Embed Size (px)
Citation preview
DR. M.ABBASIRHEUMATOLOGIST
QUMS
Periarthritis Of Shoulder Joint
EPIDEMIOLOGY
Shoulder pain
16-26% of all musculoskeletal complaints
Is the third most common MSK pain
I- LBP II- Knee pain III- Shoulder pain%50 of the population will suffer
during their life60% may experience symptoms
for a year or moreEspecially common in diabetic
patient Female>maleRight shoulder>Left shoulder In iran 14/5%
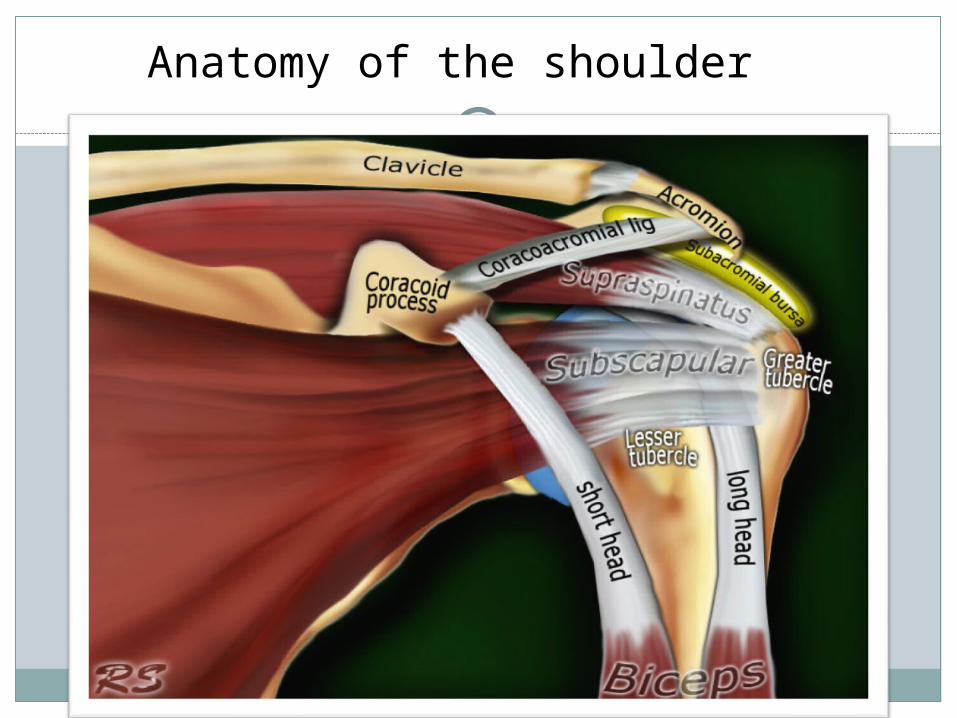
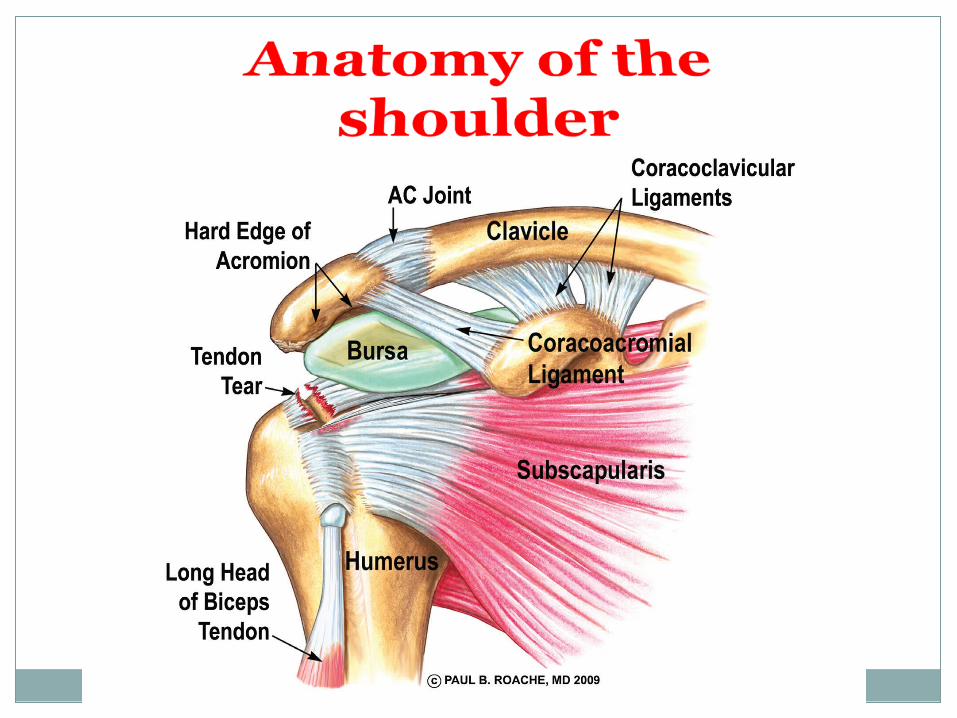
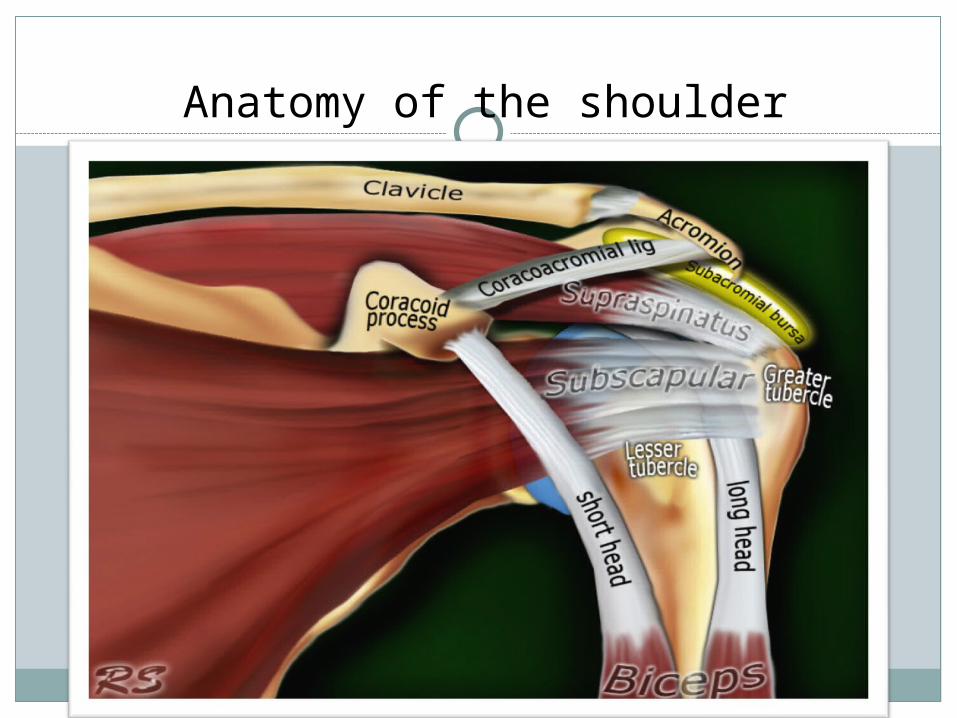
Anatomy of the shoulder
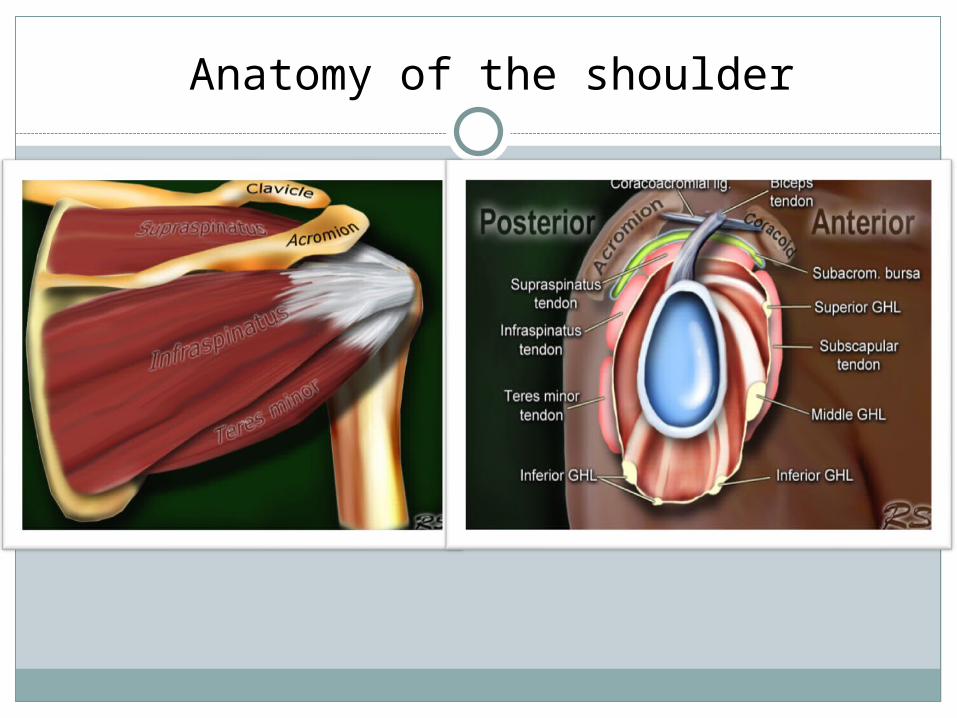
Anatomy of the shoulder
JointsJoints
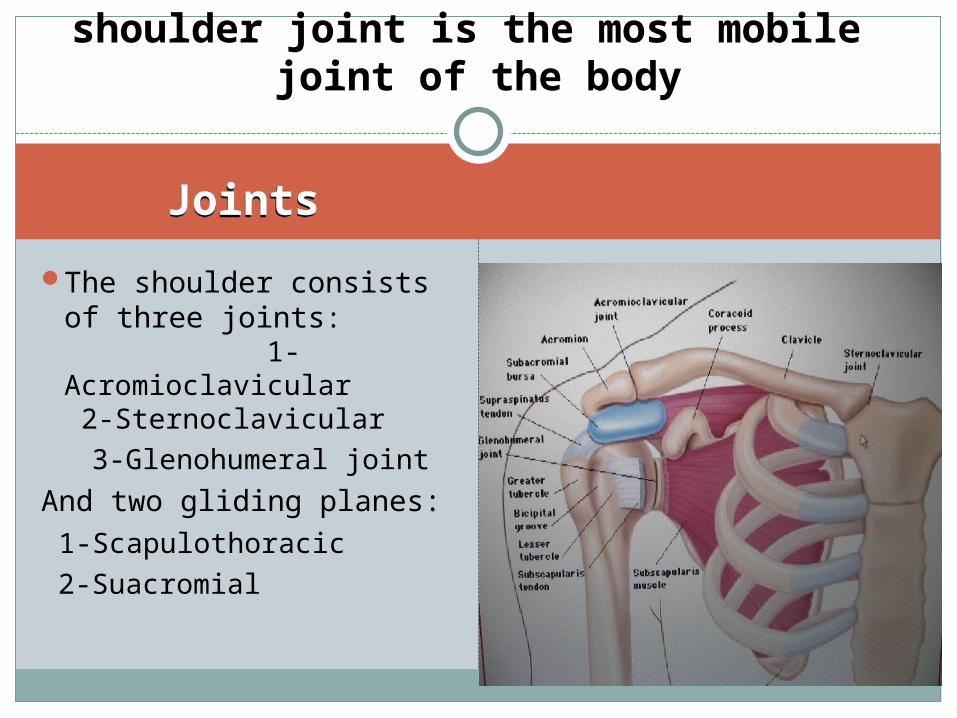
The shoulder consists of three joints: 1-Acromioclavicular 2-Sternoclavicular
3-Glenohumeral joint
And two gliding planes: 1-Scapulothoracic
2-Suacromial
shoulder joint is the most mobile joint of the body
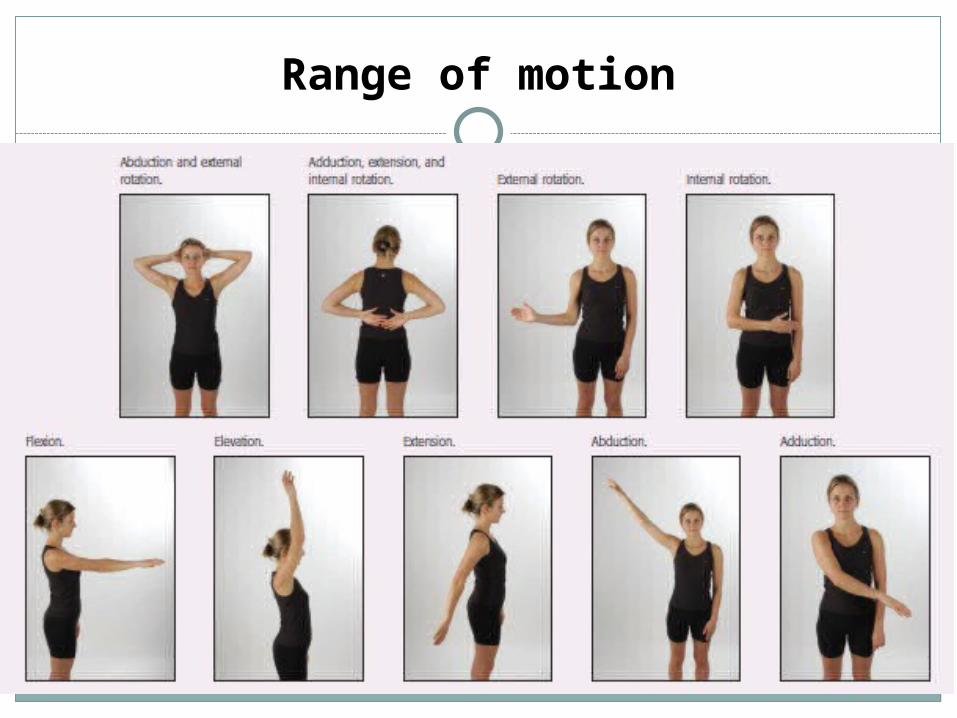
Range of motion
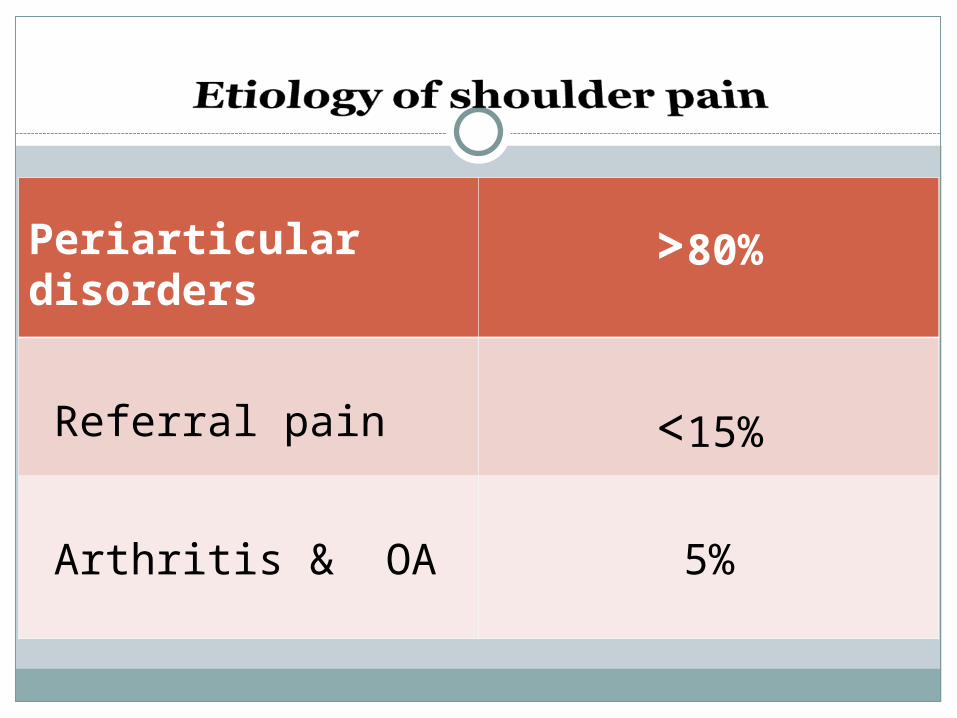
Periarticular disorders
>80%
Referral pain <15%
Arthritis & OA 5%
common causes of
periarticular disorders of
shoulder
Rotator cuff (R.C.) tendinitis or impingement syndrome
Rotator cuff tearCalcific tendinitisBicipital tendinitisFrozen shoulder

Rotator cuff tendinitis
Impingement may be defined as the encroachment
of the acromion, coracoid process or AC joint on the
rotator cuff as it passes beneath them during
glenohumeral motion
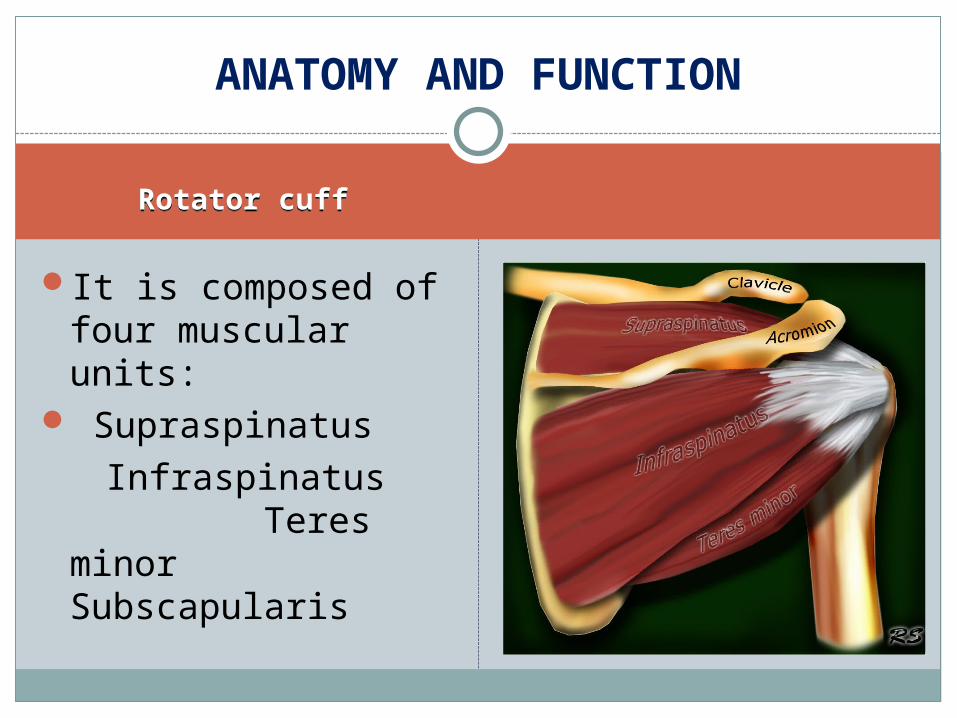
Rotator cuffRotator cuff
It is composed of four muscular units:
Supraspinatus Infraspinatus
Teres minor Subscapularis
ANATOMY AND FUNCTION
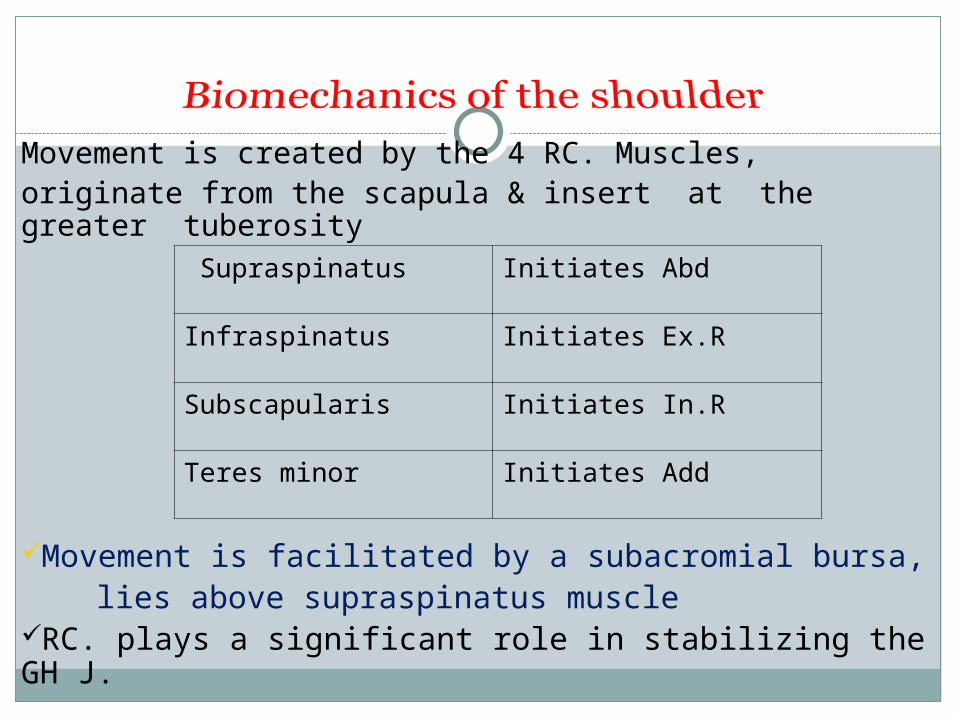
Movement is created by the 4 RC. Muscles,originate from the scapula & insert at the greater tuberosity
Movement is facilitated by a subacromial bursa, lies above supraspinatus muscleRC. plays a significant role in stabilizing the GH J.
Supraspinatus Initiates Abd
Infraspinatus Initiates Ex.R
Subscapularis Initiates In.R
Teres minor Initiates Add
Rotator cuff tendinopathy
Epidemiology of
70% shoulder pain(most common)High prevalence in female workers Athletes Age over 40 yearsThe prevalence increases with age
Etiology and pathogenesis
* Extrinsic compression
*Osteophytic spurring of
acromion
* Calcific tendinitis
* Instability
* Trauma
*Diminished vascular supply
*Intrinsic, degenerative event
*Age related degeneration
*Overuse
Clinical sign and symptoms
Mechanical shoulder pain(especially during overhead activity, Ext.Rot)
Dull Site of pain:anterolateral
aspect
Night pain (Especially when is lateral decubitus)
Weakness & pain(impingement syndrom +RC tear)
Physical examination
Inspection:
Atrophy, asymmetry, deformity
swelling(seldom)
palpation:
Tenderness point in subacromion
Ac joint, bicipital groove
ROM:
Active (Abd,Ext.Rot)
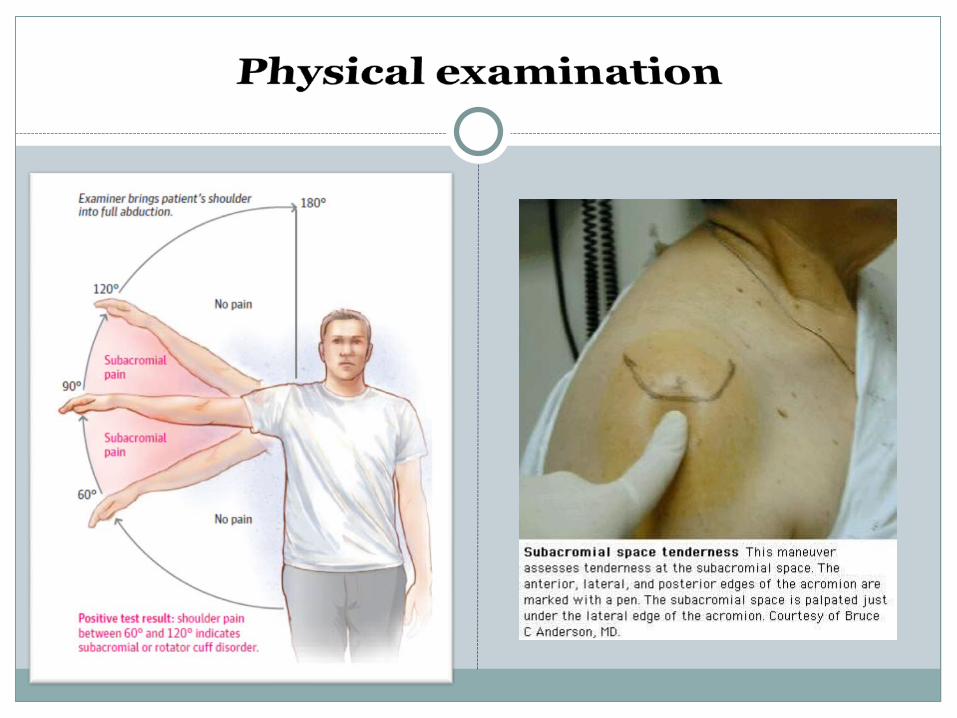
Clinical tests: painful arc
Neer impingement sign
Clancy test
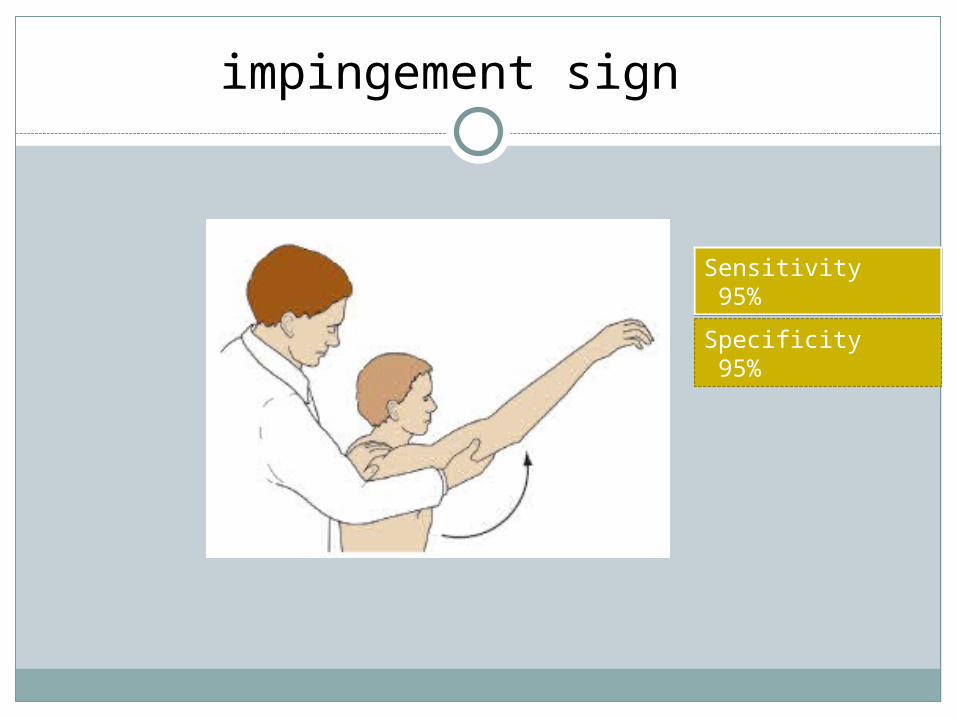
impingement sign
Sensitivity 95% Sensitivity 95%
Specificity 95%
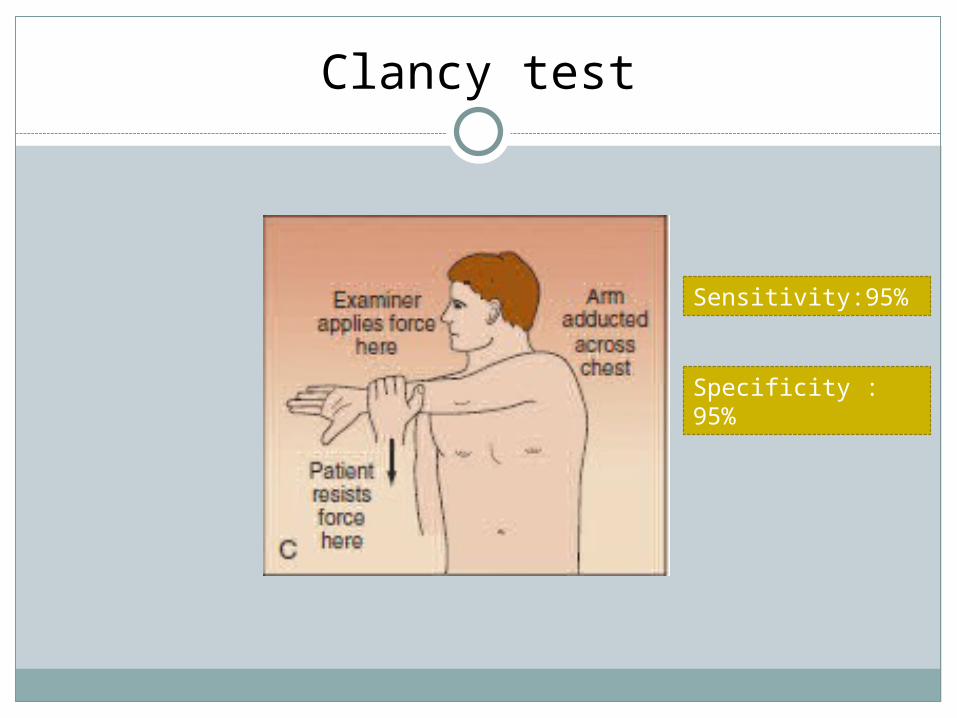
Clancy test
Sensitivity:95%
Specificity : 95%
Is predominantly clinical
A woman or man with: More than 40 years old
Mechanical shoulder painespecially during overhead activities
Impingement sign
Diagnosis
*Rest(cessation of repetitive overhead activity)
*NSAIDs
*Physical modalities
*Steroid Injection: used when the patient has
significant pain(3-injection)
*Opiate- based drugs used in the acute setting (fall)
*Exercise is mainstay of treatment
Control of symptoms stretching RC.
Improving symptoms return to normal overhead activities (sporting)

Rotator cuff tear
Rotator cuff tearing
SIZE:Small: <1cmMedium: 1-3 cmLarge: 3-5 cmMassive:>5 cmETIOLOGY: RA, SLE, renal
osteodystrophyGlucocorticoidsStage III rotator cuff
tendinitis
Etiology
Can be acute or chronic ,complete or incomplete
Acute: predominantly in young patient (falling on an outstretch- arm)
Chronic : predominantly in old patient>50 Y
History of trauma (50%)History of chronic
impingement (95%)Decreased vascularity
&cellularity
Clinical sign and symptoms
.
Acute tearing Pain & weakness of abduction and ext-Rotation
Chronic tearing Crepitation, stiffness, atrophy and weakness
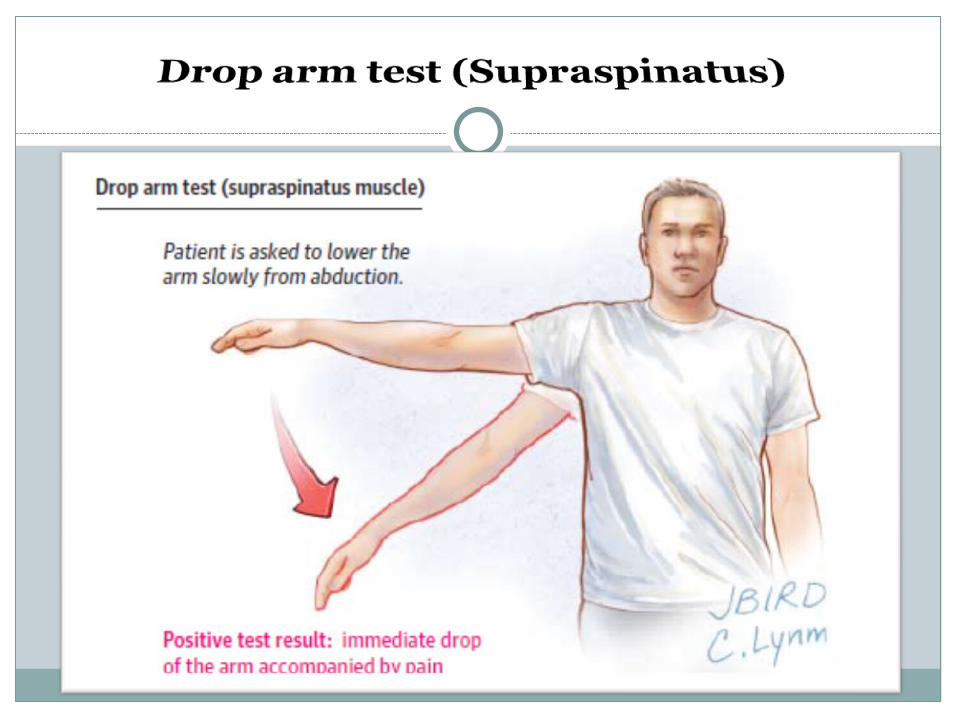
Supraspinatus tearing Inability to abduction, drop arm test Infraspinatus tearing Inability to Ext. Rotation, can't reach spoon to mouth, inability to combingext- rotation lag test
Subscapularis tearing Internal rotation lag test
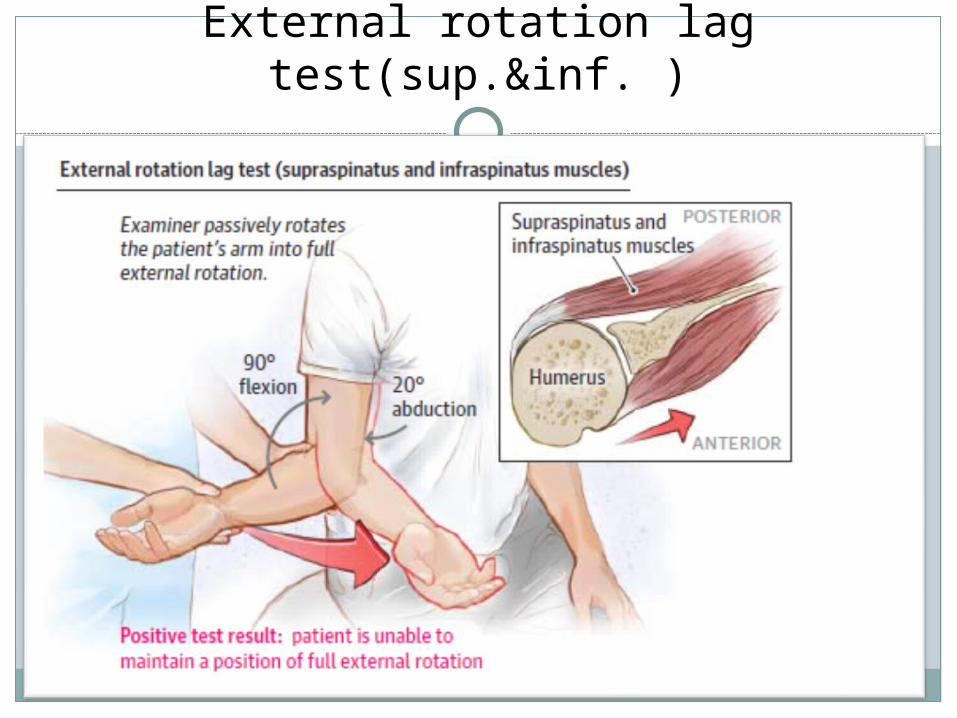
External rotation lag test(sup.&inf. )
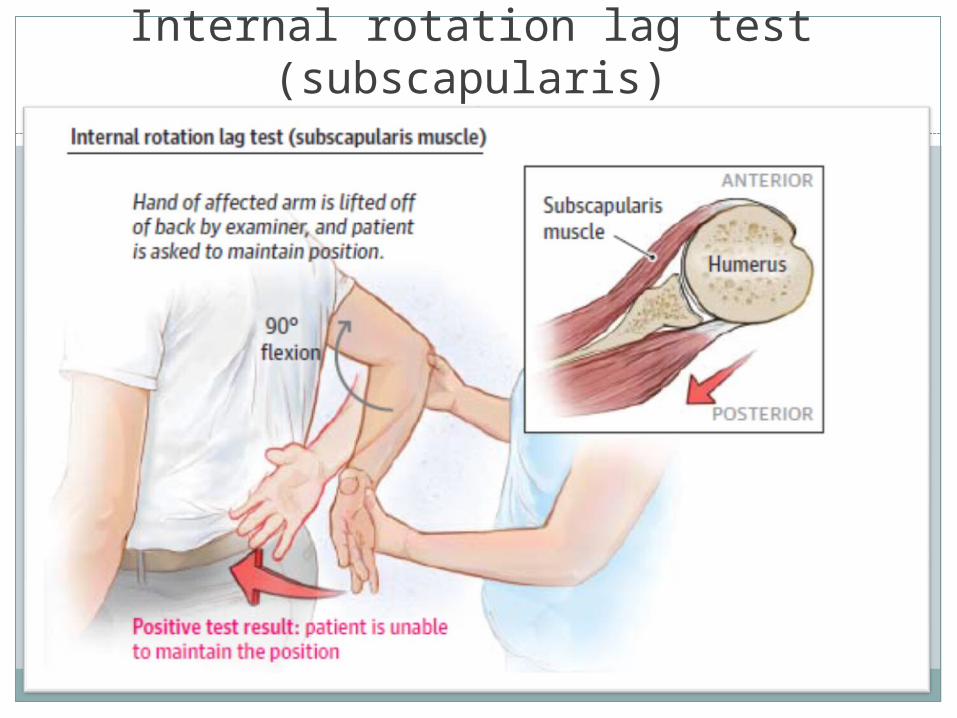
Internal rotation lag test (subscapularis)
Depend in the degree of
tear
Partial or full thickness -
tears
Age, functional status
Degree of pain
Acute
Acute Ruptures in a young or active patient (a athlete with overhead activity)
only early Surgery In an older or less active patient
Conservative 3 -6 months no acceptable function
Surgery
(Subacromial decompression, cuff repair)
Treatment
Chronic
Treatment is conservative
Surgery:1. young patients with massive tearing and weakness
2.Old patients with sever pain that don’t control 3.RC tearing +biceps tendon tearing
Response to conservative treatment (90% )

Flexion and supination of the forearm
Forward elevation of the shoulder
Biceps tendon
Anatomy of the shoulder
Epidemiology of
Bicipital
tendinitis
Men (halter)Women (gymnastic, repetitive carrying of small children)
Clinical sign and symptom
*Pain over ant- aspect of the
shoulder radiates to bicipital
groove
*Pain is exacerbated with
overhead activities, shoulder
extention & elbow flexion
Diagnostic maneuvers
The most common finding
Point tenderness by palpation
of the bicipital grooveYergason's testSpeed's test
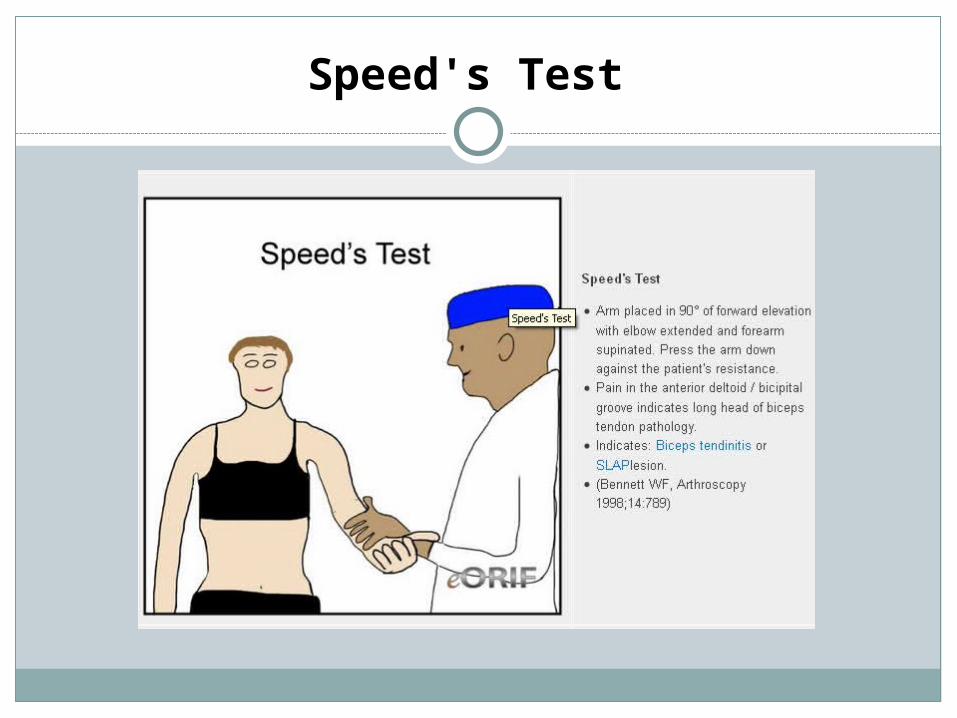
Speed's Test
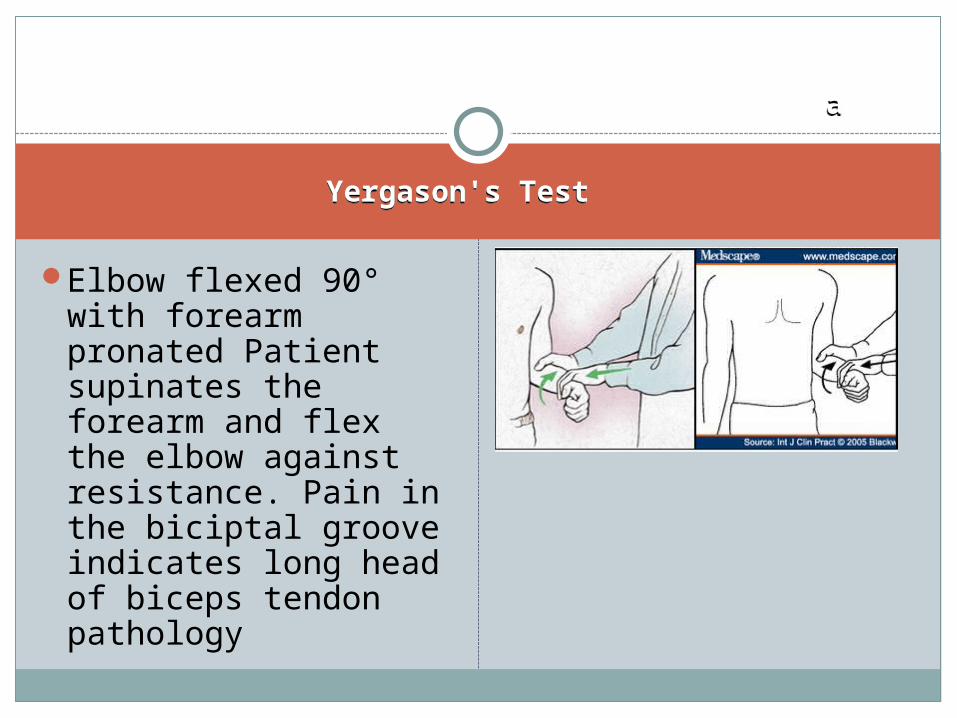
Yergason's TestYergason's Test
aa
Elbow flexed 90° with forearm pronated Patient supinates the forearm and flex the elbow against resistance. Pain in the biciptal groove indicates long head of biceps tendon pathology

*Acute rupture result from overuse in
young patient(weight-lifting)
Sudden pain
(most common)
*In older patient thinning & eventual
rupture occur spontaneously
Bicipital rupture
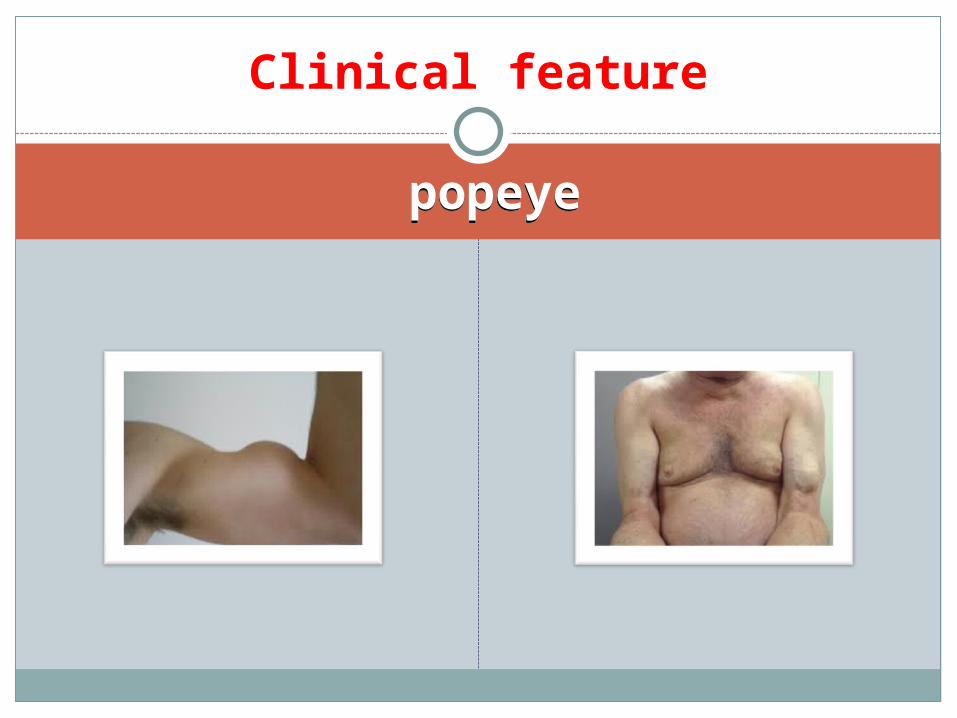
popeyepopeye
Clinical feature
Paraclinic
Plain radiography Degenerative changes in
superior border of glenoid or bicipital groove
Imaging
Ultrasonography (US)
For detection of:
Subluxation
Diagnosis of tears & tendinitis
Provides an excellent visualization for:
Superior labral complex
Biceps tendon
Bicipital groove
Bony osteophytes
Biceps tendon tears
dislocation
Treatment
Treatment of tearing Conservative Young patients(sports) : surgery Treatment of tendinitis Rest , physiotherapy, NSAIDS laser , injection in tendon sheet
Surgery Refractory bicipital tendinitisRecurrent symptom of subluxation

Calcific tendinitis
*Deposition of calcium hydroxyapatite *Symptoms develop in 35% to 45% *Age 40 to 60 y *More frequent in female ( 57% to 77%)
*Usual presentation: chronic painful condition Around the RC.(chronic impingement syndrome) *Acute presentation(7%)
pathophysiology
Precalcific: formative phase
Relatively painless
Calcific: calcium crystals are
deposited in matrix(quiescent)
Postcalcific: resorptive phase
Tends to be painful
Resorption of calcium crystals
Acute subacromial & subdeltoid bursitis
Migration of hydroxyapatite microcrystals to
bursa: induce acute inflammation
Age: 50-60 y, female
Clinical history
Acute severe pain
limiting active & passive movement
Occasionally erythema
Sometimes swelling
No history of injury or overuse
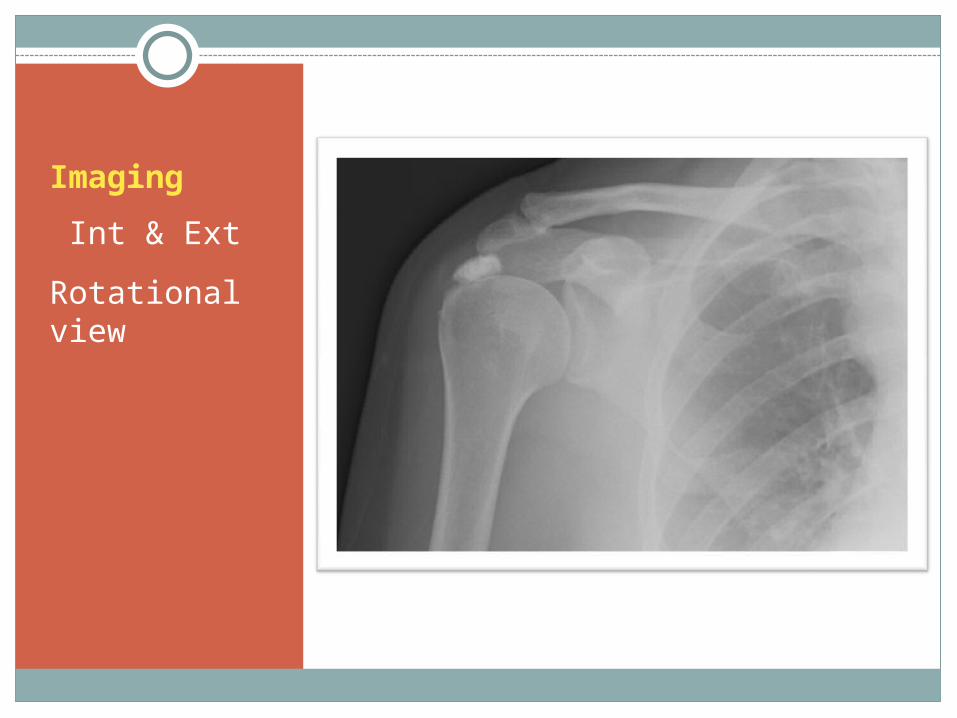
Imaging
Int & Ext
Rotational view
management
Chronic symptoms
conservative treatment
Subacromial arthroscopy(stable
phase)
Acute stage
Resting, the arm in sling
NSAIDs
Steroid injection (subacromial)
Prednisolone: 15-20mg/day - Rapidly taper
Recovery in few days or weeks

FROZEN SHOULDER (RETRACTILE CAPSULITIS)
EPIDEMIOLOGY
Etiology
Prevalence:2-3% Women 40-50 years Primary or idiopathicSecondary:Diabetes, parkinsonism, TB,
thyroid disorder, MI, lung tumor, Cervical radiculopathy
Major skeletal trauma and soft tissue injury
Change from simple or acute tendinitis to capsulitis(mixed shoulder)
pathophysiology
Stage IDiffuse inflammatory synovitis
Stage II Adherence of the capsule
Stage III Loss of ROMof normal joint
thickening and narrowing of
joint capsule
Initiation :3-8mo
Acute or insidious onset, pain at the extreme of motion, background ache in the
suprascapular and deltoid regions
Adhesive phase :4-12mo
Pain gradually decrease
Severe limitation of active & passive ROM
Resolution phase :
ROM gradually will be better, duration without treatment lasts 1-3 y
Signs and symptoms
Paraclinic
X ray : at first is normal Later :Decalcification of humerus head, joint surface are intactArthrography : the capacity of joint capsule from 28-35 cc changes to 0.5 -3 cc Radioisotope scan
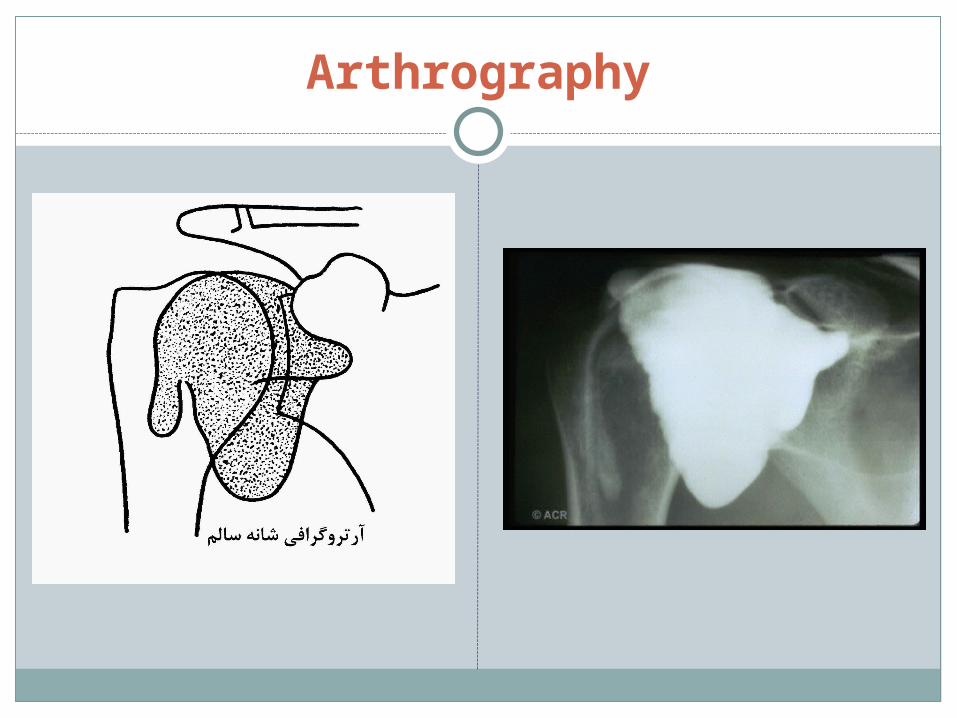
Arthrography
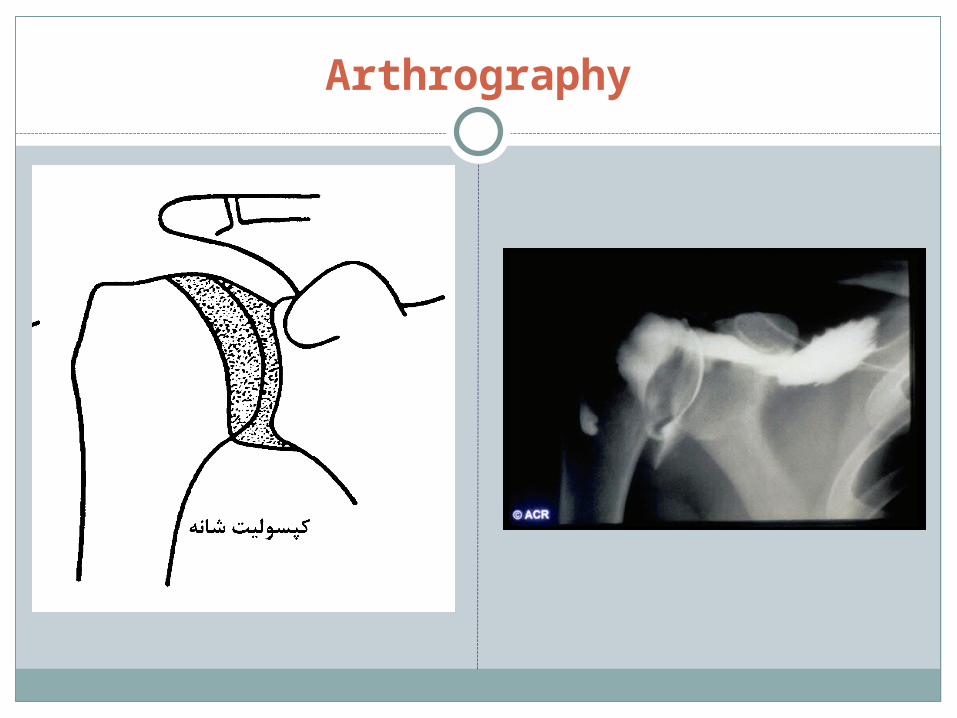
Arthrography
Treatment
Exercise is the main treatmentGentle stretching
Stage INSAIDSteroid injection Oral steroid Ice packs, ultrasound Trans cutaneous electro neuron stimulation(TENS)
Refractory conditionsClose manipulationHydraulic distentionSurgeryArthroscopic capsulotomy

Thanks