Embed Size (px)
Citation preview

Int. J. Radiation Oncology Biol. Phys., Vol. 74, No. 1, pp. 245–251, 2009Copyright � 2009 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/09/$–see front matter
doi:10.1016/j.ijrobp.2008.12.066
BIOLOGY CONTRIBUTION
DOSE–EFFECT RELATIONSHIPS FOR RECURRENCE OF KELOID AND PTERYGIUMAFTER SURGERY AND RADIOTHERAPY
HENK B. KAL, PH.D., RONALD E. VEEN, M.D., PH.D., AND INA M. JURGENLIEMK-SCHULZ, M.D., PH.D.
Department of Radiotherapy, University Medical Center Utrecht, Utrecht, The Netherlands
Purpose: To show radiation dose–response relationships for recurrence of keloid and pterygium after radiother-apy following surgery.Methods and Materials: Using PubMed, we performed a retrospective review of articles reporting incidences and/or dose–response relationships for recurrence of keloid and pterygium after radiotherapy following surgery. Theirradiation regimens identified were normalized by use of the linear–quadratic model; biologically effective doses(BEDs) were calculated.Results: For keloid recurrence after radiotherapy following keloid removal, with either teletherapy or brachyther-apy, the recurrence rate after having delivered a BED greater than 30 Gy is less than 10%. For pterygium recur-rence after bare sclera surgery and 90Sr b-irradiation, a BED of about 30 Gy seems to be sufficient also to reducethe recurrence rate to less than 10%.Conclusions: Most of the doses in the radiotherapy schemes used for prevention of keloid recurrence after surgeryare too low. In contrast, the doses applied in most regimens to prevent pterygium recurrence are too high. A schemewith a BED of 30 to 40 Gy seems to be sufficient to prevent recurrences of keloid as well as pterygium. � 2009Elsevier Inc.
LQ–BED model, Pterygium recurrence, Keloid recurrence, Fibroblasts, Radiotherapy after surgery.
INTRODUCTION
Keloids are benign fibrous dermal tumors that develop after
skin injury such as surgery or earlobe piercing. They belong
to the group of hyperproliferative diseases, such as pterygium
of the eye and Dupuytren disease. Keloid formation is due to
excessive collagen synthesis and decreased collagen degrada-
tion (1). Characteristically, the scar tissue extends beyond the
borders of the original wound. The scar does not improve with
time, and besides its unattractive visual effect, it may cause
tingling, burning, and itching. Treatment by surgery alone is
followed by recurrence in 60% to 80% of the cases (2). Com-
bination therapy is likely the optimal strategy. Methods of
treatment include intralesional steroids, 5-fluorouracil, inter-
feron, pulsed dye laser, compression with silicone sheeting,
topical tacrolimus and imiquimod, and radiotherapy (3–5).
There is no consensus about the optimal treatment. Surgical
excision followed by radiotherapy provides good results as
described in the literature. However, no consensus has been
reached on the total dosage, fractionation, or optimal timing
of the delivery of radiotherapy. Kal and Veen (6) reviewed
the literature for the recurrence rates of keloids after surgical
excision followed by radiotherapy. They concluded that an
2
optimal treatment probably is an irradiation scheme resulting
in a biologically effective dose (BED) of at least 30 Gy.
Pterygium is a complex benign disease of the supporting
orbital tissue that can cause impairment of visual function.
It belongs to the group of hyperproliferative diseases. It is as-
sociated with ultraviolet (UV) radiation, immuno-inflamma-
tory processes, genetic factors, and virus infection. For
example, UV radiation induces secretion of cytokines, and
these may activate pterygium fibroblasts, resulting in over-
growth of the conjunctiva. Pterygium typically develops be-
tween the ages of 20 and 50 years, with the greatest incidence
in dusty, hot, and dry regions in latitudes between 0� and 30�
(7, 8). Bare sclera surgery alone results in high relapse
rates—a reason to combine surgery with other treatment mo-
dalities. After surgery, therapy can include topical corticoste-
roids, thiotepa, mitomycin C, b-irradiation, and cautery.
Jurgenliemk-Schulz et al. (9) reviewed the literature for post-
operative radiotherapy and reported that treatment with
a BED of 25 Gy or greater resulted in a low relapse rate.
In this study we reviewed the literature from the past 6 years
and updated the dose–response relationships as described by
Kal and Veen (6) and Jurgenliemk-Schulz et al. (9).
Reprint requests to: Henk B. Kal, Ph.D., Department of Radiother-apy, University Medical Center Utrecht, Q00.118, Heidelberglaan100, 3584 CX Utrecht, The Netherlands. Tel: (+31) 88-755-3136;Fax: (+31) 88-755-5850; E-mail: [email protected]
45
Conflict of interest: none.Received Nov 17, 2008, and in revised form Dec 15, 2008.
Accepted for publication Dec 29, 2008.
246 I. J. Radiation Oncology d Biology d Physics Volume 74, Number 1, 2009
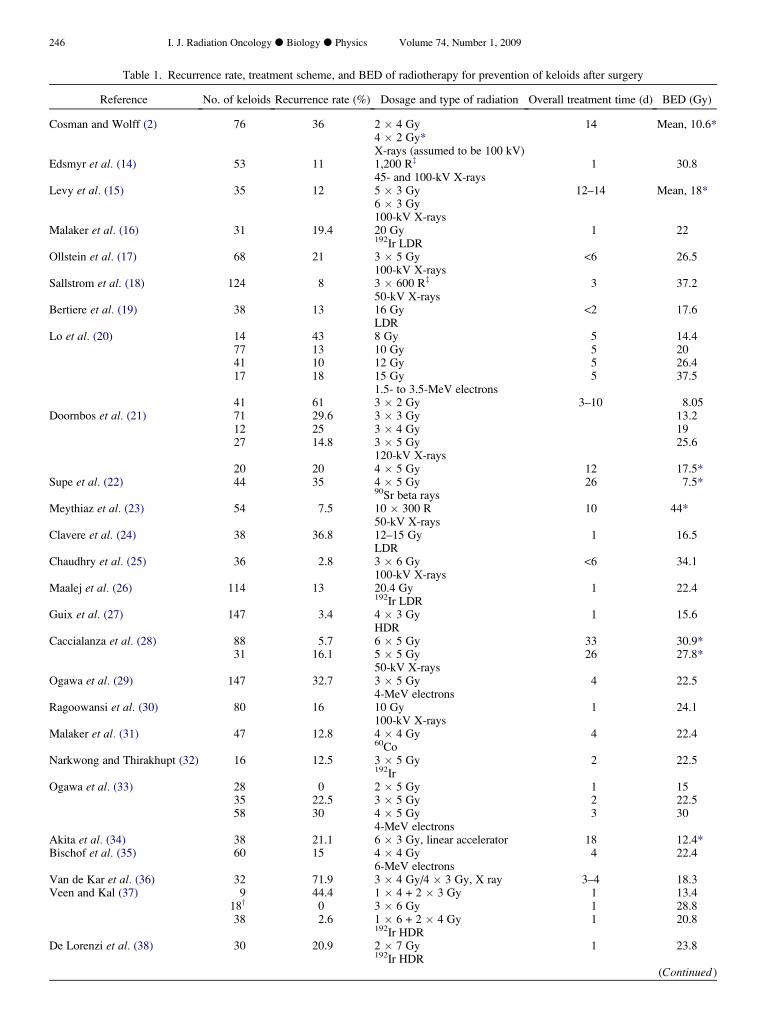
Table 1. Recurrence rate, treatment scheme, and BED of radiotherapy for prevention of keloids after surgery
Reference No. of keloids Recurrence rate (%) Dosage and type of radiation Overall treatment time (d) BED (Gy)
Cosman and Wolff (2) 76 36 2 � 4 Gy 14 Mean, 10.6*4 � 2 Gy*X-rays (assumed to be 100 kV)
Edsmyr et al. (14) 53 11 1,200 Rz 1 30.845- and 100-kV X-rays
Levy et al. (15) 35 12 5 � 3 Gy 12–14 Mean, 18*6 � 3 Gy100-kV X-rays
Malaker et al. (16) 31 19.4 20 Gy 1 22192Ir LDR
Ollstein et al. (17) 68 21 3 � 5 Gy <6 26.5100-kV X-rays
Sallstrom et al. (18) 124 8 3 � 600 Rz 3 37.250-kV X-rays
Bertiere et al. (19) 38 13 16 Gy <2 17.6LDR
Lo et al. (20) 14 43 8 Gy 5 14.477 13 10 Gy 5 2041 10 12 Gy 5 26.417 18 15 Gy 5 37.5
1.5- to 3.5-MeV electrons41 61 3 � 2 Gy 3–10 8.05
Doornbos et al. (21) 71 29.6 3 � 3 Gy 13.212 25 3 � 4 Gy 1927 14.8 3 � 5 Gy 25.6
120-kV X-rays20 20 4 � 5 Gy 12 17.5*
Supe et al. (22) 44 35 4 � 5 Gy 26 7.5*90Sr beta rays
Meythiaz et al. (23) 54 7.5 10 � 300 R 10 44*50-kV X-rays
Clavere et al. (24) 38 36.8 12–15 Gy 1 16.5LDR
Chaudhry et al. (25) 36 2.8 3 � 6 Gy <6 34.1100-kV X-rays
Maalej et al. (26) 114 13 20.4 Gy 1 22.4192Ir LDR
Guix et al. (27) 147 3.4 4 � 3 Gy 1 15.6HDR
Caccialanza et al. (28) 88 5.7 6 � 5 Gy 33 30.9*31 16.1 5 � 5 Gy 26 27.8*
50-kV X-raysOgawa et al. (29) 147 32.7 3 � 5 Gy 4 22.5
4-MeV electronsRagoowansi et al. (30) 80 16 10 Gy 1 24.1
100-kV X-raysMalaker et al. (31) 47 12.8 4 � 4 Gy 4 22.4
60CoNarkwong and Thirakhupt (32) 16 12.5 3 � 5 Gy 2 22.5
192IrOgawa et al. (33) 28 0 2 � 5 Gy 1 15
35 22.5 3 � 5 Gy 2 22.558 30 4 � 5 Gy 3 30
4-MeV electronsAkita et al. (34) 38 21.1 6 � 3 Gy, linear accelerator 18 12.4*Bischof et al. (35) 60 15 4 � 4 Gy 4 22.4
6-MeV electronsVan de Kar et al. (36) 32 71.9 3 � 4 Gy/4 � 3 Gy, X ray 3–4 18.3Veen and Kal (37) 9 44.4 1 � 4 + 2 � 3 Gy 1 13.4
18y 0 3 � 6 Gy 1 28.838 2.6 1 � 6 + 2 � 4 Gy 1 20.8
192Ir HDRDe Lorenzi et al. (38) 30 20.9 2 � 7 Gy 1 23.8
192Ir HDR(Continued )
Dose–effect relationships for recurrence of keloid and pterygium d H. B. KAL et al. 247
Table 1. Recurrence rate, treatment scheme, and BED of radiotherapy for prevention of keloids after surgery (Continued )
Reference No. of keloids Recurrence rate (%) Dosage and type of radiation Overall treatment time (d) BED (Gy)
Arneja et al. (39) 25 8 3 � 5 Gy 2 22.5192Ir HDR
Abbreviations: BED = biologically effective dose; LDR = low dose rate; HDR = high dose rate.* Corrected for overall treatment time.y Updated results.z For BED calculation, we applied 1 R = 0.96 cGy.
METHODS AND MATERIALS
Using PubMed, we performed a retrospective review of studies
reporting incidences or dose–response relationships for recurrence
of keloid and pterygium after radiotherapy following surgery.
Studies were included if the follow-up time was at least 1 year.
Studies were excluded when the recurrence rate could not be related
to a specific radiation dose or the number of cases per dose group
was smaller than 10.
For comparison of the different radiation doses and schedules that
have been described in the literature, BEDs were calculated by use
of the linear–quadratic (LQ)–BED concept. The occurrence of a bi-
ologic effect (E) depends on the dose in a linear and quadratic fash-
ion: E = n(ad + bd2), with n being the number of fractions, d being
the dose per fraction, and a and b being parameters that determine
the initial slope and curvature of the underlying cell survival curve.
From that equation, the BED can be calculated as follows: BED =
nd[1 + d/(a/b)] (10, 11).
For regimens with different overall treatment times, a correction
for proliferation can be applied. For proliferating normal tissues,
values of 0.8 to 1.3 Gy/d are frequently applied (12, 13). We applied
a value of 1 Gy/d for treatment times greater than 7 days. Pterygia
were treated especially with 90Sr b-radiation, whereas keloids
were treated with a diversity of radiation modalities: kilovolt X-
rays, 90Sr beta rays, 192Ir gamma rays, and megavolt electrons.
Corrections for differences in relative biologic effectiveness were
applied as described by Kal and Veen (6).
It is widely accepted that the a/b is equal to about 10 Gy for acute-
reacting tissues; it is in the range of 1 to 3 Gy for late-reacting tis-
sues. For keloid and pterygium as acute-reacting tissues, we applied
a/b equal to 10 Gy.
It is the strength of the LQ–BED concept that for a specific isoef-
fect, the BED values are equal for treatments with different fraction-
ation regimens.
Curve fitting was applied by use of Microsoft Excel (Microsoft
Corp., Redmond, WA) for logarithmic and linear fitting.
RESULTS
We identified 27 articles regarding keloid recurrence (2,
14–39), of which 19 (2, 14–31) were described earlier (6).
Table 1 shows the recurrence rate of keloids after radiation
therapy and the calculated BED values. The total number
of keloids in these studies was 1,945.
In most of the reports the total radiation dose administered
to the keloids was given within 1 week after surgery. In six
reports the overall treatment time exceeded 1 week (2, 15,
22, 23, 28, 34); as a consequence, the BED was corrected
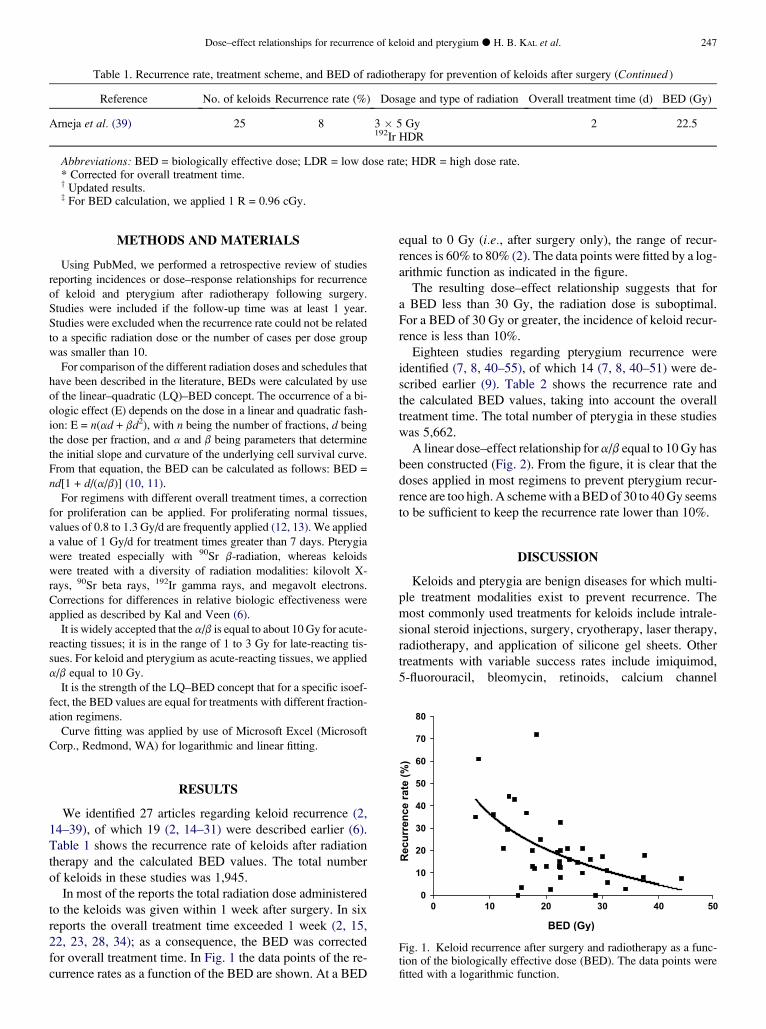
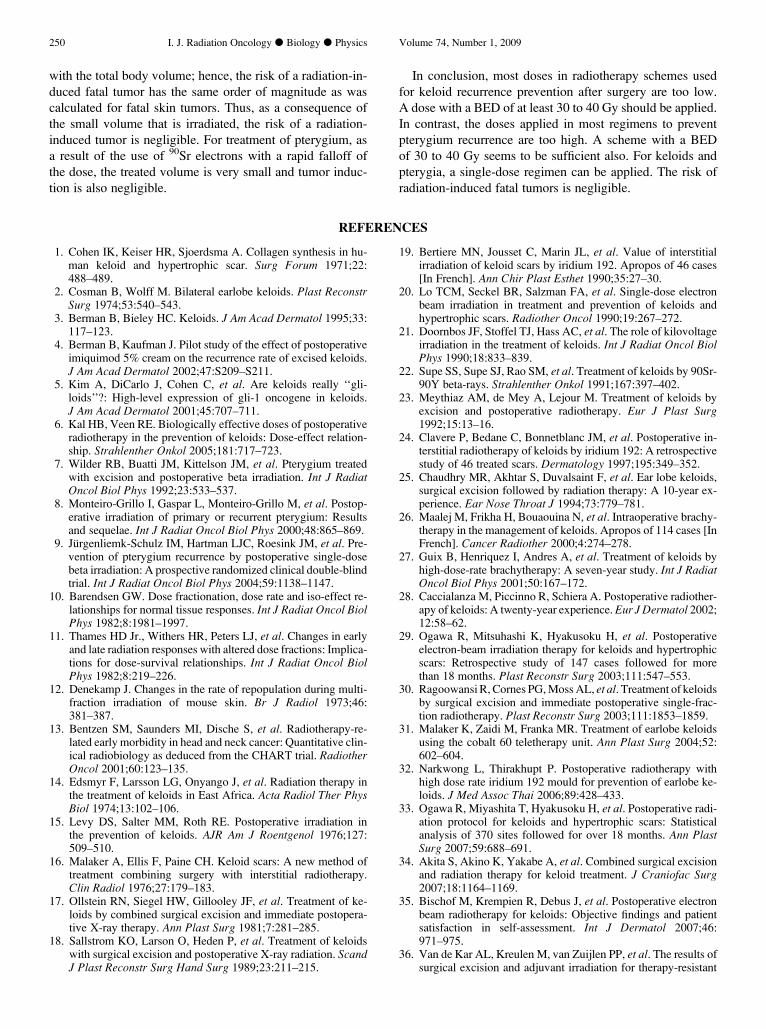
for overall treatment time. In Fig. 1 the data points of the re-
currence rates as a function of the BED are shown. At a BED
equal to 0 Gy (i.e., after surgery only), the range of recur-
rences is 60% to 80% (2). The data points were fitted by a log-
arithmic function as indicated in the figure.
The resulting dose–effect relationship suggests that for
a BED less than 30 Gy, the radiation dose is suboptimal.
For a BED of 30 Gy or greater, the incidence of keloid recur-
rence is less than 10%.
Eighteen studies regarding pterygium recurrence were
identified (7, 8, 40–55), of which 14 (7, 8, 40–51) were de-
scribed earlier (9). Table 2 shows the recurrence rate and
the calculated BED values, taking into account the overall
treatment time. The total number of pterygia in these studies
was 5,662.
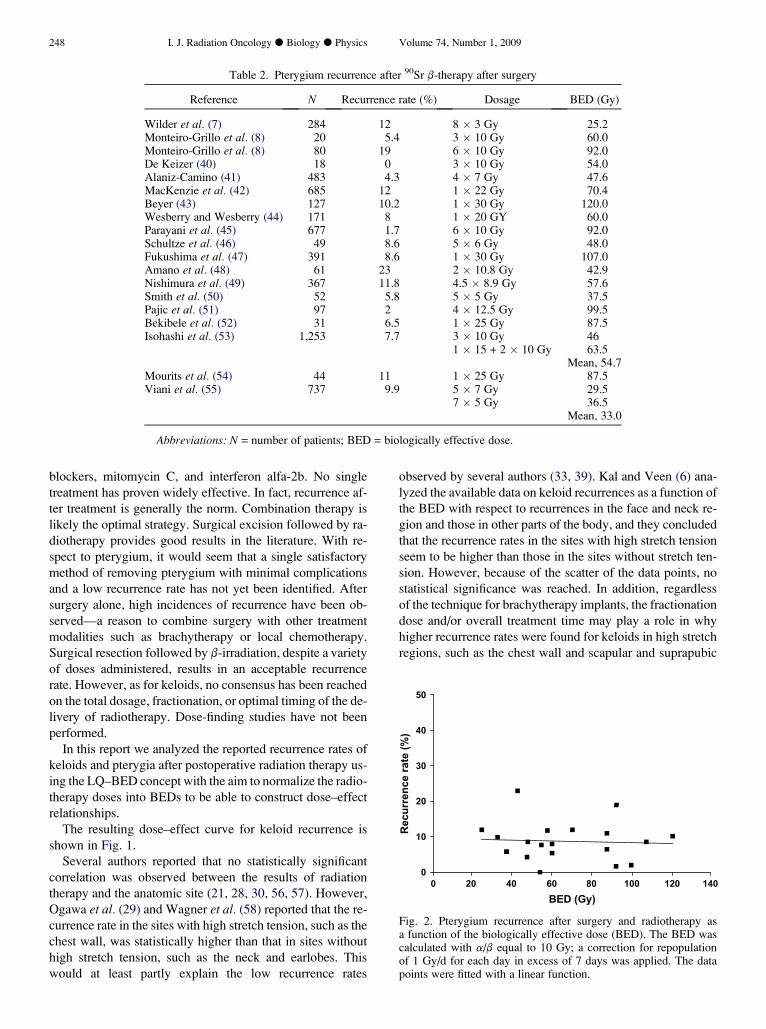
A linear dose–effect relationship for a/b equal to 10 Gy has
been constructed (Fig. 2). From the figure, it is clear that the
doses applied in most regimens to prevent pterygium recur-
rence are too high. A scheme with a BED of 30 to 40 Gy seems
to be sufficient to keep the recurrence rate lower than 10%.
DISCUSSION
Keloids and pterygia are benign diseases for which multi-
ple treatment modalities exist to prevent recurrence. The
most commonly used treatments for keloids include intrale-
sional steroid injections, surgery, cryotherapy, laser therapy,
radiotherapy, and application of silicone gel sheets. Other
treatments with variable success rates include imiquimod,
5-fluorouracil, bleomycin, retinoids, calcium channel
0
10
20
30
40
50
60
70
80
0 10 20 30 40 50
BED (Gy)
Recu
rren
ce rate (%
)
Fig. 1. Keloid recurrence after surgery and radiotherapy as a func-tion of the biologically effective dose (BED). The data points werefitted with a logarithmic function.
248 I. J. Radiation Oncology d Biology d Physics Volume 74, Number 1, 2009
Table 2. Pterygium recurrence after 90Sr b-therapy after surgery
Reference N Recurrence rate (%) Dosage BED (Gy)
Wilder et al. (7) 284 12 8 � 3 Gy 25.2Monteiro-Grillo et al. (8) 20 5.4 3 � 10 Gy 60.0Monteiro-Grillo et al. (8) 80 19 6 � 10 Gy 92.0De Keizer (40) 18 0 3 � 10 Gy 54.0Alaniz-Camino (41) 483 4.3 4 � 7 Gy 47.6MacKenzie et al. (42) 685 12 1 � 22 Gy 70.4Beyer (43) 127 10.2 1 � 30 Gy 120.0Wesberry and Wesberry (44) 171 8 1 � 20 GY 60.0Parayani et al. (45) 677 1.7 6 � 10 Gy 92.0Schultze et al. (46) 49 8.6 5 � 6 Gy 48.0Fukushima et al. (47) 391 8.6 1 � 30 Gy 107.0Amano et al. (48) 61 23 2 � 10.8 Gy 42.9Nishimura et al. (49) 367 11.8 4.5 � 8.9 Gy 57.6Smith et al. (50) 52 5.8 5 � 5 Gy 37.5Pajic et al. (51) 97 2 4 � 12.5 Gy 99.5Bekibele et al. (52) 31 6.5 1 � 25 Gy 87.5Isohashi et al. (53) 1,253 7.7 3 � 10 Gy 46
1 � 15 + 2 � 10 Gy 63.5Mean, 54.7
Mourits et al. (54) 44 11 1 � 25 Gy 87.5Viani et al. (55) 737 9.9 5 � 7 Gy 29.5
7 � 5 Gy 36.5Mean, 33.0
Abbreviations: N = number of patients; BED = biologically effective dose.
blockers, mitomycin C, and interferon alfa-2b. No single
treatment has proven widely effective. In fact, recurrence af-
ter treatment is generally the norm. Combination therapy is
likely the optimal strategy. Surgical excision followed by ra-
diotherapy provides good results in the literature. With re-
spect to pterygium, it would seem that a single satisfactory
method of removing pterygium with minimal complications
and a low recurrence rate has not yet been identified. After
surgery alone, high incidences of recurrence have been ob-
served—a reason to combine surgery with other treatment
modalities such as brachytherapy or local chemotherapy.
Surgical resection followed by b-irradiation, despite a variety
of doses administered, results in an acceptable recurrence
rate. However, as for keloids, no consensus has been reached
on the total dosage, fractionation, or optimal timing of the de-
livery of radiotherapy. Dose-finding studies have not been
performed.
In this report we analyzed the reported recurrence rates of
keloids and pterygia after postoperative radiation therapy us-
ing the LQ–BED concept with the aim to normalize the radio-
therapy doses into BEDs to be able to construct dose–effect
relationships.
The resulting dose–effect curve for keloid recurrence is
shown in Fig. 1.
Several authors reported that no statistically significant
correlation was observed between the results of radiation
therapy and the anatomic site (21, 28, 30, 56, 57). However,
Ogawa et al. (29) and Wagner et al. (58) reported that the re-
currence rate in the sites with high stretch tension, such as the
chest wall, was statistically higher than that in sites without
high stretch tension, such as the neck and earlobes. This
would at least partly explain the low recurrence rates
observed by several authors (33, 39). Kal and Veen (6) ana-
lyzed the available data on keloid recurrences as a function of
the BED with respect to recurrences in the face and neck re-
gion and those in other parts of the body, and they concluded
that the recurrence rates in the sites with high stretch tension
seem to be higher than those in the sites without stretch ten-
sion. However, because of the scatter of the data points, no
statistical significance was reached. In addition, regardless
of the technique for brachytherapy implants, the fractionation
dose and/or overall treatment time may play a role in why
higher recurrence rates were found for keloids in high stretch
regions, such as the chest wall and scapular and suprapubic
0
10
20
30
40
50
0 20 40 60 80 100 120 140
BED (Gy)
Recu
rren
ce rate (%
)
Fig. 2. Pterygium recurrence after surgery and radiotherapy asa function of the biologically effective dose (BED). The BED wascalculated with a/b equal to 10 Gy; a correction for repopulationof 1 Gy/d for each day in excess of 7 days was applied. The datapoints were fitted with a linear function.
Dose–effect relationships for recurrence of keloid and pterygium d H. B. KAL et al. 249
regions, than in regions without high stretch tension, such as
the earlobe.
Figure 1 indicates that a BED of at least 30 to 40 Gy should
be applied to keep the recurrence rate lower than 10%. A
BED of 30 to 40 Gy can be obtained with, for instance, a sin-
gle acute dose of 13 to 15 Gy, two fractions of 8.5 to 10 Gy or
three fractions of 6 to 7.5 Gy, or a single dose of 27 Gy
applied at a low dose rate. The radiation treatment should
be administered within 2 days after surgery.
For the prevention of pterygium recurrence after surgery,90Sr b-irradiation has a long history as a treatment modality
in ophthalmology. 90Sr treatment is performed with an oph-
thalmic applicator (59) and is therefore a convenient and
practical radiation method and has the advantage of minimal
tissue penetration. It has consistently been shown to be effec-
tive. However, no consensus has been reached on the total
dosage, fractionation, or optimal timing of the delivery of
radiotherapy.
From Fig. 2, it is clear that for a BED of 30 Gy or greater,
the mean recurrence rate of pterygium is lower than 10%. It
also indicates that most of the treatments that have been re-
ported in the literature are applied with doses above this
BED value. On the basis of a review of the literature, Hirst
(60) concluded that the most commonly administered physi-
cal dose is 15 Gy in either a single dose or divided doses. We
advocate a single dose of 13 to 15 Gy, which is equivalent to
a BED of 30 to 40 Gy. For equal effectiveness, when fraction-
ated radiotherapy is used, the total dose should be higher, for
example, 17 to 20 Gy in two fractions. It would be worth-
while to conduct a randomized trial comparing schemes
with a BED of 30 to 40 Gy with currently used schemes
with higher BED values. If the results at the lower dose are
equal to those at the higher dose schemes, high-dose applica-
tion should be abandoned (i.e., the principle of keeping the
dose as low as reasonably achievable).
With respect to the timing of the radiotherapy, Isohashi
et al. (53) reported that b-irradiation immediately given after
surgery, within 2 h, resulted in a higher recurrence rate than
when given with an interval of more than 2 h, even in pa-
tients who received identical doses. Other reports indicated
a better control rate in patients treated 1 to 3 days after sur-
gery than in those treated more than 3 days after surgery.
Similar to the findings for keloids, it is likely that a longer
delay in delivering the radiotherapy results in a higher recur-
rence rate (6).
Keloids are composed of intrinsically normal polyclonal
fibroblasts, which respond to an abnormal extracellular sig-
nal, resulting in increased production of scar tissue (61).
An important extracellular factor to induce pterygium is
UV radiation. UV radiation induces secretion of cytokines,
and these may activate pterygium fibroblasts, resulting in
overgrowth of the conjunctiva. Thus, in both keloid and
pterygium formation, activated fibroblasts play an important
role. Therefore it is worthwhile to determine whether the
dose–effect relationships derived for keloid and pterygium
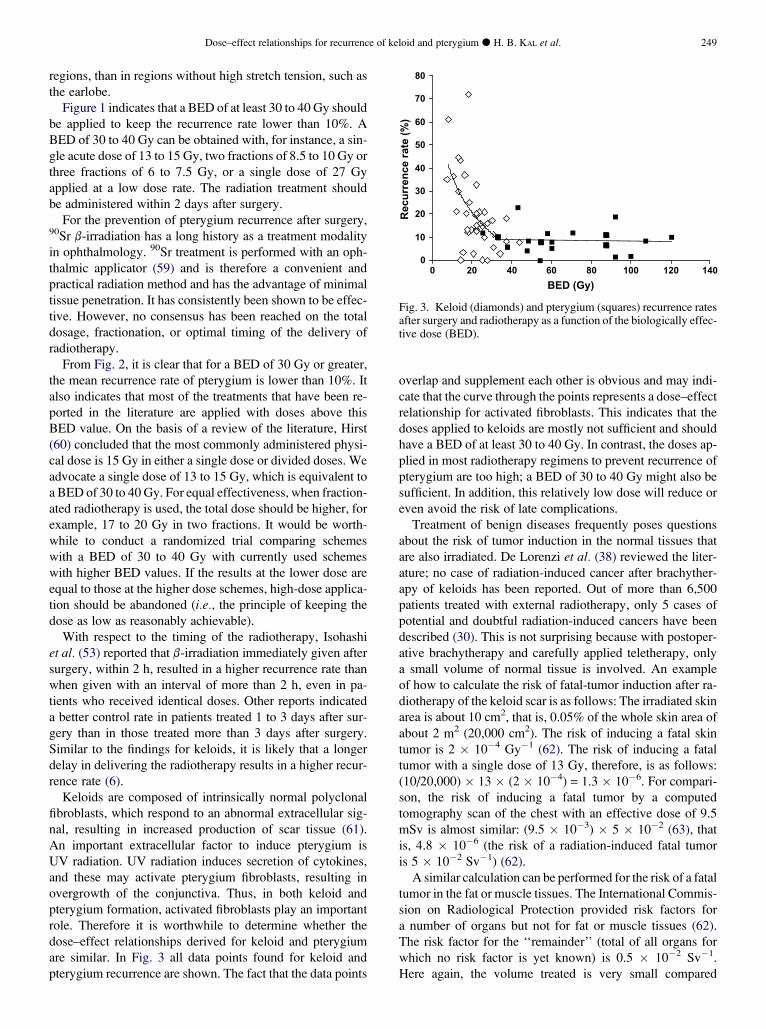
are similar. In Fig. 3 all data points found for keloid and
pterygium recurrence are shown. The fact that the data points
0
10
20
30
40
50
60
70
80
0 20 40 60 80 100 120 140
BED (Gy)
Recu
rren
ce rate (%
)
Fig. 3. Keloid (diamonds) and pterygium (squares) recurrence ratesafter surgery and radiotherapy as a function of the biologically effec-tive dose (BED).
overlap and supplement each other is obvious and may indi-
cate that the curve through the points represents a dose–effect
relationship for activated fibroblasts. This indicates that the
doses applied to keloids are mostly not sufficient and should
have a BED of at least 30 to 40 Gy. In contrast, the doses ap-
plied in most radiotherapy regimens to prevent recurrence of
pterygium are too high; a BED of 30 to 40 Gy might also be
sufficient. In addition, this relatively low dose will reduce or
even avoid the risk of late complications.
Treatment of benign diseases frequently poses questions
about the risk of tumor induction in the normal tissues that
are also irradiated. De Lorenzi et al. (38) reviewed the liter-
ature; no case of radiation-induced cancer after brachyther-
apy of keloids has been reported. Out of more than 6,500
patients treated with external radiotherapy, only 5 cases of
potential and doubtful radiation-induced cancers have been
described (30). This is not surprising because with postoper-
ative brachytherapy and carefully applied teletherapy, only
a small volume of normal tissue is involved. An example
of how to calculate the risk of fatal-tumor induction after ra-
diotherapy of the keloid scar is as follows: The irradiated skin
area is about 10 cm2, that is, 0.05% of the whole skin area of
about 2 m2 (20,000 cm2). The risk of inducing a fatal skin
tumor is 2 � 10�4 Gy�1 (62). The risk of inducing a fatal
tumor with a single dose of 13 Gy, therefore, is as follows:
(10/20,000) � 13 � (2 � 10�4) = 1.3 � 10�6. For compari-
son, the risk of inducing a fatal tumor by a computed
tomography scan of the chest with an effective dose of 9.5
mSv is almost similar: (9.5 � 10�3) � 5 � 10�2 (63), that
is, 4.8 � 10�6 (the risk of a radiation-induced fatal tumor
is 5 � 10�2 Sv�1) (62).
A similar calculation can be performed for the risk of a fatal
tumor in the fat or muscle tissues. The International Commis-
sion on Radiological Protection provided risk factors for
a number of organs but not for fat or muscle tissues (62).
The risk factor for the ‘‘remainder’’ (total of all organs for
which no risk factor is yet known) is 0.5 � 10�2 Sv�1.
Here again, the volume treated is very small compared
250 I. J. Radiation Oncology d Biology d Physics Volume 74, Number 1, 2009
with the total body volume; hence, the risk of a radiation-in-
duced fatal tumor has the same order of magnitude as was
calculated for fatal skin tumors. Thus, as a consequence of
the small volume that is irradiated, the risk of a radiation-
induced tumor is negligible. For treatment of pterygium, as
a result of the use of 90Sr electrons with a rapid falloff of
the dose, the treated volume is very small and tumor induc-
tion is also negligible.
In conclusion, most doses in radiotherapy schemes used
for keloid recurrence prevention after surgery are too low.
A dose with a BED of at least 30 to 40 Gy should be applied.
In contrast, the doses applied in most regimens to prevent
pterygium recurrence are too high. A scheme with a BED
of 30 to 40 Gy seems to be sufficient also. For keloids and
pterygia, a single-dose regimen can be applied. The risk of
radiation-induced fatal tumors is negligible.
REFERENCES
1. Cohen IK, Keiser HR, Sjoerdsma A. Collagen synthesis in hu-man keloid and hypertrophic scar. Surg Forum 1971;22:488–489.
2. Cosman B, Wolff M. Bilateral earlobe keloids. Plast ReconstrSurg 1974;53:540–543.
3. Berman B, Bieley HC. Keloids. J Am Acad Dermatol 1995;33:117–123.
4. Berman B, Kaufman J. Pilot study of the effect of postoperativeimiquimod 5% cream on the recurrence rate of excised keloids.J Am Acad Dermatol 2002;47:S209–S211.
5. Kim A, DiCarlo J, Cohen C, et al. Are keloids really ‘‘gli-loids’’?: High-level expression of gli-1 oncogene in keloids.J Am Acad Dermatol 2001;45:707–711.
6. Kal HB, Veen RE. Biologically effective doses of postoperativeradiotherapy in the prevention of keloids: Dose-effect relation-ship. Strahlenther Onkol 2005;181:717–723.
7. Wilder RB, Buatti JM, Kittelson JM, et al. Pterygium treatedwith excision and postoperative beta irradiation. Int J RadiatOncol Biol Phys 1992;23:533–537.
8. Monteiro-Grillo I, Gaspar L, Monteiro-Grillo M, et al. Postop-erative irradiation of primary or recurrent pterygium: Resultsand sequelae. Int J Radiat Oncol Biol Phys 2000;48:865–869.
9. Jurgenliemk-Schulz IM, Hartman LJC, Roesink JM, et al. Pre-vention of pterygium recurrence by postoperative single-dosebeta irradiation: A prospective randomized clinical double-blindtrial. Int J Radiat Oncol Biol Phys 2004;59:1138–1147.
10. Barendsen GW. Dose fractionation, dose rate and iso-effect re-lationships for normal tissue responses. Int J Radiat Oncol BiolPhys 1982;8:1981–1997.
11. Thames HD Jr., Withers HR, Peters LJ, et al. Changes in earlyand late radiation responses with altered dose fractions: Implica-tions for dose-survival relationships. Int J Radiat Oncol BiolPhys 1982;8:219–226.
12. Denekamp J. Changes in the rate of repopulation during multi-fraction irradiation of mouse skin. Br J Radiol 1973;46:381–387.
13. Bentzen SM, Saunders MI, Dische S, et al. Radiotherapy-re-lated early morbidity in head and neck cancer: Quantitative clin-ical radiobiology as deduced from the CHART trial. RadiotherOncol 2001;60:123–135.
14. Edsmyr F, Larsson LG, Onyango J, et al. Radiation therapy inthe treatment of keloids in East Africa. Acta Radiol Ther PhysBiol 1974;13:102–106.
15. Levy DS, Salter MM, Roth RE. Postoperative irradiation inthe prevention of keloids. AJR Am J Roentgenol 1976;127:509–510.
16. Malaker A, Ellis F, Paine CH. Keloid scars: A new method oftreatment combining surgery with interstitial radiotherapy.Clin Radiol 1976;27:179–183.
17. Ollstein RN, Siegel HW, Gillooley JF, et al. Treatment of ke-loids by combined surgical excision and immediate postopera-tive X-ray therapy. Ann Plast Surg 1981;7:281–285.
18. Sallstrom KO, Larson O, Heden P, et al. Treatment of keloidswith surgical excision and postoperative X-ray radiation. ScandJ Plast Reconstr Surg Hand Surg 1989;23:211–215.
19. Bertiere MN, Jousset C, Marin JL, et al. Value of interstitialirradiation of keloid scars by iridium 192. Apropos of 46 cases[In French]. Ann Chir Plast Esthet 1990;35:27–30.
20. Lo TCM, Seckel BR, Salzman FA, et al. Single-dose electronbeam irradiation in treatment and prevention of keloids andhypertrophic scars. Radiother Oncol 1990;19:267–272.
21. Doornbos JF, Stoffel TJ, Hass AC, et al. The role of kilovoltageirradiation in the treatment of keloids. Int J Radiat Oncol BiolPhys 1990;18:833–839.
22. Supe SS, Supe SJ, Rao SM, et al. Treatment of keloids by 90Sr-90Y beta-rays. Strahlenther Onkol 1991;167:397–402.
23. Meythiaz AM, de Mey A, Lejour M. Treatment of keloids byexcision and postoperative radiotherapy. Eur J Plast Surg1992;15:13–16.
24. Clavere P, Bedane C, Bonnetblanc JM, et al. Postoperative in-terstitial radiotherapy of keloids by iridium 192: A retrospectivestudy of 46 treated scars. Dermatology 1997;195:349–352.
25. Chaudhry MR, Akhtar S, Duvalsaint F, et al. Ear lobe keloids,surgical excision followed by radiation therapy: A 10-year ex-perience. Ear Nose Throat J 1994;73:779–781.
26. Maalej M, Frikha H, Bouaouina N, et al. Intraoperative brachy-therapy in the management of keloids. Apropos of 114 cases [InFrench]. Cancer Radiother 2000;4:274–278.
27. Guix B, Henriquez I, Andres A, et al. Treatment of keloids byhigh-dose-rate brachytherapy: A seven-year study. Int J RadiatOncol Biol Phys 2001;50:167–172.
28. Caccialanza M, Piccinno R, Schiera A. Postoperative radiother-apy of keloids: A twenty-year experience. Eur J Dermatol 2002;12:58–62.
29. Ogawa R, Mitsuhashi K, Hyakusoku H, et al. Postoperativeelectron-beam irradiation therapy for keloids and hypertrophicscars: Retrospective study of 147 cases followed for morethan 18 months. Plast Reconstr Surg 2003;111:547–553.
30. Ragoowansi R, Cornes PG, Moss AL, et al. Treatment of keloidsby surgical excision and immediate postoperative single-frac-tion radiotherapy. Plast Reconstr Surg 2003;111:1853–1859.
31. Malaker K, Zaidi M, Franka MR. Treatment of earlobe keloidsusing the cobalt 60 teletherapy unit. Ann Plast Surg 2004;52:602–604.
32. Narkwong L, Thirakhupt P. Postoperative radiotherapy withhigh dose rate iridium 192 mould for prevention of earlobe ke-loids. J Med Assoc Thai 2006;89:428–433.
33. Ogawa R, Miyashita T, Hyakusoku H, et al. Postoperative radi-ation protocol for keloids and hypertrophic scars: Statisticalanalysis of 370 sites followed for over 18 months. Ann PlastSurg 2007;59:688–691.
34. Akita S, Akino K, Yakabe A, et al. Combined surgical excisionand radiation therapy for keloid treatment. J Craniofac Surg2007;18:1164–1169.
35. Bischof M, Krempien R, Debus J, et al. Postoperative electronbeam radiotherapy for keloids: Objective findings and patientsatisfaction in self-assessment. Int J Dermatol 2007;46:971–975.
36. Van de Kar AL, Kreulen M, van Zuijlen PP, et al. The results ofsurgical excision and adjuvant irradiation for therapy-resistant
Dose–effect relationships for recurrence of keloid and pterygium d H. B. KAL et al. 251
keloids: A prospective clinical outcome study. Plast ReconstrSurg 2007;119:2248–2254.
37. Veen RE, Kal HB. Postoperative high-dose-rate brachytherapyin the prevention of keloids. Int J Radiat Oncol Biol Phys 2007;69:1205–1208.
38. De Lorenzi F, Tielemans HJ, van der Hulst RR, et al. Is the treat-ment of keloid scars still a challenge in 2006? Ann Plast Surg2007;58:186–192.
39. Arneja JS, Singh GB, Dolynchuk KN, et al. Treatment of recur-rent earlobe keloids with surgery and high-dose-rate brachyther-apy. Plast Reconstr Surg 2008;121:95–99.
40. De Keizer RJW. Pterygium excision with or without postoper-ative irradiation, a double-blind study. Doc Ophthalmol 1982;52:309–315.
41. Alaniz-Camino F. The use of postoperative beta radiation in thetreatment of pterygia. Ophthalmic Surg 1982;3:1022–1025.
42. MacKenzie FS, Hirst LW, Kynaston B, et al. Recurrence rateand complications after beta irradiation for pterygia. Ophthal-mology 1991;98:1776–1780.
43. Beyer DC. Pterygia: Single-fraction post-operative beta irradia-tion. Radiology 1991;178:569–571.
44. Wesberry JM Jr., Wesberry JM Sr. Optimal use of beta irradia-tion in the treatment of pterygia. South Med J 1993;86.633–337.
45. Parayani SB, Scott WP, Wells JW Jr., et al. Management ofpterygium with surgery and radiation therapy. The North Flor-ida Pterygium Study Group. Int J Radiat Oncol Biol Phys 1994;28:101–103.
46. Schultze J, Hinrichs M, Kimmig B. The results of strontium-90contact therapy to prevent the recurrence of pterygium. Ger JOphthalmol 1996;5:207–210.
47. Fukushima S, Onoue T, Onoue T, et al. Post-operative irradia-tion of pterygium with 90Sr eye applicator. Int J Radiat OncolBiol Phys 1999;43:597–600.
48. Amano S, Motoyama Y, Oshika T, et al. Comparative study ofintraoperative mitomycin C and beta irradiation in pterygiumsurgery. Br J Ophthalmol 2000;84:618–621.
49. Nishimura Y, Nakai A, Yoshimasu T, et al. Long-term results offractionated strontium-90 therapy for pterygia. Int J Radiat On-col Biol Phys 2000;46:137–141.
50. Smith RA, Dzugan SA, Kosko P. Postoperative beta irradiationfor control pterygium. J Miss State Med Assoc 2001;42:167–169.
51. Pajic B, Pugnale-Verillotte N, Greiner RH, et al. Results ofstrontium-yttrium-90 for pterygia [In French]. J Fr Ophthalmol2002;25:473–479.
52. Bekibele CO, Baiyeroju AM, Ajayi BG. 5-Fluorouracil vs.beta-irradiation in the prevention of pterygium recurrence. IntJ Clin Pract 2004;58:920–923.
53. Isohashi F, Inoue T, Xing S, et al. Postoperative irradiation forpterygium: Retrospective analysis of 1,253 patients from theOsaka University Hospital. Strahlenther Onkol 2006;182:437–442.
54. Mourits MP, Wyrdeman HK, Jurgenliemk-Schulz IM, et al. Fa-vorable long-term results of primary pterygium removal by baresclera extirpation followed by a single 90Strontium application.Eur J Ophthalmol 2008;18:327–331.
55. Viani GA, Stefano EJ, De Fendi LI, et al. Long-term results andprognostic factors of fractionated strontium-90 eye applicatorfor pterygium. Int J Radiat Oncol Biol Phys 2008;72:1174–1179.
56. Klumpar DI, Murray JC, Anscher M. Keloids treated with exci-sion followed by radiation therapy. J Am Acad Dermatol 1994;31:225–231.
57. Maarouf M, Schleicher U, Schmachtenberg A, et al. Radiother-apy in the management of keloids. Clinical experience withelectron beam irradiation and comparison with X-ray therapy.Strahlenther Onkol 2002;178:330–335.
58. Wagner W, Alfrink M, Micke O, et al. Results of prophylacticirradiation in patients with resected keloids—A retrospectiveanalysis. Acta Oncol 2000;39:217–220.
59. Sinclair WK, Trott NG. The construction and measurement ofbeta-ray applicators for use in ophthalmology. Br J Radiol1956;29:15–23.
60. Hirst LW. The treatment of pterygium. Surv Ophthalmol 2003;48:145–180.
61. Chevray PM, Manson PN. Keloid scars are formed by poly-clonal fibroblasts. Ann Plast Surg 2004;52:605–608.
62. ICRP 1991. International Commission on Radiological Protec-tion. 1990 Recommendations of the International Commissionon Radiological Protection. ICRP Publication 60. Ann ICRP1991;21:1–201.
63. Nishizawa K, Mori S, Ohno M, et al. Patient dose estimation formulti-detector-row CT examinations. Radiat Prot Dosimetry2008;128:98–105.
![l enta l i ic lOp Journal of Clinical & Experimental tCh f ......Recurrence of pterygium [1] following primary pterygium excision with conjunctival autograft is a common sequel that](https://img.dokumen.tips/doc/110x75/5e546962f7df7707045f8c0b/l-enta-l-i-ic-lop-journal-of-clinical-experimental-tch-f-recurrence.jpg)




























