Embed Size (px)
Citation preview
Clinical Practice GuidelinesManagement of Diabetes Mellitus(DM) in Pregnancy
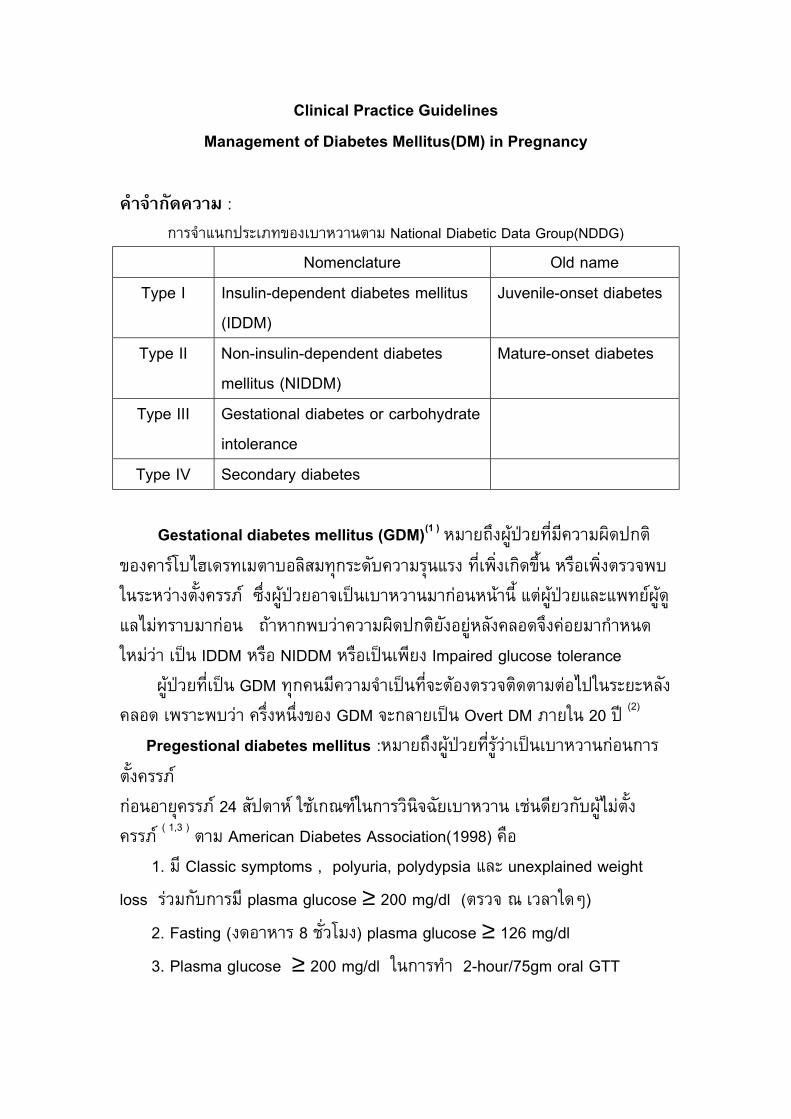
คํ าจํ ากัดความ : การจํ าแนกประเภทของเบาหวานตาม National Diabetic Data Group(NDDG)
Nomenclature Old nameType I Insulin-dependent diabetes mellitus
(IDDM)Juvenile-onset diabetes
Type II Non-insulin-dependent diabetesmellitus (NIDDM)
Mature-onset diabetes
Type III Gestational diabetes or carbohydrateintolerance
Type IV Secondary diabetes
Gestational diabetes mellitus (GDM)(1 ) หมายถึงผูปวยที่มีความผิดปกติของคารโบไฮเดรทเมตาบอลิสมทุกระดับความรุนแรง ท่ีเพ่ิงเกิดข้ึน หรือเพิ่งตรวจพบในระหวางต้ังครรภ ซึ่งผูปวยอาจเปนเบาหวานมากอนหนานี้ แตผูปวยและแพทยผูดูแลไมทราบมากอน ถาหากพบวาความผิดปกติยังอยูหลังคลอดจึงคอยมากํ าหนดใหมวา เปน IDDM หรือ NIDDM หรือเปนเพียง Impaired glucose tolerance ผูปวยที่เปน GDM ทุกคนมีความจํ าเปนที่จะตองตรวจติดตามตอไปในระยะหลังคลอด เพราะพบวา คร่ึงหน่ึงของ GDM จะกลายเปน Overt DM ภายใน 20 ป (2)
Pregestional diabetes mellitus :หมายถึงผูปวยที่รูวาเปนเบาหวานกอนการต้ังครรภกอนอายุครรภ 24 สัปดาห ใชเกณฑในการวินิจฉัยเบาหวาน เชนดียวกับผูไมตั้งครรภ ( 1,3 ) ตาม American Diabetes Association(1998) คือ 1. มี Classic symptoms , polyuria, polydypsia และ unexplained weightloss รวมกับการม ีplasma glucose ≥ 200 mg/dl (ตรวจ ณ เวลาใดๆ) 2. Fasting (งดอาหาร 8 ชั่วโมง) plasma glucose ≥ 126 mg/dl 3. Plasma glucose ≥ 200 mg/dl ในการทํ า 2-hour/75gm oral GTT
2
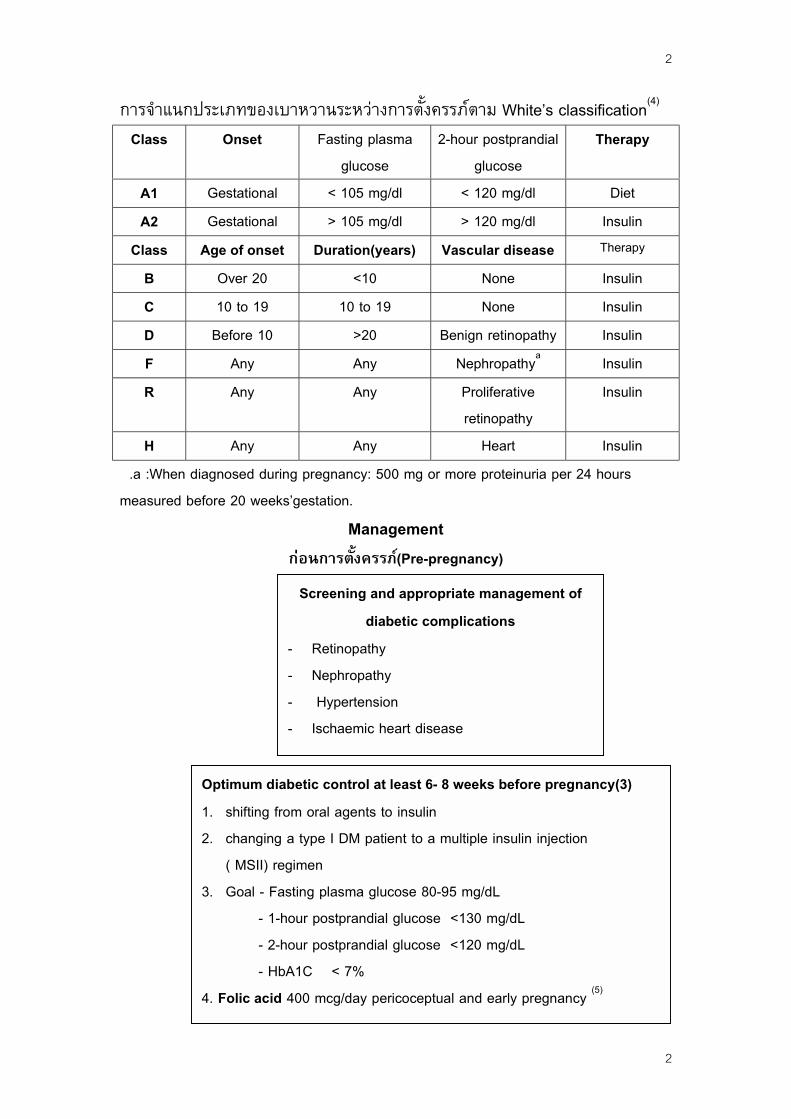
การจํ าแนกประเภทของเบาหวานระหวางการตั้งครรภตาม White’s classification(4)
Class Onset Fasting plasmaglucose
2-hour postprandialglucose
Therapy
A1 Gestational < 105 mg/dl < 120 mg/dl DietA2 Gestational > 105 mg/dl > 120 mg/dl Insulin
Class Age of onset Duration(years) Vascular disease Therapy
B Over 20 <10 None InsulinC 10 to 19 10 to 19 None InsulinD Before 10 >20 Benign retinopathy InsulinF Any Any Nephropathya InsulinR Any Any Proliferative
retinopathyInsulin
H Any Any Heart Insulin .a :When diagnosed during pregnancy: 500 mg or more proteinuria per 24 hoursmeasured before 20 weeks’gestation.
Managementกอนการต้ังครรภ(Pre-pregnancy)
----
Screening and appropriate management ofdiabetic complications
! Retinopathy! Nephropathy! Hypertension! Ischaemic heart disease
Optimum diabetic control at least 6- 8 weeks before pregnancy(3)1.! shifting from oral agents to insulin2.! changing a type I DM patient to a multiple insulin injection
( MSII) regimen3.! Goal - Fasting plasma glucose 80-95 mg/dL - 1-hour postprandial glucose <130 mg/dL - 2-hour postprandial glucose <120 mg/dL - HbA1C < 7%4. Folic acid 400 mcg/day pericoceptual and early pregnancy (5)
2
3
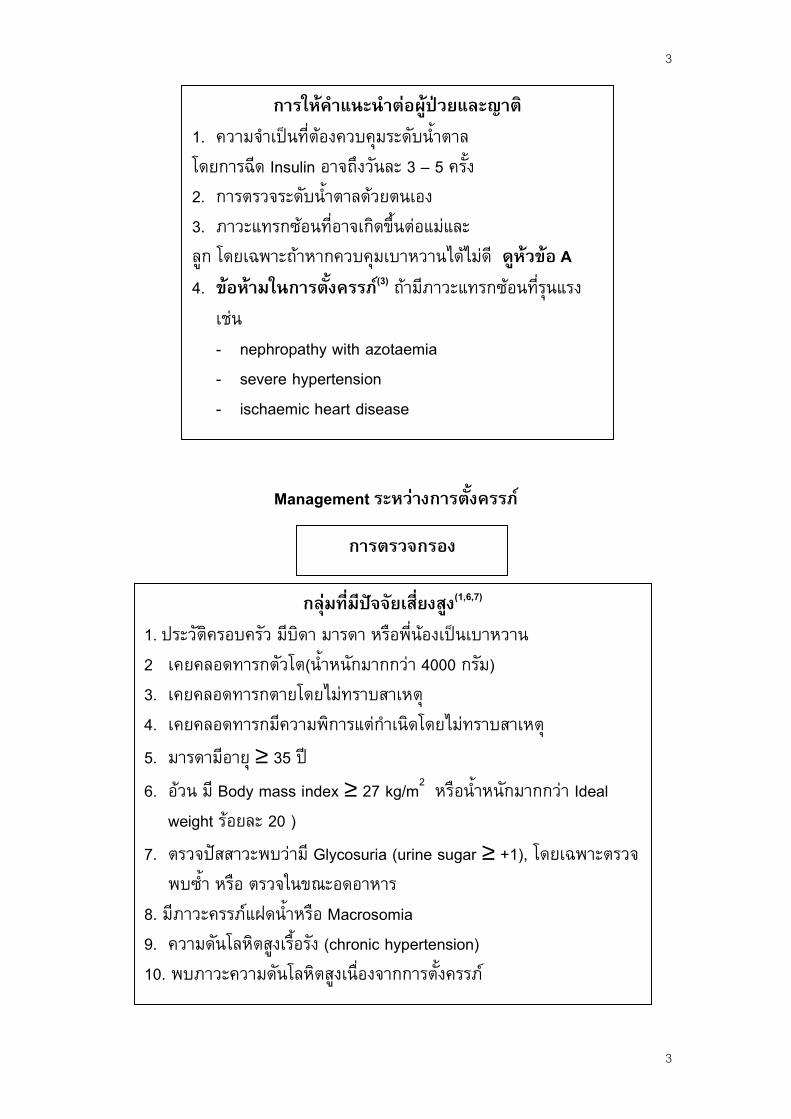
1.! ความจํ าโดยการฉีด2.! การตรว3.! ภาวะแทลูก โดยเฉพ4.! ขอหามเชน-! nep-! seve-! isch
1. ประวัติครอบครัว2! เคยคลอดทารก3.! เคยคลอดทารก4.! เคยคลอดทารก5.! มารดามีอายุ ≥6.! อวน มี Body m
weight รอยละ 7.! ตรวจปสสาวะพพบซํ้ า หรือ ตร
8. มีภาวะครรภแฝ9.! ความดันโลหิตส10. พบภาวะความ
การใหคํ าแนะนํ าตอผูปวยและญาติเปนที่ตองควบคุมระดับนํ้ าตาล
Insulin อาจถึงวันละ 3 – 5 ครั้งจระดับนํ้ าตาลดวยตนเองรกซอนที่อาจเกิดขึ้นตอแมและาะถาหากควบคุมเบาหวานไดไมดี ดูหวขอ Aในการตั้งครรภ(3) ถามีภาวะแทรกซอนที่รุนแรง
hropathy with azotaemiare hypertensionaemic heart disease
Management ระหวางการตั้งครรภ
มีบตัวโตายมีคว 35 ass20 )บวาวจในดนํ้ าูงเรื้อดันโ
การตรวจกรอง
กลุมท่ีมีปจจัยเส่ียงสูง(1,6,7)
ิดา มารดา หรือพี่นองเปนเบาหวานต(นํ้ าหนักมากกวา 4000 กรัม)โดยไมทราบสาเหตุามพิการแตกํ าเนิดโดยไมทราบสาเหตุป index ≥ 27 kg/m2 หรือนํ้ าหนักมากกวา Ideal
มี Glycosuria (urine sugar ≥ +1), โดยเฉพาะตรวจขณะอดอาหารหรือ Macrosomiaรัง (chronic hypertension)ลหิตสูงเนื่องจากการตั้งครรภ
3
4
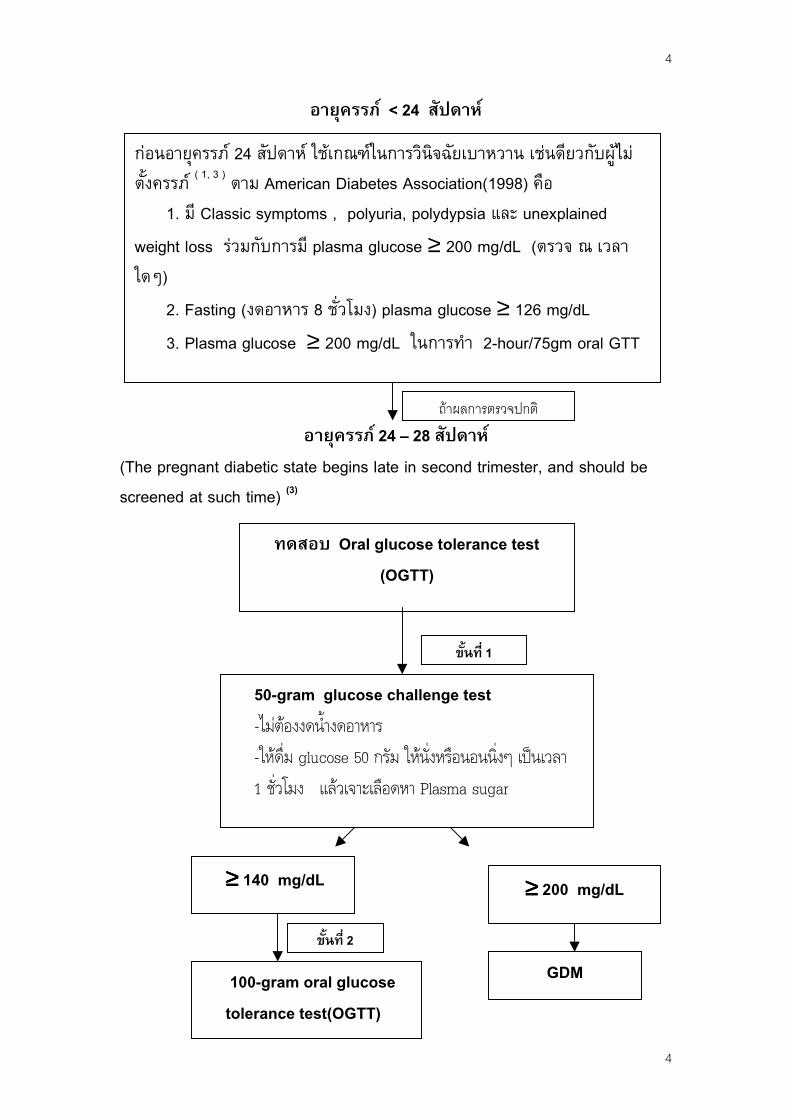
อายุครรภ < 24 สัปดาห
(Ts
กอนอายุครรภ 24 สัปดาห ใชเกณฑในการวินิจฉัยเบาหวาน เชนดียวกับผูไมต้ังครรภ ( 1, 3 ) ตาม American Diabetes Association(1998) คือ 1. มี Classic symptoms , polyuria, polydypsia และ unexplainedweight loss รวมกับการม ีplasma glucose ≥ 200 mg/dL (ตรวจ ณ เวลาใดๆ) 2. Fasting (งดอาหาร 8 ชั่วโมง) plasma glucose ≥ 126 mg/dL 3. Plasma glucose ≥ 200 mg/dL ในการทํ า 2-hour/75gm oral GTT
อายุครรภ 24 – 28 สัปดาหhe pregnant diabetic state begins late in second trimester, and should be
creened at such time) (3)
≥≥≥≥ 140
ิ
ทดสอบ Oral glucose tolerance test(OGTT)
1
50-gram glucose challenge test-ไมตองงดนํ ้างดอาหาร-ใหดื่ม glucose 50 กรัม ใหนั่งหรือนอนนิ่งๆ เปนเวลา1 ชั่วโมง แลวเจาะเลือดหา Plasma sugar
mg/dL ≥≥≥≥ 200 mg/dL
GDM
100-gram oral glucosetolerance test(OGTT)ขั้นท่ี
ขั้นท่ี 2
ถาผลการตรวจปกต
4
5
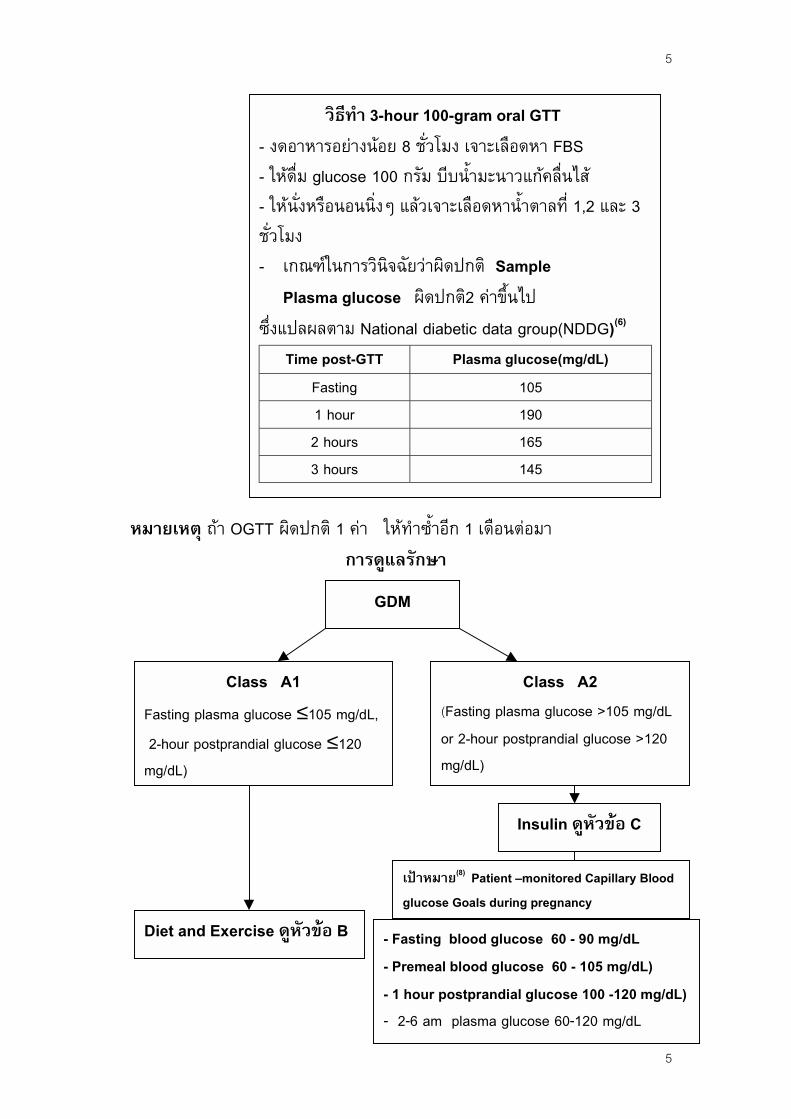
หมายเหตุ ถา OGTT ผิดปกติ 1 คา ใหทํ าซํ้ าอีก 1 เดือนตอมาการดูแลรักษา
GDM
Fasting plas 2-hour postmg/dL)
Class A2(Fasting plasma glucose >105 mg/dLor 2-hour postprandial glucose >120mg/dL)
- งดอาหา- ใหดื่ม g- ใหนั่งหชั่วโมง-! เกณฑ
Plasmซ่ึงแปลผ
TimeF123
Diet and E
Class A1ma glucose ≤105 mg/dL,prandial glucose ≤120
xercise ดูหัวข
วิธีท ํา 3-hour 100-gram oral GTTรอยางนอย 8 ชั่วโมง เจาะเลือดหา FBSlucose 100 กรัม บีบนํ้ ามะนาวแกคลื่นไสรือนอนน่ิงๆ แลวเจาะเลือดหานํ้ าตาลท่ี 1,2 และ 3
ในการวินิจฉัยวาผิดปกติ Samplea glucose ผิดปกติ2 คาข้ึนไปลตาม National diabetic data group(NDDG)(6)
post-GTT Plasma glucose(mg/dL)asting 105 hour 190 hours 165 hours 145
อ B
Insulin ดูหัวขอ C
- Fasting blood glucose 60 - 90 mg/dL- Premeal blood glucose 60 - 105 mg/dL)- 1 hour postprandial glucose 100 -120 mg/dL)- 2-6 am plasma glucose 60-120 mg/dL
เปาหมาย(8) Patient –monitored Capillary Bloodglucose Goals during pregnancy
5
6
6
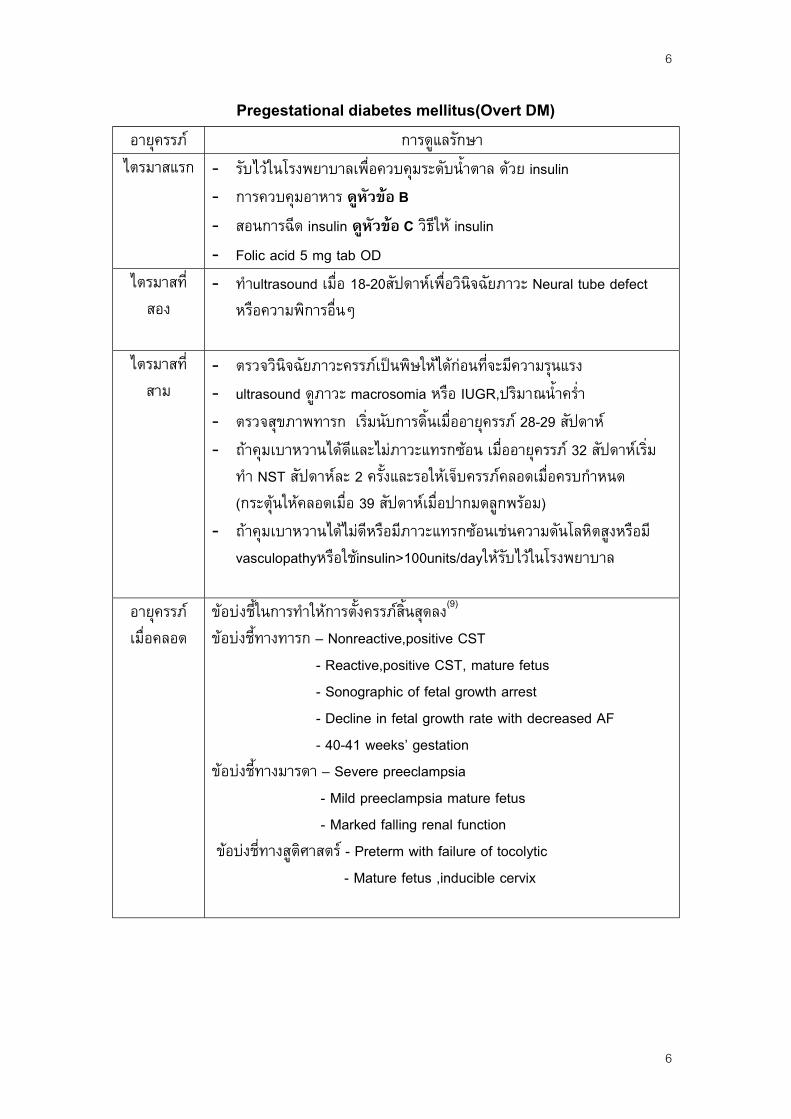
Pregestational diabetes mellitus(Overt DM)อายุครรภ การดูแลรักษาไตรมาสแรก !! รับไวในโรงพยาบาลเพ่ือควบคุมระดับน้ํ าตาล ดวย insulin
!! การควบคุมอาหาร ดูหัวขอ B!! สอนการฉีด insulin ดูหัวขอ C วิธีให insulin!! Folic acid 5 mg tab OD
ไตรมาสท่ีสอง
!! ทํ าultrasound เม่ือ 18-20สัปดาหเพื่อวินิจฉัยภาวะ Neural tube defectหรือความพิการอ่ืนๆ
ไตรมาสท่ีสาม
!! ตรวจวินิจฉัยภาวะครรภเปนพิษใหไดกอนท่ีจะมีความรุนแรง!! ultrasound ดูภาวะ macrosomia หรือ IUGR,ปริมาณน้ํ าคร่ํ า!! ตรวจสุขภาพทารก เร่ิมนับการด้ินเม่ืออายุครรภ 28-29 สัปดาห!! ถาคุมเบาหวานไดดีและไมภาวะแทรกซอน เม่ืออายุครรภ 32 สัปดาหเร่ิมทํ า NST สัปดาหละ 2 ครั้งและรอใหเจ็บครรภคลอดเมื่อครบกํ าหนด(กระตุนใหคลอดเมื่อ 39 สัปดาหเม่ือปากมดลูกพรอม)
!! ถาคุมเบาหวานไดไมดีหรือมีภาวะแทรกซอนเชนความดันโลหิตสูงหรือมีvasculopathyหรือใชinsulin>100units/dayใหรับไวในโรงพยาบาล
อายุครรภเมื่อคลอด
ขอบงช้ีในการทํ าใหการต้ังครรภส้ินสุดลง(9)
ขอบงช้ีทางทารก – Nonreactive,positive CST - Reactive,positive CST, mature fetus - Sonographic of fetal growth arrest - Decline in fetal growth rate with decreased AF - 40-41 weeks’ gestationขอบงช้ีทางมารดา – Severe preeclampsia - Mild preeclampsia mature fetus - Marked falling renal function ขอบงชี่ทางสูติศาสตร - Preterm with failure of tocolytic - Mature fetus ,inducible cervix

7
7
การดแูลระหวางคลอดและหลังคลอด
Breast feeding (ดูหัวขอ D)
contraception(ดูหัวขอ E)
-! นัดผาทองคลอด ถาประเมินนํ้ าหนักทารกมากกวา 4000 กรัม-! หลีกเล่ียงการ midpelvic operative delivery โดยเฉพาะในรายท่ี
Prolonged second stage of labor(อาจเกิด shoulder dystocia)-! ในระหวางการคลอดควบคุมระดับนํ้ าตาลใหอยูในชวง80-110
mg/dL-! Guidelines ในการใหinsulin เมื่อทํ า Elective cesarean sectionหรือ induction of labor หรือระหวางการคลอด
- ควรทํ าผาตัดในชวงเชา - ให fluid เปน 5% Dextrose Ringer’s lactate IV 125 ml/hour แนวทางการใหInsulinดูหัวขอ C ควบคุมระดับนํ้ าตาลใหได70 - 110 mg/dL เพื่อไมใหทารกเกิด hypoglycemia ตอนคลอด - วัดระดับนํ้ าตาล ทุก 2 ช่ัวโมงใน latent phase และทุก1 ช่ัวโมงในระยะ active phase - ตามกุมารแพทย - ผูปวย Pre-gestational DM หลังคลอดให insulin ตอ จนกระทั่งกินไดก็ตรวจระดับนํ้ าตาลทุก 4-6 ชั่วโมง และกลับไปใหinsulin ในขนาดท่ีไดกอนต้ังครรภ - ผูปวย GDM ใหหยุดให insulinทันทีท่ีคลอด แลวคอยประเมิน OGTTใหม 6 สัปดาหหลังคลอด

8
Elective cesarean section
- NPO after midnight- ควรผาตัดในชวงตอนเชา- ให NPH ฉีดใน Dose กอนนอนได- ตรวจ BS (Dextrostick) ตอนเชาวนัผาตดั
BS < 60 mg % BS > 60 mg %
5%D/RLS 1000 mlIV 125 ml/hr
10% D/N 1000 mlIV
- งด Insulin (คหลังคลอด)(2)- ตรวจ FBS, 1- ถา FBS > 10mg/dL ให ins- ทํ า 75 gm O
- NPO หลังผาตัด- BS q 4 hrs
BS > 120 mg/dL ฉีด RI 3 U scBS > 140 mg/dL ฉีด RI 4 U scBS > 200 mg/dL ฉีด RI 5 U scBS > 250 mg/dL ฉีด RI 10 U sc
8
เมื่อกินไดวามตองการ insulin ในGDM ลดลง 50-75 %
hr postprandial BS0 mg/dL, 1 hr postprandial BS > 150ulin (0.6 U/kg/day)หรือปรึกษาอายุรแพทยGTT หลังคลอด 6 สัปดาห
9
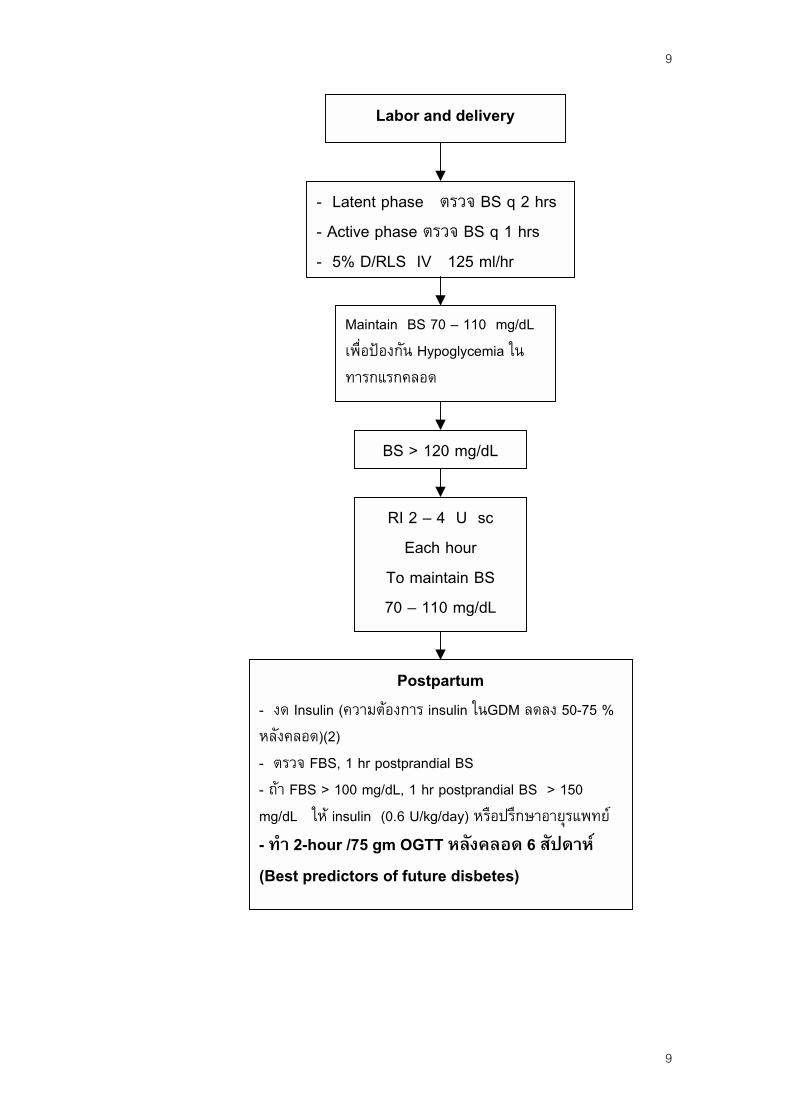
Labor and delivery
- งด Insหลังคลอ- ตรวจ - ถา FBSmg/dL - ทํ า 2-h(Best p
- Latent phase ตรวจ BS q 2 hrs- Active phase ตรวจ BS q 1 hrs- 5% D/RLS IV 125 ml/hr
Maintain BS 70 – 110 mg/dLเพื่อปองกัน Hypoglycemia ในทารกแรกคลอด
L
ulin (ความด)(2)FBS, 1 hr > 100 mgให insulin our /75 g
redictors
BS > 120 mg/d
RI 2 – 4 U scEach hour
To maintain BS70 – 110 mg/dL
ตอ
po/d
(0m o
Postpartumงการ insulin ในGDM ลดลง 50-75 %
stprandial BSL, 1 hr postprandial BS > 150.6 U/kg/day) หรือปรึกษาอายุรแพทย OGTT หลังคลอด 6 สัปดาหf future disbetes)
9
10
10
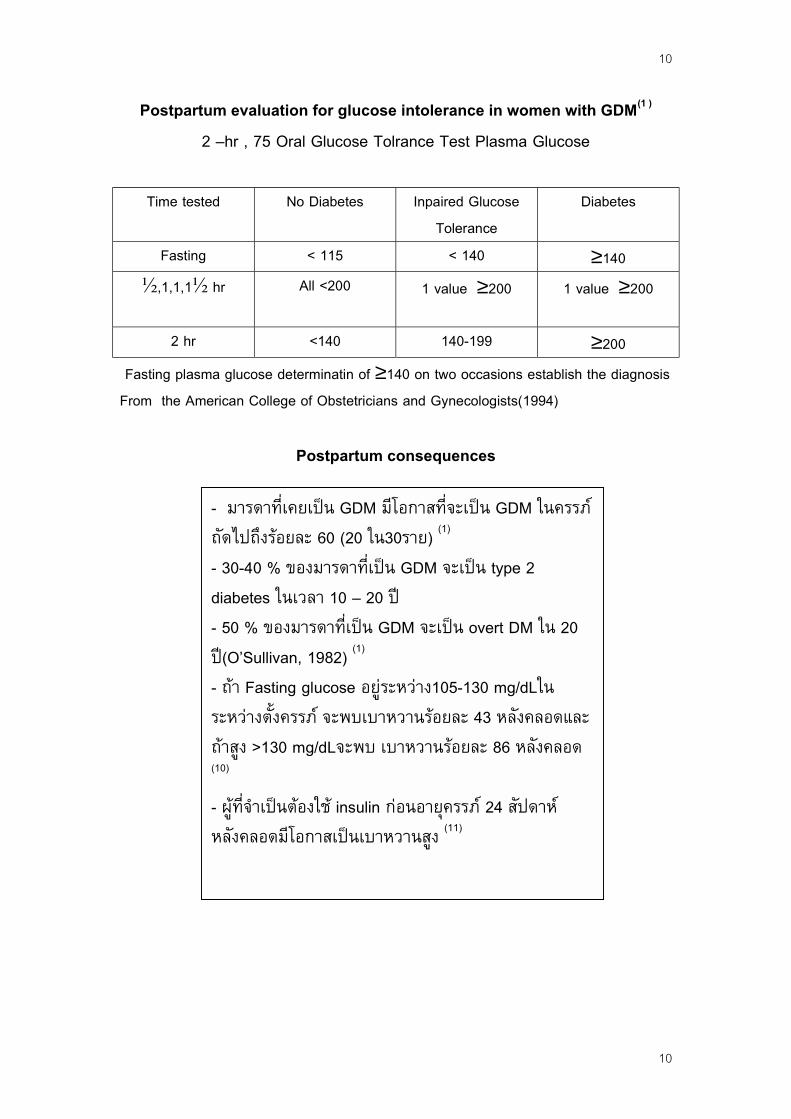
Postpartum evaluation for glucose intolerance in women with GDM(1 )
2 –hr , 75 Oral Glucose Tolrance Test Plasma Glucose
Time tested No Diabetes Inpaired GlucoseTolerance
Diabetes
Fasting < 115 < 140 ≥140",1,1,1" hr All <200 1 value ≥200 1 value ≥200
2 hr <140 140-199 ≥200 Fasting plasma glucose determinatin of ≥140 on two occasions establish the diagnosisFrom the American College of Obstetricians and Gynecologists(1994)
Postpartum consequences
- มารดาที่เคยเปน GDM มโีอกาสที่จะเปน GDM ในครรภถัดไปถึงรอยละ 60 (20 ใน30ราย) (1)
- 30-40 % ของมารดาท่ีเปน GDM จะเปน type 2diabetes ในเวลา 10 – 20 ป- 50 % ของมารดาท่ีเปน GDM จะเปน overt DM ใน 20ป(O’Sullivan, 1982) (1)
- ถา Fasting glucose อยูระหวาง105-130 mg/dLในระหวางต้ังครรภ จะพบเบาหวานรอยละ 43 หลังคลอดและถาสูง >130 mg/dLจะพบ เบาหวานรอยละ 86 หลังคลอด(10)
- ผูที่จํ าเปนตองใช insulin กอนอายุครรภ 24 สัปดาหหลังคลอดมีโอกาสเปนเบาหวานสูง (11)

11
11
หัวขอ Aผลกระทบตอมารดา และทารก
ผลกระทบตอมารดา(1,3)
-! Maternal morbidity สาเหตุที่พบไดบอยคือ: Hypertension/pre-eclampsia, ketoacidosis และ pyelonephritis.
-! Preterm labour พบไดรอยละ 20-! Pre-eclampsia มักเปนสาเหตุของการคลอดกอนกํ าหนด พบไดรอยละ15 –30 ไมวาจะควบคุมเบาหวานไดดีหรือไม risk factors คือHypertension, proteinuria/nephropathy และ vascular disease
-! Proteinuria กอน 20 สัปดาห พบ10-20% ของ Type I DM การมีNephropathyจะเพิ่มอุบัติการณของ Pre-eclampsia
-! Ketoacidosis พบได < 1% Risk factors ไดแก Hyperemesisgravidarum, infections , การใช tocolysisและ glucocorticoid เรง Lungmaturation พบ fetal loss 20 % และเพิ่มเปน 50% ถาเปนซํ้ า
-! Infections : พบได 75-80% commom sites ไดแก urogenital area,respiratory tract , TB ในประเทศกํ าลังพัฒนา- urinary tract infection พบไดรอยละ 20 เมื่อมาฝากครรภครั้งแรกจึงควรตรวจกรองภาวะ asymtomatic bacteriuria โดยการเพาะเชื้อจากปสสาวะ และทํ าซ้ํ าเม่ืออายุครรภ 32 สัปดาห และเมื่อมีอาการ
- แผลผาตัดติดเช้ือ ไดงาย ทุกรายจึงควรไดรับยาปฎิชีวนะปองกัน-! Hydramnios: พบได 10-20%-! Hypoglycemia : เกิดไดปลายไตรมาสที่สาม Nocturnal hypoglycemiaอาการฝนราย ปวดศีรษะตอนเชา
-! Diabetic retinopathy: พบ > 50% ใน type I DM, 10 % ใน type IIDM มีรายงานการต้ังครรภทํ าให retinopathy แยลง
-! Cesarean section and traumatic delivery เพิ่มขึ้น
12
12
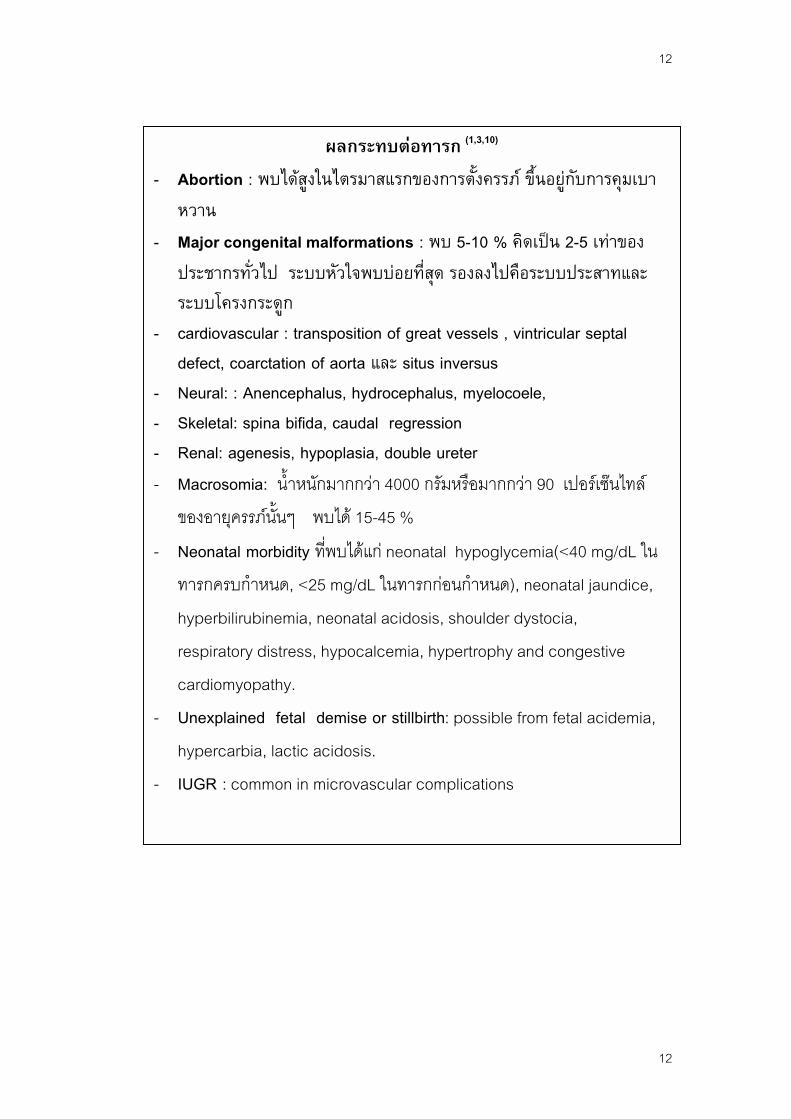
ผลกระทบตอทารก (1,3,10)
-! Abortion : พบไดสูงในไตรมาสแรกของการต้ังครรภ ขึ้นอยูกับการคุมเบาหวาน
-! Major congenital malformations : พบ 5-10 % คิดเปน 2-5 เทาของประชากรทั่วไป ระบบหัวใจพบบอยที่สุด รองลงไปคือระบบประสาทและระบบโครงกระดูก
-! cardiovascular : transposition of great vessels , vintricular septaldefect, coarctation of aorta และ situs inversus
-! Neural: : Anencephalus, hydrocephalus, myelocoele,-! Skeletal: spina bifida, caudal regression-! Renal: agenesis, hypoplasia, double ureter-! Macrosomia: น้ํ าหนักมากกวา 4000 กรัมหรือมากกวา 90 เปอรเซนไทลของอายุครรภน้ันๆ พบได 15-45 %
-! Neonatal morbidity ท่ีพบไดแก neonatal hypoglycemia(<40 mg/dL ในทารกครบกํ าหนด, <25 mg/dL ในทารกกอนกํ าหนด), neonatal jaundice,hyperbilirubinemia, neonatal acidosis, shoulder dystocia,respiratory distress, hypocalcemia, hypertrophy and congestivecardiomyopathy.
-! Unexplained fetal demise or stillbirth: possible from fetal acidemia,hypercarbia, lactic acidosis.
-! IUGR : common in microvascular complications
13
13
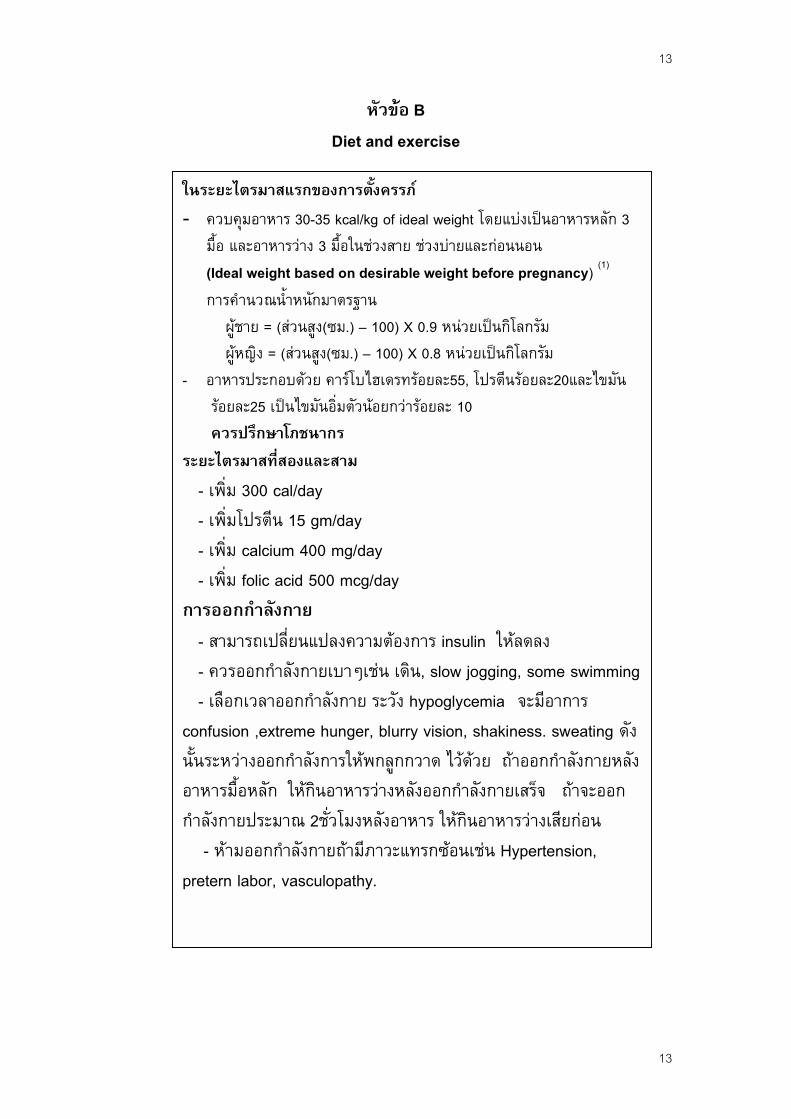
หัวขอ BDiet and exercise
ในระยะไตรมาสแรกของการต้ังครรภ!! ควบคุมอาหาร 30-35 kcal/kg of ideal weight โดยแบงเปนอาหารหลกั 3ม้ือ และอาหารวาง 3 ม้ือในชวงสาย ชวงบายและกอนนอน(Ideal weight based on desirable weight before pregnancy) (1)
การคํ านวณน้ํ าหนักมาตรฐาน ผูชาย = (สวนสูง(ซม.) – 100) X 0.9 หนวยเปนกิโลกรัม ผูหญิง = (สวนสูง(ซม.) – 100) X 0.8 หนวยเปนกิโลกรัม
- อาหารประกอบดวย คารโบไฮเดรทรอยละ55, โปรตนีรอยละ20และไขมัน รอยละ25 เปนไขมันอ่ิมตัวนอยกวารอยละ 10 ควรปรึกษาโภชนากรระยะไตรมาสที่สองและสาม - เพิ่ม 300 cal/day - เพ่ิมโปรตีน 15 gm/day - เพิ่ม calcium 400 mg/day - เพิ่ม folic acid 500 mcg/dayการออกกํ าลังกาย - สามารถเปลี่ยนแปลงความตองการ insulin ใหลดลง - ควรออกกํ าลังกายเบาๆเชน เดิน, slow jogging, some swimming - เลือกเวลาออกก ําลังกาย ระวัง hypoglycemia จะมีอาการconfusion ,extreme hunger, blurry vision, shakiness. sweating ดังนั้นระหวางออกกํ าลังการใหพกลูกกวาด ไวดวย ถาออกกํ าลังกายหลังอาหารมื้อหลัก ใหกินอาหารวางหลังออกกํ าลังกายเสร็จ ถาจะออกกํ าลังกายประมาณ 2ช่ัวโมงหลังอาหาร ใหกินอาหารวางเสียกอน - หามออกกํ าลังกายถามีภาวะแทรกซอนเชน Hypertension,pretern labor, vasculopathy.
14
14
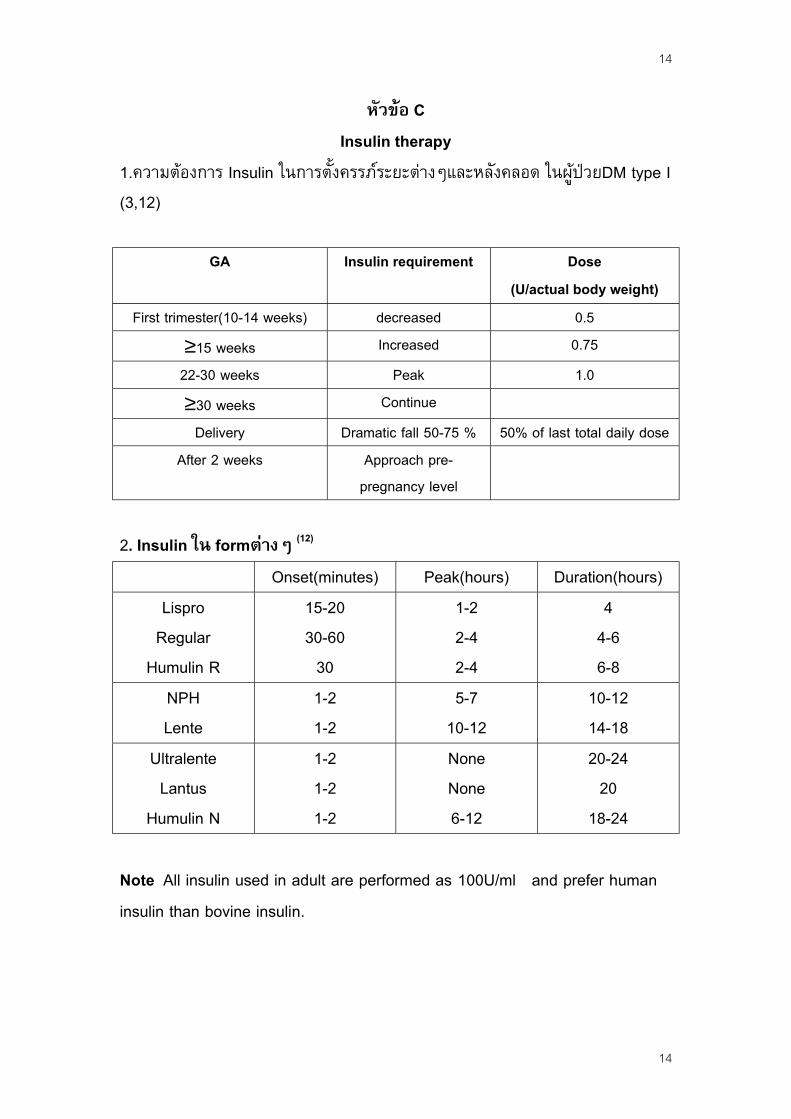
หัวขอ CInsulin therapy
1.ความตองการ Insulin ในการต้ังครรภระยะตางๆและหลังคลอด ในผูปวยDM type I(3,12)
GA Insulin requirement Dose(U/actual body weight)
First trimester(10-14 weeks) decreased 0.5≥15 weeks Increased 0.7522-30 weeks Peak 1.0≥30 weeks Continue
Delivery Dramatic fall 50-75 % 50% of last total daily doseAfter 2 weeks Approach pre-
pregnancy level
2. Insulin ใน formตางๆ (12)
Onset(minutes) Peak(hours) Duration(hours)Lispro
RegularHumulin R
15-2030-60
30
1-22-42-4
44-66-8
NPHLente
1-21-2
5-710-12
10-1214-18
UltralenteLantus
Humulin N
1-21-21-2
NoneNone6-12
20-242018-24
Note All insulin used in adult are performed as 100U/ml and prefer humaninsulin than bovine insulin.

15
15
3. Protocol for administration of insulin to pregnant(2)Regimen Before breakfast Before
lunchBeforedinner
At bedtime
1 Short acting insulin+ intermediate
- Short acting insulin+ intermediate
-
2 Short acting insulin+ intermediate
Short actinginsulin
Short acting insulin+ intermediate
-
3 Short acting insulin Short actinginsulin
Short acting insulin+ intermediate
-
4 Short acting insulin Short actinginsulin
Short actinginsulin
Intermediateor long
5 Intermediateor long acting insulin
+ Short actinginsulin
Short actinginsulin
Short acting insulin -
6 CSII(continuous subcutaneous insulin)Note All pregnant diabetics should be administered insulin by a multiplesubcutaneous insulin injection schedule or MSII(i.e. regimen 4) Follow-up : fasting and 1 hour postprandial plasma glucose every 1-2weeks, fasting urinary ketone.4.! Guideline for low-dose continuous insulin infusion for the diabetic women during the intrapartum period (1) (ACOG1994)
Blood glucose(mg/dL)
Insulin dosageU/hr *
Fluid(125ml/hr)
< 100 0 D5 lactated Ringer100 - 140 1.0 D5 lactated Ringer141 - 180 1.5 Normal saline181 - 220 2.0 Normal saline
> 220 2.5 Normal saline* 25 U of RI + 250 ml Normal saline IV sideline 10 µµµµd/min = 1U/hr1 mmol/L = 18 mg/dL

16
การให RI ตาม sliding scaleBlood glucose
mg/dL mmol/LInsulin(Units)
SC145-198 8.1 – 11.0 1-2200-234 11.1 – 13.0 2-3> 234 > 13.0 3-5
Note If significant ketonuria ,aditional insulin is likely needed and change IV to D10 W IV 125 ml/hr until ketones clear.
หัวขอ DBreast feeding
หัวขอ EContraception
หัวขอ Eการคุมกํ าเนิด
-! ควรสงเสริมใหทารกที่คลอดจากมารดาที่เปนเบาหวาน ดูดนมมารดาเร็วที่สุดเทาที่จะทํ าได
-! ทารกที่คลอดจากมารดาที่คุมเบาหวานไดดี ไมมีการบาดเจ็บจากการคลอด และไมมี Birth asphyxia สมควรใหมารดาเลี้ยงทันทีหลังคลอดภายใน 1 –2 ชั่วโมง
-! เพิ่มอาหารใหแกมารดา 100-300 แคลอรีทุกครั้งหลังใหนมลูกเพื่อ ปองกันภาวะ reactive hypoglycemia-! ในGDMการใหนมบุตรสามารถลดและ ชะลอ การเกิดเบาหวานในอนาคต
- การใช oral hypoglycemic drug ?
Combined pills-! ไมควรใชในผูปวยเบาหวานท่ีมีความเส่ียงของ vascular disease-! ใชชนิด Low dose ในผูปวยท่ีไมมี vascular disease หรือไมมีประวัติ
ischemic heart diseaseProgestin ชนิดฉีดหรือรับประทาน สามารถใชไดเพราะมีผลกระทบตอCarbohydrate metabolism นอยIUD : ไมแนะนํ าใหใชเน่ืองจากมีความเส่ียงจากการติดเช้ือBarrier methods เชน Condom เปนการคุมกํ าเนิดท่ีเหมาะท่ีสุด แตถาลูกพอแลวสมควรทํ าหมัน
16
17
17
เอกสารอางอิง1. Cunningham FG, Gant NF, Leveno KJ et al. Diabetes .Williams Obstetrics, 21th ed.Mc Graw-Hill 2001:1360-1377.2. O’Sullivan JB: Body weight and subsequent diabetes mellitus JAMA 248:949,1982.3. Atul G, Alka G :Management of fiabetes mellitus(DM) durin pregnacy . Obstetricsand Gynaecology Communications 2000:2(4):43-50.4. American College of Obstetricians and Gynecologists: Management of diabetesmellitus in pregnancy. Technical Bulletin No.92, May 1986.5. Milunsky A, Jick H,Bruell CL, MacLaughlin DS, Rothman FJ, Willett W:Multivitamin/folic acid supplementation in early pregnancy reduces the prevalence ofneural tube defect. JAMA 262:2847, 1989.6. American College of Obstetricians and Gynecologists: Diabetes and pregnancy.ACOG Tech Bull 1994:200.7. Bartha JL, Martinez – Ddel – Fresno P, comino – Delgado R. Gestational diabetesmellitus diagnosed during early pregnancy. Am J Obstet Gynecol 2000:182:346-50.8. American Diabetes Association: Medical Management of Pregnancy Complicated byDiabetes, 2nd ed. Jovanovic-Peterson L (ed). Alexandris, VA, ADA,1995.9. Moore TR, Diabetes in pregnancy . In :Creasy RK, Resnik R, editor Matenal-fetalmedicine . 4th ed. Pheadelphia:EB Sanders company, 1999:964-9.10. Landon MB, Gabbe SG,.Diabetes mellitus in :Barron WM, Lindheiner MD, DavisonJM, editor, Medical disorders during pregnancy , 2th ed . St. Louis:mosby-Year Book,Inc, 1995:63-88.11. Bartha JL, Martinez – Del – Fresno P, Comino - Delgado R. Gestational diabetesmellitus diagnosed during early pregnancy . Am J Obstet Gynecol 2000;182:346-50.12. Jose LG. Management of diabetes in pregnancy. Clin Obstet Gynecol 2002;45:165-169.
จัดทํ าโดยแพทยกลุมงานสูติ-นรีเวชกรรมฯ โรงพยาบาลสงขลา
28 มกราคม 2546

18
18
Pregnancy: Gliclazide should not be taken by pregnant women.Breast-feeding: Some sulfonylurea drugs like gliclazide are excreted in breast milk, but it is notknown whether gliclazide is one of them. Because the potential for low blood sugar in nursing infantsmay exist, a decision should be made whether to discontinue nursing or to discontinue the drug,taking into account the importance of the drug to the mother.Children: The safety and effectiveness for children of this drug have not been established.





























