Embed Size (px)
Citation preview
U L T R A S O U N DC L I N I C S
Ultrasound Clin 1 (2006) 293–301
293
Doppler Ultrasound in ObstetricsAlfred Abuhamad, MD
& Fetal arterial Doppler & Fetal cardiac Doppler
Umbilical arterial circulationMiddle cerebral circulationFetal venous DopplerDepartment of Obstetrics and Gynecology, Eastern Vi8254 Fairfax Avenue, Norfolk, VA 23507, USAE-mail address: [email protected]
1556-858X/06/$ – see front matter © 2006 Elsevier Inc. All rightsultrasound.theclinics.com
& Fetal Doppler and intrauterine growthrestriction
& References
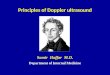
The Doppler effect, which was first reported byChristian Doppler in 1842 [1,2], describes the ap-parent variation in frequency of a light or a soundwave as the source of the wave approaches ormoves away, relative to an observer. The traditionalexample that is given to describe this physical phe-nomenon is the apparent change in sound level ofa train as the train approaches and then departs astation. The sound seems higher in pitch as thetrain approaches the station and seems lower inpitch as the train departs the station. This apparentchange in sound pitch, or what is termed the fre-quency shift, is proportional to the speed of move-ment of the sound-emitting source. In clinicalapplications, when ultrasound with a certain fre-quency (fo) is used to insonate a certain bloodvessel, the reflected frequency (fd) or frequencyshift is directly proportional to the speed withwhich the red blood cells are moving (blood flowvelocity) within that particular vessel. This fre-quency shift of the returning signal is displayed ina graphic form as a time-dependent plot. In thisdisplay, the vertical axis represents the frequencyshift and the horizontal axis represents the tem-poral change of this frequency shift as it relays tothe events of the cardiac cycle [Fig. 1]. This fre-quency shift is highest during systole, when theblood flow is at its fastest, and lowest during end-diastole, when the blood flow is at its slowest in theperipheral circulation. Given that the velocity offlow in a particular vascular bed is inversely pro-
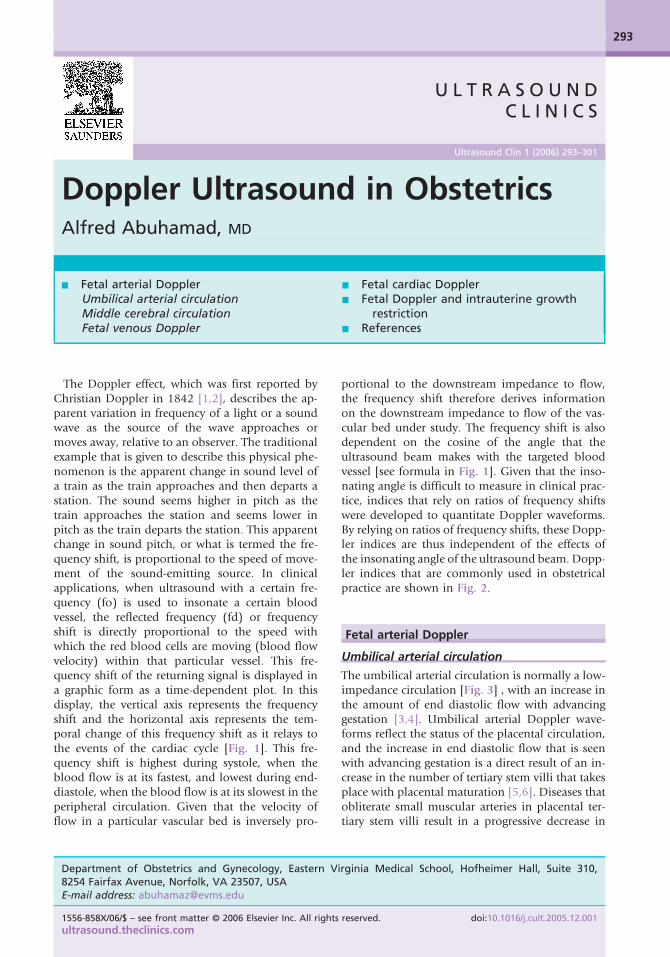
portional to the downstream impedance to flow,the frequency shift therefore derives informationon the downstream impedance to flow of the vas-cular bed under study. The frequency shift is alsodependent on the cosine of the angle that theultrasound beam makes with the targeted bloodvessel [see formula in Fig. 1]. Given that the inso-nating angle is difficult to measure in clinical prac-tice, indices that rely on ratios of frequency shiftswere developed to quantitate Doppler waveforms.By relying on ratios of frequency shifts, these Dopp-ler indices are thus independent of the effects ofthe insonating angle of the ultrasound beam. Dopp-ler indices that are commonly used in obstetricalpractice are shown in Fig. 2.
Fetal arterial Doppler
Umbilical arterial circulation
The umbilical arterial circulation is normally a low-impedance circulation [Fig. 3] , with an increase inthe amount of end diastolic flow with advancinggestation [3,4]. Umbilical arterial Doppler wave-forms reflect the status of the placental circulation,and the increase in end diastolic flow that is seenwith advancing gestation is a direct result of an in-crease in the number of tertiary stem villi that takesplace with placental maturation [5,6]. Diseases thatobliterate small muscular arteries in placental ter-tiary stem villi result in a progressive decrease in
rginia Medical School, Hofheimer Hall, Suite 310,
reserved. doi:10.1016/j.cult.2005.12.001
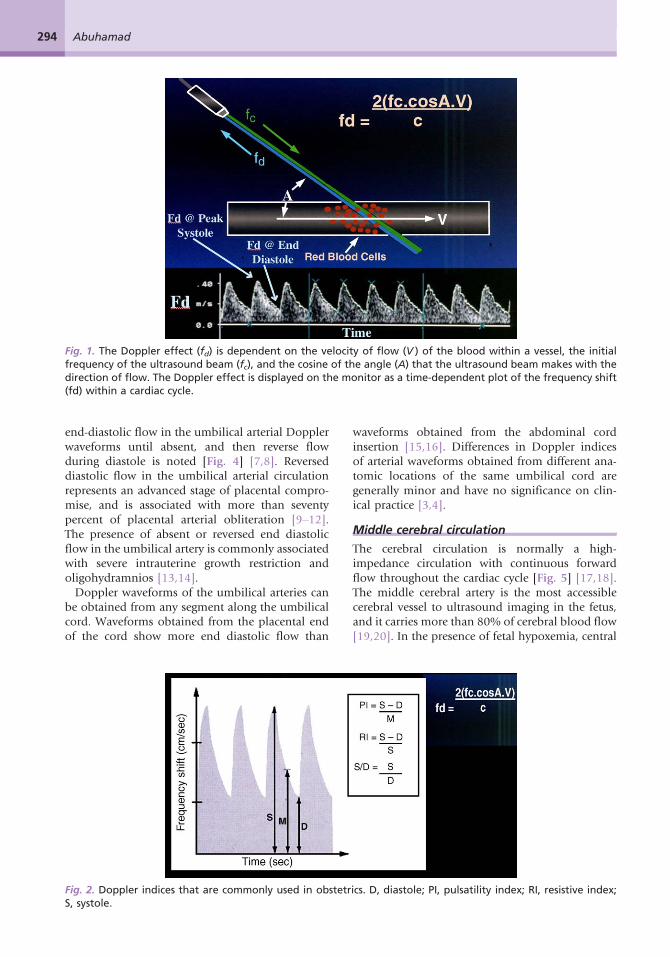
Fig. 1. The Doppler effect (fd) is dependent on the velocity of flow (V ) of the blood within a vessel, the initialfrequency of the ultrasound beam (fc), and the cosine of the angle (A) that the ultrasound beam makes with thedirection of flow. The Doppler effect is displayed on the monitor as a time-dependent plot of the frequency shift(fd) within a cardiac cycle.
294 Abuhamad
end-diastolic flow in the umbilical arterial Dopplerwaveforms until absent, and then reverse flowduring diastole is noted [Fig. 4] [7,8]. Reverseddiastolic flow in the umbilical arterial circulationrepresents an advanced stage of placental compro-mise, and is associated with more than seventypercent of placental arterial obliteration [9–12].The presence of absent or reversed end diastolicflow in the umbilical artery is commonly associatedwith severe intrauterine growth restriction andoligohydramnios [13,14].Doppler waveforms of the umbilical arteries can
be obtained from any segment along the umbilicalcord. Waveforms obtained from the placental endof the cord show more end diastolic flow than
Fig. 2. Doppler indices that are commonly used in obstetrS, systole.
waveforms obtained from the abdominal cordinsertion [15,16]. Differences in Doppler indicesof arterial waveforms obtained from different ana-tomic locations of the same umbilical cord aregenerally minor and have no significance on clin-ical practice [3,4].
Middle cerebral circulation
The cerebral circulation is normally a high-impedance circulation with continuous forwardflow throughout the cardiac cycle [Fig. 5] [17,18].The middle cerebral artery is the most accessiblecerebral vessel to ultrasound imaging in the fetus,and it carries more than 80% of cerebral blood flow[19,20]. In the presence of fetal hypoxemia, central
ics. D, diastole; PI, pulsatility index; RI, resistive index;
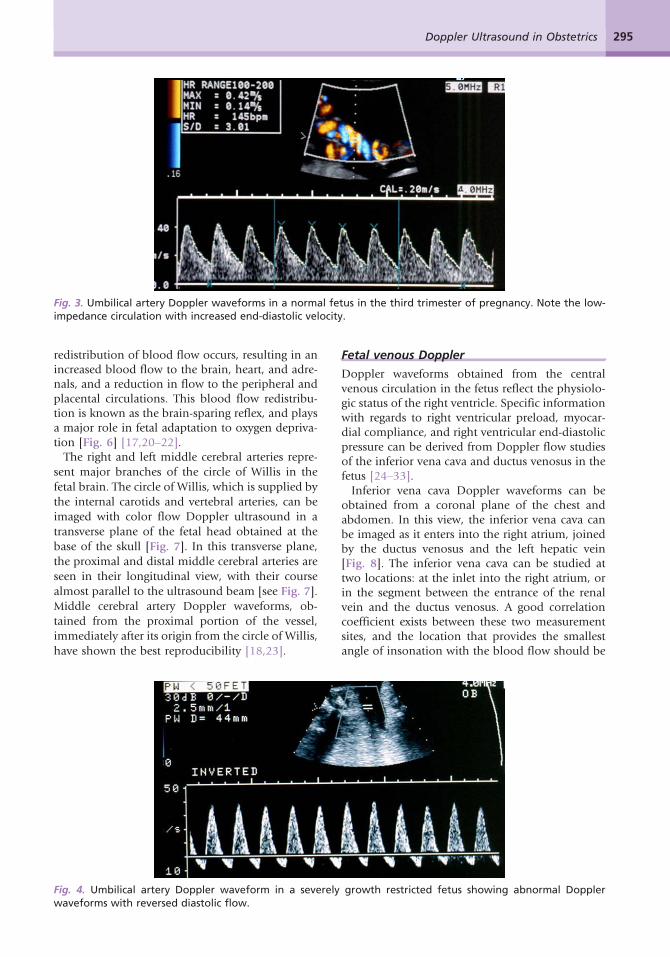
Fig. 3. Umbilical artery Doppler waveforms in a normal fetus in the third trimester of pregnancy. Note the low-impedance circulation with increased end-diastolic velocity.
295Doppler Ultrasound in Obstetrics
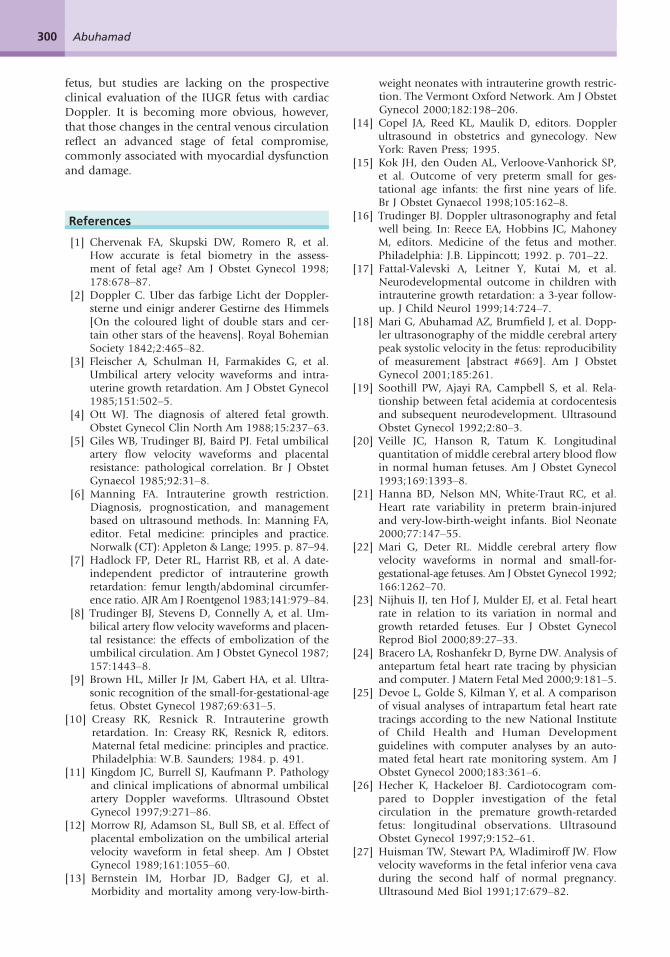
redistribution of blood flow occurs, resulting in anincreased blood flow to the brain, heart, and adre-nals, and a reduction in flow to the peripheral andplacental circulations. This blood flow redistribu-tion is known as the brain-sparing reflex, and playsa major role in fetal adaptation to oxygen depriva-tion [Fig. 6] [17,20–22].The right and left middle cerebral arteries repre-
sent major branches of the circle of Willis in the
fetal brain. The circle of Willis, which is supplied by
the internal carotids and vertebral arteries, can beimaged with color flow Doppler ultrasound in a
transverse plane of the fetal head obtained at the
base of the skull [Fig. 7]. In this transverse plane,
the proximal and distal middle cerebral arteries are
seen in their longitudinal view, with their course
almost parallel to the ultrasound beam [see Fig. 7].
Middle cerebral artery Doppler waveforms, ob-
tained from the proximal portion of the vessel,immediately after its origin from the circle of Willis,
have shown the best reproducibility [18,23].
Fig. 4. Umbilical artery Doppler waveform in a severelywaveforms with reversed diastolic flow.
Fetal venous Doppler
Doppler waveforms obtained from the centralvenous circulation in the fetus reflect the physiolo-gic status of the right ventricle. Specific informationwith regards to right ventricular preload, myocar-dial compliance, and right ventricular end-diastolicpressure can be derived from Doppler flow studiesof the inferior vena cava and ductus venosus in thefetus [24–33].Inferior vena cava Doppler waveforms can be
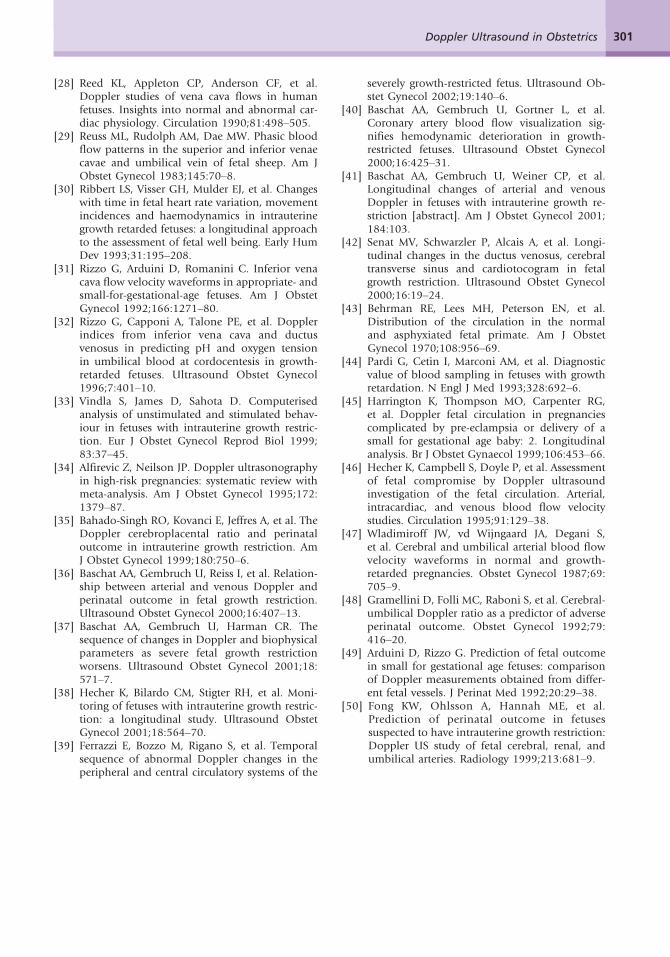
obtained from a coronal plane of the chest andabdomen. In this view, the inferior vena cava canbe imaged as it enters into the right atrium, joinedby the ductus venosus and the left hepatic vein[Fig. 8]. The inferior vena cava can be studied attwo locations: at the inlet into the right atrium, orin the segment between the entrance of the renalvein and the ductus venosus. A good correlationcoefficient exists between these two measurementsites, and the location that provides the smallestangle of insonation with the blood flow should be
growth restricted fetus showing abnormal Doppler
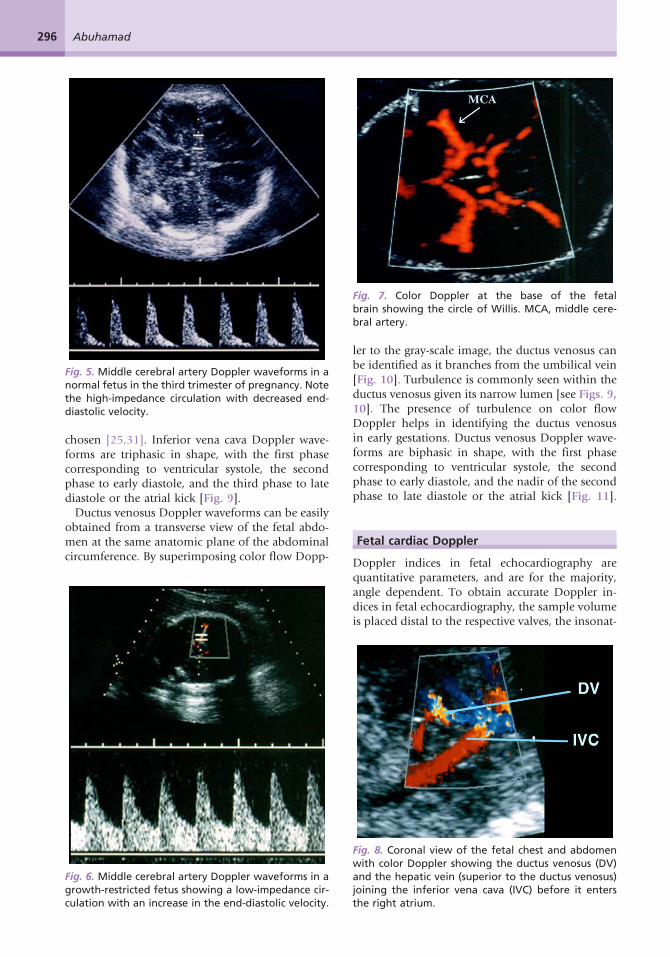
Fig. 5. Middle cerebral artery Doppler waveforms in anormal fetus in the third trimester of pregnancy. Notethe high-impedance circulation with decreased end-diastolic velocity.
Fig. 7. Color Doppler at the base of the fetalbrain showing the circle of Willis. MCA, middle cere-bral artery.
296 Abuhamad
chosen [25,31]. Inferior vena cava Doppler wave-forms are triphasic in shape, with the first phasecorresponding to ventricular systole, the secondphase to early diastole, and the third phase to latediastole or the atrial kick [Fig. 9].Ductus venosus Doppler waveforms can be easily
obtained from a transverse view of the fetal abdo-men at the same anatomic plane of the abdominalcircumference. By superimposing color flow Dopp-
Fig. 6. Middle cerebral artery Doppler waveforms in agrowth-restricted fetus showing a low-impedance cir-culation with an increase in the end-diastolic velocity.
ler to the gray-scale image, the ductus venosus canbe identified as it branches from the umbilical vein[Fig. 10]. Turbulence is commonly seen within theductus venosus given its narrow lumen [see Figs. 9,10]. The presence of turbulence on color flowDoppler helps in identifying the ductus venosusin early gestations. Ductus venosus Doppler wave-forms are biphasic in shape, with the first phasecorresponding to ventricular systole, the secondphase to early diastole, and the nadir of the secondphase to late diastole or the atrial kick [Fig. 11].
Fetal cardiac Doppler
Doppler indices in fetal echocardiography arequantitative parameters, and are for the majority,angle dependent. To obtain accurate Doppler in-dices in fetal echocardiography, the sample volumeis placed distal to the respective valves, the insonat-
Fig. 8. Coronal view of the fetal chest and abdomenwith color Doppler showing the ductus venosus (DV)and the hepatic vein (superior to the ductus venosus)joining the inferior vena cava (IVC) before it entersthe right atrium.
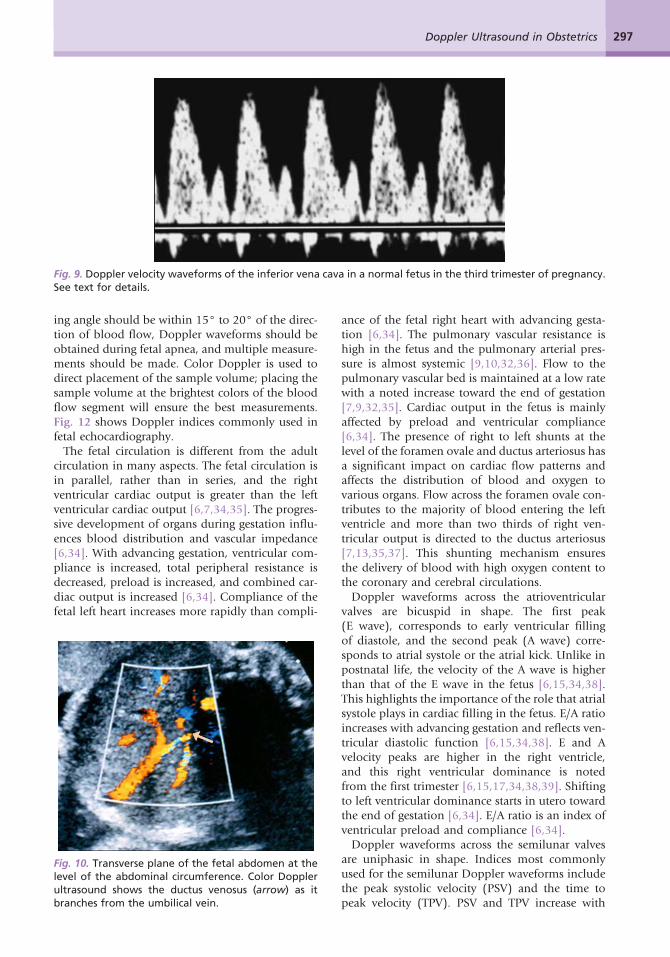
Fig. 9. Doppler velocity waveforms of the inferior vena cava in a normal fetus in the third trimester of pregnancy.See text for details.
297Doppler Ultrasound in Obstetrics
ing angle should be within 15° to 20° of the direc-tion of blood flow, Doppler waveforms should beobtained during fetal apnea, and multiple measure-ments should be made. Color Doppler is used todirect placement of the sample volume; placing thesample volume at the brightest colors of the bloodflow segment will ensure the best measurements.Fig. 12 shows Doppler indices commonly used infetal echocardiography.The fetal circulation is different from the adult
circulation in many aspects. The fetal circulation isin parallel, rather than in series, and the rightventricular cardiac output is greater than the leftventricular cardiac output [6,7,34,35]. The progres-sive development of organs during gestation influ-ences blood distribution and vascular impedance[6,34]. With advancing gestation, ventricular com-pliance is increased, total peripheral resistance isdecreased, preload is increased, and combined car-diac output is increased [6,34]. Compliance of thefetal left heart increases more rapidly than compli-
Fig. 10. Transverse plane of the fetal abdomen at thelevel of the abdominal circumference. Color Dopplerultrasound shows the ductus venosus (arrow) as itbranches from the umbilical vein.
ance of the fetal right heart with advancing gesta-tion [6,34]. The pulmonary vascular resistance ishigh in the fetus and the pulmonary arterial pres-sure is almost systemic [9,10,32,36]. Flow to thepulmonary vascular bed is maintained at a low ratewith a noted increase toward the end of gestation[7,9,32,35]. Cardiac output in the fetus is mainlyaffected by preload and ventricular compliance[6,34]. The presence of right to left shunts at thelevel of the foramen ovale and ductus arteriosus hasa significant impact on cardiac flow patterns andaffects the distribution of blood and oxygen tovarious organs. Flow across the foramen ovale con-tributes to the majority of blood entering the leftventricle and more than two thirds of right ven-tricular output is directed to the ductus arteriosus[7,13,35,37]. This shunting mechanism ensuresthe delivery of blood with high oxygen content tothe coronary and cerebral circulations.Doppler waveforms across the atrioventricular
valves are bicuspid in shape. The first peak(E wave), corresponds to early ventricular fillingof diastole, and the second peak (A wave) corre-sponds to atrial systole or the atrial kick. Unlike inpostnatal life, the velocity of the A wave is higherthan that of the E wave in the fetus [6,15,34,38].This highlights the importance of the role that atrialsystole plays in cardiac filling in the fetus. E/A ratioincreases with advancing gestation and reflects ven-tricular diastolic function [6,15,34,38]. E and Avelocity peaks are higher in the right ventricle,and this right ventricular dominance is notedfrom the first trimester [6,15,17,34,38,39]. Shiftingto left ventricular dominance starts in utero towardthe end of gestation [6,34]. E/A ratio is an index ofventricular preload and compliance [6,34].Doppler waveforms across the semilunar valves
are uniphasic in shape. Indices most commonlyused for the semilunar Doppler waveforms includethe peak systolic velocity (PSV) and the time topeak velocity (TPV). PSV and TPV increase with

Fig. 11. Doppler velocity waveforms of the ductus venosus in a normal fetus in the third trimester of pregnancy.See text for details.
298 Abuhamad
advancing gestation across the semilunar valves[2,3,5,6,8,13,19,21,23,33,34,37]. PSV is higheracross the aorta than across the pulmonary arterybecause of a decreased afterload and a smallerdiameter across the aorta [2,3,5,6,8,13,19,21,23,33,34,37]. These Doppler indices reflect ventricularcontractility, arterial pressures, and afterloads.
Fetal Doppler and intrauterine growthrestriction
Arterial Doppler abnormalities, at the level of theumbilical and middle cerebral arteries (brain-spar-ing reflex), confirm the presence of hypoxemia inthe growth-restricted fetus, and present early warn-ing signs. Once arterial centralization occurs, how-ever, no clear trend is noted in the observationalperiod, and thus arterial redistribution may not behelpful for the timing of the delivery [11,12,14,
Fig. 12. Doppler indices that are commonly used in fetal epeak velocity achieved during one cardiac cycle. (B) Accelerits peak in one cardiac cycle. (C ) Time velocity integral (TVI)TVI expresses the distance that the red blood cells would h
40–42]. On the other hand, the presence of re-versed diastolic flow in the umbilical arteries is asign of advanced fetal compromise, and strong con-sideration should be given for delivery, except forextreme prematurity. Cesarean section should begiven preference in this setting, because labor maycause further fetal compromise.The current literature suggests that venous Dopp-
ler abnormalities in the inferior vena cava andductus venosus and abnormal fetal heart rate moni-toring, even in its computerized version, followarterial Doppler abnormalities and are thus asso-ciated with a more advanced stage of fetal compro-mise [16,18,20,22,36–39,43,44].Furthermore, in the majority of severely growth-
restricted fetuses, sequential deterioration of ar-terial and venous Doppler precedes biophysicalprofile score deterioration [22,37]. At least one thirdof fetuses show early signs of circulatory deregula-
chocardiography. (A) Peak systolic velocity (PSV) is theation time (AT) is the time it takes the velocity to reachis the integral of the planimetric area under the curve.ave to cover with a constant area of the flow section.

299Doppler Ultrasound in Obstetrics
tion 1 week before biophysical profile deteriora-tion, and that in most cases, Doppler deteriorationpreceded biophysical profile deterioration by 1 day[22,37].The occurrence of such abnormal late stage
changes of vascular adaptation by the intrauterinegrowth-retarded (IUGR) fetus appears to be thebest predictor of perinatal death, independent ofgestational age and weight [39,43]. In a longitudi-nal study on Doppler and IUGR fetuses, all intra-uterine deaths and all neonatal deaths, with theexception of one case, had late Doppler changesat the time of delivery, whereas only a few of thesurviving fetuses showed such changes [39,43].This sequential deterioration of the hypoxemic,
growth-restricted fetus is rarely seen at gestationsbeyond 34 weeks [18,45,46]. Indeed, normalumbilical artery Doppler is common in growth-restricted fetuses in late gestations, and cerebropla-cental ratios have poor correlation with outcome ofIUGR fetuses at greater than 34 weeks of gestation[35,47]. Caution should therefore be exercisedwhen Doppler is used in the clinical managementof IUGR fetuses beyond 34 weeks of gestation.The pathophysiology of fetal growth restriction
has not been fully described because recent studieshave highlighted the presence of significant varia-tion in fetal adaptation to hypoxemia. The patternof incremental deterioration of arterial Dopplerabnormalities, followed by venous Doppler abnor-malities, then followed by fetal heart tracings andbiophysical profile abnormalities, is not seen inabout 20% of preterm fetuses [16,36]. Further-more, only 70% of IUGR fetuses show significantdeterioration of all vascular beds by the time theywere delivered, and about 10% showed no signifi-cant circulatory change by delivery time [22,37]. Ina prospective, observational study, more than 50%of IUGR fetuses delivered because of abnormal fetalheart rate tracings did not have venous Dopplerabnormalities [39]. In view of these findings, theuniversal introduction of venous Doppler in theclinical management of the growth-restricted fetusshould await the results of randomized trials onthis subject.IUGR is associated with several changes at the
level of the fetal heart involving preload, afterload,ventricular compliance, and myocardial contracti-lity. An increase in afterload is seen at the level ofthe right ventricle because of increased placentalimpedance [25,48]. A decrease in afterload isnoted at the level of the left ventricle because ofdecreased cerebral impedance associated with thebrain-sparing reflex [25,48]. These changes in after-load result in a redistribution of the cardiac outputfrom right to left ventricle [25,48]. Preload is re-duced at both atrioventricular valves because of
hypovolemia and decreased filling associated withIUGR [21,24,26,30,31,45,49,50]. This decrease inpreload is reflected by a decrease in the E/A ratio,decreased atrial peak, and decreased time velocityintegral at the mitral and tricuspid valves [21,24,26,45,49,50].Evidence of reduced myocardial contractility in
the presence of severe IUGR has also been reported.Ventricular ejection force, an index of ventricularsystolic function that is independent of preload andafterload is decreased at the level of the right andleft ventricle in fetal growth restriction [31,36].IUGR fetuses that have reduced ventricular ejec-tion force have a shorter time to delivery, a higherincidence of nonreassuring fetal heart rate tracing,and a lower pH at birth when compared with con-trols [31,36]. A significant correlation between theseverity of fetal acidosis at cordocentesis and ven-tricular ejection force values validates the asso-ciation of this index and the severity of fetalcompromise [31,36]. Myocardial cell damage, dem-onstrated by elevated levels of cardiac troponin-T,is seen in some fetuses that have severe growthrestriction [25,28]. This advanced stage of fetalcompromise is associated with signs of increasedsystemic venous pressure, a change in the distri-bution of cardiac output, a rise in right ventricleafterload, and a high incidence of tricuspid regur-gitation [25,28]. These findings suggest that Dopp-ler abnormalities in the proximal venous systemof the growth restricted fetus suggest fetal myo-cardial cell damage and increased systemic venouspressure [25,28].The fetal heart plays a central role in the adaptive
mechanisms for hypoxemia and placental insuffi-ciency. As discussed in this article, longitudinaldata on the hemodynamic sequence of the naturalhistory of fetal growth restriction show that theumbilical artery and middle cerebral artery are thefirst variables to become abnormal [27,34]. Thesearterial Doppler abnormalities are followed byabnormalities in the right cardiac diastolic indices,followed by the right cardiac systolic indices, andfinally by both left diastolic and systolic cardiacindices [27,34]. Preserving the left systolic functionas the last variable to become abnormal ensures anadequate left ventricular output, which supplies thecerebral and coronary circulations.Several of the Doppler changes seen in asso-
ciation with fetal IUGR in the peripheral circula-tion are directly related to the adaptation of thefetal heart. The current management of IUGRinvolves Doppler at the peripheral arterial circula-tion (middle cerebral and umbilical arteries), cen-tral venous vessels (ductus venosus and inferiorvena cava), and cardiotocography. Adding cardiacDoppler may improve management of the IUGR
300 Abuhamad
fetus, but studies are lacking on the prospectiveclinical evaluation of the IUGR fetus with cardiacDoppler. It is becoming more obvious, however,that those changes in the central venous circulationreflect an advanced stage of fetal compromise,commonly associated with myocardial dysfunctionand damage.
References
[1] Chervenak FA, Skupski DW, Romero R, et al.How accurate is fetal biometry in the assess-ment of fetal age? Am J Obstet Gynecol 1998;178:678–87.
[2] Doppler C. Uber das farbige Licht der Doppler-sterne und einigr anderer Gestirne des Himmels[On the coloured light of double stars and cer-tain other stars of the heavens]. Royal BohemianSociety 1842;2:465–82.
[3] Fleischer A, Schulman H, Farmakides G, et al.Umbilical artery velocity waveforms and intra-uterine growth retardation. Am J Obstet Gynecol1985;151:502–5.
[4] Ott WJ. The diagnosis of altered fetal growth.Obstet Gynecol Clin North Am 1988;15:237–63.
[5] Giles WB, Trudinger BJ, Baird PJ. Fetal umbilicalartery flow velocity waveforms and placentalresistance: pathological correlation. Br J ObstetGynaecol 1985;92:31–8.
[6] Manning FA. Intrauterine growth restriction.Diagnosis, prognostication, and managementbased on ultrasound methods. In: Manning FA,editor. Fetal medicine: principles and practice.Norwalk (CT): Appleton & Lange; 1995. p. 87–94.
[7] Hadlock FP, Deter RL, Harrist RB, et al. A date-independent predictor of intrauterine growthretardation: femur length/abdominal circumfer-ence ratio. AJR Am J Roentgenol 1983;141:979–84.
[8] Trudinger BJ, Stevens D, Connelly A, et al. Um-bilical artery flow velocity waveforms and placen-tal resistance: the effects of embolization of theumbilical circulation. Am J Obstet Gynecol 1987;157:1443–8.
[9] Brown HL, Miller Jr JM, Gabert HA, et al. Ultra-sonic recognition of the small-for-gestational-agefetus. Obstet Gynecol 1987;69:631–5.
[10] Creasy RK, Resnick R. Intrauterine growthretardation. In: Creasy RK, Resnick R, editors.Maternal fetal medicine: principles and practice.Philadelphia: W.B. Saunders; 1984. p. 491.
[11] Kingdom JC, Burrell SJ, Kaufmann P. Pathologyand clinical implications of abnormal umbilicalartery Doppler waveforms. Ultrasound ObstetGynecol 1997;9:271–86.
[12] Morrow RJ, Adamson SL, Bull SB, et al. Effect ofplacental embolization on the umbilical arterialvelocity waveform in fetal sheep. Am J ObstetGynecol 1989;161:1055–60.
[13] Bernstein IM, Horbar JD, Badger GJ, et al.Morbidity and mortality among very-low-birth-
weight neonates with intrauterine growth restric-tion. The Vermont Oxford Network. Am J ObstetGynecol 2000;182:198–206.
[14] Copel JA, Reed KL, Maulik D, editors. Dopplerultrasound in obstetrics and gynecology. NewYork: Raven Press; 1995.
[15] Kok JH, den Ouden AL, Verloove-Vanhorick SP,et al. Outcome of very preterm small for ges-tational age infants: the first nine years of life.Br J Obstet Gynaecol 1998;105:162–8.
[16] Trudinger BJ. Doppler ultrasonography and fetalwell being. In: Reece EA, Hobbins JC, MahoneyM, editors. Medicine of the fetus and mother.Philadelphia: J.B. Lippincott; 1992. p. 701–22.
[17] Fattal-Valevski A, Leitner Y, Kutai M, et al.Neurodevelopmental outcome in children withintrauterine growth retardation: a 3-year follow-up. J Child Neurol 1999;14:724–7.
[18] Mari G, Abuhamad AZ, Brumfield J, et al. Dopp-ler ultrasonography of the middle cerebral arterypeak systolic velocity in the fetus: reproducibilityof measurement [abstract #669]. Am J ObstetGynecol 2001;185:261.
[19] Soothill PW, Ajayi RA, Campbell S, et al. Rela-tionship between fetal acidemia at cordocentesisand subsequent neurodevelopment. UltrasoundObstet Gynecol 1992;2:80–3.
[20] Veille JC, Hanson R, Tatum K. Longitudinalquantitation of middle cerebral artery blood flowin normal human fetuses. Am J Obstet Gynecol1993;169:1393–8.
[21] Hanna BD, Nelson MN, White-Traut RC, et al.Heart rate variability in preterm brain-injuredand very-low-birth-weight infants. Biol Neonate2000;77:147–55.
[22] Mari G, Deter RL. Middle cerebral artery flowvelocity waveforms in normal and small-for-gestational-age fetuses. Am J Obstet Gynecol 1992;166:1262–70.
[23] Nijhuis IJ, ten Hof J, Mulder EJ, et al. Fetal heartrate in relation to its variation in normal andgrowth retarded fetuses. Eur J Obstet GynecolReprod Biol 2000;89:27–33.
[24] Bracero LA, Roshanfekr D, Byrne DW. Analysis ofantepartum fetal heart rate tracing by physicianand computer. J Matern Fetal Med 2000;9:181–5.
[25] Devoe L, Golde S, Kilman Y, et al. A comparisonof visual analyses of intrapartum fetal heart ratetracings according to the new National Instituteof Child Health and Human Developmentguidelines with computer analyses by an auto-mated fetal heart rate monitoring system. Am JObstet Gynecol 2000;183:361–6.
[26] Hecher K, Hackeloer BJ. Cardiotocogram com-pared to Doppler investigation of the fetalcirculation in the premature growth-retardedfetus: longitudinal observations. UltrasoundObstet Gynecol 1997;9:152–61.
[27] Huisman TW, Stewart PA, Wladimiroff JW. Flowvelocity waveforms in the fetal inferior vena cavaduring the second half of normal pregnancy.Ultrasound Med Biol 1991;17:679–82.
301Doppler Ultrasound in Obstetrics
[28] Reed KL, Appleton CP, Anderson CF, et al.Doppler studies of vena cava flows in humanfetuses. Insights into normal and abnormal car-diac physiology. Circulation 1990;81:498–505.
[29] Reuss ML, Rudolph AM, Dae MW. Phasic bloodflow patterns in the superior and inferior venaecavae and umbilical vein of fetal sheep. Am JObstet Gynecol 1983;145:70–8.
[30] Ribbert LS, Visser GH, Mulder EJ, et al. Changeswith time in fetal heart rate variation, movementincidences and haemodynamics in intrauterinegrowth retarded fetuses: a longitudinal approachto the assessment of fetal well being. Early HumDev 1993;31:195–208.
[31] Rizzo G, Arduini D, Romanini C. Inferior venacava flow velocity waveforms in appropriate- andsmall-for-gestational-age fetuses. Am J ObstetGynecol 1992;166:1271–80.
[32] Rizzo G, Capponi A, Talone PE, et al. Dopplerindices from inferior vena cava and ductusvenosus in predicting pH and oxygen tensionin umbilical blood at cordocentesis in growth-retarded fetuses. Ultrasound Obstet Gynecol1996;7:401–10.
[33] Vindla S, James D, Sahota D. Computerisedanalysis of unstimulated and stimulated behav-iour in fetuses with intrauterine growth restric-tion. Eur J Obstet Gynecol Reprod Biol 1999;83:37–45.
[34] Alfirevic Z, Neilson JP. Doppler ultrasonographyin high-risk pregnancies: systematic review withmeta-analysis. Am J Obstet Gynecol 1995;172:1379–87.
[35] Bahado-Singh RO, Kovanci E, Jeffres A, et al. TheDoppler cerebroplacental ratio and perinataloutcome in intrauterine growth restriction. AmJ Obstet Gynecol 1999;180:750–6.
[36] Baschat AA, Gembruch U, Reiss I, et al. Relation-ship between arterial and venous Doppler andperinatal outcome in fetal growth restriction.Ultrasound Obstet Gynecol 2000;16:407–13.
[37] Baschat AA, Gembruch U, Harman CR. Thesequence of changes in Doppler and biophysicalparameters as severe fetal growth restrictionworsens. Ultrasound Obstet Gynecol 2001;18:571–7.
[38] Hecher K, Bilardo CM, Stigter RH, et al. Moni-toring of fetuses with intrauterine growth restric-tion: a longitudinal study. Ultrasound ObstetGynecol 2001;18:564–70.
[39] Ferrazzi E, Bozzo M, Rigano S, et al. Temporalsequence of abnormal Doppler changes in theperipheral and central circulatory systems of the
severely growth-restricted fetus. Ultrasound Ob-stet Gynecol 2002;19:140–6.
[40] Baschat AA, Gembruch U, Gortner L, et al.Coronary artery blood flow visualization sig-nifies hemodynamic deterioration in growth-restricted fetuses. Ultrasound Obstet Gynecol2000;16:425–31.
[41] Baschat AA, Gembruch U, Weiner CP, et al.Longitudinal changes of arterial and venousDoppler in fetuses with intrauterine growth re-striction [abstract]. Am J Obstet Gynecol 2001;184:103.
[42] Senat MV, Schwarzler P, Alcais A, et al. Longi-tudinal changes in the ductus venosus, cerebraltransverse sinus and cardiotocogram in fetalgrowth restriction. Ultrasound Obstet Gynecol2000;16:19–24.
[43] Behrman RE, Lees MH, Peterson EN, et al.Distribution of the circulation in the normaland asphyxiated fetal primate. Am J ObstetGynecol 1970;108:956–69.
[44] Pardi G, Cetin I, Marconi AM, et al. Diagnosticvalue of blood sampling in fetuses with growthretardation. N Engl J Med 1993;328:692–6.
[45] Harrington K, Thompson MO, Carpenter RG,et al. Doppler fetal circulation in pregnanciescomplicated by pre-eclampsia or delivery of asmall for gestational age baby: 2. Longitudinalanalysis. Br J Obstet Gynaecol 1999;106:453–66.
[46] Hecher K, Campbell S, Doyle P, et al. Assessmentof fetal compromise by Doppler ultrasoundinvestigation of the fetal circulation. Arterial,intracardiac, and venous blood flow velocitystudies. Circulation 1995;91:129–38.
[47] Wladimiroff JW, vd Wijngaard JA, Degani S,et al. Cerebral and umbilical arterial blood flowvelocity waveforms in normal and growth-retarded pregnancies. Obstet Gynecol 1987;69:705–9.
[48] Gramellini D, Folli MC, Raboni S, et al. Cerebral-umbilical Doppler ratio as a predictor of adverseperinatal outcome. Obstet Gynecol 1992;79:416–20.
[49] Arduini D, Rizzo G. Prediction of fetal outcomein small for gestational age fetuses: comparisonof Doppler measurements obtained from differ-ent fetal vessels. J Perinat Med 1992;20:29–38.
[50] Fong KW, Ohlsson A, Hannah ME, et al.Prediction of perinatal outcome in fetusessuspected to have intrauterine growth restriction:Doppler US study of fetal cerebral, renal, andumbilical arteries. Radiology 1999;213:681–9.

![[PPT]Doppler Evaluation in Obstetrics - Echo ED: Diagnostic ... · Web viewWhat are the safety considerations for the usage of Doppler in obstetrics? The safety of Doppler ultrasound](https://img.dokumen.tips/doc/110x75/5aaed5ce7f8b9a59478c92a2/pptdoppler-evaluation-in-obstetrics-echo-ed-diagnostic-viewwhat-are-the.jpg)