Embed Size (px)
Citation preview

7/28/2019 Distribution of Subclass IgG
http://slidepdf.com/reader/full/distribution-of-subclass-igg 1/6
Nephrol Dial Transplant (2004) 19: 574–579
DOI: 10.1093/ndt/gfg616
Original Article
Distribution of glomerular IgG subclass deposits
in malignancy-associated membranous nephropathy
Hiroshi Ohtani1, Hideki Wakui1, Atsushi Komatsuda1, Shin Okuyama1, Rie Masai1,Nobuki Maki1, Akihiro Kigawa1, Ken-ichi Sawada1 and Hirokazu Imai1,2
1The Third Department of Internal Medicine, Akita University School of Medicine, Akita and2The Department of Nephrology and Rheumatology, Aichi Medical University, Aichi, Japan
Abstract
Background. Several studies have shown a predomi-nant glomerular deposition of IgG4 in patients withidiopathic membranous nephropathy (MN), whereassignificant depositions of other IgG subclasses havebeen shown in patients with lupus-associated MN andbucillamine-induced MN.Methods. We examined the distribution patterns of glomerular IgG subclass deposits in 10 patients withmalignancy-associated MN (M-MN) and in 15 patientswith idiopathic MN by immunofluorescence (IF)microscopy.Results. The glomerular IF intensities of IgG1 andIgG2 were significantly stronger in the malignancy
group than in the idiopathic group (P<0.05). Incontrast, there were no differences in glomerular IFintensities of IgG3 and IgG4 between the two groups.Conclusion. Our findings suggest that the distributionpatterns of glomerular IgG subclass deposits aredifferent in idiopathic MN and M-MN. The strongIF intensity of glomerular IgG1 and IgG2 in M-MNmay provide a possible predictor for this condition.
Keywords: IgG subclasses; immune complex; immuno-fluorescence; malignancy; membranous nephropathy
Introduction
Membranous nephropathy (MN), the common causeof the adult nephrotic syndrome, is characterized byglomerular subepithelial IgG deposits. Human IgG isdivided into four subclasses (IgG1, IgG2, IgG3 andIgG4) according to antigenic differences in their heavy
chains. Each subclass differs in terms of several aspects:
encoding genes, molecular weights, isoelectric pointand interaction with complements [1]. These IgG sub-classes are produced preferentially in response todifferent antigens [2].
A number of studies have shown differing distribu-tion patterns of glomerular IgG subclass deposits inpatients with glomerular diseases [3–8]. For example, apredominant glomerular deposition of IgG4 is char-acteristic of idiopathic MN [3,4,6,7,9]. In the case of lupus-associated MN, several reports have shown theglomerular deposition of IgG1, IgG2 and IgG3, as wellas IgG4 [6,7]. Furthermore, Nagahama et al . [8] showedglomerular deposition of IgG2 and/or IgG3, in addi-
tion to IgG4, in bucillamine-induced MN. Altogther,these findings suggest that the pathogenesis of idio-pathic MN is different from that of some secondaryforms of MN.
It has been documented that 10% of MN cases areassociated with malignancy [10–12]. In fact, severalinvestigators have reported both resolution and exacer-bation of malignancy-associated MN (M-MN) duringtumour treatment in certain patients [10,13,14]. Thesefindings suggested a causal relationship between MNand malignancy.
In the present study, we examined by immunofluo-rescence (IF) microscopy the distribution of glomerularIgG subclass deposits in 10 patients with M-MN and
in 15 patients with idiopathic MN. We found thatthe glomerular IF intensity of IgG1 and IgG2 in themalignancy group was significantly stronger than in theidiopathic group. These findings suggest that M-MNand idiopathic MN result from different immunologi-cal mechanisms.
Subjects and methods
Patients with biopsy-proven MN were selected for review inthis study. The biopsies were performed at Akita University
Correspondence and offprint requests to: Hiroshi Ohtani, MD, ThirdDepartment of Internal Medicine, Akita University School of Medicine, 1-1-1 Hondo, Akita City, Akita 010-8543, Japan. Email:[email protected]
Nephrol Dial Transplant Vol. 19 No. 3ß
ERA–EDTA 2004; all rights reserved

7/28/2019 Distribution of Subclass IgG
http://slidepdf.com/reader/full/distribution-of-subclass-igg 2/6
Hospital and its affiliated hospitals from 1985 to 2002. In all,we found 311 cases with MN. Among them, 15 patients(4.8%) were diagnosed as having M-MN by the following
criteria: (i) the existence of malignancy discovered at thetime of or after the biopsy, as well as in treated cases; or
(ii) the reduction or disappearance of proteinuria aftertherapy for malignancy. We selected 10 of these 15 casesthat had adequate frozen tissues available for stainingglomerular IgG subclass deposits. In addition, 15 cases
were selected randomly from patients with idiopathic MN inwhom malignancy was excluded using basic routine cancerscreening procedures.
Renal biopsy specimens were processed using standard
light and electron microscopy techniques. MN lesions wereclassified into four stages based on microscopy findings. Forthe IF studies, frozen renal tissues were cut into 4mm sectionswith a cryostat, and were stained with fluorescein isothio-
cyanate (FITC)-conjugated rabbit monospecific antibodiesagainst human IgG, IgA and IgM heavy chains, and lightchains, C3, C1q and fibrinogen (DAKO A/S, Glostrup,
Denmark) at a 10-fold dilution. The sections were alsostained with FITC-conjugated mouse monoclonal antibodiesagainst human IgG1 (Fc), IgG2 (Fab), IgG3 (F(ab’)2) and
IgG4 (pFc) (The Binding Site Ltd, Birmingham, UK) at a10-fold dilution. The names of theclones of theses monoclonalantibodies were: anti-human IgG1, 8c/6–39; anti-humanIgG2, HP6014; anti-human IgG3, HP6050; and anti-human
IgG4, HP6023. IF intensity was graded as: negative (score 0),weakly positive (score 0.5), 1þ (score 1.0), 2þ (score 2.0) and3þ (score 3.0). This assessment was performed by three
observers that were blind to the background data. The inter-observer comparisons showed good agreement ( values [15]:0.72, 0.73 and 0.87). When different scores were obtainedfrom the observers, only the majority scores were adopted.
We compared the intensity of IgG subclasses in the M-MNand idiopathic MN groups using Mann–Whitney U -tests,
because the data did not show a Gaussian distribution.
Results
Background of patients
Profiles of the 25 patients in this study are shownin Table 1. Six M-MN patients and eight idiopathicMN patients presented with nephrotic range protein-uria (>3.5 g/day). The time between clinical onset of proteinuria and recognition of the tumour ranged from7 days to 9 months. All patients had solid tumours of various types. In terms of treatment, tumours werecompletely resected in five patients. In six M-MN
patients, proteinuria improved after the treatment of the tumour. The remaining four patients were nottreated because they had multiple metastasis at the timeof diagnosis. Proteinuria persisted in these patients, andall of them died due to the malignancy.
Histological findings
Histological findings for each case in both of the groupsare shown in Table 2. Mesangial proliferation wasabsent or mild in all the patients. In addition, the meanstages of MN did not differ between the two groups.
The IF intensity of IgG, IgA, IgM, , , C3, C1q andfibrinogen was similar in the two groups.
IF intensity of glomerular IgG subclass deposits
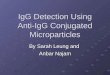
IF intensities of glomerular IgG subclass deposits in thetwo groups are shown in Table 3. In addition,representative IF findings are shown in Figures 1 and 2.
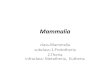
In Figure 3, the glomerular IF intensities of each IgGsubclass from the two groups are shown. The intensitiesof IgG1 and IgG2 in the M-MN group were signifi-cantly stronger than in the idiopathic MN group(P<0.05). In further studies, we examined whetherthe glomerular IF intensity of IgG1 and IgG2 could beused as a predictor of M-MN. The potential values of IgG1 and IgG2 glomerular staining for distinguishingM-MN from idiopathic MN are illustrated in Table 4.When scoring levels were set at 1.0 for both IgG1 andIgG2 IF intensities, the sensitivity and specificity were70 and 80%, respectively.
Discussion
In a previous IF study that used a set of anti-IgGsubclass monoclonal antibodies, we found strikingdifferences in the distribution of glomerular IgGsubclass deposits between patients with membranopro-liferative glomerulonephritis, idiopathic MN and lupusnephritis [7]. The present study used the same set of antibodies and showed differing distribution patternsof glomerular IgG subclass deposits in patients withM-MN and idiopathic MN.
Idiopathic MN is now regarded as an IgG4-mediateddisease [9]. In contrast, there are several reports that
lupus-associated MN [6,7] and bucillamine-inducedMN [8] are characterized by other IgG subclassglomerular deposits. These observations suggest thatimmune complexes containing other than IgG4 may beimportant factors in certain secondary forms of MN.
Approximately 10% of MN cases are associated withmalignancy, and diagnosis of MN is sometimes thefirst clue to the presence of malignancy [10–12].Brueggemeyer et al . [11] found that the incidence of malignancy in MN patients was almost five timesgreater than in a control population. Also, the findingsthat tumour treatment produced resolution of thenephrotic syndrome and that relapse occurred followingtumour recurrence or metastasis suggest a causal
relationship between MN and malignancy [10,13,14].Furthermore, tumour-related antigens or antibodies tothese antigens have been detected in the glomerulardeposits in some cases of M-MN [16–18], althoughtumour-specific antigen–antibody complexes have notyet been identified.
To our knowledge, there have been no detailedanalyses of glomerular IgG subclass deposits in M-MN.In the present study, we showed a more dominantglomerular deposition of IgG1 and IgG2 in patientswith M-MN than in those with idiopathic MN. Incontrast, there were no differences in glomerular IF
IgG subclasses in malignancy-associated MN 575

7/28/2019 Distribution of Subclass IgG
http://slidepdf.com/reader/full/distribution-of-subclass-igg 3/6
T a b l e
1 . P r o fi l e s o f 1 0 p a t i e n t s w i t h
M - M N
a n d 1 5 p a t i e n t s w i t h i d i o p a t h i c M
N
C a s e n o .
A g e
S e x
S C r
( m g / d l )
T . P / A l b
( m g
/ d l )
P r o t e i n u r i a
( g / d a y )
O n s e t o f
p r o t e i n u r i a
R e c o g n i t i o n
o f t u m o u r
T y p e o f
m a l i g n a n c y
H
i s t o l o g y
o f t u m o u r
T r e a t m e n t
f o r t u m o u r
C h a n g e o f
p r o t e i n u r i a
P a t i e n t
o u t c o m e
1
6 5
M
1 . 2
6 . 1 / 3 . 6
4 . 8
J u n e 1 9 8 5
J u l y
1 9 8 5
C o l o n i c c a n c e r
A
d e n o c a r c i n o m a
C o l o n e c t o m y
C R
A l i v e
2
6 0
M
0 . 8
3 . 3 / 1 . 3
1 0 . 0
O c t o b e r 1 9 9 4
N o v
e m b e r 1 9 9 4
L u n g c a n c e r
S q u a m o u s c e l l c a r c i n o m a
N o t r e a t m e n t
N o c h a n g e
D e a d
3
6 0
M
0 . 9
5 . 0 / 2 . 6
1 5 . 0
J u l y 1 9 9 5
O c t o
b e r 1 9 9 5
O e s o p h a g e a l c a n c e r
S q u a m o u s c e l l c a r c i n o m a
N o t r e a t m e n t
N o c h a n g e
D e a d
4
8 0
M
0 . 9
7 . 2 / 2 . 8
2 . 0
O c t o b e r 1 9 9 5
J u l y
1 9 9 6
C o l o n i c c a n c e r
A
d e n o c a r c i n o m a
N o t r e a t m e n t
N o c h a n g e
D e a d
5
6 2
F
0 . 4
6 . 1 / 3 . 8
1 . 6
J u l y 1 9 9 6
A u g u s t 1 9 9 6
G a s t r i c c a n c e r
A
d e n o c a r c i n o m a
G a s t r e c t o m y
C R
A l i v e
6
7 4
M
1 . 0
4 . 0 / N A
5 . 0
O c t o b e r 1 9 9 9
N o v
e m b e r 1 9 9 9
R e n a l c a n c e r
R
e n a l c e l l c a r c i n o m a
N e p h r e c t o m y
r e d u c e d
A l i v e
7
6 4
M
0 . 8
5 . 3 / 3 . 0
0 . 7
N o v e m b e r 1 9 9 9
A u g u s t 2 0 0 0
P r o s t a t i c c a n c e r
A
d e n o c a r c i n o m a
P r o s t a t e c t o m y
C R
A l i v e
8
7 5
M
0 . 9
4 . 3 / N A
1 0 . 2
J u l y 2 0 0 0
N o v
e m b e r 2 0 0 0
L u n g c a n c e r
N
A
N o t r e a t m e n t
N o c h a n g e
D e a d
9
5 4
M
1 . 1
5 . 7 / 3 . 5
4 . 7
J u n e 2 0 0 2
J u n e
2 0 0 2
G a s t r i c c a n c e r
A
d e n o c a r c i n o m a
G a s t r e c t o m y
R e d u c e d
A l i v e
1 0
6 4
F
0 . 6
6 . 2 / 3 . 6
2 . 5
J u l y 2 0 0 2
O c t o
b e r 2 0 0 2
M e t a s t a t i c b r a i n t u m o u r M
a l i g n a n t t h y m o m a e
T h y m o t e c t o m y ,
I R
R e d u c e d
A l i v e
1 1
6 9
M
0 . 7
3 . 9 / 2 . 0
2 . 8
S e p t e m b e r 1 9 8 1
C R
A l i v e
1 2
4 6
F
0 . 4
4 . 7 / 2 . 2
4 . 5
A u g u s t 1 9 8 3
C R
A l i v e
1 3
7 9
M
1 . 9
5 . 0 / 2 . 5
4 . 8
J a n u a r y 1 9 9 0
P R
A l i v e
1 4
5 2
M
0 . 7
5 . 1 / 2 . 4
4 . 5
O c t o b e r 1 9 9 2
N o c h a n g e
D e a d
1 5
5 7
F
0 . 5
6 . 5 / 3 . 7
0 . 7
A p r i l 1 9 9 3
C R
A l i v e
1 6
5 0
M
0 . 4
6 . 7 / 3 . 4
2 . 4
N o v e m b e r 1 9 9 3
P R
A l i v e
1 7
4 0
F
0 . 5
7 . 1 / 4 . 1
0 . 9
J u n e 1 9 9 4
P R
A l i v e
1 8
3 7
M
0 . 9
6 . 0 / 3 . 6
3 . 7
J a n u a r y 1 9 9 5
P R
A l i v e
1 9
7 9
M
1 . 0
4 . 9 / 1 . 9
3 . 5
F e b r u a r y 1 9 9 5
C R
A l i v e
2 0
7 5
M
1 . 0
4 . 0 / 1 . 7
4 . 5
F e b r u a r y 1 9 9 5
P R
A l i v e
2 1
5 3
M
0 . 6
5 . 9 / 3 . 7
2 . 5
M a r c h 1 9 9 5
P R
A l i v e
2 2
6 6
F
1 . 1
5 . 2 / 3 . 0
2 . 3
A p r i l 1 9 9 5
C R
A l i v e
2 3
6 5
M
0 . 8
4 . 8 / 1 . 9
1 0 . 0
J u n e 1 9 9 5
C R
A l i v e
2 4
4 9
F
0 . 4
6 . 6 / 4 . 0
1 . 8
A u g u s t 1 9 9 7
C R
A l i v e
2 5
6 0
F
0 . 5
5 . 2 / 2 . 7
6 . 0
J u n e 1 9 9 8
C R
A l i v e
C a s e n o s 1 – 1 0 , m a l i g n a n c y g r o u p ; c a s e n o s 1 1 – 2 5 ,
i d i o p a t h i c g r o u p .
S C r , s e r u m
c r e a t i n i n e ; T . P
/ A l b , s e r u m
t o t a l p r o t e i n / a l b u m i n ; N A , n o t a v a i l a b l e ; I R ,
i r r a d i a t i o n ; C R , c o m p l e t e r e m i s s i o n ; P R , p a r t i a l r e m i s s i o n .
576 H. Ohtani et al .

7/28/2019 Distribution of Subclass IgG
http://slidepdf.com/reader/full/distribution-of-subclass-igg 4/6
intensity of IgG4 between the two groups. Interestingly,Ullenhag et al . [19] demonstrated IgG1, IgG2 andIgG4 responses against vaccination with the recombi-nant carcinoembryonic antigen in combination withgranulocyte–macrophage colony-stimulating factor. A
recent review by Holdsworth et al . [20] assessed therelevance of Th1/Th2 responses to a variety of antigenswith IgG subclass profiles in mice and humans. HumanIgG1 and IgG2 are Th1-related isotypes [interleukin(IL)-12 and interferon- driven], while IgG4 is a Th2-related isotype (IL-4 driven). In malignant diseases,both the tumour itself and several tumour-relatedproducts can act as antigens. Certain ILs activatedby these various antigens may stimulate IgG1- andIgG2-mediated mechanisms (Th1-type), as well as theIgG4-mediated mechanism (Th2-type).
Several investigators have indicated that there is aclear association between MN and malignancy [10–12].This association is of clinical importance since protein-
uria may be the first sign of occult malignancy.Although the present study had a limited methodo-logical approach and small sample size, the datain Table 4 indicate that the glomerular IF intensity of IgG1 and IgG2 could be used as a possible predictor of M-MN. In addition, it would be prudent to analyseglomerular IgG subclass deposits in patients with MN,especially in those over the age of 40 who have clinicalor laboratory evidence of possible occult malignancy.When a strong glomerular deposition of IgG1 andIgG2 is observed, we recommend careful examinationfor malignancy in such cases.
Table 2. Histological findings in 10 patients with M-MN and 15 patients with idiopathic MN
Caseno.
Mesangialproliferation
Stage of MN
Glomerular IF intensity
IgG IgA IgM C3 C1q Fibrinogen
1 (–) 3 3 1 1 3 2 0.5 0.5 12 Mild 2 2 1 0.5 2 2 1 0 13 Mild 1–2 2 0 1 2 2 1 0 0
4 Mild 1 2 0 1 3 2 2 0 05 Mild 2 3 0.5 1 2 2 0 0 0.56 (–) 1 3 0.5 0 2 2 1 1 0.57 Mild 2 3 0 0 3 3 2 0 08 Mild 2 3 1 0.5 3 3 2 0.5 19 Mild 2 3 1 1 2 2 0 0 0
10 Mild 1 2 0 0 2 2 0.5 0.5 011 (–) 2–3 3 1 1 2 2 1 0 012 Mild 2 3 1 1 3 3 2 0 213 Mild 1 2 2 1 2 2 2 0 014 Mild 1–2 2 0.5 0 2 2 0.5 0 0.515 (–) 1–2 3 0 0 2 2 0 0 016 Mild 1–2 3 0.5 2 3 3 0 0 017 Mild 1 3 0 0.5 3 2 2 0.5 018 Mild 2 3 2 1 3 2 0 0 019 Mild 1–2 3 1 1 3 3 2 0 120 Mild 2 3 0 0 2 2 3 0 2
21 Mild 2 3 0.5 0.5 3 2 0 0 0.522 (–) 1–2 3 0 0 3 3 2 0 123 Mild 2 3 0 1 2 2 2 0 0.524 Mild 2 2 1 1 2 2 0.5 0 125 Mild 2 3 0.5 0.5 3 3 2 0 0
Case nos 1–10, malignancy group; case nos 11–25, idiopathic group.
Table 3. IF intensity of glomerular IgG subclass deposits in 10patients with M-MN and 15 patients with idiopathic MN
Case no. IgG1 IgG2 IgG3 IgG4
1 0.0 0.5 0.0 1.02 1.0 2.0 0.5 0.03 2.0 2.0 1.0 2.04 3.0 3.0 0.5 0.55 1.0 0.5 1.0 2.06 2.0 1.0 1.0 0.57 3.0 3.0 0.5 3.08 2.0 2.0 0.5 0.59 0.0 1.0 0.0 2.0
10 1.0 1.0 0.5 0.511 2.0 1.0 0.0 3.012 1.0 0.0 0.0 2.013 0.0 1.0 0.0 2.014 0.0 0.0 0.0 2.015 1.0 0.0 0.0 1.016 1.0 1.0 0.5 3.017 1.0 1.0 1.0 3.0
18 0.5 2.0 0.0 3.019 0.5 0.5 0.5 3.020 0.0 0.0 1.0 0.021 0.0 0.0 0.0 1.022 0.5 1.0 0.0 3.023 0.5 1.0 0.0 2.024 0.0 1.0 0.0 1.025 0.5 0.5 1.0 3.0
Case nos 1–10, malignancy group; case nos 11–25, idiopathicgroup.
IgG subclasses in malignancy-associated MN 577

7/28/2019 Distribution of Subclass IgG
http://slidepdf.com/reader/full/distribution-of-subclass-igg 5/6
Fig. 2. IF study of a patient with idiopathic MN (case 19). IgG4 was graded as 3þ (score: 3.0), and IgG1, IgG2 and IgG3 were all weaklypositive (score: 0.5).
Fig. 1. IF study of a patient with M-MN (case 3). IgG1, IgG2 and IgG4 were graded as 2þ (score: 2.0), and IgG3 was 1þ (score: 1.0).
578 H. Ohtani et al .

7/28/2019 Distribution of Subclass IgG
http://slidepdf.com/reader/full/distribution-of-subclass-igg 6/6
Conflict of interest statement. None declared.
References
1. Parslow TG. Immunoglobulins and immunoglobulin genes. In:
Foltin J, Nogueira I, Holton B, eds. Medical Immunology, 10th
edn. McGraw-Hill, New York; 2001: 95–1142. Spiegelberg HL. Biological activities of immunoglobulins of
different classes and subclasses. Adv Immunol 1974; 19: 259–294
3. Doi T, Mayumi M, Kanatsu K, Suehiro F, Hamashima Y.
Distribution of IgG subclasses in membranous nephropathy.
Clin Exp Immunol 1984; 58: 57–624. Noe ¨l L-H, Aucouturier P, Monterio RC, Preud’homme J-L,
Lesavre P. Glomerular and serum immunoglobin G subclasses
in membranous nephropathy and anti-glomerular basementmembrane nephritis. Clin Immunol Immunopathol 1988; 46:
186–194
5. Aucouturier P, Monteiro RC, Noe ¨l LH, Preud’homme JL,
Lesavre P. Glomerular and serum immunoglobulin Gsubclasses in IgA nephropathy. Clin Immunol Immunopathol
1989; 51: 338–347
6. Haas M. IgG subclass deposits in glomeruli of lupus and
nonlupus membranous nephropathies. Am J Kidney Dis 1994;
23: 358–3647. Imai H, Hamai K, Komatsuda A, Ohtani H, Miura AB. IgG
subclasses in patient with membranoproliferative glomerulone-
phritis, membranous nephropathy, and lupus nephritis. Kidney
Int 1997; 51: 270–2768. Nagahama K, Matsushita H, Hara M et al . Bucillamine
induces membranous glomerulonephritis. Am J Kidney Dis
2002; 39: 706–712
9. Oliveira DBG. Membranous nephropathy: an IgG4-mediateddisease. Lancet 1998; 351: 670–671
10. Yamauchi H, Linsey MS, Biava CG, Hopper J Jr. Cure of
membranous nephropathy after resection of carcinoma. Arch
Intern Med 1985; 145: 2061–2063
11. Brueggemeyer CD, Ramirez G. Membranous nephropathy: a
concern for malignancy. Am J Kidney Dis 1987; 9: 23–26
12. Burstein DM, Korbet SM, Schwartz MM. Membranous
glomerulonephritis and malignancy. Am J Kidney Dis 1993;22: 5–10
13. Coltharp WH, Lee SM, Miller RF, Averbuch MS. Nephrotic
syndrome complicating adenocarcinoma of the lung withresolution after resection. Ann Thorac Surg 1991; 51: 308–309
14. Ashman N, Steele JPC, Sheaff M, Rudd RM, Onwubalili J.
Membranous nephropathy resolving with treatment of bron-
chial carcinoid tumor. Am J Kidney Dis 2000; 36: E1515. Silcocks PBS. Measuring repeatability and validity of
histological diagnosis—a brief review with some practical
examples. J Clin Pathol 1983; 36: 1269–1275
16. Costanza ME, Pinn V, Schwarz RS, Nathanson L.Carcinoembryonic antigen–antibody complexes in a patient
with colonic carcinoma and nephrotic syndrome. N Engl J Med
1973; 289: 520–52217. Couser WG, Wagonfeld JB, Spargo BH, Lewis EJ. Glomerular
deposition of tumor antigen in membranous nephropathyassociated with colonic carcinoma. Am J Med 1974; 57:
962–97018. Borochovitz D, Kam WK, Nolte M, Graner S, Kiss J.
Adenocarcinoma of the palate associated with nephrotic
syndrome and epimembranous carcinoembryonic antigen
deposition. Cancer 1982; 49: 2097–2102
19. Ullenhag GJ, Fro ¨ din J-E, Striga ˚ rd K, Mellstedt H, MagnussonCGM. Induction of IgG subclass responses in colorectal
carcinoma patients vaccinated with recombinant carcinoem-
bryonic antigen. Cancer Res 2002; 62: 1364–1369
20. Holdsworth SR, Kitching AR, Tipping PG. Th1 and Th2T helper cell subsets affect patterns of injury and outcomes in
glomerulonephritis. Kidney Int 1999; 55: 1198–1216
Received for publication: 31.3.03Accepted in revised form: 18.9.03
3
2
1
0.5
0
IgG1 IgG2 IgG3 IgG4
M I M I M I M I
* *
Fig. 3. IF intensities of glomerular IgG subclasses in patients withM-MN and idiopathic MN. Box and whisker plots of the data arein Table 3. The lower bar indicates the lower extreme; the upperbar, the upper extreme; the lower line of the box, the lower quartile;the upper line of the box, the upper quartile; and the circle showsthe median. The intensities of IgG1 and IgG2 in the malignancygroup (M) are significantly stronger than in the idiopathic group(I). *P<0.05.
Table 4. IF intensity of glomerular IgG1 and IgG2 deposits in 10patients with M-MN and 15 patients with idiopathic MN
Complication of malignancy
Yes (n¼10) No (n¼15)
IF scores of IgG1 1.0and IgG2 1.0
7 3
IF scores of IgG1<1.0or IgG2<1.0
3 12
Sensitivity/specificity 70/80%
IgG subclasses in malignancy-associated MN 579