic researchconducted > 25 years ago. Pioneers in this early field includ-ing C Dinarello, J-M Dayer, D Wallach, W Arend, B Beutler,G Kollias and countless others can now see their vision ‘real-ised’ through seriously ill patients who have been given a sec-ond chance with these biological therapeutics. The stage iscurrently set to capitalise on these early advances in molecularmedicine to design novel small-molecule agents throughadvanced proteomic techniques [23] that can specificallyinhibit adverse cytokine- and chemokine-driven processes inthe host with hopefully a greater degree of safety to thepatient. This conference provided an excellent example ofhow the academic research world is now closely interfacingwith this industry to meet these drug discovery challenges ininflammatory diseases.
Acknowledgements
The author wishes to express his gratitude to the followingprofessional drug discovery colleagues who provided supportfor this article: A Stuetz, J Vollmer, A Lewis, L Pagliaro,C Korstanje, M Sjöberg, K Asadullah, M Pallidino, G Grützand R Horuk. Special thanks also go to D Baron for her crea-tive artistry on the manuscript figures and Yi-Yang Yvonne Lifor her careful review of the manuscript.

Edwards III
Expert Opin. Ther. Targets (2004) 8(2) 163
BibliographyPapers of special note have been highlighted as either of interest (•) or of considerable interest (••) to readers.
1. KALTHOFF FS, CHUNG J, STUETZ A: Pimecrolimus inhibits up-regulation of OX-40 and synthesis of inflammatory cytokines upon secondary T cell activation by allogeneic dendritic cells. Clin. Exp. Immunol. (2002) 130(1):85-92.
2. RAPPERSBERGER K, KOMAR M, EBELIN ME et al.: Pimecrolimus identifies a common genomic anti-inflammatory profile, is clinically highly effective in psoriasis and is well tolerated. J. Invest. Dermatol. (2002) 119(4):876-887.
3. BENNETT BL, SATOH Y, LEWIS AJ: JNK: a new therapeutic target for diabetes. Curr. Opin. Pharmacol. (2003) 3(4):420-425.
4. KORSTANJE C: Shifting attention from one cell type to another in dermatological research, but where are the new drugs? Curr. Opin. Investig. Drugs (2001) 2(5):624.
5. HOUSTON P, GOODMAN J, LEWIS A et al.: Homing markers for atherosclerosis: applications for drug delivery, gene delivery and vascular imaging. FEBS Lett. (2001) 492(1-2):73-77.
6. ASADULLAH K, STEERY W, STEPHANEK K et al.: IL-10 is a key cytokine in psoriasis. Proof of principle by IL-10 therapy: a new therapeutic approach. J. Clin. Invest. (1998) 101(4):783-794.
• This is the first paper to demonstrate the effects of rhuIL-10 in psoriasis.
7. ASADULLAH K, DOECKE WD, EBELING M et al.: Interleukin 10 treatment of psoriasis: clinical results of a Phase II trial. Arch. Dermatol. (1999) 135(2):187-192.
8. JUNG M, SABAT R, KRAETZSCHMAR J et al.: Expression profiling of IL-10-regulated genes in human monocytes and peripheral blood mononuclear cells from psoriatic patients during IL-10 therapy. Eur. J. Immunol. (2004) 34(2):481-493.
•• This paper describes the effects of IL-10 treatment on gene expression ex vivo.
9. ECONOMIDES AN, CARPENTER LR, RUDGE JS et al.: Cytokine traps: multi-component, high-affinity blockers of cytokine action. Nat. Med. (2003) 9(1):47-52.
10. DINARELLO CA: Setting the cytokine trap for autoimmunity. Nat. Med. (2003) 9(1):20-22.
11. EDWARDS CK III, MARTIN SW, SEELY J et al.: Design of PEGylated soluble tumor necrosis factor receptor Type I (PEG sTNF-RI) for chronic inflammatory diseases. Adv. Drug Deliv. Rev. (2003) 55(10):1315-1336.
12. PALLADINO MA, BAHJAT FR, THEODORAKIS EA et al.: Anti-TNF-α therapies: the next generation. Nat. Rev. Drug Discov. (2003) 2(9):736-746.
13. LAM T, LING T, CHOWDHURY C et al.: Synthesis of a novel family of diterpenes and their evaluation as anti-inflammatory agents. Bioorg. Med. Chem. Lett. (2003) 13(19):3217-3221.
14. ONUFFER J, MCCARRICK MA, DUNNING L et al.: Structure function differences in nonpeptide CCR1 antagonists for human and mouse CCR1. J. Immunol. (2003) 170(4):1910-1916.
15. BOZKURT B, TORRE-AMIONE G, WARREN MS et al.: Results of targeted anti-tumor necrosis factor therapy with etanercept (Enbrel) in patients with advanced heart failure. Circulation (2001) 103(8):1044-1047.
16. SLIFMAN NR, GERSHON SK, LEE JH et al.: Listeria monocytogenes infection as a complication of treatment with tumor necrosis factor α-neutralizing agents. Arthritis Rheum. (2003) 48(2):319-324.
• This paper describes infections observed in patients being treated with TNF blockers.
17. LEE JH, SLIFMAN NR, GERSHON SK et al.: Life-threatening histoplasmosis complicating immunotherapy with tumor necrosis factor α antagonists infliximab and etanercept. Arthritis Rheum. (2002) 46(10):2565-2570.
18. NETEA MG, RADSTASKE T, JOOSTEN LA et al.: Salmonella septicemia in rheumatoid arthritis patients receiving
anti-tumor necrosis factor therapy. Arthritis Rheum. (2003) 48(7):1853-1857.
19. FRISHMAN JI, EDWARDS CK III, SONNENBERG MG, KOHNO T, COHEN AM, DINARELLO CA: Tumor necrosis factor (TNF)-α-induced interleukin-8 in human blood cultures discriminates neutralization by the p55 and p75 TNF soluble receptors. J. Infect. Dis. (2000) 182(6):1722-1730.
•• Describes the effects of p75 and p55 soluble TNF receptors in human whole blood.
20. SCALLON B, CAI A, SOLOWSKI N et al.: Binding and functional comparisons of two types of tumor necrosis factor antagonists. J. Pharmacol. Exp. Ther. (2002) 301(2):418-426.
21. VAN DEVENTER SJ: Transmembrane TNF-α, induction of apoptosis, and the efficacy of TNF-targeting therapies in Crohn’s disease. Gastroenterology (2001) 121(5):1242-1246.
22. VAN DEN BRANDE JM, BRAAT H, VAN DEN BRINK GR et al.: Infliximab but not etanercept induces apoptosis in lamina propria T-lymphocytes from patients with Crohn’s disease. Gastroenterology (2003) 124(7):1774-1785.
• Describes the mechanism of action of infliximab in Crohn’s disease.
23. BOUWMEESTER T, BAUCH A, RUFFNER H et al.: A physical and functional map of the human TNF-α/NF-κB signal transduction pathway. Nat. Cell Biol. (2004) 6(2):97-105.
Website101. http://www.FDA.gov
AffiliationCarl K Edwards III PhDHead, Research Business Area Dermatology, USA; Schering AG/Berlex Biosciences, 2600 Hilltop Drive, Richmond, CA 94804-0099, USA; The University of Colorado Health Sciences Center, School of Medicine, Division of Infectious Diseases, 4200 Colorado Blvd, Denver, CO 80208, USATel: +1 510 669 4584; Fax: +1 510 669 4270;E-mail: [email protected]