Embed Size (px)
Citation preview

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 1 of 19
Document Control
Title
Antibiotic Guidelines for Infections of the Central Nervous System in Adults
Author Consultant Microbiologist
Author’s job title Consultant Microbiologist
Directorate Diagnostics
Department Pathology
Version Date
Issued Status Comment / Changes / Approval
0.1 Sep 2011 Draft First draft for consultation
0.2 Oct 2011 Draft After consultation with Dr Honan, Consultant Neurologist, changes to duration recommendations and imaging recommendations
0.3 Nov 2011
Draft After discussion with Consultant Radiologists. Removal of encephalitis and MRI audit criterion. Removal of requirement for CT before LP. Change to imaging recommendations in toxoplasmosis and encephalitis.
0.4 Nov 2011
Draft Addition of public health contact and meningitis UK reference.
0.5 Feb 2012 Draft Approved by AWG. Change recommended antibiotic for meningitis and brain abscess to meropenem. Clarify advice on encephalitis. Clarify advice on chemoprophylaxis.
1.0 Mar 2012
Final Ratified by Drug and Therapeutics Committee on 8th March 2012.
1.1 Jun 2012 Revision Minor amendment by Corporate Governance to header and footer, table of contents, document control report and added hyperlinks.
1.2 May 2016
Revision Updated with new guidance, references updated. Change recommended antibiotics from meropenem combinations to ceftriaxone combinations for brain abscess and bacterial meningitis.
Main Contact Consultant Microbiologist, North Devon District Hospital Raleigh Park Barnstaple, EX31 4JB
Tel: Direct Dial – 01271 322798
Lead Director Director of Infection Prevention and Control
Superseded Documents None
Issue Date May 2016
Review Date May 2019
Review Cycle Three years

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 2 of 19
Consulted with the following stakeholders: (list all)
Antibiotic Working Group Drug and Therapeutics Group Consultant Neurologist Consultant Radiologists
Approval and Review Process
Drug and Therapeutics Committee
Local Archive Reference G:\ANTIBIOTIC STEWARDSHIP\Stewardship\Antibiotic policies\Archived policies Local Path G:\ANTIBIOTIC STEWARDSHIP\Stewardship\Antibiotic policies\Published policies Filename Antibiotic Guidelines for CNS Indications v1.2 Apr16
Policy categories for Trust’s internal website (Bob) Pharmacy, Microbiology, Antibiotics
Tags for Trust’s internal website (Bob) Meningitis, Encephalitis, Brain Abscess

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 3 of 19
CONTENTS
Document Control........................................................................................................................ 1
1. Purpose ................................................................................................................................ 3
2. Responsibilities .................................................................................................................... 4
2.1 Role of Antibiotic Working Group (AWG) ........................................................................... 4
3. Contacts ............................................................................................................................... 4
4. Investigation, Treatment and Prophylaxis of CNS Infections ................................................... 4
5. Monitoring Compliance with and the Effectiveness of the Policy ............................................ 5
5.1 Suggested audit criteria ...................................................................................................... 5
5.2 Process for Implementation and Monitoring Compliance and Effectiveness .................... 5
6. Equality Impact Assessment .................................................................................................. 5
7. References and Supporting Evidence ..................................................................................... 6
8. Associated Documentation ................................................................................................... 6
Appendix A: Bacterial Meningitis .................................................................................................. 7
Appendix B: Viral Meningitis ...................................................................................................... 11
Appendix C: other non-viral aseptic meningitis ........................................................................... 13
Appendix D: chemoprophylaxis for contacts ............................................................................... 14
Appendix E: Encephalitis ............................................................................................................ 15
Appendix F: brain abscess .......................................................................................................... 17
1. Purpose
This document sets out Northern Devon Healthcare NHS Trust’s best practice guidelines for appropriate microbiological investigation and antimicrobial prescribing in adult patients with infections of central nervous system (CNS) focus.
This guideline applies to all adults and must be adhered to. Special considerations exist for pregnant and breastfeeding patients; liaise with specialist clinicians as appropriate in these cases. See separate guidance for paediatric patients.
Non-compliance with this guideline may be for valid clinical reasons only. The reason(s) for non-compliance must be documented clearly in the patient’s notes.
This guideline is primarily aimed at all prescribing teams but other staff (e.g. nursing staff, pharmacists) may need to familiarise themselves with some aspects of the guideline.
Implementation of this guideline will ensure that:
CNS infections are managed according to current evidence and standards of practice in the wider healthcare community.
A standard of care is specified to facilitate a consistent approach between neurology, microbiology and pharmacy in terms of patient management, specimen processing and drug availability.

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 4 of 19
Non-neurology clinicians recognise symptoms which require referral to neurology for specialist management.
2. Responsibilities
Responsibility for education and training lies with the Lead Consultant Microbiologist for Antibiotic Stewardship. It will be provided through formal study days and informal training on the ward.
The author will be responsible for ensuring the guidelines are reviewed and revisions approved by the Drug and Therapeutics Group in accordance with the Document Control Report.
All versions of these guidelines will be archived in electronic format by the author within the Antibiotic Stewardship policy archive.
Any revisions to the final document will be recorded on the Document Control Report.
To obtain a copy of the archived guidelines, contact should be made with the author.
Monitoring of implementation, effectiveness and compliance with these guidelines will be the responsibility of the Lead Clinician for Antibiotic Stewardship. Where non-compliance is found, the reasons for this must have been documented in the patient’s medical notes.
2.1 Role of Antibiotic Working Group (AWG)
The AWG is responsible for:
Leading antibiotic guideline development and review within Northern Devon Healthcare Trust
Involving all relevant stakeholders in guideline development and review
3. Contacts
Contact numbers:
Microbiologist Bleep 193. Via switchboard out of hours.
Antibiotic Pharmacist Bleep 029 (Mon-Fri only)
4. Investigation, Treatment and Prophylaxis of CNS Infections
See appendices
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 5 of 19
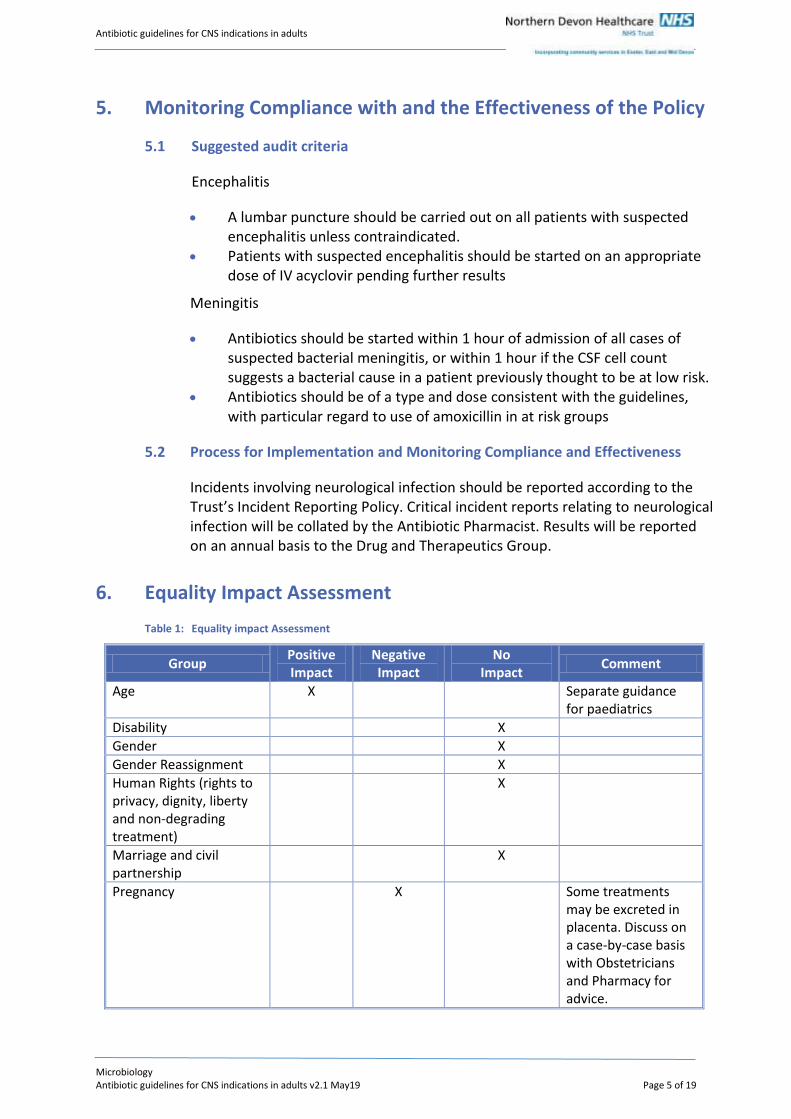
5. Monitoring Compliance with and the Effectiveness of the Policy
5.1 Suggested audit criteria
Encephalitis
A lumbar puncture should be carried out on all patients with suspected encephalitis unless contraindicated.
Patients with suspected encephalitis should be started on an appropriate dose of IV acyclovir pending further results
Meningitis
Antibiotics should be started within 1 hour of admission of all cases of suspected bacterial meningitis, or within 1 hour if the CSF cell count suggests a bacterial cause in a patient previously thought to be at low risk.
Antibiotics should be of a type and dose consistent with the guidelines, with particular regard to use of amoxicillin in at risk groups
5.2 Process for Implementation and Monitoring Compliance and Effectiveness
Incidents involving neurological infection should be reported according to the Trust’s Incident Reporting Policy. Critical incident reports relating to neurological infection will be collated by the Antibiotic Pharmacist. Results will be reported on an annual basis to the Drug and Therapeutics Group.
6. Equality Impact Assessment
Table 1: Equality impact Assessment
Group Positive Impact
Negative Impact
No Impact
Comment
Age X Separate guidance for paediatrics
Disability X
Gender X
Gender Reassignment X
Human Rights (rights to privacy, dignity, liberty and non-degrading treatment)
X
Marriage and civil partnership
X
Pregnancy X Some treatments may be excreted in placenta. Discuss on a case-by-case basis with Obstetricians and Pharmacy for advice.
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 6 of 19
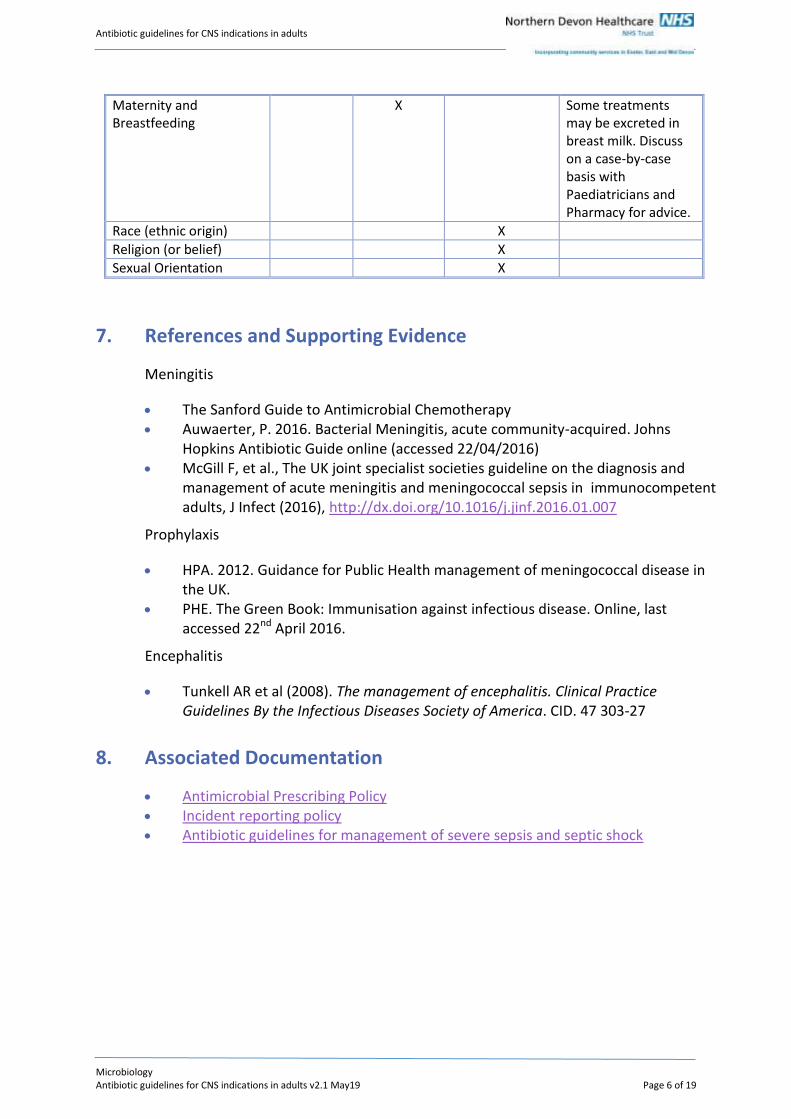
Maternity and Breastfeeding
X Some treatments may be excreted in breast milk. Discuss on a case-by-case basis with Paediatricians and Pharmacy for advice.
Race (ethnic origin) X
Religion (or belief) X
Sexual Orientation X
7. References and Supporting Evidence
Meningitis
The Sanford Guide to Antimicrobial Chemotherapy Auwaerter, P. 2016. Bacterial Meningitis, acute community-acquired. Johns
Hopkins Antibiotic Guide online (accessed 22/04/2016) McGill F, et al., The UK joint specialist societies guideline on the diagnosis and
management of acute meningitis and meningococcal sepsis in immunocompetent adults, J Infect (2016), http://dx.doi.org/10.1016/j.jinf.2016.01.007
Prophylaxis
HPA. 2012. Guidance for Public Health management of meningococcal disease in the UK.
PHE. The Green Book: Immunisation against infectious disease. Online, last accessed 22nd April 2016.
Encephalitis
Tunkell AR et al (2008). The management of encephalitis. Clinical Practice Guidelines By the Infectious Diseases Society of America. CID. 47 303-27
8. Associated Documentation
Antimicrobial Prescribing Policy Incident reporting policy Antibiotic guidelines for management of severe sepsis and septic shock
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 7 of 19
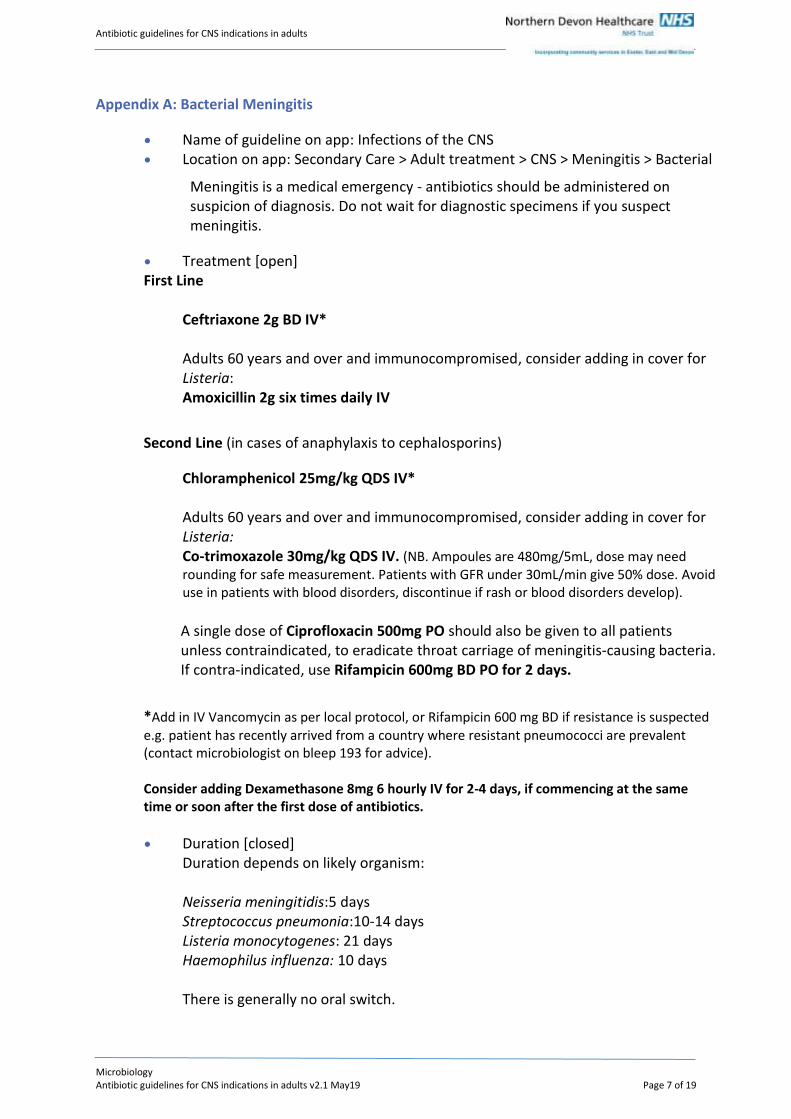
Appendix A: Bacterial Meningitis
Name of guideline on app: Infections of the CNS Location on app: Secondary Care > Adult treatment > CNS > Meningitis > Bacterial
Meningitis is a medical emergency - antibiotics should be administered on suspicion of diagnosis. Do not wait for diagnostic specimens if you suspect meningitis.
Treatment [open] First Line
Ceftriaxone 2g BD IV* Adults 60 years and over and immunocompromised, consider adding in cover for Listeria: Amoxicillin 2g six times daily IV
Second Line (in cases of anaphylaxis to cephalosporins)
Chloramphenicol 25mg/kg QDS IV* Adults 60 years and over and immunocompromised, consider adding in cover for Listeria: Co-trimoxazole 30mg/kg QDS IV. (NB. Ampoules are 480mg/5mL, dose may need rounding for safe measurement. Patients with GFR under 30mL/min give 50% dose. Avoid use in patients with blood disorders, discontinue if rash or blood disorders develop).
A single dose of Ciprofloxacin 500mg PO should also be given to all patients unless contraindicated, to eradicate throat carriage of meningitis-causing bacteria. If contra-indicated, use Rifampicin 600mg BD PO for 2 days.
*Add in IV Vancomycin as per local protocol, or Rifampicin 600 mg BD if resistance is suspected e.g. patient has recently arrived from a country where resistant pneumococci are prevalent (contact microbiologist on bleep 193 for advice). Consider adding Dexamethasone 8mg 6 hourly IV for 2-4 days, if commencing at the same time or soon after the first dose of antibiotics.
Duration [closed] Duration depends on likely organism: Neisseria meningitidis:5 days Streptococcus pneumonia:10-14 days Listeria monocytogenes: 21 days Haemophilus influenza: 10 days There is generally no oral switch.

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 8 of 19
Assess patient’s clinical condition when making the decision to stop, some patients may require longer courses if source control is not achieved.
Samples and Investigations [closed]
Ensure that forms have “suspected meningitis” or similar wording on them: Blood cultures x 2 bottles FBC, U+Es, CRP, LFTs, clotting screen, glucose Lumbar puncture, once the patient is stable and assessment made to rule
out raised intra-cranial pressure eg. CT scan. Even if an organism cannot be isolated, the cell count and biochemical properties of the CSF may aid subsequent management. Molecular techniques can be used after discussion with a microbiologist.
http://app.rx-guidelines.com/UserUploads/6/CSF%20SOP.pdf
Further tests if no aetiology identified at first:
Discuss with Consultant Microbiologist
Pharyngeal swabs and serology samples are not routinely required if other samples as above can be sent. If in doubt, discuss with Microbiologist.
Help notes [closed] Clinical features include :
Headache (more than 90%) Fever (more than 90%) Meningismus (more than 85%) Kernig’s sign (more than 50%) Rash (50%) – may be macular, evolving into petechiae/purpura Seizure (30%) Focal findings (10%) Confusion / altered mental status (more than 90% in the elderly)
Have you considered encephalitis (new confusion or seizures)?
Elderly patients with meningitis may present insidiously with lethargy or obtundation.
Predisposing factors for meningitis include : immunocompromise, basilar skull fracture, neurosurgery, cerebrospinal shunts. Presence of these factors may suggest more unusual pathogens and the cases should be discussed urgently with a microbiologist.
Lumbar puncture is contraindicated in the following:
Signs of severe sepsis or rapidly evolving rash Respiratory or cardiac compromise Anticoagulant therapy/known thrombocytopenia Infection at the site of LP Focal neurological signs †

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 9 of 19
Presence of papilloedema*† Continuous or uncontrolled seizures† GCS ≤12**†
* inability to see the fundus is not a contraindication to LP ** LP may be safe at lower levels of consciousness †Neuroimaging should be performed before LP for these indications. Once the patient is stable and if meningitis is likely (with or without sepsis) an LP may still be diagnostically useful, even after several days.
In bacterial meningitis, CSF typically shows raised neutrophils (polymorphs). The protein is usually raised, and the CSF glucose is less than 60% of the peripheral glucose.
Have you considered viral meningitis? Viral meningitis often presents with relatively mild signs and symptoms. It is reasonable to withhold antibiotics in a patient who is systemically well if you are confident that bacterial meningitis is not the diagnosis. This decision should be reviewed with results of the lumbar puncture.
CT / MRI may give important diagnostic information – discuss with radiologist.
Public Health must be notified on suspicion of diagnosis. Contact via switchboard.
Penicillin resistant pneumococci are uncommon in the UK but more prevalent in eg Spain and US. Inform Microbiology if patients from the continent are admitted with meningitis, as this may change their management.
Up to date European and worldwide data on resistance can be found via the European Centre for Disease Prevention and Control website or the World Health Organisation (http://bit.ly/1Kosckx and http://bit.ly/1rOb3cx)
Isolate patients for first 24 hours of treatment and consider chemoprophylaxis of contacts (see Appendix E). Note chloramphenicol is not reliable for eradication of throat carriage in the index case. See treatment advice for recommendations.
Where source control is not possible or collections are suspected/known, liaise with microbiology for further guidance.
Organism and sensitivity data [closed]
Organisms and sensitivity data. Resistance data is based on all sputum specimens sent to the laboratory. This is likely to over-represent the incidence of resistance in first line agents, as many specimens are only sent in cases of treatment failure.
Bacteria % sensitivity to cephalosporin
% sensitivity to chloramphenicol
Pneumococcus 97%
Meningococcus 100%
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 10 of 19
Listeria
Common
Pneumococcus. Penicillin resistance in the UK is very low (<1%)
Meningococcus. All sensitive to penicillin
Less Common (mainly in the unvaccinated elderly)
Haemophilus influenzae. Low rates of amoxicillin resistance
Rare (>50 years)
Listeria. Sensitive to amoxicillin and co-trimoxazole. Inherently resistant to cephalosporins.
Version control [closed]
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 11 of 19
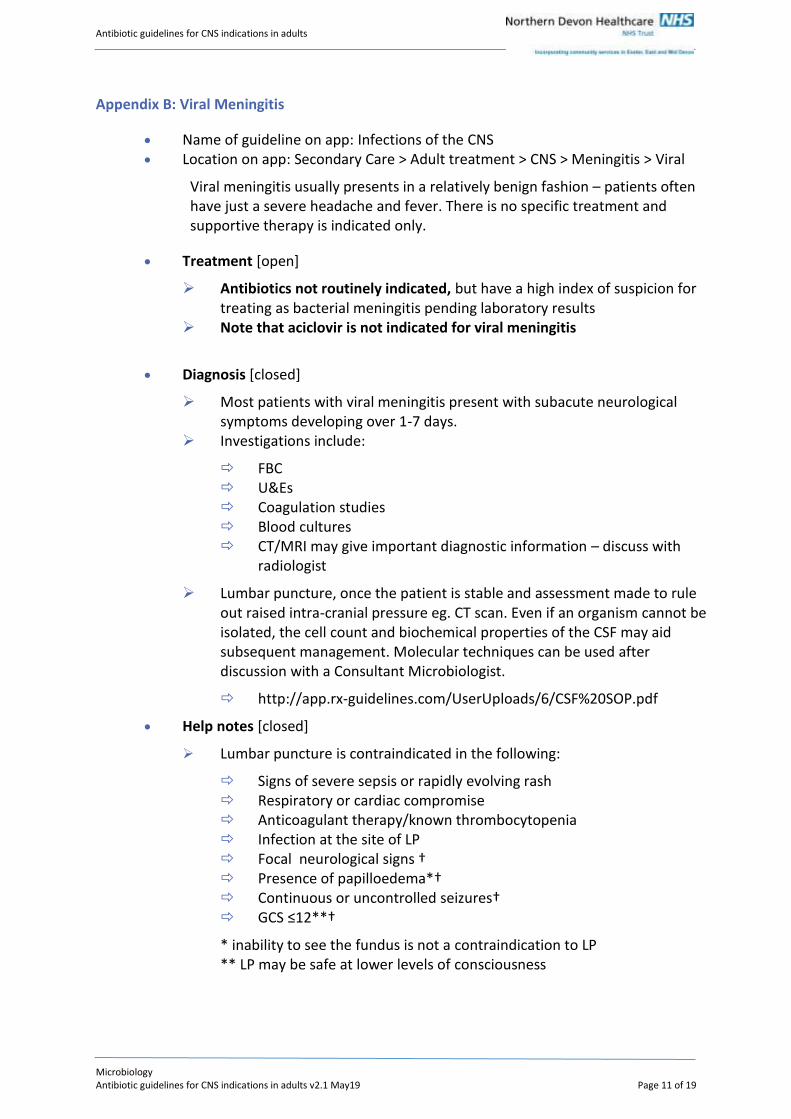
Appendix B: Viral Meningitis
Name of guideline on app: Infections of the CNS Location on app: Secondary Care > Adult treatment > CNS > Meningitis > Viral
Viral meningitis usually presents in a relatively benign fashion – patients often have just a severe headache and fever. There is no specific treatment and supportive therapy is indicated only.
Treatment [open]
Antibiotics not routinely indicated, but have a high index of suspicion for treating as bacterial meningitis pending laboratory results
Note that aciclovir is not indicated for viral meningitis
Diagnosis [closed]
Most patients with viral meningitis present with subacute neurological symptoms developing over 1-7 days.
Investigations include:
FBC U&Es Coagulation studies Blood cultures CT/MRI may give important diagnostic information – discuss with
radiologist
Lumbar puncture, once the patient is stable and assessment made to rule out raised intra-cranial pressure eg. CT scan. Even if an organism cannot be isolated, the cell count and biochemical properties of the CSF may aid subsequent management. Molecular techniques can be used after discussion with a Consultant Microbiologist.
http://app.rx-guidelines.com/UserUploads/6/CSF%20SOP.pdf
Help notes [closed]
Lumbar puncture is contraindicated in the following:
Signs of severe sepsis or rapidly evolving rash Respiratory or cardiac compromise Anticoagulant therapy/known thrombocytopenia Infection at the site of LP Focal neurological signs † Presence of papilloedema*† Continuous or uncontrolled seizures† GCS ≤12**†
* inability to see the fundus is not a contraindication to LP ** LP may be safe at lower levels of consciousness

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 12 of 19
†Neuroimaging should be performed before LP for these indications. Once the patient is stable and if meningitis is likely (with or without sepsis) an LP may still be diagnostically useful, even after several days.
Note: In bacterial meningitis blood and CSF cultures may still be negative – especially if the patient has already had prior treatment with antibiotics. There are no routine molecular tests for bacterial causes other than pneumococcus/meningococcus.
Further tests if no aetiology identified at first:
Discuss with Consultant Microbiologist
Organisms and sensitivity data
Viral meningitis is often caused by:
Enteroviruses Mumps Herpes virus, including Epstein-Barr virus, Herpes simplex viruses,
Varicella-zoster virus (which also causes chicken pox and shingles) Measles Influenza

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 13 of 19
Appendix C: Other non-viral aseptic meningitis
Name of guideline on app: Infections of the CNS Location on app: Secondary Care > Adult treatment > CNS > Meningitis > Other
non-viral aseptic Aseptic meningitis is defined as an inflammation of the meninges in the absence of organisms that can be identified using the normal range of tests.
Treatment
Please discuss with a Microbiology Consultant if a non-viral aseptic cause of meningitis is suspected
Help notes
Causes of non-viral aseptic meningitis include:
Tuberculosis, Cryptococcus, Lyme disease, Syphilis Drugs: NSAIDs, antimicrobials, azathioprine, IV immunoglobulin,
intrathecal methotrexate, intrathecal cystine arabinoside, vaccines, allopurinol.
Systemic diseases: Sarcoidosis, leptomeningeal cancer, post-transplantation lymphoproliferative disorder, SLE, Wegener’s Granulomatosis, CNS vasculitis, Behçet disease.
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 14 of 19
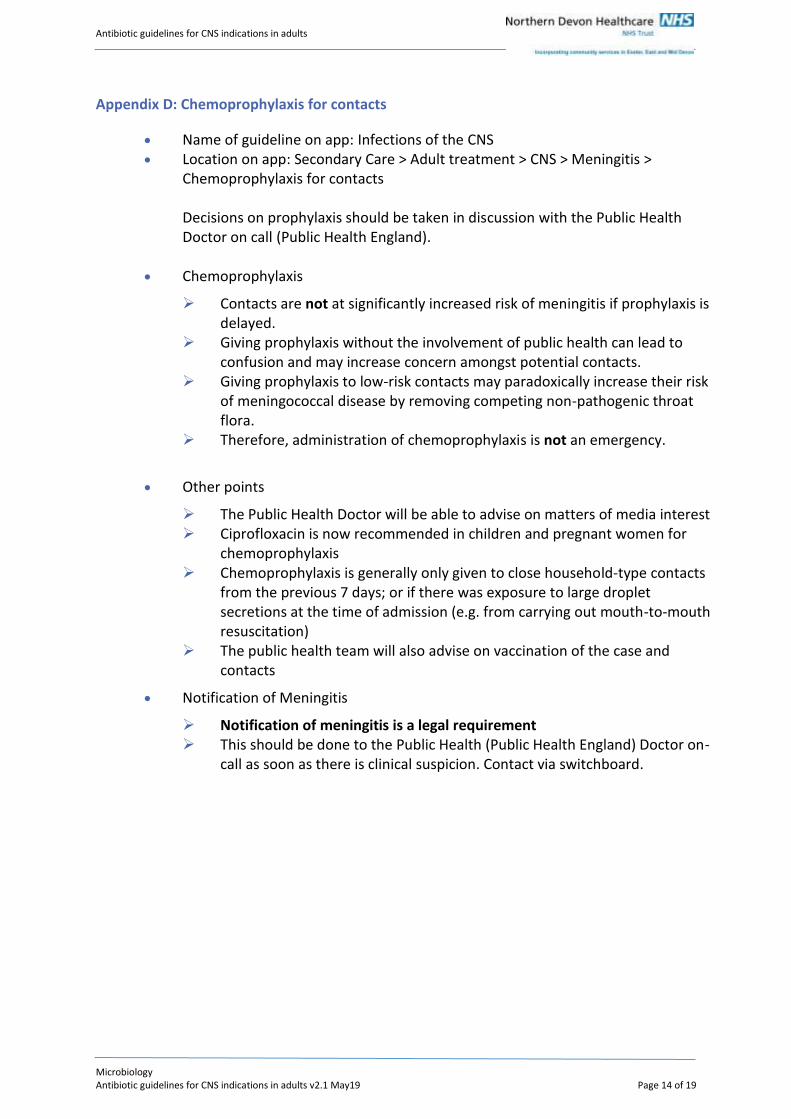
Appendix D: Chemoprophylaxis for contacts
Name of guideline on app: Infections of the CNS Location on app: Secondary Care > Adult treatment > CNS > Meningitis >
Chemoprophylaxis for contacts Decisions on prophylaxis should be taken in discussion with the Public Health Doctor on call (Public Health England).
Chemoprophylaxis
Contacts are not at significantly increased risk of meningitis if prophylaxis is delayed.
Giving prophylaxis without the involvement of public health can lead to confusion and may increase concern amongst potential contacts.
Giving prophylaxis to low-risk contacts may paradoxically increase their risk of meningococcal disease by removing competing non-pathogenic throat flora.
Therefore, administration of chemoprophylaxis is not an emergency.
Other points
The Public Health Doctor will be able to advise on matters of media interest Ciprofloxacin is now recommended in children and pregnant women for
chemoprophylaxis Chemoprophylaxis is generally only given to close household-type contacts
from the previous 7 days; or if there was exposure to large droplet secretions at the time of admission (e.g. from carrying out mouth-to-mouth resuscitation)
The public health team will also advise on vaccination of the case and contacts
Notification of Meningitis
Notification of meningitis is a legal requirement This should be done to the Public Health (Public Health England) Doctor on-
call as soon as there is clinical suspicion. Contact via switchboard.

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 15 of 19
Appendix E: Encephalitis
Name of guideline on app: Infections of the CNS Location on app: Secondary Care > Adult treatment > CNS > Encephalitis
Viruses are the most common cause of encephalitis; however, consider combining with treatment for bacterial meningitis pending CSF results.
Treatment [closed]
Aciclovir 10mg/kg TDS IV
Duration and Oral Switch Treat for 14-21 days Oral switch not generally recommended. Discuss with Microbiology, bleep 193.
Diagnosis
CT: A late sign is bilateral low-density regions in both temporal lobes seen with Herpes simplex encephalitis. This is not useful for early diagnosis, but CT is essential before performing lumbar puncture.
MRI: Most sensitive investigation method in patients with encephalitis. Higher sensitivity for temporal lobe oedema, and may be more sensitive than HSV PCR. Discuss imaging with Consultant Radiologist.
Lumbar puncture after CT screening: Usually shows raised protein and lymphocytic pleocytosis. HSV PCR must be carried out on the CSF.
HSV PCR has more than 95% sensitivity, although it may be negative in the first 3 days of illness.
Lumbar puncture should be repeated if diagnostic uncertainty remains
Strongly consider HIV testing (send in clotted blood vial) If respiratory symptoms present: consider sputum PCR for respiratory
viruses (including adenovirus and influenza) and serology (in clotted blood vial) for Q-fever and Mycoplasma
If skin vesicles present, take swabs for HSV and VZV PCR. VZV is associated with cerebellar signs.
Samples of serum and CSF are required for viral and immunological studies, as paired studies are required to show rising titres.
EEG: In herpetic encephalitis, the EEG shows diffuse slowing with periodic discharges. This is more useful than a CT scan in the first week of illness.
Help Notes
Consider encephalitis if any of:
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 16 of 19
Altered conscious state Behavioural change Seizures Meningeal signs/headache may be present Fever history and a prodromal illness of a few days (present in most
patients with HSV)
Note: Bacterial meningitis may present atypically with confusion and an absence of meningeal signs
Note: Aseptic meningitis is not the same as encephalitis and there is usually no role for aciclovir
Consider: Syphilis and Lyme disease (encephalitis may be an early feature shortly after erythema)
Consider Rickettsial disease in patients with history of travel to endemic areas. Discuss with microbiology and consider starting doxycycline.
Travel-associated viruses include: Japanese encephalitis, West Nile viruses, Tick-borne encephalitis, rabies.
A wide range of aetiologies can cause symptoms of encephalitis in the immunocompromised. Discuss with Microbiology on bleep 193.
Consider non-infectious aetiologies, including ADEM
Organisms and sensitivity data
Viruses are the most common cause of encephalitis. Herpes simplex virus is the most usual cause of encephalitis in the UK, and the only one with a validated specific treatment.
HIV infection is of increasing importance Other common viral causes are herpes zoster, Epstein-Barr virus, mumps,
measles and enteroviruses.

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 17 of 19
Appendix F: Brain abscess
Name of guideline on app: Infections of the CNS Location on app: Secondary Care > Adult treatment > CNS > Brain abscess
All suspected cases must be discussed with Neurosurgery.
Treatment First line Ceftriaxone 2g BD IV Plus Metronidazole 500mg TDS IV (400mg TDS PO) NB. This combination has no activity against MRSA. Phone to discuss with Microbiology Consultant if MRSA may be involved. Cephalosporin allergy: Vancomycin IV (dose according to Trust protocol) Plus Ciprofloxacin 400mg BD IV (500mg BD PO) Plus Metronidazole 500mg TDS IV (400mg TDS PO)
Duration Depends on culture results, but generally 4-6 weeks with adequate source control
Suspected fungal infection
Phone Microbiology Consultant for advice Usually voriconazole or posaconazole ± Ambisome®
Diagnosis
FBC: marked leukocytosis. Raised ESR and CRP. Renal function and electrolytes: serum sodium levels may be lowered as a
result of inappropriate antidiuretic hormone production. Blood cultures: at least two, and preferably before antibiotics are started. Serology is helpful : nearly all patients will be IgG positive. In the presence
of characteristic lesions and positive serology, a therapeutic trial may be warranted.
Cerebrospinal fluid: lumbar puncture is rarely helpful (unless required to rule out meningitis) and is contra-indicated if increased
Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 18 of 19
intracranial pressure is present. Lumbar puncture in the presence of raised intracranial pressure can precipitate a tentorial or tonsillar herniation.
CT scanning is the investigation of choice. Cerebral abscesses appear as a radiolucent space-occupying lesion:
As the disease progresses, a distinctive 'ring enhancement' appears on contrast-enhanced CT, as the abscess wall thickens.
They are often surrounded by oedema. The position, size and number of abscesses may suggest underlying
pathology. Aspergillosis may present as a cerebral infarct. MRI scans provide greater contrast between cerebral oedema and the
brain and early detection of satellite lesions.
Aspiration of abscess for culture. Biopsy of lesion is desirable. It defines the pathogen, or suggests non-
infective causes (eg. Lymphoma). If possible, this should be done after scanning but before antibiotics
Help Notes
Surgery is essential for lesions more than 2.5cm. Common signs and symptoms include :
Headache (70%) Mental status changes (70%) Focal neurological deficits (more than 60%) Fever (50%) Seizures (30%) Nausea (30%) Nucal rigidity (35%) Papilloedema (25%)
Triad of fever, focal signs and headache in under 50% In toxoplasmosis, there are usually multiple abscesses, although may be
single lesions in up to 30%. Nocardial abscesses often nonspecific with fever and headache. Mucormycocis is an acute, fulminant fungal infection. Most cases are
associated with diabetes or severe immunosuppresion. Candidates for non-surgical management:
Small abscess (< 2.5cm) Glasgow Coma Score > 12 and for which the aetiology is known (e.g.,
from blood culture) Multiple abscesses Abscesses arising after surgery or patient in whom surgery poses
grave risks

Antibiotic guidelines for CNS indications in adults
Microbiology Antibiotic guidelines for CNS indications in adults v2.1 May19 Page 19 of 19
Organisms and sensitivity data
Causative organisms include: Bacteria: common bacterial causes include Staphylococcus aureus,
and Streptococcus, Bacteroides and Listeria species. Fungi: Aspergillus, Candida, Cryptococcus, Coccidioides, Histoplasma, and
Blastomyces species. Protozoa: Toxoplasma gondii, Entamoeba histolytica, Trypanosoma
cruzi, and Schistosoma spp Identification of single organism may not be representative: 25% of
abscesses are multi-organism.