Embed Size (px)
Citation preview
Dr Rajendra Prasad FRCS(Glas) FRCS(Neurosurgery)
Senior Consultant NeurosurgeonApollo Hospitals. New Delhi. India
The goal of prophylaxis against VT is to reduce the incidence of DVT and, by doing so, decrease the morbidity associated with the postthrombotic syndrome and the morbidity and mortality associated with PE. Acceptable means of prophylaxis must be not only effective but also demonstrably safe. many neurosurgeons have not modified their thromboprophylaxis strategies, presumably for safety reasons.
Both mechanical and pharmacologic methods of prophylaxis are available and are used to varying degrees to prevent perioperative VT. While most general and orthopedic surgeons have shifted away from relying solely on mechanical methods of prophylaxis, and now use pharmacologic agents to a greater degree.
Prevention of thromboembolism after neurosurgery for brain and spinal tumors. (Original Article).Publication: Southern Medical JournalPublication Date: 01-JAN-03
Article ExcerptObjective: Deep venous thrombosis (DVT) is a major cause of morbidity and mortality after surgery for primary and metastatic brain tumors.
Methods: We conducted a confidential survey of American neurosurgeons interested in tumor surgery to assess DVT risk awareness and thromboprophylaxis patterns.
Results: Of the 172 respondents, 108 (63%) underestimated the DVT risk after brain tumor surgery. After performing brain tumor surgery, 76.2% of respondents reported using solely mechanical methods of prophylaxis "always" or "most of the time."
Conclusion: American neurosurgeons tend to underestimate the risk of DVT associated with brain tumor surgery and to use mechanical thromboprophylaxis despite the availability of effective pharmacologic anti-thrombotics. A better appreciation of the risk of thrombosis, combined with clinical studies to address safety, may enhance the use of prophylaxis and the perceived safety of antithrombotics in this setting.
04/18/23
VENOUS THROMBOEMBOLISM AND SPINAL SURGERY .T. Pitham; A. Cree; A. Kam; M. Dexter; G. Dandie; C. New; M. Fearnside; J. Cummine; K. Hitos; K. Saker; and J. Fletcher Journal of Bone and Joint Surgery - British Volume, Vol 87-B, Issue SUPP_III, 401-402.
A prospective cohort study was conducted to assess the incidence of venous thromboembolism (VTE) in 300 patients undergoing elective spinal surgery
. Bilateral lower extremity venous duplex scans
were performed pre-operatively, within one week postoperatively and at 4 to 6 weeks post-operatively. Information was collected regarding age, gender, body mass index, type and duration of surgical procedure, intra-operative blood loss and blood transfusion, pre- and post-operative mobility and other risk factors for VTE. All patients received vigorous mechanical prophylaxis with 56% of patients receiving pharmacological prophylaxis (unfractionated or low molecular weight heparin) according to surgeon preference.
Results The overall incidence of post-operative deep vein thrombosis (DVT) was 3.4%. The incidence in those receiving pharmacological prophylaxis was 1.2% versus 6.3% in those who received mechanical prophylaxis alone (p<0.05).
A 27.8% incidence of pre-operative venous abnormalities may reflect pre-operative immobility due to pain in this group of patients, and justifies the use of ultrasound scanning as an important pre-operative screening tool. In addition, the high incidence of late-onset DVT justifies the need for follow-up scanning several weeks after discharge.
Perioperative assessment of coagulability in neurosurgical patients using thromboelastographyJohn M. Abrahams, M.D., Maria B. Torchia, R.N., Michael M. McGarvey, M.D., Mary Putt, Sc.D., Ph.D., Dimitri Baranov, M.D., Grant P. Sinson, M.D.
Thrombelastography is a useful technique for evaluating coagulability. We hypothesized that it could be used to determine postoperative hematologic complications during and after neurologic surgery.
CONCLUSIONS
Increased coagulability begins between induction of anesthesia and skin incision, and continues to increase throughout surgery. These changes are more pronounced in patients undergoing craniotomy compared to patients undergoing spine procedures.
Risk factors and prophylaxis for deep venous thrombosis in neurosurgery. Smith SF, Biggs MT, Sekhon LH. Surg Technol Int. 2005;14:69-76. Neurosurgery Department and Spinal Injuries Unit, Royal North Shore Hospital, St. Leonards, New South Wales, Australia.
Acceptance is increasing for pharmacological prophylaxis against deep vein thrombosis (DVT) and pulmonary embolism (PE) for most types of surgery, but its use remains controversial in neurosurgical patients because of the threat of catastrophic hemorrhage. Consequently, mechanical measures such as sequential calf compression and graduated compression stockings are currently the preferred prophylaxis for neurosurgical patients. However, some patients remain at high risk despite these measures and may require prophylaxis with low molecular weight heparins or unfractionated heparin. In neurosurgical patients, known risk factors for DVT or PE include advanced age, malignancy, limb weakness, prolonged surgery, and cranial as opposed to spinal surgery.
HISTORY
27 year old malePolio one month after birthWas able to walk without supportAlso had dorso lumbar scoliosisDeveloped low back pain since 2 monthsProgressive weakness of both lower limbsComplete paralysis since 2weeks with bladder
and bowel incontinence
ON EXAMINATION
Power of grade 0/5 in both lower limbsDecreased tone in both lower limbsPlantars muteSensory level of D9Dorso lumbar scoliosis , no spinal tenderness
SURGERY
POST OP (Day 1)
Developed acute DVT left leg.
Had massive pulmonary embolism
Sudden drop in saturation, seizure, hypotension, bradycardia.
Could not be revived.
Deep vein thrombosis after posterior spinal surgeryspine,vol25,number22,2962-2967.
Ferree and wright – U/S- 185 patients- 2%.Smith et al-317 patient- (0.6%)Rokito et al- 329-(0.3%)Tetzlaff et al-venography-306(10.8%)This paper- 110 patients 15.5%Prevelance of proximal deep venous
thrombosis-0.9%Lumbar procedures have higher risk of DVT
than cervical proceduresScreening for detection of asymptomatic
thrombosis?
Our Tomorrow Starts Now! Covidien | | Confidential
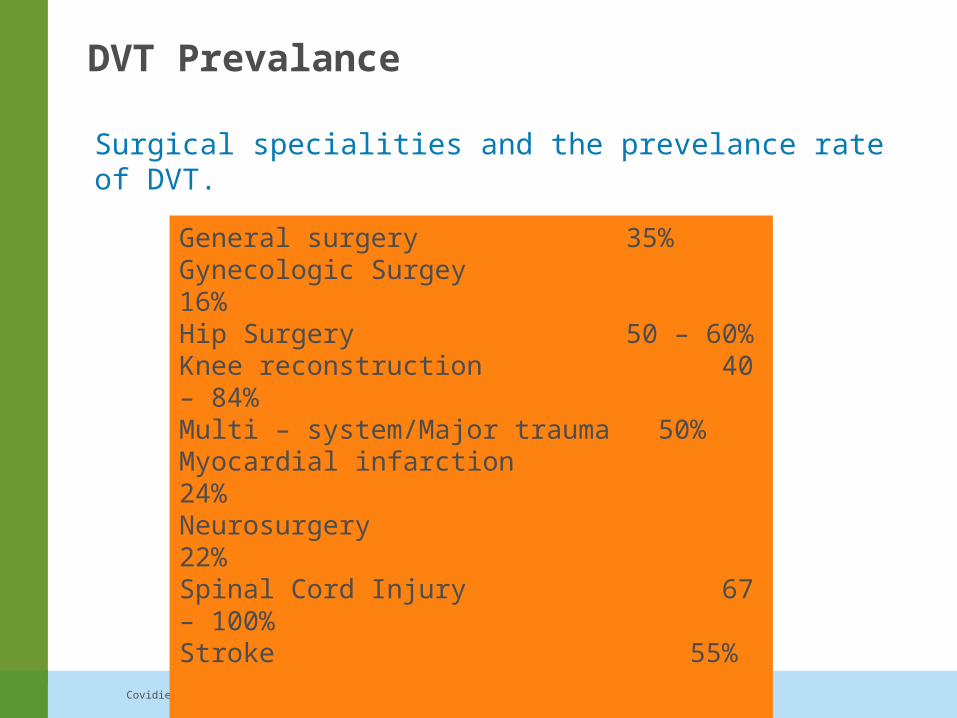
DVT Prevalance
Surgical specialities and the prevelance rate of DVT.
General surgery 35%Gynecologic Surgey 16%Hip Surgery 50 – 60%Knee reconstruction 40 – 84%Multi – system/Major trauma 50%Myocardial infarction 24%Neurosurgery 22%Spinal Cord Injury 67 – 100%Stroke 55%
ACCP 2001
Our Tomorrow Starts Now! Covidien | | Confidential
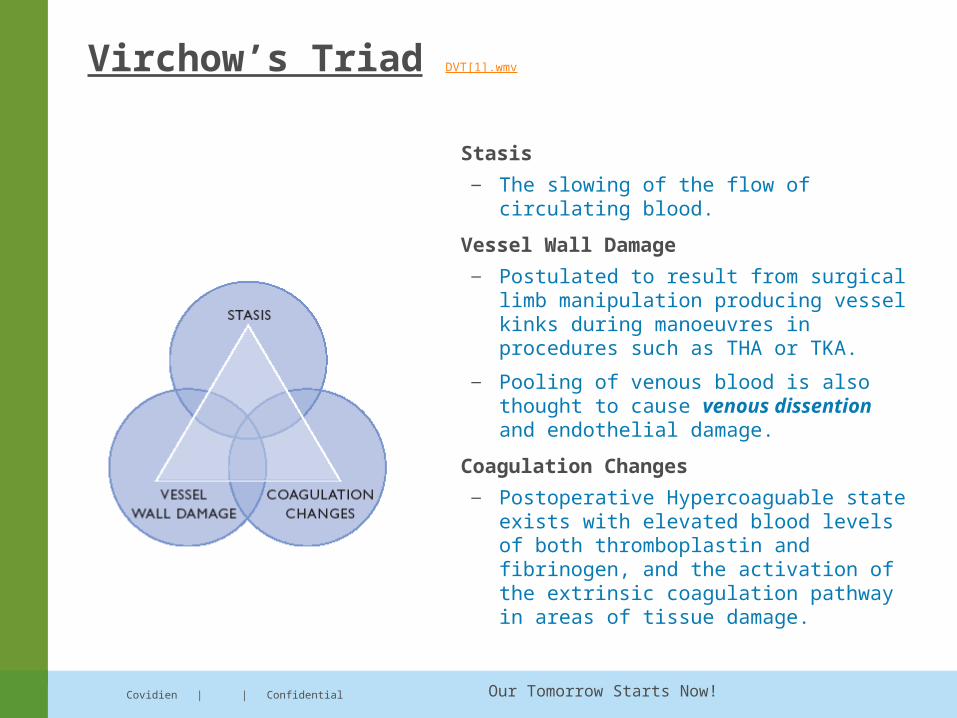
Virchow’s Triad DVT[1].wmv
Stasis — The slowing of the flow of circulating
blood.
Vessel Wall Damage — Postulated to result from surgical limb
manipulation producing vessel kinks during manoeuvres in procedures such as THA or TKA.
— Pooling of venous blood is also thought to cause venous dissention and endothelial damage.
Coagulation Changes — Postoperative Hypercoaguable state
exists with elevated blood levels of both thromboplastin and fibrinogen, and the activation of the extrinsic coagulation pathway in areas of tissue damage.
Our Tomorrow Starts Now! Covidien | | Confidential
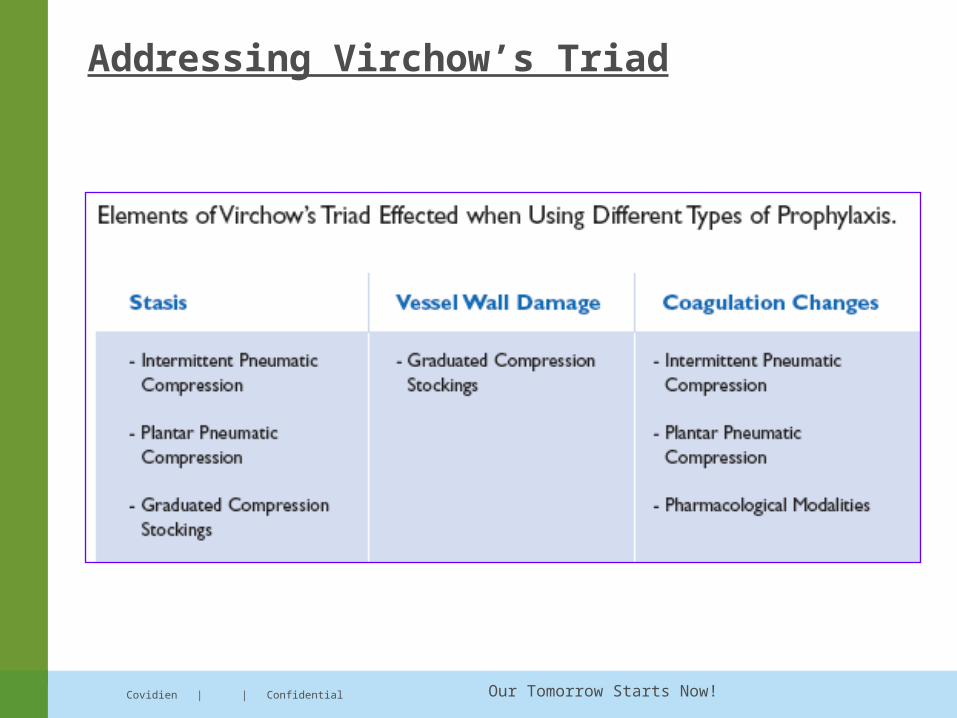
Addressing Virchow’s Triad
Our Tomorrow Starts Now! Covidien | | Confidential
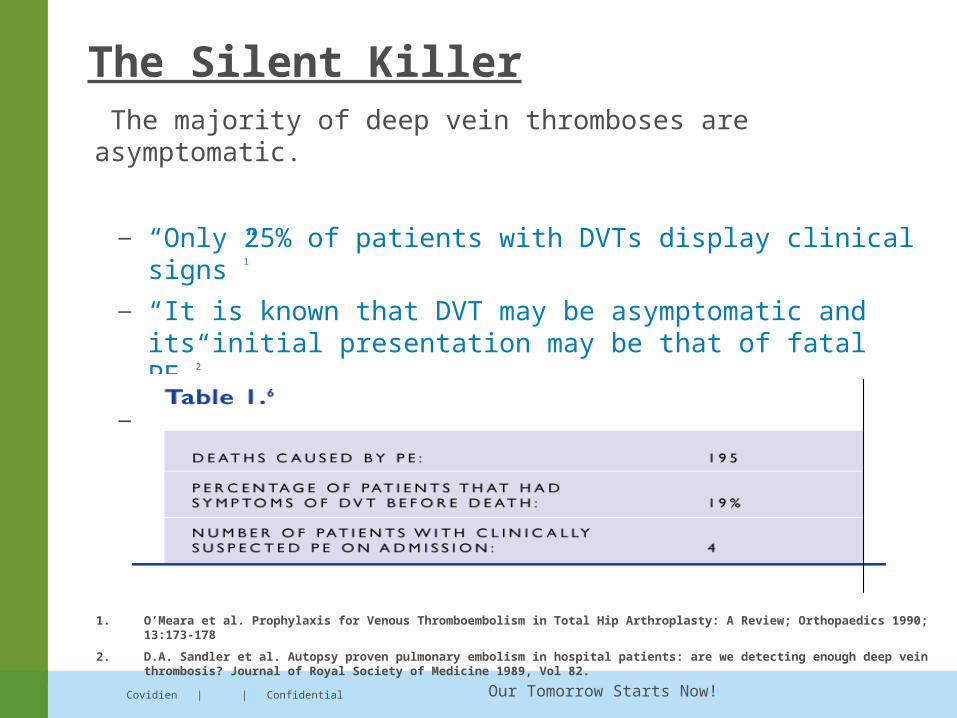
The majority of deep vein thromboses are asymptomatic.
— “Only 25% of patients with DVTs display clinical signs”1
— “It is known that DVT may be asymptomatic and its initial presentation may be that of fatal PE”2.
— 60% to 80% of fatal pulmonary emboli are unsuspected and undiagnosed.
The Silent Killer
1. O’Meara et al. Prophylaxis for Venous Thromboembolism in Total Hip Arthroplasty: A Review; Orthopaedics 1990; 13:173-178
2. D.A. Sandler et al. Autopsy proven pulmonary embolism in hospital patients: are we detecting enough deep vein thrombosis? Journal of Royal Society of Medicine 1989, Vol 82.
Our Tomorrow Starts Now! Covidien | | Confidential
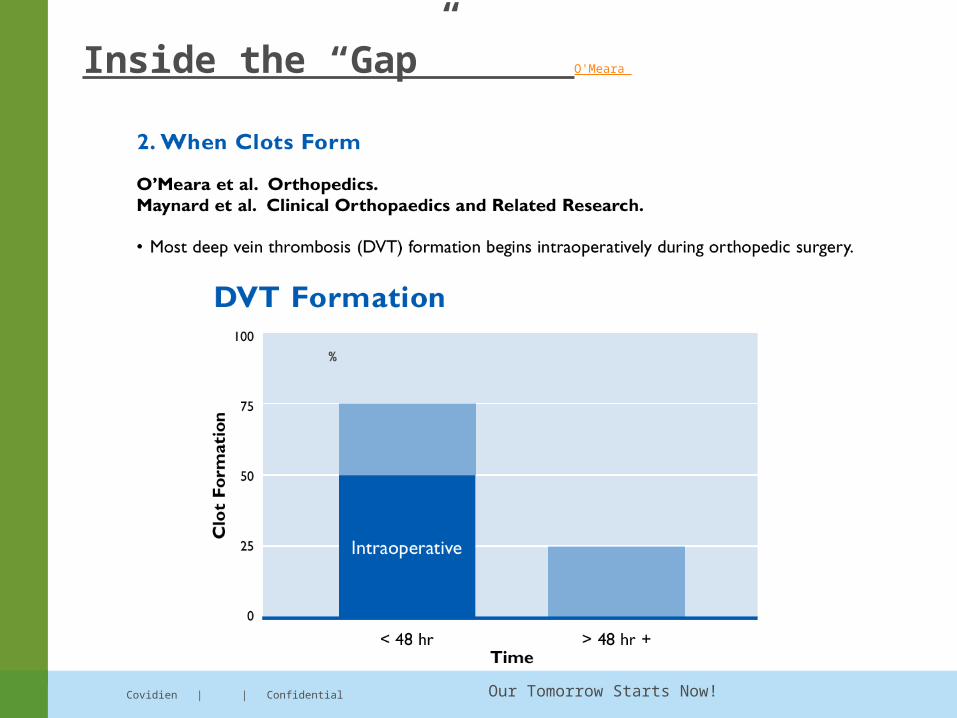
Inside the “Gap”
The “Gap” in protection is when the patient is at risk for DVT, but the
administration of pharmacological prophylaxis cannot begin.
“50% of deep vein thromboses (DVT) begin intraoperatively”1
“75% of DVT develop within the first 48 hours after surgery”1
1. O’Meara and Kaufman. Prophylaxis for Venous Thromboembolism in Total Hip Arthroplasty: A Review. Orthopaedics. 1990 13(2):173-178
Our Tomorrow Starts Now! Covidien | | Confidential
Inside the “Gap” O'Meara
%
Our Tomorrow Starts Now! Covidien | | Confidential
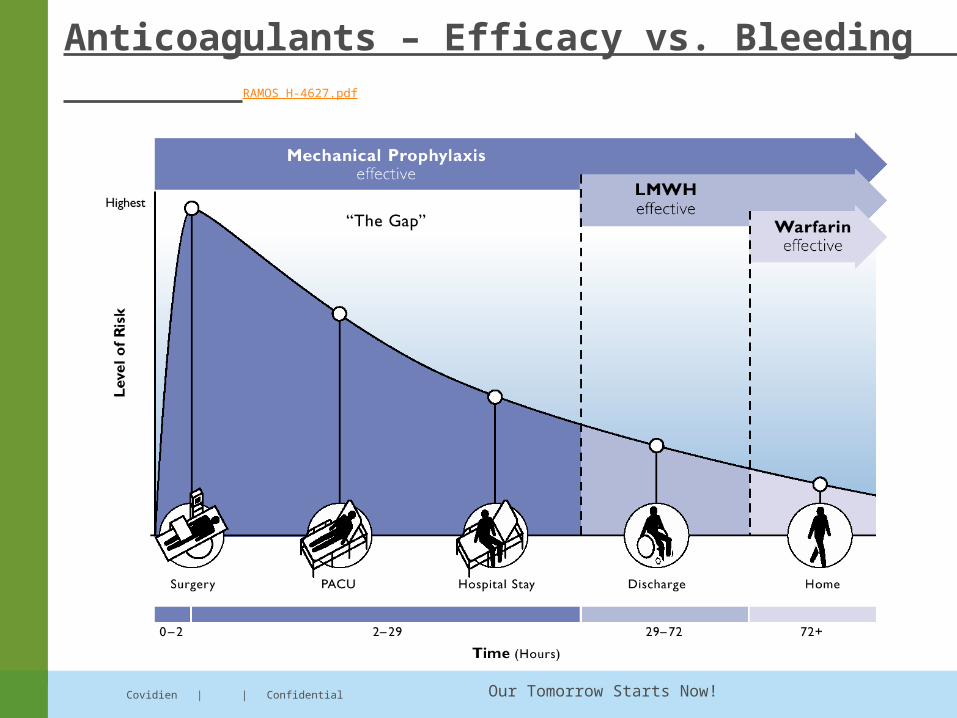
Anticoagulants – Efficacy vs. Bleeding RAMOS H-4627.pdf
Our Tomorrow Starts Now!
Risk Factors
Age older than 50 years
History of varicose veins
History of myocardial infarction
History of cancer
History of atrial fibrillation
History of ischemic stroke
History of diabetes mellitus
Other additional factors included previous deep venous thrombosis (DVT), heart failure, obesity, paralysis, or the presence of an inhibitor deficiency state.
The strongest risk factor (odds ratio >10) for venous thromboembolism (VTE) was seen after hip or leg fracture/replacement, major general surgery, major trauma, or spinal cord injury.
Covidien | | Confidential
Our Tomorrow Starts Now!
How Should High Risk Patients Be Prophylaxed?
With aggresive prophylaxis:—LMWH at prophylaxis dose
—OR Coumadin at INR 2-3 range
—OR Arixtra
If above contraindicated, then consider:— IVC filter (prevents PE, not DVT)
—Pneumatic compression > 23hr/day
—Serial doppler surveillance
Our Tomorrow Starts Now!
Contraindications to antithrombotic or anticoagulant therapy
Active bleeding, severe bleeding diathesis or platelet count less than 20,000/µL
Neurosurgery, ocular surgery, or intracranial bleeding within the past 10 days.
Relative contraindications include mild to moderate bleeding diathesis or platelet count of 20,000-100,000/µl
Brain metastases or recent major trauma,
Major abdominal surgery within the past 2 days,
Gastrointestinal or genitourinary bleeding within the past 14 days,
Infective endocarditis, or malignant hypertension.
Covidien | | Confidential
Our Tomorrow Starts Now!
What Other Special Considerations for Anticoagulation Exist?
Discontinue use of LDUH or LMWH 12 hours prior to the placement/removal of a spinal catheter.
Hold LDUH or LMWH for at least 2 hours after placement of removal of spinal catheter.
Platelet count < 30 X 109/L
Status post brain, spinal, or ophthalmic surgery.
Hemorrhagic stroke
Bacterial endocarditis
Diabetic retinopathy
Concomitant antiplatelet therapy
Our Tomorrow Starts Now!
How Should These Considerations Be Handled?
In most cases, neurosurgery- permits aggressive prophylaxis after a week post-op brain or spinal surgery or a week post intracerebral bleed.
Our Tomorrow Starts Now!
A review of the risks and benefits of differing prophylaxis regimens for the treatment of deep venous thrombosis and pulmonary embolism in neurosurgery.Epstein NE. Bronx, NY 10461, USA. Surg Neurol. 2005 Oct;64(4):295-301.
METHODS: Neurosurgical studies focusing on different methods of prophylaxis used for the prevention of DVT and PE were reviewed. The efficacy, risks, and benefits of varied treatment options were evaluated, with particular emphasis on minor and major hemorrhages occurring where heparin-based protocols were used.
Covidien | | Confidential
Our Tomorrow Starts Now!
.
RESULTS: In Flinn et al series (Arch Surg. 1996;131(5):472-80), the incidence of DVT was greater for cranial (7.7%) than spinal procedures (1.5%). Although intermittent pneumatic compression devices provided adequate reduction of DVT/PE in some cranial and combined cranial/spinal series, low-dose subcutaneous unfractionated heparin or low molecular-weight heparins further reduced the incidence, not always of DVT, but of PE (Br J Neurosurg 1995;9(2):159-63; J Intensive Care Med 2003;18(2):59-79).
Nevertheless, low-dose heparin-based prophylaxis in cranial and spinal series risks minor and major postoperative hemorrhages: 2% to 4% in a cranial series, 3.4% minor and 3.4% major hemorrhages in a combined cranial/spinal series, and a 0.7% incidence of major/minor hemorrhages in a spinal series (J Neurosurg 2003;99(4):680-4; Neurosurgery 1986;18(4):440-5; Eur Spine J 2004;13(1):1-8; J Intensive Care Med 2003;18(2):59-79.
Covidien | | Confidential
Our Tomorrow Starts Now!
• CONCLUSIONS: Although mechanical prophylaxis provided effective prophylaxis against DVT/PE in many series, the added efficacy of low-dose heparin regimens has to be weighed against risks of major postoperative hemorrhages and their neurological sequelae.
Covidien | | Confidential
Our Tomorrow Starts Now!
Our protocol
Screening for DVT for para/quadriplegics with grade0-2/5 power.
Graduated compression stocking- Graduated compression stocking reduces venous stasis by applying a gradient pressure pattern on the limb and prevents vein wall distention.
Covidien | | Confidential
Our Tomorrow Starts Now!
Low molecular weight heparin - binds to anti-thrombin III as a catalyst for anti-Factor X-a; therefore, there is no need to monitor partial thromboplastin time.- till patient is discharged.
DVT Pump- at the time of surgery till patient has been mobilised.
Early mobilisation-patients are mobilized as early as postoperative day 2.
Limb physiotherapy
Covidien | | Confidential
Our Tomorrow Starts Now!
Apollo Hospital New Delhi
• Orthopaedics
• Obstetrics & Gynaecology
• Oncology
• Surgery
• Neuroscience
• Cardiology and Vascular Surgery
• Urology

Our Tomorrow Starts Now! Covidien | | Confidential
THANK YOU





























